
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 14 March 2025
Sec. Pediatric Cardiology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1452353
 Marjan Tariverdi1
Marjan Tariverdi1 Mohammadbagher Rahmati2Maryam Mohammadian1Shahrokh Rajaei3Mohammadreza Kargarfard Jahromy3Niloufar Rahimi4Saeed Hosseini Teshnizi5Mohammad Tamaddondar6*Shiva Badri7Hossein Abdollahi4,†
Mohammadbagher Rahmati2Maryam Mohammadian1Shahrokh Rajaei3Mohammadreza Kargarfard Jahromy3Niloufar Rahimi4Saeed Hosseini Teshnizi5Mohammad Tamaddondar6*Shiva Badri7Hossein Abdollahi4,†
Background: Children account for a small percentage of COVID-19 cases and tend to exhibit milder symptoms compared to adults. Cardiovascular involvement has been observed in pediatric COVID-19 cases. This study aimed to determine the frequency of cardiac disorders in children hospitalized with COVID-19.
Methods: This cross-sectional study was conducted on pediatric patients admitted to Bandar Abbas Children Hospital, Iran, from March to September 2020. Patients with negative RT-PCR results for SARS-CoV-2, non-COVID-19 pulmonary involvement or pre-existing cardiovascular conditions were excluded. COVID-19 diagnostic subgroups were determined based on national guidelines. Clinical evaluations included chest CT scans to assess pulmonary involvement and cardiac assessments such as clinical symptoms, electrocardiography and echocardiography. Cardiac abnormalities were defined as clinical heart failure, dysrhythmias or abnormal echocardiography. Multivariable logistic regression was applied to analyze the associations between cardiac abnormalities, age and lung involvement, with statistical significance set at P < 0.05.
Results: This cross-sectional study was conducted in 2020 on 475 children aged 1 month to 14 years. Among the participants, 48.4% had suspected, 30.5% had probable, and 21.1% had confirmed COVID-19. Cardiac abnormalities were identified in 35.2% of patients, including dysrhythmia (20.2%), heart failure (7.6%), and abnormal echocardiography findings (13.1%). The odds of cardiac abnormalities were 3.3 times higher in children with unilateral lung involvement and 5.9 times higher in those with bilateral lung involvement compared to those without lung involvement. Additionally, older age was associated with a 5.7% reduction in the odds of cardiac abnormalities.
Conclusions: Cardiac abnormalities in pediatric COVID-19 patients show a significant correlation with pulmonary involvement, highlighting their link to disease severity. Routine cardiac assessments may help identify complications and guide management, especially during sporadic cases and seasonal outbreaks.
Since its emergence as an outbreak of atypical pneumonia in Wuhan, China, in December 2019, coronavirus disease 2019 (COVID-19) has rapidly spread worldwide (1), prompting the World Health Organization (WHO) to declare it a pandemic in March 2020 (2). COVID-19 is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1). Substantial evidence indicates that children account for a smaller proportion of COVID-19 cases compared to adults (3). Most children present with mild symptoms; however, infants have been reported to be at a higher risk of critical illness compared to older children (4). One proposed explanation for the milder presentations in children is the presence of fewer functional angiotensin-converting enzyme 2 (ACE2) receptors, which SARS-CoV-2 uses for cellular entry. Nevertheless, this hypothesis remains inconclusive (5). Although hospital admission and mortality rates are lower in children with COVID-19, severe disease manifestations, including cardiovascular injury, can occur in a minority of cases (6, 7). The underlying mechanisms of cardiac involvement in COVID-19 include myocardial ischemia due to hypoxia, endothelial overactivation, microvascular thrombi from a hyperinflammatory response, and direct myocardial damage caused by SARS-CoV-2 entering cardiomyocytes via ACE2 receptors (8–10).
Myocarditis, pericardial effusion, coronary thrombosis, and other electrocardiographic and echocardiographic abnormalities have been reported as instances of cardiac involvement in COVID-19 (11). The most serious complication in children with COVID-19 is multisystem inflammatory syndrome (MIS-C), which involves cardiovascular manifestations in 80%–100% of affected children (12, 13). Consequently, most studies examining cardiovascular manifestations of COVID-19 in children focus on those with MIS-C. In this study, we aimed to describe and analyze cardiac involvement in a cohort of children hospitalized with suspicious, probable, or confirmed COVID-19, focusing on heart failure symptoms, cardiac dysrhythmias and abnormal echocardiography findings.
This cross-sectional study was performed on 475 consecutive children aged 1 month to 14 years with suspicious, probable, or confirmed COVID-19 disease admitted to Bandar Abbas Children Hospital, Bandar Abbas, Iran, from March 20, 2020, to September 21, 2020. Children with at least two negative reverse transcriptase-polymerase chain reaction (RT-PCR) results for SARS-CoV-2 virus, 24 h apart, any evidences of pulmonary involvements other than COVID-19 in chest radiography or CT scanning and those with any evidence of underlying cardiovascular disorders such as congenital heart diseases before exposing COVID-19 were all excluded from the study.
In this study, based on the Iranian National Guideline for the Diagnosis and Treatment of COVID-19 in Children, three diagnostic subgroups for pediatric COVID-19 cases were included in the study:
This group includes children with acute respiratory illness characterized by fever and at least one symptom of respiratory disease such as cough or shortness of breath combined with a history of travel to or residence in areas with reported community transmission of COVID-19 within 14 days prior to symptom onset. It also encompasses children presenting with acute respiratory illness who have had close contact with a confirmed or probable COVID-19 case during the 14 days before symptom onset. Additionally, children with severe acute respiratory illness defined as fever, at least one respiratory symptom and hospitalization are included when no alternative diagnosis thoroughly explains the clinical presentation.
This category includes children initially classified as suspicious COVID-19 cases who meet additional diagnostic criteria indicative of COVID-19. This includes children with inconclusive results from COVID-19 testing (e.g., indeterminate RT-PCR findings) or cases where testing could not be performed for any reason. It also encompasses children with pneumonia who exhibit an inadequate clinical response despite proper treatment and whose condition deteriorates rapidly, or who die unexpectedly. Additionally, cases with imaging findings strongly suggestive of COVID-19, based on radiological assessments, are included in this subgroup.
This group includes children with laboratory-confirmed COVID-19 infection, as evidenced by a positive SARS-CoV-2 RT-PCR test, regardless of clinical signs or symptoms (14).
The study received ethics approval from the Ethics Committee of Hormozgan University of Medical Sciences under the ethics code IR.HUMS.REC.1400.005 and complies with the statements of the Declaration of Helsinki. The study's retrospective design waived the requirement to obtain informed consent from the parents/guardians of the participants. Baseline characteristics of the children, including demographics (gender, age) and medical history, were extracted from patients’ hospital records. Data on clinical assessments and investigations were retrospectively analyzed as part of this study. During the early stages of the COVID-19 pandemic, clinical protocols for suspected pediatric COVID-19 cases mandated comprehensive evaluations, including chest CT scans and cardiac assessments. Accordingly, all children underwent initial evaluation by CT scan using a Philips V2.0 CT scanner (Philips Medical Systems, Netherlands) to assess the degree of pulmonary involvement.
Cardiac assessments were conducted as part of routine clinical practice and included evaluating clinical manifestations of cardiac dysfunction or failure (e.g., chest pain, trouble breathing, excessive sweating while feeding or exercising), electrocardiography (to detect cardiac dysrhythmias), and 2D echocardiography (to rule out or confirm structural or functional heart abnormalities) using the Vivid™ device (General Electric Company, United States). Cardiac abnormalities were defined as the presence of one or more of the following: clinical manifestations of heart failure, cardiac dysrhythmias or abnormal echocardiography findings.
Data analysis was performed using the (SPSS) software, version 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were described using mean ± standard deviation, while categorical variables were reported as frequencies and percentages. Multivariable logistic regression analysis was applied to examine the association between COVID-19 probability and cardiac abnormalities, considering baseline parameters such as age and lung involvement. Odds ratios (OR) and their corresponding 95% confidence intervals (CI) were calculated to interpret the strength and direction of associations. A significance level of P < 0.05 was used for all statistical tests (15).
Of the 475 pediatric patients evaluated in this study, with a mean age of 50.39 ± 47.71 months, 243 (51.2%) were male, and 232 (48.8%) were female. COVID-19 was suspicious in 230 (48.4%), probable in 145 (30.5%), and confirmed in 100 (21.1%) of these children. Overall, cardiac abnormalities were found in 167 (35.2%), including dysrhythmia in 96 (20.2%), heart failure in 36 (7.6%), abnormal echocardiography in 62 (13.1%), and elevated troponin in 101 (21.3%) patients (Table 1). In multivariable logistic regression analysis, confirmed COVID-19 was associated with a 69.3% reduction in the odds of cardiac abnormalities compared to suspected COVID-19 cases (OR = 0.31, 95% confidence interval: 0.12–1.01). Moreover, the odds of cardiac abnormalities were 3.3 and 5.9 times higher in children with unilateral and bilateral lung involvement than in those without lung involvement. Also, older age decreased the odds of cardiac abnormalities by 5.7% (OR = 0.94, 95% confidence interval: 0.89; 1.00) (Table 2). However, COVID-19 probability was not linked to dysrhythmia, heart failure, or abnormal echocardiography.

Table 1. Demographics and general findings of the study.
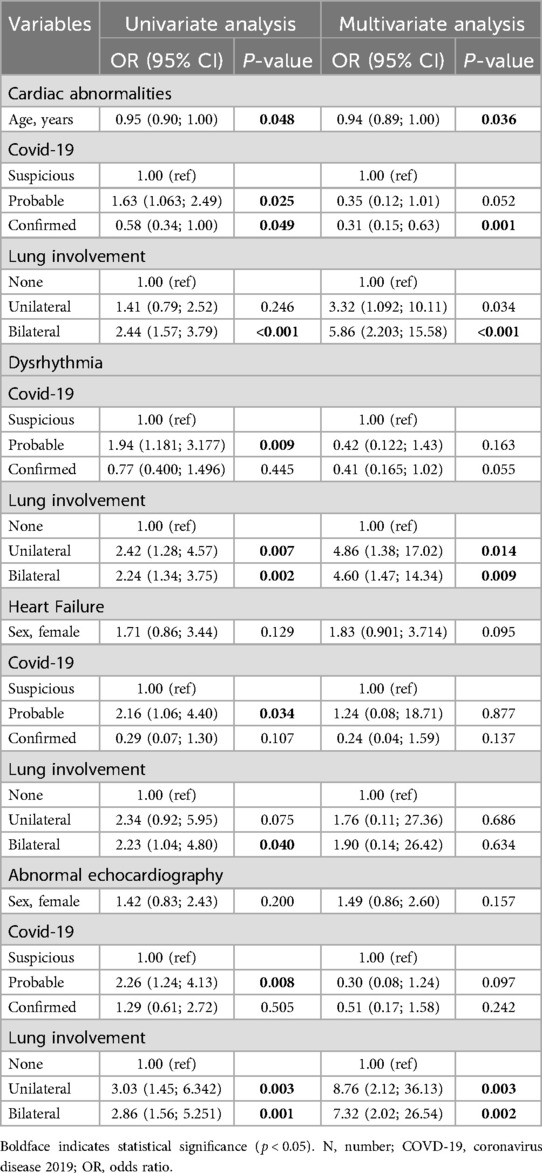
Table 2. Association of COVID-19 probability with cardiac abnormalities using logistic regression.
In the current study, cardiac abnormalities were found in approximately one-third of affected children, dysrhythmia in 20.2%. 13.1% of children suffered from abnormal echocardiography, 7.6% had evidences of acute heart failure. cardiac damages following COVID-19 infection in children may be manifested by a wide range of cardiac defects such as arrhythmias, myocarditis, heart failure even cardiomyopathy. In a multicenter study by Cantarutti et al. (16), cardiac involvement was reported in 29% of children with SARS-CoV-2 infection;. Another study that evaluated cardiac abnormalities associated with COVID-19 in children and young adults, using a multimodality approach, including cardiac computed tomography (CT), cardiac magnetic resonance imaging (CMR) and three-dimensional echocardiography, reported abnormal tissue Doppler indices and strain in almost all patients (17). Minocha et al. showed at least one cardiac abnormality in 73% of children with COVID-19 (18).
Regarding initial clinical manifestations of cardiac dysfunction in affected children include palpitations, dyspnea, chest pain, tightness, conjunctival effusion, polymorphic skin rash and hypotension that if cardiac dysfunction continues and worsens, it will lead to cardiogenic shock, reduced cardiac function capacity, and ultimately acute heart failure (18–20). Also, according to the literature, acute myocardial injury in children suffering COVID-19 is frequently accompanied with raised serum levels of troponin I/T, creatine kinase MB and/or lactate dehydrogenase that increasing the level of troponin I. In the current study, 20.2% of patients were found to have dysrhythmia. A systematic review (9) reported an overall rate of electrocardiogram anomalies at 5.3%, suggesting a higher prevalence of such abnormalities in our study population. Literature indicates that electrocardiographic changes associated with childhood COVID-19 commonly include sinus tachycardia, T-wave inversions, ST-segment abnormalities, right-axis deviation, QT interval prolongation, as well as various arrhythmias and conduction disturbances. Among adolescents, tachycardia is the most frequently observed abnormality, followed by bradycardia (19–21). In the current study, echocardiography-based abnormalities were observed in 13.1% of patients, which falls within the wide range of 9% to 75% reported in the literature for children with COVID-19 (14). This variation in prevalence across studies may reflect differences in study populations, disease severity, diagnostic protocols, or the availability and use of advanced imaging techniques.
Another notable finding of the current study was the significant association between cardiac abnormalities and bilateral lung involvement. To the best of our knowledge, this specific correlation has not been previously investigated in pediatric studies. However, existing evidence indicates that cardiac involvement in COVID-19 is strongly linked to disease severity (22, 23), and pulmonary involvement is known to be more extensive in patients with severe or critical disease compared to those with mild to moderate presentations (24). Additionally, Eslami et al. demonstrated that CT-measured cardiac indices can serve as valuable tools for risk stratification in hospitalized COVID-19 patients, providing insights into the relationship between lung involvement, cardiac dysfunction (25).
We observed that older age in children was associated with reduced odds of cardiac abnormalities, while no significant correlation was found between cardiac abnormalities and sex. Interestingly, a recent study by Brizuela et al. (26) reported a higher mortality rate among male children and increased hospitalization rates in this group. However, it remains unclear whether these outcomes were partially attributable to cardiac involvement. Additionally, infants have been consistently identified as being at higher risk for critical illness compared to older children (4), and this heightened vulnerability may include a greater likelihood of cardiac complications. These findings highlight the need for further research to clarify the relationships between age, sex and cardiac involvement in children with COVID-19, as well as to better understand the underlying mechanisms contributing to these differences.
One limitation of the current study was that only children aged ≤14 years were included, which restricts the generalizability of our findings to the broader pediatric population, typically defined as patients under 18 years of age. This age restriction was due to insurance coverage policies in Iran, which only apply to children ≤14 years. Another limitation was the retrospective nature of the study, which precluded determining the exact timing of cardiac evaluations and whether cardiac abnormalities were directly caused by COVID-19 or influenced by medications used during treatment. Additionally, SARS-CoV-2 RT-PCR was not performed in all patients, leading to a potential underestimation of cardiac abnormalities associated with confirmed COVID-19 cases. Lastly, while echocardiography served as an important diagnostic tool in our study, it has lower sensitivity for detecting cardiac lesions compared to cardiac MRI, potentially resulting in an underestimation of the prevalence and severity of cardiac involvement in the study population (13). The absence of cardiac MRI in our study may have led to an underestimation of the prevalence and extent of cardiac abnormalities in our population.
Based on the results of the current study, Cardiac abnormalities were observed in pediatric patients with COVID-19, indicating notable cardiovascular involvement in this population. These abnormalities demonstrated a significant correlation with the extent of pulmonary involvement, underscoring their potential association with disease severity. Although the COVID-19 pandemic has ended, sporadic cases and seasonal outbreaks continue to occur. Understanding such complications remains crucial for effective management in these instances and for informing future experiences. Therefore, routine cardiac assessments in pediatric COVID-19 cases could be helpful in identifying potential complications and guiding management strategies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee of Hormozgan University of Medical Sciences the ethics code: IR.HUMS.REC.1400.005. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MT: Conceptualization, Validation, Writing – original draft, Writing – review & editing. MR: Conceptualization, Validation, Writing – review & editing. MM: Writing – review & editing. SR: Supervision, Writing – review & editing. MK: Supervision, Writing – review & editing. NR: Project administration, Writing – review & editing. SH: Formal analysis, Writing – review & editing. MT: Writing – review & editing. SB: Formal analysis, Writing – review & editing. HA: Formal analysis, Investigation, Methodology, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
We are sincerely thankful to our counselors in the Clinical Research Development Center of Children's Hospital, Bandar Abbas, Iran.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382(8):692–4. doi: 10.1056/NEJMoa2001017
2. World Health O. Organization. Coronavirus disease 2019 (COVID-19): situation report 113. World Health Organization (2020). p. 1–17. Available online at: https://reliefweb.int/report/world/coronavirus-disease-covid-19-situation-report-113-12-may-2020
3. Badal S, Bajgain KT, Badal S, Thapa R, Bajgain BB, Santana MJ. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: a systematic review and meta-analysis. J Clin Virol. (2021) 135:104715. doi: 10.1016/j.jcv.2020.104715
4. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiology of COVID-19 among children in China. Pediatrics. (2020) 145(6):e20200702. doi: 10.1542/peds.2020-0702
5. Tan W, Aboulhosn J. The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on congenital heart disease. Int J Cardiol. (2020) 309:70–7. doi: 10.1016/j.ijcard.2020.03.063
6. Abi Nassif T, Fakhri G, Younis NK, Zareef R, Al Amin F, Bitar F, et al. Cardiac manifestations in COVID-19 patients: a focus on the pediatric population. Canad J Infect Dis Med Microbiol. (2021) 2021(1):1–12. doi: 10.1155/2021/5518979
7. Loke Y-H, Berul CI, Harahsheh AS. Multisystem inflammatory syndrome in children: is there a linkage to kawasaki disease? Trends Cardiovasc Med. (2020) 30(7):389–96. doi: 10.1016/j.tcm.2020.07.004
8. Böhm M, Frey N, Giannitsis E, Sliwa K, Zeiher AM. Coronavirus disease 2019 (COVID-19) and its implications for cardiovascular care: expert document from the German cardiac society and the world heart federation. Clin Res Cardiol. (2020) 109:1446–59. doi: 10.1007/s00392-020-01656-3
9. Giustino G, Pinney SP, Lala A, Reddy VY, Johnston-Cox HA, Mechanick JI, et al. Coronavirus and cardiovascular disease, myocardial injury, and arrhythmia: JACC focus seminar. J Am Coll Cardiol. (2020) 76(17):2011–23. doi: 10.1016/j.jacc.2020.08.059
10. Zareef RO, Younis NK, Bitar F, Eid AH, Arabi M. COVID-19 in pediatric patients: a focus on CHD patients. Front Cardiovasc Med. (2020) 7:612460. doi: 10.3389/fcvm.2020.612460
11. Capucho A, Resende PLS, Mascarenhas DA, Silva C, Sawamura KSS, Menezes C, et al. Cardiac manifestations in pediatric COVID-19. Clinics (Sao Paulo). (2021) 76:e3001. doi: 10.6061/clinics/2021/e3001
12. Pereira MFB, Litvinov N, Farhat SCL, Eisencraft AP, Gibelli MABC, Carvalho W, et al. Severe clinical spectrum with high mortality in pediatric patients with COVID-19 and multisystem inflammatory syndrome. Clinics. (2020) 75:e2209. doi: 10.6061/clinics/2020/e2209
13. Safadi MAP, Silva C. The challenging and unpredictable Spectrum of COVID-19 in children and adolescents. Rev Paul Pediatr. (2020) 39:e2020192. doi: 10.1590/1984-0462/2020/38/2020192
14. Soltani J, Sedighi I, Shalchi Z, Sami G, Moradveisi B, Nahidi S. Pediatric coronavirus disease 2019 (COVID-19): an insight from west of Iran. North Clin Istanb. (2020) 7(3):284–91. doi: 10.14744/nci.2020.90277
15. Olivier J, May WL, Bell ML. Relative effect sizes for measures of risk. Commun Stat Theory Methods. (2017) 46(14):6774–81. doi: 10.1080/03610926.2015.1134575
16. Cantarutti N, Battista V, Adorisio R, Cicenia M, Campanello C, Listo E, et al. Cardiac manifestations in children with SARS-COV-2 infection: 1-year pediatric multicenter experience. Children. (2021) 8(8):717. doi: 10.3390/children8080717
17. Theocharis P, Wong J, Pushparajah K, Mathur SK, Simpson JM, Pascall E, et al. Multimodality cardiac evaluation in children and young adults with multisystem inflammation associated with COVID-19. Eur Heart J Cardiovasc Imaging. (2021) 22(8):896–903. doi: 10.1093/ehjci/jeaa212
18. Minocha PK, Phoon CKL, Verma S, Singh RK. Cardiac findings in pediatric patients with multisystem inflammatory syndrome in children associated with COVID-19. Clin Pediatr (Phila). (2021) 60(2):119–26. doi: 10.1177/0009922820961771
19. Ciccarelli GP, Bruzzese E, Asile G, Vasallo E, Pierri L, De Lucia V, et al. Bradycardia associated with multisystem inflammatory syndrome in children with COVID-19: a case series. Eur Heart J Case Rep. (2021) 5(12):1–9. doi: 10.1093/ehjcr/ytab405
20. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American College of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 2. Arthritis Rheumatol. (2021) 73(4):e13–29. doi: 10.1002/art.41616
21. Liu PP, Blet A, Smyth D, Li H. The science underlying COVID-19: implications for the cardiovascular system. Circulation. (2020) 142:68–78. doi: 10.1161/CIRCULATIONAHA.120.047549
22. Li C, Jiang J, Wang F, Zhou N, Veronese G, Moslehi JJ, et al. Longitudinal correlation of biomarkers of cardiac injury, inflammation, and coagulation to outcome in hospitalized COVID-19 patients. J Mol Cell Cardiol. (2020) 147:74–87. doi: 10.1016/j.yjmcc.2020.08.008
23. Chen C, Yan JT, Zhou N, Zhao JP, Wang DW. Analysis of myocardial injury in patients with COVID-19 and association between concomitant cardiovascular diseases and severity of COVID-19. Zhonghua Xin Xue Guan Bing Za Zhi. (2020) 48(7):567–71. doi: 10.3760/cma.j.cn112148-20200225-00123
24. Li K, Wu J, Wu F, Guo D, Chen L, Fang Z, et al. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Invest Radiol. (2020) 55(6):327–31. doi: 10.1097/RLI.0000000000000672
25. Eslami V, Abrishami A, Zarei E, Khalili N, Baharvand Z, Sanei-Taheri M. The association of CT-measured cardiac indices with lung involvement and clinical outcome in patients with COVID-19. Acad Radiol. (2021) 28(1):8–17. doi: 10.1016/j.acra.2020.09.012
Keywords: children, COVID-19, heart, echocardiography, cardiac disorder
Citation: Tariverdi M, Rahmati M, Mohammadian M, Rajaei S, Kargarfard Jahromy M, Rahimi N, Hosseini Teshnizi S, Tamaddondar M, Badri S and Abdollahi H (2025) Cardiac complications associated with COVID-19: a single-center study from Southern Iran. Front. Pediatr. 13:1452353. doi: 10.3389/fped.2025.1452353
Received: 20 June 2024; Accepted: 25 February 2025;
Published: 14 March 2025.
Edited by:
Antoine AbdelMassih, Cairo University, EgyptReviewed by:
Alberto García-Salido, Niño Jesús University Children’s Hospital, SpainCopyright: © 2025 Tariverdi, Rahmati, Mohammadian, Rajaei, Kargarfard Jahromy, Rahimi, Hosseini Teshnizi, Tamaddondar, Badri and Abdollahi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Tamaddondar, dGFtYWRkb25kYXI0OTFAZ21haWwuY29t
†ORCID:
Hossein Abdollahi
orcid.org/0000-0002-6308-7137
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.