
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Pediatr., 10 March 2025
Sec. Pediatric Gastroenterology, Hepatology and Nutrition
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1523613
 Rosan Meyer1*
Rosan Meyer1* Lauren Arpe2
Lauren Arpe2 Aydan Kansu3Veronica Kelly4
Aydan Kansu3Veronica Kelly4 Keith Lindley2Mairéad O'Meara4Maria del Carmen Rivero5
Keith Lindley2Mairéad O'Meara4Maria del Carmen Rivero5 Suzanne van Zundert6Saioa Vicente-Santamaría7
Suzanne van Zundert6Saioa Vicente-Santamaría7 Orjena Žaja8
Orjena Žaja8 Elena Oliveros9Leanne Olivier10
Elena Oliveros9Leanne Olivier10 Koen Joosten11
Koen Joosten11
Undernutrition is defined as “a condition resulting from imbalanced nutrition or abnormal utilization of nutrients.” In this paper, the term malnutrition is used to refer to undernutrition. Malnutrition may be driven by poor socioeconomic conditions or by disease, and it is estimated that disease-related malnutrition (DRM) impacts up to 28% of hospitalized children in Europe. Malnutrition results in alterations in gastrointestinal function that lead to malabsorption of macro- and micro-nutrients. It can lead to altered gut motility and a deficiency of stomach acid, which can result in intestinal colonization by pathogens, causing diarrhoea and high burdens of intestinal infection. The presence of compromised gastrointestinal function in children with DRM is critical as it negatively impacts the efficacy of nutritional support and recovery. When choosing novel strategies and nutritional therapies for malnourished children, consideration should be given to gut-protective interventions that promote better treatment tolerance. When breastmilk is unavailable, whole protein feeds are currently considered as first-line treatment for malnutrition in children with a normal functioning gastrointestinal tract. However, peptide-based feeds have been associated with improved gastrointestinal tolerance and absorption, reduced diarrhoea, reduced inflammation, improved growth and have restored gut integrity compared with free amino acid and whole-protein feeds. At a recent meeting, experts in this area have identified significant research gaps in the literature on peptide-based feeds in children and possible gaps in clinical practice. Whilst the group acknowledges that further work is needed, this paper provides an overview on this topic to further drive research in this area.
Paediatric undernutrition is defined by the European Society for Paediatric Gastroenterology, Hepatology & Nutrition (ESPGHAN) as “a condition resulting from imbalanced nutrition or abnormal utilization of nutrients which causes clinically meaningful adverse effects on tissue function and/or body size/composition with subsequent impact on health outcomes” (1). Whilst the term malnutrition encompasses both undernutrition and overnutrition, malnutrition is extensively used to refer to undernutrition and will be used in this context throughout. The World Health Organization (WHO) has established anthropometric indicators (z scores) for malnutrition diagnosis. Undernutrition presents in four broad forms: wasting (low weight-for-height), often indicating recent or severe weight loss due to inadequate food intake and/or infectious disease; stunting (low height-for-age), linked to chronic or recurrent undernutrition and factors like poverty, poor maternal health and nutrition, frequent illness and/or inappropriate early-life care; and underweight (low weight-for-age), which may also involve stunting, wasting, or both; there is another form of malnutrition that refers to deficiencies in vitamins and minerals, called hidden hunger (2). In 2022, 149 million children under the age of 5 years were estimated to be stunted and 45 million were estimated to be wasted (2).
Disease-related malnutrition (DRM) impacts up to 28% of hospitalized children in Europe, depending on the country, patient population and diagnostic criteria used (3, 4). In addition, DRM has been shown to be associated with increased healthcare costs for hospitalized children (5). Malnutrition can affect gastrointestinal function, resulting in alterations in intestinal blood flow, pancreatic exocrine insufficiency, villus atrophy and increased intestinal permeability leading to loss of digestive enzymes, malabsorption of carbohydrate, fat, protein and other nutrients, secondary lactose intolerance, loss of absorption in the colon and diarrhoea (6–9). As a result of this, the impaired absorption of available nutrients during the treatment of malnutrition together with the risk of refeeding-mediated diarrhoea can affect the speed and extent of recovery (10). Furthermore, malnutrition can lead to altered gut motility and a deficiency of stomach acid which, combined with impaired cell immunity, can result in intestinal colonization by pathogens causing diarrhoea and high burdens of intestinal infection (6, 7, 11, 12).
Novel strategies and therapies are needed to provide nutritional support for affected individuals, to improve the effect of nutritional intervention and also to target other aspects of malnutrition such as inflammation and malabsorption (10, 12). A UK national survey across four tertiary paediatric centres involving 191 children with a median age of 19 months reported that 17% were on amino acid-based feeds and 83% were on extensively hydrolysed feeds for conditions other than cow's milk allergy. Whilst specialized feeds are commonly used in clinical practice, the evidence-based research supporting the use of these different types of feed was scarce (13).
This article focuses on key gastrointestinal changes that occur in malnutrition, the impact that some of these changes can have when providing nutritional support to malnourished paediatric patients, including the challenge of tolerance, and nutritional considerations when making feed choices (when breastmilk is insufficient or not available) in children over 1 year of age, utilizing a methodological literature search to review the available evidence and extract relevant published articles.
The PubMed, EMBASE and Dimensions databases were searched up to August 2023 using the search terms: peptide-based/hydrolysed/semi-elemental formula/feed AND malnutrition AND children/pediatric/paediatric; peptide-based/hydrolysed/semi-elemental formula/feed AND undernutrition AND children/pediatric/paediatric; peptide-based/hydrolysed/semi-elemental formula/feed AND failure to thrive/faltering growth AND children/pediatric/paediatric; peptide-based/hydrolysed/semi-elemental formula/feed AND malabsorption AND children/pediatric/paediatric.
Initially, 660 articles were identified in the PubMed and EMBASE databases and 500 articles in the Dimensions database. These were reviewed for relevance by two reviewers, with a third to resolve any disputes. Inclusion criteria included: articles in English language, full text articles, randomized controlled trials, case cohort studies, retrospective observational studies and review papers. Exclusion criteria included: studies in infants, adolescent or adults, preclinical studies, no peptide-based feeds studies or studies evaluating irrelevant outcomes for the purpose of this paper. After considering the inclusion and exclusion criteria, 643 and 498 articles were excluded and the number of relevant articles to 19, comprising 12 clinical studies and 7 review articles. This included all publications that conformed to the inclusion criteria. Supplementary Figure S1 and Table S1 provide details of each included publication.
The recent 2023 WHO guideline on the prevention and management of wasting in infants and children under 5 years of age recommends that all infants and young children should be triaged as soon as they enter a health facility or have contact with a health worker to ensure that those with emergency or danger signs receive immediate life-saving care. In addition, the identification of nutritional status is a vital aspect of the initial assessment to ensure that children with malnutrition receive prompt and appropriate nutritional interventions (14). The WHO definitions for moderate and severe paediatric malnutrition using a single data point are well established and include weight-for-height z score, body mass index (BMI)-for-age z score, mid upper arm circumference (MUAC) z score (for all three, moderate: −2 to −2.9; severe: −3 or below), and length/height-for-age z score (moderate: −2 to −3; severe: below −3) (14). Easy-to-use tools such as the MUAC z score tape are readily available and may help with the accurate and early identification of children at risk (15, 16). In particular, the MUAC z score tape can provide a more reliable assessment in children with neurological conditions such as cerebral palsy due to the challenges with joint contractures, movement disorders and muscle atrophy. It may also be helpful in patients with fluid shifts such as ascites or oedema as well as patients with hepato-/splenomegaly or solid tumor mass where body weight may be affected (17) (see Supplementary Material).
The main purpose of the gastrointestinal tract is to provide nutrients to the body by digesting food into small fragments that are absorbed into the blood. Childhood malnutrition has been reported to affect digestive physiology and result in impaired reabsorption of bile salts, excessive bile salt deconjugation, pancreatic exocrine insufficiency (reduced lipase, trypsin, chymotrypsin, and amylase secretion) and impaired intestinal cell function (reduced disaccharidase content, and terminal ileal dysfunction) (6–9). In addition, intestinal bacterial overgrowth (SIBO) and diarrhoea in childhood malnutrition can result in alterations of the gut microbiota and further diarrhoea (10, 12).
The small intestine is responsible for most of the nutrient absorption and is covered in finger-like projections called villi which increase its surface area, providing a larger area for absorption to occur. Together, these microvilli form the brush border of the intestinal epithelial cells. In malnutrition, there is a histological impact which results in thinning of the intestinal wall and the mucosal lining together with reduced height of the brush border. There is also a predominance of cuboidal rather than columnar mucosal cells (18). This thinning of the intestinal wall and the mucosal lining increases gut permeability and negatively impacts the absorption of amino acids, proteins, carbohydrates, lipids, electrolytes, and other micronutrients (19, 20). Malnutrition has also been documented to be associated with altered intestinal blood flow, reduced villus height and villus atrophy, crypt hyperplasia and marked cellular infiltration (inflammation) in the lamina propria in adults (21) and in children aged between 12 and 18 months with possible environmental enteric dysfunction (22) (Figure 1). These changes result in decreased availability of absorptive surface area leading to impaired nutrient absorption.
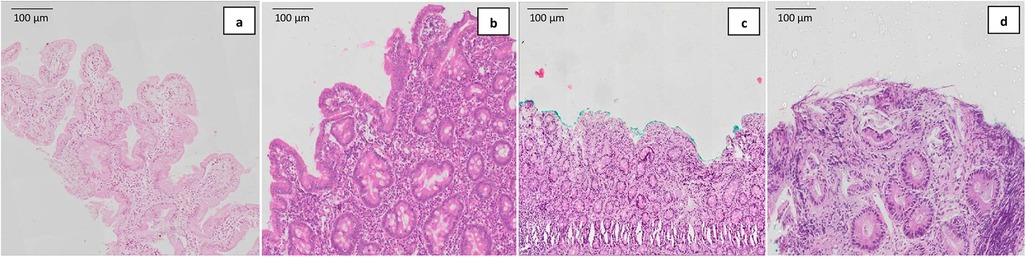
Figure 1. Representative histological images of: (a) normal villous architecture, (b) mild villous atrophy, (c) subtotal villous atrophy, and (d) total villous atrophy with crypt hyperplasia obtained using hematoxylin and eosin (H&E) stain in stunted Bangladeshi children aged between 12 and 18 months with possible environmental enteric dysfunction. Figure reproduced from Hossain et al. (22). This work is licensed under Creative Commons (CC by 4.0 https://creativecommons.org/licenses/by/4.0/).
Most of the nutrient absorption, including macronutrients, occurs in the small intestine. Carbohydrates, lipids, and proteins are absorbed differently, and malnutrition can negatively impact the absorptive capacity.
Once digested, carbohydrates are broken down into monosaccharides and absorbed into intestinal mucosal cells by either active transport (glucose and galactose) or facilitated transport (fructose). The reduced villus height and/or villus blunting observed in the small intestine of malnourished children can lead to a reduced intestinal capacity for carbohydrate digestion and absorption (23), effects that are also observed in adults (21). Furthermore, lactose intolerance may develop in some children due to secondary lactase deficiency (23, 24). The resulting accumulation of unabsorbed carbohydrates in the gastrointestinal tract leads to increased water retention within the bowel and increased flow through the bowel, causing osmotic diarrhoea (12, 23).
Absorption of peptides and amino acids occurs in the intestine via a dual protein-carrier system (Figure 2) consisting of two separate, independent, non-competing transport systems. One system carries free amino acids that are absorbed via active transport across the intestinal wall and then enter the portal vein; the other carries di- and tripeptides that are absorbed across the intestinal wall where they are hydrolysed by intracellular peptidases into amino acids and then absorbed into the portal vein (27). The two protein carrier systems operate independently and noncompetitively, meaning the efficiency of one system does not affect the other. Hydrolyzed protein systems, which contain both free amino acids and short-chain peptides, utilise these independent carrier systems to deliver protein-derived nitrogen into the portal circulation more rapidly than formulas containing only free amino acids or intact protein. This enhances nitrogen absorption.
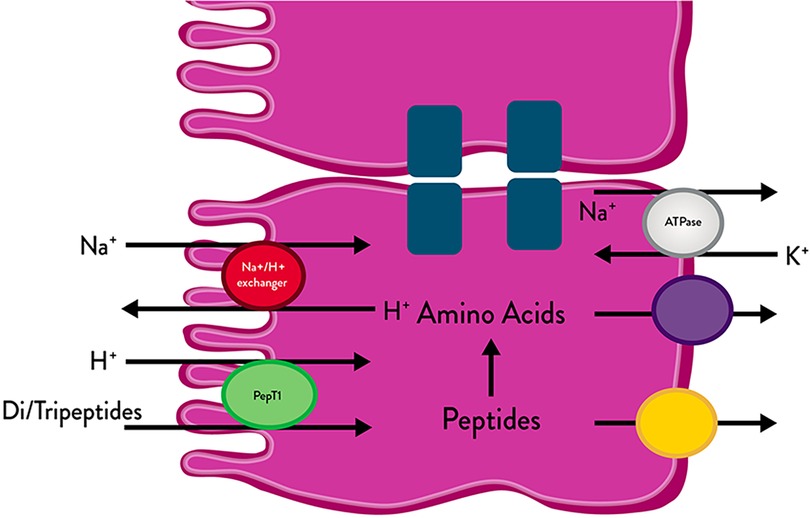
Figure 2. Di- and tripeptide transport across the gastrointestinal epithelium. Figure adapted from Jackman et al. (25) and Adibi (26).
In malnourished children, protein maldigestion and malabsorption are considered likely due to pancreatic insufficiency (i.e., when there is a reduction in the production of pancreatic enzymes and hence reduced digestion and absorption of nutrients) and villus atrophy in the small intestine, as well as increased protein loss due to increased intestinal permeability (20). The resultant deficiency of specific essential amino acids can further worsen gastrointestinal mucosal atrophy and so reduce protein absorption even further (11, 18). Malnutrition has dramatic effects on small intestinal mucosal structure and transport function. Peptide transport is less affected by malnutrition, injury, and disease than free amino acid transport.
In pathological states with impaired mucosal absorption, peptide absorption is less severely affected than free amino acid absorption (28). One possible reason for this is because peptide transport systems are more efficient and rapid than the uptake of free amino acids (29). The existence of specific peptide carrier systems in the intestinal brush border that are independent of free amino acid carrier systems are thought to be of importance in the effective treatment of patients with intestinal malabsorption (30, 31).
In addition to the efficient and rapid uptake of di- and tripeptides compared with free amino acids, studies have indicated an improved gastrointestinal tolerance with peptide-based diets, with the rate of absorption and the degree of tolerance being dependent on the presence of small molecular weight di- and tripeptides (28).
Long chain triglycerides (LCTs) are hydrolysed within the lumen of the small intestine by the pancreatic enzyme lipase through bile salts. The resulting products, bile salts and lecithin form mixed micelles that are absorbed into the enterocytes. Fatty acids and monoglycerides are absorbed into the enterocytes where they are re-synthesized into triglycerides and packaged into chylomicrons that are transported to the blood via the thoracic duct. Medium-chain triglycerides (MCTs) are absorbed by a different process, being hydrolysed more rapidly and effectively, and since the process does not depend on pancreatic lipolysis, go directly to the liver via the portal vein.
When this fat absorption step fails, steatorrhea develops. Protein intake can affect the severity of steatorrhea and the levels of triglycerides and free fatty acids in the faeces, suggesting that a change in lipolytic activity is not the primary reason for the increase in fat in the faeces that is observed in malnutrition (18). Furthermore, abnormalities in the gastrointestinal handling of lipids together with impaired lipid solubilization and/or hydrolysis can contribute to the malabsorption of fats (32). Bacterial overgrowth in the small bowel in children can also contribute to changes in fat absorption (32). In addition, diarrhoea-related reduction in the concentrations of conjugated bile acids observed in malnutrition leads to steatorrhea (18).
Due to the impact of protein deficiency on fat absorption, improvement in fat absorption is thought to occur concomitantly with protein repletion, reaching normality in the absence of diarrhoea and after restoration of body protein (18, 33).
The WHO has clear guidance with a stepwise approach to the management of both chronic and acute malnutrition, together with that of refeeding syndrome which may occur in severely malnourished patients receiving nutritional rehabilitation (orally, enterally or parenterally) (14, 34).
Appropriate nutritional support in malnourished children is critical for long-term development and survival. Metabolic disturbances such as refeeding syndrome or hypoglycemia may occur when rapid and excessive food intake is given to severely malnourished individuals. Refeeding syndrome reflects the change from catabolic to anabolic metabolism and may cause serious clinical complications and pathophysiological changes such as hypophosphatemia, hypomagnesemia, hypokalemia, vitamin deficiency and fluid retention during refeeding (35, 36).
Monitoring key parameters such as vital functions, fluid balance, plasma biochemistry and urinary electrolytes, heart rate, ventilatory functions, and blood gases is of paramount importance during the refeeding phase of nutritional support. It is critical that energy, protein and micronutrient intakes are adjusted, depending on the phase of the rehabilitation, as per WHO guidelines (14), and gradually increased until daily nutritional requirements, including those for catch-up growth are met (35, 36). As previously mentioned, a number of different types of feed are available.
Most data have been published on the use of whole protein feeds in malnutrition and these are considered the first-line treatment option (14, 37). However, as a result of the impaired gastrointestinal function and severe mucosal abnormalities and malabsorption observed in malnourished children, tolerability can be an issue in some children receiving whole protein feeds leading to gastrointestinal symptoms including nausea, vomiting, alteration of bowel movements, gastroesophageal reflux symptoms, and/or abdominal pain (38). Many children with DRM also have underlying diagnoses that impair gastrointestinal function and further exacerbate the problem of tolerance. For example, children with congenital heart disease suffer from protein-losing enteropathy and abnormal gut perfusion and/or hypoxemia to the gut which can lead to dysbiosis and intestinal barrier dysfunction (39, 40). Such tolerability issues and symptoms have been reported to frequently interrupt enteral nutrition undertaken either in the home or hospital setting (38, 41–43).
Once a patient develops intolerance to a whole protein feed the best clinical approach remains undetermined, with lack of consensus guidance due to limited data in the literature. Dilution of feeds to achieve adequate tolerance and to prevent diarrhoea is not an appropriate approach in malnourished children given that they are already nutritionally compromised (44, 45). Providers may utilize strategies to reduce diarrhoea such as adding or removing fiber, slowing down feeding rate, adding pre- or probiotics, or changing to alternative formulas, which may includacid or peptide-based feeds (46, 47). At present, there is paucity of data to define which type of feed should be used second line when intolerance to a whole protein feed develops.
Feeds consisting of protein in the form of free amino acids are available (28, 48). These feeds are primarily used for the treatment of cow's milk protein allergy (CMPA) and other gastrointestinal conditions, and not specifically for malnutrition, where absorption of free amino acids has been shown to be less efficient than peptide absorption (13, 28). Intestinal inflammation in food allergy responds well to exclusion of the offending dietary antigen or, if the offending antigen is unknown, a hypoallergenic elemental feed composed of single amino acids (49). However, a study in 95 children aged 6–23 months with complicated severe acute malnutrition reported no difference in the level of intestinal inflammation or clinical benefits in those randomized to either a standard feed, an elemental feed or a polymeric feed for 14 days (50). Amino acid-based feeds can induce vomiting, diarrhoea and electrolyte imbalance as a result of their high osmolality (28, 51) so require careful monitoring when used.
The development of peptide-based feeds is a significant milestone in the advancement of nutritional care of nutritionally compromised patients. Peptide-based feeds contain protein in the form of di- and tripeptides, which are absorbed via specific and discrete uptake systems in the gastrointestinal tract that are considered to be more rapid and efficient than those for free amino acids (52). There are emerging data to support the use of peptide-based feeds in patients who are intolerant to whole protein feeds in paediatric (and adult) populations (38, 53–55). Peptide-based feeds are associated with improved gastrointestinal tolerance, a lower risk of diarrhoea, and a better maintained and/or restored gut integrity compared with free amino acid or whole protein feeds (54, 56). Studies have suggested improved weight gain and growth associated with peptide-based feeds in different paediatric populations (54, 56, 57) (Table 1). Additionally, there may be some benefit in the management and prevention of functional gastrointestinal disorders, and it is thought that peptide-based feeds might be closer to the protein composition of human milk than intact cow's milk protein (59, 60).
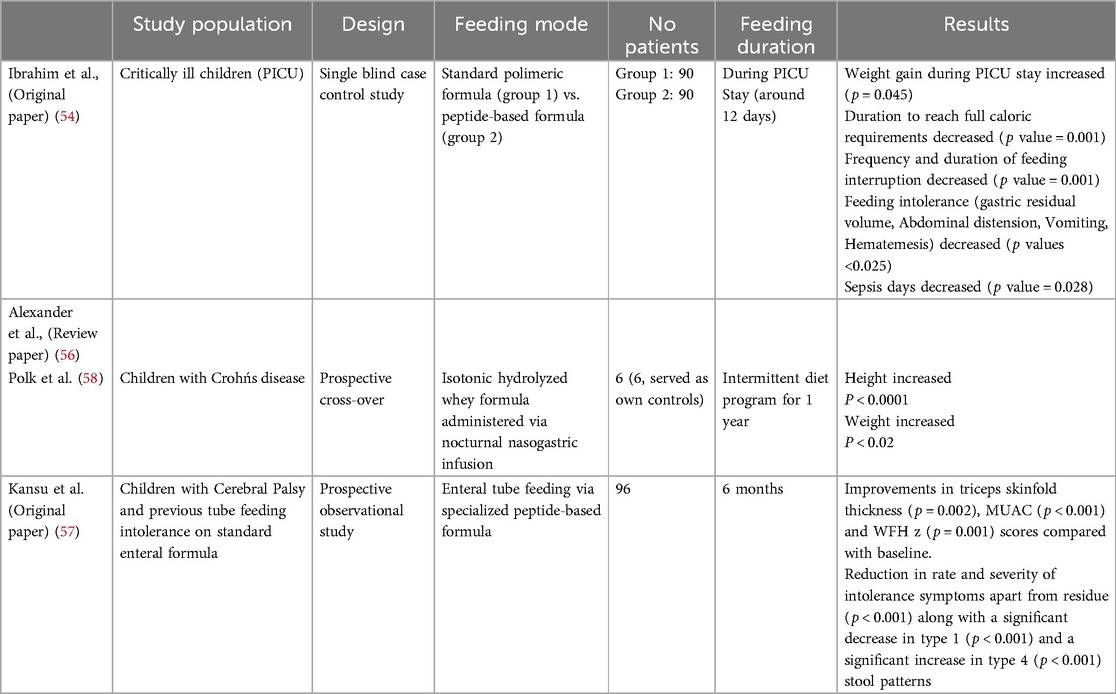
Table 1. Summary of peptide-based feeds clinical positive results on growth and tolerance.
Often the increase in energy density of feeds is achieved by increasing the lipid content, but caution is needed as children with severe malnutrition have dysfunctional lipid metabolism (32). The fat component in peptide-based feeds, which can vary considerably in type and amount, is often in the form of MCTs, which have a smaller molecular weight than LCTs and can be hydrolysed faster and more completely (38).
The carbohydrate component of peptide-based feeds mainly consists of glucose oligosaccharides, which are metabolized during luminal hydrolysis and mucosal absorption (28). However, the stimulation of insulin secretion by carbohydrates in malnourished children may result in the development of refeeding syndrome. Individual circumstances including the phase of disease should be considered when initiating nutritional support to avoid overfeeding (35, 36, 61).
It should be noted that some peptide-based feeds do not contain any fiber, but different types of fiber can be added separately if required (see Supplementary Material).
Malnutrition in children is often associated with a considerable number of pathophysiological gastrointestinal changes, including increased permeability, inflammation, malabsorption and diarrhoea. These changes in gastrointestinal function observed in malnourished children negatively impact the efficacy of nutritional support and increase the likelihood of patients initially experiencing worsening gastrointestinal symptoms, both of which combine to increase the time taken to recover from malnutrition. Hence, when choosing nutritional therapy in malnourished children with compromised gastrointestinal function, consideration should be given to gut-protective interventions that promote better treatment tolerance, are appropriate for the phase of the acute stress response (62) and improve long-term outcomes.
Whilst a whole protein feed is currently the first-line treatment for malnutrition, the use of peptide-based feeds in malnourished children have been associated with improved gastrointestinal tolerance and absorption, reduced diarrhoea, reduced inflammation and improved growth and have maintained/restored gut integrity compared with free amino acids and whole-protein feeds. This is believed to be due to their rapid and efficient absorption (28, 44, 54, 56). Peptide feeds currently face limitations such as higher costs and lower availability compared to whole protein feeds. However, emerging data indicate that peptide feeds may improve clinical outcomes, reduce healthcare utilization, and potentially lower overall care costs (63). The combined characteristics of more efficient uptake of di- and tripeptides and a lower osmolality of peptide feeds compared to amino acid feeds may be advantageous for enteral nutrition management of various disease states (56).
At present, due to a lack of research in this area, gaps in clinical practice exist. As clinical practice often relies on past experience for decision making in malnourished children, the sharing of best practices between healthcare professionals from different specialties may be beneficial as the role of peptide-based feeds becomes more established. Further research in this area is needed to fill these knowledge gaps.
The original contributions presented in the article are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
RM: Conceptualization, Investigation, Writing – review & editing. LA: Investigation, Writing – review & editing. AK: Investigation, Writing – review & editing. VK: Investigation, Writing – review & editing. KL: Investigation, Writing – review & editing. MO: Investigation, Writing – review & editing. Md: Investigation, Writing – review & editing. Sv: Investigation, Writing – review & editing. SV-S: Investigation, Writing – review & editing. OŽ: Investigation, Writing – review & editing. EO: Data curation, Investigation, Resources, Writing – review & editing. LO: Data curation, Investigation, Resources, Writing – review & editing. KJ: Investigation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article. Editorial assistance provided for this article was funded by Abbott.
Editorial assistance was provided by Inizio Evoke Comms.
EO is an employee of Abbott. LO is an employee of Abbott. Honorarium from Abbott was paid to the remaining authors to contribute to the discussion.
The authors declare that this study received funding from Abbott. The funder Abbott had the following involvement in the study: study design, collection, analysis, interpretation of data, the writing of this article, and the decision to submit it for publication.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1523613/full#supplementary-material
1. Hulst JM, Huysentruyt K, Gerasimidis K, Shamir R, Koletzko B, Chourdakis M, et al. Special interest group clinical malnutrition of ESPGHAN. A practical approach to identifying pediatric disease-associated undernutrition: a position statement from the ESPGHAN special interest group on clinical malnutrition. J Pediatr Gastroenterol Nutr. (2022) 74:693–705. doi: 10.1097/MPG.0000000000003437
2. World Health Organization. Malnutrition. (2024) Available online at: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed October 3, 2024).
3. Katsagoni CN, Cheirakaki O, Hatzoglou A, Zerva O, Koulieri A, Loizou K, et al. Malnutrition in hospitalised children — an evaluation of the efficacy of two nutritional screening tools. Nutrients. (2021) 13:1279. doi: 10.3390/nu13041279
4. Chourdakis M, Hecht C, Gerasimidis K, Joosten KF, Karagiozoglou-Lampoudi T, Koetse HA, et al. Malnutrition risk in hospitalized children: use of 3 screening tools in a large European population. Am J Clin Nutr. (2016) 103:1301–10. doi: 10.3945/ajcn.115.110700
5. Freijer K, van Puffelen E, Joosten KF, Hulst JM, Koopmanschap MA. The costs of disease related malnutrition in hospitalized children. Clin Nutr ESPEN. (2018) 23:228–33. doi: 10.1016/j.clnesp.2017.09.009
6. Amadi B, Besa E, Zyambo K, Kaonga P, Louis-Auguste J, Chandwe K, et al. Impaired barrier function and autoantibody generation in malnutrition enteropathy in Zambia. EBioMedicine. (2017) 22:191–9. doi: 10.1016/j.ebiom.2017.07.017
7. Saunders J, Smith T, Stroud M. Malnutrition and undernutrition. Medicine. (2019) 47:152–8. doi: 10.1016/j.mpmed.2018.12.012
8. Bartels RH, Meyer SL, Stehmann TA, Bourdon C, Bandsma RHJ, Voskuijl WP. Both exocrine pancreatic insufficiency and signs of pancreatic inflammation are prevalent in children with complicated severe acute malnutrition: an observational study. J Pediatr. (2016) 174:165–70. doi: 10.1016/j.jpeds.2016.04.013
9. Ferdous F, Filteau S, Schwartz NB, Gumede-Moyo S, Cox SE. Association of postnatal severe acute malnutrition with pancreatic exocrine and endocrine function in children and adults: a systematic review. Br J Nutr. (2023) 129(4):576–609. doi: 10.1017/S0007114522001404
10. Saunders J, Smith T. Malnutrition: causes and consequences. Clin Med. (2010) 10:624–7. doi: 10.7861/clinmedicine.10-6-624
11. Salazar-Lindo E, Allen S, Brewster DR, Elliott EJ, Fasano A, Phillips AD, et al. Intestinal infections and environmental enteropathy: working group report of the second world congress of pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. (2004) 39:S662–9. doi: 10.1097/00005176-200406002-00013
12. Bhutta ZA, Berkley JA, Bandsma RHJ, Kerac M, Trehan I, Briend A. Severe childhood malnutrition. Nat Rev Dis Primers. (2017) 3:17067. doi: 10.1038/nrdp.2017.67
13. Meyer R, Smith C, Sealy L, Mancell S, Marino LV. The use of extensively hydrolysed and amino acid feeds beyond cow's Milk allergy: a national survey. J Hum Nutr Diet. (2021) 34:13–23. doi: 10.1111/jhn.12794
14. World Health Organization. WHO guideline on the prevention and management of wasting and nutritional oedema (acute malnutrition) in infants and children under 5 years. (2023). Available online at: https://files.magicapp.org/guideline/a3fe934f-6516-460d-902f-e1c7bbcec034/published_guideline_7330-1_1.pdf (accessed October 3, 2024).
15. Miller MA, Mallory K, Escobedo M, Tarot AC, Abdel-Rahman S. Assessing effectiveness of a novel mid-upper arm circumference Z-score tape in a community setting in Guatemala. Arch Public Health. (2019) 77:44. doi: 10.1186/s13690-019-0370-0
16. Thaete K, Rowzer K, Stephens K, Abdel-Rahman SM. User-informed medical device development: a case study for pediatric malnutrition assessment. Glob Pediatr Health. (2019) 6:2333794X19861575. doi: 10.1177/2333794X19861575
17. Aydın K, Dalgıç B, Kansu A, Özen H, Selimoğlu MA, Tekgül H, et al. The significance of MUAC z-scores in diagnosing pediatric malnutrition: a scoping review with special emphasis on neurologically disabled children. Front Pediatr. (2023) 11:1081139. doi: 10.3389/fped.2023.1081139
18. Viteri FE, Schneider RE. Gastrointestinal alterations in protein-calorie malnutrition. Med Clin North Am. (1974) 58:1487–505. doi: 10.1016/S0025-7125(16)32085-5
19. Keusch GT, Denno DM, Black RE, Duggan C, Guerrant RL, Lavery JV, et al. Environmental enteric dysfunction: pathogenesis, diagnosis, and clinical consequences. Clin Infect Dis. (2014) 59(Suppl. 4):S207–12. doi: 10.1093/cid/ciu485
20. Semba RD, Shardell M, Trehan I, Moaddel R, Maleta KM, Ordiz MI, et al. Metabolic alterations in children with environmental enteric dysfunction. Sci Rep. (2016) 6:28009. doi: 10.1038/srep28009
21. Hossain MS, Begum SMKN, Rahman MM, Mazumder RN, Parvez M, Gazi MA, et al. Alterations in the histological features of the intestinal mucosa in malnourished adults of Bangladesh. Sci Rep. (2021) 11:2355. doi: 10.1038/s41598-021-82079-6
22. Hossain MS, Begum SMKN, Rahman MM, Parvez M, Mazumder RN, Sarker SA, et al. Environmental enteric dysfunction and small intestinal histomorphology of stunted children in Bangladesh. PLoS Negl Trop Dis. (2023) 17(1):e0010472. doi: 10.1371/journal.pntd.0010472
23. Kvissberg MA, Dalvi PS, Kerac M, Voskuijl W, Berkley JA, Priebe MG, et al. Carbohydrate malabsorption in acutely malnourished children and infants: a systematic review. Nutr Rev. (2016) 74:48–58. doi: 10.1093/nutrit/nuv058
24. Heyman MB. Lactose intolerance in infants, children and adolescents. Pediatrics. (2006) 118(3):1279–86. doi: 10.1542/peds.2006-1721
25. Jackman MJ, Davies NM, Bak A, Puri S. Landscape for oral delivery of peptides. In: Tyagi P, Subramony JA, editors. Oral Delivery of Therapeutic Peptides and Proteins. Academic Press (2022). p. 1–50. doi: 10.1016/B978-0-12-821061-1.00001-0
26. Adibi SA. Regulation of expression of the intestinal oligopeptide transporter (Pept-1) in health and disease. Am J Physiol Gastrointest Liver Physiol. (2003) 285:G779–88. doi: 10.1152/ajpgi.00056.2003
27. Kiela PR, Ghishan FK. Physiology of intestinal absorption and secretion. Best Pract Res Clin Gastroenterol. (2016) 30(2):145–59. doi: 10.1016/j.bpg.2016.02.007
28. Brinson RR, Hanumanthu SK, Pitts WM. A reappraisal of the peptide-based enteral formulas: clinical applications. Nutr Clin Pract. (1989) 4:211–7. doi: 10.1177/0115426589004006211
29. Sleisenger MH, Kim YS. Protein digestion and absorption. N Engl J Med. (1979) 300:659–63. doi: 10.1056/NEJM197906213002511
30. Adibi SA, Fogel MR, Agrawal RM. Comparison of free amino acid and dipeptide absorption in the jejunum of sprue patients. Gastroenterology. (1974) 15:494–501.
31. Milla PJ, Kilby A, Rassan UB, Ersser R, Harries JT. Small intestinal absorption at amino acids and a dipeptide in pancreatic insufficiency. Gut. (1983) 24:818–24. doi: 10.1136/gut.24.9.818
32. Murphy JL, Badaloo AV, Chambers B, Forrester TE, Wootton SA, Jackson AA. Maldigestion and malabsorption of dietary lipid during severe childhood malnutrition. Arch Dis Child. (2002) 87:522–5. doi: 10.1136/adc.87.6.522
33. Viteri FE, Flores M, Alvarado J, Béhar M. Intestinal malabsorption in malnourished children before and during recovery. Relation between severity of protein deficiency and the malabsorption process. Am J Dig Dis. (1973) 18:201–11. doi: 10.1007/BF01071974
34. Ashworth A, Khanum S, Jackson A, Schofield CE. (2003). Guidelines for the inpatient treatment of severely malnourished children. Available online at: https://iris.who.int/handle/10665/42724 (accessed October 3 2024).
35. Corsello A, Trovato CM, Dipasquale V, Bolasco G, Labriola F, Gottrand F, et al. Refeeding syndrome in pediatric age, an unknown disease: a narrative review. J Pediatr Gastroenterol Nutr. (2023) 77(6):e75–83. doi: 10.1097/MPG.0000000000003945
36. Krutkyte G, Wenk L, Odermatt J, Schuetz P, Stanga Z, Friedli N. Refeeding syndrome: a critical reality in patients with chronic disease. Nutrients. (2022) 14(14):2859. doi: 10.3390/nu14142859
37. World Health Organization (WHO). Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children. Geneva, Switzerland: World Health Organization (2013). Available online at: https://www.who.int/publications/i/item/9789241506328 (accessed October 3 2024).
38. Mohamed Elfadil O, Steien DB, Narasimhan R, Velapati SR, Epp L, Patel I, et al. Transition to peptide-based diet improved enteral nutrition tolerance and decreased healthcare utilization in pediatric home enteral nutrition. J Parenter Enteral Nutr. (2022) 46:626–34. doi: 10.1002/jpen.2202
39. Feng D, Christensen JT, Yetman AT, Lindsey ML, Singh AB, Salomon JD. The microbiome’s relationship with congenital heart disease: more than a gut feeling. J Congenit Heart Dis. (2021) 5:5. doi: 10.1186/s40949-021-00060-4
40. Clode M, Tran D, Majumdar A, Ayer J, Ferrie S, Cordina R. Nutritional considerations for people living with a Fontan circulation: a narrative review. Cardiol Young. (2024) 34(2):238–49. doi: 10.1017/S1047951123004389
41. Mundi MS, Mohamed Elfadil O, Abdelmagid MG, Patel A, Pattinson A, Epp L, et al. Home enteral nutrition program: a single tertiary referral center experience. Poster abstracts. J Parenter Enteral Nutr. (2022) 46(S1):S157–9.
42. Gungabissoon U, Hacquoil K, Bains C, Irizarry M, Dukes G, Williamson R, et al. Prevalence, risk factors, clinical consequences, and treatment of enteral feed intolerance during critical illness. J Parenter Enteral Nutr. (2015) 39(4):441–8. doi: 10.1177/0148607114526450
43. Wang K, McIlroy K, Plank LD, Petrov MS, Windsor JA. Prevalence, outcomes, and management of enteral tube feeding intolerance: a retrospective cohort study in a tertiary center. J Parenter Enteral Nutr. (2017) 41:959–67. doi: 10.1177/0148607115627142
44. Phillips EM, Short N, Turner C, Rece J. Peptide-based formulas: the nutraceuticals of enteral feedings. ECPN. (2005) 2005:40–4.29.
45. Selimoglu MA, Kansu A, Aydogdu S, Sarioglu AA, Erdogan S, Dalgic B, et al. Nutritional support in malnourished children with compromised gastrointestinal function: utility of peptide-based enteral therapy. Front Pediatr. (2021) 9:610275. doi: 10.3389/fped.2021.610275
46. Kambale RM, Nancy FI, Ngaboyeka GA, Kasengi JB, Bindels LB, Van der Linden D. Effects of probiotics and synbiotics on diarrhea in undernourished children: systematic review with meta-analysis. Clin Nutr. (2021) 40(5):3158–69. doi: 10.1016/j.clnu.2020.12.026
47. Whelan K, Schneider S. Mechanisms, prevention, and management of diarrhea in enteral nutrition. Curr Opin Gastroenterol. (2011) 27:152–9. doi: 10.1097/MOG.0b013e32834353cb
48. Koretz RL, Meyer JR. Elemental diets – facts and fantasies. Gastroenterology. (1980) 78:393–410. doi: 10.1016/0016-5085(80)90594-6
49. Hartman C, Eliakim R, Shamir R. Nutritional status and nutritional therapy in inflammatory bowel diseases. World J Gastroenterol. (2009) 15:2570–8. doi: 10.3748/wjg.15.2570
50. Bartels RH, Chimwezi E, Watson V, Pei L, Potani I, Allubha B, et al. Hypoallergenic and anti-inflammatory feeds in children with complicated severe acute malnutrition: an open randomised controlled 3-arm intervention trial in Malawi. Sci Rep. (2019) 9:2304. doi: 10.1038/s41598-019-38690-9
51. Verduci E, Salvatore S, Bresesti I, Di Profio E, Pendezza E, Bosetti A, et al. Semi-elemental and elemental formulas for enteral nutrition in infants and children with medical complexity-thinking about cow’s milk allergy and beyond. Nutrients. (2021) 13(12):4230. doi: 10.3390/nu13124230
52. Silk DB, Grimble GK, Rees RG. Protein digestion and amino acid and peptide absorption. Proc Nutr Soc. (1985) 44:63–72. doi: 10.1079/PNS19850011
53. Mundi MS, Velapati S, Kuchkuntla AR, Hurt RT. Reduction in healthcare utilization with transition to peptide-based diets in intolerant home enteral nutrition patients. Nutr Clin Pract. (2020) 35:487–94. doi: 10.1002/ncp.10477
54. Ibrahim H, Mansour M, El Gendy YG. Peptide-based formula versus standard-based polymeric formula for critically ill children: is it superior for patients’ tolerance? Arch Med Sci. (2020) 16:592–6. doi: 10.5114/aoms.2020.94157
55. Minor G, Ochoa JB, Storm H, Periman S. Formula switch leads to enteral feeding tolerance improvements in children with developmental delays. Glob Pediatr Health. (2016) 3:2333794X16681887. doi: 10.1177/2333794X16681887
56. Alexander DD, Bylsma LC, Elkayam L, Nguyen DL. Nutritional and health benefits of semi-elemental diets: a comprehensive summary of the literature. World J Gastrointest Pharmacol Ther. (2016) 7:306–19. doi: 10.4292/wjgpt.v7.i2.306
57. Kansu A, Kutluk G, Caltepe G, Arikan C, Urganci N, Tumgor G, et al. Use of a specialized peptide-based enteral formula containing mediumchain triglycerides for enteral tube feeding in children with cerebral palsy and previous tube feeding intolerance on standard enteral formula: a prospective observational TolerUP study. Front Pediatr. (2025) 13. doi: 10.3389/fped.2025.1448507
58. Polk DB, Hattner JA, Kerner JA Jr. Improved growth and disease activity after intermittent administration of a defined formula diet in children with crohn’s disease. J Parenter Enteral Nutr. (1992) 16(6):499–504. doi: 10.1177/0148607192016006499
59. Makola D. Elemental and semi-elemental formulas: are they superior to polymeric formulas? Pract Gastroenterol. (2005) 29:59–64 + 69.
60. Vandenplas Y, Ksiażyk J, Luna MS, Migacheva N, Picaud JC, Ramenghi LA, et al. Partial hydrolyzed protein as a protein source for infant feeding: do or don't? Nutrients. (2022) 14:1720. doi: 10.3390/nu14091720
61. Afroze F, Khoshnevisan F, Harawa PP, Islam Z, Bourdon C, Khoswe S, et al. Trajectories of resting energy expenditure and performance of predictive equations in children hospitalized with an acute illness and malnutrition: a longitudinal study. Sci Rep. (2024) 14(1):3613. doi: 10.1038/s41598-024-53791-w
62. Joosten KF, Kerklaan D, Verbruggen SC. Nutritional support and the role of the stress response in critically ill children. Curr Opin Clin Nutr Metab Care. (2016) 19(3):226–33. doi: 10.1097/MCO.0000000000000268
Keywords: disease-related malnutrition, gastrointestinal function, children, nutritional support, malabsorption, diarrhoea, peptide-based enteral therapy
Citation: Meyer R, Arpe L, Kansu A, Kelly V, Lindley K, O'Meara M, del Carmen Rivero M, van Zundert S, Vicente-Santamaría S, Žaja O, Oliveros E, Olivier L and Joosten K (2025) Gastrointestinal changes in paediatric malnutrition that may impact on nutrition choice. Front. Pediatr. 13:1523613. doi: 10.3389/fped.2025.1523613
Received: 6 November 2024; Accepted: 5 February 2025;
Published: 10 March 2025.
Edited by:
Thomai Karagiozoglou-Lampoudi, International Hellenic University, GreeceReviewed by:
Le Liu, Southern Medical University, ChinaCopyright: © 2025 Meyer, Arpe, Kansu, Kelly, Lindley, O'Meara, del Carmen Rivero, van Zundert, Vicente-Santamaría, Žaja, Oliveros, Olivier and Joosten. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosan Meyer, cm9zYW4ucmVzZWFyY2hAcm9zYW4tcGFlZGlhdHJpY2RpZXRpdGlhbi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.