 Leticia Serra1,2
Leticia Serra1,2 Débora Patrícia Rios2
Débora Patrícia Rios2 Mino Rios3
Mino Rios3 Breno Lima de Almeida1
Breno Lima de Almeida1 Kelly de Souza Fernandes2
Kelly de Souza Fernandes2 Rita Lucena4
Rita Lucena4 Isadora Cristina de Siqueira1*
Isadora Cristina de Siqueira1*
- 1Laboratorio de Investigação em Saúde Global e Doenças Negligenciadas, Instituto Gonçalo Moniz- Fundação Oswaldo Cruz, Salvador, Brazil
- 2Centro Estadual de Prevenção e Reabilitação da Pessoa com Deficiência (CEPRED), Salvador, Brazil
- 3Departamento de Psicologia, Universidade do Estado da Bahia, Salvador, Brazil
- 4Departamento de Neurociências e Saúde Mental, Faculdade de Medicina da Bahia, Universidade Federal da Bahia, Salvador, Brasil
Background: The Zika virus outbreak, which occurred from 2015 to 2016 in Brazil, resulted in the birth of neonates with brain malformations arising from Congenital Zika Syndrome (CZS). The characterization of primitive reflexes and their relationships with other motor characteristics, easily clinically detectable by health professionals, can aid in establishing motor prognosis in affected children.
Objective: To describe reflex patterns in children with Cerebral Palsy (CP) due to CZS, and investigate associations with other motor features. Method: Observational cross-sectional study involving infants with CZS aged between 12 and 36 months. Primitive reflexes, protective reaction and markers of motor phenotype were evaluated.
Results: 48 children, median age: 19 months, were enrolled, most (79.2%) presented very severe CP (GMFCS 5), the persistence of more than 5 primitive reflexes (55%) and motor development age between 3 and 6 months (33.3%) (Bayley-III). A reduced ability to acquire motor skills was associated with the total number of persistent reflexes (rho = −0.45, p < 0.01). Asymmetrical Tonic Neck Reflex (ATNR) correlated with GMFCS level (rho = 0.49, p < 0.001). Lower motor development age was linked to abnormal posturing (p < 0.001) and absence of Parachute Reaction (p < 0.001).
Conclusion: Infants with CP due to CZS present severe motor abnormalities. Lower motor development age is associated with the persistence of more than 5 primitive reflexes, abnormal posturing and the absence of Parachute Reaction. Parachute Reaction appears to be a prognostic marker of motor impairment severity in CZS-affected infants.
Introduction
The Zika virus (ZIKV) is an emergent flavivirus transmitted by the Aedes mosquitoes (1). In 2015, ZIKV transmission was confirmed in Brazil (2), resulting in a large-scale epidemic that later spread to other countries throughout the Americas. In late 2015, an unexpected outbreak of newborns with microcephaly prompted a state of public health emergency in Brazil. The ZIKV maternal-fetal transmission was confirmed, and until 2020, 3,563 cases of Congenital Zika Infection (CZI) were confirmed (3).
CZI can result in a spectrum of clinical manifestations, including asymptomatic cases (4). Congenital Zika Syndrome (CZS) is characterized by neurodevelopmental delays, microcephaly, and severe Cerebral Palsy (CP) (5, 6). Severe motor delay, persistence of primitive reflexes, and postural abnormalities have been described (7–11). However, the literature contains no studies associating the responses of primitive reflexes in children with CVS with other phenotypic markers. The present study aimed to investigate reflex responses in infants with CP arising from CZS, and explore their associations with other phenotypic markers.
Methods
Study design and participants
The present observational, cross-sectional study evaluated reflex responses and motor characteristics in infants with CZS presenting CP. Study participants were recruited at the Center for Prevention and Rehabilitation of Disabilities of the State of Bahia (CEPRED), located in the city of Salvador (Bahia, Brazil). The CEPRED is the state reference center for follow-up of children with CZS in the local public health system.
Infant age ranged between 12 and 36 months, including both sexes, born during the 2015–2016 outbreak of the Zika virus in Brazil. The inclusion criteria consisted of CZS, either confirmed by ZIKV test positivity or not, as well as clinical findings including neurological malformations and/or specific neuroimaging findings (12). All other congenital infections were excluded. Children presenting arthrogryposis were also excluded, as this condition could interfere with the results obtained from the assessment.
Microcephaly was defined according to the International Fetal and Newborn Growth consortium for the 21st Century (Intergrowth-21) criteria. Microcephaly was considered when the head circumference at birth measured less than two standard deviations below the average, while severe microcephaly was determined when measurements were less than three standard deviations below the average (13).
Assessments and procedures
Motor function testing and reflex responses were assessed via clinical and instrumental analysis. Clinical evaluations included the inspection of the infant's posture and movements (14–16). Postural symmetry was considered when an imaginary line through the shoulders and hip joints runs parallel (14). Abnormal tonic posturing was considered when an infant was placed in a supine position and was unable to actively move their limbs, remaining tonically fixed in an abnormal posture.
Gross Motor Subtest raw scores, derived from the Bayley-III Scales of Infant and Toddler Development, were used to estimate the developmental age of child motor development. The Bayley III is a standardized and specific instrument for evaluating cognitive, language, and motor development (17, 18). The Gross Motor Function Classification System (GMFCS) is a five-level framework designed to describe and categorize the severity of motor impairments in children with cerebral palsy (CP) and it has been utilized to classify the motor function of individuals with CP. Level I represents the best gross motor abilities (CP children and youth who walk without limitations), and level V represents the poorest function (children who require a wheelchair) (19). Finally, a checklist was elaborated to evaluate CP topography, global tone, posture and active mobility, as well as reflexes, protective reaction and motor skills (15–21).
The following reflexes were evaluated: Moro Reflex, Asymmetrical Cervical Tonic Reflex, Symmetrical Cervical Tonic Reflex, Labyrinthine Tonic Reflex, Palmar Grasp, Plantar Grasp, Positive Support Reflex, Gait Reflex, Cross Extension Reflex. The Parachute Reaction was employed to assess protective reaction (15, 16, 22). Based on tools and studies (17, 20, 22), the following acquired motor skills were evaluated: complete/incomplete cervical control, partial/total rolling, sitting with/without support, crawling movement, transition from supine to sitting position, standing from sitting position, standing with/without support, walking with/without support, maintenance of crawling position, crawling on stomach.
Procedures
The evaluation sequence was similar for all children, starting with a visual inspection, in the supine position, of posture, CP topography and active movements. Next, the Bayley-III and GMFCS scales were applied. Finally, motor skills, reflexes and protective reaction were evaluated. All children were evaluated by the same trained physical therapist with experience in infants with CZS.
Data management and statistical analysis
Data entry and management were performed using REDCap 9.3.1 software (© 2021 Vanderbilt University). Statistical analysis was performed using SPSS v21.0 software for Windows. Descriptive statistics were calculated for the clinical and motor parameters evaluated. Student's T test was used to determine differences between mean values of the number of motor skills and the presence of Parachute Reaction and Abnormal Posturing. Also, for Motor Development Age and presence of Parachute Reaction. Spearman's correlation coefficient was used to determine associations between the number of motor skills acquired and Palmar Grip Reflex response grade, Motor Development Age and total number of Persistent Reflexes. Simple linear regression was applied to verify correlations between Motor Development Age and the presence of Parachute Reaction, Intergrowth and total number of Primitive Reflexes. Statistical significance was considered when p < 0.05.
Ethical considerations
The present study was approved by the Institutional Review Board of the Gonçalo Muniz Institute, Oswaldo Cruz Foundation (IGM-FIOCRUZ, protocol no. 1.935.854/2016). The legal guardians of all infants provided written informed consent.
Results
Eighty-five children were recruited, 20 of whom did not attend their scheduled evaluations, six were excluded due to arthrogryposis and two did not complete the entire assessment. In all, 48 infants were enrolled.
The maternal socioeconomic profile is detailed in Table 1. The majority of the mothers self-identified as Black or mixed-race, and their household monthly income was predominantly low, with a mean of 1.3 ± 0.6 Brazilian minimum wages.
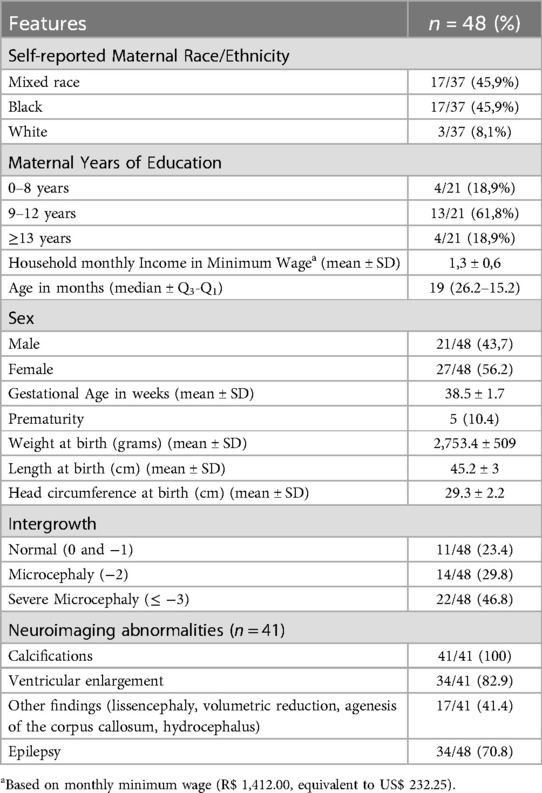
Table 1. Clinical and demographical features of 48 infants with Congenital Zika Syndrome (Salvador, Bahia-Brazil).
The median age of the infants was 19 (26.2–15.5) months; 56.2% were female. Mean gestational age at birth was 38 ± 1.7 weeks, with prematurity identified in 10.4%. Regarding head circumference at birth, 46.8% presented severe microcephaly (Intergrowth ≤−3). The clinical and demographical characteristics of the participants are shown in Table 1.
The main features observed were axial hypotonia with hypertonic limbs, symmetric posture, bilateral CP topography, and abnormal posturing in a supine position and few children without movement restrictions. The motor characteristics of the studied infants are shown in Figure 1.
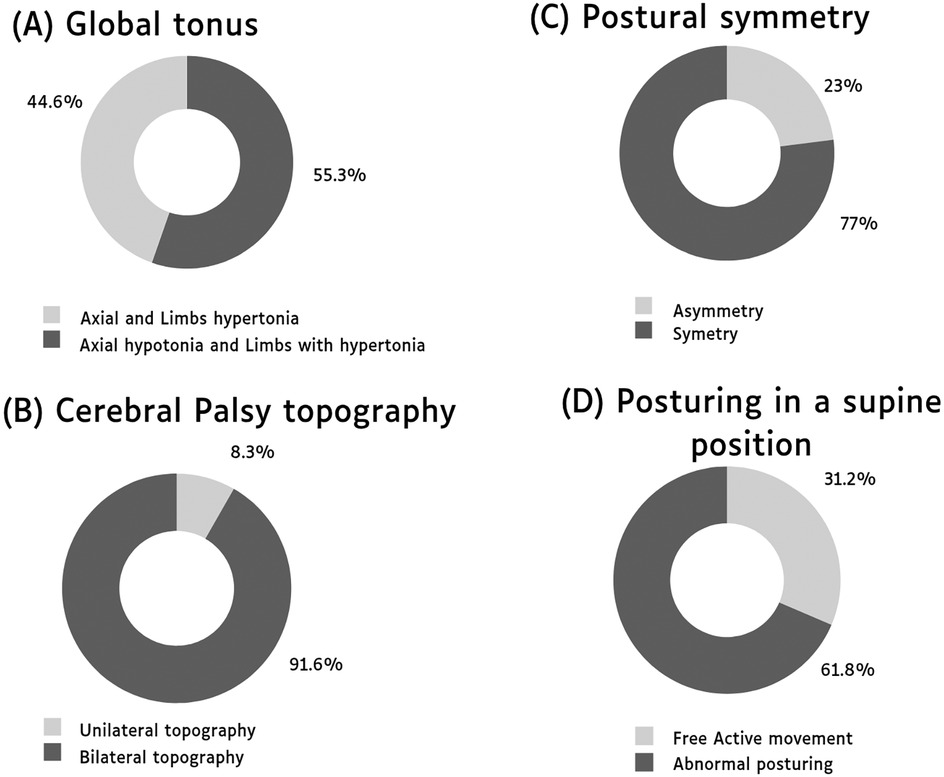
Figure 1. Distribution of key motor characteristics in individuals with cerebral palsy due to Congenital Zika Syndrome. (A) Global tonus. (B) Cerebral palsy topography. (C) Postural symmetry. (D) Posturing in a supine position.
Twenty-two children (45.8%) had no motor skill acquisition, followed by 14 (29.2%) with at least incomplete cervical control. There was a predominance of children with GMFCS level 5 and motor age between 3 and 6 months. The acquisition of motor skills in these children is detailed in Table 2. The Parachute Reaction was observed in nine (19.1%) infants, with detailed information on Primitive Reflexes listed in Table 3.
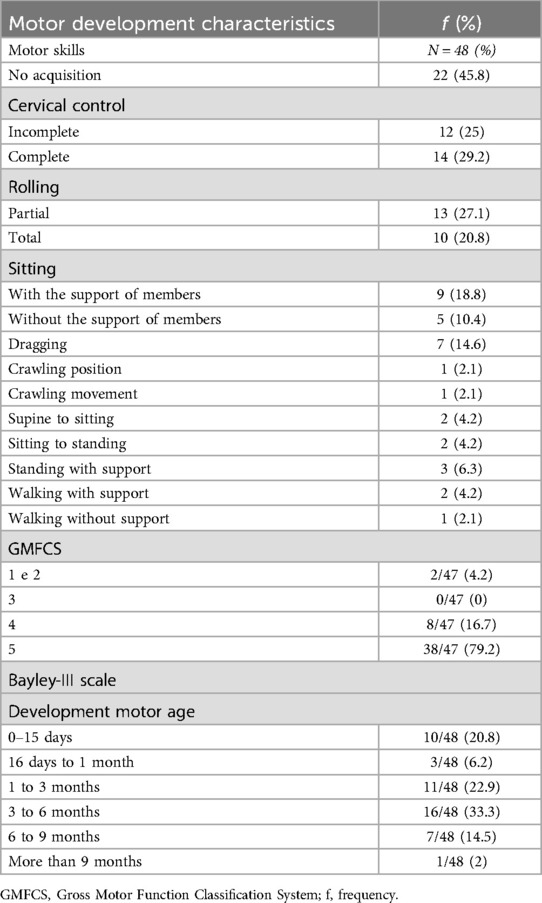
Table 2. Motor development characteristics in infants with Congenital Zika Syndrome, (Salvador, Bahia-Brazil).
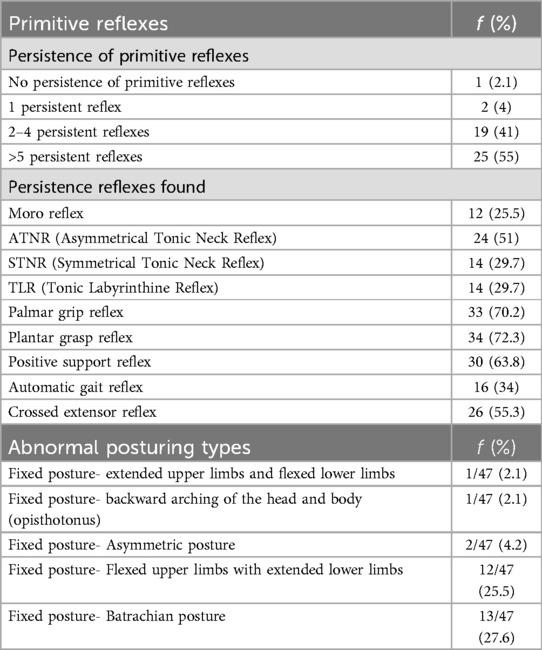
Table 3. Frequency of persistent primitive reflexes and types of abnormal posturing in infants with Congenital Zika Syndrome (Salvador, Bahia-Brazil).
Primitive reflexes and motor skills
The lack of ability to acquire motor skills was correlated with higher grades of Palmar Grip Reflex responses (Left rho = −0.37, p < 0.01; Right rho = −0.45, p < 0.05), and the total number of persistent reflexes (rho = −0.45, p < 0.01). The presence of the Moro Reflex did not seem to significantly affect the number of motor skills acquired.
Primitive reflexes and CP
The presence of Asymmetrical Tonic Neck Reflex (ATNR) was found to be correlated with GMFCS classification (rho = 0.49, p < 0.001).
Motor development age, abnormal posturing and parachute reaction
We identified a correlation between Motor Development Age and the Number of Persistent Reflexes (rho = −0.3, p < 0.05). In addition, abnormal posturing was significantly associated (p < 0.001) with Motor Development Age, as a lower average development age was observed in the presence of abnormal posturing.
A younger Motor Development Age was also associated with the absence of the Parachute Reaction (p < 0.001). Accordingly, the presence of the Parachute Reaction was identified as a predictor of greater Motor Development Age (β=0.743; p < 0.001). By contrast, Intergrowth measures offered lower predictive power of Motor Development Age (β=0.407; p < 0.001).
Discussion
The study was conducted at a public rehabilitation center in Bahia, Brazil, one of the regions most severely impacted by the Zika epidemic. The maternal socioeconomic profile observed in this study aligns with findings from other Brazilian studies involving pregnant women infected with ZIKV (23, 24).
The present study investigated reflex patterns in infants with CP due to CZS, as well as motor characteristics. In children with severe CP, marked impairment of global motricity was observed. In addition, these children also presented the persistence of more than five primitive reflexes, different presentations of abnormal posturing in the supine position, and impaired limb mobility and motor development. A very low age of motor development was also noted, as well as a low number of acquisitions of motor milestones, e.g., the ability to maintain sitting or standing positions. The presence of hypotonia in combination with hypertonia was also observed, similar to another previous study (25).
Other studies have previously demonstrated the persistence of primitive reflexes in children with CZS (8, 9, 10, 26, 27). A study by Armani et al. (28) evaluated six reflexes, with persistence identified in 56% of the participants. Our study aimed to expand the scope of reflex evaluations by testing nine reflexes, with persistence observed in 97.8% of the infants studied.
Several presentations of abnormal posturing were observed in 68.1% of our sample. Other studies on CZS in infants have reported the presence of abnormal posturing, such as axial extensor postures or flexor postures (6), in 74.7% of the population studied, while dystonic postures (8) were present in 95.2% of infants. Hull, Parnes and Jankovic (29) suggested that abnormal posturing, such as opisthotonos, is often associated with dystonic posturing of the limbs. While it is possible that an association between dystonia and abnormal posturing in our population, this aspect was not investigated.
We identified a correlation between the persistence of primitive reflexes and lower number of acquired Motor Skills, younger Motor Development Age, and greater CP severity. Despite a high prevalence of primitive reflexes, the presence of abnormal posturing appeared to be strongly associated with younger Motor Development Age. It is possible that, when lying in a supine position, exacerbated basal tonus restrains the free movement of the body, severely limiting motor acquisition, as was suggested by Van der linden et al. (8), who argued that the severity and quality of dystonic postures, among other factors, can vary in accordance with body position. Abnormal posturing, when present, provokes discomfort, and its consequences may lead to contractures and deformities (29). On the other hand, it is possible that while primitive reflexes may be observed when elicited by a certain stimulus, these are not necessarily the only factors underlying the inhibition of global motricity. More studies are needed to fully elucidate the mechanisms involved in motor behavior in the context of CZS.
The Parachute Reaction is known to offer predictive value in CP after nine months of age (30). Herein, all of the enrolled infants exhibited some degree of CP. Our findings indicate that, in the children with CP due to CZS who were 12 months or older, the absence of a parachute reaction may constitute a prognostic marker of younger Motor Development Age. While other studies have demonstrated associations between Intergrowth score and motor development (31, 32), as was observed herein, our results suggest a correlation between the Parachute Reaction and higher Motor Development Age.
This study aimed to comprehensively detail reflex patterns and establish associations with other relevant clinical characteristics. Our findings demonstrate that infants with CP due to CZS exhibit severe motor abnormalities, abnormal posturing, and the persistence of primitive reflexes, all of which are associated with impaired motor development. Parachute Reaction appears to be a prognostic marker of motor impairment severity in CZS-affected infants.
A selection bias may exist, since severe CP presentations predominated in our sample, as the study was carried out at a Reference Rehabilitation Service specializing in auditory, physical and mental impairment. Children with milder presentations may not have been referred to the rehabilitation center. Indeed, herein, this fact proved to be advantageous, offering the possibility to describe as extensively as possible the characteristics of CZS-associated impairment in these children, similarly to other studies conducted in different regions of Brazil (7, 8, 9, 25). Moreover, further studies are needed to clarify the role of the Parachute Reaction and to validate its use as a clinical marker for motor prognosis in this population. Additionally, research involving children with less severe CZI is necessary, as the majority of participants in this study had CP with severe disabilities, classified as GMFCS levels IV and V.
Given the widespread presence of Aedes mosquitoes and the ongoing threat of future ZIKV outbreaks (33), the findings presented here provide valuable insights and could contribute to the management and monitoring of newly affected children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The present study was approved by the Institutional Review Board of the Gonçalo Muniz Institute, Oswaldo Cruz Foundation (IGM-FIOCRUZ, protocol no. 1.935.854/2016). The legal guardians of all infants provided written informed consent.
Author contributions
LS: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. DR: Investigation, Methodology, Writing – original draft, Writing – review & editing. MR: Formal Analysis, Writing – original draft, Writing – review & editing. BA: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. KF: Investigation, Supervision, Writing – original draft, Writing – review & editing. RL: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. IS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Financial support was provided by CNPq-National Council for Scientific and Technological Development (443875/2018-9) and PPSUS/BA-FAPESB/SESAB/CNPq/MS (5125/2017). ICS was supported by CNPq (316456/2021-7).
Acknowledgments
The authors are grateful to the participants, their parents, and the health professionals at CEPRED who were involved in the patients' clinical treatment. In addition, Andris K. Walter provided assistance with English language revision and manuscript copyediting.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Musso D, Cao-Lormeau VM, Gubler DJ. Zika Virus: following the path of dengue and chikungunya? Lancet. (2015) 386:243–4. doi: 10.1016/S0140-6736(15)61273-9
2. Zanluca C, Melo VC, Mosimann AL, Santos GI, Santos CN, Luz K. First report of autochthonous transmission of Zika virus in Brazil. Mem Inst Oswaldo Cruz. (2015) 110(4):569–72. doi: 10.1590/0074-02760150192
3. Ministério da Saúde (Brasil), Boletim Epidemiológico, Secretaria de Vigilância em Saúde. Situação epidemiológica da síndrome congênita associada à infecção pelo vírus Zika em 2020, até a SE 45. Volume 51 | No 47. (2020). Disponível em. Available online at: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/boletins-epidemiologicos/edicoes/2020/boletim_epidemiologico_svs_47.pdf (Accessed August 15, 2024).
4. de Almeida BL, Giovanetti M, Oliveira JV, Carvalho TCX, Figueiredo EM, Pellegrini R, et al. Detection and sequencing of Zika virus in normocephalic newborns with congenital Zika infection. Int J Infect Dis. (2022) 114:128–31. doi: 10.1016/j.ijid.2021.10.051
5. Moore CA, Staples JE, Dobyns WB, Pessoa A, Ventura CV, da Fonseca EB, et al. Characterizing the pattern of anomalies in congenital Zika syndrome for pediatric clinicians. JAMA Pediatr. (2017) 171(3):288–95. doi: 10.1001/jamapediatrics.2016.3982
6. Del Campo M, Feitosa IM, Ribeiro EM, Horovitz DDG, Pessoa ALS, França GVA, et al. The phenotypic spectrum of congenital Zika syndrome. Am J Med Genet A. (2017) 173(4):841–57. doi: 10.1002/ajmg.a.38170
7. Marques FJP, Teixeira MCS, Barra RR, de Lima FM, Dias BLS, Pupe C, et al. Children born with congenital Zika syndrome display atypical gross motor development and a higher risk for cerebral palsy. J Child Neurol. (2019) 34(2):81–5. doi: 10.1177/0883073818811234
8. van der Linden H, Silveira-Moriyama L, van der Linden V, et al. Movement disorders in children with congenital Zika virus syndrome. Brain Dev. (2020) 42(10):720–9. doi: 10.1016/j.braindev.2020.06.016
9. da Silva AAm, Ganz JSS, da Silva Sousa P, Doriqui MJR, Ribeiro MRC, Branco MDRFC, et al. Early growth and neurologic outcomes of infants with probable congenital Zika virus syndrome. Emerg Infect Dis. (2016) 22(11):1953–6. doi: 10.3201/eid2211.160956
10. Pessoa A, van der Linden V, Yeargin-Allsopp M, Carvalho MDCG, Ribeiro EM, Van Naarden Braun K, et al. Motor abnormalities and epilepsy in infants and children with evidence of congenital Zika virus infection. Pediatrics. (2018) 141(Suppl 2):S167–79. doi: 10.1542/peds.2017-2038F
11. Brasil P, Pereira JP Jr, Moreira ME, Ribeiro Nogueira RM, Damasceno L, Wakimoto M, et al. Zika virus infection in pregnant women in Rio de Janeiro. N Engl J Med. (2016) 375(24):2321–34. doi: 10.1056/NEJMoa1602412
12. França GV, Schuler-Faccini L, Oliveira WK, Henriques CMP, Carmo EH, Pedi VD, et al. Congenital Zika virus syndrome in Brazil: a case series of the first 1501 livebirths with complete investigation. Lancet. (2016) 388(10047):891–7. doi: 10.1016/S0140-6736(16)30902-3
13. Villar J, Cheikh Ismail L, Victora CG, Ohuma EO, Bertino E, Altman DG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project. Lancet. (2014) 384(9946):857–68. doi: 10.1016/S0140-6736(14)60932-6
14. Einspieler C, Bos AF, Krieber-Tomantschger M, Alvarado E, Barbosa VM, Bertoncelli N, et al. Cerebral palsy: early markers of clinical phenotype and functional outcome. J Clin Med. (2019) 8(10):1616. doi: 10.3390/jcm8101616
15. Gherpelli JLD. Propedêutica neurológica do recém-nascido e sua evolução. Rev Med. (2003) 82(1–4):22–3. doi: 10.11606/issn.1679-9836.v82i1-4p22-33
16. Araújo MGM. Avaliação clínico-neurológica de recém-nascidos subnutridos e normais a termo: acompanhamento do desenvolvimento no primeiro ano de vida e detecção de alterações (Doctoral thesis). Campinas, SP: Campinas State University (1998).
17. Bayley N. Bayley Scales of Infant and Toddler Development. 3rd ed. Santo Antônio: Psychological Corporation (2006).
18. Madaschi V, Mecca TP, Macedo EC, Silvestre Paula C. BayleyIII scales of infant and toddler development: transcultural adaptation and psychometric properties. Paid (Ribeirão Preto). (2016) 26(64):189–97. doi: 10.1590/1982-43272664201606
19. Silva DBR, Pfeifer LI, Funayama CAR. GMFCS—E&R: Sistema de classificação da função motora grossa- ampliado e revisto. [S.l: s.n.] (2010).
20. Romeo DM, Ricci D, Brogna C, Mercuri E. Use of the hammersmith infant neurological examination in infants with cerebral palsy: a critical review of the literature. Dev Med Child Neurol. (2016) 58(3):240–5. doi: 10.1111/dmcn.12876
21. Rosenbaum P, Paneth N, Leviton A, Goldstein M, Baz M. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol. (2007) 109:8–14. doi: 10.1111/j.1469-8749.2007.tb12610.x
22. Flehmig I. Texto e Atlas do Desenvolvimento Motor Normal e Seus Desvios no Lactente: Diagnóstico e Tratamento Precoce do Nascimento até 18 mês. São Paulo: Atheneu (2002).
23. França TLB, Medeiros WR, Souza NL, Longo E, Pereira SA, França TBDO, et al. Growth and development of children with microcephaly associated with congenital Zika virus syndrome in Brazil. Int J Environ Res Public Health. (2018) 125(9):1990. doi: 10.3390/ijerph15091990
24. de Araújo TVB, Ximenes RAA, Miranda-Filho DB, Souza WV, Montarroyos UR, de Melo APL, et al. Association between microcephaly, Zika virus infection, and other risk factors in Brazil: final report of a case-control study [published correction appears in Lancet Infect Dis. 2018 Feb;18(2):139. doi: 10.1016/S1473-3099(18)30001-X]. Lancet Infect Dis. (2018) 18(3):328–36. doi: 10.1016/S1473-3099(17)30727-2
25. Pereira HVFS, Dos Santos SP, Amâncio APRL, de Oliveira-Szejnfeld PS, Flor EO, de Sales Tavares J, et al. Neurological outcomes of congenital Zika syndrome in toddlers and preschoolers: a case series. Lancet Child Adolesc Health. (2020) 4(5):378–87. doi: 10.1016/S2352-4642(20)30041-9
26. Ventura PA, Lage MLC, de Carvalho AL, Fernandes AS, Taguchi TB, Nascimento-Carvalho CM. Early gross motor development among Brazilian children with microcephaly born right after Zika virus infection outbreak. J Dev Behav Pediatr. (2020) 41(2):134–40. doi: 10.1097/DBP.0000000000000722
27. Carvalho AL, Ventura P, Taguchi T, Brandi I, Brites C, Lucena R. Cerebral palsy in children with congenital Zika syndrome: a 2-year neurodevelopmental follow-up. J Child Neurol. (2020) 35(3):202–7. doi: 10.1177/0883073819885724
28. Armani-Franceschi G, Luz C, Lucena PH, d’Afonseca D, Sales H, Carvalho AL, et al. Botulinum toxin type A in the spasticity of cerebral palsy related to congenital Zika syndrome: an observational study. Dev Neurorehabil. (2022) 25(3):162–9. doi: 10.1080/17518423.2021.1960917
29. Hull M, Parnes M, Jankovic J. Botulinum neurotoxin injections in childhood opisthotonus. Toxins (Basel). (2021) 13(2):137. doi: 10.3390/toxins13020137
30. Hamer EG, Hadders-Algra M. Prognostic significance of neurological signs in high-risk infants—a systematic review. Dev Med Child Neurol. (2016) 58(Suppl 4):53–60. doi: 10.1111/dmcn.13051
31. Massetti T, Herrero D, Alencar J, Silva T, Moriyama C, Gehrke F, et al. Clinical characteristics of children with congenital Zika syndrome: a case series. Arq Neuropsiquiatr. (2020) 78(7):403–11. doi: 10.1590/0004-282X20200020
32. Melo A, Gama GL, Da Silva Júnior RA, De Assunção PL, Tavares JS, Da Silva MB, et al. Motor function in children with congenital Zika syndrome. Dev Med Child Neurol. (2020) 62(2):221–6. doi: 10.1111/dmcn.14227
33. WHO. Zika epidemiology update—May 2024. (2024). Available online at: https://www.who.int/publications/m/item/zika-epidemiology-update-may-2024 (cited 2025 January 18).
Keywords: Congenital Zika Syndrome, developmental disabilities, cerebral palsy, abnormal reflex, motor skills, abnormal posturing
Citation: Serra L, Rios DP, Rios M, de Almeida BL, Fernandes KdS, Lucena R and de Siqueira IC (2025) Primitive reflexes in infants with cerebral palsy due to Congenital Zika Syndrome and its relationship with other motor features. Front. Pediatr. 13:1483959. doi: 10.3389/fped.2025.1483959
Received: 21 August 2024; Accepted: 27 January 2025;
Published: 7 March 2025.
Edited by:
Hans Van Rostenberghe, University of Science Malaysia (USM), MalaysiaReviewed by:
Simon Carlo, Ponce Health Sciences University, Puerto RicoAshok Kumar Banskota, Hospital and Rehabilitation Centre for Disabled Children, Nepal
Copyright: © 2025 Serra, Rios, Rios, de Almeida, Fernandes, Lucena and de Siqueira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Isadora Cristina de Siqueira, aXNhZG9yYS5zaXF1ZWlyYUBmaW9jcnV6LmJy