
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 27 February 2025
Sec. Neonatology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1492716
 Sezin Unal1,†
Sezin Unal1,† Serdar Beken2*†,‡
Serdar Beken2*†,‡ Deniz Anuk Ince1
Deniz Anuk Ince1 Ozden Turan1
Ozden Turan1 Ayse Korkmaz Toygar2
Ayse Korkmaz Toygar2 Ayse Ecevit1
Ayse Ecevit1 Abdullah Baris Akcan3Mustafa Ali Akın4
Abdullah Baris Akcan3Mustafa Ali Akın4 Selma Aktas5
Selma Aktas5 Nukhet Aladag Ciftdemir6
Nukhet Aladag Ciftdemir6 Emel Altuncu7Huseyin Altunhan8
Emel Altuncu7Huseyin Altunhan8 Baran Cengiz Arcagok9
Baran Cengiz Arcagok9 Didem Armangil10Esra Arun Ozer11
Didem Armangil10Esra Arun Ozer11 Banu Aydın12Handan Bezirganoglu13
Banu Aydın12Handan Bezirganoglu13 Leyla Bilgin14Erhan Calısıcı15
Leyla Bilgin14Erhan Calısıcı15 Sebnem Calkavur16Kıymet Celik17
Sebnem Calkavur16Kıymet Celik17 Yalcın Celik18Bilin Cetinkaya19
Yalcın Celik18Bilin Cetinkaya19 Merih Cetinkaya20Atalay Demirel21
Merih Cetinkaya20Atalay Demirel21 Gamze Demirel22Nazan Neslihan Dogan23Pelin Doğan24Mehtap Durukan25
Gamze Demirel22Nazan Neslihan Dogan23Pelin Doğan24Mehtap Durukan25 Defne Engur26Tugba Erener Ercan27Zeynel Gokmen28Ipek Guney Varal29
Defne Engur26Tugba Erener Ercan27Zeynel Gokmen28Ipek Guney Varal29 Selvi Gulası30
Selvi Gulası30 Ayla Gunlemez31Tugba Gursoy32Handan Hakyemez Toptan33
Ayla Gunlemez31Tugba Gursoy32Handan Hakyemez Toptan33 Serif Hamitoğlu34Fatih Isleyen35
Serif Hamitoğlu34Fatih Isleyen35 Irem Iyigun36Sebnem Kader37Dilek Kahvecioğlu38
Irem Iyigun36Sebnem Kader37Dilek Kahvecioğlu38 Gozdem Kaykı39Murat Kostu40
Gozdem Kaykı39Murat Kostu40 Dilek Kurnaz41Tural Mammadalıyev42
Dilek Kurnaz41Tural Mammadalıyev42 Ilke Mungan Akin43Nejat Narlı44
Ilke Mungan Akin43Nejat Narlı44 Emel Okulu45
Emel Okulu45 Nilufer Okur46
Nilufer Okur46 Ozgur Olukman47
Ozgur Olukman47 Fahri Ovalı48Beyza Ozcan49Ahmet Ozdemir50Ozmert Ozdemir51
Fahri Ovalı48Beyza Ozcan49Ahmet Ozdemir50Ozmert Ozdemir51 Hilal Ozkan52Gonca Sandal53
Hilal Ozkan52Gonca Sandal53 Dilek Sarıcı54
Dilek Sarıcı54 Cansu Sivrikaya55
Cansu Sivrikaya55 Betul Siyah Bilgin56
Betul Siyah Bilgin56 Saime Sundus57
Saime Sundus57 Ozge Surmeli Onay58Huseyin Simsek59
Ozge Surmeli Onay58Huseyin Simsek59 Umit Ayse Tandırcıoğlu60
Umit Ayse Tandırcıoğlu60 Sema Tanrıverdi61
Sema Tanrıverdi61 Kadir Serafettin Tekgunduz62
Kadir Serafettin Tekgunduz62 Demet Terek63Gaffari Tunc64
Demet Terek63Gaffari Tunc64 Turan Tunc65
Turan Tunc65 Ercan Tutak66Eda Tufekcioğlu67
Ercan Tutak66Eda Tufekcioğlu67 Funda Tuzun Erdogan68Ersin Ulu69
Funda Tuzun Erdogan68Ersin Ulu69 Dilek Ulubas Isik70Nurdan Uras71Sait Ilker Uslu72Irem Unal73Fatma Hilal Yılmaz74Ariorad Moniri75
Dilek Ulubas Isik70Nurdan Uras71Sait Ilker Uslu72Irem Unal73Fatma Hilal Yılmaz74Ariorad Moniri75
Objective: Caffeine is a proven medication used for the prevention and treatment of apnea in premature infants, offering both short- and long-term benefits. International guidelines provide a range of recommendations regarding the preterm population eligible for caffeine prophylaxis, including the timing, dosage, and duration of treatment. Our national guidelines, published prior to the most recent updates of the international guidelines, recommend the use of caffeine citrate starting from the first day after delivery for preterm infants with a gestational age of <28 weeks. For infants up to 32 weeks, if positive pressure ventilation is required, the decision should be made on an individual basis. This study aims to describe the variability in caffeine usage across neonatal intensive care units in our country.
Methods: An online survey was sent to neonatologist who are members of the Turkish Neonatology Society to describe the variability in caffeine usage in neonatal intensive care units in our country.
Results: We collected responses from 74 units. Prophylactic caffeine usage was observed as; GA ≤276/7: 98.6%, GA 280/7–286/7: 89.0%, GA 290/7–296/7: 75.3%, GA 300/7–316/7: 53.4%. 62.2% of units reported administering loading dose within the first two hours. The initial maintenance dose was 5 mg/kg in 64.8% of units, 10 mg/kg in 32.4% of units, and intermediate dose in 5.3% of units. 47.3% of units reported no routine dose adjustment. The postmenstrual age that caffeine treatment was stopped was found to be 34 (min-max; 32–36) weeks for infants without apnea and respiratory support, 36 (min-max; 34–52) weeks for infants without apnea but any respiratory support. The time to discharge after treatment cessation was found as; 1–4 days: 37.8%, 5–7 days: 68.9%. Among the 56 units with multiple responsible physicians, 32.1% reported intra-unit variations.
Conclusion: The significant differences in caffeine usage characteristics between and within units highlight the need for clear recommendations provided by standardized guidelines.
The routine clinical approach of prophylactic caffeine in neonatal intensive care units (NICUs) has become well-established due to its positive outcomes in both the early and late stages, and it is recommended in both international and national guidelines (1–5). Common recommendations regarding caffeine usage are based on the methodology of the CAP study; caffeine should be administered within the first 72 h to preterm infants at high risk of apnea, with a loading dose of 20 mg/kg and a maintenance dose between 5 and 10 mg/kg (6). However, these guidelines do not provide specific recommendations regarding which preterm infants should receive caffeine treatment, the exact timing of caffeine initiation, dosage adjustments, and the duration of treatment. Instead, they offer a range of options.
In Turkiye, caffeine treatment in premature neonates is outlined in two recommendation papers: one on the prevention and management of bronchopulmonary dysplasia and the other on the management of respiratory distress syndrome and surfactant treatment, both of which have been in 2018. These guidelines recommend the use of caffeine citrate starting from the first day after delivery for infants with a gestational age of <28 weeks. For infants up to 32 weeks, if positive pressure ventilation is required, the decision should be made on an individual basis.
Two globally accepted guidelines, The European Consensus Guidelines on the Management of Respiratory Distress Syndrome and the Specialist Neonatal Respiratory Care for Babies Born Preterm-NICE guideline, both of which were published after our national guidelines, still do not provide specific recommendations. This leads to individual variations in caffeine usage both among and within units. Therefore, optimal dosage adjustments, as well as the timing and course of caffeine treatment, still require further research.
Studies from different countries have examined the prescribing variability in units and emphasized the necessity of standardizing caffeine usage, suggesting that variations in caffeine usage may not yield positive outcomes for the health of preterm infants (7–10). Grainge et al. from the United Kingdom emphasized some variation in practice regarding the timing of caffeine initiation, gestational age cut-off for routine caffeine prescription, and discontinuation (7). Ji et al. focused on the discontinuation timing of caffeine premature infants in the United States (8).
This survey study was planned to investigate the variability in caffeine usage practices. Questions were formulated regarding the patient population, initiation timing, loading and maintenance doses, dose adjustments, and duration of treatment. It was planned to compare the data from our country with studies in the literature showing similar variations.
Between February and March 2024, we conducted a prospective online survey. The institutional ethical committee approved the study (KA23/428). In Türkiye, the total number of NICUs including neonatologists on the medical staff is 134 (11). All neonatologists are members of the Turkish Neonatal Society and communication between them occurs via Google Groups platform. The survey was formed with Survey Monkey and the link was sent through an invitation mail in Google Groups. One neonatologist from each unit was requested to respond to the survey on behalf of the unit. It was requested to check multiple choices in case of different opinions within the unit.
The survey encompassed two inquiries regarding personal data four inquiries regarding unit demographics and 15 questions directly addressing caffeine usage. Query topics included caffeine indication for initiation, loading and maintenance dosage, adjustments, discontinuation, and discharge with caffeine treatment. The questions on caffeine usage, detailed in Supplementary, include three questions on caffeine treatment initiation regarding gestational age and indication, two questions on dose and time of loading, four questions on maintenance treatment, five questions on discontinuation, and one question on discharge with caffeine treatment. The 15 questions addressing caffeine usage were designed to include one matrix question, three open-ended questions, one multiple-choice question, and 10 checkbox questions.
A chi-square test was conducted to evaluate the association between gestational age groups and decision criteria. The analysis included all decision-making categories to ensure a comprehensive comparison across gestational age groups. Results indicated a highly significant relationship (p < 0.001) between gestational age and NICU preferences, confirming that caffeine therapy decisions vary significantly across gestational age groups.
The methodology involved both statistical analysis and visualization techniques to identify significant patterns and trends. Data was visualized using line and bar plots to examine trends in caffeine initiation preferences across gestational age groups.
The distribution of responses to the matrix question asking which indication caffeine therapy was given for, based on gestational age, was evaluated using descriptive statistics, specifically “variance.” For this purpose, the responses for each gestational week category (<276/7, 280–6/7, 290–6/7, 300/7–316/7, 320/7–336/7, 340/7–366/7, >370/7) were numbered from 1 to 6 based on the frequency of answers.
Intersection Analysis (UpSet Plot) of time intervals for initiation of caffeine therapy and discharge time. The bar plot quantifies the size of intersections, indicating the number of data points shared between specific combinations of intervals. An UpSet plot was used to analyze overlaps and intersections of specific decision categories across time of initiation of caffeine treatment and discharge time. This visualization provided a clear understanding of how categories interact and overlap.
A total of 74 NICUs responded, accounting for 55% of all neonatology units that include neonatologists on their medical staff. Of the NICUs surveyed, 32 units (43.8%) reported following a standardized protocol. There were 56 units with multiple consultant physicians and 18 of them (32.1%) reported intra-unit variations. The variability in consultant decisions within the units ranged from 16% to 1.8%. The largest difference observed was in the starting dose of the maintenance dose, with a 16% variation. The least variation was observed in the loading dose, treatment duration, and adjustment of the maintenance dose (Figure 1).
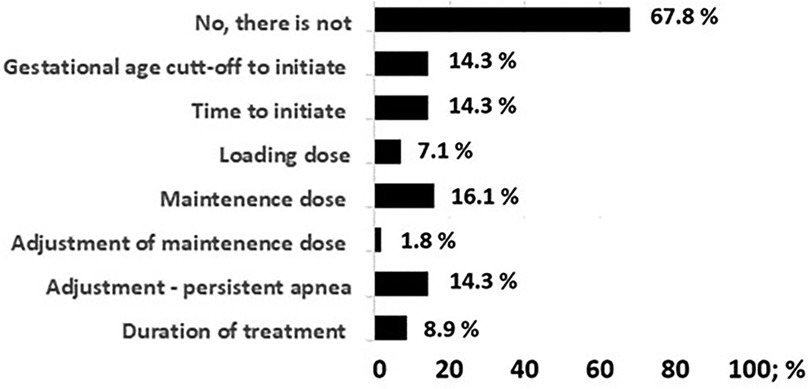
Figure 1. Bar graphic demonstrating the differences in the caffeine treatment protocol among physicians in 56 units with more than one neonatology specialist with decision-making authority.
Detailed data of survey is presented in Table 1. The variability in prophylactic caffeine usage based on gestational age (GA) was observed among units for cases not receiving respiratory support: GA < 276/7: n = 73; 98.6%, GA = 280–6/7:n = 65; 89.0%, GA = 290–6/7:n = 55; 75.3%, GA = 300/7–316/7:n = 39; 53.4%. 26 (35.1%) units indicated initiating caffeine for any respiratory support between GA = 32/0–33/6. For apnea treatment, 41 (55.4%) units reported using caffeine for late preterm infants, while 8 (11.4%) units reported its use for term infants. Table 2 shows the preferences for starting caffeine in infants regarding to gestational age and respiratory support. Our results show that the greatest variation occurs in gestational age between 30 and 32 weeks. These variations can be visualized in Figure 2. The variance value for each gestational age group was found as follows; GA < 276/7: 0.163, GA = 280–6/7: 1.047, GA = 290–6/7: 1.348, GA = 300/7–316/7: 2.091, GA = 320/7–336/7: 2.097, GA = 340/7–366/7: 0.828, GA > 370/7: 0.101.
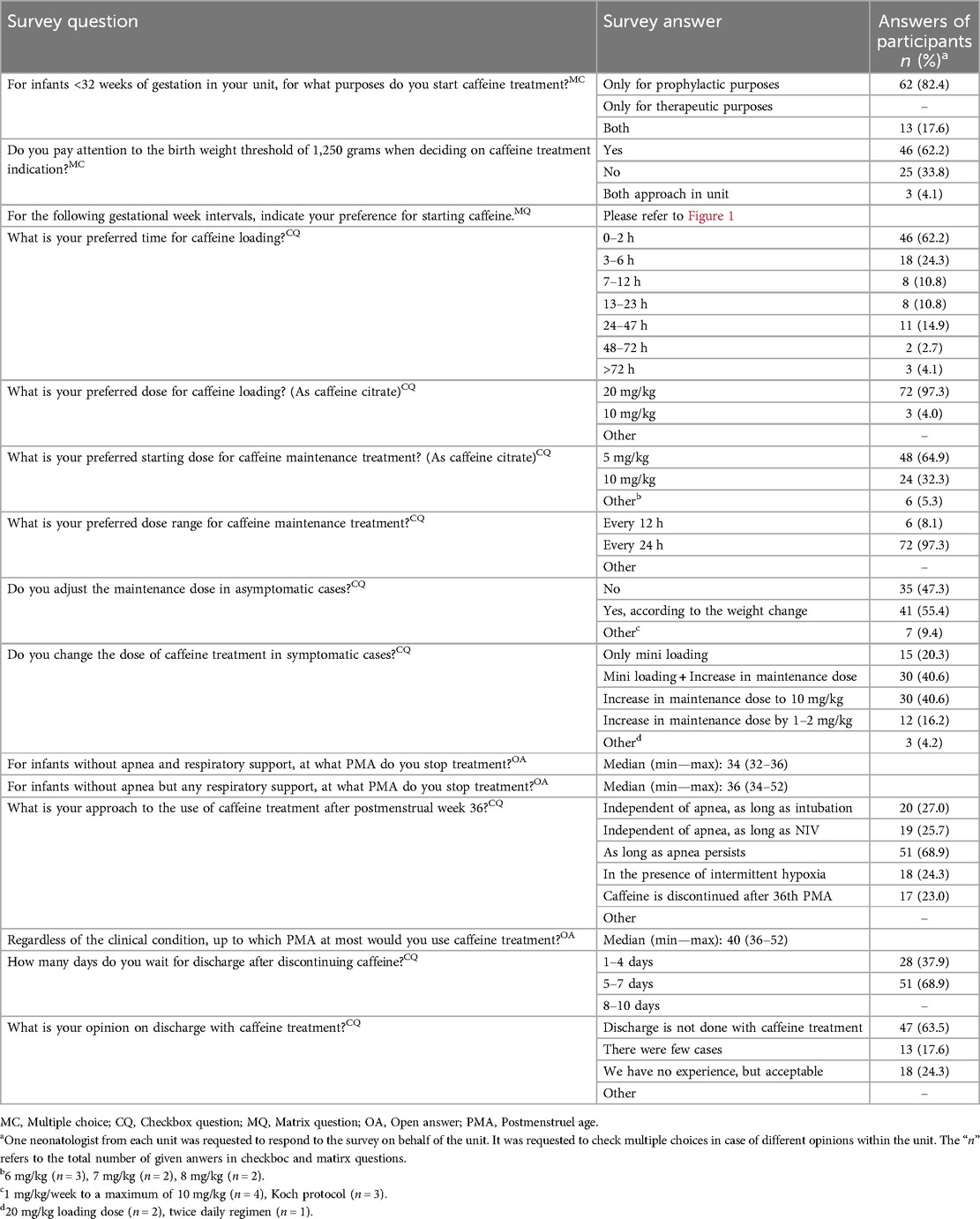
Table 1. Survey questions and answers of participants regarding the details of caffeine treatment.
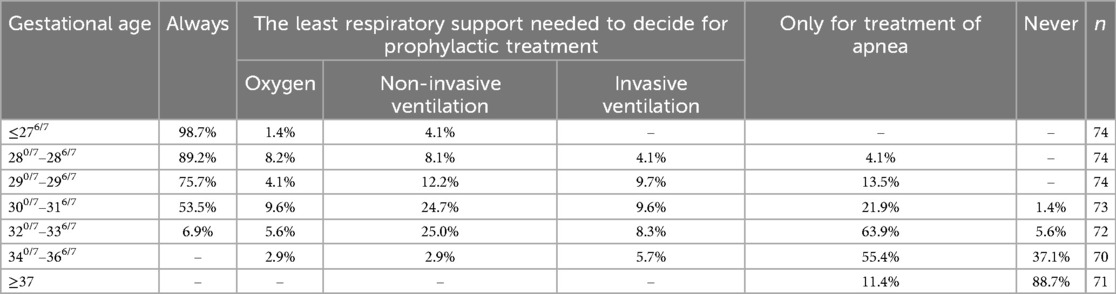
Table 2. Q: for the following gestational week intervals please indicate your preference for starting caffeine.Matrix question.
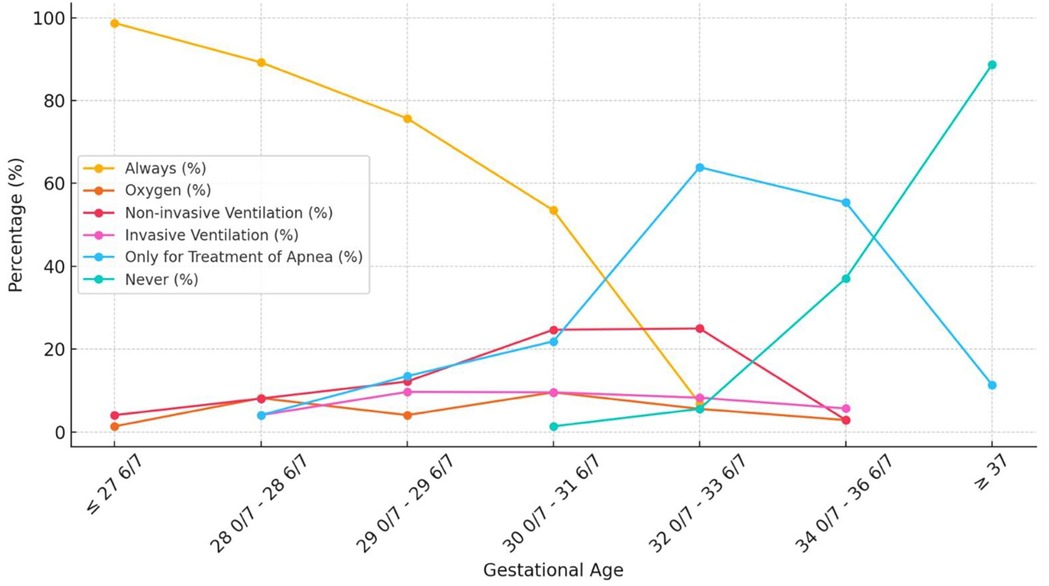
Figure 2. The variability in caffeine practices by gestational age and respiratory support. The variance value for each gestational age group was found as follows; GA < 276/7: 0.163, GA = 280–6/7: 1.047, GA = 290–6/7: 1.348, GA = 300/7–316/7: 2.091, GA = 320/7–336/7: 2.097, GA = 340/7–366/7: 0.828, GA > 370/7: 0.101.
Administering caffeine loading dose within the first two hours was reported in 46 (62.2%) units. The starting dose for caffeine maintenance was 5 mg/kg in 48 (64.8%) units, 10 mg/kg in 24 (32.4%) units, and intermediate dose in 6 units. 35 (47.3%) units reported no routine dose adjustment.
Different practices were reported for caffeine dose management in the presence of apnea: mini-loading: n = 15; 20.3%, mini-loading and increase in maintenance dose: n = 30; 40.6%, increasing maintenance dose to 10 mg/kg: n = 30; 40.6%, and increasing maintenance dose: n = 12; 16.2%. One unit reported shortening the dose interval.
For cases without apnea but ongoing respiratory support, caffeine treatment was discontinued between postmenstrual weeks 33–52, and in 14 units, caffeine was not used after postmenstrual week 36. Variability was also observed in discharge timing after treatment cessation; 1–4 days: n = 28; 37.8%, 5–7 days: n = 51; 68.9%. For neonates without respiratory support, the most common age for caffeine discontinuation is 34 weeks, followed by 36 weeks. However, practices vary widely with some units extending to 40 weeks or beyond. For neonates with respiratory support, caffeine often continues until respiratory support is discontinued (36–40 weeks). There was no correlation between caffeine initiation time and discharge time after discontinuation. The intersection of various time intervals for caffeine therapy, providing insights into both individual and combined interval contributions are given in Figure 3.
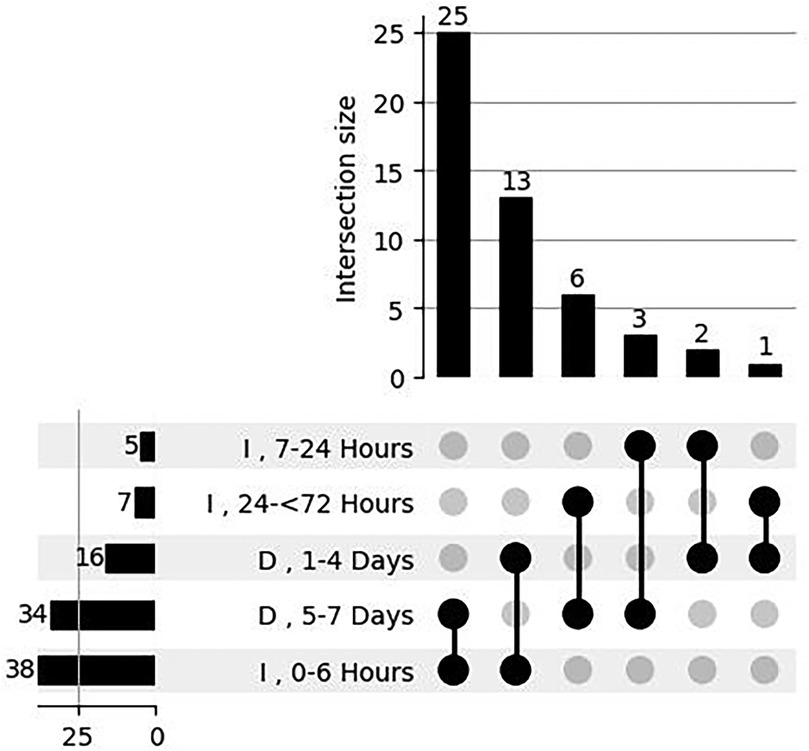
Figure 3. Intersection analysis of time intervals for initiation of caffeine therapy and discharge time. The bar plot quantifies the size of intersections, indicating the number of data points shared between specific combinations of intervals. The intersection matrix at the bottom visually maps these combinations, with vertical lines connecting dots to represent overlapping intervals. On the left, horizontal bars summarize the total count of data points for each individual time interval, offering a clear overview of category sizes. This comprehensive visualization highlights the dominant time intervals and their overlap in caffeine therapy application. I: Initiation, D: Discharge.
Caffeine citrate began to find its place in the care of premature infants with the groundbreaking study by Jacop Aranda in 1977 (12). Initially used for the treatment of premature apnea, caffeine citrate gradually became more commonly used in neonatal intensive care units over the years. Concerns regarding the mechanism of action of caffeine, namely adenosine receptor blockade, led to the initiation of the CAP study as a safety measure, which reported groundbreaking results regarding the benefits of caffeine (6). With the accumulation of these results, the purpose of caffeine therapy evolved. Now, the aim of caffeine therapy is not only to treat apnea but also to prevent it, as well as to reduce bronchopulmonary dysplasia, and achieve positive neurodevelopmental outcomes (13–15). The accumulation of evidence that premature retinopathy, patent ductus arteriosus, acute kidney injury, and inflammation may also be reduced in infants receiving caffeine led to a shift in the perspective on caffeine therapy in neonatology (16–18).
Current guidelines provide varying recommendations for the gestational age threshold at which caffeine therapy should be initiated. The European RDS Consensus guideline recommends caffeine therapy for all premature infants born below 32 weeks gestation receiving positive pressure ventilation, while the United Kingdom guidelines suggest its use for all infants born below 30 weeks gestation (2, 3). The American Academy of Pediatrics guidelines recommend caffeine therapy for all infants born below 28 weeks gestation and for those born between 28 and 32 weeks gestation who are receiving positive pressure ventilation (1). Similarly, our national guidelines recommend caffeine for all preterm infants with a gestational age of <28 weeks and suggest an individualized approach for infants between 28 and 32 weeks requiring positive pressure ventilation. The recommendations endorsed by our association closely align with the AAP guidelines (4, 5). Therefore, indications for caffeine therapy may vary in infants born between 28 and 32 weeks' gestation depending on the guidelines followed.
Our survey indicated that nearly all participating units administered caffeine therapy to infants born before 29 weeks gestation, regardless of respiratory support. Beyond 29 weeks, respiratory support became an increasingly important factor in therapy decisions. The greatest variability in practices was observed between 30 and 34 weeks gestation, particularly at 30–32 weeks, reflecting the complexity of clinical decision-making during this period. This variability highlights a gap in international guidelines, which provide limited recommendations for caffeine therapy in this range, leading to reliance on individual judgment and institutional preferences. Comprehensive, evidence-based guidelines are needed to harmonize practices and improve outcomes for preterm infants. Similarly, Greinge et al. found wide variation in caffeine initiation thresholds among units but did not assess respiratory support, which may limit the applicability of their findings (7).
Caffeine use in moderate and late preterm infants remains debated. Apnea occurs in 20% of infants born at 32–34 weeks and 10% at 34–36 weeks gestation (19, 20). Intermittent hypoxia, associated with adverse outcomes, is also common in these groups (21). While evidence on caffeine therapy for these infants is limited, some studies suggest potential benefits (22–24). Our survey found greater variability in initiating caffeine therapy among moderate preterm infants compared to late preterm infants, with half of the units administering it therapeutically between 32 and 37 weeks gestation.
The favor of early caffeine treatment was first shown by CAP trial subgroup analyses (25). Early treatment, defined as administration within the first 3 days of life, is supported by meta-analyses and systematic reviews showing reduced rates of bronchopulmonary dysplasia, patent ductus arteriosus, periventricular leukomalacia, intraventricular hemorrhage, and severe retinopathy of prematurity, along with improved neurodevelopmental outcomes (2, 26–32). However, the optimal timing within these 3 days remains unclear, and the question of whether “earlier is always better” persists. While very early caffeine use, such as at birth or within 2 h, has shown benefits like improved lung mechanics and reduced ventilation needs, concerns about mesenteric blood flow disturbances remain (33–37). Research comparing timing within the first 72 h has not found significant clinical differences. Notably, our survey is the first to provide detailed data on loading dose timing, revealing that two-thirds of units administer caffeine within the first day, with significant variation, and about one-sixth start it on the second day.
Recent reviews show that high-dose regimens reduce apnea, extubation failure, and BPD without affecting mortality, though evidence on neurodevelopmental outcomes is conflicting (24, 38–45). Current guidelines recommend 20 mg/kg as a loading dose and 5–10 mg/kg for maintenance, but the two-fold range in maintenance dosing highlights uncertainty about the optimal starting dose. While higher maintenance doses improve short-term respiratory outcomes and reduce bronchopulmonary dysplasia, initiating with 10 mg/kg remains limited to clinical research (46–48). Surveys from the United Kingdom and New Zealand, consistent with our findings, reported 20 mg/kg and 5 mg/kg as the most common doses, with one-third of units using a maintenance dose of 10 mg/kg (7, 10).
Dose adjustment in asymptomatic patients lacks clear guidelines. Dose adjustment in asymptomatic patients is another issue of debate. The CAP study protocol, which starts with a 5 mg/kg maintenance dose and increases weekly based on weight, is an acceptable minimum approach. Some studies have used intermediate doses (49, 50). A United Kingdom survey reported that 86% of units regularly optimize caffeine doses based on weight, while our survey found that 55% of units adjust doses weekly. The lack of clear guidance in international guidelines may explain why dose adjustments based on weight are not performed in half of the units.
As caffeine therapy's role has expanded from treating apnea to providing multisystemic benefits, studies have focused on the concentration-effect relationship. Serum caffeine levels between 5 and 20 mg/dl are considered sufficient for apnea prevention, with higher levels (15–20 mg/dl) showing a positive impact on chronic lung disease (13, 51, 52). While pharmacokinetic data can optimize dosing, they are not always available in routine practice. Studies have considered factors like weight gain and liver metabolism in neonates to determine the appropriate serum level (53–57). Koch et al. recommend gradually escalating the dose to 8 mg/kg from the 5th week onward, a protocol endorsed by the latest European RDS guidelines (2, 57). However, this approach is not widely adopted, with only two units reporting its use.
There is also uncertainty about how to increase the dose in cases with ongoing apnea of prematurity. The CAP trial indicated that the maintenance dose was increased to 10 mg/kg. However, there is evidence that a small loading dose together with an increased maintenance dose is successful in decreasing apnea (58). Gray et al. stated that the maintenance dose was increased in the majority of units (10). Yet, we also observed that just the increase of the maintenance dose or mini loading plus an increase of the maintenance dose wer equally preferred within units.
While the benefits of caffeine therapy are well-established, it is unclear when to discontinue it relative to the baby's discharge. Neonatologists typically require an “event-free” period after stopping caffeine before discharge, but there is no consensus on how long this apnea-free period should be. American Academy of Pediatrics suggests stopping caffeine treatment when the corrected age of the baby reaches 33–34 weeks and they have been free from apnea/positive pressure for one week, which is later while United Kingdom guidelines recommendation includes the farthest outcome (1, 3). In the United Kingdom, 34% of units would stop caffeine at 34 weeks, regardless of respiratory support, while 11% would continue if respiratory support was needed (7). A similar variability was observed in a study by Ji et al. The authors emphasized that respiratory support at the time of discontinuation was common but variable, with 0%–57% of infants receiving positive airway pressure at caffeine discontinuation by site (8). Ducrocq et al. reported that postmenstrual age for discontinuation ranged from 32 to 40 weeks in France (9). Our survey showed a trend of prolonged caffeine treatment based on respiratory support needs, with similar variations observed in caffeine use beyond 36 weeks postmenstrual age. The ongoing apnea or intermittent hypoxemia in premature infants after 34 weeks, along with the benefits of caffeine, forms the clinical approach to this undefined guideline issue (26, 59–61).
The safe serum level considered for discharge after caffeine therapy is <5 mg/dl, which indicates subtherapeutic levels. As can be understood, the time required for the serum level to drop to this level is dose-dependent due to the long half-life (62). Chung et al. showed that the proportion of cases with serum levels higher than the subtherapeutic level after discontinuation of caffeine therapy at ≥5 mg/kg/dose was approximately 50% between 5 and 7 days and around 25% between 8 and 10 days (63). The lack of guidelines results in variable durations for discharge after cessation of caffeine therapy (10).
While our survey garnered responses from 55% of neonatal units, it's significant that the majority of these responses originated from units with long-standing staff. The fact that only one doctor exists in some units may limit the accuracy of the data. Additionally, the response rate is comparable to other multicenter studies guided by the Turkish Neonatal Society suggesting that these responses likely reflect the sentiments of neonatologists across Türkiye (11, 64). Notably, our response rate mirrors that of the study by Grainge et al., a survey conducted in the United Kingdom (7).
One noteworthy aspect of our survey is the documentation of intra-unit preferences. The fact that our national guidelines were published in 2018, followed by the update of the NICE guideline in 2019 and the European Consensus Guidelines on the Management of Respiratory Distress Syndrome in 2022, indicates that neonatologists have clearly followed global guidelines. The significant differences in caffeine usage preferences between units may stem from the lack of clarity in the recommendations of the updated international guidelines. Unlike the United Kingdom survey, which lacked an acknowledgment of physician bias, our survey sheds light on this issue, adding an important dimension to the discussion. The other strength of the current survey is that caffeine use in infants greater than 32 weeks was evaluated. It's important to highlight that there were variations in multiple aspects of caffeine usage.
In conclusion, our survey revealed discrepancies concerning the timing of both caffeine initiation and cessation, gestational age threshold for routine caffeine commencement, and as well as dose adjustment. Intra-unit variability other than national variations underscores the necessity of more focused guidelines. These findings emphasize significant disparities in caffeine utilization across neonatal units in Türkiye.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by This study was approved by Baskent University Institutional Review Board and EthicsCommittee (Project no:KA23/428). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
SeU: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DA: Writing – original draft, Writing – review & editing. OT: Writing – original draft, Writing – review & editing, Conceptualization, Investigation. AK: Writing – original draft, Writing – review & editing, Methodology, Supervision. AE: Methodology, Supervision, Writing – original draft, Writing – review & editing. AA: Writing – original draft, Writing – review & editing. MA: Writing – original draft, Writing – review & editing. SA: Writing – original draft, Writing – review & editing. NC: Writing – original draft, Writing – review & editing. EA: Writing – original draft, Writing – review & editing. HA: Writing – original draft, Writing – review & editing. BarA: Writing – original draft, Writing – review & editing. DA: Writing – original draft, Writing – review & editing. EA: Writing – original draft, Writing – review & editing. BanA: Writing – original draft, Writing – review & editing. HB: Writing – original draft, Writing – review & editing. LB: Writing – original draft, Writing – review & editing. EC: Writing – original draft, Writing – review & editing. ŞÇ: Writing – original draft, Writing – review & editing. KC: Writing – original draft, Writing – review & editing. YC: Writing – original draft, Writing – review & editing. BC: Writing – original draft, Writing – review & editing. MC: Writing – original draft, Writing – review & editing. AD: Writing – original draft, Writing – review & editing. GD: Writing – original draft, Writing – review & editing. ND: Writing – review & editing, Writing – original draft. PD: Writing – original draft, Writing – review & editing. MD: Writing – original draft, Writing – review & editing. DE: Writing – original draft, Writing – review & editing. TE: Writing – original draft, Writing – review & editing. ZG: Writing – original draft, Writing – review & editing. IG: Writing – original draft, Writing – review & editing. SG: Writing – original draft, Writing – review & editing. AG: Writing – original draft, Writing – review & editing. TG: Writing – original draft, Writing – review & editing. HH: Writing – original draft, Writing – review & editing. SH: Writing – original draft, Writing – review & editing. FI: Writing – original draft, Writing – review & editing. II: Writing – original draft, Writing – review & editing. SK: Writing – original draft, Writing – review & editing. DilekKa: Writing – original draft, Writing – review & editing. GK: Writing – original draft, Writing – review & editing. MK: Writing – original draft, Writing – review & editing. DilekKu: Writing – original draft, Writing – review & editing. TM: Writing – original draft, Writing – review & editing. IM: Writing – original draft, Writing – review & editing. NN: Writing – original draft, Writing – review & editing. EmO: Writing – original draft, Writing – review & editing. NO: Writing – original draft, Writing – review & editing. OzgO: Writing – original draft, Writing – review & editing. FO: Writing – original draft, Writing – review & editing. BO: Writing – original draft, Writing – review & editing. AO: Writing – original draft, Writing – review & editing. OzmO: Writing – original draft, Writing – review & editing. HO: Writing – original draft, Writing – review & editing. GS: Writing – original draft, Writing – review & editing. DS: Writing – original draft, Writing – review & editing. CS: Writing – original draft, Writing – review & editing. BS: Writing – original draft, Writing – review & editing. SS: Writing – original draft, Writing – review & editing. OS: Writing – original draft, Writing – review & editing. HS: Writing – original draft, Writing – review & editing. UT: Writing – original draft, Writing – review & editing. ST: Writing – original draft, Writing – review & editing. KT: Writing – original draft, Writing – review & editing. DT: Writing – original draft, Writing – review & editing. GT: Writing – original draft, Writing – review & editing. TT: Writing – original draft, Writing – review & editing. ErT: Writing – original draft, Writing – review & editing. EdT: Writing – original draft, Writing – review & editing. FT: Writing – original draft, Writing – review & editing. EU: Writing – original draft, Writing – review & editing. DU: Writing – original draft, Writing – review & editing. NU: Writing – original draft, Writing – review & editing. SaU: Writing – original draft, Writing – review & editing. İU: Writing – original draft, Writing – review & editing. FH: Writing – original draft, Writing – review & editing. AM: Formal analysis, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Eichenwald EC, Watterberg Kristi L, Aucott S, Benitz WE, Cummings JJ, Goldsmith J, et al. Apnea of Prematurity. Pediatrics. (2016) 137:e20153757. doi: 10.1542/peds.2015-3757
2. Sweet DG, Carnielli VP, Greisen G, Hallman M, Klebermass-Schrehof K, Ozek E, et al. European consensus guidelines on the management of respiratory distress syndrome: 2022 update. Neonatology. (2023) 120:3–23. doi: 10.1159/000528914
3. National Institute for Health and Care Excellence. Specialist neonatal respiratory care for babies born preterm NICE guideline (NG124) Published: 03 April 2019. Available online at: https://www.nice.org.uk/guidance/ng124 (Accessed July 07, 2024).
4. Arsan S, Korkmaz A, Oğuz S. Turkish neonatal society guideline on prevention and management of bronchopulmonary dysplasia. Turk Pediatri Ars. (2018) 25(Suppl 1):138–S150. doi: 10.5152/TurkPediatriArs.2018.01814
5. Özkan H, Erdeve Ö, Kutman HGK. Turkish neonatal society guideline on the management of respiratory distress syndrome and surfactant treatment. Turk Pediatri Ars. (2018) 25(Suppl 1):45–54. doi: 10.5152/TurkPediatriArs.2018.01806
6. Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, et al. Caffeine for apnea of prematurity trial group. Caffeine therapy for apnea of prematurity. N Engl J Med. (2006) 354:2112–2021. doi: 10.1056/NEJMoa054065
7. Grainge S, Nair V, Kannan Loganathan P. National survey on caffeine use in neonatal units across the United Kingdom. Acta Paediatr. (2023) 112:1865–9. doi: 10.1111/apa.16635
8. Ji D, Smith PB, Clark RH, Zimmerman KO, Laughon M, Ku L, et al. Wide variation in caffeine discontinuation timing in premature infants. J Perinatol. (2020) 40:288–93. doi: 10.1038/s41372-019-0561-0
9. Ducrocq S, Biran-Mucignat V, Lebas F, Baudon JJ, Gold F. Utilisation du citrate de caféine pour le traitement des apnées idiopathiques du prématuré dans les équipes françaises de médecine néonatale (caffeine citrate utilization for treatment of apnea in French neonatal units). Arch Pediatr. (2006) 13:1305–8. doi: 10.1016/j.arcped.2006.06.007
10. Gray PH, Chauhan M. Use of caffeine for preterm infants in Australia and New Zealand: a survey. J Paediatr Child Health. (2016) 52:1121–2. doi: 10.1111/jpc.13366
11. Koc E, Demirel N, Bas AY, Ulubas Isik D, Hirfanoglu IM, Tunc T, et al. Early neonatal outcomes of very-low-birth-weight infants in Turkey: a prospective multicenter study of the Turkish neonatal society. PLoS One. (2019) 18:e0226679. doi: 10.1371/journal.pone.0226679
12. Aranda JV, Gorman W, Bergsteinsson H, Gunn T. Efficacy of caffeine in treatment of apnea in the low-birth-weight infant. J Pediatr. (1977) 90:467–72. doi: 10.1016/S0022-3476(77)80718-X
13. Jensen EA, Foglia EE, Schmidt B. Evidence-based pharmacologic therapies for prevention of bronchopulmonary dysplasia: application of the grading of recommendations assessment, development, and evaluation methodology. Clin Perinatol. (2015) 42:755–79. doi: 10.1016/j.clp.2015.08.005
14. Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, et al. Caffeine for apnea of prematurity trial group. Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med. (2007) 357:1893–902. doi: 10.1056/NEJMoa073679
15. Schmidt B, Roberts RS, Anderson PJ, Asztalos EV, Costantini L, Davis PG, et al. Caffeine for apnea of prematurity (CAP) trial group. Academic performance, motor function, and behavior 11 years after neonatal caffeine citrate therapy for apnea of prematurity: an 11-year follow-up of the CAP randomized clinical trial. JAMA Pediatr. (2017) 171:564–72. doi: 10.1001/jamapediatrics.2017.0238
16. Aranda JV, Qu J, Valencia GB, Beharry KD. Pharmacologic interventions for the prevention and treatment of retinopathy of prematurity. Semin Perinatol. (2019) 43:360–6. doi: 10.1053/j.semperi.2019.05.009
17. Yuan Y, Yang Y, Lei X, Dong W. Caffeine and bronchopulmonary dysplasia: clinical benefits and the mechanisms involved. Pediatr Pulmonol. (2022) 57:1392–400. doi: 10.1002/ppul.25898
18. Aithal N, Kandasamy Y. The babyccino: the role of caffeine in the prevention of acute kidney injury in neonates—A literature review. Healthcare (Basel). (2024) 12:529. doi: 10.3390/healthcare12050529
19. Eichenwald EC, Zupancic JA, Mao WY, Richardson DK, McCormick MC, Escobar GJ. Variation in diagnosis of apnea in moderately preterm infants predicts length of stay. Pediatrics. (2011) 127:e53–8. doi: 10.1542/peds.2010-0495
20. Olivier F, Nadeau S, Caouette G, Piedboeuf B. Association between apnea of prematurity and respiratory distress syndrome in late preterm infants: an observational study. Front Pediatr. (2016) 4:e105. doi: 10.3389/fped.2016.00105
21. Mandala VK, Bollaboina SKY, Changala B, Kotha R Sr, Kasula L. Intermittent hypoxia in preterm neonates and its effect on neonatal morbidity and mortality: a systematic review. Cureus. (2023) 15:e45561. doi: 10.7759/cureus.45561
22. Bahari M, Jose Carlos A, Featherstone R, Kumar M. Caffeine use for apnea of prematurity in moderate and late preterm infants: a systematic review. J Clin Neonatol. (2019) 8:162–5. doi: 10.4103/jcn.JCN_34_19
23. Yangın Ergon E, Colak R, Kıvılcım M, Yildiz M, Ozdemir SA, Kulali F, et al. Benefits of caffeine: birth weigth over 1250 g infants with respiratuar distress. Forbes J Med. (2020) 1:68–74. doi: 10.5222/forbes.2020.57441
24. Oliphant EA, McKinlay CJ, McNamara D, Cavadino A, Alsweiler JM. Caffeine to prevent intermittent hypoxaemia in late preterm infants: randomised controlled dosage trial. Arch Dis Child Fetal Neonatal Ed. (2023) 108:106–13. doi: 10.1136/archdischild-2022-324010
25. Davis PG, Schmidt B, Roberts RS, Doyle LW, Asztalos E, Haslam R, et al. Caffeine for apnea of prematurity trial group. Caffeine for apnea of prematurity trial: benefits may vary in subgroups. J Pediatr. (2010) 156:382–7. doi: 10.1016/j.jpeds.2009.09.069
26. Dobson NR, Rhein LM, Darnall RA, Corwin MJ, Heeren TC, Eichenwald E, et al. Caffeine decreases intermittent hypoxia in preterm infants nearing term-equivalent age. J Perinatol. (2017) 37:1135–40. doi: 10.1038/jp.2017.82
27. Lodha A, Seshia M, McMillan DD, Barrington K, Yang J, Lee SK, et al. Association of early caffeine administration and neonatal outcomes in very preterm neonates. JAMA Pediatr. (2015) 169:33–8. doi: 10.1001/jamapediatrics.2014.2223
28. Taha D, Kirkby S, Nawab U, Dysart KC, Genen L, Greenspan JS, et al. Early caffeine therapy for prevention of bronchopulmonary dysplasia in preterm infants. J Matern Fetal Neonatal Med. (2014) 27:1698–702. doi: 10.3109/14767058.2014.885941
29. Park HW, Lim G, Chung S-H, Chung S, Kim KS, Kim S-N. Early caffeine use in very low birth weight infants and neonatal outcomes: a systematic review and meta-analysis. J Korean Med Sci. (2015) 30:1828–35. doi: 10.3346/jkms.2015.30.12.1828
30. Kua KP, Lee SW. Systematic review and meta-analysis of clinical outcomes of early caffeine therapy in preterm neonates. Br J Clin Pharmacol. (2017) 83:180–91. doi: 10.1111/bcp.13089
31. Gupte AS, Gupta D, Ravichandran S, Ma MM, Chouthai NS. Effect of early caffeine on neurodevelopmental outcome of very low-birth weight newborns. J Matern Fetal Neonatal Med. (2016) 29:1233–7. doi: 10.3109/14767058.2015.1041493
32. Lodha A, Entz R, Synnes A, Creighton D, Yusuf K, Lapointe A, et al. Early caffeine administration and neurodevelopmental outcomes in preterm infants. Pediatrics. (2019) 143:e20181348. doi: 10.1542/peds.2018-1348
33. Katheria A, Sauberan J, Akotia D, Rich W, Durham J, Finer N. A pilot randomized controlled trial of early versus routine caffeine in extremely premature infants. Am J Perinatol. (2015) 32:879–886. doi: 10.1055/s-0034-1543981
34. Dekker J, Hooper SB, van Vonderen JJ, Witlox RSGM, Lopriore E, te Pas AB. Caffeine to improve breathing effort of preterm infants at birth: a randomized controlled trial. Pediatr Res. (2017) 82:290–6. doi: 10.1038/pr.2017.45
35. Borszewska-Kornacka MK, Hożejowski R, Rutkowska M, Lauterbach R. Shifting the boundaries for early caffeine initiation in neonatal practice: results of a prospective, multicenter study on very preterm infants with respiratory distress syndrome. PLoS One. (2017) 12:e0189152. doi: 10.1371/journal.pone.0189152
36. Abdel-Hady H, Nasef N, Shabaan AE, Nour I. Caffeine therapy in preterm infants. World J Clin Pediatr. (2015) 4:81–93. doi: 10.5409/wjcp.v4.i4.81
37. Ozkan H, Cetinkaya M, Cakir SC, Saglam O, Koksal N. Effects of different onset times of early caffeine treatment on mesenteric tissue oxygenation and necrotizing enterocolitis: a prospective, randomized study. Am J Perinatol. (2023) 40:28–34. doi: 10.1055/s-0041-1727157
38. Brattström P, Russo C, Ley D, Bruschettini M. High-versus low-dose caffeine in preterm infants: a systematic review and meta-analysis. Acta Paediatr. (2019) 108:401–10. doi: 10.1111/apa.14586
39. Chen J, Jin L, Chen X. Efficacy and safety of different maintenance doses of caffeine citrate for treatment of apnea in premature infants: a systematic review and meta-analysis. Biomed Res Int. (2018) 2018:e9061234. doi: 10.1155/2018/9061234
40. Vliegenthart R, Miedema M, Hutten GJ, van Kaam AH, Onland W. High versus standard dose caffeine for apnoea: a systematic review. Arch Dis Child Fetal Neonatal Ed. (2018) 103:F523–9. doi: 10.1136/archdischild-2017-313556
41. Pakvasa MA, Saroha V, Patel RM. Optimizing caffeine use and risk of bronchopulmonary dysplasia in preterm infants: a systematic review, meta-analysis, and application of grading of recommendations assessment, development, and evaluation methodology. Clin Perinatol. (2018) 45:273–91. doi: 10.1016/j.clp.2018.01.012
42. Bruschettini M, Brattström P, Russo C, Onland W, Davis PG, Soll R. Caffeine dosing regimens in preterm infants with or at risk for apnea of prematurity. Cochrane Database Syst Rev. (2023) 4:CD013873. doi: 10.1002/14651858.CD013873.pub2
43. Steer P, Flenady V, Shearman A, Charles B, Gray PH, Henderson-Smart D, et al. Caffeine collaborative study group steering group. High dose caffeine citrate for extubation of preterm infants: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. (2004) 89:F499–503. doi: 10.1136/adc.2002.023432
44. McPherson C, Neil JJ, Tjoeng TH, Pineda R, Inder TE. A pilot randomized trial of high-dose caffeine therapy in preterm infants. Pediatr Res. (2015) 78:198–204. doi: 10.1038/pr.2015.72
45. McPherson C, Lean RE, Cyr PEP, Inder TE, Rogers CE, Smyser CD. Five-year outcomes of premature infants randomized to high or standard loading dose caffeine. J Perinatol. (2022) 42:631–5. doi: 10.1038/s41372-022-01333-5
46. Yang Y, Lu KY, Cheng R, Zhou Q, Fang GD, Li H, et al. Clinical effect of different maintenance doses of caffeine citrate in the treatment of preterm infants requiring assisted ventilation: a pilot multicenter study. Zhongguo Dang Dai Er Ke Za Zhi. (2022) 24:240–8. doi: 10.7499/j.issn.1008-8830.2109144
47. Li XL, Cai YJ, Zhang Z, Li J, Chen XW, Song YY, et al. Effect of different maintenance doses of caffeine citrate on ventilator weaning in very preterm infants with respiratory distress syndrome: a prospective randomized controlled trial. Zhongguo Dang Dai Er Ke Za Zhi. (2021) 23:1097–102. doi: 10.7499/j.issn.1008-8830.2107167
48. Wan L, Huang L, Chen P. Caffeine citrate maintenance doses effect on extubation and apnea postventilation in preterm infants. Pediatr Pulmonol. (2020) 55:2635–40. doi: 10.1002/ppul.24948
49. Leon AE, Michienzi K, Ma CX, Hutchison AA. Serum caffeine concentrations in preterm neonates. Am J Perinatol. (2007) 24:39–47. doi: 10.1055/s-2006-958163
50. Rosen C, Taran C, Hanna M, Gueta I, Loebstein R, Strauss T, et al. Caffeine citrate for apnea of prematurity—One dose does not fit all a prospective study. J Perinatol. (2021) 41:2292–7. doi: 10.1038/s41372-021-01172-w
51. Dobson NR, Hunt CE. Caffeine: an evidence-based success story in VLBW pharmacotherapy. Pediatr Res. (2018) 84:333–40. doi: 10.1038/s41390-018-0089-6
52. Alur P, Bollampalli V, Bell T, Hussain N, Liss J. Serum caffeine concentrations and short-term outcomes in premature infants of ≤29 weeks of gestation. J Perinatol. (2015) 35:434–8. doi: 10.1038/jp.2014.226
53. Aranda JV, Beharry KD. Pharmacokinetics, pharmacodynamics and metabolism of caffeine in newborns. Semin Fetal Neonatal Med. (2020) 25:101183. doi: 10.1016/j.siny.2020.101183
54. Taguchi M, Kawasaki Y, Katsuma A, Mito A, Tamura K, Makimoto M, et al. Pharmacokinetic variability of caffeine in routinely treated preterm infants: preliminary considerations on developmental changes of systemic clearance. Biol Pharm Bull. (2021) 44:69–74. doi: 10.1248/bpb.b20-00616
55. Engbers AGJ, Völler S, Poets CF, Knibbe CAJ, Reiss IKM, Koch BCP, et al. The pharmacokinetics of caffeine in preterm newborns: no influence of doxapram but important maturation with age. Neonatology. (2021) 118:106–13. doi: 10.1159/000513413
56. Lim SY, May CB, Johnson PN, Miller JL. Caffeine dosing in premature neonates: impact of birth weight on a pharmacokinetic simulation study. Pediatr Res. (2023) 93:696–700. doi: 10.1038/s41390-022-02172-y
57. Koch G, Datta AN, Jost K, Schulzke SM, van den Anker J, Pfister M. Caffeine citrate dosing adjustments to assure stable caffeine concentrations in preterm neonates. J Pediatr. (2017) 191:50–6. doi: 10.1016/j.jpeds.2017.08.064
58. Tabacaru CR, Jang SY, Patel M, Davalian F, Zanelli S, Fairchild KD. Impact of caffeine boluses and caffeine discontinuation on apnea and hypoxemia in preterm infants. J Caffeine Res. (2017) 7:103–10. doi: 10.1089/jcr.2017.0002
59. Eichenwald EC, Aina A, Stark AR. Apnea frequently persists beyond term gestation in infants delivered at 24–28 weeks. Pediatrics. (1997) 100:354–9. doi: 10.1542/peds.100.3.354
60. Di Fiore JM, Bloom JN, Orge F, Schutt A, Schluchter M, Cheruvu VK, et al. A higher incidence of intermittent hypoxemic episodes is associated with severe retinopathy of prematurity. J Pediatr. (2010) 157:69–73. doi: 10.1016/j.jpeds.2010.01.046
61. Rhein LM, Dobson NR, Darnall RA, Corwin MJ, Heeren TC, Poets CF, et al. Caffeine pilot study group. Effects of caffeine on intermittent hypoxia in infants born prematurely: a randomized clinical trial. JAMA Pediatr. (2014) 168:250–7. doi: 10.1001/jamapediatrics.2013.4371
62. Charles BG, Townsend SR, Steer PA, Flenady VJ, Gray PH, Shearman A. Caffeine citrate treatment for extremely premature infants with apnea: population pharmacokinetics, absolute bioavailability, and implications for therapeutic drug monitoring. Ther Drug Monit. (2008) 30:709–16. doi: 10.1097/FTD.0b013e3181898b6f
63. Chung J, Tran Lopez K, Amendolia B, Bhat V, Nakhla T, Slater-Myer L, et al. Stopping caffeine in premature neonates: how long does it take for the level of caffeine to fall below the therapeutic range? J Matern Fetal Neonatal Med. (2022) 35:551–5. doi: 10.1080/14767058.2020.1729117
64. Bas AY, Demirel N, Koc E, Ulubas Isik D, Hirfanoglu İM, Tunc T. Incidence, risk factors and severity of retinopathy of prematurity in Turkey (TR-ROP study): a prospective, multicentre study in 69 neonatal intensive care units. Br J Ophthalmol. (2018) 102:1711–6. doi: 10.1136/bjophthalmol-2017-311789
Keywords: caffeine, premature neonate, apnea of prematurity, neonatal intensive care unit, guideline
Citation: Unal S, Beken S, Anuk Ince D, Turan O, Korkmaz Toygar A, Ecevit A, Akcan AB, Akın MA, Aktas S, Ciftdemir NA, Altuncu E, Altunhan H, Arcagok BC, Armangil D, Arun Ozer E, Aydın B, Bezirganoglu H, Bilgin L, Calısıcı E, Calkavur S, Celik K, Celik Y, Cetinkaya B, Cetinkaya M, Demirel A, Demirel G, Dogan NN, Doğan P, Durukan M, Engur D, Erener Ercan T, Gokmen Z, Guney Varal I, Gulası S, Gunlemez A, Gursoy T, Hakyemez Toptan H, Hamitoğlu S, Isleyen F, Iyigun I, Kader S, Kahvecioğlu D, Kaykı G, Kostu M, Kurnaz D, Mammadalıyev T, Mungan Akin I, Narlı N, Okulu E, Okur N, Olukman O, Ovalı F, Ozcan B, Ozdemir A, Ozdemir O, Ozkan H, Sandal G, Sarıcı D, Sivrikaya C, Siyah Bilgin B, Sundus S, Surmeli Onay O, Simsek H, Tandırcıoğlu UA, Tanrıverdi S, Tekgunduz KS, Terek D, Tunc G, Tunc T, Tutak E, Tufekcioğlu E, Tuzun Erdogan F, Ulu E, Ulubas Isik D, Uras N, Uslu SI, Unal I, Yılmaz FH and Moniri A (2025) Caffeine use in preterm neonates: national insights into Turkish NICU practices. Front. Pediatr. 13:1492716. doi: 10.3389/fped.2025.1492716
Received: 7 September 2024; Accepted: 28 January 2025;
Published: 27 February 2025.
Edited by:
Jeroen J. van Vonderen, Máxima Medical Center, NetherlandsReviewed by:
Enrique Gomez-Pomar, University of Kentucky, United StatesCopyright: © 2025 Unal, Beken, Anuk Ince, Turan, Korkmaz Toygar, Ecevit, Akcan, Akın, Aktas, Ciftdemir, Altuncu, Altunhan, Arcagok, Armangil, Arun Ozer, Aydın, Bezirganoglu, Bilgin, Calısıcı, Calkavur, Celik, Celik, Cetinkaya, Cetinkaya, Demirel, Demirel, Dogan, Doğan, Durukan, Engur, Erener Ercan, Gokmen, Guney Varal, Gulası, Gunlemez, Gursoy, Hakyemez Toptan, Hamitoğlu, Isleyen, Iyigun, Kader, Kahvecioğlu, Kaykı, Kostu, Kurnaz, Mammadalıyev, Mungan Akin, Narlı, Okulu, Okur, Olukman, Ovalı, Ozcan, Ozdemir, Ozdemir, Ozkan, Sandal, Sarıcı, Sivrikaya, Siyah Bilgin, Sundus, Surmeli Onay, Simsek, Tandırcıoğlu, Tanrıverdi, Tekgunduz, Terek, Tunc, Tunc, Tutak, Tufekcioğlu, Tuzun Erdogan, Ulu, Ulubas Isik, Uras, Uslu, Unal, Yılmaz and Moniri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Serdar Beken, c2VyYmVrZW5AZ21haWwuY29t
†These authors share first authorship
The evaluation of caffeine treatment usage in neonates admitted to neonatal intensive care units in Turkiye: A survey study
‡ORCID:
Serdar Beken
orcid.org/0000-0002-8609-2684
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.