 Loes Oomen1*
Loes Oomen1* Charlotte M. H. H. T. Bootsma-Robroeks2,3
Charlotte M. H. H. T. Bootsma-Robroeks2,3 Antonia H. M. Bouts4Mar Carbonell Pradas5Romy Gander6
Antonia H. M. Bouts4Mar Carbonell Pradas5Romy Gander6 Katrin Kienzl-Wagner7Paul König8
Katrin Kienzl-Wagner7Paul König8 Pedro Lopez Pereira9Olivier Dunand10Sara M. F. S. Mosca11Michal Pac12
Pedro Lopez Pereira9Olivier Dunand10Sara M. F. S. Mosca11Michal Pac12 Ludmila Podracka13
Ludmila Podracka13 Agnieszka A. Prytula14Maria Sangermano15Renata Vitkevic16
Agnieszka A. Prytula14Maria Sangermano15Renata Vitkevic16 Jakub Zieg17
Jakub Zieg17 Loes F. M. van der Zanden18
Loes F. M. van der Zanden18 Wout F. J. Feitz1,†
Wout F. J. Feitz1,† Liesbeth L. de Wall1,†
Liesbeth L. de Wall1,†
- 1Division of Pediatric Urology, Department of Urology, Radboudumc Amalia Children’s Hospital, Nijmegen, Netherlands
- 2Department of Pediatric Nephrology, Radboudumc Amalia Children’s Hospital, Nijmegen, Netherlands
- 3Department of Pediatrics, Pediatric Nephrology, Beatrix Children’s Hospital, University of Groningen, University Medical Centre Groningen, Groningen, Netherlands
- 4Department of Pediatric Nephrology, Emma Children’s Hospital, Amsterdam University Medical Center, Amsterdam, Netherlands
- 5Department of Pediatric Surgery, Hospital Sant Joan de Déu, Universitat de Barcelona, Barcelona, Spain
- 6Pediatric Urology and Renal Transplant Unit, Department of Pediatric Surgery, University Hospital Vall d´Hebron Barcelona, Barcelona, Spain
- 7Department of Visceral, Transplant and Thoracic Surgery, Medical University of Innsbruck, Innsbruck, Austria
- 8Department of Urology and Pediatric Urology, Universitätsklinikum Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
- 9Department of Pediatric Urology, University Hospital La Paz, Madrid, Spain
- 10Department of Pediatric Nephrology, University Hospital of Réunion, La Réunion, France
- 11Department of Pediatric Nephrology, Centro Materno Infantil do Norte, Centro Hospitalar Universitário de Santo António, Porto, Portugal
- 12Department of Nephrology, Kidney Transplantation and Hypertension, Children’s Memorial Health Institute, Warsaw, Poland
- 131st Dept Pediatric Children’s Hospital, Comenius University, Bratislava, Slovakia
- 14Department of Paediatric Nephrology and Rheumatology, Ghent University Hospital, ERKNet Centre, Ghent, Belgium
- 15Pediatric Nephrology, Dialysis and Transplant Unit, Department of Women’s and Children’s Health, Padua University Hospital, Padua, Italy
- 16Department of Pediatrics, Vilnius University Hospital Santaros Klinikos, Vilnius, Lithuania
- 17Department of Pediatrics, Second Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czechia
- 18IQ Health Science Department, Radboudumc, Nijmegen, Netherlands
Background: Pediatric kidney transplantations are rarely performed, and there is limited knowledge about the diversity in current clinical practices across Europe. This study aims to explore the utility of clinical snapshot studies in identifying these disparities, establishing a foundation for future snapshot studies and standardization efforts.
Methods: A pilot clinical snapshot study was conducted, with invitations extended to all 109 pediatric kidney transplant centres in Europe. Each participating centre provided pre-, peri-, and postoperative data concerning their most recent thirty transplantations. The primary outcomes encompassed the evaluation of disparities in donor-recipient selection, surgical techniques, post-operative drainage procedures, and immunosuppressive therapy protocols. Secondary outcomes involved the analysis of rejection rates, incidence of infections, and graft survival.
Results: The study involved 439 patients from fifteen centres (14%) in twelve countries, with varying transplant volumes (range 1–29 transplantations per year) and follow-up periods. Significant differences were found among centres in terms of donor types, cold and warm ischemia time, pre-emptive transplant rates, and kidney transplant drainage methods. The rate of living donors varied between 3% and 90% and the median duration of cold ischemia ranged was 770 min after deceased donation and 147 min after living donation. Basiliximab was the dominant induction therapy, yet steroid withdrawal varied widely. Infection, rejection, and graft survival rates also varied significantly between centres.
Conclusion: This study revealed substantial variation in clinical practices among European centres performing pediatric kidney transplantations. These findings could serve as a stimulus for international dialogue and collaboration.
1 Introduction
Pediatric kidney transplantations (PKT) remain a rarity, with only 500–600 performed in Europe annually, compared to over 21,000 procedures in adults (1, 2). Previously, we identified 109 centres within the European Union that perform PKT revealing significant variations in the level of centralization across countries (3). This raises questions about the divergence in clinical practices throughout Europe. Considering the improvements in immunosuppressive strategies, surgical techniques, and utilization of living (unrelated) donors (LD) in recent decades, there might be a considerable variation in daily practices among European centres and countries. Despite the presence of national PKT protocols, international guidelines are primarily designed for adult transplants with no specific European guideline for PKT (4, 5).
For enhanced coordination and care evaluation, gaining better insights into current practices is of importance. This information might allow comparison of clinical management among expert centres, replication of best practices in different countries, and improving the quality of care where possible. The low incidence of PKT poses challenges for traditional research methods. A recent publication showed that only 39% of the PKT centres contribute their data to existing European, multi-national registries, and these registries show substantial differences in the parameters they collect (3). Besides, information on peri-operative urological factors is lacking in all of these registries. Therefore, this multi-centre retrospective cohort study aims to explore variations in clinical practices across Europe marking the initial step toward potential standardization efforts.
2 Methods
2.1 Study design
This clinical snapshot pilot is an international retrospective cohort study. Snapshot studies allow researchers to efficiently collaborate with numerous clinicians, and to swiftly collect data from a diverse range of patients within a short timeframe. In this pilot, the use of snapshot studies to explore clinical variety is examined.
2.2 Study process
An electronic Case Report Form (eCRF) was developed to obtain information about the clinical practice of PKT. The variables were based on existing literature on prognostic factors influencing transplantation outcomes and the expertise and consensus of five expert clinicians. The eCRF covered six primary topics with a total of thirty-three questions. These topics included Characteristics (recipient, donor and transplantation), Surgical parameters, Graft Function, Immunosuppression, Infection, and Rejection (Supplementary Material 1).
Between March 2022 and November 2022, all 109 PKT centres across Europe were invited to participate, with a reminder sent after 1 month to non-responsive centres. To ensure anonymity, participating centres were identified by codes (e.g., C1, C2).
Data was collected from November 2022 to July 2023. Each participating centre contributed pseudonymized retrospective data for the last thirty consecutive patients who underwent PKT (The number of thirty patients was chosen to ensure a balance between data quantity, quality, and feasibility. While the primary focus was pediatric patients under nineteen, some centres extended the age range to include those up to 20 years.
Patients who received multiorgan transplants or had less than 1 month of observation were excluded due to differing clinical management and limited information. Only patients with a follow-up duration of at least 6 months were included in the analysis of follow-up events.
Data underwent rigorous validation through initial analysis by the primary researcher and cross-verification by individual centres to ensure reliability. Pseudonymized research data were securely entered into CastorEDC, a password-protected, cloud-based clinical data platform, with specific roles assigned (e.g., study coordinator, investigator). Data management and monitoring took place within CastorEDC.
The Committee for Human Research from Radboudumc waived the requirement for informed consent (file number: 2022-16138), respecting patient privacy and confidentiality. The study report adhered to the STROBE guidelines, with the comprehensive STROBE checklist available in Supplementary Material 3.
2.3 Definitions
To enhance the readability of the manuscript and facilitate data collection, causes of kidney failure were divided into two categories: urological conditions (vesico-ureteral reflux, neurogenic bladder, or posterior urethral valves) and nephrological conditions (all other cases). Immunosuppressive therapy was split into two categories as well: induction therapy (specific drugs given before surgery) and maintenance therapy (immunosuppressive medication prescribed at discharge after transplantation). In small children where extraperitoneal placement is not feasible, the graft may be placed intra-abdominally, defined as intraperitoneal kidney transplant with anastomosis within the abdominal cavity (6). Follow-up duration was calculated as the time between the last visit and the transplantation date.
Graft function was assessed by creatinine clearance, calculated using the Schwartz formula to estimate glomerular filtration rate (eGFR) with a maximum of 90 (7). This approach was chosen due to the widespread availability of its parameters, in contrast to more sophisticated methods for measuring renal function (8). Graft loss was defined as the start of dialysis or re-transplantation, while patient deaths with functioning grafts were considered as graft survival. Rejection was defined as a biopsy-proven acute rejection using the Banff classification (9).
Urinary tract infection (UTI) was defined as urine culture demonstrating the presence of >50,000 colony forming units/ml of a single pathogen in combination with clinical symptoms. Cytomegalovirus (CMV) and Epstein-Barr virus (EBV) infections were defined as the presence of CMV/EBV viremia or DNAemia at any point during follow-up (10). BK-virus (BKV) replication was quantified using real-time quantitative PCR assay using BKV specific primers. Infection and rejection rates were calculated per year of follow-up, while graft deterioration was measured as the change in eGFR from discharge to the last known value, divided by follow-up time.
2.4 Statistical analysis
Baseline characteristics of the study cohort were presented as numbers/percentages, median/interquartile ranges (IQR)/total ranges for skewed data or mean/standard deviation (SD) for normally distributed data. Missing data were handled through pairwise deletion.
To examine potential variations in patient characteristics, protocols, and outcomes among centres, chi-square tests, one-way ANOVA, and logistic regression analyses were used, all adjusted for follow-up duration. Logistic regression parameters were limited to a maximum of 10% relative to total events.
Graft survival curves were constructed using the Kaplan-Meier method and assessed with the log-rank test to identify significant differences in graft survival among groups. Statistical significance was defined at p < 0.05. Data analysis was performed using SPSS Statistics 25.0.
3 Results
Of 109 invited centres, 71 did not respond and 23 centres provided reasons for their non-participation such as lack of time/resources (N = 10, 43%) and local legislation (N = 5, 22%). Ultimately, fifteen centres (14%) in twelve countries* contributed patient data (Figure 1A) (* Austria, Belgium, Czechia, Germany, France, Italy, Lithuania, the Netherlands, Poland, Portugal, Slovakia, Spain).
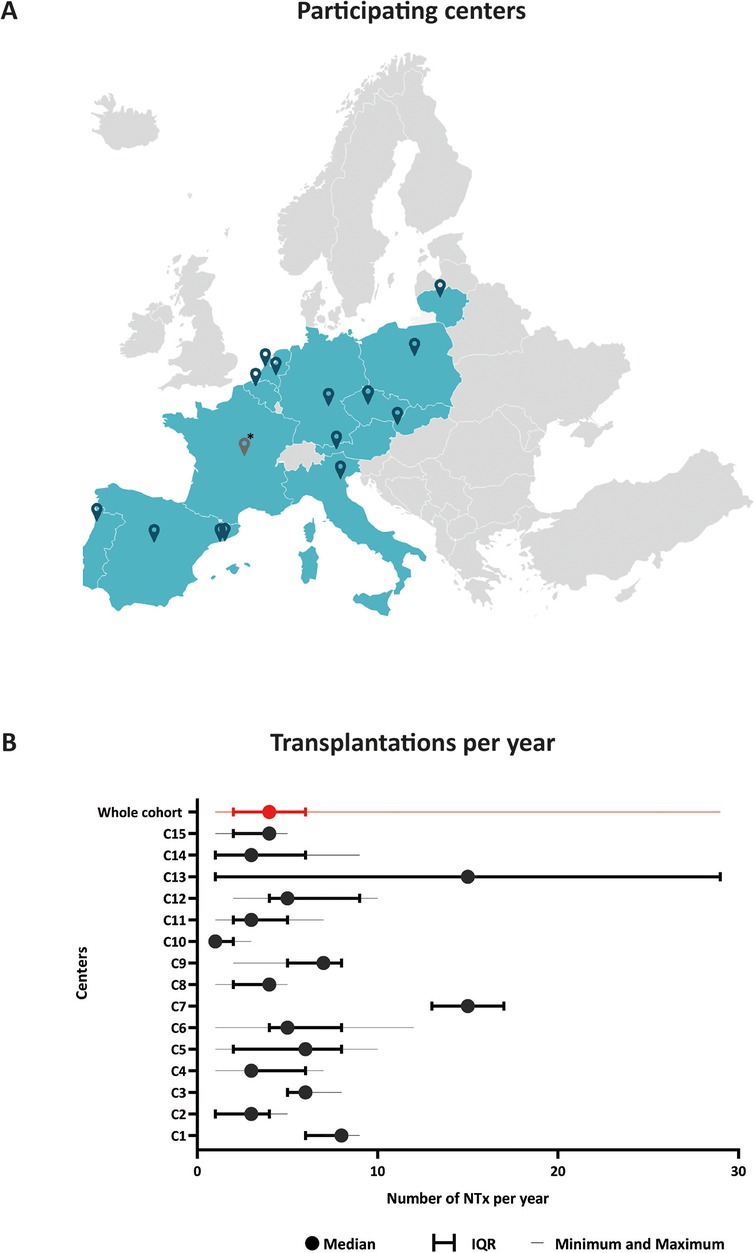
Figure 1. Overview of participating centers. (A) Geographical distribution of participating centers within Europe. (B) Number of pediatric kidney transplantations performed per year (n = 439). * Located in La Réunion, a French island not shown on this map. IQR, interquartile range; NTx, kidney transplantation.
Data from 439 transplantations (2011–2023) were available for analysis. Eleven patients were missing from one centre since this centre only recently started PKT. Median follow-up time was 26 months (range: 1–140 months, IQR: 10–46 months). The median annual transplantation rate was 4 (range: 1–29, IQR: 2–6), indicating varying degrees of centralization (Figure 1B).
3.1 Recipient/transplantation characteristics
Significant variations were observed in patient and transplantation characteristics across participating centers (Figure 2, Supplementary Table 1). All characteristics showed statistical significance except for the underlying disease causing renal failure (p = 0.16).
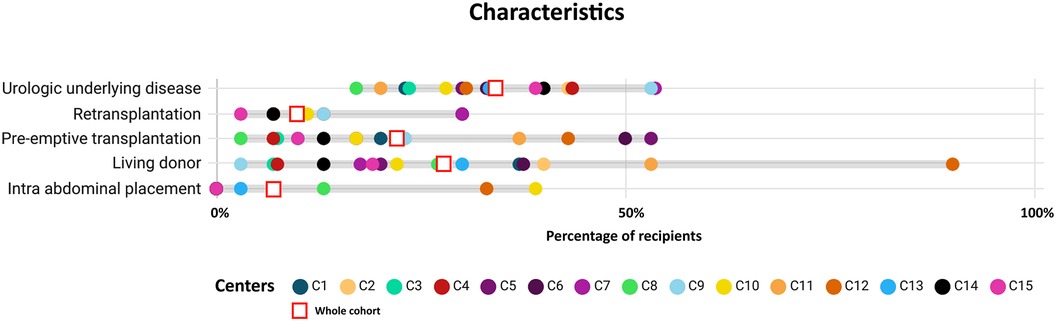
Figure 2. Comparison of main characteristics by centre. Percentage of recipients depicted by centre (n = 439). All characteristics were statistically significant (p < 0.05) except for underlying disease. Urologic underlying disease is defined as either vesico-ureteral reflux, neurogenic bladder, or posterior urethral valves. Intra-abdominal placement is defined as intraperitoneal placement of the kidney transplant with anastomosis within the abdominal cavity.
The type of donor also exhibited considerable disparities, with the majority of transplantations being performed after deceased donation (DD), 14 (3%) after circulatory death, 287 (65%) after brainstem death. Only one center showed a significant difference in recipient age between LD and DD transplants (Supplementary Material 2, Supplementary Figure 1). Furthermore, all centers included in the study performed transplants in recipients under the age of five, with five centers specifically conducting transplants in children younger than 3 years old (Supplementary Material 2, Supplementary Figure 1).
While it might be expected that LD would be more commonly used in pre-emptive transplantations, as seen in C3 and C4, this pattern was not consistent across all centers. For example, in C5 and C9, the majority of pre-emptive transplantations were conducted with DD (Supplementary Material 2, Supplementary Figure 2).
The number of human leucocyte antigen (HLA) mismatches showed significant differences with five centres permitting up to 6 mismatches, while 3 centres had a maximum allowance of 4 mismatches.
3.2 Surgical parameters
3.2.1 Peri-operative parameters
In 16% of the patients, the graft was placed intraperitoneal (intraabdominal placement). The age associated with intra-abdominal placement differed across centers. Three centers exclusively reserved this approach for recipients under 5 years old, while four centers employed it for recipients of all ages.
Furthermore, the ischemia duration showed wide variability, even when adjusted for donor type (p < 0.05) (Figure 3A,B). The median duration of cold ischemia time (CIT) was 770 min (range 15–1,000, IQR 600–968) for DD and 147 min (range 2–540, IQR 106–192) for LD. No differences in duration of warm ischemia (WIT) were found between LD and DD.
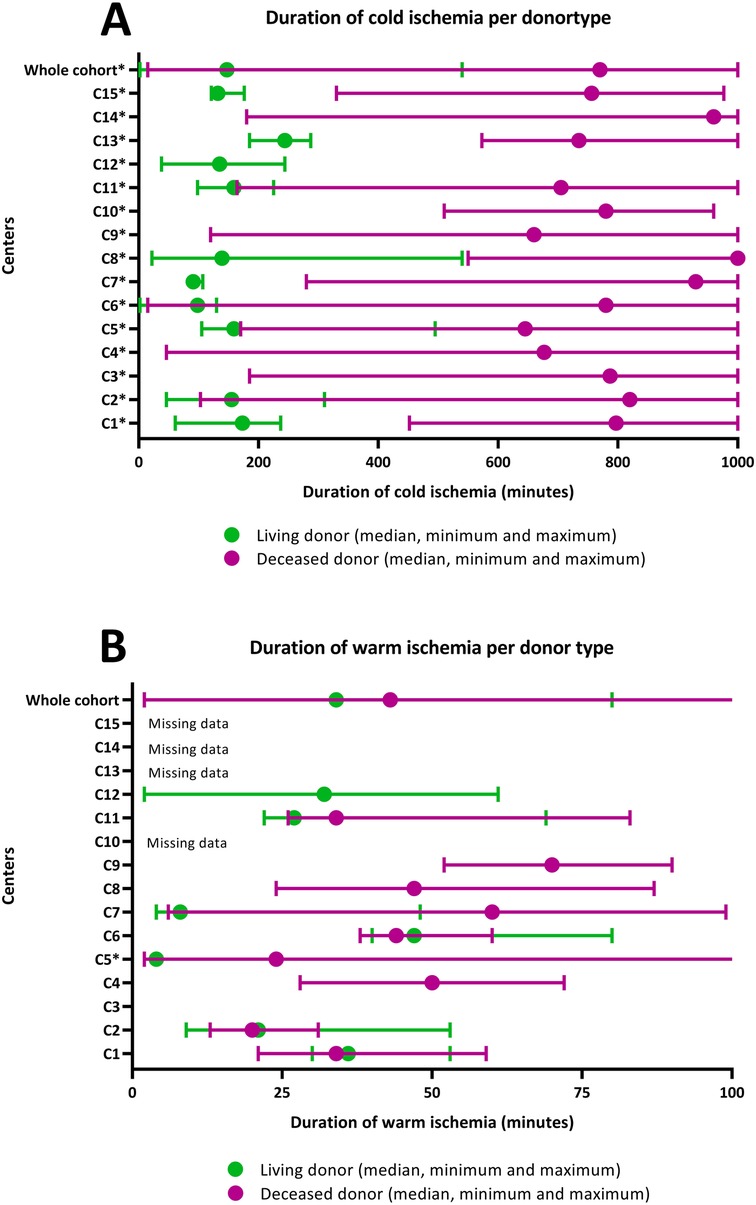
Figure 3. Duration of ischemia by centre. (A) Minutes of cold ischemia time per donor type, median with minimum and maximum (n = 384). (B) Minutes of warm ischemia time per donor type, median with minimum and maximum (n = 267). The default maximum cold ischemia time was set at 1,000 min. When n < 3 data were not shown. *Indicates a significant difference between donor types.
3.2.2 Post-operative parameters
Significant variations were observed in post-operative drainage protocols among the centres (p < 0.01). Figure 4 illustrates that the prevailing approach combined a transurethral catheter with either a double J stent (JJ) or a ureteral splint. Notably, eleven patients had a vesicostomy at the time of transplant, with the majority (N = 10, 91%) having a urological cause of kidney failure.
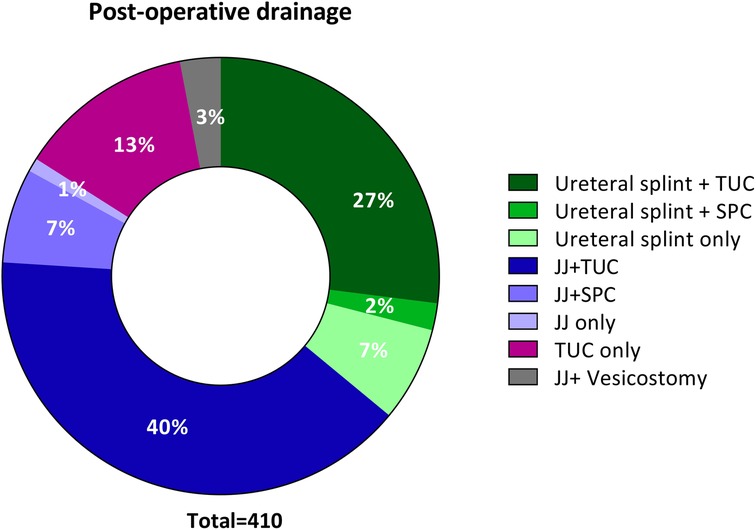
Figure 4. Post-operative kidney and bladder drainage (n = 410). JJ, Double J stent; SPC, suprapubic catheter; TUC, transurethral catheter.
The median bladder drainage duration was 8 days [IQR 5–11] (n = 169). For those using a ureteral splint, the median drainage duration was 7 days [IQR 6–10] (n = 155), while for JJ drainage, it was 38 days [IQR 21–51] (n = 199). However, a substantial amount of data regarding bladder drainage duration was missing (N = 190) as it could not be retrieved from patient files. The method of drainage did not influence the outcome of transplantation in terms of urinary tract infections (p = 0.08) or graft failure (p = 0.79).
3.3 Immunosuppressive regimens
Basiliximab served as the primary induction therapy agent (Figure 5A), followed by Antithymocyte globulin or Antilymphocyte globulin (ATG/ALG). Notably, C4 and C13 refrained from using any immunosuppressive medication prior to transplantation in most of their patients.
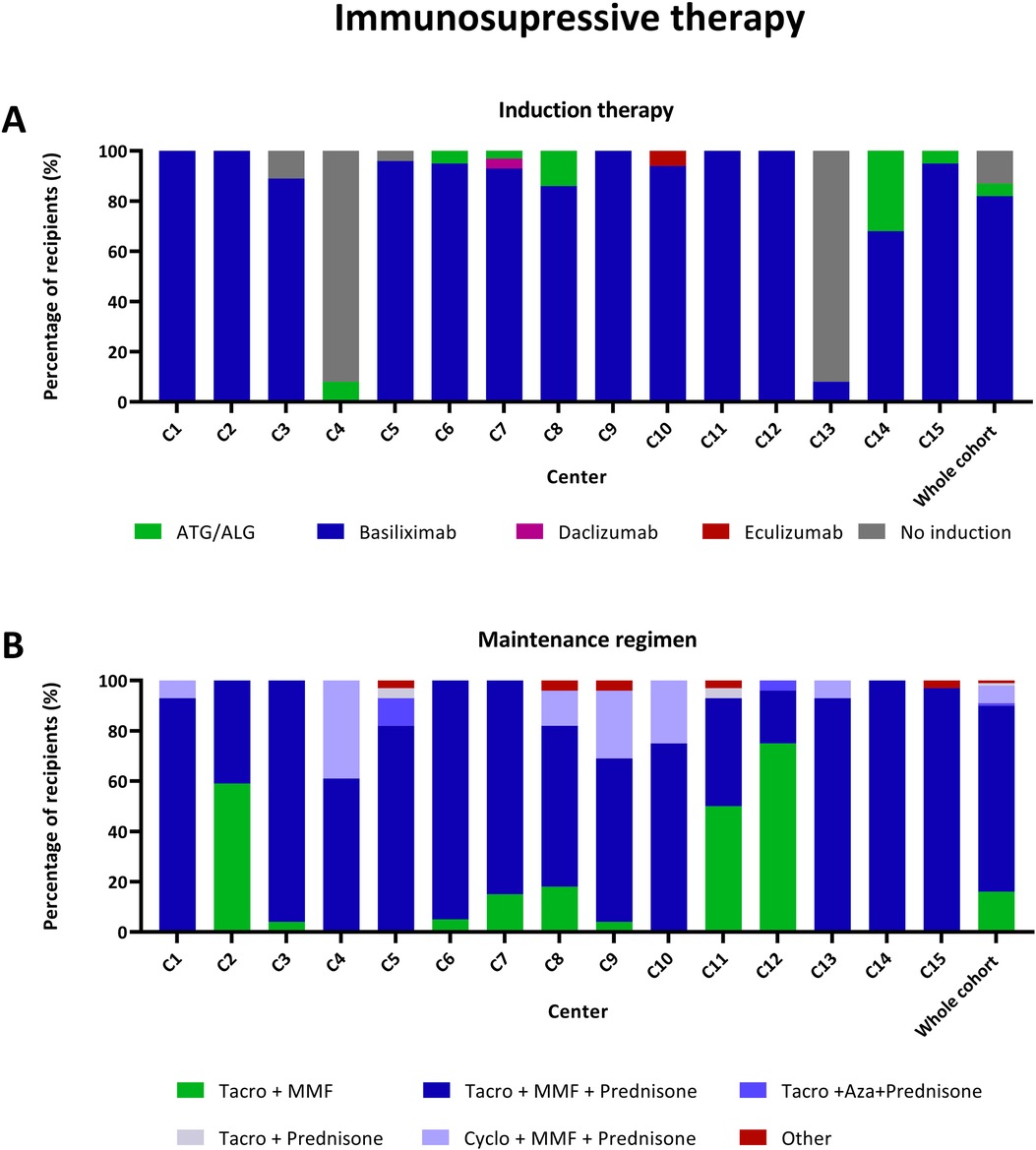
Figure 5. Immunosuppressive regimens in recipients that received their first transplantation (n = 384). (A) Immunosuppressive induction therapy by centre. (B) Immunosuppressive maintenance regimen prescribed at discharge by centre. Other: Tacrolimus monotherapy (n = 3), MMF + Prednisone (n = 2). ATG/ALG, Antithymocyte globulin/Antilymphocyte globulin; Aza, Azathioprine; MMF, Mycophenolate mofetil; Tacro, Tacrolimus.
Upon discharge, the prevailing immunosuppressive regimen for most recipients involved a combination of a calcineurin inhibitor, mycophenolate mofetil, and prednisone (Figure 5B). However, in four centres, a considerable number of recipients followed a steroid-sparing regimen, where prednisone was not prescribed upon discharge.
3.4 Infections
CMV prophylaxis usage varied among centres, ranging from 27% to 97% (Supplementary Material 2, Supplementary Figure 3). A significant correlation was found between CMV prophylaxis and the CMV donor-recipient status, with most centres employing prophylaxis more often when the donor-recipient CMV status posed a higher risk of subsequent infections (D + R−). CMV prophylaxis was not associated with the number of CMV infections per year (p = 0.41).
Differences in CMV and BKV infections were observed between centres (p < 0.01 and p = 0.02, respectively) after adjusting for the duration of follow-up (Supplementary Material 2, Supplementary Figure 4). There was no difference in EBV infections (p = 0.08). The number of UTI differed across centres (p = 0.01), however no information on antibiotic prophylaxis was available.
The rate of EBV infections was related to the use of prednisone, even when corrected for the EBV status of the donor and recipient prior to transplantation (Supplementary Material 2, Supplementary Table 2). The use of prednisone at discharge significantly increased the risk of EBV infection during the follow-up period.
3.5 Graft outcome
Figure 6 illustrates graft survival with a considerable 95% confidence interval after 5 years, suggesting variability in graft outcomes. Graft survival varied between centres (p = 0.02), as did the incidence of biopsy-proven rejection (p < 0.01) (Supplementary Material 2, Supplementary Figure 4). Rejection episodes occurred in 12% of recipients within the first year post-transplant, with rates varying across centres (ranging from 3% to 43%, p < 0.01). Despite these findings, the sample size in this study was insufficient to identify significant risk factors for graft survival.
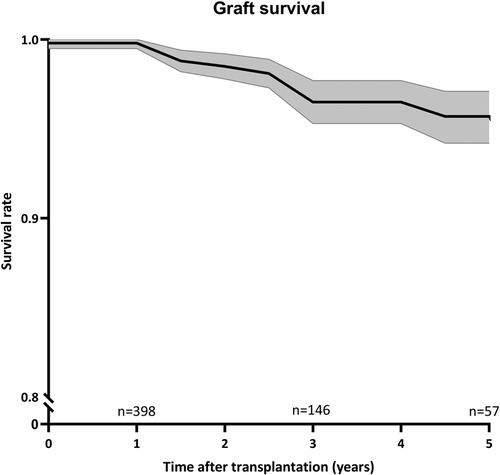
Figure 6. Graft survival over time. Kaplan-Meier curve for graft survival with 95% confidence interval (n = 439). Number of remaining cases were indicated every 2 years.
4 Discussion
This pilot snapshot study on pediatric kidney transplantation practices revealed substantial variations in clinical care across European centers. These variances encompass donor-recipient selection, transplantation volume, immunosuppressive regimens, kidney and bladder drainage, as well as differences in transplantation outcomes across centers. Additionally, the annual transplantation rates vary among centers. This prompts further inquiry into the ideal proficiency, expertise threshold and potential merits of further centralizing. Contento et al. reported higher graft survival in high-volume centers (>8 per year) compared to low-volume centers (<4 per year) (11). While centralizing PKT care may enhance outcomes by ensuring collective expertise of a multidisciplinary team, these advantages should be outweighted against disadvantages like geographical, logistical, and financial factors within countries (2, 12).
4.1 Pre-operative parameters
The main modifiable pre-transplant factor is donor selection, favoring LD over DD when feasible (13, 14). LD transplantations ranged between 3% and 90%, suggesting differences in protocols and allocation systems throughout European centers (2). Prioritizing pediatric patients on waiting lists may result in a higher number of young DD being allocated to these patients (1). The Council of Europe recommends the use of living (un)related donors as an opportunity to expand the number of potential donors, despite common hesitations (15).
Variations in allocation may partly explain differences in preemptive transplantations. Despite the advantages of pre-emptive transplantation, most patients underwent dialysis before their transplant. Differences could potentially be influenced by factors like varying acceptance of HLA mismatches (2, 16, 17). To choose pre-emptive transplantation with a suboptimal donor (e.g., DD, full mismatch) or to wait for an ideal donor (LD, full match) while on dialysis poses a complex dilemma (if feasible). Debates and establishing evidence-based international guidelines could be useful for improving long-term outcomes. Unfortunately, this study did not collect detailed donor information, such as age, comorbidities, or details about the composition of the surgical team. However, these factors would be valuable areas of focus for future research.
4.2 Peri-operative parameters
Peri-operative factors encompass a range of elements, including the surgical procedure itself, healthcare providers involved, and patient characteristics, all of which collectively influence outcomes. CIT and WIT are established determinants of transplantation success (18, 19). Variations in ischemia times persist between centers, influenced by organ procurement, transportation processes, and geographical distances across Europe (2).
While CIT primarily reflects allocation policies and travel distances, necessitating continuous international attention, variations in WIT may indicate modifiable local factors, such as surgical practices. Beyond patient-specific factors (vasculature, body mass), differences in surgical skills, techniques (e.g., intra- or extraperitoneal placement), and the surgeons’ specialties (transplant, vascular, urology, pediatric) might impact outcomes. Lack of more centralized care may lead to disparities in surgeons’ experience and expertise (18). Donor nephrectomy method (laparoscopic vs. open) could also impact WIT, though this study did not collect this data.
The choice of post-operative drainage method and duration remains an ongoing debate, balancing prevention of post-operative complications against infection risks (20, 21).
4.3 Post-operative factors
Despite the introduction of steroid-sparing regimens in 2012, many of the contributing centres still rely on prednisone for maintenance therapy after a first transplantation (22, 23). Uncertainty about the metabolic benefits and long-term safety of corticosteroid withdrawal were reported earlier, despite previous research demonstrating its safety in selected patients (23, 24). In this study, the use of prednisone as maintanance therapy was associated with EBV infection, although bias might exist. In children, steroid withdrawal should be seriously considered due to the potential impact of steroids on growth and development. Tönshoff et al. advocate for everolimus use to enable both steroid withdrawal and reduced exposure to calcineurin inhibitors, though none of the recipients in this study received everolimus at discharge after transplantation (25). Future research should focus on long-term effects of steroid withdrawal and identify obstacles to discontinuing prednisone. Ongoing advancements in immunosuppressive medications, including new drugs like belatacept could optimise future care.
4.4 Outcome
Due to the limited number of participating centers, patients, and the relatively short follow-up time, the study refrains from drawing definitive conclusions on transplantation outcomes. However, some variability in reported outcomes was observed. Generally, rejection rates in the first year were consistent with existing literature (26). However, significant discrepancies among centers, including one reporting a 43% rejection rate, raise questions about the uniformity of definitions. This variation may also relate to the use of protocol biopsies, a topic under ongoing debate. In-depth research should focus on differences and the impact and cost-effectiveness of protocol biopsies.
The 5-year graft survival rate, consistent with other research findings, was notably high at 92%, with few retransplantations performed (13, 26, 27). Long-term outcomes may vary between centers, and although the relation between clinical practice and graft survival is essential for future decision-making this falls beyond the scope of this study.
4.5 Future perspectives
The extensive variability in this study may stem from differences in work processes, education, individual habits, and notably, the absence of standardized PKT guidelines. Likewise, Voet et al. recently revealed a large variation in anesthesia and ICU care in pediatric kidney transplantation centers across Europe (28). The lack of international PKT guidelines may be partly attributed to local legislative disparities and variations in the roles and levels of involvement of specialists across centers. These include pediatric and adult urologists, nephrologists, transplantation surgeons, and general surgeons.
This reported diversity offers a valuable learning opportunity. Further snapshot research could help assess the impact of clinical practice diversity on transplant outcomes and assess the potential benefits of establishing best practices. Developing specific guidelines can serve as a valuable roadmap for clinicians, ensuring consistency and improve quality. The integration of evidence-based protocols with personalised medicine holds the potential to enhance the furhter optimisation of PKT care.
Addressing knowledge gaps remains crucial for evidence-based medicine. Despite the existence of multiple PKT registries in Europe, data collection is still scattered and incomplete. Further collaborations among international registries could prove valuable in aggregating new data and studying effects of various protocols on a larger scale. The establishment of European Reference Networks (ERNs) for rare and complex diseases represents a significant advancement in fostering international collaboration and, probably the harmonization of care (29, 30). Currently, three ERNs are involved in the field of pediatric kidney transplantation (PKT): ERKNet, ERN eUROGEN, and ERN TransplantChild. A collaborative effort between these networks to initiate a prospective study on variations in clinical practice would be a valuable step in the advancement of PKT care.
4.6 Strengths and limitations
This is a unique study in the field of PKT, providing valuable insights and a first step for further optimising PKT care. Its strengths stem from the diversity of the cohort, encompassing participants from various European countries, including those often overlooked in international analyses. Rigorous data validation processes enhance reliability of findings, and the relatively short study duration provides a snapshot of current practices.
However, a significant limitation is the restricted number of collaborating centers (14%) affecting the generalizability of the findings. This study provides only a sample from European centers rather than a comprehensive representation. However, incorporating data from more centers would likely increase the observed variability. Additionally, some definitions and measurement tools are not state of the art due to variations in diagnostics and classifications across centers. Therefore, less advanced definitions were employed to facilitate the inclusion of more patients. The substantial amount of missing and unreliable data underscores the significance of thorough documentation.
4.7 Conclusion
This inventory of pediatric kidney transplantation (PKT) practices in Europe revealed a wide range of clinical approaches among a sample of European centers. It serves as a stimulus for international dialogue and collaboration, emphasizing the importance of a unified effort within the transplantation community.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by METC Oost-Nederland The Netherlands. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LO: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Writing – original draft. CB-R: Conceptualization, Methodology, Supervision, Writing – review & editing. AB: Resources, Writing – review & editing. MC: Resources, Writing – review & editing. RG: Resources, Writing – review & editing. KK-W: Resources, Writing – review & editing. PK: Resources, Writing – review & editing. PP: Resources, Writing – review & editing. OD: Resources, Writing – review & editing. SM: Resources, Writing – review & editing. MP: Resources, Writing – review & editing. LP: Resources, Writing – review & editing. AP: Resources, Writing – review & editing. MS: Resources, Writing – review & editing. RV: Resources, Writing – review & editing. JZ: Resources, Writing – review & editing. LZ: Resources, Writing – review & editing. WF: Conceptualization, Methodology, Resources, Supervision, Writing – review & editing. LW: Conceptualization, Methodology, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank Alberto Caldas Afonso, Gabriel Kolveck and Marion Marc. Besides, we thank the ERN for Rare Urogenital Diseases and Complex Conditions (ERN eUROGEN) for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1432027/full#supplementary-material
References
1. Bonthuis M, Vidal E, Bjerre A, Aydoğ Ö, Baiko S, Garneata L, et al. Ten-year trends in epidemiology and outcomes of pediatric kidney replacement therapy in Europe: data from the ESPN/ERA-EDTA registry. Pediatr Nephrol. (2021) 36(8):2337–48. doi: 10.1007/s00467-021-04928-w
2. Harambat J, van Stralen KJ, Schaefer F, Grenda R, Jankauskiene A, Kostic M, et al. Disparities in policies, practices and rates of pediatric kidney transplantation in Europe. Am J Transplant. (2013) 13(8):2066–74. doi: 10.1111/ajt.12288
3. Oomen L, De Wall LL, Krupka K, Tönshoff B, Wlodkowski T, Van Der Zanden LF, et al. The strengths and complexities of European registries concerning paediatric kidney transplantation health care. Front Pediatr. (2023) 11. doi: 10.3389/fped.2023.1121282
4. Chapman JR. The KDIGO clinical practice guidelines for the care of kidney transplant recipients. Transplantation. (2010) 89(6):644–5. doi: 10.1097/TP.0b013e3181d62f1b
5. Rodríguez Faba O, Boissier R, Budde K, Figueiredo A, Taylor CF, Hevia V, et al. European association of urology guidelines on renal transplantation: update 2018. Eur Urol Focus. (2018) 4(2):208–15. doi: 10.1016/j.euf.2018.07.014
6. Etesami K, Hogen R, Lestz R. Pediatric kidney transplantation, a technical update. Curr Opin Organ Transplant. (2021) 26(4):356–9. doi: 10.1097/MOT.0000000000000898
7. Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics. (1976) 58(2):259–63. doi: 10.1542/peds.58.2.259
8. Jančič SG, Močnik M, Marčun Varda N. Glomerular filtration rate assessment in children. Children. (2022) 9(12):1991–5. doi: 10.3390/children9121995
9. Roufosse C, Simmonds N, Clahsen-van Groningen M, Haas M, Henriksen KJ, Horsfield C, et al. A 2018 reference guide to the banff classification of renal allograft pathology. Transplantation. (2018) 102(11):1795–814. doi: 10.1097/TP.0000000000002366
10. Ljungman P, Boeckh M, Hirsch HH, Josephson F, Lundgren J, Nichols G, et al. Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin Infect Dis. (2017) 64(1):87–91. doi: 10.1093/cid/ciw668
11. Contento MN, Vercillo RN, Malaga-Dieguez L, Pehrson LJ, Wang Y, Liu M, et al. Center volume and kidney transplant outcomes in pediatric patients. Kidney Med. (2020) 2(3):297–306. doi: 10.1016/j.xkme.2020.01.008
12. Wijnen MHWA, Hulscher JBF. Centralization of pediatric surgical care in the Netherlands: lessons learned. J Pediatr Surg. (2022) 57(2):178–81. doi: 10.1016/j.jpedsurg.2021.10.023
13. Oomen L, Bootsma-Robroeks C, Cornelissen E, de Wall L, Feitz W. Pearls and pitfalls in pediatric kidney transplantation after 5 decades. Front Pediatr. (2022) 10:856630. doi: 10.3389/fped.2022.856630
14. Chandar J, Chen L, Defreitas M, Ciancio G, Burke G 3rd. Donor considerations in pediatric kidney transplantation. Pediatr Nephrol. (2021) 36(2):245–57. doi: 10.1007/s00467-019-04362-z
15. Europe Co. Recommendation Rec(2006)16 of the committee of ministers to member states on quality improvement programmes for organ donatio. Available online at: www.CEO.int2006 (accessed October 09, 2023).
16. Kim JK, Lorenzo AJ, Farhat WA, Chua ME, Ming JM, Dos Santos J, et al. A comparison of post-transplant renal function in pre-emptive and post-dialysis pediatric kidney transplant recipients. Pediatr Transplant. (2019) 23(3):e13377. doi: 10.1111/petr.13377
17. Chinnakotla S, Verghese P, Chavers B, Rheault MN, Kirchner V, Dunn T, et al. Outcomes and risk factors for graft loss: lessons learned from 1,056 pediatric kidney transplants at the university of Minnesota. J Am Coll Surg. (2017) 224(4):473–86. doi: 10.1016/j.jamcollsurg.2016.12.027
18. Tennankore KK, Kim SJ, Alwayn IPJ, Kiberd BA. Prolonged warm ischemia time is associated with graft failure and mortality after kidney transplantation. Kidney Int. (2016) 89(3):648–58. doi: 10.1016/j.kint.2015.09.002
19. Debout A, Foucher Y, Trébern-Launay K, Legendre C, Kreis H, Mourad G, et al. Each additional hour of cold ischemia time significantly increases the risk of graft failure and mortality following renal transplantation. Kidney Int. (2015) 87(2):343–9. doi: 10.1038/ki.2014.304
20. Wilson CH, Rix DA, Manas DM. Routine intraoperative ureteric stenting for kidney transplant recipients. Cochrane Database Syst Rev. (2013) 6:Cd004925. doi: 10.1002/14651858.CD004925.pub3
21. Friedersdorff F, Weinberger S, Biernath N, Plage H, Cash H, El-Bandar N. The ureter in the kidney transplant setting: ureteroneocystostomy surgical options, double-J stent considerations and management of related complications. Curr Urol Rep. (2020) 21(1):3. doi: 10.1007/s11934-020-0956-7
22. Grenda R, Watson A, Trompeter R, Tönshoff B, Jaray J, Fitzpatrick M, et al. A randomized trial to assess the impact of early steroid withdrawal on growth in pediatric renal transplantation: the TWIST study. Am J Transplant. (2010) 10(4):828–36. doi: 10.1111/j.1600-6143.2010.03047.x
23. Woodle ES, Gill JS, Clark S, Stewart D, Alloway R, First R. Early corticosteroid cessation vs. long-term corticosteroid therapy in kidney transplant recipients: long-term outcomes of a randomized clinical trial. JAMA Surg. (2021) 156(4):307–14. doi: 10.1001/jamasurg.2020.6929
24. Oomen L, de Wall LL, Cornelissen EA, Feitz WFJ, Charlotte BR. Steroid withdrawal in pediatric kidney recipients: is it safe? Int J Transplant Plast Surg. (2021) 5(1). doi: 10.23880/IJTPS-16000159
25. Tönshoff B, Tedesco-Silva H, Ettenger R, Christian M, Bjerre A, Dello Strologo L, et al. Three-year outcomes from the CRADLE study in de novo pediatric kidney transplant recipients receiving everolimus with reduced tacrolimus and early steroid withdrawal. Am J Transplant. (2021) 21(1):123–37. doi: 10.1111/ajt.16005
26. Lentine KL, Smith JM, Miller JM, Bradbrook K, Larkin L, Weiss S, et al. OPTN/SRTR 2021 annual data report: kidney. Am J Transplant. (2023) 23(2 Suppl 1):S21–S120. doi: 10.1016/j.ajt.2023.02.004
27. Verghese PS. Pediatric kidney transplantation: a historical review. Pediatr Res. (2017) 81(1):259–64. doi: 10.1038/pr.2016.207
28. Voet M, Lemson J, Cornelissen M, Malagon I. Anesthesia and intensive care unit care in pediatric kidney transplantation: an international survey. Paediatr Anaesth. (2024) 34(3):235–42. doi: 10.1111/pan.14810
29. Bassanese G, Wlodkowski T, Servais A, Heidet L, Roccatello D, Emma F, et al. The European rare kidney disease registry (ERKReg): objectives, design and initial results. Orphanet J Rare Dis. (2021) 16(1):251. doi: 10.1186/s13023-021-01872-8
Keywords: pediatric kidney transplantation, clinical practice snapshot, Europe, donor type, graft survival, registries
Citation: Oomen L, Bootsma-Robroeks CMHHT, Bouts AHM, Carbonell Pradas M, Gander R, Kienzl-Wagner K, König P, Pereira PL, Dunand O, Mosca SMFS, Pac M, Podracka L, Prytula AA, Sangermano M, Vitkevic R, Zieg J, van der Zanden LFM, Feitz WFJ and de Wall LL (2024) Pediatric kidney transplantation in Europe, a clinical snapshot pilot. Front. Pediatr. 12:1432027. doi: 10.3389/fped.2024.1432027
Received: 13 May 2024; Accepted: 7 October 2024;
Published: 24 October 2024.
Edited by:
Pierluigi Marzuillo, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Nicos Kessaris, Guy’s Hospital, United KingdomMilena Taskovska, University Medical Centre Ljubljana, Slovenia
Copyright: © 2024 Oomen L, Bootsma-Robroeks, Bouts, Carbonell Pradas, Gander, Kienzl-Wagner, König, Pereira, Dunand, Mosca, Pac, Podracka, Prytula, Sangermano, Vitkevic, Zieg, van der Zanden, Feitz and de Wall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Loes Oomen, bG9lcy5vb21lbkByYWRib3VkdW1jLm5s
†These authors have contributed equally to this work