 Rémy Assathiany
Rémy Assathiany Marc Sznajder1
Marc Sznajder1 Fabienne Cahn-Sellem
Fabienne Cahn-Sellem- 1Association Française de Pédiatrie Ambulatoire (AFPA), Ancenis, France
- 2MPedia, Bordeaux, France
Background: Bronchiolitis is a respiratory infection of viral origin and is often linked to syncytial respiratory virus. It is the most frequent cause of hospitalisation in children aged under 2 years and sometimes requires transfer to intensive care. Infectious complications may also arise in the short term, and longer-term progression towards asthma is also possible. The occurrence of bronchiolitis in children may affect families in different ways, and may have psychological, organisational, employment-related, and possibly financial consequences.
Objective: The aim of the study was to determine the familial and socioeconomic repercussions of bronchiolitis in infants.
Setting: Parents with a child with bronchiolitis between January 2021 and May 2022, who were registered at the site of the Association Française de Pédiatrie Ambulatoire (Mpedia site) or at the site of the Malin Programme, which serves families experiencing financial difficulties, were included in the study.
Participants: All parents consenting to participate in the study.
Results: A total of 2,059 valid questionnaires were retrieved: 1,318 (64%) were obtained from parents through the Mpedia website and 741 (36%) were obtained through the Malin Programme. Parents associated with the Malin Programme had more children, as well as higher rates of unemployment and financial difficulties, and required greater medical assistance. Hospitalisation was necessary in 37% of cases and was comparable between groups. During the illness, moderate to severe anxiety was present in 73% of parents; this percentage rose to 87% if the child required hospitalisation. Many parents reported effects on daily home (84%) and work life (90%), and 60% had taken a leave of absence from work.
Conclusion: Beyond the immediate or longer-term medical consequences of bronchiolitis in infants, the illness affects families in multiple ways and can lead to anxiety, as well as changes in day-to-day home and work life. Physicians should have greater awareness of these consequences and should strive to decrease their impact.
Introduction
Bronchiolitis, a viral illness that leads to obstruction of the bronchioles, infects infants aged under 2 years during epidemics that occur during the fall and winter months. Respiratory syncytial virus (RSV) is the virus most often responsible for this condition. In an annual cohort, the number of infants affected by bronchiolitis has been estimated to be 20%, thus indicating that it is the major cause of hospitalisation in infants aged under 1 year in developed countries. Each year, 2%–3% of infants, particularly younger infants, are hospitalised for bronchiolitis (1) for an average of 5.1 days (2). Transfer to intensive care, mainly for oxygen administration, is required for 1%–2% of hospitalised infants (3). Mortality rates associated with bronchiolitis are high in developing countries but are almost nil in North America and Europe (4). Literature data examining trends in the numbers of infants hospitalised for bronchiolitis and the number transferred to intensive care are conflicting. In England, the number of infants hospitalised for bronchiolitis grew by a factor of 7 between 1979 and 2011 (5), whereas this number was stable in Ontario between 2004 and 2018 (6), and even decreased in the United States between 2000 and 2016 (7). Those studies have also reported that the number of infants transferred to intensive care was either stable (5) or increased (6, 7). In Europe, the number of cases has also increased in the past 20 years (8). In France, during the winter of 2020–2021, 39% of children presenting with bronchiolitis in a hospital emergency department were hospitalised (9).
The progression of this very common illness is marked by immediate or longer-term medical complications. Among immediate complications, superinfection should be noted, as well as acute middle-ear infection, which occurs in 57% of children aged under 3 years (10). Acute pyelonephritis is much less common, but the possibility of its occurrence should be systematically examined in infants with high fever (11). Among later-onset complications, infants who contract bronchiolitis in the first 6 months of life have an elevated probability of occurrence of acute middle-ear infection, pneumonia, and infections requiring antibiotic treatment between the ages of 6 and 12 months (12). Later development of asthma is frequent, particularly if a rhinovirus is responsible for the bronchiolitis (13); the mechanism, which remains under discussion, appears to involve environmental or genetic factors (14), among which individual and/or familial atopic tendencies appear to play a determining role (15).
Beyond these medical complications, hospitalisation of an infant is a stressful event for any family and can have profound consequences for both parents and siblings. These consequences may be psychological in nature, arising from the stress of hospitalisation, or may involve changes in the family's employment, financial, and daily life situations. These non-medical effects of bronchiolitis are scarcely documented.
The aim of the present study was to evaluate the familial and socioeconomic consequences of the occurrence of bronchiolitis within family units.
Materials and methods
We did not use the questionnaire from a prior study, because it was complex and pertained to only hospitalised infants (16). Instead, we developed a questionnaire consisting of closed-ended questions, which was validated by the Association Française de Pédiatrie Ambulatoire (AFPA) committee of experts. The questionnaire included questions regarding how the illness was managed, as well as its psychological, organisational, and work-related consequences on the families. Information relating to family socioeconomic status was also requested.
The criterion for inclusion was the occurrence of bronchiolitis in an infant aged under 2 years between January 2021 and the date of administration of the questionnaire (April–May 2022). The data were collected using SurveyMonkey® software (SurveyMonkey Inc.).
The anonymous questionnaire was administered in April and May 2022 to 9,300 parent's registered with the parent website of the AFPA (www.mpedia.fr). The questionnaire was also made available on social networks (i.e., Facebook and Instagram). To counterbalance the over-representation of higher socioeconomic categories among families registered at the AFPA website, the questionnaire was also distributed to all 47,146 families registered with the Malin Programme. The Malin Programme is a non-profit recognised association within the scope of the French law of 1901; it aims to give parents, particularly those under tight budgetary constraints, advice from pregnancy onwards; this advice comes from French paediatric health societies and concerns nutrition, breastfeeding, sleep, screens, and physical activity. All families can register on the website (programme malin.fr); financial assistance may be granted for families in precarious situations, which are defined by the agency responsible for child allowances according to the ratio of family income to family size.
Parents who completed the questionnaire on the Mpedia website were denoted Mpedia families or parents, whereas those belonging to the Malin Programme were denoted Malin Programme families or parents. All questionnaires, including those with partial responses, were considered.
The study was approved by the AFPA ethics committee.
Statistical analyses
The only data analysed were categorical in nature and are presented as frequencies and proportions. The results were compared between groups (Mpedia vs. Malin Programme) using Fisher's exact test. The level of significance was set to 0.05. Statistical analyses were conducted using GraphPad QuickCalcs software.
Results
A total of 2,059 questionnaires were partially or fully valid: 1,318 (64%) were obtained from the parents on the Mpedia website and 741 (36%) were obtained from parents participating in the Malin Programme. Responses were obtained from all French departments except five (Creuse, Gers, Lozère, Nièvre, and Yonne), and the largest number of responses was received from the Gironde. A large proportion of questionnaires was completed by mothers (94%) aged over 25 years (95%).
Family characteristics
Table 1 presents the characteristics of the families from the two groups. Parents from the Malin Programme were characterised by younger maternal age, less frequent rates of cohabitation as couples (83% vs. 99%; p < 0.0001), and more children. Moreover, higher rates of unemployment were observed among these parents (58% vs. 13%; p < 0.0001). In terms of employment categories, parents in the Mpedia group were mainly managers and professionals (43% vs. 6%; p < 0.0001). Families who were part of the Malin Programme had higher rates of financial difficulty (47% vs. 10%; p < 0.0001) and had greater recourse to medical assistance programs (33% vs. 3%; p < 0.0001) such as Couverture Maladie Universelle (CMU) or Aide Médicale de l'Etat (AME).
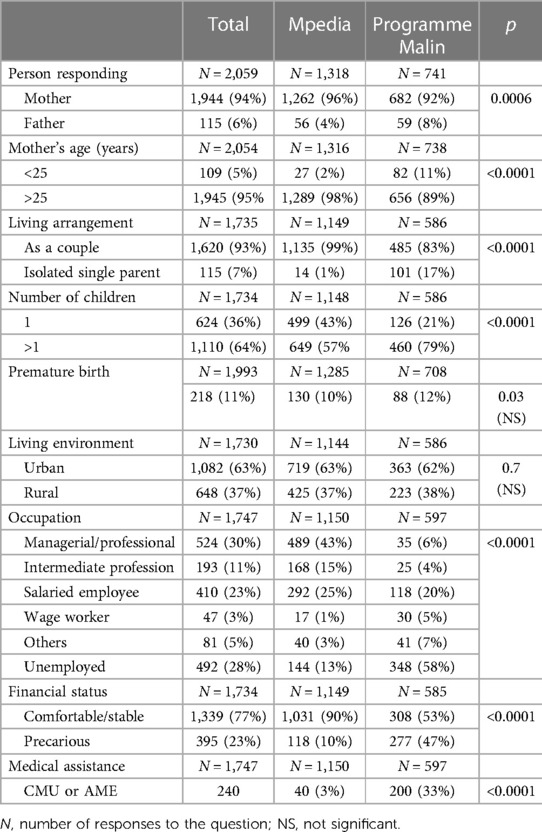
Table 1 Family characteristics.
Management of bronchiolitis
Because of missing or incomplete data, 1,993 files concerning the management of bronchiolitis were usable. Table 2 details how the occurrence of bronchiolitis was managed. The number of medical consultations varied, and 58% of the infants had two or more consultations. Hospitalisation was necessary in 37% of cases, typically for more than 3 days; this percentage was comparable between groups. In total, 75 (10%) infants required a transfer to another hospital, most often in another city. The distribution of transfers in the same city versus another city was significantly different in the two groups: they were more prevalent among Malin Programme families (4% vs. 0%; p < 0.0048). Transfer to intensive care was required in 144 cases, which amounted to 7% of the total number of bronchiolitis cases studied.
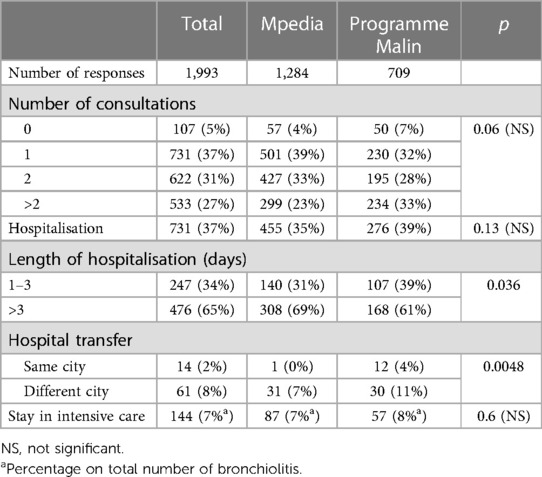
Table 2 Management of bronchiolitis.
Consequences of illness among families
The consequences of a child's illness on the family were manifold and varied (Table 3). Moderate to severe anxiety was reported by 73% of parents after the initial diagnosis, and higher rates of anxiety were reported as the illness progressed (82%), particularly in cases requiring hospitalisation (87%). The effects on daily life were considerable and were reported by 84% of parents. Changes in childcare arrangements were reported by 20% of families, more often in the Mpedia group (23% vs. 15%; p = 0.0004).
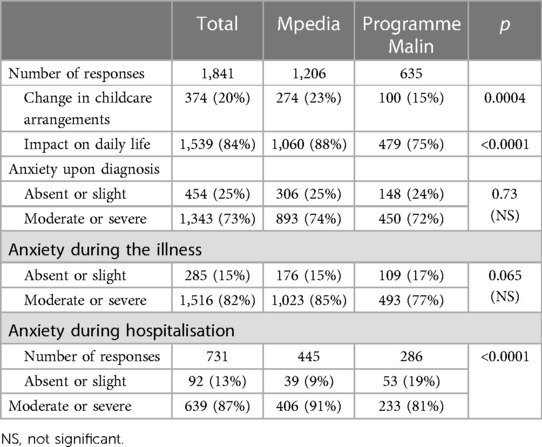
Table 3 Familial impact of bronchiolitis.
Employment-related consequences of illness
Approximately 90% of parents reported that the child's illness had affected the quality of their work (Table 4). Almost two-thirds (60%) of parents took a leave of absence because of the child's illness, and 13% were absent from work for more than 5 days.
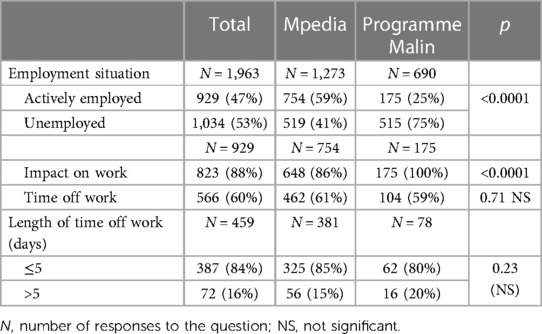
Table 4 Impact on work during bronchiolitis.
Discussion
This study involving more than 2,000 families allowed us to evaluate the effects of the occurrence of bronchiolitis on families. In this study, the questionnaires were completed primarily by mothers, as previously reported (17). A total of 37% of infants with bronchiolitis were hospitalised, findings comparable to those of Santé Publique France, in which 39% of such infants were hospitalised after presenting to the emergency department in the 2020–2021 winter (9). The hospitalisation rate was comparable in the two sub-populations studied, whereas in the United States, it was higher in families in a precarious socio-economic situation (18, 19).
The non-medical consequences observed in families were manifold and varied, and affected not only family life and organisation, but also parental work life. Anxiety is reported by three-quarters of parents responding to the survey; such anxiety when confronted with an illness involving respiratory distress, is legitimate and understandable; it would be even stronger in the case of bronchiolitis than in the case of infant hospitalisation for other reasons (20); this is understandable, as seeing his child struggling to breathe is very stressful for a parent. In our study, anxiety is more important in the Mpedia parents; indeed, it seems that the most qualified employees and managers are most at risk for anxiety symptoms (21); a previous study of parents of children hospitalized for bronchiolitis has also shown that this type of anxiety is proportional to the parents' number of years of education (17). Paradoxically, in this last study, higher levels of anxiety were not observed in cases in which the hospitalised infants had been born prematurely or experienced congenital cardiopathy, although these conditions are risk factors for hospitalisation in bronchiolitis (17). Good relationships with caregivers whom parents can trust is an important factor in relieving anxiety in this situation (22). Even if parents' anxiety attenuates over time, they may continue to experience difficulties several months after hospitalisation; thus, quality of life can be diminished for as many as 9 months after the occurrence of bronchiolitis (17, 20), particularly if atopic dermatitis is associated (23).
In our study, taking a leave of absence from work, which enabled parents to be present at the sick child's bedside, was reported by 60% of the families participating in the questionnaire. In the Malin Programme study sample, only 25% of parents were employed when the child was diagnosed with bronchiolitis, and all reported that the illness had affected their work.
The frequency at which parents took time off work for a child's bronchiolitis (60%) was comparable to findings from a Finnish study reporting that 52% of parents were absent from work for an average of 2.6 days; notably, taking time off work was more prevalent among parents of the youngest children (10). Another research study focusing on Spain and Italy has reported that 60% of parents took more than 1 week off work (22). Moreover, a study in Canada has observed that both parents spent an equivalent of 7 days at the hospital, thus amounting to a 3-day absence from work for each parent (2).
It is probably not easy to focus on your work when your child is hospitalised; this may affect the quality of the work performed. Thus, almost all parents (88%) who continued their daily activities during the child's illness indicated that the quality of their work had declined; a comparable frequency (82%) has been found in a Canadian study (2). Moderate to severe effects on work quality have also been reported by 37% of parents in a European study (22).
These complications must be considered by medical and paramedical personnel to help families successfully navigate this period of anxiety, which also affects home and work lives.
The present study has some limitations. First, we performed a retrospective analysis in which parents were questioned about the child's illness, which could have occurred as many as 17 months earlier. This aspect of the design could have led to recollection bias, although the occurrence of bronchiolitis in an infant is certainly a major event for any family. Moreover, additional statistical analyses, such as regression analyses, were not performed for this study; further analysis is needed in future studies to determine the true associations between the socioeconomic status of a family and the familial impacts of bronchiolitis.
The high occurrence rate of bronchiolitis, which affects 30% of infants each winter (8), justifies the development of a preventive vaccine to curb more severe forms of bronchiolitis and limit transmission. A vaccine could also decrease medical and non-medical complications of bronchiolitis, as well as the number of antibiotic prescriptions, as have been observed after the development of the influenza vaccine (24). RSV infection was previously preventable only in severely premature babies and certain other at-risk children (e.g., those with severe cardiopathy or immunodeficiency) by administering monoclonal antibodies (palivizumab), but administration had to be repeated every month during the period of community RSV infection risk. In 2020, 38 candidate vaccines were under development by the pharmaceutical industry, 19 of which were undergoing clinical trials (25). Two recent studies have shown encouraging results. The first involves a vaccine administered to pregnant women, which provides early protection for infants, and has shown good tolerance and satisfactory transplacental passage of protective antibodies (26). The second uses a long-lasting monoclonal antibody (nirsevimab) that can be injected once into an infant and has been demonstrated to effectively prevent RSV infections (27). This vaccine was certified by the European Commission in November 2022 and has been available in France since September 2023 to all infants aged under 1 year.
Conclusion
This study, based on a sample of more than 2,000 families, highlights the importance of the psychological, familial, and socioeconomic effects of infant RSV infections on families. These consequences may sometimes be minimised or misunderstood by caregivers. Although these consequences were observed in both sub-populations studied, their importance varied. In the Mpedia group, anxiety during the illness—particularly during hospitalisation if required—was more frequent, whereas parents in the Malin Programme group reported more profound effects on work life. A complementary sociological study could define these differences more precisely and deepen understanding of this issue.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
RA: Conceptualization, Writing – original draft, Writing – review & editing. MS: Methodology, Software, Writing – review & editing. FC-S: Conceptualization, Investigation, Supervision, Writing – review & editing. CD: Conceptualization, Investigation, Writing – original draft. AW: Methodology, Conceptualization, Writing – review & editing, Supervision.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
Investigations were supported financially by Sanofi.
Conflict of interest
This study was commissioned by the Sanofi laboratory to AFPA R&D.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hasegawa K, Tsugawa Y, Brown DFM, Mansbach JM, Camargo CA. Trends in bronchiolitis hospitalizations in the United States, 2000–2009. Pediatrics. (2013) 132:28–36. doi: 10.1542/peds.2012-3877
2. Mitchell I, Defoy I, Grubb E. Burden of respiratory syncytial virus hospitalizations in Canada. Can Respir J. (2017):1–9. doi: 10.1155/2017/4521302
3. Barben J, Regamey N, Hammer J. Bronchiolite aiguë—une mise à jour. Forum Méd Suisse—Swiss Med Forum (2020). Available online at: https://doi.emh.ch/fms.2020.08460 (accessed October 5, 2023).
4. Nair H, Nokes DJ, Gessner BD, Dherani M, Madhi SA, Singleton RJ, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. (2010) 375:1545–55. doi: 10.1016/S0140-6736(10)60206-1
5. Green CA, Yeates D, Goldacre A, Sande C, Parslow RC, McShane P, et al. Admission to hospital for bronchiolitis in England: trends over five decades, geographical variation and association with perinatal characteristics and subsequent asthma. Arch Dis Child. (2016) 101:140–6. doi: 10.1136/archdischild-2015-308723
6. Mahant S, Parkin PC, Thavam T, Imsirovic H, Tuna M, Knight B, et al. Rates in bronchiolitis hospitalization, intensive care unit use, mortality, and costs from 2004 to 2018. JAMA Pediatr. (2022) 176:1–11. doi: 10.1001/jamapediatrics.2021.5177
7. Fujiogi M, Goto T, Yasunaga H, Fujishiro J, Mansbach JM, Camargo CA, et al. Trends in bronchiolitis hospitalizations in the United States: 2000–2016. Pediatrics. (2019) 144:e20192614. doi: 10.1542/peds.2019-2614
8. Linssen RS, Teirlinck AC, van Boven M, Biarent D, Stona L, Amigoni A, et al. Increasing burden of viral bronchiolitis in the pediatric intensive care unit: an observational study. J Crit Care. (2022) 68:165–8. doi: 10.1016/j.jcrc.2021.07.009
9. Bronchiolite: Bilan de la surveillance hivernale 2020–2021 (2023). Available online at: https://www.santepubliquefrance.fr/les-actualites/2021/bronchiolite-bilan-de-la-surveillance-hivernale-2020-2021 (accessed October 5, 2023).
10. Heikkinen T, Ojala E, Waris M. Clinical and socioeconomic burden of respiratory syncytial virus infection in children. J Infect Dis. (2017) 215:17–23. doi: 10.1093/infdis/jiw475
11. Swaminathan A, Hom J. Do febrile infants aged 60–90 days with bronchiolitis require a septic evaluation? Ann Emerg Med. (2012) 60:605–6. doi: 10.1016/j.annemergmed.2012.02.014
12. Abreo A, Wu P, Donovan BM, Ding T, Gebretsadik T, Huang X, et al. Infant respiratory syncytial virus bronchiolitis and subsequent risk of pneumonia, otitis media, and antibiotic utilization. Clin Infect Dis. (2020) 71:211–4. doi: 10.1093/cid/ciz1033
13. Makrinioti H, Hasegawa K, Lakoumentas J, Xepapadaki P, Tsolia M, Castro-Rodriguez JA, et al. The role of respiratory syncytial virus- and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma—a systematic review and meta-analysis. Pediatr Allergy Immunol. (2022) 33(3):e13741. doi: 10.1111/pai.13741
14. Jartti T, Gern JE. Role of viral infections in the development and exacerbation of asthma in children. J Allergy Clin Immunol. (2017) 140:895–906. doi: 10.1016/j.jaci.2017.08.003
15. Sznajder M, Stheneur C, Albonico V, Dib S, Cau D, Chevallier B, et al. Respiratory development of 5- to 6-year-old children experiencing a first bronchiolitis episode before age one. Eur Ann Allergy Clin Immunol. (2005) 37:392–6. PMID: 1652890316528903
16. Lapillonne A, Regnault A, Gournay V, Gouyon JB, Benmedjahed K, Anghelescu D, et al. Development of a questionnaire to assess the impact on parents of their infant’s bronchiolitis hospitalization. BMC Health Serv Res. (2013) 13:272. doi: 10.1186/1472-6963-13-272
17. Lapillonne A, Regnault A, Gournay V, Gouyon JB, Gilet H, Anghelescu D, et al. Impact on parents of bronchiolitis hospitalization of full-term, preterm, and congenital heart disease infants. BMC Pediatr. (2012) 12:171. doi: 10.1186/1471-2431-12-171
18. McLaurin KK, Farr AM, Wade SW, Diakun DR, Stewart DL. Respiratory syncytial virus hospitalization outcomes and costs of full-term and preterm infants. J Perinatol. (2016) 36:990–6. doi: 10.1038/jp.2016.113
19. Inagaki K, Blackshear C, Burns PA, Hobbs CV. Racial/ethnic disparities in the incidences of bronchiolitis requiring hospitalization. Clin Infect Dis. (2021) 72:668–74. doi: 10.1093/cid/ciaa113
20. Leidy NK, Margolis MK, Marcin JP, Flynn JA, Frankel LR, Johnson S, et al. The impact of severe respiratory syncytial virus on the child, caregiver, and family during hospitalization and recovery. Pediatrics. (2005) 115:1536–46. doi: 10.1542/peds.2004-1149
21. Murcia M, Chastang JF, Cohidon C, Niedhammer I, Samotrace Study Group. Contribution of occupational factors to social inequalities in self-reported health among French employees. Int Arch Occup Environ Health. (2013) 86(5):541–52. doi: 10.1007/s00420-012-0784-2
22. Carbonell-Estrany X, Dall’Agnola A, Fullarton JR, Rodgers-Gray BS, Girardi E, Mussa A, et al. Interaction between healthcare professionals and parents is a key determinant of parental distress during childhood hospitalisation for respiratory syncytial virus infection [European RSV Outcomes Study (EROS)]. Acta Paediatr. (2018) 107:854–60. doi: 10.1111/apa.14224
23. Rolfsjord LB, Skjerven HO, Bakkeheim E, Carlsen K, Hunderi JOG, Kvenshagen BK, et al. Children hospitalised with bronchiolitis in the first year of life have a lower quality of life nine months later. Acta Paediatr. (2015) 104:53–8. doi: 10.1111/apa.12792
24. Younas M, Royer J, Winders HR, Weissman SB, Bookstaver PB, Ann Justo J, et al. Temporal association between influenza vaccination coverage and ambulatory antibiotic use in children. Pediatr Infect Dis J. (2022) 41:600–2.35363650
25. Mejias A, Rodríguez-Fernández R, Oliva S, Peeples ME, Ramilo O. The journey to a respiratory syncytial virus vaccine. Ann Allergy Asthma Immunol. (2020) 125:36–46. doi: 10.1016/j.anai.2020.03.017
26. Simões EAF, Center KJ, Tita ATN, Swanson KA, Radley D, Houghton J, et al. Prefusion F protein-based respiratory syncytial virus immunization in pregnancy. N Engl J Med. (2022) 386:1615–26. doi: 10.1056/NEJMoa2106062
Keywords: bronchiolitis, RSV, epidemic, family, family life, familial impact
Citation: Assathiany R, Sznajder M, Cahn-Sellem F, Dolard C and Werner A (2024) Effects of infant bronchiolitis on family life. Front. Pediatr. 12:1343045. doi: 10.3389/fped.2024.1343045
Received: 22 November 2023; Accepted: 29 April 2024;
Published: 19 June 2024.
Edited by:
Stephen Aronoff, Temple University, United StatesReviewed by:
Shaili Amatya, Penn State Hershey Children's Hospital, United StatesPéter Altorjai, European Academy of Paediatrics (EAP), Belgium
© 2024 Assathiany, Sznajder, Cahn-Sellem, Dolard and Werner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rémy Assathiany, YXNzYXRoaWFueUB3YW5hZG9vLmZy