
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr., 14 March 2025
Sec. Pediatric Orthopedics
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1474412
 Huthaifa Atallah1*
Huthaifa Atallah1* Rabee Naeem2Amneh Alshawabka1
Rabee Naeem2Amneh Alshawabka1 Anas S. Said3Huda Alfatafta4
Anas S. Said3Huda Alfatafta4 Evelin Derkács4Dorottya Varga4
Evelin Derkács4Dorottya Varga4 Bálint Molics5
Bálint Molics5
Introduction: Metopic craniosynostosis results in a deformed skull and hence, impacts brain growth and development. Surgery is usually applied to treat this trigonocephalic head malformation. Helmet therapy is also utilized in craniosynostosis treatment after the surgery. However, data on use of 3D printed helmets in treatment of metopic craniosynostosis is lacking. Most of the studies are published about molding helmets. Moreover, there is a lack of evidence on its clinical outcomes. Therefore, the aim of this study was to assess the use of a 3D printed helmet in treating a metopic craniosynostosis, after the endoscopy-assisted craniotomy surgical intervention.
Case description: A 7-month-old infant who was diagnosed with metopic craniosynostosis was referred from the neurosurgeon for a custom-made 3D printed helmet, after a surgical intervention. A certified orthotist has performed further assessment, scanning, designing, and printing a customized 3D printed helmet. Thereafter, fitting and delivery were successfully completed. Patient has come for two follow-up appointments, at 2 and 5 months.
Results: Five months after the initial fitting, the head shape correction and reduction of deformity were noticed through anthropometric measures. The cranial vault asymmetrical index (CVAI) decreased from 7% to 2% and the cranial vault asymmetry (CVA) reduced from 7 mm to 3 mm.
Conclusion: This case report illustrates the utilization of 3D printing technology in the treatment of metopic craniosynostosis. 3D printed helmets may offer an appropriate option for treating selective infants with metopic craniosynostosis. Thus, would introduce the 3D helmet as a following intervention for such cases after the endoscopy-assisted craniotomy surgical intervention. Further studies with a higher number of cases are compulsory to assess the effectiveness of treating metopic craniosynostosis by 3D printed helmets instead of molding helmets.
The metopic suture extends anteriorly from the nose to the sagittal suture at the top of the skull. It is the first skull suture to close physiologically, starting as early as 3 months (1–3). Premature fusion of the metopic suture in infants results in a condition called metopic craniosynostosis. Generally, when there is premature fusion of the sutures, the skull growth in that direction will be restricted, resulting in a continued growth perpendicular to other sutures that are open. This results in a deformed skull. A newborn with metopic craniosynostosis typically has a head that is formed like a triangle, with the widest half in the rear and the narrowest part in the front (4). Consequently, this trigonocephalic head malformation can impact brain growth and development. Severity of metopic craniosynostosis may vary and can result in long term complications. It can range from increase in intracranial pressure to neurodevelopment delays (2). Children with metopic craniosynostosis have been shown to be linked with the highest percentage of neurodevelopmental problems among all the single suture synostoses. Intellectual disability has been reported to be twice as high (4.8%) in children with metopic craniosynostosis as compared to those with sagittal or coronal synostosis (5). The incidence of metopic craniosynostosis varies widely, ranging from 1:700 to 1:15,000 newborns (6, 7). In the last few decades, its incidence has been rising, currently making it the second most common type of craniosynostosis (2).
Various treatment guidelines and studies have analysed the use of helmets especially in positional head deformities (8–17). Custom-made molding helmets are also used in various forms of craniosynostosis treatment; especially in patients undergoing endoscopy-assisted craniotomy surgery (18–25). To our knowledge, there is no study reporting the use of a 3D printed helmet with metopic craniosynostosis infants. Therefore, the purpose of this case study was to assess the use of a custom-made 3D printed helmet in treatment of metopic craniosynostosis, following an endoscopy-assisted craniotomy surgery. The cranial vault asymmetry (CVA) and cranial vault asymmetry index (CVAI) were calculated to evaluate the functionality of the 3D-printed helmet.
A 7-month-old infant was brought for initial physician assessment due to concerns of abnormal head symmetry. Birth and developmental history were insignificant. There was no intellectual disability and milestones were not delayed. She was born full term by normal vaginal delivery. There was no family history of craniosynostosis. History revealed that she was diagnosed with metopic craniosynostosis at the age of 5 weeks. Physical examination suggested closure of metopic suture. This was confirmed with radiological assessment by Computed tomography (CT) scan with 3D reconstruction (Figure 1). The patient was assessed by neurosurgery and an endoscopy-assisted craniotomy surgical intervention was applied at the age of 5 months. Unfortunately, and due to lack of certified orthotist with helmet experiences, she was referred to a certified orthotist for a custom-made helmet at the age of 7 months.
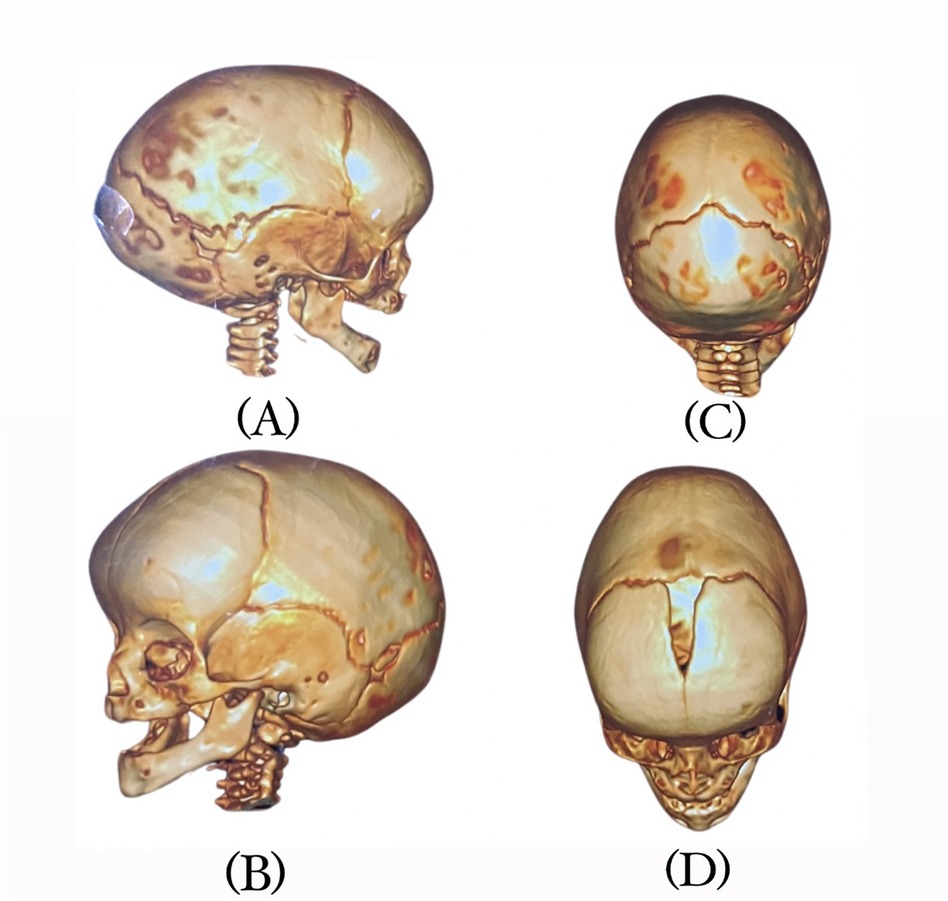
Figure 1. CT scan views of the infant's head: (A) right side, (B) left side, (C) superior, and (D) anterio-superior.
Ethical approval was obtained from the Ministry of Health (IRB-5680). Further orthotist assessment included measurements of head circumference, cranial diameters, palpation of the fontanelle and suture lines, and observational assessments of head shape, posturing and movements. Examination of head showed forward displacement of right ear, posterior flattening, and anterior bossing of the forehead (Figure 1). There was no abnormal head or neck posturing, rotation or tilting, and the range of motion was within normal. Multiple factors were considered in the decision to proceed with helmet therapy which was carried out after consulting with referring physician and parent's agreement. The main factors were age of the patient, moderate severity of deformity, skull pliability and parent's preferences. The first goal was to keep the abnormality from worsening. The second was to correct the deformity and restore the head to its natural shape as much as possible.
A certified orthotist utilized a patch to refer to landmarks including the glabella, opisthocranion, ears, occipital bone, orbital area, exocanthion, and tragion onto the infant's head, while the head was maintained in a neutral position (26). The anterior-posterior (A-P) and medio-lateral (M-L) diameters, and circumference at the apex of asymmetry were measured using computed metrics in Rodin4D software (Rodin4D, Eqwal group family, France). To compare the results before and after helmet therapy, the cranial vault asymmetry (CVA) and cranial vault asymmetrical index (CVAI) were computed and selected as reference measurements. The structural sensor scanner with a resolution of 1280960 pixels was used which takes 3 to 5 min to scan (Figure 2). Mesh mixer software (Autodesk company, United states) was used to clean up the scan.
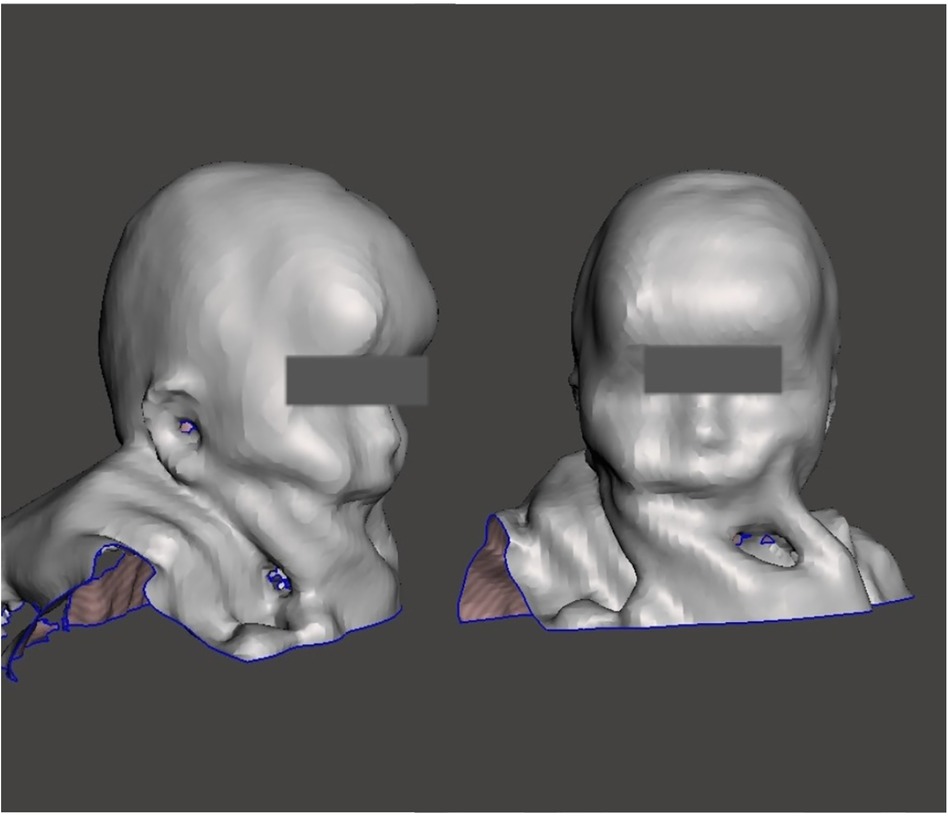
Figure 2. 3D scan of the infant's head.
After the scanning and measurements, the three-dimensional file was converted into Rodin4D-neo software format (Rodin4D, Eqwal group family, France) for rectification process. Meshmixer software (Autodesk company, United states) was used to create the trim lines that extend above the glabella to the inferior occipital bone above vertebra C2. ZBrush software was used to convert the mesh into a quad mesh so that it could be edited in CAD software.
Fusion 360 software (Autodesk company, United states) was utilized to generate the design of solid CAD for the helmet, with 4 mm (0.16 cm) thickness. Holes and padding measurements were added to the design. ZBrush software (Maxon company, German) was used to add personal features like pattern and text. Based on the necessary rigidity and flexibility of the helmet, the infill parameters were determined. The 3D design was sliced using the Cura Computer-Aided Manufacturing (CAM) software, which generated the instructions for the printer. The cube infill type was selected to provide the best impact resistance. The following printer settings were used; nozzle temperature 220° Celsius, bed temperature 60° Celsius, infill 85%, infill type cube, vase printing mood, direct extrusion, printing speed 30 mm (about 1.18 in)/S, and nozzle size 0.4 mm (about 0.02 inches). Printing was carried out using Anycubic Cobra Max printer (Anycubic, China, Shenzhen) and thermoplastic polyurethane (TPU) filament with hardness 98 Shore A. This material can apply gentle pressure after fronto-orbital advancement surgery, as there is no need for a stiffer material.
After the initial check was successful, as shown in Figure 3. Checking any readiness was performed to assess the helmet's fitting. Pressure areas were assessed for pressure, friction or skin irritation. Afterwards, a strap was added, and 4 mm (about 0.16 in) of plastazote was applied for internal coverage to increase protection. Parents were advised to require their child to wear the helmet for approximately twenty-three hours per day. Bossing was controlled by pressure at the forehead. The helmet featured a posterior expansion area that would allow the bone to develop in that direction.

Figure 3. Infant fitted with a 3D-printed helmet.
The patient had two follow-up appointments; the first one took place two months after the initial fitting. Parents did not report any difficulty in compliance, or side effects like bruises, lacerations or skin damage. There were no concerns of neurological or developmental impairments. Repeat cranial assessment was done and measurements were recorded (Table 1). The variations in diameters and circumferences demonstrate the growth pattern of the head. This is accompanied by a decrease in CVA and CVAI, which shows head shape correction and reduction of deformity. Craniosynostosis progressed from moderate to mild in severity. Three months later, at the second follow-up, The CVAI decreased from 7% to 2% and the CVA reduced from 7 mm to 3 mm. Given the improvement of head appearance supported by anthropometric measures, the outcomes of helmet therapy were considered more than satisfactory. Parents reported that they found the helmet comfortable and light weight and were satisfied with the results of the helmet therapy.

Table 1. Measurements before and after helmet therapy, at 2 and 5 months.
The use of 3D printing technology is getting popular in medicine (27). Among broad range of 3D printed products, manufacturing of helmets using 3D printing technology is still uncommon in clinical practice. It has not become a standard of care; although there is a trend to adapt this technology among tech companies, manufacturers and commercial stakeholders (28–32). Food and Drug Authority (FDA) approvals have been obtained for 3D helmet manufacturing, which are largely based on non-clinical performance data (32, 33). It is interesting to observe that, in spite of commercial availability of these products, scientific data on clinical efficacy and outcomes is rarely documented (34). Similarly, data comparing safety and clinical efficacy of 3D printed helmet vs. molding helmets in treatment of paediatric skull deformities is also lacking.
The use of molding helmet is well documented for use of positional skull deformities such as plagiocephaly; while its use in metopic synostosis is mainly reported in relation to surgery (2). The findings of this study underscore the use of 3D helmet therapy and satisfactory reconstruction in a case of metopic craniosynostosis, after the endoscopy-assisted craniotomy surgical intervention. Our case had demonstrated the utilization of 3D-printed helmets following a surgical intervention appears to play a pivotal role in guiding and facilitating the natural skull reshaping of the infants. The personalized nature of these helmets, tailored to the unique cranial morphology of each patient, contributes significantly to the efficacy of the treatment by providing directed pressure to specific regions, thus promoting favourable growth patterns. The observed outcomes align with previous research highlighting the advantages of using 3D printing technology in the medical field (27, 34). By harnessing the precision and customization capabilities of this technology, clinicians can create comfortably fitting helmets, ensuring consistent pressure distribution without causing discomfort to the infant. Moreover, the ability to monitor and adjust the helmet design throughout the treatment period allows for dynamic adaptation to the changing needs of the patient, optimizing the therapeutic process.
The combination of precision and comfort in 3D-printed cranial helmets has been advocated as a transformative technology in the treatment of positional skull deformities. Conceptually, the principles of its use in single suture synostoses are not any different. Hence, it was considered to use this technology in an infant with metopic craniosynostosis. Molding helmets are typically made from rigid materials involving casting, rectification, and molding, which might not provide an optimal fit for every child. 3D printing allows for precision in creating helmets using scanning technologies to match the contours of an infant's head. This process is more comfortable to apply in infants as compared to the conventional process. The level of customization in 3D technology ensures a targeted pressure application, optimizing the corrective process, and preventing discomfort or skin related problems. Unlike molding helmets, 3D printed versions are often lighter and more breathable, which minimizes discomfort for infants. improving compliance with the recommended wear time. Consequently, this would enhance the effectiveness of the treatment. The prototyping and adjustments can be done quickly, offering early and timely interventions for patients. The positive outcomes of our case may be attributed to the benefits of 3D printed technology over conventional methods as mentioned above. Also, such a trial has not been attempted before and it opens an opportunity to consider 3D helmet technology when skull viability permits the treatment with conservative measures.
The standardization in manufacturing, printing, fabrication, application and maintenance of 3D printed medical devices could be a challenging process, especially in under resources places. Approvals from governing authorities may require a complex interplay of stakeholders who may not be well versed with this technology. Other than the hardware cost, financial aspects of licensure, software, staff training and maintenance contracts require formulation of policies and procedures to ensure a sustainable service. Various published guidelines may be used to advocate the need in a particular health setting. Since treatment of paediatric skull deformities require multidisciplinary services, institutional clinical management guidelines can help to ensure well formulated structure for orthotic use in cephalic disorders.
Published literature has largely emphasized the technical benefits, manufacturing accuracy and ease of application of 3D helmets (27, 28, 35–37); however, the outcome assessment should not only be limited to anthropometric measurements only. The skull deformities in infancy can be associated with neurodevelopmental delays and other neurological problems, which may manifest later in life (2, 38, 39). Since the helmet application is generally for months altogether, the changes in skull morphology occurs overtime. Similar to previous published literature on long term follow up using correction of cranial deformities with conventionally manufactured helmets (40), it is important to compare the long term outcomes with use of helmets manufactured using 3D printed technology. For neurocognitive or development delays which may demonstrate later in life, it may be difficult to determine if it was due to natural course of disease or helmet application or both. Also, outcomes of 3D helmet patients who already have neurological problems need to be studied as well. This renders the need of robust trials and scientific data to establish safety and clinical efficacy of use of 3D printed helmets.
This study highlights the utilization of 3D printing technology in the treatment of metopic craniosynostosis after an endoscopy-assisted craniotomy surgical intervention. Helmet printed with 3D technology may offer a suitable treatment option for metopic craniosynostosis in selective cases. It also highlights the possibility of exploring 3D helmet therapy rather than molding helmets for metopic craniosynostosis. The clinical efficacy of 3D printed helmets in craniosynostosis need to be further explored. As advancements continue in both medical imaging and manufacturing technologies, the potential for further refinement and broader application of 3D-printed helmets in treating craniosynostosis is becoming increasingly viable. Long-term follow-up studies with larger sample sizes are imperative to comprehensively evaluate the durability, safety and clinical efficacy of 3D helmets in craniosynostosis.
The study identifies a novel application of 3D printing technology; however, the scope could benefit from a broader discussion of comparative outcomes with traditional molding helmets. Skull growth and reshaping in infants is a complex phenomenon, involving various innate pathophysiological processes. Attempts to reshape skull using 3D technology requires different use of materials and design as compared to molding helmets. Given the nature of this study as a single case report, the cause-effect relationship cannot be reliably concluded, and requires robust multicentre trials to test the observed relationship. Thus would restricts the generalizability of the findings. In this study, patient was followed up for short duration. Long term clinical outcomes other than anthropometric measures also need to be considered in reporting. Also, obtaining the parent feedback would be more scientific if it was taken through a questionnaire rather than verbally. Finally, potential challenges and limitations in implementing 3D printing technology in clinical settings include cost, accessibility, and regulatory hurdles.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by The Ministry of Health—Al Basheer Hospital—Jordan. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
HA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. RN: Conceptualization, Data curation, Software, Writing – original draft, Methodology. AA: Methodology, Validation, Visualization, Writing – original draft. AS: Investigation, Methodology, Software, Writing – review & editing, Data curation. HA: Conceptualization, Resources, Visualization, Writing – review & editing. ED: Writing – review & editing, Resources. DV: Resources, Writing – review & editing. BM: Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research and/or publication of this article. The research was financed by the Thematic Excellence Program 2021 Health Sub-programme of the Ministry for Innovation and Technology in Hungary, within the framework of the EGA-10 project of the Pécs of University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Shruthi N, Gulati S. Craniosynostosis: a pediatric neurologist’s perspective. J Pediatr Neurosci. (2022) 17(Suppl 1):S54–60. doi: 10.4103/jpn.JPN_25_22
2. van der Meulen J. Metopic synostosis. Childs Nerv Syst. (2012) 28(9):1359–67. doi: 10.1007/s00381-012-1803-z
3. Alghamdi M, Alhumsi TR, Altweijri I, Alkhamis WH, Barasain O, Cardona-Londoño KJ, et al. Clinical and genetic characterization of craniosynostosis in Saudi Arabia. Front Pediatr. (2021) 9(582816). doi: 10.3389/fped.2021.582816
4. Kronig OD, Kronig SA, Vrooman H, Veenland J, Van Adrichem L, Surgery M. New method for quantification of the relative severity and (a) symmetry of isolated metopic synostosis. Int J Oral Maxillofac Surg. (2021) 50(11):1477–84. doi: 10.1016/j.ijom.2021.03.003
5. Shillito J Jr, Matson DD. Craniosynostosis: a review of 519 surgical patients. Pediatrics. (1968) 41(4):829–53. doi: 10.1542/peds.41.4.829
6. Alderman BW, Fernbach SK, Greene C, Mangione EJ, Ferguson SW. Diagnostic practice and the estimated prevalence of craniosynostosis in Colorado. Arch Pediatr Adolesc Med. (1997) 151(2):159–64. doi: 10.1001/archpedi.1997.02170390049009
7. Lajeunie E, Merrer ML, Marchac D, Renier D. Syndromal and nonsyndromal primary trigonocephaly: analysis of a series of 237 patients. Am J Med Genet. (1998) 75(2):211–5. doi: 10.1002/(SICI)1096-8628(19980113)75:2%3C211::AID-AJMG19%3E3.0.CO;2-S
8. Littlefield TR. Cranial remodeling devices: treatment of deformational plagiocephaly and postsurgical applications. Semin Pediatr Neurol. (2004) 4:268–77. doi: 10.1016/j.spen.2004.10.004
9. Dörhage KW, Beck-Broichsitter BE, von Grabe V, Sonntag A, Becker ST, Wiltfang J. Therapy effects of head orthoses in positional plagiocephaly. J Craniomaxillofac Surg. (2016) 44(10):1508–14. doi: 10.1016/j.jcms.2016.06.035
10. Freudlsperger C, Steinmacher S, Saure D, Bodem JP, Kühle R, Hoffmann J, et al. Impact of severity and therapy onset on helmet therapy in positional plagiocephaly. J Craniomaxillofac Surg. (2016) 44(2):110–5. doi: 10.1016/j.jcms.2015.11.016
11. Kluba S, Kraut W, Calgeer B, Reinert S, Krimmel M. Treatment of positional plagiocephaly–helmet or no helmet? J Craniomaxillofac Surg. (2014) 42(5):683–8. doi: 10.1016/j.jcms.2013.09.015
12. Wilbrand J-F, Wilbrand M, Malik CY, Howaldt H-P, Streckbein P, Schaaf H, et al. Complications in helmet therapy. J Craniomaxillofac Surg. (2012) 40(4):341–6. doi: 10.1016/j.jcms.2011.05.007
13. Couture DE, Crantford JC, Somasundaram A, Sanger C, Argenta AE, David LR. Efficacy of passive helmet therapy for deformational plagiocephaly: report of 1050 cases. Neurosurg Focus. (2013) 35(4):E4. doi: 10.3171/2013.8.FOCUS13258
14. Han M-h, Kang JY, Han HY, Cho Y-h, Jang D. Relationship between starting age of cranial-remolding-orthosis therapy and effectiveness of treatment in children with deformational plagiocephaly. Childs Nerv Syst. (2017) 33:1349–56. doi: 10.1007/s00381-017-3427-9
15. Kelly KM, Littlefield TR, Pomatto JK, Ripley CE, Beals SP, Joganic EF. Importance of early recognition and treatment of deformational plagiocephaly with orthotic cranioplasty. Cleft Palate Craniofac J. (1999) 36(2):127–30. doi: 10.1597/1545-1569_1999_036_0127_ioerat_2.3.co_2
16. Kluba S, Kraut W, Reinert S, Krimmel M. What is the optimal time to start helmet therapy in positional plagiocephaly? Plast Reconstr Surg. (2011) 128(2):492–8. doi: 10.1097/PRS.0b013e31821b62d6
17. Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. (2004) 114(4):970–80. doi: 10.1542/peds.2003-0668-F
18. Delye H, Borstlap W, Van Lindert EJ. Endoscopy-assisted craniosynostosis surgery followed by helmet therapy. Surg Neurol Int. (2018) 9:59. doi: 10.4103/sni.sni_17_18
19. Skolnick GB, Yu JL, Patel KB, David LR, Couture DE, Smyth MD, et al. Comparison of 2 sagittal craniosynostosis repair techniques: spring-assisted surgery versus endoscope-assisted craniectomy with helmet molding therapy. Cleft Palate Craniofac J. (2021) 58(6):678–86. doi: 10.1177/1055665620966521
20. Ravi S, Aziz W, AlOlama M, Stenger C, AlSaadawi G, Baldrighi C, et al. Integrated endoscopic craniosynostosis surgery and cranial orthosis program. J Craniofac Surg. (2024) 35(2):564–7. doi: 10.1097/SCS.0000000000009916
21. Berry-Candelario J, Ridgway EB, Grondin RT, Rogers GF, Proctor MR. Endoscope-assisted strip craniectomy and postoperative helmet therapy for treatment of craniosynostosis. Neurosurg Focus. (2011) 31(2):E5. doi: 10.3171/2011.6.FOCUS1198
22. Zapatero ZD, Slawinski SK, Kosyk MS, Kalmar CL, Cheung L, Carlson AR, et al. Utility of preoperative helmet molding therapy in patients with isolated sagittal craniosynostosis. J Craniofac Surg. (2022) 33(2):480–4. doi: 10.1097/SCS.0000000000008251
23. Taheri Z, Babaee T, Moradi E, Hajiaghaei B, Mohammadi HR. Minimally invasive craniectomy and postoperative cranial remolding orthotic treatment in infants with craniosynostosis: a multicenter prospective study. World Neurosurg X. (2023) 19:100207. doi: 10.1016/j.wnsx.2023.100207
24. Sakar M, Haidar H, Sönmez Ö, Erdoğan O, Saçak B, Bayri Y, et al. A new method for quantification of frontal retrusion and complex skull shape in metopic craniosynostosis: a pilot study of a new outcome measure for endoscopic strip craniectomy. J Neurosurg Pediatr. (2022) 29(6):650–8. doi: 10.3171/2022.1.PEDS21553
25. Zubovic E, Skolnick GB, Naidoo SD, Bellanger M, Smyth MD, Patel KB. Endoscopic treatment of combined metopic-sagittal craniosynostosis. J Neurosurg Pediatr. (2020) 26(2):113–21. doi: 10.3171/2020.2.PEDS2029
27. Aimar A, Palermo A, Innocenti B. The role of 3D printing in medical applications: a state of the art. J Healthc Eng. (2019) 2019:5340616. doi: 10.1155/2019/5340616
28. Wang H, Cui D, Jin J, Wang X, Li Y, Liu Z, et al. 3D-printed helmet-type neuro-navigation approach (I-helmet) for transcranial magnetic stimulation. Front Neurosci. (2023) 17:1224800. doi: 10.3389/fnins.2023.1224800
29. Lucano LRG, de la Peña Brambila FJ, Pérez JE, Rosales P. Customized low-cost 3D printed helmet as a temporary measure for a patient with acrania. Indian J Plast Surg. (2019) 52(02):252–3. doi: 10.1055/s-0039-1696077
30. TECHMED3D. Reshaping baby heads: how 3D printed cranial helmets are transforming plagiocephaly treatment: TECHMED3D; (2023). Available online at: https://techmed3d.com/blog/reshaping-baby-heads-how-3d-printed-cranial-helmets-are-transforming-plagiocephaly-treatment/ (Cited 2024).
31. Commission E. SmartOrthosis: Self-adjusting helmet corrects cranial deformities in children (2021). (Cited March 20, 2024).
32. FDA Starband. U.S. FOOD & DRUG. (2021). Available online at: https://www.accessdata.fda.gov/cdrh_docs/pdf20/K203098.pdf (Cited 2024).
33. FDA Talee. U.S. FOOD & DRUG. (2022). Available online at: https://www.accessdata.fda.gov/cdrh_docs/pdf22/K220681.pdf (Cited 2024).
34. Paul GM, Rezaienia A, Wen P, Condoor S, Parkar N, King W, et al. Medical applications for 3D printing: recent developments. Mo Med. (2018) 115(1):75.30228688
35. Shock LA, Greer S, Sheahan LD, Muzaffar AR, Aldridge K. Consistency of cranial shape measures obtained from laser surface and computed tomography imaging. J Craniofac Surg. (2021) 32(8):2763–7. doi: 10.1097/SCS.0000000000007885
36. Abdel-Alim T, Tio P, Kurniawan M, Mathijssen I, Dirven C, Niessen W, et al. Reliability and agreement of automated head measurements from 3-dimensional photogrammetry in young children. J Craniofac Surg. (2023) 34(6):1629–34. doi: 10.1097/SCS.0000000000009448
37. Kropla F, Hoffmann M, Winkler D, Krause M, Scholz S, Grunert R. Development of an individual helmet orthosis for infants based on a 3D scan. 3D Print Med. (2023) 9(1):22. doi: 10.1186/s41205-023-00187-7
38. Panchal J, Amirsheybani H, Gurwitch R, Cook V, Francel P, Neas B, et al. Neurodevelopment in children with single-suture craniosynostosis and plagiocephaly without synostosis. Plast Reconstr Surg. (2001) 108(6):1492–8. doi: 10.1097/00006534-200111000-00007
39. Knight S. Positional plagiocephaly/brachycephaly is associated with later cognitive and academic outcomes. J Pediatr. (2019) 210:239–42. doi: 10.1016/j.jpeds.2019.04.042
Keywords: 3D printing, helmet, metopic, craniosynostosis, case report
Citation: Atallah H, Naeem R, Alshawabka A, Said AS, Alfatafta H, Derkács E, Varga D and Molics B (2025) Customized 3D printed helmet in the treatment of metopic craniosynostosis in a 7-month-old infant, a case report. Front. Pediatr. 13:1474412. doi: 10.3389/fped.2025.1474412
Received: 8 August 2024; Accepted: 28 February 2025;
Published: 14 March 2025.
Edited by:
Nihad A. Almasri, Qatar University, QatarReviewed by:
Flavio Giordano, University of Florence, ItalyCopyright: © 2025 Atallah, Naeem, Alshawabka, Said, Alfatafta, Derkács, Varga and Molics. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huthaifa Atallah, aC5hdGFsbGFoQGp1LmVkdS5qbw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.