 Franziska Köber1
Franziska Köber1- 1Section of Neonatology, Department of Pediatrics, University Hospital Jena, Jena, Germany
- 2Department of Obstetrics, University Hospital Jena, Jena, Germany
- 3Institute of Medical Statistics, Information Sciences and Documentation, University Hospital Jena, Jena, Germany
Background: Preterm birth and fetal growth restriction are the main determinants of perinatal mortality. In the absence of therapeutic interventions, management is restricted to the observation of fetal growth and fetoplacental perfusion to determine the timing of delivery. Fetal circulatory redistribution, known as “brain sparing,” represents a sign of fetal hypoxia and has been implemented in algorithms for when to deliver. In the absence of any other option, the nitric oxide donor pentaerythrityl tetranitrate (PETN), which has been shown to improve fetoplacental flow and reduce preterm birth in high-risk patients, is offered to patients as a personal therapy attempt. The aim of this study was to evaluate determinants related to pregnancy, including PETN intake during pregnancy, on immediate neonatal outcomes in a cohort of growth-restricted infants born before 32 completed weeks of gestation.
Methods: We performed a retrospective cohort study of 98 infants born with a birth weight below the 10th percentile before 32 completed weeks of gestation at our tertiary care center between 2010 and 2019. PETN was offered to all mothers with a history of severe adverse pregnancy outcomes who were at high risk of developing fetal growth restriction as an individual therapy attempt.
Results: The mean gestational age at birth was 188.5 days, and the mean birth weight was 549 g, corresponding to a median percentile of three. In 73 (79.3%) cases, brain sparing occurred during pregnancy. A total of 22 (22.4%) neonates were stillborn, 20 died postnatally, and 37.3% developed a severe complication. Multivariable analysis revealed birth weight percentile, gestational age at birth, and gestational age when brain sparing first occurred to be robust predictors of mortality or severe neonatal morbidity. In 39 neonates of mothers taking PETN, this impact of brain sparing was not observed.
Conclusion: Our study is the first to demonstrate a significant association between the early occurrence of brain-sparing and severe neonatal outcomes in a cohort of very early preterm, growth-restricted newborns. The data suggest that PETN intake may ameliorate the effect of brain sparing in the affected neonates.
1 Introduction
According to the World Health Organization (WHO), the global preterm birth rate remains at approximately 11%, and associated complications are responsible for an estimated 35% of the world's 3.1 million annual neonatal deaths. The WHO defines preterm birth as any birth before 37 completed weeks of gestation (1). Preterm birth can further be classified as extremely preterm before 28 completed weeks and very preterm before 32 completed weeks, while preterm birth after 32 weeks is denoted as moderate or late preterm. These subdivisions are important since decreasing gestational age is associated with increasing mortality and short-term and lifelong morbidity (2).
Immediate complications of prematurity include increased risks of neonatal respiratory conditions, such as respiratory distress syndrome, bronchopulmonary dysplasia (BPD) and pulmonary hypertension (PHT), necrotizing enterocolitis, sepsis, cerebral impairments, such as periventricular leukomalacia, intraventricular hemorrhage (IVH), cerebral palsy, and hypoxic-ischemic encephalopathy along with visual and hearing disabilities. Consequently, preterm birth has been linked to poor neurodevelopmental outcomes in childhood (3).
In addition to gestational age, birth weight, according to gestational age, is an important predictor of neonatal outcome. Infants who do not reach their genetically determined growth potential due to placental insufficiency leading to fetal growth restriction (FGR) experience significantly more complications compared to infants born at the same gestational age with an appropriate gestational weight (4). FGR is one of the most common pregnancy complications, affecting up to 10% of all pregnancies. The definition of FGR still varies between guidelines and countries. According to an international consensus published in 2016, FGR is defined as cases in which estimated fetal weight (EFW) and/or the abdominal circumference (AU) drop below the 3rd percentile or below the 10th percentile if signs of impaired fetal or placental perfusion are present. Impaired perfusion is established when the pulsatility index in the umbilical artery (UA-PI) and/or the mean PI of the two uterine arteries exceed the 95th percentile (5). FGR not only constitutes the main risk factor for stillbirth, but these infants have a fourfold risk of postnatal death and show worse neurodevelopmental outcomes with higher rates of conditions associated with prematurity, particularly respiratory distress syndrome and necrotizing enterocolitis (6). The detection of fetal brain sparing, defined as a relative increase in UA-PI and a corresponding decrease in PI in the arteria cerebri media (ACM-PI), represented as the cerebroplacental ratio (CPR), has been previously described as a predictor of perinatal outcome in late preterm fetal growth restriction (7, 8).
The nitric oxide (NO) donor pentaerythrityl tetranitrate (PETN) reduces the impedance in the uteroplacental vessels and has been shown to possess a protective effect on the maternal endothelium (9). In a randomized controlled pilot study, our group verified the beneficial effect of PETN on pregnancies, recognized by impaired uteroplacental perfusion at mid-gestation, being at risk for the development of FGR (10). In this study, the gestational age at which CPR dropped below the threshold of 1 was postponed in the PETN group (11). After the publication of our data, we offered PETN as an off-label individual therapy attempt to pregnant women with a particularly high risk of poor pregnancy outcomes due to FGR.
The aim of this study was to investigate prenatal features influencing the immediate perinatal and postnatal outcomes of infants born early, preterm, and growth-restricted. The factors analyzed included maternal demographic data, Doppler data, gestational age at birth, and birth weight, as well as the intake of PETN.
2 Patients and methods
We conducted a retrospective single-center analysis of all infants born before 32 completed weeks of gestation with a birth weight below the 10th percentile (12) at our tertiary care hospital between 1 January 2010 and 31 December 2019. We observed a total of 124 newborns. After excluding non-singleton pregnancies (n = 17), cases with severe congenital malformations (n = 7), and 2 women who participated in the ongoing randomized blinded PETN multicenter trial, 98 cases were included in our analysis. High-risk pregnancies and neonates were cared for according to German guidelines. During the study period, mothers affected by FGR were offered PETN treatment as an individual therapy attempt. A total of 39 mothers requested PETN and took 50 mg twice a day (Figure 1). Ethical approval was obtained from the Ethical Committee of our institution (2019-1565-Daten).
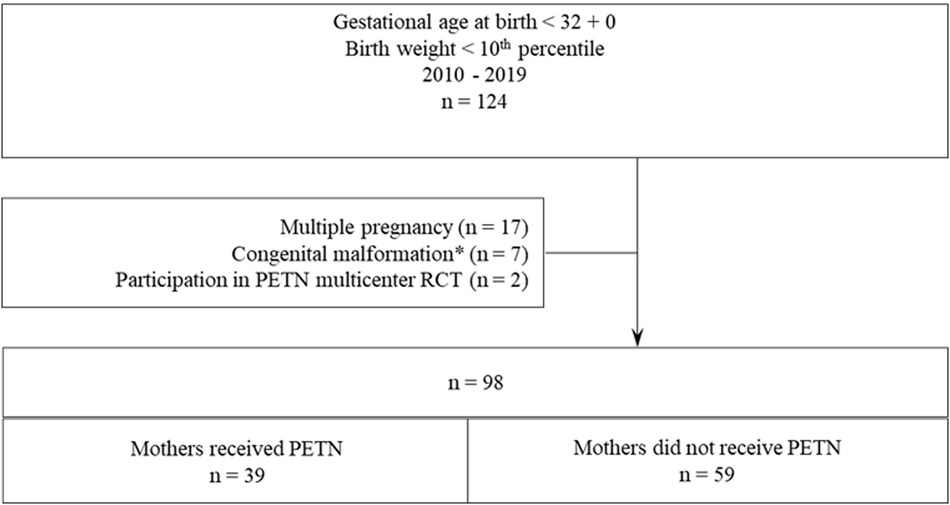
Figure 1 Cohort composition.
Outcome data were retrieved from hospital records. Fetal biometry and Doppler measurements were performed using standardized anatomic views according to international society of ultrasound in obstetrics and gynecology (ISUOG) guidelines (13). Intrauterine percentiles were calculated based on gestational age and estimated weight using the HADLOCK 1991 formula (14). Reported Doppler parameters include uterine blood flow, the CPR calculated as the ratio of the PI of the arteria cerebri media and UA-PI (15), the absence of or reverse end-diastolic flow in the umbilical arteries (AEDF and REDF), and a negative A-wave in the ductus venosus. CPR was interpreted to be pathologic at a cutoff of 1 or lower, indicating cerebral redistribution of the fetus (16).
Neonatal outcome parameters reported are gestational age at birth; birth weight and birth weight percentile; pre- and postnatal death; any death (including pre- and postnatal death); IVH (any); severe IVH (grade III or III+); PHT (any); PHT requiring NO therapy; gastrointestinal complications requiring surgery; BPD; retinopathy of prematurity (ROP); and for survivors, the length of stay in the neonatal intensive care unit (NICU).
As the main outcome measures to describe neonatal mortality and morbidity, we chose three composite parameters. “Mortality or severe neonatal morbidity” describes any death or severe neonatal morbidity, “postnatal mortality or severe neonatal morbidity” describes a postnatal death before discharge and/or the occurrence of severe neonatal morbidity, and “severe neonatal morbidity” is reported for those who were discharged alive with severe neonatal morbidity. Severe neonatal morbidity was defined as the presence of severe IVH and/or gastrointestinal complications requiring surgery and/or PHT requiring NO therapy.
Statistical analysis was performed with SPSS 26.0. Statistical significance was defined as p ≤ 0.05. Since all analyses were exploratory, no correction for multiple testing was applied. Patient characteristics were reported as medians with 25th/75th percentiles for steady variables and as numbers of cases and relative frequencies for categorical variables. A chi-square test or Fisher's exact test was applied to compare categorical variables regarding the intake of PETN. A Mann–Whitney U test was performed to compare continuous variables between these two groups. Linear regression was applied for continuous outcomes, and logistic regression analysis was applied for binary outcomes to assess the influence of different independent variables.
3 Results
Group characteristics and neonatal outcome data are presented in Table 1. Of the neonates, 22 (22.4%) were stillborn, and 20 of the 76 live-born children died in the NICU before discharge, resulting in an overall death rate of 42 (42.9%). The median gestational age at delivery was 188.5 days (range: 22 + 0 to 31 + 6 weeks), and the median birth weight was 549 g (range: 195–1,290 g). The combined outcome of “mortality or severe neonatal morbidity” occurred in 54 (55.7%) of the 98 cases. “Postnatal mortality or severe neonatal morbidity” occurred in 32 (42.7%) cases, and “severe neonatal morbidity” was reported in 28 (37.3%) cases of 76. One infant was transferred to an external hospital, and detailed information about the status is missing except that it was discharged alive (Table 1). Of the mothers, 37 (37.8%) were hypertensive during their pregnancy, of whom 18 (18.4%) developed pre-eclampsia or hemolysis, elevated liver enzymes low platelets (HELLP) syndrome. CPR dropped below the threshold of one, signifying cerebral redistribution, in 73 (79.3%) cases and showed a median of 0.62 (25th/75th percentile: 0.47/0.86) before delivery. The median gestational age when CPR dropped below the threshold of 1 was 24 weeks (25th/75th percentile: 22.5/28) (Table 1).
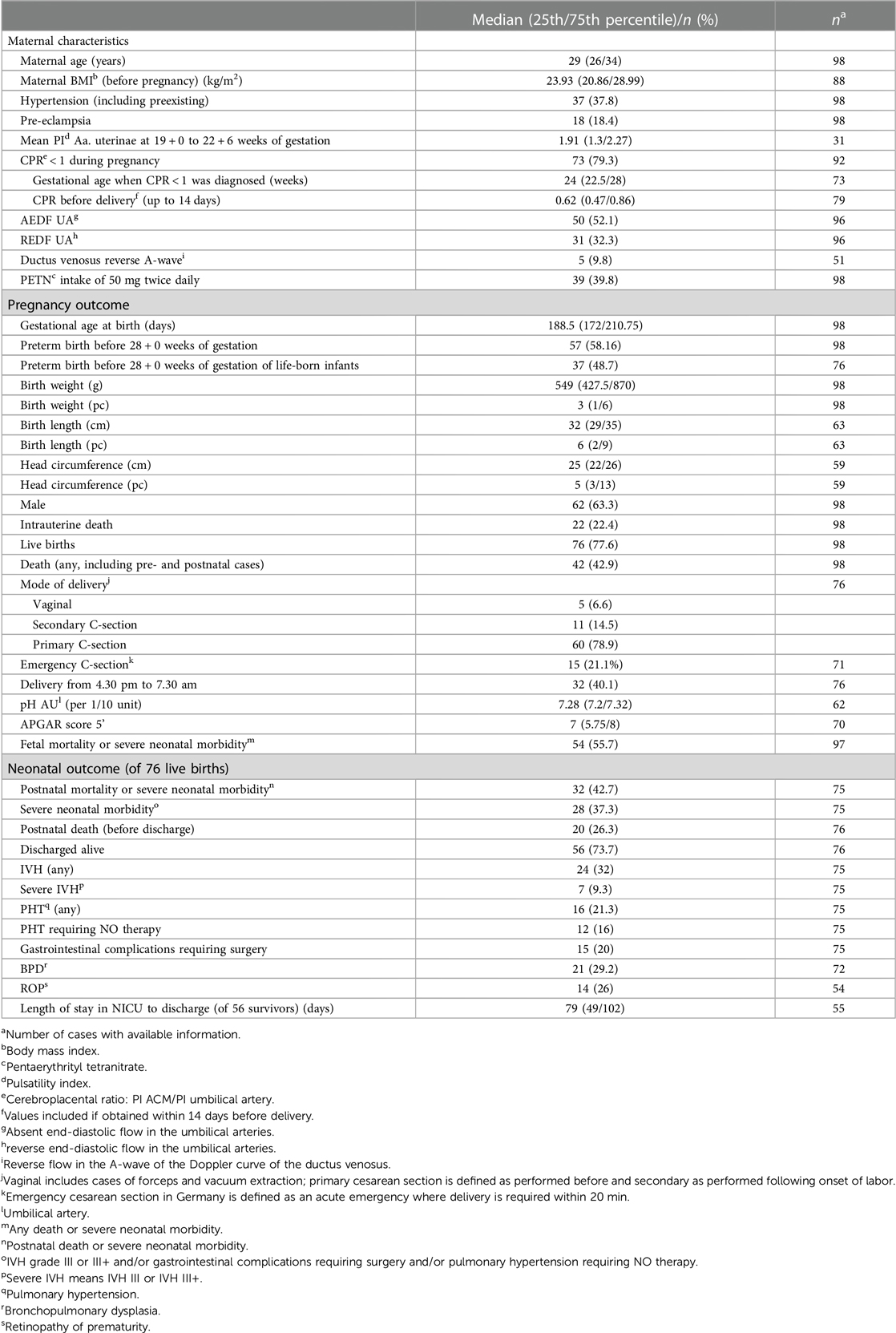
Table 1 Maternal characteristics and neonatal outcomes.
Data on a group comparison of maternal characteristics and neonatal outcome data of 39 mothers who took PETN during pregnancy and 59 who did not are presented in Table 2. Mothers receiving PETN were older [median (25th/75th percentile): 31 (28/34) vs. 28 (25/33) years; p = 0.012] and had a higher median body mass index (BMI) [24.5 (21.9/31.8) vs. 22.6 (20.3/28.0); p = 0.047]. The number of cases with placental insufficiency characterized by impaired uteroplacental perfusion detected by Doppler was significantly higher in the PETN group (Table 2). Fetal brain sparing was diagnosed in 37 (94.9%) of the 39 mothers taking PETN compared to 36 of 59 mothers (67.9%) not taking PETN (p = 0.002). The median time point at which a CPR drop below the threshold of 1 was diagnosed was 23 (21.5/25) weeks in the PETN group compared to 26 (24/28) weeks (p = 0.001), and an absent or reversed flow in the umbilical artery was observed in 48.7% of those in the PETN group compared to 21.1% (p = 0.007). The median birth weight percentile was 2 (1/4) in the PETN group compared to 4 (1/7) in the no PETN group (p = 0.037). Regarding neonatal outcome parameters, there were no significant differences reported between the two groups (Table 2).
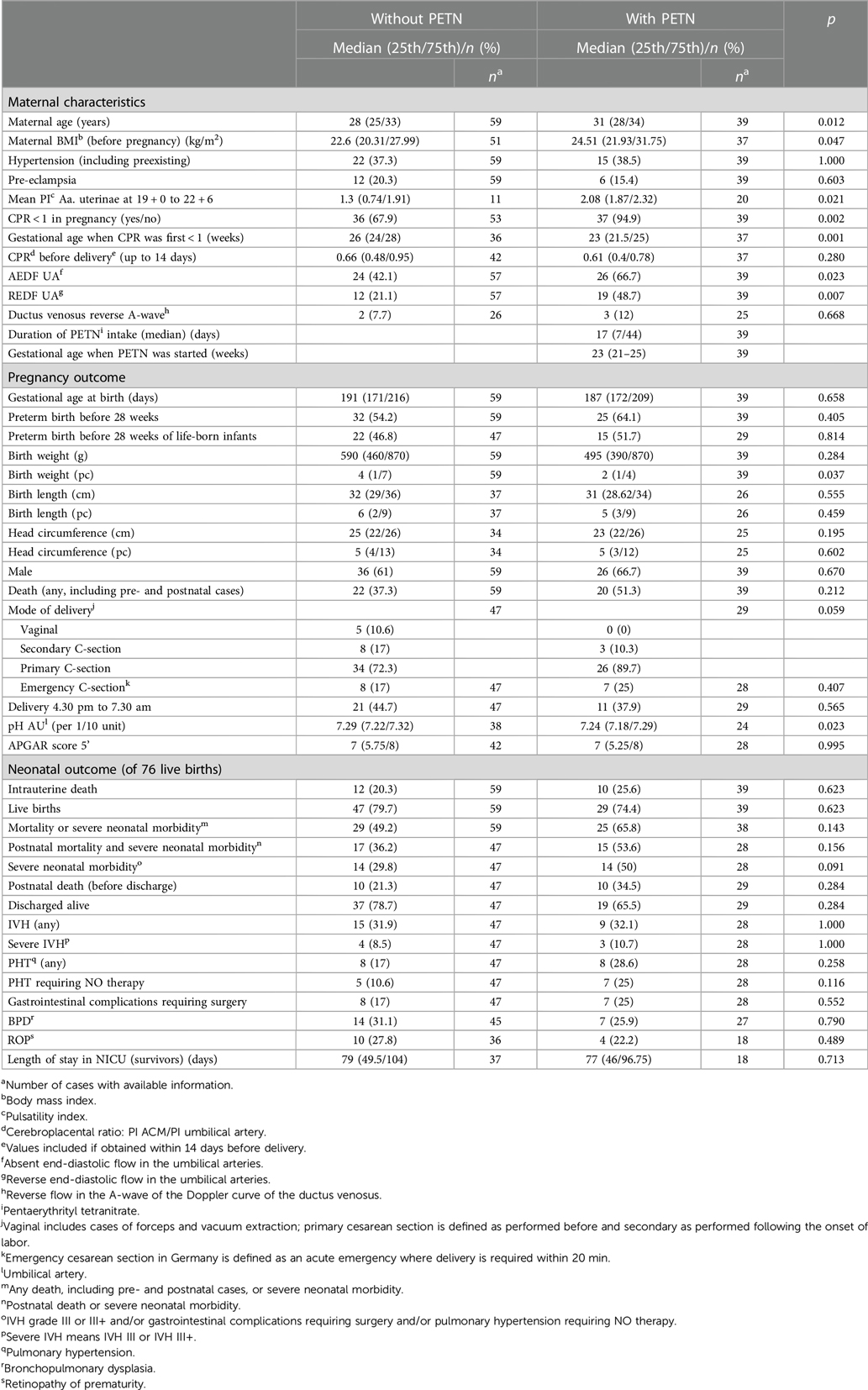
Table 2 Comparison of group characteristics according to PETN intake during pregnancy.
Using univariable analysis, we tested the influence of different risk factors on neonatal outcome parameters. Significant results are reported in Table 3. The gestational age when CPR dropped below the threshold of 1 significantly impacted all considered outcomes except IVH (Table 3).
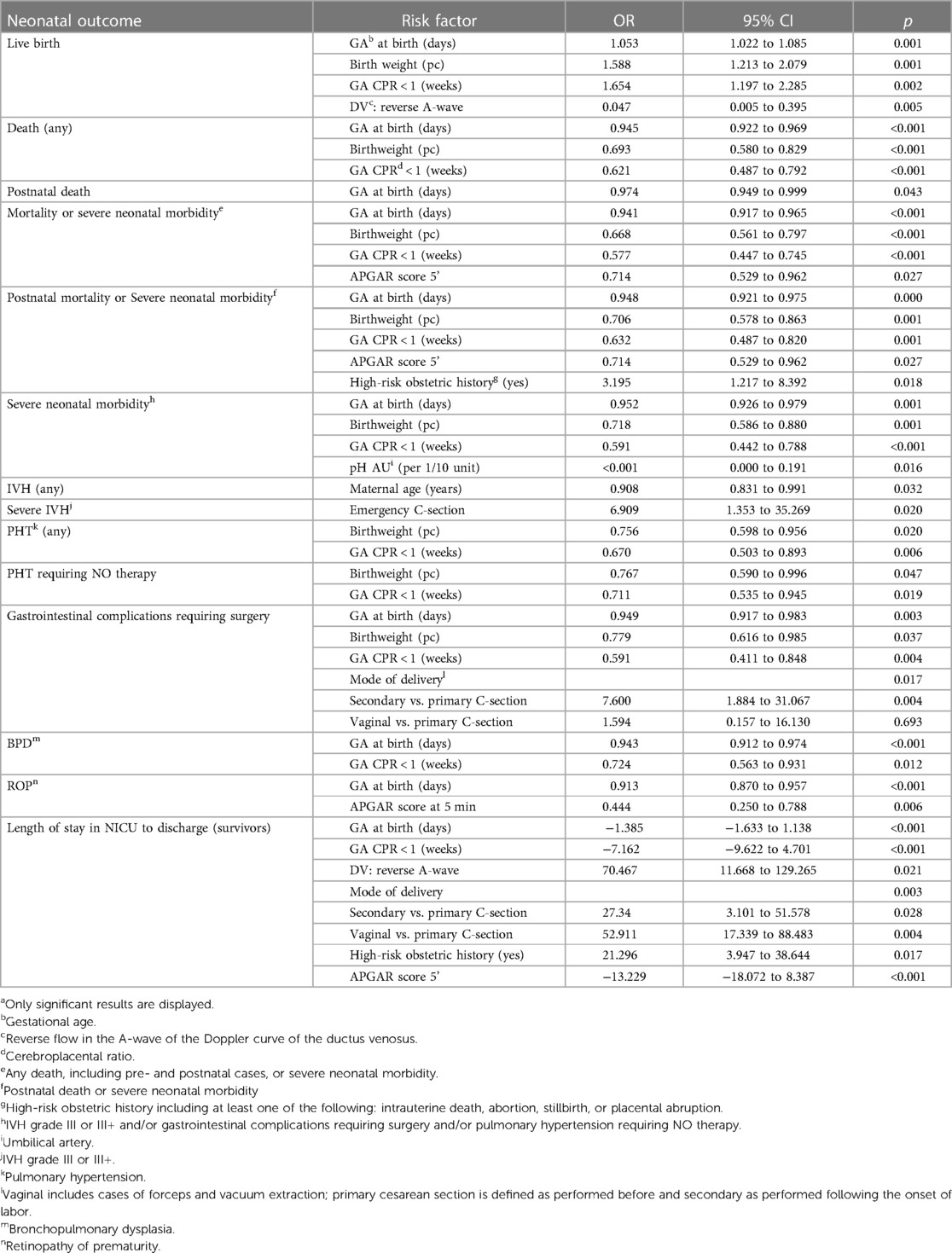
Table 3 Univariable analysis of the impact of different risk factors on neonatal outcome.a
Subsequently, we tested the impact of significant risk factors on neonatal outcomes in a multivariable analysis. Each outcome parameter was adjusted for significant risk factors identified in the univariable analysis. An additional adjustment was made for the sex of the newborn, maternal age, and BMI. Furthermore, we performed a multivariable analysis to test for the impact of PETN. The complete results are displayed in Supplementary Table S1. In Table 4 and Figure 2, we show the results for the adjusted effects of gestational age at birth, birth weight percentile, gestational age at which the drop in CPR below the threshold was detected, and PETN intake (Table 4 and Figure 2).
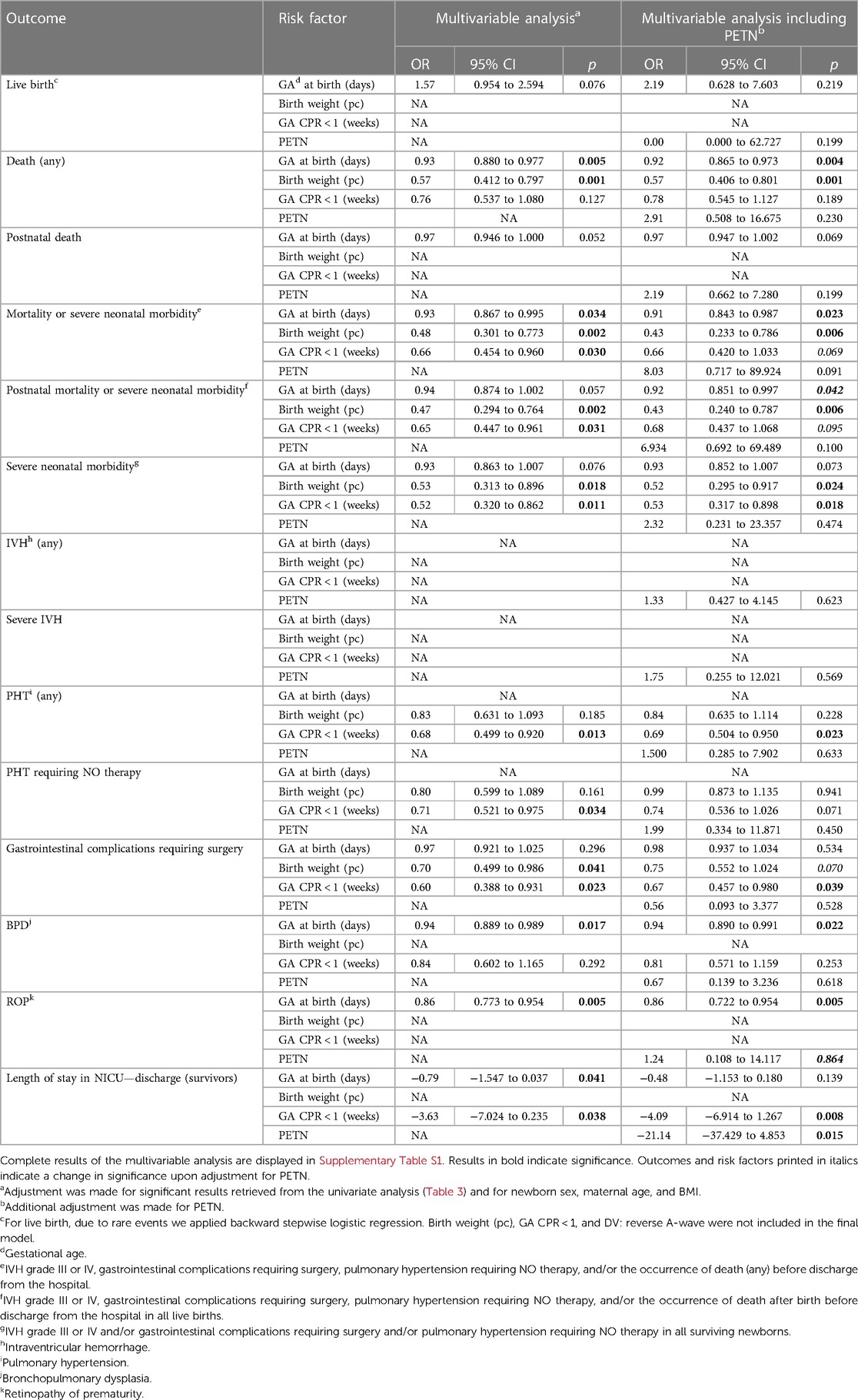
Table 4 Multivariable analysis of gestational age at birth, birth weight percentile, gestational age when CPR indicates fetal central redistribution, and PETN intake on neonatal outcome.
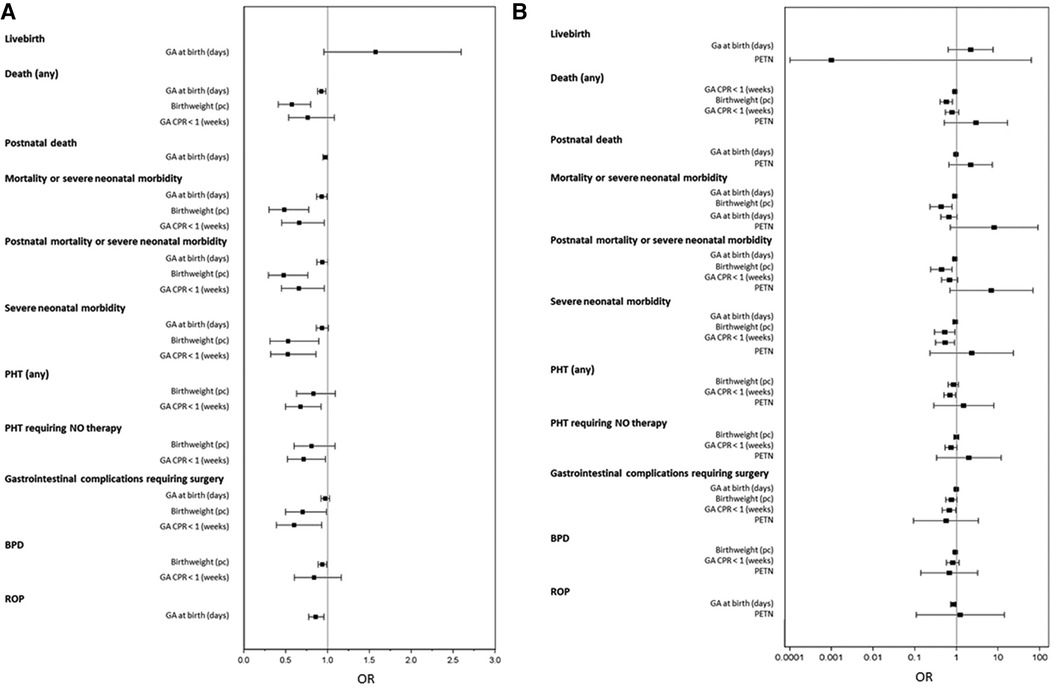
Figure 2 Forest plot of adjusted OR for neonatal outcome. (A) Adjustment was made for significantly impacting characteristics revealed from the unadjusted analysis (Table 3), for newborn sex, maternal age, and maternal BMI, and (B) additionally for PETN. Results are displayed for the characteristics such as gestational age at birth, birth weight percentile, gestational age when CPR dropped below the threshold of 1, and PETN in (B).
The multivariable analysis revealed that gestational age at birth still significantly impacted any death, “mortality or severe neonatal morbidity,” BPD, and the length of stay in the NICU. The odds of any death decreased per achieved day of pregnancy length with an odds ratio (OR) of 0.927 (95% CI: 0.880–0.977) and for the composite outcome of “mortality or severe neonatal morbidity” with an OR of 0.929 (95% CI: 0.867–0.995) (Table 4 and Figure 2).
The birth weight percentile significantly influenced any death, “mortality or severe neonatal morbidity,” “postnatal death or severe neonatal morbidity,” “severe neonatal morbidity,” and the occurrence of gastrointestinal complications requiring surgery. Per additionally gained birthweight percentile, the odds of the following was decreased: any death (OR 0.573; 95% CI: 0.412–0.797); the composite outcome of “mortality or severe neonatal morbidity” (OR 0.482; 95% CI: 0.301–0.773); “postnatal death or severe neonatal morbidity” (OR 0.474; 95% CI: 0.294–0.764); and for the surviving neonates, the odds of “severe neonatal morbidity” (OR 0.529; 95% CI: 0.313–0.896) (Table 4 and Figure 2).
Gestational age, when a drop in CPR below the threshold of 1 was first diagnosed, significantly affected all composite outcome parameters, as well as the occurrence of PHT, PHT requiring NO therapy, gastrointestinal complications requiring surgery, and the length of stay in the NICU. For each week of pregnancy gained before the drop of CPR below 1, the odds of the composite outcome “mortality or severe neonatal morbidity” was reduced (OR 0.660; 95% CI: 0.454–0.960), “postnatal death or severe neonatal morbidity” was reduced (OR 0.655; 95% CI: 0.447–0.961); and “severe neonatal morbidity” was reduced (OR 0.525; 95% CI: 0.320–0.862) (Table 4 and Figure 2).
In the multivariable analysis including PETN intake, PETN was not shown to independently impact the reported outcome parameters except for the length of stay in the NICU, which was significantly reduced by a mean of 21 days (Table 4 and Figure 2).
4 Discussion
Our data, retrieved from a retrospective cohort analysis of 98 cases of FGR neonates born early preterm, confirm the tremendous impact of both gestational age at birth and birth weight percentile on neonatal outcome. In our cohort, the odds of developing any of the chosen composite outcome parameters or of mortality was reduced by nearly 8% per prolonged day of pregnancy and nearly halved with each achieved percentile in birth weight (Table 4).
Furthermore, the early occurrence of fetal brain sparing, indicated by a drop in CPR below the threshold, significantly impacted neonatal outcomes. In our cohort, we observed a reduction in the odds of developing any of the chosen composite outcome parameters by approximately 40% with each achieved week of gestational age before brain sparing was detected. In addition, the odds of developing PHT or a PHT requiring NO therapy and gastrointestinal complications requiring surgery was reduced by 30% and 40%, respectively, with each achieved week of gestation before CPR dropping below 1 (Table 4).
Within our study cohort of 98 mothers, 39 received PETN during pregnancy. A comparison of group characteristics between mothers who received PETN and those who did not are displayed in Table 2, demonstrating that mothers who received PETN were older and had a higher BMI. Impaired fetoplacental and uteroplacental perfusion was diagnosed more frequently in the PETN cases, reflecting that PETN was given predominantly in cases with a high risk of impaired fetal development and in which alterations in fetal perfusion were detected at an earlier gestational age and were more severe (Table 2). Taking this into account, it is remarkable that no difference in neonatal outcome was observed between the groups (Table 2).
A multivariable analysis including PETN revealed that PETN intake reduced the length of stay in the NICU by approximately 21 days; however, we could not demonstrate an independent influence of PETN on the chosen composite outcome parameters. Interestingly, upon adjusting for PETN intake, gestational age when fetal brain sparing was diagnosed no longer impacted the composite outcomes of “mortality or severe neonatal morbidity” and “postnatal death or severe neonatal morbidity” and the development of any PHT (Figure 2). Although the data must be interpreted with caution, they suggest an effect of PETN, predominantly in cases of altered fetoplacental perfusion. This concurs with our results from the PETN pilot study (10). However, the number of included cases in our study is low, the study is of a retrospective nature, and the confidence intervals retrieved by the multivariable analysis are partially large (Figure 2).
The mortality rates in our cohort correlate with otherwise reported frequencies of 22.4% prenatally, 26.3% postnatally, and 42.9% for any death. In a comprehensive review of the outcome of extremely premature infants, summarizing the data from the last two decades of the last century, the authors report mortality rates in the range of 30%–50% (17). In a more recent review reporting the data of two large multicenter trials, 78% of extremely preterm-born children survived into childhood (18). Mortality rates of growth-restricted neonates born preterm can be retrieved from the STRIDER study, which included pregnant women with a growth-restricted fetus at weeks 26–30 who then received either sildenafil or placebo (19). The reported perinatal mortality was 15%–30%, which is consistent with our data (20, 21).
The risk of developing severe morbidity in early preterm infants is summarized by Glass et al. as being 63.7 for any ROP, 14.1 for severe IVH, 10.1 for surgical NEC, and approximately 40 for BPD (17), also in line with the data observed in this study (Table 1). The frequencies in the STRIDER studies, which analyzed a growth-restricted preterm cohort corresponding to our cohort, were reported to be 17% for ROP, 26% for IVH (any), 21% for NEC, and 80% for composite perinatal adverse outcomes (defined as perinatal death or neonatal morbidity) (21). The rates observed in our study were markedly lower (Table 1). This could be explained by the demonstrated impact of gestational age at birth and birth weight centile, both of which were lower in the STRIDER cohorts (19–21).
Data on infants born with very low birth weight (<1,500 g) describe frequencies in the range of 20%–25% for IVH (22). The higher incidence of 32% in our cohort can be explained by the increased IVH risk in growth-restricted neonates. The reported prevalence of PHT in preterm neonates is 23%–37% (23). In our cohort of early preterm growth-restricted neonates, the observed rates of 21% for PHT and 16% for PHT requiring NO therapy are comparably low (Table 4 and Figure 2).
In addition to the known influence of gestational age and birth weight percentile on neonatal outcome, this study revealed a profound impact of gestational age on mortality and severe neonatal morbidity when fetal brain sparing occurs (Table 4 and Figure 2). With each additional week of gestation gained before fetal brain sparing was observed, the probability of severe neonatal morbidity decreased by approximately 40% (combined outcome parameters), and of the development of PHT, or gastrointestinal complications requiring surgery, decreased by 30% and 40%, respectively (Table 4). This coincides with published data that states that as gestational age increases, the overall outcome improves. However, the impact of gestational age when fetal brain sparing was detected was still significant after the adjustment for gestational age at birth (Table 4).
Studies investigating the impact of CPR values on outcomes in growth-restricted preterm infants with gestational age at birth below 32 weeks are few. Summarizing data from 128 studies and a total of 47,748 pregnancies, CPR determined before delivery has been shown to be predictive for adverse perinatal outcomes (24). However, the study population was heterogeneous, including growth-restricted and appropriate-grown neonates and preterm birth was defined as birth before 37 weeks of gestation. The review by DeVore et al. summarized data on CPR differentiating between small for gestational age (SGA) and appropriate for gestational age (AGA) born children, as well as between early-onset SGA (before 34 weeks) and late-onset SGA (34 weeks and older) (7). The authors demonstrated that in early-onset SGA with abnormal CPR, gestational age at birth, mean birth weight, and mean birth weight centile were lower, and frequencies of cesarean delivery due to fetal distress, APGAR scores at 5 min of less than 7 points, neonatal acidosis, admission to the NICU, and perinatal death were higher (7). The PORTO study, a prospective observational study investigating a large case series of 881 growth-restricted fetuses, found a cutoff of 1.0 for CPR to be predictive of an unfavorable perinatal outcome with a specificity of 85% and a sensitivity of 66% (8). The mean gestational age at birth was 37.7 weeks, and the mean gestational age at detection of abnormal CPR was 33 weeks (25th/75th percentile: 28.7/35.9). In accordance, we set the cutoff for defining an abnormal CPR in our cohort as 1.0. However, different cutoff values and percentiles for CPR according to gestational age have been published (25). It has been discussed that gestational age-specific cutoff values are not superior to categorical cutoffs (26). Since our study includes a heterogeneous cohort and our data were retrieved over a long period, we decided to use a threshold of 1 to define pathological CPR, as this was used as the clinical cutoff during the time the study participants were managed.
Recently, a number of studies investigating CPR in term infants demonstrated a predictive value of CPR below the 5th percentile for adverse perinatal outcomes to be favorable. These data from AGA uncomplicated pregnancies demonstrate an association between a preterm drop in CPR and perinatal outcome (25, 27). It is not only the drop in CPR below the cutoff that corresponds to the perinatal outcome but also the actual. As the CPR decreases, the severity of neonatal morbidity increases (28). In a recent study presenting the secondary analysis of the PORTO trial, growth-restricted pregnancies with a CPR < 1 had a significantly increased risk of delayed neurodevelopment at 3 years of age when compared with pregnancies with abnormal UA-PI alone. These data strongly confirm our observation that fetal brain sparing predicts adverse outcomes in FGR fetuses (29). To our knowledge, there has been no study investigating the impact of the first detection of fetal brain sparing. Our results indicate that upcoming studies should emphasize this distinction.
To summarize, there is profound evidence that CPR below the threshold is associated with an adverse perinatal outcome. In our cohort, the disadvantage of being diagnosed with brain sparing was not as evident, which could be assigned to the PETN treatment, although the evidence is weak and needs to be confirmed in further studies. However, some support for this assumption can be driven by data retrieved from the PETN pilot study, demonstrating a later gestational age before CPR dropped below the threshold in the PETN cohort (11).
A strength of our study is the monocentric setting, which ensured comparable postnatal treatment in the cases evaluated. Furthermore, the data quality is good, providing complete data sets for the majority of the cases meeting the inclusion criteria. Nevertheless, our study has all the disadvantages of being a retrospective study. Moreover, the effect of PETN in pregnancies with early-onset FGR can only be of a descriptive nature, since the reasons for deciding on PETN treatment were particularly heterogeneous and PETN treatment was predominantly offered to severe cases and not to all women on a regular basis.
In conclusion, we provide data on the significant impact of not only gestational age and birth weight percentile on the immediate outcome of very preterm growth-restricted newborns but also demonstrate a significant impact of the time point at which fetal brain sparing is first diagnosed during pregnancy. This finding will enable obstetricians to further differentiate between fetuses at risk when managing pregnancies complicated by growth restrictions. PETN intake did reduce the impact of early brain sparing on postnatal death and might have the potential to mitigate adverse outcomes in severe cases of early FGR.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethical Board of Friedrich Schiller University Jena. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because this is a retrospective analysis based on hospital data resources without the involvement of individual patient data. This research is covered by the state law of Thuringia, Germany.
Author contributions
FK: Data curation, Investigation, Writing – original draft, Formal Analysis, Methodology. YH: Data curation, Formal Analysis, Methodology, Writing – review & editing. TL: Formal Analysis, Methodology, Writing – review & editing, Supervision, Validation. ES: Supervision, Writing – review & editing, Resources. HP: Resources, Supervision, Writing – review & editing, Conceptualization, Formal Analysis. TG: Conceptualization, Supervision, Writing – review & editing, Data curation, Investigation, Project administration, Validation, Writing – original draft.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank the hospital manager and all data encoders for their contributions in providing necessary information. We would also like to thank Anna Multhaup who, as a native speaker, revised the manuscript for language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1377982/full#supplementary-material
References
1. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. (2012) 379(9832):2162–72. doi: 10.1016/S0140-6736(12)60820-4
2. Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. (2012) 379(9832):2151–61. doi: 10.1016/S0140-6736(12)60560-1
3. Johnson S, Evans TA, Draper ES, Field DJ, Manktelow BN, Marlow N, et al. Neurodevelopmental outcomes following late and moderate prematurity: a population-based cohort study. Arch Dis Child Fetal Neonatal Ed. (2015) 100(4):F301–8. doi: 10.1136/archdischild-2014-307684
4. Baiao AER, de Carvalho PRN, Moreira MEL, de Sa RAM, Junior SCG. Predictors of perinatal outcome in early-onset fetal growth restriction: a study from an emerging economy country. Prenat Diagn. (2020) 40(3):373–9. doi: 10.1002/pd.5596
5. Gordijn SJ, Beune IM, Thilaganathan B, Papageorghiou A, Baschat AA, Baker PN, et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound Obstet Gynecol. (2016) 48(3):333–9. doi: 10.1002/uog.15884
6. Audette MC, Kingdom JC. Screening for fetal growth restriction and placental insufficiency. Semin Fetal Neonatal Med. (2018) 23(2):119–25. doi: 10.1016/j.siny.2017.11.004
7. DeVore GR. The importance of the cerebroplacental ratio in the evaluation of fetal well-being in SGA and AGA fetuses. Am J Obstet Gynecol. (2015) 213(1):5–15. doi: 10.1016/j.ajog.2015.05.024
8. Flood K, Unterscheider J, Daly S, Geary MP, Kennelly MM, McAuliffe FM, et al. The role of brain sparing in the prediction of adverse outcomes in intrauterine growth restriction: results of the multicenter PORTO study. Am J Obstet Gynecol. (2014) 211(3):288.e1–5. doi: 10.1016/j.ajog.2014.05.008
9. Daiber A, Wenzel P, Oelze M, Munzel T. New insights into bioactivation of organic nitrates, nitrate tolerance and cross-tolerance. Clin Res Cardiol. (2008) 97(1):12–20. doi: 10.1007/s00392-007-0588-7
10. Schleussner E, Lehmann T, Kahler C, Schneider U, Schlembach D, Groten T. Impact of the nitric oxide-donor pentaerythrityl-tetranitrate on perinatal outcome in risk pregnancies: a prospective, randomized, double-blinded trial. J Perinat Med. (2014) 42(4):507–14. doi: 10.1515/jpm-2013-0212
11. Bowkalow S, Schleussner E, Kahler C, Schneider U, Lehmann T, Groten T. Pentaerythrityltetranitrate (PETN) improves utero- and feto-placental Doppler parameters in pregnancies with impaired utero-placental perfusion in mid-gestation—a secondary analysis of the PETN-pilot trial. J Perinat Med. (2018) 46(9):1004–9. doi: 10.1515/jpm-2017-0238
12. Voigt M, Rochow N, Straube S, Briese V, Olbertz D, Jorch G. Birth weight percentile charts based on daily measurements for very preterm male and female infants at the age of 154-223 days. J Perinat Med. (2010) 38(3):289–95. doi: 10.1515/jpm.2010.031
13. Salomon LJ, Alfirevic Z, Berghella V, Bilardo C, Hernandez-Andrade E, Johnsen SL, et al. Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. (2011) 37(1):116–26. doi: 10.1002/uog.8831
14. Hadlock FP, Harrist RB, Martinez-Poyer J. In utero analysis of fetal growth: a sonographic weight standard. Radiology. (1991) 181(1):129–33. doi: 10.1148/radiology.181.1.1887021
15. Baschat AA, Gembruch U. The cerebroplacental Doppler ratio revisited. Ultrasound Obstet Gynecol. (2003) 21(2):124–7. doi: 10.1002/uog.20
16. Chainarong N, Petpichetchian C. The relationship between intrapartum cerebroplacental ratio and adverse perinatal outcomes in term fetuses. Eur J Obstet Gynecol Reprod Biol. (2018) 228:82–6. doi: 10.1016/j.ejogrb.2018.06.016
17. Glass HC, Costarino AT, Stayer SA, Brett CM, Cladis F, Davis PJ. Outcomes for extremely premature infants. Anesth Analg. (2015) 120(6):1337–51. doi: 10.1213/ANE.0000000000000705
18. Taylor GL, O’Shea TM. Extreme prematurity: risk and resiliency. Curr Probl Pediatr Adolesc Health Care. (2022) 52(2):101132. doi: 10.1016/j.cppeds.2022.101132
19. Pels A, Kenny LC, Alfirevic Z, Baker PN, von Dadelszen P, Gluud C, et al. STRIDER (Sildenafil TheRapy in dismal prognosis early onset fetal growth restriction): an international consortium of randomised placebo-controlled trials. BMC Pregnancy Childbirth. (2017) 17(1):440. doi: 10.1186/s12884-017-1594-z
20. Groom KM, McCowan LM, Mackay LK, Lee AC, Gardener G, Unterscheider J, et al. STRIDER NZAus: a multicentre randomised controlled trial of sildenafil therapy in early-onset fetal growth restriction. BJOG. (2019) 126(8):997–1006. doi: 10.1111/1471-0528.15658
21. Sharp A, Cornforth C, Jackson R, Harrold J, Turner MA, Kenny LC, et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): a multicentre, randomised, placebo-controlled, double-blind trial. Lancet Child Adolesc Health. (2018) 2(2):93–102. doi: 10.1016/S2352-4642(17)30173-6
22. Valdez Sandoval P, Hernandez Rosales P, Quinones Hernandez DG, Chavana Naranjo EA, Garcia Navarro V. Intraventricular hemorrhage and posthemorrhagic hydrocephalus in preterm infants: diagnosis, classification, and treatment options. Childs Nerv Syst. (2019) 35(6):917–27. doi: 10.1007/s00381-019-04127-x
23. Weismann CG, Asnes JD, Bazzy-Asaad A, Tolomeo C, Ehrenkranz RA, Bizzarro MJ. Pulmonary hypertension in preterm infants: results of a prospective screening program. J Perinatol. (2017) 37(5):572–7. doi: 10.1038/jp.2016.255
24. Vollgraff Heidweiller-Schreurs CA, De Boer MA, Heymans MW, Schoonmade LJ, Bossuyt PMM, Mol BWJ, et al. Prognostic accuracy of cerebroplacental ratio and middle cerebral artery Doppler for adverse perinatal outcome: systematic review and meta-analysis. Ultrasound Obstet Gynecol. (2018) 51(3):313–22. doi: 10.1002/uog.18809
25. Kalafat E, Khalil A. Clinical significance of cerebroplacental ratio. Curr Opin Obstet Gynecol. (2018) 30(6):344–54. doi: 10.1097/GCO.0000000000000490
26. Odibo AO, Riddick C, Pare E, Stamilio DM, Macones GA. Cerebroplacental Doppler ratio and adverse perinatal outcomes in intrauterine growth restriction: evaluating the impact of using gestational age-specific reference values. J Ultrasound Med. (2005) 24(9):1223–8. doi: 10.7863/jum.2005.24.9.1223
27. Moreira RS, Magalhaes LC, Alves CR. Effect of preterm birth on motor development, behavior, and school performance of school-age children: a systematic review. J Pediatr (Rio J). (2014) 90(2):119–34. doi: 10.1016/j.jped.2013.05.010
28. Meher S, Hernandez-Andrade E, Basheer SN, Lees C. Impact of cerebral redistribution on neurodevelopmental outcome in small-for-gestational-age or growth-restricted babies: a systematic review. Ultrasound Obstet Gynecol. (2015) 46(4):398–404. doi: 10.1002/uog.14818
29. Monteith C, Flood K, Pinnamaneni R, Levine TA, Alderdice FA, Unterscheider J, et al. An abnormal cerebroplacental ratio (CPR) is predictive of early childhood delayed neurodevelopment in the setting of fetal growth restriction. Am J Obstet Gynecol. (2019) 221(3):273.e1–e9. doi: 10.1016/j.ajog.2019.06.026
Keywords: fetal growth restriction, preterm birth, very low birth weight, very preterm birth, brain sparing, pentaerythrityl tetranitrate (PETN)
Citation: Köber F, Heimann Y, Lehmann T, Schleußner E, Proquitté H and Groten T (2024) Gestational age at birth, birth weight, and gestational age when intrauterine brain sparing occurs determines the neonatal outcome in growth-restricted infants born before 32 weeks of gestation: a retrospective cohort analysis. Front. Pediatr. 12:1377982. doi: 10.3389/fped.2024.1377982
Received: 28 January 2024; Accepted: 3 June 2024;
Published: 4 July 2024.
Edited by:
Jonathan Michael Davis, Tufts University, United StatesReviewed by:
Gabriela Corina Zaharie, University of Medicine and Pharmacy Iuliu Hatieganu, RomaniaMichael Zujkowski, Tufts Medical Center, United States
© 2024 Köber, Heimann, Lehmann, Schleußner, Proquitté and Groten. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tanja Groten, tanja.groten@med.uni-jena.de