 Yung-Yi Lan
Yung-Yi Lan Rujith Kovinthapillai
Rujith Kovinthapillai Andrzej Kędzia
Andrzej Kędzia Elżbieta Niechciał
Elżbieta Niechciał- Department of Pediatric Diabetes, Clinical Auxology and Obesity, Poznan University of Medical Sciences, Poznan, Poland
Type 1 diabetes is rising in the pediatric population, affecting approximately 1.2 million children and adolescents globally. Its complex pathogenesis involves the interaction between genetic predisposition and environmental factors, leading to T cell-mediated destruction of insulin-producing pancreatic beta-cells. This destruction results in insulin insufficiency and hyperglycemia. Hence, managing type 1 diabetes requires a comprehensive approach that includes various aspects such as blood glucose monitoring, insulin therapy, carbohydrate counting, caloric intake monitoring, considering family habits and food preferences, planning daily schedules, and incorporating physical activity. Children with type 1 diabetes encounter age-specific challenges in disease management that may exacerbate the risk of metabolic complications and adverse health outcomes. These risk factors may be neurological, physiological, behavioral, psychological, or social, complicate management and necessitate tailored approaches for effective care. Regardless of the age group, primary caregivers have a high responsibility to maintain optimal glycemic control, including monitoring diet, daily activity, and administering insulin. By reviewing research on the challenges faced by pediatric patients with type 1 diabetes, we summarized key insights aimed at developing targeted interventions and support systems that enhance diabetes management and improve health outcomes in this vulnerable population.
Introduction
Type 1 diabetes (T1D), affecting 1.2 million children and adolescents younger than 20 years, is the predominant autoimmune endocrine disorder observed in the pediatric population, with a rising global occurrence that varies among different races, countries, and regions (1, 2). This condition results from an immune-mediated destruction of insulin-producing beta-cells in the pancreas, which leads to insulin insufficiency and hyperglycemia (3). Therefore, effectively managing T1D involves a multifaceted approach encompassing frequent glucose monitoring, insulin dosing, assessing carbohydrate and caloric intake, adjusting treatment according to family habits, food preferences, and daily schedule, and encouraging physical activity (4, 5).
A comprehensive approach to T1D care is essential for optimal glucose control and long-term survival (5, 6). Recent studies emphasize the long-term benefits of ensuring optimal blood glucose control during childhood and adolescence in preventing complications in adulthood (6). Effective T1D management in children relies heavily on self-management, which includes managing symptoms, treatment, and the physical and psychosocial impacts of the condition, as well as lifestyle adjustments (7). Thus, T1D treatment should be supported by structured diabetes education (4). T1D control in the pediatric population is influenced by factors such as growth and developmental stages, psychological attributes, co-existing diseases, family dynamics, and care outside of the home (8). Innovative technologies for managing T1D, ranging from blood glucose sensors, insulin pumps, and decision support tools, aid in maintaining target glucose levels (9). However, these technologies can be overwhelming for some patients, introducing obstacles such as increased treatment costs, visibility of devices, and intrusive alarms (10, 11). These factors raise the complexity of T1D care in the pediatric population, causing challenges in achieving good metabolic control (8, 10, 11). This review comprehensively examines the unique obstacles faced by individuals with T1D at different stages of development from early childhood to adolescence.
Data sources and searches
This narrative review did not involve a systematic literature search; each author identified and critically reviewed the most relevant papers. The work presents several studies on age-based challenges to T1D management in the pediatric population. The following electronic databases were searched for relevant full-text articles in the English language: PubMed, Google Scholar, Scopus, EMBASE, and Web of Science. The search time was from October 2023 up to May 2024 using the following keywords: type 1 diabetes; management; treatment; regimen; pediatric diabetes care, age-based challenges; infants; toddlers; preschoolers; early-elementary school-age children; school-aged children; adolescents; youth; children; transitional age; transition into adult diabetes care; developmental stages; limited cognitive capacities; communicational skills; autonomous behaviors; risky behaviors; glycemic control; self-management; awareness of hypoglycemia, signs of hyperglycemia; parental distress; parental burnout; type 1 diabetes burnout; adherence; non-adherence; compliance; drug use; alcohol use; family dynamics; financial; practical issues; social support; lifestyle; school; diabetes education; teachers. All articles published between July 2004 and May 2024 were checked by title, abstract, and full text. It aimed to detect the most clinically significant papers related to the topic and provide a theoretical point of view, which is considered a valuable educational tool in continuing medical education.
Infants and toddlers
Managing T1D in younger children, particularly infants and toddlers, is troublesome due to their limited expressive language skills, making it difficult for them to reliably detect and report early signs of hypoglycemia (6). Additionally, a frequent feeding pattern, typical for this age group, may pose difficulties in T1D management, causing fluctuation in glucose levels between hyperglycemia and hypoglycemia (12).
During infancy, cognitive capacities hinder the understanding of the intricate aspects of T1D management. Consequently, the responsibility for disease management squarely rests on the shoulders of caregivers, underscoring their primary obligation to actively engage in a comprehensive T1D management plan (12, 13). Essential developmental milestones in infancy include establishing a bond with primary caregivers. Disruption of this process may lead to an underdeveloped trusting relationship between the infant and the caregiver. This impaired relationship is likely to complicate adherence to recommended Diabetes Self-Management Education (DSME). The DSME advocates for caregivers to ensure warmth and comfort following invasive procedures, such as replacing insulin pumps, establishing feeding and sleep routines, and maintaining vigilance for hypoglycemia, which are pivotal aspects of pediatric care (12). The presence of a distrusting and uncooperative child further exacerbates these challenges and fails to promote a supportive environment for both the infant and the caregivers.
As children progress into the toddler phase, a significant shift toward autonomy occurs, reflecting a natural strive for independence and control (14). However, this newfound autonomy can create challenges during feeding, as many toddlers exhibit picky eating behaviors and resist consuming offered food (15). This autonomy may negatively impact T1D management by causing significant fluctuations in blood glucose levels. Picky eating in children with T1D can lead to blood glucose fluctuations due to inconsistent carbohydrate intake and the potential for skipping meals. Favoring high-glycemic foods can cause rapid spikes and drops in blood glucose levels. These dietary inconsistencies complicate accurate insulin dosing, further contributing to glycemic variability. As a result, effectively managing a picky eater involves implementing limit-setting strategies and addressing the challenges associated with a toddler's non-cooperation with established routines (12, 14).
Hence, caregivers are compelled to adapt their parenting practices and integrate various daily tasks to enhance the quality of life for infants and toddlers managing T1D. Consequently, approximately one in five parents experience psychological distress within the initial four years following their child's diabetes diagnosis (16). Furthermore, managing T1D introduces significant changes in familial dynamics, causing notable transformations in both the parent-child relationship and the dynamics between partners (17). These exceptional challenges in caring for young children with diabetes contribute to heightened parental concerns and an increased impact on overall family well-being (17).
Preschoolers and early-elementary school aged children
Treating T1D in the preschool phase and early elementary school-aged children involves exceptional complexities, requiring understanding a confluence of physiological, developmental, and psychosocial factors (18). These multifaceted concerns necessitate tailored interventions that address both the child's medical and emotional needs as well as parental distress and family burden.
Similarly, in early childhood, the ability to recognize and communicate symptoms of hypoglycemia may be limited (18). Moreover, parents may struggle to distinguish between behavioral signals of hypoglycemia or hyperglycemia and typical developmental behaviors, such as temper tantrums, lingering at mealtime, and refusing to eat presented food (15). Parenting dilemmas may arise concerning appropriate disciplinary measures for children with T1D, particularly in balancing an understanding of their condition while fostering accountability for their actions. Some parents justify a lenient approach by acknowledging the significant burdens already faced by children with T1D, believing these children already face considerable challenges (19).
Another issue in managing T1D is balancing physical activity with insulin dosing and food intake. Some data show that children diagnosed with T1D before the age of 7 often demonstrate markedly lower levels of physical activity compared to their healthy counterparts of the same age and gender (20). This decrease can be attributed to a variety of factors. Parents may refrain from encouraging physical activity for their young children due to concerns about hypoglycemia, or they may fail to adjust their child's diabetes management effectively in response to changes in physical activity levels (21, 22). The ramifications of diminished physical activity may result in heightened insulin resistance and an elevated susceptibility to complications associated with T1D, such as cardiovascular disease.
Parents often face challenging decisions regarding employment due to the demanding nature of caring for a child with T1D (19). Research by Harrington et al. (23) highlighted that 55% of parents require the need for flexible work arrangements, adversely affecting family dynamics. Specifically, 57% of parents express concerns about their child's well-being while away from home, especially as they spend more time in kindergarten. Another study showed that 44% of parents reported their child's T1D diagnosis influenced school enrollment decisions, and 12% had withdrawn their child from school or daycare due to difficulties managing the condition (24). Parents of younger children were particularly apprehensive about a school's ability to manage T1D effectively.
School-aged children
School-aged children with T1D face significant troubles when assuming new responsibilities for managing their condition. Despite their potential capabilities, many rely heavily on parental assistance for various diabetes-related tasks. This dependence may stem from a desire to take breaks from daily management duties, engage in leisure activities, or avoid potential errors (25). Additionally, children often struggle with complex tasks such as carbohydrate counting and insulin dosing, further reinforcing their reliance on adults for support. This lack of proficiency not only impacts their daily activities but also restricts their participation in social events like sleepovers or school trips. These barriers highlight the need for tailored support and education initiatives to empower school-aged children with T1D to manage their condition effectively (26). Furthermore, children may experience negative emotions, including anger, fear, and sadness, due to the impact of their condition on social life and independence, with strict dietary restrictions being a significant source of dissatisfaction (27). Hence, they are at a higher risk of depression compared to their healthy peers. Symptoms of depression may manifest as irritability, mood changes, sleep or appetite disturbances, loss of interest in activities, decreased school performance, poor diabetes management, and feelings of being overwhelmed. Unfortunately, parents may misinterpret these signs as laziness or indifference rather than recognizing them as signs of depression. Childhood depression not only diminishes the child's quality of life but also correlates with poorer T1D control and increased instances of diabetic ketoacidosis (28).
As highlighted in various studies, the lack of information and training about T1D among teachers and classmates is a significant issue (1). Nearly half of the interviewed teachers were tasked with instructing students with T1D, yet only a few have undergone targeted training. This knowledge gap impairs their ability to effectively manage the condition, including monitoring blood sugar levels, administering insulin, and responding to emergencies (29). The need for specialized healthcare professionals, such as school nurses, underscores the reliance on external support systems to meet the needs of students with T1D, which may result in delayed or inadequate care during emergencies (30).
Adolescents
Enhanced risk-taking behavior during adolescence, marked by increased experimentation with drugs and alcohol, accidental deaths, and unprotected sexual activity, has been extensively documented in studies (31, 32). For individuals with T1D, substance use is especially problematic in that it increases the likelihood of acute complications and hospitalization. Alcohol inhibits gluconeogenesis and glycogenolysis in the liver, leading to decreased blood glucose levels for several hours after consumption, which can be life-threatening when combined with insulin therapy (33). Additionally, alcohol intoxication impairs cognitive function, which may result in missed insulin doses, miscalculated dosages, or delayed blood glucose monitoring, further exacerbating the risk of hypoglycemia. Therefore, it is crucial for adolescents to be aware of these risks, regularly screened for alcohol intake, and provided with appropriate education (34, 35).
Drugs can worsen hypoglycemia unawareness because their symptoms often mimic those of hypoglycemia. As a result, both the person with T1D and those around them may mistake signs of hypoglycemia for symptoms of intoxication. A hypoglycemic event that is not recognized and treated quickly can result in loss of consciousness and/or seizure, necessitating more intensive care and increasing morbidity and mortality (36–38).
Adolescents with T1D are significantly more likely to develop eating disorders (ED), with research showing a 2.5-fold increased risk compared to their healthy peers (39). For every occurrence of ED in healthy teenagers, approximately two to three adolescents with T1D are similarly affected. Key factors contributing to this comorbidity include elevated body mass index (BMI), recurrent weight fluctuations due to frequent dieting, dissatisfaction with body image, depressive symptoms, and ineffective coping mechanisms (40, 41). Adolescents with T1D may turn to insulin restriction to achieve their desired body weight, driven by factors such as peer influence, normalization of unhealthy behaviors, and underlying mental health issues such as depression and anxiety. Addressing these multifaceted factors is crucial for interventions aimed at promoting healthy weight management and overall well-being in this population (42–46).
Disease perceptions, encompassing individuals’ beliefs and understanding of their condition, have been shown to influence the management of T1D in adolescents significantly. Negative perceptions may lead to reluctance to engage in essential self-care behaviors, causing fluctuations in glucose levels and increasing the risk of complications. Furthermore, such perceptions may deter individuals from seeking necessary healthcare support, exacerbating difficulties in management and increasing the likelihood of adverse health outcomes (47–49).
Peer support is crucial in managing T1D, as it offers adolescents a comforting outlet to share their experiences. Adolescents with T1D often grapple with a spectrum of negative emotions like anger, fear, and distress stemming from the perceived intrusion of the condition into their lives or from perceiving T1D as a barrier to “normal” life (27, 50). These feelings contribute to resistance in adhering to management routines, exacerbated by resentment towards the condition, especially regarding its impact on social life and independence. Concerns about peer perceptions may trigger social withdrawal and avoidance of activities, worsening emotional distress (51, 52).
Transition age
Transitioning from adolescence to adulthood presents numerous challenges in the management of T1D. Mistry et al. (53) reported that 32% of adolescents fail to attend a scheduled appointment within a year after their transition from pediatric to adult clinics, exemplifying the need for tailored support during this critical period. Some findings suggested that those diagnosed with T1D at a younger age may face difficulties in transitioning and managing T1D into adulthood, potentially due to less autonomy in T1D management as parental involvement declines (53). Ladd et al. (54), however, concluded that being diagnosed at a young age and having a longer T1D duration prepared adolescents for better adjustment and transitioning of self-management compared to those diagnosed late in adolescence. The lack of preparation for independent management, as well as insufficient engagement, is compounded by parental endorsement of attending all diabetes clinic visits, with the majority admitting to not having initiated discussions regarding transition plans with their adolescent (65%) or the diabetes care team (60%) (55). Some adolescents regard the transition process as daunting, expressing a desire for developmentally appropriate interactions and meaningful conversations about diabetes care. Social support and coordination between pediatric and adult care providers are crucial for ensuring a smooth transition and mitigating the risk of complications later in life. This highlights the importance of identifying high-risk patients and providing individualized support to facilitate successful transitions and long-term disease management. Table 1 summarizes the challenges encountered by individuals with T1D and their caregivers, along with proposed solutions regarding the management, while Figure 1 highlights the main age-based obstacles in T1D management in the pediatric population.
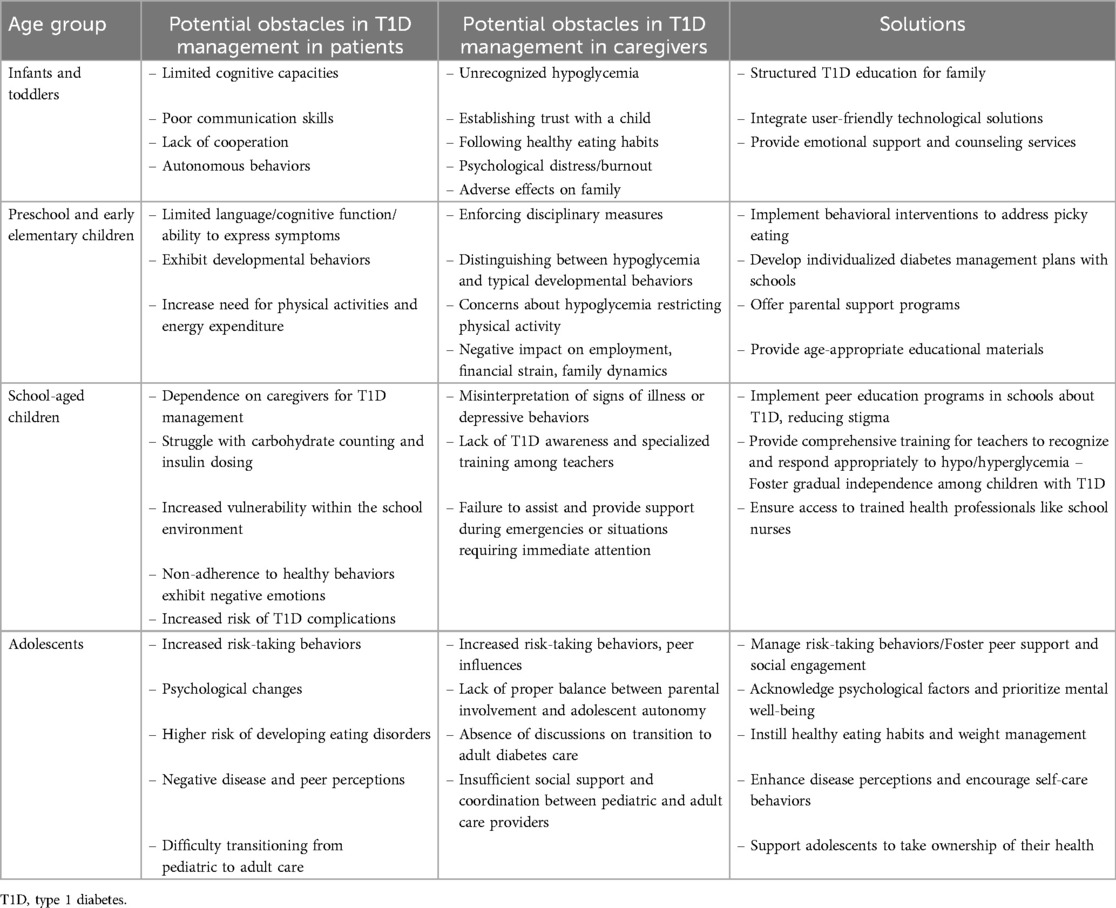
Table 1. Summary of challenges encountered by individuals with T1D and their caregivers with proposed solutions.
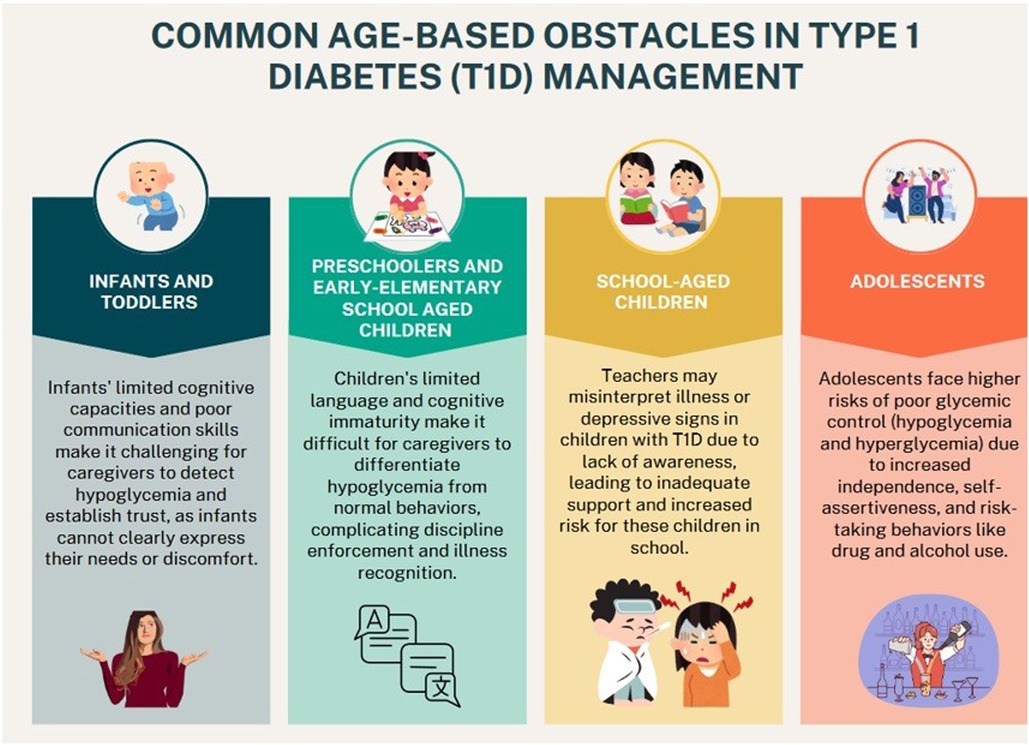
Figure 1. The main age-based obstacles in type 1 diabetes management in the pediatric population.
The strengths and limitations of the review
This narrative review offers a practical and detailed examination of age-based challenges in managing T1D among pediatric populations, enhancing the existing pediatric diabetes guidelines by addressing specific obstacles encountered at different developmental stages. The review integrates a broad spectrum of studies to highlight the complex interplay of physical, psychological, social, and environmental factors influencing T1D management from infancy through adolescence. It provides actionable strategies and tailored interventions that complement general recommendations in current guidelines, offering a nuanced perspective on addressing the unique needs of young patients and their caregivers.
However, as a narrative review rather than a systematic review, it has certain limitations. It may not cover all relevant issues or include every pertinent study, potentially leaving out some aspects of the complex management of T1D. The review's findings are based on selected literature and expert opinion, which may not fully represent the breadth of evidence available in comprehensive guidelines. Consequently, while the review provides valuable insights and practical solutions, it should be considered alongside more exhaustive systematic reviews and clinical practice standards for a complete understanding of pediatric T1D management.
Conclusions
In conclusion, managing T1D in pediatric populations requires a comprehensive approach tailored to the unique challenges encountered at different developmental stages. From infancy through adolescence, individuals with T1D and their caregivers face diverse obstacles related to physical, psychological, social, and environmental factors. Integrating user-friendly technological solutions, providing caregiver education and support, addressing picky eating behaviors, collaborating with schools, offering peer support programs, and facilitating the transition to adult care are crucial strategies. By implementing these interventions, healthcare providers and support systems can empower pediatric patients with T1D to thrive despite their condition, leading to improved long-term outcomes and quality of life.
Author contributions
Y-YL: Data curation, Investigation, Writing – original draft. RK: Data curation, Investigation, Writing – original draft. AK: Writing – review & editing. EN: Conceptualization, Data curation, Investigation, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. de Cássia Sparapani V, Liberatore RDR, Damião EBC, de Oliveira Dantas IR, de Camargo RAA, Nascimento LC. Children with type 1 diabetes mellitus: self-management experiences in school. J Sch Health. (2017) 87(8):623–9. doi: 10.1111/josh.12529
2. International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Brussels: International Diabetes Federation (2021). https://www.diabetesatlas.org (Accessed February 09, 2024).
3. Giwa AM, Ahmed R, Omidian Z, Majety N, Karakus KE, Omer SM, et al. Current understandings of the pathogenesis of type 1 diabetes: genetics to environment. World J Diabetes. (2020) 11(1):13. doi: 10.4239/wjd.v11.i1.13
4. Olinder AL, DeAbreu M, Greene S, Haugstvedt A, Lange K, Majaliwa ES, et al. ISPAD clinical practice consensus guidelines 2022: diabetes education in children and adolescents. Pediatr Diabetes. (2022) 23(8):1229. doi: 10.1111/pedi.13418
5. Committee ADAPP, ElSayed NA, Aleppo G, Bannuru RR, Bruemmer D, Collins BS, et al. Children and adolescents: standards of care in diabetes—2024. Diabetes Care. (2024) 47(Supplement_1):S258–81. doi: 10.2337/dc24-S014
6. Lawton J, Waugh N, Barnard KD, Noyes K, Harden J, Stephen J, et al. Challenges of optimizing glycaemic control in children with type 1 diabetes: a qualitative study of parents’ experiences and views. Diabetic Med. (2015) 32(8):1063–70. doi: 10.1111/dme.12660
7. Koller D, Khan N, Barrett S. Pediatric perspectives on diabetes self-care: a process of achieving acceptance. Qual Health Res. (2015) 25(2):264–75. doi: 10.1177/1049732314551057
8. Deeb A, Akle M, Al Ozairi A, Cameron F. Common issues seen in paediatric diabetes clinics, psychological formulations, and related approaches to management. J Diabetes Res. (2018) 2018:1684175. doi: 10.1155/2018/1684175
9. Elian V, Popovici V, Ozon EA, Musuc AM, Fița AC, Rusu E, et al. Current technologies for managing type 1 diabetes mellitus and their impact on quality of life—a narrative review. Life. (2023) 13(8):1663. doi: 10.3390/life13081663
10. Kilvert A, Fox C. The impact of diabetes technology advances on quality of life: addressing the barriers to uptake. Pract Diabetes. (2023) 40(5):23–8. doi: 10.1002/pdi.2476
11. Brew-Sam N, Chhabra M, Parkinson A, Hannan K, Brown E, Pedley L, et al. Experiences of young people and their caregivers of using technology to manage type 1 diabetes mellitus: systematic literature review and narrative synthesis. JMIR Diabetes. (2021) 6(1):e20973. doi: 10.2196/20973
12. Chiang JL, Kirkman MS, Laffel LMB, Peters AL. Type 1 diabetes through the life span: a position statement of the American diabetes association. Diabetes Care. (2014) 37(7):2034. doi: 10.2337/dc14-1140
13. Nagy E. The newborn infant: a missing stage in developmental psychology. Infant Child Dev. (2011) 20(1):3–19. doi: 10.1002/icd.683
14. Van Der Horst K, Sleddens EFC. Parenting styles, feeding styles and food-related parenting practices in relation to toddlers’ eating styles: a cluster-analytic approach. PLoS One. (2017) 12(5):e0178149. doi: 10.1371/journal.pone.0178149
15. Hilliard ME, Monaghan M, Cogen FR, Streisand R. Parent stress and child behaviour among young children with type 1 diabetes. Child Care Health Dev. (2011) 37(2):224–32. doi: 10.1111/j.1365-2214.2010.01162.x
16. Lindström C, Åman J, Norberg AL, Forssberg M, Anderzén-Carlsson A. “Mission impossible”; the mothering of a child with type 1 diabetes – from the perspective of mothers experiencing burnout. J Pediatr Nurs. (2017) 36:149–56. doi: 10.1016/j.pedn.2017.06.002
17. Iversen AS, Graue M, Haugstvedt A, Råheim M. Being mothers and fathers of a child with type 1 diabetes aged 1 to 7 years: a phenomenological study of parents’ experiences. Int J Qual Stud Health Well-Being. (2018) 13(1):1487758. doi: 10.1080/17482631.2018.1487758
18. Oser TK, Oser SM, McGinley EL, Stuckey HL. A novel approach to identifying barriers and facilitators in raising a child with type 1 diabetes: qualitative analysis of caregiver blogs. JMIR Diabetes. (2017) 2(2):e8966. doi: 10.2196/diabetes.8966
19. Pierce JS, Aroian K, Caldwell C, Ross JL, Lee JM, Schifano E, et al. The ups and downs of parenting young children with type 1 diabetes: a crowdsourcing study. J Pediatr Psychol. (2017) 42(8):846–60. doi: 10.1093/jpepsy/jsx056
20. Sundberg F, Forsander G, Fasth A, Ekelund U. Children younger than 7 years with type 1 diabetes are less physically active than healthy controls. Acta Paediatr. (2012) 101(11):1164–9. doi: 10.1111/j.1651-2227.2012.02803.x
21. Giblin S, Scully P, Dalton N, Connolly M, Mccaffrey A, Sheikhi A, et al. Parent and child perceptions of physical activity with type 1 diabetes. BMJ Open Diab Res Care. (2022) 10:2977. doi: 10.1136/bmjdrc-2022-002977
22. Yardley J, Mollard R, MacIntosh A, MacMillan F, Wicklow B, Berard L, et al. Vigorous intensity exercise for glycemic control in patients with type 1 diabetes. Can J Diabetes. (2013) 37(6):427–32. doi: 10.1016/j.jcjd.2013.08.269
23. Harrington KR, Boyle CT, Miller KM, Hilliard ME, Anderson BJ, Van Name M, et al. Management and family burdens endorsed by parents of youth <7 years old with type 1 diabetes. J Diabetes Sci Technol. (2017) 11(5):980–7. doi: 10.1177/1932296817721938
24. Herbert LJ, Clary L, Owen V, Monaghan M, Alvarez V, Streisand R. Relations among school/daycare functioning, fear of hypoglycaemia and quality of life in parents of young children with type 1 diabetes. J Clin Nurs. (2015) 24(9–10):1199–209. doi: 10.1111/jocn.12658
25. Commissariat P V, Volkening LK, Guo Z, ElBach JL, Butler DA, Laffel LM. Associations between major life events and adherence, glycemic control, and psychosocial characteristics in teens with type 1 diabetes. Pediatr Diabetes. (2018) 19(1):85–91. doi: 10.1111/pedi.12523
26. Rankin D, Harden J, Barnard K, Bath L, Noyes K, Stephen J, et al. Barriers and facilitators to taking on diabetes self-management tasks in pre-adolescent children with type 1 diabetes: a qualitative study. BMC Endocr Disord. (2018) 18(1):1–9. doi: 10.1186/s12902-018-0302-y
27. Lowes L, Eddy D, Channon S, McNamara R, Robling M, Gregory JW. The experience of living with type 1 diabetes and attending clinic from the perception of children, adolescents, and carers: analysis of qualitative data from the DEPICTED study. J Pediatr Nurs. (2015) 30(1):54–62. doi: 10.1016/j.pedn.2014.09.006
28. Ayala JM, Murphy K. Managing psychosocial issues in a family with diabetes. MCN Am J Matern Child Nurs. (2011) 36(1):49–55. doi: 10.1097/NMC.0b013e3181fc5e94
29. Junco LA, Fernández-Hawrylak M. Teachers and parents’ perceptions of care for students with type 1 diabetes mellitus and their needs in the school setting. Children. (2022) 9(2):143. doi: 10.3390/children9020143
30. Siminerio LM, Albanese-O’Neill A, Chiang JL, Hathaway K, Jackson CC, Weissberg-Benchell J, et al. Care of young children with diabetes in the child care setting: a position statement of the American diabetes association. Diabetes Care. (2014) 37(10):2834–42. doi: 10.2337/dc14-1676
31. Peeters M, Oldehinkel T, Vollebergh W. Behavioral control and reward sensitivity in adolescents’ risk taking behavior: a longitudinal TRAILS study. Front Psychol. (2017) 8(FEB):247559. doi: 10.3389/fpsyg.2017.00231
32. Somerville LH, Hare T, Casey BJ. Frontostriatal maturation predicts cognitive control failure to appetitive cues in adolescents. J Cogn Neurosci. (2011) 23(9):2123–34. doi: 10.1162/jocn.2010.21572
33. Van De Wiel A. Diabetes mellitus and alcohol. Diabetes Metab Res Rev. (2004) 20(4):263–7. doi: 10.1002/dmrr.492
34. Barnard KD, Dyson P, Sinclair JM, Lawton J, Anthony D, Cranston M, et al. Alcohol health literacy in young adults with type 1 diabetes and its impact on diabetes management. Diabetic Med. (2014) 31(12):1625–30. doi: 10.1111/dme.12491
35. MacNaught N, Holt P. Type 1 diabetes and alcohol consumption. Nurs Stand. (2015) 29(50):41. doi: 10.7748/ns.29.50.41.e9812
36. Pastor A, Conn J, MacIsaac RJ, Bonomo Y. Alcohol and illicit drug use in people with diabetes. Lancet Diabetes Endocrinol. (2020) 8(3):239–48. doi: 10.1016/S2213-8587(19)30410-3
37. Pastor A, Conn J, Loh M, O’Brien CL, Teng J, Finch S, et al. Glucose patterns following alcohol and illicit drug use in young adults with type 1 diabetes: a flash glucose monitoring study. Endocrinol Diabetes Metab. (2021) 4(3):e00257. doi: 10.1002/edm2.257
38. Pursey KM, Hay P, Bussey K, Trompeter N, Lonergan A, Pike KM, et al. Diabetes and disordered eating behaviours in a community-based sample of Australian adolescents. J Eat Disord. (2020) 8(1):1–9. doi: 10.1186/s40337-020-0282-y
39. Grigolon RB, Dunker KLL, Almeida MC, Achôa DC, Claudino AM. Dietary patterns as a red flag for higher risk of eating disorders among female teenagers with and without type I diabetes mellitus: adolescents with type I diabetes mellitus are a risk factor for eating disorders: a case-control study. Eat Weight Disord. (2019) 24(1):151–61. doi: 10.1007/s40519-017-0442-5
40. Gagnon C, Aimé A, Bélanger C. Predictors of comorbid eating disorders and diabetes in people with type 1 and type 2 diabetes. Can J Diabetes. (2017) 41(1):52–7. doi: 10.1016/j.jcjd.2016.06.005
41. Goebel-Fabbri AE. Disturbed eating behaviors and eating disorders in type 1 diabetes: clinical significance and treatment recommendations. Curr Diab Rep. (2009) 9(2):133–9. doi: 10.1007/s11892-009-0023-8
42. Chou WC, Chou YY, Pan YW, Ou TY, Tsai MC. Correlates of disordered eating and insulin restriction behavior and its association with psychological health in Taiwanese youths with diabetes mellitus. J Eat Disord. (2023) 11(1):1–8. doi: 10.1186/s40337-022-00727-2
43. Jaensch L, Goddard G, Oxlad M, Franke E. Health professionals’ experiences supporting people with type 1 diabetes Mellitus who deliberately restrict and/or omit insulin for weight, shape, and/or appearance: a meta-synthesis. Can J Diabetes. (2023) 47(6):532–42. doi: 10.1016/j.jcjd.2023.03.003
44. Pinna F, Diana E, Sanna L, Deiana V, Manchia M, Nicotra E, et al. Assessment of eating disorders with the diabetes eating problems survey - revised (DEPS-R) in a representative sample of insulin-treated diabetic patients: a validation study in Italy. BMC Psychiatry. (2017) 17(1):1–11. doi: 10.1186/s12888-017-1434-8
45. Wisting L, Frøisland DH, Skrivarhaug T, Dahl-Jørgensen K, Rø Ø. Disturbed eating behavior and omission of insulin in adolescents receiving intensified insulin TreatmentA nationwide population-based study. Diabetes Care. (2013) 36(11):3382–7. doi: 10.2337/dc13-0431
46. Young-Hyman DL, Davis CL. Disordered eating behavior in individuals with diabetes: importance of context, evaluation, and classification. Diabetes Care. (2010) 33(3):683. doi: 10.2337/dc08-1077
47. Akbari M, Seydavi M, Rowhani NS, Nouri N. Psychological predictors of treatment adherence among patients with diabetes (types I and II): modified information–motivation–behavioural skills model. Clin Psychol Psychother. (2022) 29(6):1854–66. doi: 10.1002/cpp.2746
48. Wisting L, Bang L, Skrivarhaug T, Dahl-Jørgensen K, Rø Ø. Adolescents with type 1 diabetes – the impact of gender, age, and health-related functioning on eating disorder psychopathology. PLoS One. (2015) 10(11):e0141386. doi: 10.1371/journal.pone.0141386
49. Wisting L, Bang L, Skrivarhaug T, Dahl-Jørgensen K, Rø Ø. Psychological barriers to optimal insulin therapy: more concerns in adolescent females than males. BMJ Open Diabetes Res Care. (2016) 4(1):e000203. doi: 10.1136/bmjdrc-2016-000203
50. Wisting L, Reas DL, Bang L, Skrivarhaug T, Dahl-Jørgensen K, Rø Ø. Eating patterns in adolescents with type 1 diabetes: associations with metabolic control, insulin omission, and eating disorder pathology. Appetite. (2017) 114:226–31. doi: 10.1016/j.appet.2017.03.035
51. Ryninks K, Sutton E, Thomas E, Jago R, Shield JPH, Burren CP. Attitudes to exercise and diabetes in young people with type 1 diabetes mellitus: a qualitative analysis. PLoS One. (2015) 10(10):e0137562. doi: 10.1371/journal.pone.0137562
52. Williams C, Sharpe L, Mullan B. Developmental challenges of adolescents with type 1 diabetes: the role of eating attitudes, family support and fear of negative evaluation. Psychol Health Med. (2014) 19(3):324–34. doi: 10.1080/13548506.2013.808750
53. Mistry B, Van Blyderveen S, Punthakee Z, Grant C. Condition-related predictors of successful transition from paediatric to adult care among adolescents with type 1 diabetes. Diabetic Med. (2015) 32(7):881–5. doi: 10.1111/dme.12746
54. Ladd JM, Reeves-Latour J, Dasgupta K, Bell LE, Anjachak N, Nakhla M. Toward a better understanding of transition from paediatric to adult care in type 1 diabetes: a qualitative study of adolescents. Diabetic Med. (2022) 39(5):e14781. doi: 10.1111/dme.14781
Keywords: age-based challenges, type 1 diabetes, management, glycemic control, developmental stages, self-management, children, adolescent
Citation: Lan Y-Y, Kovinthapillai R, Kędzia A and Niechciał E (2024) Age-based challenges to type 1 diabetes management in the pediatric population. Front. Pediatr. 12:1434276. doi: 10.3389/fped.2024.1434276
Received: 17 May 2024; Accepted: 20 August 2024;
Published: 2 September 2024.
Edited by:
Giulio Maltoni, IRCCS University Hospital of Bologna Sant Orsola Polyclinic, ItalyReviewed by:
Luca Bernardini, University of Bologna, ItalyAngela Zanfardino, University of Campania Luigi Vanvitelli, Italy
Copyright: © 2024 Lan, Kovinthapillai, Kędzia and Niechciał. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elżbieta Niechciał, ZS5uaWVjaGNpYWxAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship