
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr., 03 July 2024
Sec. Neonatology
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1401468
 Lavinia Di Meglio1*
Lavinia Di Meglio1* Giordana Sica2Paolo Toscano3
Giordana Sica2Paolo Toscano3 Giuliana Orlandi3Luigi Manzo3Laura Letizia Mazzarelli3,4Carmine Sica4Aniello Di Meglio4
Giuliana Orlandi3Luigi Manzo3Laura Letizia Mazzarelli3,4Carmine Sica4Aniello Di Meglio4
Introduction: Vein of Galen malformations (VGMs) account for less than 1% of all intracranial vascular malformations. However, in fetal and pediatric populations, they represent the most common vascular malformation of the brain. For the effective management of this condition, an optimal knowledge of its prenatal and postnatal clinical features is mandatory.
Methods: Articles published between 1 January 2003 and 31 January 2024, reported in PubMed and EMBASE, were evaluated for a systematic review analyzing the prenatal and postnatal features and management of fetal VGMs.
Results: Thirty-one papers reporting information on 51 prenatally diagnosed VGMs were included. The most common prenatal features were fetal hydrocephalus (39%) and cardiomegaly (56%). Postnatal data for 43 VGM cases are described. The overall mortality was 58.14%. In total, 77.78% of the survivors had normal development.
Conclusions: Close follow-up and a multidisciplinary approach are mandatory to manage this condition. Our study aimed to provide a guide for gynecologists, neonatologists, cardiologists, and neuroradiologists.
Vein of Galen malformations (VGMs), also known as vein of Galen aneurysmal malformations (VGAMs), are extremely rare congenital arteriovenous malformations involving the intracranial vessels. The incidence of VGMs is 1:10,000–25,000, accounting for less than 1% of all intracranial vascular malformations (1, 2). However, in fetal and pediatric populations, VGMs represent the most common intracranial vascular anomaly, accounting for 30% of all endocranial vascular malformations (1–3).
VGMs involve multiple arteriovenous shunts draining into a dilated vein called the prosencephalic vein of Markowski (MProsV), which normally disappears during embryogenesis and represents the precursor of Galen's vein. During neurogenesis, in the choroidal stage between the 6th and 11th weeks, the choroid plexus supplies the developing brain, and the MProsV represents the main draining vessel. Later, with the development of the main cortical arterials and cerebral veins, the choroidal arteries and the anterior part of the MProsV disappear, with its posterior segment forming Galen's vein. The genesis of VGAM arises from an anomaly of this process, where the anterior part of the MProsV does not disappear but enlarges due to the high pressure of the choroidal feeders, forming a vascular malformation (2–6). The diagnosis can be achieved prenatally, soon after birth (also defined as “neonatal VGM,” with early development of heart failure) or later (also defined as “infant type,” with the development of neurological signs and symptoms such as seizure, macrocephaly, and hydrocephalus).
According to the Lasjaunias classification, VGMs can be divided into choroidal type and mural type (5, 7).
The choroidal type is the most frequent and severe: multiple feeding arteries form a nidus before entering the anterior part of the MProsV. The feeders are all choroidal arteries, and due to the multiple high-flow fistulas, this type is associated with a neonatal presentation and is more prone to causing heart failure. In addition, this type represents most of the prenatally diagnosed VGMs. The mural type is characterized by single or multiple fistulas that drain directly into the wall of the MProsV. Compared to the choroidal type, the smaller number of fistulas are less prone to induce precocious cardiac failure; however, the mural type is more prone to producing a larger dilatation of the MProsV, leading to macrocephaly and hydrocephalus in infancy (7).
In this paper, we conducted a retrospective study and performed a systematic literature review. Our study aimed to investigate the role of prenatal diagnosis of VGMs, identify prenatal predictive features, and define the best prenatal and postnatal approach for the management of VGMs.
We conducted a systematic review in PubMed and EMBASE from 1 January 2003 to 31 January 2024 using the following keywords: fetal vein of Galen aneurysmal malformation, fetal VGAM, arteriovenous malformation of Galen vein, fetal Vein of Galen malformation, and prenatal diagnosis. We searched for papers describing prenatally diagnosed VGMs. Only case reports and case series were included. In total, 179 articles were selected. Data extraction from individual studies was performed in triplicate (LDM, LLM, and GS). After reading titles and abstracts and eliminating duplicates, 31 papers were selected and assessed by the authors (Figure 1). We assessed the gestational age (GA) at diagnosis, the presence of prenatal hydrocephalus, cardiomegaly, associated anomalies, the pregnancy outcomes, and birth and postnatal outcomes. In each included paper, we evaluated all variables. For each variable, we reported the total number of cases in which that variable was available; when a variable was not described, it was considered “not valuable.” All data were collected in a dedicated database and analyzed by a statistician using SPSS for Windows (version 23.0, SPSS Inc., Chicago, IL). Categorical data are presented as numbers and percentages, and continuous data are reported as mean/median and range, according to their statistical distribution.
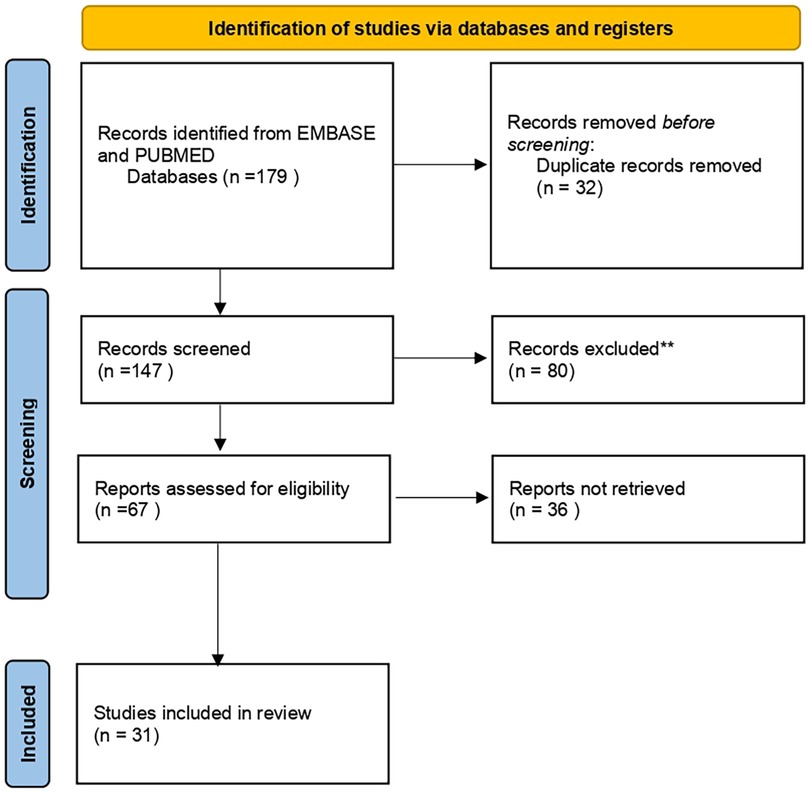
Figure 1 PRISMA chart.
Thirty-one papers reporting 51 cases were included (8–38). All pregnancies were singleton except for one twin pregnancy. Data regarding prenatal and birth outcomes are depicted in Table 1. The diagnosis was performed around the 31st week of GA (22–37). Fetal hydrocephalus was present in 39.21% (20/51), cardiomegaly in 56.86% (29/51), and fetal heart failure was present in 65.51% (19/29) of fetuses with cardiomegaly. Fetal MRI was performed in 62.79% (76/43) of cases. The associated anomalies included two cases of polyhydramnios, one case of oligohydramnios, one case of vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities (VACTERL) syndrome, one case of recurrent hydrothorax, and one case of adrenal hemorrhage. We have postnatal data for 43 VGAM cases (4 cases opted for voluntary termination of pregnancy, and no data regarding postnatal care were present in 4 cases). The median GA at birth was 38 weeks (28–41). The postnatal outcomes are depicted in Table 2. In total, 23.26% (10/43) were discharged home in stable condition, with the indication of elective embolization at 5 months. Of these, four received elective embolization: in three cases, the embolization was successful and uneventful; in one case, embolization was complicated by secondary hemorrhage, resulting in the patient developing hemiparesis. Of the 10, 1 experienced spontaneous thrombosis, 2 developed hydrocephalus and seizure at 3 months, and 1 developed hydrocephalus at 2 months, requiring urgent embolization, which resulted in a full recovery. Two of the 10 were still waiting for elective embolization. We found that 78.53% (33/42) were admitted to the neonatal intensive care unit (NICU), with the median day of admission being the first day of life (1–15). Heart failure was the main cause of NICU admission (Table 2). All these patients received cardiovascular therapy. Of these, 20 died, with their condition being too severe to perform embolization; the median day of death was 4th day. In 12 cases, urgent embolization was performed, and 7 patients survived after the procedure. In one case, embolization was not performed, and the patient survived with severe neurocognitive development delay. A ventriculoperitoneal shunt was positioned in four patients. The overall mortality was 58.14% (25/43). In the survivors’ group, 77.78% (14/18) had normal development, 11.10% (2/18) had a mild neurological disability (mild psychomotor impairment and right hemiparesis that improved after physiotherapy and occupational therapy), and 11.10% (2/18) presented with severe neurological disability. Death occurred due to heart failure and brain injury. Table 3 depicts the difference between the fetal features of VGM patients with favorable outcomes (normal or mild cognitive impairment) and those with unfavorable outcomes (exitus or severe cognitive impairment). The presence of prenatal cardiomegaly, heart failure, and hydrocephalus is associated with a poor outcome.
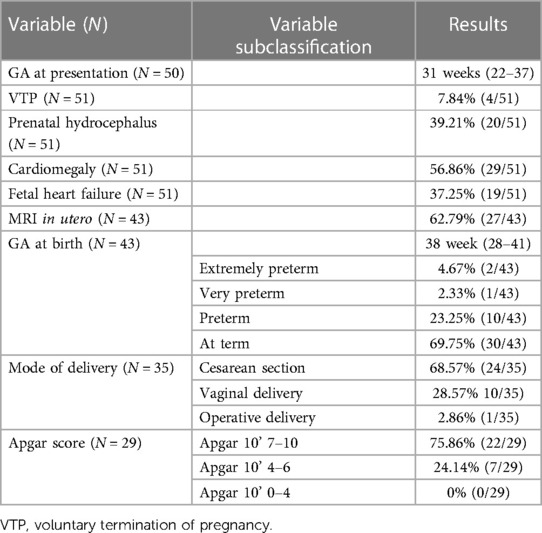
Table 1 Prenatal and birth features.

Table 2 Postnatal features.
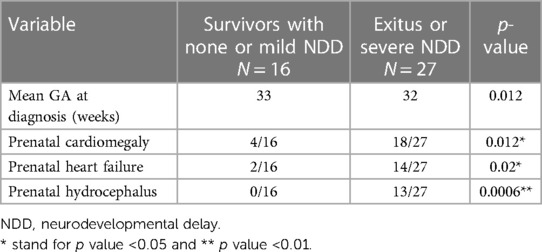
Table 3 Prenatal features in good and poor postnatal outcomes.
VGMs account for less than 1% of all intracranial vascular malformations; however, in fetal and pediatric populations, they represent the most common vascular malformation of the brain [(1, 2)]. The diagnostic process starts in fetal life, and a multidisciplinary approach is needed to diagnose and treat this condition.
The features of the VGM and its complications, mainly cardiopulmonary failure and encephalomalacia, are not the same in the fetus and in the newborn. Early diagnosis before birth has multiple benefits: the mother can receive adequate information, a specific postnatal team can be consulted prenatally, and the parents can be fully informed and able to organize postnatal care.
Prenatal diagnosis is achieved in almost 30% of cases (1). It is usually made during the third trimester. In the sagittal plane, the ultrasound appearance of a VGM is characterized by a hypoechogenic midline tubular structure localized in the posterior part of the third ventricular, described as a “comet tail” or “keyhole sign.” Doppler imaging shows turbulent arterial and venous flow (1, 18). In the coronal plane, a VGM appears as a round cystic structure. The differential diagnosis includes arachnoid cysts, porencephalic cysts, choroidal papillomas, and brain tumors; the use of color Doppler can easily help differentiate these conditions (1, 18, 19, 21, 23, 26, 29). The two most common prenatal features are fetal hydrocephalus and fetal cardiomegaly.
Hydrocephalus is present in almost 40% of cases and results either from high venous pressure, which interferes with the cerebrospinal fluid (CSF) drainage, or from the compressive effect of the malformation. In our study, the presence of prenatal hydrocephalus was associated with a poor outcome (15, 39).
Cardiomegaly is present in almost 60% of cases. The increment of the cardio thorax index is mainly due to the dilatation of the superior vena cava and the right ventricle, probably due to the high venous return from the brain (40). Cardiac involvement is less pronounced in fetal life compared to the postnatal period due to the low vascular resistance of VGMs being balanced by the low resistance of the uteroplacental unit (3, 41).
A prenatal neuroradiological, cardiological, and neonatological evaluation should be offered to explain the possible complications and postnatal management to the pregnant woman. We also advise a genetic consultation. A fetal ultrasound with fetal echocardiography should be offered at least every 2 weeks (3, 39, 40). The type of birth should be personalized for each case; in the absence of cardiological dysfunction and no other contraindications, vaginal delivery can be performed safely (1). From our review, vaginal delivery was performed in almost one-third of cases.
In previous studies, the presence of fetal cardiomegaly and ventriculomegaly were associated with poor outcomes (3, 40, 42, 43). Our prenatal data overlaps with those from previous studies; in our review, the presence of prenatal cardiomegaly, heart failure, and hydrocephalus was associated with a worse postnatal outcome, and none of the newborns discharged home with elective embolization had presented these conditions prenatally. When these features are present, we recommend delivering the newborn in a fully equipped center.
When there is a suspicion of a VGM, performing a fetal MRI should always be advised for a better study of brain anatomy and to predict the clinical outcome (17, 32, 33). The role of MRI has many clinical impacts. First, MRI can better define the VGM anatomy and its dimensions; in addition, it gives information about the presence of hydrocephalus and the development of brain parenchyma, including the presence of diffuse brain injury or hemorrhage, which may impact future clinical management. Arko et al. have shown that in fetal and postnatal MRI, the mediolateral diameter or cross-sectional area of the straight or falcine sinus at its shortest section serves as a predictor of neonatal mortality and an indication for intervention. The lesser constriction of this point was associated with neonatal-onset VGMs and thus a more severe outcome (44). Saliou et al. described how the presence of “pseudofeeders” and increased CSF volume, defined by an Evans index of >0.31, are predictive of the development of heart failure after birth and of a worse outcome. Pseudofeeders are the cortical branches of the MCA and are not choroidal arteries; they supply the brain parenchyma and are not the vessels involved in the VGM (45). The prenatal MRI features have not been included in this review due to a lack of data.
From the latest discoveries, the prenatal MRI findings, such as diffuse parenchymal brain injury or hemorrhage, dilatation of the falcine sinus at its shortest section, and the presence of pseudofeeders or an Evans index of >0.31, play a pivotal role in the decision algorithm (44–46).
At birth and during the first hours or days of life, patients with VGMs usually present in good and stable condition. However, instability can develop within hours or days, mainly due to the transition from fetal to postnatal circulation and the type of VGMs. The choroidal type tends to be diagnosed in the newborn due to its hemodynamic impact, while the mural type may be diagnosed after the neonatal period. Newborns with VGMs should be assisted or rapidly transferred to a specialized center where a neuroradiologist, neonatologist, pediatric cardiologist, and neurosurgeon are present (43).
Embolization is the main treatment for VGMs: the approach can be transarterial, transvenous, or both, but transarterial close is the most commonly used method. The transvenous approach is less effective and carries a higher risk of complications (31, 44, 47). Usually, more than one procedure is needed to achieve the occlusion of the malformation, as the amount of parenteral fluid and contrast is limited in newborns and infants (11). Various agents and devices can be used for embolization, including N-butyl cyanoacrylate (NBCA) glue, liquid embolic agents, and coils, with liquid glue being the most frequently used. The main goals of embolization are to reduce cardiovascular stress and high pressure on the brain to favor CSF drainage and allow normal brain development. The timing of embolization is governed by cardiac hemodynamics and the extent of brain involvement (11, 43, 47). Other techniques are microsurgery, radiosurgery, or a combination of several procedures (11, 31, 44, 47).
Lajaunias has proposed “The Bicetre score,” which assesses the cardiological, neurological, hepatic, renal, and respiratory function. If the score is <8, the condition is too severe for embolization; a score between 8 and 12 indicates that the patient is a candidate for urgent treatment, while a score >12 suggests elective treatment should be proposed if the patient is at least 5 months old (43, 48). This score is, however, not yet used, and there is always more focus on prenatal and postnatal predictive markers, including the presence of dilatation of the falcine sinus at its shortest section, the presence of pseudofeeders or an Evans index of >0.31, and prenatal heart failure. In addition, the presence of diffuse parenchymal brain injury or hemorrhage before the procedure, even in the absence of cardiovascular involvement, is a prognostic indicator of a poor outcome. Each case must be analyzed to decide the best approach. In our review, the outcome was negative in newborns who were not eligible for embolization; conversely, more than half of the newborns who underwent embolization survived with good odds of normal development or only mild disability (44–46).
In cases of hemodynamic and brain stability, a pediatric assessment should be performed at least every 2 weeks, with a stable assessment of head circumference, and head CT or MRI should be performed at 4, 8, 16, and 24 weeks (48). Embolization is usually performed around the 5th month (43, 48, 49). This occurs in only 20% of prenatally diagnosed VGMs.
Almost 80% of newborns with VGMs tend to present cardiac insufficiency during the first days of life, with hemodynamic instability being the main cause of death. Lowering pulmonary circle pressure and closing the patent ductus arteriosus (PDA) increase systemic vascular resistance and can trigger cardiac insufficiency. This condition arises due to the volume and pressure overload in the right chambers of the heart. Due to the low vascular resistance in the head, the majority of the ejection fraction is directed toward the brain (the steal effect of VGMs) (40). This phenomenon can cause lactic acidosis and may also cause cardiac and systemic ischemia. Pulmonary hypertension can be present, mainly due to the volume overload in pulmonary arteries (40, 50). On echocardiography, the heart appears structurally normal, but there is cardiomegaly, and the right chambers appear dilated and hypokinetic, while the left chambers are hyperdynamic. Cardiological treatment usually involves diuretics and volume restriction to reduce preload, as well as vasoactive agents, including low-dose epinephrine, dobutamine, and other inotropic agents. In particular, milrinone and levosimendan have been proposed and have shown good results (41, 50–53). A pediatric cardiologist plays a main role in VGM management, and during hospitalization, especially after the embolization, daily assessment is mandatory.
From our review, the overall mortality of prenatally diagnosed VGMs was almost 60%; however, favorable neurological development was achieved in the majority of survivors. Our results are in line with previous studies (3, 29, 42, 43, 46, 54). It is essential to follow up on the neurodevelopment of these patients by evaluating their milestones using approved tools, such as Bayley Scales of Infant or Toddler Development3rd Edition (BSID-III), and neuro-electrophysiological assessments (54).
In the genetic era, it is recommended that all VGM patients should receive a genetic evaluation.
By performing genome-wide linkage analysis, mutations in RASA1, ENG, ACVRL1, ALK1, SMAD4, and EPHB4 have been associated with genetic VGMs. A specific next generation sequencing (NGS) panel for genetic mutations associated with VGMs should be offered prenatally or after birth. Autosomal dominant mutations of RASA1 gene are responsible for almost one-third of VGM cases, followed by EPHB4, which accounts for 10% of VGM cases (2, 54–57). RASA1 encodes for RAS GTPase activating protein1, which enhances the intrinsic GTPase activity. Studies conducted on RASA1 knockout mice have demonstrated how this gene is fundamental to embryonic vessel formation. Heterozygous mutations leading to the loss of function of EPHB4 are linked to genetic non-immune hydrops fetalis in cutaneous capillary malformation-arteriovenous malformation syndrome and recently to VGM development. This is not surprising since EPHB4 is essential for venous development and differentiation (57). ALK1 is a TGF-β receptor that interacts with endoglin encoded by ENG to activate SMAD4; this is one of the main pathways for angiogenesis. Mutations in ALK1 result in type 2 hereditary hemorrhagic telangiectasia; mutations in ENG and SMAD4 result in vascular malformation (54–57).
As reported previously, the transition from fetal to postnatal circulation represents a critical point for VGM patients. To date, few case reports dealing with fetal endovascular treatment with interesting results have been published. Naggara et al. presented a case of a 31-week and 4-day fetus with a novel diagnosis of the VGM. At that time, the fetus exhibited cardiomegaly without heart failure, and the MRI performed at 34 weeks and 5 days revealed a mediolateral diameter of the dilated falcine sinus at its narrowest section measuring 10.4 mm. A transutero embolization was performed using detachable platinum coils at 33 weeks without any complications; this procedure resulted in a reduction of the cardiomegaly and the dilatation of the falcine sinus. Labor was induced at 38 weeks. However, on day 5 of life, an urgent transfemoral arterial endovascular approach was needed for acute heart failure; a second procedure was performed at 2 months of life. At 11 months, normal neural development was observed (58). Orbach et al. presented a case of ultrasound-guided percutaneous, transuterine, transcranial embolization performed on a fetus at 34 weeks and 2 days of gestation. The indication for intervention was a dilated falcine sinus associated with a 99% likelihood of neonatal decompensation. The procedure was uneventful, resulting in a 43% reduction in total cardiac output and a reduction in the caliber of the prosencephalic varix and falcine sinus. However, 2 days later, labor started following premature rupture of membranes. The neonatal outcome was good, and after 30 days, no cardiovascular support was needed (59).
Our study provides data on the prenatal main characteristics of VGMs and includes information regarding prenatal, birth, and postnatal management. To the best of our knowledge, this is the largest review conducted to date. We highlight the importance of personalized management based on neurological and cardiological status. However, our study is limited by the small sample size, primarily due to the rarity of the disease. Also, variability in equipment and medical possibilities across different studies from which the data were extracted presents another limitation. We aimed to offer gynecologists, neonatologists, cardiologists, and neuroradiologists a uniform guide for managing VGMs.
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
LDM: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. GS: Data curation, Formal Analysis, Writing – original draft. PT: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. GO: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. LM: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review & editing. LLM: Conceptualization, Data curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. CS: Supervision, Validation, Writing – original draft, Writing – review & editing. ADM: Methodology, Supervision, Writing – original draft, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
CS, LLM, and ADM are employed at Diagnositica Ecografia e Prenatale di A. Di Meglio, Naples, Italy. ADM is the Scientific Director of the center.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
VGMs, vein of Galen malformations; VGAMs, vein of Galen aneurysmal malformations; MProsV, prosencephalic vein of Markowski; GA, gestational age; NICU, neonatal intensive care unit; CSF, cerebrospinal fluid; NDD, neurodevelopmental delay.
1. Society for Maternal-Fetal Medicine, Monteagudo A. Vein of Galen aneurysmal malformation. Am J Obstet Gynecol. (2020) 223(6):B27–9. doi: 10.1016/j.ajog.2020.08.181
2. Lawton MT, Rutledge WC, Kim H, Stapf C, Whitehead KJ, Li DY, et al. Brain arteriovenous malformations. Nat Rev Dis Primers. (2015) 1:15008. doi: 10.1038/nrdp.2015.8
3. Deloison B, Chalouhi GE, Sonigo P, Zerah M, Millischer AE, Dumez Y, et al. Hidden mortality of prenatally diagnosed vein of Galen aneurysmal malformation: retrospective study and review of the literature. Ultrasound Obstet Gynecol. (2012) 40(6):652–8. doi: 10.1002/uog.11188
4. Gailloud P, O'Riordan DP, Burger I, Levrier O, Jallo G, Tamargo RJ, et al. Diagnosis and management of vein of Galen aneurysmal malformations. J Perinatol. (2005) 25(8):542–51. doi: 10.1038/sj.jp.7211349
5. Mortazavi MM, Griessenauer CJ, Foreman P, Bavarsad Shahripour R, Shoja MM, Rozzelle CJ, et al. Vein of Galen aneurysmal malformations: critical analysis of the literature with proposal of a new classification system. J Neurosurg Pediatr. (2013) 12(3):293–306. doi: 10.3171/2013.5.PEDS12587
6. Hoang S, Choudhri O, Edwards M, Guzman R. Vein of Galen malformation. Neurosurg Focus. (2009) 27(5):E8. doi: 10.3171/2009.8.FOCUS09168
7. Lasjaunias PL, Chng SM, Sachet M, Alvarez H, Rodesch G, Garcia-Monaco R. The management of vein of Galen aneurysmal malformations. Neurosurgery. (2006) 59(5 Suppl 3):S184–13. doi: 10.1227/01.NEU.0000237445.39514.16
8. Herghelegiu D, Ionescu CA, Pacu I, Bohiltea R, Herghelegiu C, Vladareanu S. Antenatal diagnosis and prognostic factors of aneurysmal malformation of the vein of Galen: a case report and literature review. Medicine. (2017) 96(30):e7483. doi: 10.1097/MD.0000000000007483
9. Li TG, Zhang YY, Nie F, Peng MJ, Li YZ, Li PL. Diagnosis of foetal vein of Galen aneurysmal malformation by ultrasound combined with magnetic resonance imaging: a case series. BMC Med Imaging. (2020) 20(1):63. doi: 10.1186/s12880-020-00463-6
10. Beucher G, Fossey C, Belloy F, Richter B, Herlicoviez M, Dreyfus M, et al. Diagnostic anténatal et prise en charge d’un anévrisme de la veine de Galien. J Gynecol Obstet Biol Reprod. (2005) 34:613–9. doi: 10.1016/S0368-2315(05)82889-3
11. Michaels AY, Sood S, Frates MC. Vein of Galen aneurysmal malformation. Ultrasound Q. (2016) 32(4):366–9. doi: 10.1097/RUQ.0000000000000222
12. Alimi A, Abbassi H, Masmoudi M, Ouazzani K, Briki R, Bibi M. VP26.09: prenatal diagnosis of a vein of Galen aneurysmal malformation. Ultrasound Obstet Gynecol. (2021) 58:208–9. doi: 10.1002/uog.24416
13. Calheiros-Trigo F, Cadilhe A, Reis J, Silva N, Pereira A. Vein of Galen malformation: prenatal diagnosis, postnatal monitoring and treatment. J Pediatr Neonat Individual Med. (2020) 9(2):e090217. doi: 10.7363/090217
14. Darji PJ, Gandhi VS, Banker H, Chaudhari H. Antenatal diagnosis of aneurysmal malformation of the vein of Galen. BMJ Case Rep. (2015). doi: 10.1136/bcr-2015-213785
15. Guil-Ibáñez JJ, García-Pérez F, Gomar-Alba M, Huete-Allut A, Narro-Donate JM, Masegosa-González J. ETV as treatment for obstructive hydrocephalus in an aneurysmal malformation of the vein of Galen in infants: case report and review of literature. Childs Nerv Syst. (2023) 39(6):1667–72. doi: 10.1007/s00381-023-05877-5
16. Bohiltea RE, Turcan N, Mihalea C, Dorobat B, Cinteza EE, Dan A, et al. Ultrasound prenatal diagnosis and emergency interventional radiologic therapy of Galen aneurysmal malformation in a newborn. Maedica (Bucur). (2016) 11(4):334–40. PMID: 28828053
17. Kośla K, Majos M, Polguj M, Antosik-Biernacka A, Stefańczyk L, Majos A. Prenatal diagnosis of a vein of Galen aneurysmal malformation with MR imaging—report of two cases. Pol J Radiol. (2013) 78(4):88–92. doi: 10.12659/PJR.889613
18. Pires P, Martins LBA, Pires NMTB, Werner H, Ferreira AC, Araujo Júnior E. Prenatal diagnosis of Galen vein aneurysm using ultrasonography and magnetic resonance imaging and perinatal and long-term neurological outcomes: a case series. Rev Bras Ginecol Obstet. (2017) 39(6):309–14. doi: 10.1055/s-0037-1601401
19. Ergenoğlu MA, Yeniel AÖ, Akdemir A, Akercan F, Karadadaş N. Role of 3D power Doppler sonography in early prenatal diagnosis of Galen vein aneurysm. J Turk Ger Gynecol Assoc. (2013) 14(3):178–81. doi: 10.5152/jtgga.2013.87847
20. Kong JC, Cheng KM, Cheung YL, Chan CM. Transarterial embolisation with Guglielmi detachable coils in an infant with a vein of Galen aneurysmal malformation. Hong Kong Med J. (2012) 18(5):435–8. PMID: 23018073
21. Mannaerts D, Muys J, Ramaekers P, Jacquemyn Y. Relapsing fetal bilateral hydrothorax, an isolated expression of a vein of Galen aneurysmal malformation. BMJ Case Rep. (2015) 2015:bcr2014208384. doi: 10.1136/bcr-2014-208384
22. Santo S, Pinto L, Clode N, Cardoso E, Marques JP, Melo A, et al. Prenatal ultrasonographic diagnosis of vein of Galen aneurysms—report of two cases. J Matern Fetal Neonatal Med. (2008) 21(3):209–11. doi: 10.1080/14767050801924357
23. Gün I, Müngen E, Kurdoğlu M, Babacan A, Muhcu M, Atay V. Is prenatal volumetric evaluation of aneurysm of the vein of Galen important in the prediction of adverse fetal outcome? J Clin Ultrasound. (2010) 38(8):443–5. doi: 10.1002/jcu.20672
24. Hartung J, Heling KS, Rake A, Zimmer C, Chaoui R. Detection of an aneurysm of the vein of Galen following signs of cardiac overload in a 22-week old fetus. Prenat Diagn. (2003) 23(11):901–3. doi: 10.1002/pd.724
25. Fayyaz A, Qureshi IA. Vein of Galen aneurysm: antenatal diagnosis: a case report. J Pak Med Assoc. (2005) 55(10):455–6. PMID: 16304858
26. Karadeniz L, Coban A, Sencer S, Has R, Ince Z, Can G. Vein of Galen aneurysmal malformation: prenatal diagnosis and early endovascular management. J Chin Med Assoc. (2011) 74(3):134–7. doi: 10.1016/j.jcma.2011.01.029
27. Firdouse M, Agarwal A, Mondal T. Vein of Galen arteriovenous malformation mimicking coarctation of the aorta. J Ultrasound. (2014) 17(4):297–301. doi: 10.1007/s40477-014-0080-y
28. Mohan R, Nayyar R, Ryder L, Lord D, Athayde N. Vein of Galen aneurysm. Australas J Ultrasound Med. (2016) 19(2):75–7. doi: 10.1002/ajum.12009
29. Sepulveda W, Vanderheyden T, Pather J, Pasquini L. Vein of Galen malformation: prenatal evaluation with three-dimensional power Doppler angiography. J Ultrasound Med. (2003) 22(12):1395–8. doi: 10.7863/jum.2003.22.12.1395
30. De Rosa G, De Carolis MP, Tempera A, Pedicelli A, Rollo M, Morena TC, et al. Outcome of neonates with vein of Galen malformation presenting with severe heart failure: a case series. Am J Perinatol. (2019) 36(2):169–75. doi: 10.1055/s-0038-1666813
31. Deepti S, Juneja R, Devarajan Sebastian LJ. Endovascular management of vein of Galen aneurysmal malformation in a neonate. Ann Pediatr Cardiol. (2018) 11(3):304–7. doi: 10.4103/apc.APC_33_18
32. Zhou LX, Dong SZ, Zhang MF. Diagnosis of vein of Galen aneurysmal malformation using fetal MRI. J Magn Reson Imaging. (2017) 46(5):1535–9. doi: 10.1002/jmri.25478
33. Wagner MW, Vaught AJ, Poretti A, Blakemore KJ, Huisman TA. Vein of Galen aneurysmal malformation: prognostic markers depicted on fetal MRI. Neuroradiol J. (2015) 28(1):72–5. doi: 10.15274/NRJ-2014-10106
34. Kütük MS, Doğanay S, Özdemir A, Görkem SB, Öztürk A. Sonographic diagnosis of fetal adrenal hemorrhage complicating a vein of Galen aneurysmal malformation. Balkan Med J. (2016) 33(1):112–4. doi: 10.5152/balkanmedj.2015.151118
35. Cordova EG, Levy P, Kheir JN, Orbach DB, Barnewolt C, Estroff JA. Vein of Galen malformation. Neoreviews. (2020) 21(10):e678–86. doi: 10.1542/neo.21-10-e678
36. Moradi B, Tahmasebpour A-R, Kazemi MA, Sharifian H, Rokni-Yazdi H. Prenatal diagnosis of concurrent facial and cerebralvascular malformation which caused congestive heart failure. Middle East Fertil Soc J. (2017) 22:343–34. doi: 10.1016/j.mefs.2017.04.006
37. Yukhayev A, Meirowitz N, Madankumar R, Timor-Tritsch IE, Monteagudo A. Uncommon second-trimester presentation of vein of Galen malformation. Ultrasound Obstet Gynecol. (2018) 51(3):421–3. doi: 10.1002/uog.17462
38. Shaikh A, Khan A, Mohsin F, Haq TU. Fetal choroid plexus arteriovenous malformation, masquerading as a neoplastic lesion. BMJ Case Rep. (2024) 17(1):e258254. doi: 10.1136/bcr-2023-258254
39. Lomachinsky V, Taborsky J, Felici G, Charvat F, Benes V III, Liby P. Endoscopic third ventriculostomy in an infant with vein of Galen aneurysmal malformation treated by endovascular occlusion: case report and a review of literature. Neurochirurgie. (2022) 68(5):540–3. doi: 10.1016/j.neuchi.2021.12.001
40. Mendez A, Codsi E, Gonzalez Barlatay F, Lapointe A, Raboisson MJ. Pulmonary hypertension associated with vein of Galen malformation. Fetal cardiac hemodynamic findings and physiological considerations. J Perinatol. (2022) 42(1):143–8. doi: 10.1038/s41372-021-01297-y
41. Madhuban A, van den Heuvel F, van Stuijvenberg M. Vein of Galen aneurysmal malformation in neonates presenting with congestive heart failure. Child Neurol Open. (2016) 3:2329048X15624704. doi: 10.1177/2329048X15624704
42. Paladini D, Deloison B, Rossi A, Chalouhi GE, Gandolfo C, Sonigo P, et al. Vein of Galen aneurysmal malformation (VGAM) in the fetus: retrospective analysis of perinatal prognostic indicators in a two-center series of 49 cases. Ultrasound Obstet Gynecol. (2017) 50(2):192–9. doi: 10.1002/uog.17224
43. McSweeney N, Brew S, Bhate S, Cox T, Roebuck DJ, Ganesan V. Management and outcome of vein of Galen malformation. Arch Dis Child. (2010) 95(11):903–9. doi: 10.1136/adc.2009.177584
44. Arko L, Lambrych M, Montaser A, Zurakowski D, Orbach DB. Fetal and neonatal MRI predictors of aggressive early clinical course in vein of Galen malformation. AJNR Am J Neuroradiol. (2020) 41(6):1105–11. doi: 10.3174/ajnr.A6585
45. Saliou G, Vraka I, Teglas JP, Senat MV, Durand P, Colmant C, et al. Pseudofeeders on fetal magnetic resonance imaging predict outcome in vein of Galen malformations [published correction appears in Ann Neurol. 2017 Jun;81(6):912. doi: 10.1002/ana.24942]. Ann Neurol. (2017) 81(2):278–86. doi: 10.1002/ana.24873
46. Buratti S, Mallamaci M, Tuo G, Severino M, Tortora D, Parodi C, et al. Vein of Galen aneurysmal malformation in newborns: a retrospective study to describe a paradigm of treatment and identify risk factors of adverse outcome in a referral center. Front Pediatr. (2023) 11:1193738. doi: 10.3389/fped.2023.1193738
47. Wagner KM, Ghali MGZ, Srinivasan VM, Lam S, Johnson J, Chen S, et al. Vein of Galen malformations: the Texas children’s hospital experience in the modern endovascular era [published correction appears in Oper Neurosurg (Hagerstown). 2022 May 1;22(5):343. doi: 10.1227/ons.0000000000000153]. Oper Neurosurg. (2019) 17(3):286–92. doi: 10.1093/ons/opy369
48. Berenstein A, Paramasivam S, Sorscher M, Molofsky W, Meila D, Ghatan S. Vein of Galen aneurysmal malformation: advances in management and endovascular treatment [published correction appears in Neurosurgery. 2018 Sep 1; 83(3):593]. Neurosurgery. (2019) 84(2):469–78. doi: 10.1093/neuros/nyy100
49. Lasjaunias P, Wuppalapati S, Alvarez H, Rodesch G, Ozanne A. Intracranial aneurysms in children aged under 15 years: review of 59 consecutive children with 75 aneurysms. Childs Nerv Syst. (2005) 21(6):437–50. doi: 10.1007/s00381-004-1125-x
50. Mathews AZ, Ibhanesebhor S, Richens T, Manjunatha CM. Heart failure in the new born; vein of Galen aneurysmal malformation. BMJ Case Rep. (2013) 2013:bcr0320126132. doi: 10.1136/bcr.03.2012.6132
51. Cory MJ, Durand P, Sillero R, Morin L, Savani R, Chalak L, et al. Vein of Galen aneurysmal malformation: rationalizing medical management of neonatal heart failure. Pediatr Res. (2023) 93(1):39–48. doi: 10.1038/s41390-022-02064-1
52. Smith A, Abruzzo T, Mahmoud M. Vein of Galen malformation and high-output cardiac failure. Anesthesiology. (2016) 125(3):597. doi: 10.1097/ALN.0000000000001095
53. Landolfo F, Giliberti P, De Rose DU, Pugnaloni F, Santisi A, Columbo C, et al. Use of levosimendan in hemodynamic management of heart failure in two neonates with intracranial arteriovenous shunts: a case series. Ital J Pediatr. (2023) 49(1):141. doi: 10.1186/s13052-023-01537-1
54. Campi F, De Rose DU, Pugnaloni F, Ronci S, Calì M, Pro S, et al. Neurodevelopmental and genetic findings in neonates with intracranial arteriovenous shunts: a case series. Front Pediatr. (2023) 11:1111527. doi: 10.3389/fped.2023.1111527
55. Duran D, Karschnia P, Gaillard JR, Karimy JK, Youngblood MW, DiLuna ML, et al. Human genetics and molecular mechanisms of vein of Galen malformation. J Neurosurg Pediatr. (2018) 21(4):367–74. doi: 10.3171/2017.9.PEDS17365
56. Chida A, Shintani M, Wakamatsu H, Tsutsumi Y, Iizuka Y, Kawaguchi N, et al. ACVRL1 gene variant in a patient with vein of Galen aneurysmal malformation. J Pediatr Genet. (2013) 2(4):181–9. doi: 10.3233/pge-13067
57. Vivanti A, Ozanne A, Grondin C, Saliou G, Quevarec L, Maurey H, et al. Loss of function mutations in EPHB4 are responsible for vein of Galen aneurysmal malformation. Brain. (2018) 141(4):979–88. doi: 10.1093/brain/awy020
58. Naggara O, Stirnemann J, Boulouis G, Orbach DB, Grévent D, James S, et al. Prenatal treatment of a vein of Galen malformation by embolization and 1-year follow-up. Am J Obstet Gynecol. (2024) 230(3):372–4. doi: 10.1016/j.ajog.2023.11.1248
Keywords: vein of Galen malformations, vein of Galen aneurysmal malformations, fetus, prenatal diagnosis, VGM, VGMs, VGAM, VGOM
Citation: Di Meglio L, Sica G, Toscano P, Orlandi G, Manzo L, Mazzarelli LL, Sica C and Di Meglio A (2024) A systematic review of prenatally diagnosed vein of Galen malformations: prenatal predictive markers and management from fetal life to childhood. Front. Pediatr. 12:1401468. doi: 10.3389/fped.2024.1401468
Received: 15 March 2024; Accepted: 3 June 2024;
Published: 3 July 2024.
Edited by:
Domenico Umberto De Rose, Bambino Gesù Children's Hospital (IRCCS), ItalyReviewed by:
Flavio Giordano, University of Florence, Italy© 2024 Di Meglio, Sica, Toscano, Orlandi, Manzo, Mazzarelli, Sica and Di Meglio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lavinia Di Meglio, bGF2aW5pYWRpbWVnbGlvQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.