 Sarah AlHarbi
Sarah AlHarbi Areej Taha
Areej Taha Ahmed Ashi
Ahmed Ashi Naglla Elimam1,2
Naglla Elimam1,2 Sami Althubaiti
Sami Althubaiti- 1Department of Pediatric Oncology, King Abdullah Specialized Children’s Hospital, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Jeddah, Saudi Arabia
- 2King Abdullah International Medical Research Center, King Abdul Aziz Medical City, Jeddah, Saudi Arabia
- 3King Saud Bin Abdulaziz University for Health Sciences, Makkah—Jeddah Hwy, King Abdul Aziz Medical City, Jeddah, Saudi Arabia
Background: Children with acute lymphoblastic leukemia (ALL) have excellent outcomes, with >85% survival without relapse following contemporary therapies. Clinical and complete blood count (CBC) assessments are commonly used surveillance methods to detect relapses. We aimed to evaluate the efficacy of routine blood testing for detecting relapse using a systematic method of assessing normal and abnormal results.
Methods: This a retrospective, single center study included children aged 1–14 years diagnosed with ALL who completed therapy and were in complete remission. Demographic data, leukemia subtypes, risk stratification, treatment responses, and outcomes were also reviewed. CBC tests were evaluated, and abnormal results were categorized. The relapse groups were classified as asymptomatic and symptomatic relapses. The clinical outcomes of relapse and complications were analyzed. The sensitivity, specificity, positive predictive value, and negative predictive value of surveillance laboratory tests for predicting relapse after the end of treatment were evaluated.
Results: In total, 187 patients underwent 2074 CBC tests. Ten patients underwent full surveillance, whereas the remaining patients underwent partial surveillance. The median number of surveillance blood draws per patient was 12. Relapse was observed in nine patients. Only three patients had asymptomatic relapses. Neutropenia, leukopenia, pancytopenia, thrombocytopenia, and anemia were observed in 98, 89, 10, 6, and 3 patients respectively. The sensitivity and specificity of neutropenia, leukopenia, thrombocytopenia, anemia, and pancytopenia were 11.11% and 47.9%, 0% and 50%, 33.3% and 98.31%, 0% and 99.4%, and 33.3% and 96.07%, respectively. No differences were observed between patients who had asymptomatic relapses and those whose clinical outcomes or consequences had symptomatic relapses.
Conclusion: Relapse after completion of therapy in ALL is rare. Regular blood count surveillance does not predict clinical outcomes or relapse. Prospective studies are required to assess appropriate risk-based surveillance and its effects on patient outcomes and quality of life.
Introduction
Acute lymphoblastic leukemia (ALL) is the most prevalent childhood cancer, occurring in approximately 25% of all children aged 0–14 years (1). When treated based on risk adaptation using multi-agent chemotherapy protocols, children show remarkable improvements in survival rates, with an overall survival (OS) rate >90% (2).
Relapse is the leading cause of ALL treatment failure, particularly in patients with B-cell ALL. The relapse rate in patients with ALL ranges from 15%–20%, and the OS rate after relapse ranges from 40 to 70%. All relapses can be classified according to the site as isolated bone marrow relapse, extramedullary relapse, or combined bone marrow with extramedullary relapse, whereas timing can range between early (occurring within 18 months of diagnosis) and late (after 36 months) (3). The addition of blinatumomab, a bispecific antibody targeting CD3 and CD19, in patients with high-risk relapsed B-ALL led to better outcome (4, 5).
Only 5%–17% of ALL relapses are asymptomatic, with no difference in survival rates between relapses detected using abnormal cell counts and symptomatic relapses (6, 7).
Data on the sensitivity and specificity of routine blood count surveillance for detecting relapse and its effects on disease outcomes and complications are scarce. We aimed to evaluate the efficacy of routine blood testing using a systematic method of assessing normal and abnormal results.
Methods
We conducted a retrospective cohort study between 2014 and 2021 in patients diagnosed with ALL aged 1–14 years treated at our institution. For B-cell ALL, our center risk stratifies, treats, and assesses responses according to the Children's Oncology Group (COG) AALL0932 and AALL1131 for standard risk (SR) and high risk (HR), respectively (8, 9). For T-cell ALL, we treat patients according to AALL0434 (10) with modifications (11). Risk and relapse patients were stratified according to COG AALL1331 (4), and patients were identified from the hospital database. All patients with leukemia who had been treated and completed therapy in complete response and were followed up at our institution were included. Patients with Down syndrome or inherited cytopenia were excluded from this study. Data abstracted from electronic health records included patient demographics; leukemia subtype; risk stratification; response and outcome; follow-up laboratory testing results, including white blood cell count, hemoglobin level, platelet count, and absolute neutrophil count; relapse site and time; and post-relapse complications. Follow-up data were collected after primary treatment completion, with the last date of chemotherapy used as the date of completion.
The patients were followed up according to the institutional guidelines, which included clinic visits and laboratory tests every 1 month for the first 6 months, every 2 months for the second 6 months of the first year and every 3–4 months for the second and third years, every 6 months thereafter for the fourth year, and annually thereafter. This study was approved by the institutional review board (No: NRJ21J-205-08).
The patients were classified into full laboratory surveillance (100% adherence to surveillance protocol), partial surveillance (<100% adherence), and no surveillance groups. The relapse groups were classified as asymptomatic (relapse diagnosed using routine blood tests) and symptomatic (diagnosed clinically). The clinical outcomes related to relapse or complications were analyzed for each category.
For each surveillance laboratory component, we assessed whether the test results were normal or abnormal based on the Common Terminology Criteria for Adverse Events version 5.5.
The patients were considered to have abnormal results if their test abnormalities were grade 2 or higher.
Statistical analyses
Baseline patient characteristics are expressed as absolute frequency (%) and interquartile range (IQR) values. Categorical data were compared using Fisher's exact tests, and continuous data are presented as medians and IQRs and compared using the Mann–Whitney U test. The value of blood count in detecting relapse was assessed using sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV). Number needed to screen (NNS) is defined as the number of patients that need to be screened for the duration to detect relapse event. Statistical tests were performed using GraphPad Prism version 9.0.0.
Results
Between January 2014 and December 2021, 187 patients with ALL met the eligibility criteria for this study. The median age of the patients was 12 (range, 10–16) years, and 161 (86.10%) had B-cell ALL. In total, 113 (60.4%) patients had National Cancer Institute Standard-risk (SR). Ninety-three (49.4%) patients were assigned to the SR treatment group, whereas 74 (39%) patients were assigned to the High-risk (HR) group. Most patients [130 (69.5%)] had favorable cytogenetics, and 158 (84.4%) patients attained negative minimal residual disease by the end of induction. No cases of treatment-related leukemia were identified in our cohort (Table 1).
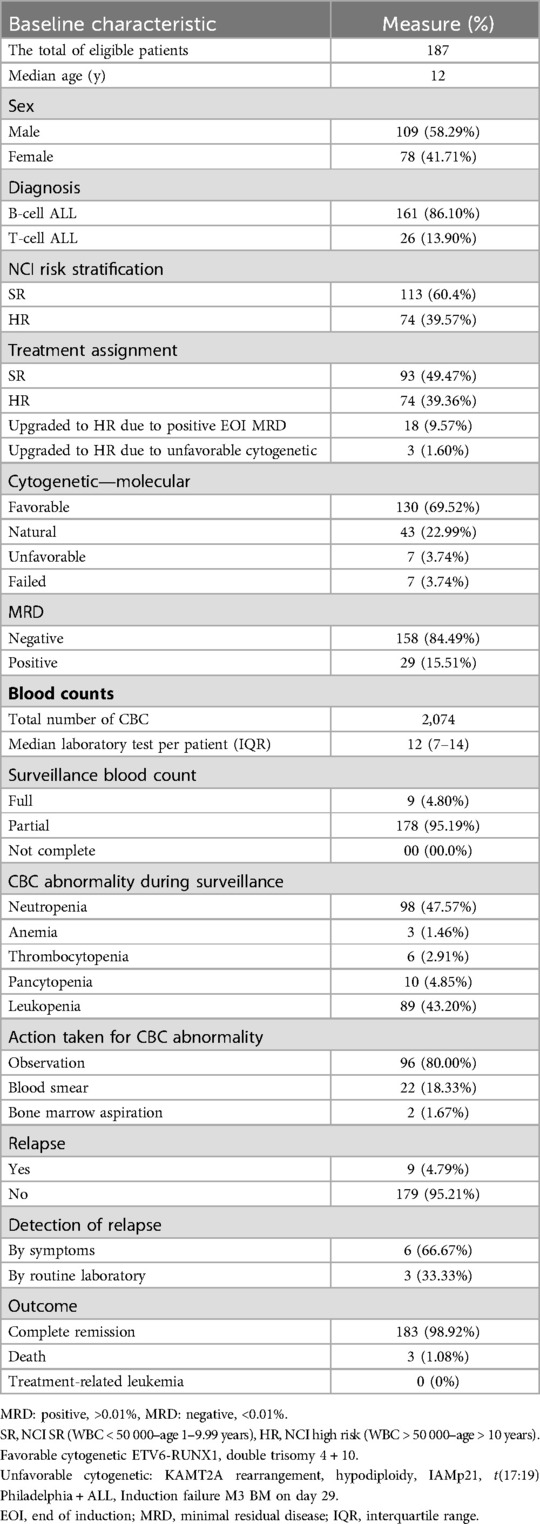
Table 1. Patient and disease characteristics.
Disease surveillance
The total complete blood count (CBC) tests performed for the whole cohort were 2074; the median laboratory test per patient was 12 (IQR, 7–14). Laboratory abnormalities were detected in 201 tests; the most common abnormalities detected were neutropenia 98 (47.57%) and leukopenia 89 (43.2%). Most patients [96 (80%)] were observed; 22 (18.3) and 2 (1.6%) patients underwent blood smear and bone marrow assessment, respectively.
Most patients [178 (95.1%)] underwent partial surveillance; nine (4.79%) patients relapsed at a median follow-up period of 18 months. Of the total 187 patients, only three relapses were identified through routine blood tests (Table 1). The calculated number needed to screen (NNS) to detect a relapse was 63.
The most frequent abnormal laboratory results were thrombocytopenia [n = 3 (33%)] and pancytopenia [n = 3 (33%)]. The median blast percentage at relapse was 70% (IQR, 52%-76%) (Table 2). Comparing the blast percentage between the two groups at initial presentation of relapse, the symptomatic and asymptomatic blast percentages were 57% (IQR, 32%-72%) and 76.5% (IQR, 70%-83%) (p = 0.0397), respectively.
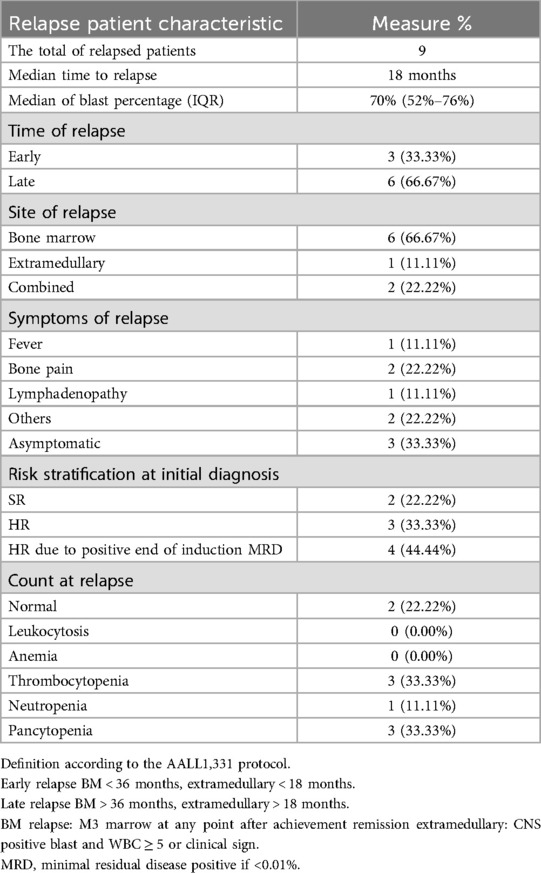
Table 2. Relapse characteristics.
The sensitivity and specificity of neutropenia, leukopenia, thrombocytopenia, anemia, and pancytopenia were 11.11% and 47.9%, 0% and 50%, 33.3% and 98.31%, 0% and 99.4%, and 33.3% and 96.07%, respectively. PPV and NPV were assessed for each abnormal blood count and are summarized in Table 3.
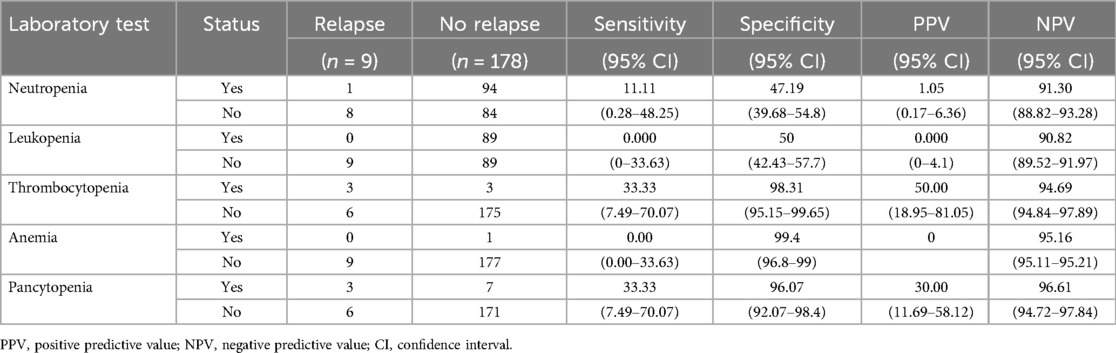
Table 3. Measurement of screening accuracy.
Relapse characteristics and outcomes
Out of the nine patients with relapse, 66.6% (n = 6) had late relapse. Bone marrow relapse was the most common relapse (66.6%), and most relapse occurred in the high-risk group [n = 7 (77.7%)]. No predominant symptoms were associated with symptomatic relapse.
Treatment-related complications, including infection, tumor lysis syndrome, and medication toxicity, were comparable between the two groups (Table 4).
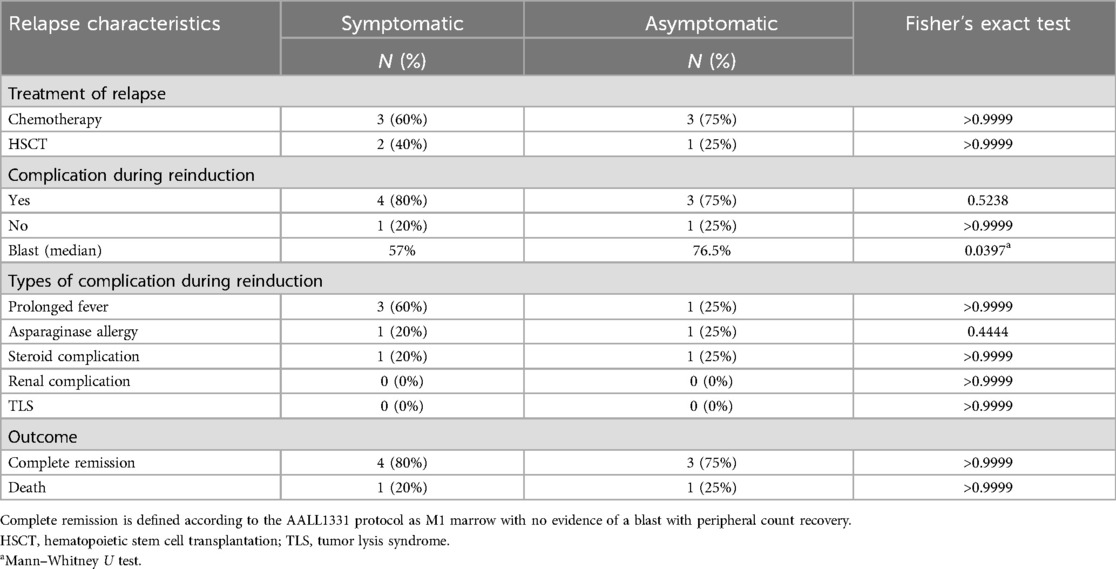
Table 4. Relapse treatment and outcomes.
Seven patients achieved remission after reinduction therapy, and three patients underwent hematopoietic stem cell transplantation. Seven patients were alive at the median follow-up period of 30 (IQR, 12–36) months (Table 4).
Discussion
Treatment outcomes of children with ALL have improved over the last few years (2). An ideal surveillance protocol should encompass modalities capable of detecting most cancer types commonly found in at-risk individuals. Additionally, the selected modalities should demonstrate effectiveness in the early detection of asymptomatic tumors that can be successfully managed with minimal treatment-related morbidities. Moreover, surveillance protocols must be assessed to demonstrate that early detection of asymptomatic tumors ultimately leads to improved overall patient survival (12). Several attempts to identify relapsed acute lymphoblastic leukemia earlier through surveillance failed to show its effects on outcomes (6, 7, 13). The outcomes of patients with relapse largely rely on disease phenotype, timing of relapse, sites of relapse, and response to therapy (3). It is imperative to assess whether the surveillance tool used to identify relapse is sensitive and specific and can detect disease at low burden, enhance outcomes, and minimize complications. Our data showed that relapse was uncommon after therapy completion. Only nine of our patients relapsed after treatment completion. Our patient population underwent a large number of post-treatment tests, with an average of 12 tests per patient (range, 7–14), but only three patients showed evidence of suspected relapse based on blood count, no patient developed treatment-related leukemia, and in patients with non-relapse, or persistent cytopenia required intervention.
In our cohort, 39% of patients were classified as high risk indicating a significant proportion at risk of relapse.
Abnormal blood counts following therapy for acute lymphoblastic leukemia (ALL) were prevalent, with 57% of our patients' exhibiting abnormalities in one or more CBC tests. The sensitivity, specificity, and positive predictive value (PPV) of the blood tests were low. However, the negative predictive values, were high ranging from 90.0%–96.6% across different CBC parameters, underscores the reliability of CBC as low-risk method for ruling out relapses. Nevertheless, the high likelihood of benign abnormal results may substantially impact the quality of life (QoL) for patients and their families, contributing to increased anxiety and prompting additional testing. No differences were observed in treatment-related complications or responses. We observed a slightly higher blast percentage in asymptomatic relapse cases than in symptomatic relapse cases. This observation may indicate the presence of subtle symptoms and signs that were not readily apparent to either the family or treating physician. This study highlights the necessity for a balanced approach to surveillance that weighs the benefits of early detection against the psychological effects of frequent testing for both high-risk and standard-risk groups. Our study highlights the limitations of routine blood testing for detecting relapse in children with ALL and underscores the importance of developing more sensitive and specific diagnostic methods. The comparable clinical outcomes and treatment-related complications between symptomatic and asymptomatic relapse cases challenge the need for post-treatment surveillance. Furthermore, considering the limitations of routine blood testing in detecting relapse, an important question arises as to whether clinical judgment alone can replace laboratory assessment in relapse surveillance. Our study has some limitations, including the inherent limitations of retrospective studies, a small sample size, and the fact that the effects of such extensive surveillance on QoL was not evaluated. A prospective study evaluating the effectiveness of clinical assessment as a stand-alone approach versus a combined approach involving laboratory assessment and evaluate their effects on patients' QoL, with the aim of enhancing the post-treatment evaluation and management of children with ALL.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by King Abdullah International Medical Research Center, institutional review board (No: NRJ21J-205-08). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AT: Data curation, Writing – review & editing. AA: Data curation, Writing – review & editing. NE: Formal Analysis, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ALL, acute lymphoblastic leukemia; CBC, complete blood count; COG, Children's oncology group; HR, high risk; IQR, interquartile range; NPV, negative predictive value; PPV, positive predictive value; QoL, quality of life; SR, standard risk.
References
1. Kakaje A, Alhalabi MM, Ghareeb A, Karam B, Mansour B, Zahra B, et al. Rates and trends of childhood acute lymphoblastic leukaemia: an epidemiology study. Sci Rep. (2020) 10:6756. doi: 10.1038/s41598-020-63528-0
2. Hunger SP, Loh ML, Whitlock JA, Winick NJ, Carroll WL, Devidas M, et al. Children’s oncology group’s 2013 blueprint for research: acute lymphoblastic leukemia. Pediatr Blood Cancer. (2013) 60:957–63. doi: 10.1002/pbc.24420
3. Hunger SP, Raetz EA. How I treat relapsed acute lymphoblastic leukemia in the pediatric population. Blood. (2020) 136:1803–12. doi: 10.1182/blood.2019004043
4. Brown PA, Ji L, Xu X, Devidas M, Hogan LE, Borowitz MJ, et al. Effect of postreinduction therapy consolidation with blinatumomab vs chemotherapy on disease-free survival in children, adolescents, and young adults with first relapse of B-cell acute lymphoblastic leukemia: a randomized clinical trial. JAMA. (2021) 325:833–42. doi: 10.1001/jama.2021.0669
5. Locatelli F, Zugmaier G, Rizzari C, Morris J, Gruhn B, Klingebiel T, et al. Effect of blinatumomab vs chemotherapy on event-free survival among children with high-risk first-relapse B-cell acute lymphoblastic leukemia: a randomized clinical trial. JAMA. (2021) 325(9):843–54. doi: 10.1001/jama.2021.0987
6. Gandhi M, Rao K, Chua S, Saha V, Lilleyman J, Shankar A. Routine blood counts in children with acute lymphoblastic leukaemia after completion of therapy: are they necessary? British J Haematol. (2003) 122:451–3. doi: 10.1046/j.1365-2141.2003.04453.x
7. Rubnitz JE, Hijiya N, Zhou Y, Hancock ML, Rivera GK, Pui C-H. Lack of benefit of early detection of relapse after completion of therapy for acute lymphoblastic leukemia. Pediatr Blood Cancer. (2005) 44:138–41. doi: 10.1002/pbc.20166
8. Angiolillo AL, Schore RJ, Kairalla JA, Devidas M, Rabin KR, Zweidler-McKay P, et al. Excellent outcomes with reduced frequency of vincristine and dexamethasone pulses in standard-risk B-lymphoblastic leukemia: results from children’s oncology group AALL0932. J Clin Oncol. (2021) 39:1437–47. doi: 10.1200/JCO.20.00494
9. Salzer WL, Burke MJ, Devidas M, Chen S, Gore L, Larsen EC, et al. Toxicity associated with intensive postinduction therapy incorporating clofarabine in the very high-risk stratum of patients with newly diagnosed high-risk B-lymphoblastic leukemia: a report from the children’s oncology group study AALL1131. Cancer. (2018) 124:1150–9. doi: 10.1002/cncr.31099
10. Winter SS, Dunsmore KP, Devidas M, Wood BL, Esiashvili N, Chen Z, et al. Improved survival for children and young adults with T-lineage acute lymphoblastic leukemia: results from the children’s oncology group AALL0434 methotrexate randomization. J Clin Oncol. (2018) 36:2926–34. doi: 10.1200/JCO.2018.77.7250
11. Jastaniah W, Elimam N, Abdalla K, AlAzmi AA, Aseeri M, Felimban S. High-dose methotrexate vs. capizzi methotrexate for the treatment of childhood T-cell acute lymphoblastic leukemia. Leuk Res Rep. (2018) 10:44–51. doi: 10.1016/j.lrr.2018.10.001
12. Dobrow MJ, Hagens V, Chafe R, Sullivan T, Rabeneck L. Consolidated principles for screening based on a systematic review and consensus process. CMAJ. (2018) 190:E422–9. doi: 10.1503/cmaj.171154
Keywords: acute lymphoblastic leukemia, complete blood count, surveillance, relapse, children
Citation: AlHarbi S, Taha A, Ashi A, Elimam N and Althubaiti S (2025) Value of routine blood count surveillance in detecting relapse in acute lymphoblastic leukemia. Front. Pediatr. 12:1488686. doi: 10.3389/fped.2024.1488686
Received: 30 August 2024; Accepted: 2 December 2024;
Published: 6 January 2025.
Edited by:
Michael James Burke, Medical College of Wisconsin, United StatesReviewed by:
Anna Maria Testi, Sapienza University of Rome, ItalyJeffrey R. Andolina, University of Rochester Medical Center, United States
Copyright: © 2025 AlHarbi, Taha, Ashi, Elimam and Althubaiti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sami Althubaiti, ZHJfc2FtaV9hbHRodWJhaXRpQGhvdG1haWwuY29t