
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 12 February 2024
Sec. Neonatology
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1221863
This article is part of the Research TopicArtificial Intelligence and Machine Learning in NeonatologyView all 5 articles
 Alvaro G. Moreira1*
Alvaro G. Moreira1* Ameena Husain2,†Lindsey A. Knake3,†
Ameena Husain2,†Lindsey A. Knake3,† Khyzer Aziz4,†
Khyzer Aziz4,† Kelsey Simek2,†Charles T. Valadie1Nisha Reddy Pandillapalli1Vanessa Trivino1James S Barry5
Kelsey Simek2,†Charles T. Valadie1Nisha Reddy Pandillapalli1Vanessa Trivino1James S Barry5  for Neonatal Machine learning INnovations Development Intelligence (NeoMIND-AI)
for Neonatal Machine learning INnovations Development Intelligence (NeoMIND-AI)
Bronchopulmonary dysplasia (BPD) is a complex, multifactorial lung disease affecting preterm neonates that can result in long-term pulmonary and non-pulmonary complications. Current therapies mainly focus on symptom management after the development of BPD, indicating a need for innovative approaches to predict and identify neonates who would benefit most from targeted or earlier interventions. Clinical informatics, a subfield of biomedical informatics, is transforming healthcare by integrating computational methods with patient data to improve patient outcomes. The application of clinical informatics to develop and enhance clinical therapies for BPD presents opportunities by leveraging electronic health record data, applying machine learning algorithms, and implementing clinical decision support systems. This review highlights the current barriers and the future potential of clinical informatics in identifying clinically relevant BPD phenotypes and developing clinical decision support tools to improve the management of extremely preterm neonates developing or with established BPD. However, the full potential of clinical informatics in advancing our understanding of BPD with the goal of improving patient outcomes cannot be achieved unless we address current challenges such as data collection, storage, privacy, and inherent data bias.
Bronchopulmonary dysplasia (BPD) is a chronic lung disease affecting extremely preterm neonates, characterized by disruptions in the development of the alveolar and vascular compartments leading to long-term pulmonary complications (1–3). Despite significant progress in neonatal care, the incidence of BPD has remained relatively unchanged, particularly with the increasing survival rates of extremely preterm neonates. To put this problem into perspective, it is essential to note that BPD represents a substantial burden on both healthcare systems (e.g., up to $442,468 per neonate in the first year of life) and affected families (4). The financial healthcare costs associated with managing BPD, coupled with the emotional and physical toll it takes on families, underscore the urgency of addressing this condition.
Interestingly, some studies have suggested that the incidence of BPD may be decreasing among moderately preterm infants, possibly due to improved respiratory support techniques, antenatal steroids, and surfactant replacement therapy (5). However, this positive trend might not hold true for extremely preterm infants. This evolving scenario underscores the importance of innovative approaches as current therapies (e.g., oxygen, bronchodilators, and glucocorticoids) have limited benefits apart from symptom management. There is a critical need not only for newer, more effective therapies for BPD but also for approaches that may predict and potentially identify neonates who would benefit most from targeted or earlier interventions (6–8). By diligently tracking these trends and facilitating personalized care strategies for infants at risk of BPD, we can better navigate the complex dynamics of BPD incidence and improve both the prevention and management of this challenging condition.
Clinical informatics, a rapidly expanding field in biomedical informatics, is transforming healthcare by integrating computational methods with patient data to improve outcomes [(9–11), Figure 1]. This approach has demonstrated significant success in various areas of healthcare. For instance, clinical informatics has played a pivotal role in advancing cancer care, where it facilitates precision medicine by tailoring treatments based on genetic and clinical data, ultimately leading to more effective therapies and improved patient outcomes (12–14). In the realm of critical care medicine, clinical informatics has led to enhanced patient monitoring systems, predictive analytics for the early detection of deteriorating conditions, and streamlined communication among healthcare teams, resulting in better patient management and reduced mortality rates (15–17).

Figure 1. Schematic demonstrating disciplines and applications of clinical informatics.
Within neonatal care, clinical informatics has made substantial contributions as well. Two notable examples include retinopathy of prematurity (ROP) screening and neonatal intensive care unit (NICU) workflow optimization. Clinical informatics has been instrumental in developing algorithms that analyze retinal images to identify preterm infants at risk of ROP. By automating this process, clinicians can make quicker and more accurate decisions about when to initiate treatment, preventing vision loss in vulnerable neonates (18–20). Clinical informatics tools have also been employed to optimize workflows in the NICU. These tools assist in managing patient data, monitoring vital signs, and coordinating care among healthcare professionals. Such optimization not only improves the quality of care but also reduces the burden on healthcare providers (21–24). These examples illustrate how clinical informatics is revolutionizing healthcare by harnessing data-driven approaches to enhance patient outcomes across a wide range of medical specialties.
In terms of BPD, clinical informatics presents new and exciting opportunities to enhance clinical therapy. For example, leveraging electronic health records (EHRs) or continuous vital sign data to capture nuanced ventilator or physiologic data can aid in identifying patients for targeted approaches. Machine learning algorithms can also analyze EHRs to identify complex patterns that may predict or subclassify BPD or provide prognostic measures for long-term respiratory outcomes [e.g., need for home oxygen, tracheostomy (25–28)]. Beyond EHRs, mobile health and clinical decision support systems are additional clinical informatics tools that can benefit neonates with BPD.
This review highlights the innovative potential of clinical informatics in improving the management of BPD, specifically in predicting extubation success, identifying clinically relevant phenotypes, and developing clinical decision support tools. While these informatics tools offer a promising avenue to provide clinicians with more accurate and timely information, several challenges need to be addressed. It is important to note that one significant hurdle is the collection of data from multiple institutions. Collaborative efforts to aggregate data from various healthcare facilities can enhance the generalizability of clinical and research findings, enabling a broader understanding of BPD. Additionally, the need for ethical and secure storage of data generated by EHRs poses a critical challenge. Ensuring patient privacy and data security is paramount in clinical informatics, especially when dealing with sensitive neonatal information. By proactively addressing these challenges, clinical informatics can play a pivotal role in advancing our understanding of BPD in neonates and improving patient outcomes. The collaboration among institutions and the implementation of robust data security measures are crucial steps toward harnessing the full potential of informatics tools in enhancing neonatal care for BPD.
The limited advances in the treatment and prevention of BPD can be attributed to several interconnected factors within the field of neonatal care. Firstly, the multifactorial nature of BPD, which involves genetic predisposition, developmental lung immaturity, and various environmental factors, makes it a complex and challenging condition to address comprehensively (29–31). These intricate interactions have hindered the development of targeted therapies, as the underlying mechanisms of BPD remain incompletely understood.
Secondly, the lack of effective interventions to modify the natural course of BPD in its early stages has contributed to the stagnation in therapeutic progress (32). Current treatment options primarily focus on managing symptoms and providing respiratory support, but there is a significant gap in therapies that can halt or reverse the disease progression. This limitation is compounded by the vulnerability of extremely preterm neonates, who often face multiple health challenges beyond BPD, making it challenging to prioritize research efforts in this specific area.
Moreover, conducting clinical trials and research involving neonates, especially extremely preterm infants, presents ethical and logistical challenges (33). The need to balance the potential benefits of experimental treatments with the vulnerability of this patient population has led to cautious and conservative approaches in clinical research. As a result, the development and testing of novel therapeutic strategies for BPD have been slow-paced.
The financial burden associated with neonatal care, particularly the management of BPD, has also played a role in the limited advances in this field (34). Healthcare systems are often strained by the high costs of caring for extremely preterm infants, diverting resources away from research and innovation. This financial constraint has hindered the pursuit of new therapeutic avenues for BPD.
In summary, the relatively slow progress in treating and preventing BPD can be attributed to the complexity of the condition, the lack of effective interventions, ethical considerations in neonatal research, and financial constraints on healthcare systems. Addressing these challenges will be crucial in advancing our understanding of BPD and developing more effective therapies for affected neonates.
Clinical informatics plays a pivotal role in healthcare by integrating advanced computational methods with patient data to improve patient outcomes and enhance the overall quality of care. This rapidly evolving field harnesses the power of data analysis, EHRs, machine learning, and artificial intelligence (AI) to transform healthcare delivery across various medical specialties. This paradigm shift toward data-driven decision-making has proven particularly effective in oncology, where precision medicine and personalized treatment plans are revolutionizing cancer care.
In cancer treatment, clinical informatics has emerged as a game-changer. By analyzing vast datasets encompassing genetic, genomic, and clinical information, healthcare providers can tailor treatments to the specific genetic and molecular characteristics of a patient's cancer. This approach, known as precision oncology, has led to the development of targeted therapies that are more effective and less toxic than traditional chemotherapy. For example, drugs like Herceptin (trastuzumab) have been successful in treating breast cancer patients with HER2-positive tumors (35).
Furthermore, clinical informatics aids in the identification of novel therapeutic targets and the prediction of treatment responses. Through the analysis of genomic data, researchers can pinpoint genetic mutations that drive cancer growth and progression. This knowledge enables the development of new drugs and treatment strategies that directly target these mutations, such as the use of tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia (CML) (36).
Additionally, clinical informatics facilitates the management of large patient data within oncology departments and research institutions. EHRs help streamline the recording and retrieval of patient information, ensuring that healthcare providers have access to up-to-date and comprehensive data and protocols to make informed decisions. This not only improves patient care but also aids in research by providing a wealth of structured data for retrospective analyses and future clinical trials (37). In summary, clinical informatics is reshaping the landscape of healthcare, with cancer treatment serving as a prime example of its transformative potential. By leveraging data-driven insights, precision medicine, and streamlined data management, clinical informatics is improving patient outcomes and transforming the way healthcare is delivered.
Neonatal nutrition is a critical aspect of the care of premature infants, who often require specialized feeding plans. Clinical informatics has helped optimize the nutritional support provided to these vulnerable neonates. EHRs enable healthcare providers to monitor and track the nutritional intake of neonates accurately. These systems allow for the precise recording of feeding volumes, nutritional supplements, growth curves, and caloric intake. By analyzing this data, healthcare teams can tailor nutrition plans to meet the specific needs of each neonate, ensuring they receive adequate nourishment to support growth and development (38). Through data analysis, informatics tools can identify trends in neonatal growth and nutritional status. If a neonate's growth trajectory deviates from the expected, the system can generate alerts, prompting healthcare providers to assess and adjust the nutrition plan accordingly. This proactive approach helps prevent undernutrition and its associated complications in neonates (39, 40).
Another practical example of clinical informatics in neonatology involves neonatal infection control, a significant concern when caring for premature infants. EHRs play a central role in tracking and monitoring neonatal infections. These systems allow healthcare providers to record and analyze data related to infection risk factors, microbiology results, antibiotic usage, and infection outcomes (41). Informatics tools can automatically generate alerts when certain infection risk factors are identified, such as prolonged antibiotic use or central line-associated bloodstream infections (CLABSIs). These alerts prompt healthcare teams to take real-time action, such as adjusting antibiotic regimens or implementing infection control measures. Additionally, informatics systems facilitate the timely retrieval of microbiology results, aiding clinicians in diagnosing and treating infections promptly (42).
Furthermore, clinical informatics supports the surveillance and reporting of neonatal infection rates. By aggregating and analyzing infection data from multiple NICUs, informatics tools enable healthcare professionals to identify trends, outbreaks, and areas for improvement in infection control practices. This data-driven approach helps NICUs implement evidence-based strategies to reduce infection rates and improve neonatal outcomes (43). The Kaiser Permanente sepsis calculator, which has now been implemented in some EHRs, has also helped clinicians calculate risk (44).
Clinical informatics has demonstrated its transformative potential in various healthcare domains, making it prudent to explore its role in BPD prevention and treatment.
Clinical informatics is fundamentally data-driven, harnessing the power of EHRs, computational methods, and artificial intelligence to derive meaningful insights from a vast array of data. In the case of BPD, the substantial amount of data available in neonatal care can be leveraged to gain a deeper understanding of the condition. This method can elucidate hidden patterns, identify risk factors, and inform evidence-based interventions, potentially modernizing our approach to BPD (45).
BPD is not a uniform condition, and neonates exhibit considerable variability in their response to treatments and outcomes. Clinical informatics offers the promise of personalized medicine tailored to the unique needs of each neonate. By analyzing patient-specific data, including genetic markers, clinical history, and physiological parameters, informatics tools can help clinicians predict which neonates are at the highest risk of developing severe BPD and tailor interventions accordingly. This personalized approach aligns with the growing trend in medicine toward precision care and could lead to more effective treatments for BPD (46, 47).
Clinical informatics enables the systematic monitoring of trends and outcomes over time. This capability is invaluable in the context of BPD, where understanding the evolving landscape of the condition is critical. By analyzing large-scale data from multiple neonatal care units, informatics tools can help researchers and clinicians identify shifts in BPD incidence, potentially pinpoint areas with rising prevalence, and assess the effectiveness of various interventions. Such insights can guide healthcare policies and resource allocation, ultimately improving BPD prevention and management strategies (48–50).
In neonatal care, where rapid interventions can be life-saving, informatics tools can provide clinicians with timely information and decision-support algorithms. For example, predictive models integrated into EHRs can help identify neonates at a high risk of developing severe BPD, prompting clinicians to implement preventive measures or consider alternative treatment strategies. This proactive approach can potentially reduce the severity of BPD, improve long-term outcomes for affected neonates, and reduce healthcare costs (51, 52).
In conclusion, exploring the role of clinical informatics in BPD prevention and treatment is a promising avenue that aligns with the evolving landscape of healthcare. Leveraging data-driven insights, personalizing care, tracking trends, and providing clinical decision support can improve how we approach BPD (Figure 2). The subsequent sections of this review paper will delve deeper into the specific applications and advancements in clinical informatics for BPD, including definitions, phenotyping, prediction models, and interventions, contributing to the ongoing goal of mitigating the impact of BPD on premature infants.
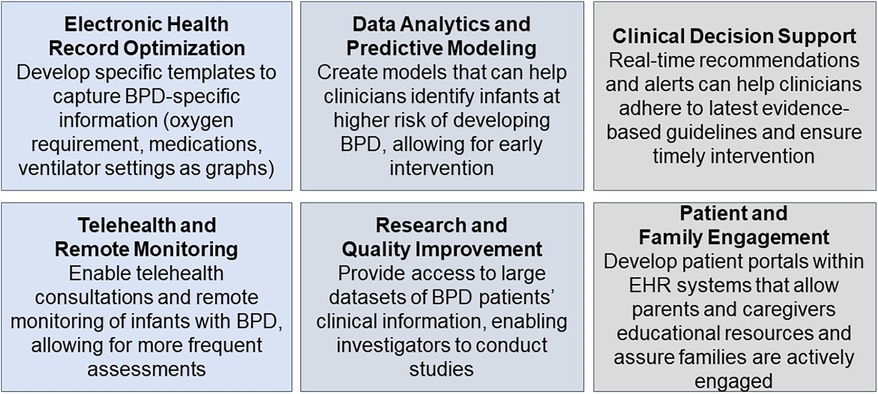
Figure 2. Application of clinical informatics for BPD.
BPD is a heterogeneous condition in terms of its pathophysiology, clinical presentation, and treatment response. Hence, there is a compelling rationale for categorizing BPD patients into distinct subgroups or phenotypes based on their unique clinical and molecular profiles. Phenotypes are artificial constructs consisting of observable characteristics or traits of disease (53). Traditionally, BPD severity has been classified based on the requirement for oxygen therapy or positive pressure ventilation at 28 days and/or 36 weeks postmenstrual age (3, 54). However, these approaches fail to capture the heterogeneity of the disease and its underlying mechanisms.
Clinical phenotyping offers an alternative strategy for optimizing therapeutic interventions and refining risk stratification, mirroring the successful subcategorization of conditions like asthma based on clinical presentation. This approach enables more precise guidance for tailored therapies (55). The intricate interplay of prenatal risk factors, including but not limited to pregnancy-induced maternal hypertension, intrauterine growth restriction, genetic predisposition, chorioamnionitis, and other causes of fetal systemic inflammation, creates a dynamic landscape that influences the future clinical phenotype of a neonate (56, 57). These factors, combined with postnatal influences such as prematurity, birth weight, oxidative stress, mechanical ventilation, sepsis, the presence of a clinically significant patent ductus arteriosus, and respiratory microbial dysbiosis, contribute not only to the development of BPD but also shape the challenges clinicians must address. This interplay informs the need for tailored interventions to meet the unique needs of each neonate (58).
An approach to classifying BPD based on phenotypes holds considerable clinical implications, such as clinical trial recruitment, retrospective cohort analysis, outcome studies, and cost analyses (5, 6). Recent studies have applied clustering techniques to describe BPD phenotypes based on various clinical and molecular features. In a study of 76 neonates with severe BPD, Wu et al. stratified phenotypic presentations according to 1) moderate-severe parenchymal lung disease, 2) pulmonary hypertension, and 3) large airway disease (59). The authors defined parenchymal lung disease by scoring severity via chest tomography with angiography. Specifically, the criteria assessed the existence and intensity of ten distinct lung radiographic attributes, employing a scale that spans from 0 to 2. The attributes include hyper-expansion, mosaic attenuation pattern, intercostal bulging, air cysts, bullae, blebs, cyst size, triangular subpleural opacities, distortion and thickening of bronchovascular bundle, consolidation, and a subjective assessment of overall lung disease severity. Pulmonary hypertension was defined by having one or more of the following: a systolic pulmonary artery pressure ≥40 mm Hg, a bidirectional or right-to-left shunt through a patent ductus arteriosus, or a flattened or bowing interventricular septum at the end of systole. Large airway disease included tracheomalacia and/or bronchomalacia documented on bronchoscopy and/or tracheoscopy by a pediatric otolaryngologist or pulmonologist. Outcomes were then described according to the three prespecified phenotypes. Neonates with pulmonary hypertension or large airway disease phenotypes had higher odds of mortality, tracheostomy, or pulmonary vasodilator use at discharge when compared to those classified with parenchymal lung disease (OR 5.4 vs. 5.1 vs. 0.59, respectively).
bpd phenotyping plays a crucial role in not only enhancing the precision of BPD definition but also in improving clinical care and guiding future intervention studies. By employing unsupervised machine learning algorithms, we can achieve a finer stratification of BPD severity, allowing for more tailored and effective therapeutic approaches. Additionally, it is imperative that future models consider the dynamic shifts in clinical phenotypes that occur as interventions are administered or discontinued during the course of hospitalization. This adaptive approach ensures that the therapeutic strategies remain aligned with the evolving needs of the neonate.
Minimizing the number of mechanical ventilation days and the need for multiple courses of mechanical ventilation is one of the major initiatives aimed at preventing the development of BPD and/or decreasing its severity (60). However, early extubation to prevent BPD must be balanced with the risks of failed extubation and increased morbidity and mortality in extremely preterm infants (61, 62). This is especially challenging for the highest-risk group of 22–24-week gestational-age infants. In the Swedish national quality registry, which has over 50% survival for 22-week gestational age infants, the median duration of mechanical ventilation was 54 days for 22-week GA infants, 32 days for 23-week infants, and 22 days for 24-week infants (63). While several prediction models using logistic regression or ML methods have been developed to aid clinicians in determining the appropriate timing for extubation in extremely preterm infants, the models do not include many patients in the high-risk category of 22–24 weeks GA and none have been routinely adopted into clinical practice (64–68). Moreover, it is worth noting that the extubation prediction models available have been developed for patients who are at risk of developing BPD and not for patients who have already been diagnosed with the condition (69). Therefore, the development of extubation prediction models for neonates with BPD could prove to be even more valuable.
The timeline for diagnosing BPD and its impact on the development of extubation prediction models is indeed a crucial aspect to consider. Currently, the diagnosis of BPD is typically made based on clinical criteria, often at 28 days or 36 weeks postmenstrual age. In the context of developing extubation prediction models, this timeline poses challenges. Timing of extubation models should take into consideration how the diagnosis of BPD impacts their utility. To address this gap, it is essential for these models to take into account the dynamic shifts in clinical phenotypes that occur during the course of hospitalization. Several strategies for achieving this include:
Comprehensive data collection, including clinical, physiological, and treatment-related variables, from neonates with diagnosed BPD is essential. This data should encompass the entire hospitalization period and should be routinely updated to reflect changes in the patient's condition.
Machine learning algorithms, particularly those with adaptability and the ability to handle dynamic data, should be employed. These algorithms can be trained on the collected data to make real-time predictions about the optimal timing for extubation for individual patients.
An important aspect of these models is continuous monitoring of the patient's clinical status. As interventions are administered or discontinued, the models should adapt and refine their predictions based on their clinical changes.
Collaboration among healthcare institutions is crucial. By aggregating data from a larger cohort of neonates with BPD, we can enhance the generalizability and accuracy of these models.
Additionally, it is worth noting that as of now, no randomized control trials have investigated extubation practices for neonates with BPD. Consensus guidelines recommend ventilator practices that include a slow rate, high tidal volume (7–12 ml/kg), and prolonged inspiratory times (>0.6 s) to account for the varying levels of airway resistance and altered distal lung compliance, which leads to diverse and different time constants (7). Furthermore, extubation should be considered once infants are on a stable low oxygen requirement, which indicates adequate lung growth and healing rather than relying on data such as carbon dioxide or end-tidal carbon dioxide (7).
Some centers have a standardized approach for deciding when to attempt extubation or consider tracheostomy for patients with severe BPD. In the Bronchopulmonary Dysplasia collaborative, only five of the 15 institutions (33%) have a ventilator weaning protocol or extubation protocol (70). Artificial intelligence-based algorithms, such as ML models, may assist in suggesting ventilator weaning strategies, predicting extubation success, or the probability of long-term mechanical ventilation. Advanced deep learning ML algorithms may be necessary to process all the complex data required for prediction, such as dynamic ventilator settings, pulse oximeter saturation and stability, blood gas results, growth velocity, chest x-ray image analysis, and other relevant factors.
There has been a recent emphasis on developing clinical decision support (CDS) tools to predict and prevent BPD. While many prediction models have been developed, no single tool has been universally adopted. A recent systematic review and meta-analysis identified 64 studies that developed or validated 53 BPD prediction models, which incorporated perinatal factors such as gestational age and birth weight, along with specific clinical features evaluated at different timepoints (5). However, the determination of significant predictors and BPD definitions varies across regions and patient cohorts, underscoring the importance of developing and validating prediction tools in neonatal networks worldwide (71–73).
There are several advantages to the shift toward using informatics to build models to predict BPD and its outcomes. In the 2021 study by Jasseem-Bobowicz et al, a prediction model was created using clinical factors including gestational age, number of RBC transfusions, number of surfactant administrations, and patent ductus arteriosus data. These factors were determined by machine learning tools including regression coefficients to establish a categorical risk scoring system that was then used to create risk categories for this model (74). The advantage of this study was its performance (AUC 0.932) and its simplicity and ease of use in clinical practice. However, drawbacks include a single-center was used to build the model, limiting generalizability. In a more recent 2023 study by Gao et al, multivariate logistic regression analysis using a stepwise fashion was performed for risk factor selection, and the least absolute shrinkage and selection operator (LASSO) was carried out for factor selection. A nomogram model was developed using a R Package “rms” to predict BPD outcomes. This model also did well with an AUC of 0.910 in the training and 0.9051 in the validation cohort. The strengths of this study were the comparison of two predictor selection methods and external validation of the risk factors, while a limitation included a small sample size from one institution (75). Another recent 2023 study by Ou et al. also used the LASSO method by 5-fold cross-validation to select the most useful predictive proteins for BPD prediction. The protein model yielded an AUC of 0.96 in the test cohort (76). The advantages of this approach included a computational and molecular integration to predict BPD. Overall, there have been more than 100 prediction models that have been developed to predict BPD, as summarized in a systemic review by Romjin et al. (77).
While numerous prediction models for BPD have been developed, their full potential remains underutilized due to several key challenges. One of the primary limitations is the lack of external validation (6). For a CDS tool to be truly effective, it must not only provide accurate predictions but also demonstrate its generalizability and reliability in real-world clinical settings. External validation, often referred to as replication, plays a pivotal role in this process, as it involves testing prediction models with data generated independently from the dataset used for model creation. One promising example in the field is the National Institutes of Childhood and Health Development (NICHD) Neonatal Research Network BPD Outcome Estimator, which employs a series of multinomial logistic regressions incorporating six critical risk factors to predict the severity of BPD or mortality (78–80). The model was internally and externally validated; however, it is still associated with racial and regional bias. To enhance its clinical translation and overcome these biases, efforts have been made to create the online “BPD Estimator” and update it in 2022 with a more recent dataset and refined BPD definition (80).
To address the current limitations and promote wider adoption of such prediction tools, a multifaceted approach is needed. This should include:
To ensure the reliability and generalizability of prediction models for BPD, it is imperative to conduct ongoing external validation. This process involves testing the models using diverse patient populations and across various healthcare settings, including different regions and institutions. By doing so, we can assess how well these models perform in real-world scenarios, which may vary in terms of patient demographics, clinical practices, and environmental factors. This continuous validation process not only enhances the models’ accuracy but also builds trust among healthcare providers, making them more likely to integrate these tools into their clinical decision-making processes.
The development of prediction models should not be a one-time effort. Instead, it should be an iterative process that involves continuous evaluation and refinement. Regularly assessing model performance is crucial to identifying changes in accuracy over time, potential biases that may emerge, or changes in the patient population that the model serves. This evaluation should be data-driven and should lead to updates and improvements in the models as new data become available. In essence, it is about ensuring that the prediction tools remain relevant and effective.
Recognizing and addressing biases within prediction models is important. Models should be carefully scrutinized to identify any biases related to race, ethnicity, socioeconomic status, or geographic location. These biases can lead to disparities in healthcare outcomes. Mitigating biases involves refining the algorithms, diversifying the training datasets, and incorporating fairness and equity considerations into model development. By actively working to reduce biases, we can ensure that these prediction tools provide equitable care to all neonates, irrespective of their background or location.
One significant barrier to the adoption of prediction tools is a lack of awareness and understanding among healthcare providers. Efforts should be made to educate neonatal care teams about the availability, benefits, and utility of these tools. This can involve publishing in reputable journals and presenting data in conferences or workshops, with the eventual goal of integrating into EHRs. When healthcare providers are well-informed about the potential of these tools to enhance patient care, they are more likely to incorporate them into their clinical workflows, ultimately benefiting neonates at risk of BPD.
While a single intervention to prevent BPD has been elusive, there are likely adaptable strategies across fetal, neonatal, infant, and childhood stages that can have a tangible summative effect (81). The strategies could target crucial developmental windows that our current research/QI methodologies might overlook. Leveraging artificial intelligence/machine learning/deep learning techniques can enhance our understanding by discerning patterns from pertinent and complex clinical and biological data and provide CDS tools to clinicians over a care continuum.
An illustrative example of clinical informatics’ impact can be observed in the field of oncology. In cancer care, clinical informatics has enabled the integration of genetic and clinical data tools to facilitate the identification of specific cancer subtypes and the tailoring of treatments to individual patients. For instance, the Molecular Analysis for Therapy Choice (MATCH) trial, conducted by the National Cancer Institute (NCI), employs informatics-driven genomic profiling to match cancer patients with targeted therapies, resulting in more effective treatments and improved patient outcomes (82).
In the field of critical care medicine, clinical informatics has revolutionized patient monitoring and early condition detection. For instance, the implementation of predictive analytics and clinical decision support systems has significantly improved patient management in ICUs. The eICU Collaborative Research Database, a notable example, collects data from thousands of ICU patients across the United States and employs informatics-driven algorithms to predict adverse events, allowing healthcare teams to intervene proactively and reduce mortality rates (83).
Translating this success to neonatology, clinical informatics holds the potential to develop predictive models and clinical decision support tools that assist neonatal care teams in optimizing care strategies for infants at risk of BPD. By analyzing complex data from NICUs, these tools can provide early warnings of deteriorating conditions, helping clinicians take timely actions to prevent or mitigate the severity of BPD.
At present, available CDS tools for BPD still have several limitations. Often, these models were created with data from a single center, have a small sample size, lack good quality external validation, and may only apply to specific high-risk infants such as those on ventilators, limiting their generalizability. Moreover, over half of the published models use data from infants born over a decade ago, which may not reflect present-day clinical practice (6). Additionally, existing models do not account for the infant's clinical trajectory over time, which could provide a dynamic approach for better personalized preventive treatment and targeted trial recruitment. Nonetheless, a recent machine learning (ML)-based prediction model demonstrated the predictive power of postnatal respiratory support for 14 consecutive days (84). While this model was developed at a single center without validation, it demonstrates how prediction models and tools are evolving to better meet clinical needs.
To address the limitations of current CDS tools for BPD, there are several potential solutions that can be considered. First, efforts should be made to collect and integrate data from multiple centers to create more robust and generalizable models. Collaborative initiatives can help gather a larger and more diverse dataset, ensuring that the models are applicable across different clinical settings. Furthermore, it is crucial to validate these models externally to confirm their accuracy and reliability in various populations. Additionally, updating the datasets with recent clinical data is essential to reflect the current clinical practice, as BPD management and patient characteristics evolve over time. To provide a more dynamic approach, future models can incorporate the infant’s clinical trajectory over time, enabling personalized preventive treatment strategies and more targeted recruitment for clinical trials. While the recent ML-based prediction model for postnatal respiratory support is a step in the right direction, future research should focus on refining and validating such models to ensure their clinical utility and effectiveness across multiple healthcare systems. This collaborative and evolving approach to CDS tools can significantly enhance their effectiveness in managing BPD.
Clinical informatics has the potential to make significant strides in the prevention and reduction of the severity of BPD among neonates. One of the key applications is early risk prediction. Informatics tools can analyze a multitude of data points, including gestational age, birth weight, respiratory parameters, and maternal health records, to identify neonates at high risk of developing BPD. By flagging these high-risk cases, healthcare teams can implement preventive measures promptly, such as optimizing respiratory support strategies or initiating lung-protective ventilation strategies. In addition to early risk prediction, clinical informatics can also play a crucial role in improving communication and coordination among healthcare providers involved in the care of neonates with BPD. Informatics tools can facilitate seamless sharing of patient data, treatment plans, and progress updates among neonatologists, pulmonologists, nurses, and other healthcare professionals. This enhanced collaboration can lead to more effective and timely interventions, ultimately reducing the severity of BPD (4).
Clinical informatics can offer a valuable tool in the form of automated weekly reminders and graphical representation of ventilator parameters to assess respiratory progress in neonates with BPD. These reminders can prompt healthcare providers to systematically evaluate the infant’s respiratory status on a regular basis, ensuring that no critical changes or deteriorations go unnoticed. Furthermore, informatics systems can generate graphical displays of ventilator parameters over the past few weeks, allowing clinicians to visualize trends and deviations in respiratory support. Such visualizations can highlight improvements or declines in a neonate's lung function, enabling healthcare teams to make informed decisions regarding adjustments to ventilation strategies or other therapeutic interventions. This proactive approach not only supports timely interventions but also aids in fine-tuning treatment plans to optimize respiratory care and minimize the severity of BPD.
Informatics systems enable continuous monitoring and data analysis of neonatal patients in real-time. By tracking physiological parameters, like oxygen saturation levels and respiratory rates, clinical informatics can detect subtle changes that may indicate evolving BPD (85). When these early warning signs are identified, healthcare providers can adjust treatment plans and interventions, potentially preventing or mitigating the progression of the disease (86). Another critical aspect is the personalization of care plans. Clinical informatics can assist in tailoring therapeutic approaches based on individual patient data. For instance, informatics tools can analyze a neonate's response to specific treatments and medications, enabling the adjustment of therapy to maximize effectiveness while minimizing potential side effects. This personalized approach can optimize outcomes and decrease the overall severity of BPD (47).
Clinical informatics can also contribute to the care of neonates with established BPD by streamlining medication management, integrating clinical data, enabling remote consultations, supporting quality assurance efforts, and engaging patients and their families.
Clinical informatics provides a platform for the management of medications in neonates with established BPD. It assists clinicians in maintaining accurate and up-to-date medication records, tracking dosages, and monitoring adverse effects. This ensures that infants receive their prescribed medications consistently and safely. Moreover, informatics systems can generate alerts for potential drug interactions or dosage adjustments, helping clinicians make informed decisions regarding pharmacological interventions (87).
Managing the care of neonates with established BPD often involves a multitude of clinical data sources, including laboratory results, imaging reports, and patient histories. Clinical informatics excels at integrating these data sets into a unified and accessible format. It allows clinicians to access a comprehensive view of each patient's health status, and prior response to medications/treatments, streamlining decision-making and reducing the risk of oversight (88).
In situations where neonates with established BPD require specialized care or consultations from experts, clinical informatics facilitates remote consultations and telehealth services. Clinicians can securely share patient data and images with specialists, enabling timely expert opinions and guidance without the need for physical presence. This extends access to expertise and can be particularly valuable in managing complex cases (89).
Clinical informatics offers tools for quality assurance and benchmarking in the care of neonates with BPD. Clinicians can compare their treatment outcomes and practices with national or international standards and benchmarks. This data-driven approach allows for continuous improvement in care protocols, ensuring that the latest evidence-based practices are adopted to enhance patient outcomes (90).
Informatics systems also have a role in engaging patients and their families in the care process. Neonates with established BPD often require extended hospital stays, and informatics can provide a means for families to stay informed about their infant's progress. It offers patient portals and educational resources to empower families with information and facilitate communication with clinicians, promoting a collaborative approach to care (91).
Current data collection and storage methods supporting BPD research are varied. Some databases aim to collect general demographic, clinical, and outcomes data on very low-birthweight infants, while others are dedicated to sponsored multi-site trials investigating BPD as a primary or secondary outcome. Additionally, some databases focus on more granular data derived from a single-site center. Large databases targeting VLBW infants exist both in the US and internationally, and most data is entered manually by principal investigators or trained data abstractors at participating sites (92–96). However, the United Kingdom's National Neonatal Database stands out as an exception due to its use of a common EHR shared among participating sites, allowing data to flow automatically into the database on a quarterly basis. Quality assessment of the extracted data is then published for participants to review (95). A preliminary search conducted on PubMed on January 8, 2024, using the keywords “National Neonatal Research Database (NNRD)” returned 26 publications, primarily centered around neonatal nutrition. Surprisingly, none of the studies identified in this initial search were specifically focused on BPD. We believe future research questions will delve into the utilization of the NNRD to investigate BPD's epidemiology, risk factors, outcomes, and potential interventions.
Despite the existence of these databases, challenges remain in data collection, including the labor-intensive nature of manual data entry, incomplete data, evolving definitions of disease, inability to capture longitudinal data, inherent data bias, data governance, and privacy concerns. These challenges highlight the need for continued work on improving data collection and storage methods to support BPD research (refer to Table 1).
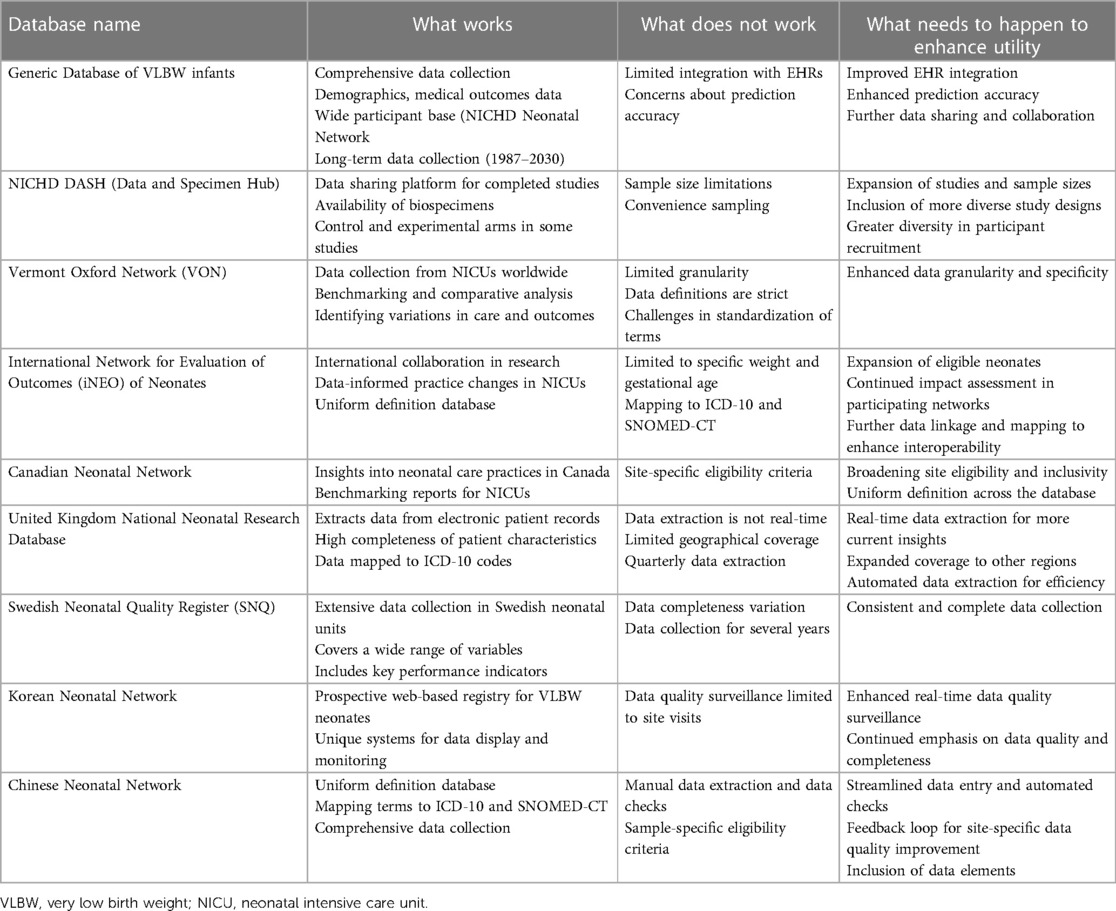
Table 1. Table of select existing national registries of neonates with or at risk for BPD.
Moreover, without consensus on a minimum standard dataset, comparing and combining data across databases becomes challenging. In addition, the lack of standardized definitions and terminologies hinders cross-site analysis and increases the risk of errors in data interpretation. To address this, initiatives such as the Neonatal Research Network (NRN) have developed standardized definitions for outcomes and clinical variables, which have been adopted by many large databases. Despite these initiatives, there is still a need for more widespread adoption of standardized definitions and terminologies to improve interoperability and facilitate collaboration across different databases and research groups. The use of common data models, such as the OMOP CDM, may help in achieving this goal by providing a standardized structure for data collection and storage that can be shared across different institutions and studies.
Improving the collection and storage of BPD data is crucial for advancing our knowledge of the disease and enhancing patient outcomes. To achieve this goal, it is necessary to leverage automated data extraction and mapping of a minimum dataset to standard definitions and terms. The lack of BPD-specific data granularity in current VLBW databases limits their research potential in answering questions about candidate treatments or management approaches. Standardization of data elements has been recognized by some registries, but many remain unmapped to accepted standard dictionaries such as International Statistical Classification of Diseases and Related Health Problems-10 (ICD-10) or Systematized Nomenclature of Medicine-Clinical Terms (SNOMED-CT), which limits collaboration and interoperability (96, 97). The UK model demonstrates the potential for automated data extraction with high fidelity and provides a roadmap for streamlining epidemiologic data collection (98, 99). By better capturing demographic, clinical, and outcome data, we can perform retrospective investigations and explore disease incidence and risk factors. Ultimately, this can inform the development of improved management approaches and more effective treatments for patients with BPD.
Due to center-specific variations in patient care and outcomes, multi-center collaborations are necessary to advance our understanding of the disease, identify best practices, and improve patient outcomes (1, 70, 100). Multi-center collaborations offer numerous benefits in BPD research, including a better understanding of disease mechanisms, lung repair, and regeneration. Through these collaborations, disease phenotypes can be better classified and novel therapeutic targets can be better explored. Multi-center collaborations can identify variations in neonatal outcomes between centers, leading to national and international benchmarking, quality improvement activities, and implementation of “best practice” strategies (1, 7, 100).
Multi-center collaborations, exemplified by initiatives like the BPD Collaborative encompassing 27 centers across the USA and one in Sweden, have undeniably propelled BPD research forward and have improved patient care outcomes (7, 58, 100, 101). Within these collaborations, clinical informatics has emerged as a critical component, serving to enhance the efficiency and effectiveness of research endeavors. Clinical informatics systems provide a secure and standardized platform for the exchange of patient data and research findings among participating centers. This data sharing facilitates the aggregation of extensive datasets from diverse clinical settings, empowering researchers to conduct comprehensive analyses spanning multiple institutions. By harnessing the power of data integration, clinical informatics enables the identification of trends and insights that might otherwise remain elusive when working solely with isolated datasets. Furthermore, informatics tools play a central role in harmonizing clinical practices and standardizing data collection protocols across collaborating institutions, ensuring consistent data collection and adhering to predefined standards (58). This standardization minimizes variations in data quality and enhances the reliability of research outcomes. In the context of the BPD Collaborative, clinical informatics has been instrumental in facilitating the implementation of essential strategies, such as optimizing ventilator management and nutritional practices. By tracking patient responses and outcomes using informatics tools, the collaborative has identified best practices and areas for improvement, contributing to the enhanced quality of care and improved patient outcomes (100, 101).
In the study by Guaman et al, clinical informatics played a key role in understanding neonates with severe BPD. For instance, clinical informatics facilitated the uniform collection of clinical data across the eight NICUs. A standardized clinical data form was designed and implemented, ensuring that essential patient information, including gestational age, respiratory support requirements, and medication usage, was consistently recorded for all inpatients born at <32 weeks. The study defined severe BPD based on specific criteria, including the need for ≥30% supplemental oxygen and/or positive pressure ventilation at 36 weeks postmenstrual age. Clinical informatics played a key role in applying these criteria uniformly across participating NICUs. Clinical informatics also facilitated the analysis of management practices across the participating NICUs. The study examined differences in the use of interventions such as mechanical ventilation, diuretics, inhaled corticosteroids, and inhaled β-agonists. By collecting and analyzing these data using informatics tools, the researchers identified variations in the management of infants with severe BPD among different centers (102).
In addressing the significant challenges that persist in multi-center collaborations for BPD research, it is essential to recognize the multifaceted nature of this condition. The complex and multifactorial etiology of BPD, encompassing factors such as prematurity, inflammation, and genetic predisposition, contributes to the intricate clinical landscape (58, 100). Furthermore, BPD is not a one-size-fits-all condition. It presents a wide spectrum of patient characteristics, including variations in gestational age, birth weight, and comorbidities, necessitating diverse and tailored management approaches that can evolve over the course of a patient's hospitalization and even throughout their lifetime (103).
The challenges extend to data collection and management practices. Current data collection methods are labor-intensive and often fraught with incompleteness, preventing a comprehensive and real-world representation of the clinical phenotype of BPD (1, 79). Moreover, the evolving definitions of disease pose an ongoing challenge. The field continuously refines diagnostic criteria and treatment strategies, making it critical to capture longitudinal data to track changes in patient care and outcomes over time. However, this longitudinal perspective remains elusive due to existing data limitations.
Data governance and privacy concerns also loom large, impeding the seamless sharing of critical information among institutions. Protecting patient privacy while facilitating data sharing demands sophisticated solutions and adherence to stringent regulations (1, 79). Additionally, BPD lacks a universally accepted “single” therapy, further complicating research efforts. Tailoring treatments to individual patients requires nuanced real-world data to inform decision-making and optimize care.
Efforts such as the OHDSI (Observational Health Data Sciences and Informatics) OMOP CDM (Common Data Model) present a promising avenue to overcome the substantial challenges in multi-center collaborations for bronchopulmonary dysplasia (BPD) research (104). The OHDSI initiative is at the forefront of harnessing clinical informatics to standardize and streamline data collection and analysis. The OMOP CDM, an integral component of OHDSI, serves as a standardized clinical data framework that allows the extraction, ingestion, and collation of pertinent variables from diverse sources, enabling the creation of disease-specific observational research registries like a BPD registry (105, 106).
Central to the success of these initiatives are widely recognized clinical terminologies, such as SNOMED CT (Systematized Nomenclature of Medicine Clinical Terms) and LOINC (Logical Observation Identifiers Names and Codes) (107, 108). SNOMED CT provides a comprehensive and standardized clinical vocabulary that enhances interoperability and consistency in healthcare data, while LOINC facilitates the uniform identification of medical laboratory observations, ensuring data accuracy and comparability across institutions.
These standardized clinical data frameworks empower researchers to securely store data, conduct rigorous analyses, and efficiently share information among participating sites, thereby reducing the barriers to collaboration and facilitating data-driven research efforts. The concept of a “living BPD registry,” driven by OHDSI OMOP CDM and bolstered by SNOMED CT and LOINC, holds the potential to revolutionize BPD research and collaborative endeavors. It offers the opportunity for reproducible research in phenotype definitions and comparative analyses, leveraging a wealth of standardized real-world data across institutions. Ultimately, these initiatives not only lower the activation energy required for collaboration but also hold the promise of driving meaningful advancements in BPD care and research outcomes.
BPD research and the integration of clinical informatics have undoubtedly made significant progress, yet several formidable challenges persist (106). The current definition of BPD, based on respiratory support at 36 weeks postmenstrual age, represents a crucial step forward in standardizing diagnostic criteria and understanding long-term patient-centered outcomes (79). However, it remains an oversimplified representation of the intricate clinical reality and heterogeneity that exists within the BPD spectrum.
To address these challenges effectively, it is imperative to delve into the nuances that distinguish children with varying degrees of BPD severity. A more granular understanding can guide the development of interventions tailored to specific subgroups of patients while minimizing potential harm. This nuanced approach acknowledges the multifaceted nature of BPD and recognizes that each neonate’s clinical phenotype is unique.
Despite the existence of risk stratification tools for BPD, their full potential has not been realized due to limited integration with EHRs and concerns regarding prediction accuracy. This stands in stark contrast to the robust adoption of other neonatal tools, such as those used for predicting early-onset sepsis or guiding phototherapy recommendations (52, 78). To comprehensively address the complexities of defining, preventing, and treating BPD, CDS tools must not only seamlessly integrate with EHRs but also offer comprehensive treatment guidance. Achieving this requires a strategic approach focused on tailored care rather than advocating for a one-size-fits-all reduction in care.
Our proposed clinical informatics approach aims to empower clinicians with timely, individualized information for optimized decision-making. By harnessing data-driven insights and predictive models, we provide care providers with the tools to make informed decisions that align with each neonate's specific risk profile. This approach takes into account both clinical severity and individual risk factors. While some moderate-risk neonates may indeed benefit from escalated care, applying the same approach universally could lead to overutilization of resources and unnecessary interventions. Clinical informatics enables the identification of moderate-risk neonates most likely to benefit from escalated care, thereby maximizing the utility of interventions while minimizing potential harm or resource inefficiency.
Collaborative efforts involving multiple centers are imperative for advancing our understanding of BPD. Such collaborations bring together larger sample sizes, diverse patient populations, and a broader range of expertise. Nevertheless, challenges related to data collection, storage, and the lack of standardization of terms and definitions persist. To facilitate seamless collaboration and interoperability, the standardization of data elements and mapping to recognized clinical terminologies such as ICD-10 and SNOMED-CT is essential. Additionally, the establishment of a “living BPD registry” is crucial, capable of efficiently collecting and storing data while incorporating more granular information such as clinical biomarkers, echocardiography/radiographic data, and high-resolution vital signs and ventilator data. This approach enables more accurate clinical phenotyping, thereby advancing our understanding of BPD and facilitating tailored care.
In conclusion, BPD is a complex disease that affects premature infants and is responsible for significant morbidity and healthcare costs. While clinical informatics holds promise in improving BPD prevention, management, and outcomes through the use of clinical decision support tools, we are still in the very early stages of using these applications effectively. Research efforts utilizing multi-center collaborations and state-of-the-art analysis techniques may help identify clinical phenotypes of BPD. However, many challenges remain in BPD research and clinical informatics, including the need for standardized data collection and definitions, full integration with EMR, the development of precise and personalized treatments for different BPD subtypes, and the logistics and governance issues with data storage, utilization, and collaboration. Overall, while there is promise in the integration of clinical informatics into BPD management and research, much work remains to be done to fully realize its potential in improving outcomes for these vulnerable patients.
AM: manuscript idea, creation of figure, manuscript writing, and approval of the final manuscript; AH: manuscript writing and approval of the final manuscript; LK: manuscript writing and approval of the final manuscript; KA: manuscript writing and approval of the final manuscript; KS: creation of table, manuscript writing, and approval of final manuscript; CV: manuscript writing and approval of final manuscript; NP: manuscript writing and approval of final manuscript; VT: manuscript writing and approval of final manuscript; JB: oversight, manuscript writing, and approval of final manuscript. All authors contributed to the article and approved the submitted version.
AM- Parker B. Francis Foundation; the National Institutes of Health (NIH) Eunice Kennedy Shriver National Institute of Child Health and Human Development K23HD10170, NIH National Heart Lung and Blood Institute 5R25HL126140-06 Subaward.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Thébaud B, Goss KN, Laughon M, Whitsett JA, Abman SH, Steinhorn RH, et al. Bronchopulmonary dysplasia. Nat Rev Dis Primer. (2019) 5(1):78. doi: 10.1038/s41572-019-0127-7
2. Jensen EA, Schmidt B. Epidemiology of bronchopulmonary dysplasia. Birt Defects Res A Clin Mol Teratol. (2014) 100(3):145–57. doi: 10.1002/bdra.23235
3. Northway WH, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N Engl J Med. (1967) 276(7):357–68. doi: 10.1056/NEJM196702162760701
4. Humayun J, Löfqvist C, Ley D, Hellström A, Gyllensten H. Systematic review of the healthcare cost of bronchopulmonary dysplasia. BMJ Open. (2021) 11(8):e045729. doi: 10.1136/bmjopen-2020-045729
5. Higgins RD, Jobe AH, Koso-Thomas M, Bancalari E, Viscardi RM, Hartert TV, et al. Bronchopulmonary dysplasia: executive summary of a workshop. J Pediatr. (2018) 197:300–8. doi: 10.1016/j.jpeds.2018.01.043
6. Kwok TC, Batey N, Luu KL, Prayle A, Sharkey D. Bronchopulmonary dysplasia prediction models: a systematic review and meta-analysis with validation. Pediatr Res. (2023) 94:1–12. doi: 10.1038/s41390-022-02451-8
7. Abman SH, Collaco JM, Shepherd EG, Keszler M, Cuevas-Guaman M, Welty SE, et al. Interdisciplinary care of children with severe bronchopulmonary dysplasia. J Pediatr. (2017) 181:12–28.e1. doi: 10.1016/j.jpeds.2016.10.082
8. Chess PR, D’Angio CT, Pryhuber GS, Maniscalco WM. Pathogenesis of bronchopulmonary dysplasia. Semin Perinatol. (2006) 30(4):171–8. doi: 10.1053/j.semperi.2006.05.003
9. Nadler JJ, Downing GJ. Liberating health data for clinical research applications. Sci Transl Med. (2010) 2(18):18cm6. doi: 10.1126/scitranslmed.3000764
10. Lorenzi NM, Kouroubali A, Detmer DE, Bloomrosen M. How to successfully select and implement electronic health records (EHR) in small ambulatory practice settings. BMC Med Inform Decis Mak. (2009) 9(1):15. doi: 10.1186/1472-6947-9-15
11. Adhikari N, Lapinsky SE. Medical informatics in the intensive care unit: overview of technology assessment. J Crit Care. (2003) 18(1):41–7. doi: 10.1053/jcrc.2003.YJCRC9
12. Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. (2015) 348(6230):124–8. doi: 10.1126/science.aaa1348
13. Walsh S, de Jong EEC, van Timmeren JE, Ibrahim A, Compter I, Peerlings J, et al. Decision support systems in oncology. JCO Clin Cancer Inform. (2019) 3:1–9. doi: 10.1200/CCI.18.00001
14. Anashkina AA, Leberfarb EY, Orlov YL. Recent trends in cancer genomics and bioinformatics tools development. Int J Mol Sci. (2021) 22(22):12146. doi: 10.3390/ijms222212146
15. Reyna MA, Josef CS, Jeter R, Shashikumar SP, Westover MB, Nemati S, et al. Early prediction of sepsis from clinical data: the PhysioNet/computing in cardiology challenge 2019. Crit Care Med. (2020) 48(2):210–7. doi: 10.1097/CCM.0000000000004145
16. Subbe CP, Duller B, Bellomo R. Effect of an automated notification system for deteriorating ward patients on clinical outcomes. Crit Care Lond Engl. (2017) 21(1):52. doi: 10.1186/s13054-017-1635-z
17. Koyner JL, Adhikari R, Edelson DP, Churpek MM. Development of a multicenter ward-based AKI prediction model. Clin J Am Soc Nephrol CJASN. (2016) 11(11):1935–43. doi: 10.2215/CJN.00280116
18. Campbell JP, Ataer-Cansizoglu E, Bolon-Canedo V, Bozkurt A, Erdogmus D, Kalpathy-Cramer J, et al. Expert diagnosis of plus disease in retinopathy of prematurity from computer-based image analysis. JAMA Ophthalmol. (2016) 134(6):651–7. doi: 10.1001/jamaophthalmol.2016.0611
19. Chiang MF, Jiang L, Gelman R, Du YE, Flynn JT. Interexpert agreement of plus disease diagnosis in retinopathy of prematurity. Arch Ophthalmol Chic Ill 1960. (2007) 125(7):875–80. doi: 10.1001/archopht.125.7.875
20. Rao DP, Savoy FM, Tan JZE, Fung BPE, Bopitiya CM, Sivaraman A, et al. Development and validation of an artificial intelligence based screening tool for detection of retinopathy of prematurity in a South Indian population. Front Pediatr. (2023) 11:1197237. doi: 10.3389/fped.2023.1197237
21. Gephart SM, Tolentino DA, Quinn MC, Wyles C. Neonatal intensive care workflow analysis informing NEC-zero clinical decision support design. CIN Comput Inform Nurs. (2023) 41(2):94. doi: 10.1097/CIN.0000000000000929
22. Khazaei H, Mench-Bressan N, McGregor C, Pugh JE. Health informatics for neonatal intensive care units: an analytical modeling perspective. IEEE J Transl Eng Health Med. (2015) 3:3000109. doi: 10.1109/JTEHM.2015.2485268
23. Lacey S, Smith JB, Cox K. Pediatric safety and quality. In: Hughes RG, editors. Patient Safety and Quality: An Evidence-based Handbook for Nurses. Chapter 47. Rockville, MD: Agency for Healthcare Research and Quality (US) (2008). p. 1–59. (Advances in Patient Safety). (Cited January 8, 2024). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK2662/
24. Babaie M, Nourian M, Atashzadeh-Shoorideh F, Manoochehri H, Nasiri M. Patient safety culture in neonatal intensive care units: a qualitative content analysis. Front Public Health. (2023) 11:1065522. doi: 10.3389/fpubh.2023.1065522
25. Bassin L, Raubenheimer J, Bell D. The implementation of a real time early warning system using machine learning in an Australian hospital to improve patient outcomes. Resuscitation. (2023) 188:109821. doi: 10.1016/j.resuscitation.2023.109821
26. Pollack MM, Trujillo Rivera E, Morizono H, Patel AK. Clinical instability is a sign of severity of illness: a cohort study. Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensive Crit Care Soc. (2023). 24:e425–33. doi: 10.1097/PCC.0000000000003255
27. Yalçın N, Kaşıkcı M, Çelik HT, Demirkan K, Yiğit Ş, Yurdakök M. Development and validation of machine learning-based clinical decision support tool for identifying malnutrition in NICU patients. Sci Rep. (2023) 13(1):5227. doi: 10.1038/s41598-023-32570-z
28. Grunwell JR, Rad MG, Ripple MJ, Yehya N, Wong HR, Kamaleswaran R. Identification of a pediatric acute hypoxemic respiratory failure signature in peripheral blood leukocytes at 24h post-ICU admission with machine learning. Front Pediatr. (2023) 11:1159473. doi: 10.3389/fped.2023.1159473
29. Bancalari E, Jain D. Bronchopulmonary dysplasia: 50 years after the original description. Neonatology. (2019) 115(4):384–91. doi: 10.1159/000497422
30. Kallapur SG, Jobe AH. Contribution of inflammation to lung injury and development. Arch Dis Child Fetal Neonatal Ed. (2006) 91(2):F132–135. doi: 10.1136/adc.2004.068544
31. Rojas MA, Gonzalez A, Bancalari E, Claure N, Poole C, Silva-Neto G. Changing trends in the epidemiology and pathogenesis of neonatal chronic lung disease. J Pediatr. (1995) 126(4):605–10. doi: 10.1016/S0022-3476(95)70362-4
32. Bhandari A, Bhandari V. Pitfalls, problems, and progress in bronchopulmonary dysplasia. Pediatrics. (2009) 123(6):1562–73. doi: 10.1542/peds.2008-1962
33. Meadow W, Lee G, Lin K, Lantos J. Changes in mortality for extremely low birth weight infants in the 1990s: implications for treatment decisions and resource use. Pediatrics. (2004) 113(5):1223–9. doi: 10.1542/peds.113.5.1223
34. Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal outcomes of extremely preterm infants from the NICHD neonatal research network. Pediatrics. (2010) 126(3):443–56. doi: 10.1542/peds.2009-2959
35. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. (2001) 344(11):783–92. doi: 10.1056/NEJM200103153441101
36. Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, et al. Effects of a selective inhibitor of the abl tyrosine kinase on the growth of bcr-abl positive cells. Nat Med. (1996) 2(5):561–6. doi: 10.1038/nm0596-561
37. Adler-Milstein J, Holmgren AJ, Kralovec P, Worzala C, Searcy T, Patel V. Electronic health record adoption in US hospitals: the emergence of a digital “advanced use” divide. J Am Med Inform Assoc JAMIA. (2017) 24(6):1142–8. doi: 10.1093/jamia/ocx080
38. Hay WW. Nutritional support strategies for the preterm infant in the neonatal intensive care unit. Pediatr Gastroenterol Hepatol Nutr. (2018) 21(4):234–47. doi: 10.5223/pghn.2018.21.4.234
39. Moltu SJ, Strømmen K, Blakstad EW, Almaas AN, Westerberg AC, Brække K, et al. Enhanced feeding in very-low-birth-weight infants may cause electrolyte disturbances and septicemia—a randomized, controlled trial. Clin Nutr. (2013) 32(2):207–12. doi: 10.1016/j.clnu.2012.09.004
40. Embleton NE, Pang N, Cooke RJ. Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics. (2001) 107(2):270–3. doi: 10.1542/peds.107.2.270
41. Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD neonatal research network. Pediatrics. (2002) 110(2 Pt 1):285–91. doi: 10.1542/peds.110.2.285
42. Cantey JB, Milstone AM. Bloodstream infections: epidemiology and resistance. Clin Perinatol. (2015) 42(1):1–16. vii. doi: 10.1016/j.clp.2014.10.002
43. Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA. (2004) 292(19):2357–65. doi: 10.1001/jama.292.19.2357
44. Kuzniewicz MW, Puopolo KM, Fischer A, Walsh EM, Li S, Newman TB, et al. A quantitative, risk-based approach to the management of neonatal early-onset sepsis. JAMA Pediatr. (2017) 171(4):365–71. doi: 10.1001/jamapediatrics.2016.4678
45. Valadie CT, Arya S, Arora T, Pandillapalli NR, Moreira A. A bioinformatics approach towards bronchopulmonary dysplasia. Transl Pediatr. (2023) 12(6):1213–24. doi: 10.21037/tp-23-133
46. Cheema Z, Kwinta P, Moreira A, Tovar M, Mustafa SB. Big data for tiny patients: a precision medicine approach to bronchopulmonary dysplasia. Pediatr Ann. (2022) 51(10):e396–404. doi: 10.3928/19382359-20220803-06
47. Onland W, Hutten J, Miedema M, Bos LD, Brinkman P, Maitland-van der Zee AH, et al. Precision medicine in neonates: future perspectives for the lung. Front Pediatr. (2020) 8:586061. doi: 10.3389/fped.2020.586061
48. Bayne LE. Big data in neonatal health care: big reach, big reward? Crit Care Nurs Clin North Am. (2018) 30(4):481–97. doi: 10.1016/j.cnc.2018.07.005
49. Kumar N, Akangire G, Sullivan B, Fairchild K, Sampath V. Continuous vital sign analysis for predicting and preventing neonatal diseases in the twenty-first century: big data to the forefront. Pediatr Res. (2020) 87(2):210–20. doi: 10.1038/s41390-019-0527-0
50. Malhotra A, Molloy EJ, Bearer CF, Mulkey SB. Emerging role of artificial intelligence, big data analysis and precision medicine in pediatrics. Pediatr Res. (2023) 93(2):281–3. doi: 10.1038/s41390-022-02422-z
51. Logan JW, Lynch SK, Curtiss J, Shepherd EG. Clinical phenotypes and management concepts for severe, established bronchopulmonary dysplasia. Paediatr Respir Rev. (2019) 31:58–63. doi: 10.1016/j.prrv.2018.10.004
52. Beam K, Wang C, Beam A, Clark R, Tolia V, Ahmad K. National needs assessment of utilization of common newborn clinical decision support tools. Am J Perinatol. (2023). doi: 10.1055/a-2096-2168
53. Chung KF, Adcock IM. How variability in clinical phenotypes should guide research into disease mechanisms in asthma. Ann Am Thorac Soc. (2013) 10:S109–17. doi: 10.1513/AnnalsATS.201304-087AW
54. Jobe AJ. The new BPD: an arrest of lung development. Pediatr Res. (1999) 46(6):641–641. doi: 10.1203/00006450-199912000-00007
55. Bel EH. Clinical phenotypes of asthma. Curr Opin Pulm Med. (2004) 10:44–50. doi: 10.1097/00063198-200401000-00008
56. Kim CJ, Romero R, Chaemsaithong P, Chaiyasit N, Yoon BH, Kim YM. Acute chorioamnionitis and funisitis: definition, pathologic features, and clinical significance. Am J Obstet Gynecol. (2015) 213(4 Suppl):S29–52. doi: 10.1016/j.ajog.2015.08.040
57. Kalikkot Thekkeveedu R, Guaman MC, Shivanna B. Bronchopulmonary dysplasia: a review of pathogenesis and pathophysiology. Respir Med. (2017) 132:170–7. doi: 10.1016/j.rmed.2017.10.014
58. Sindelar R, Shepherd EG, Ågren J, Panitch HB, Abman SH, Nelin LD, et al. Established severe BPD: is there a way out? Change of ventilatory paradigms. Pediatr Res. (2021) 90(6):1139–46. doi: 10.1038/s41390-021-01558-8
59. Wu KY, Jensen EA, White AM, Wang Y, Biko DM, Nilan K, et al. Characterization of disease phenotype in very preterm infants with severe bronchopulmonary dysplasia. Am J Respir Crit Care Med. (2020) 201(11):1398–406. doi: 10.1164/rccm.201907-1342OC
60. Jensen EA, DeMauro SB, Kornhauser M, Aghai ZH, Greenspan JS, Dysart KC. Effects of multiple ventilation courses and duration of mechanical ventilation on respiratory outcomes in extremely low-birth-weight infants. JAMA Pediatr. (2015) 169(11):1011–7. doi: 10.1001/jamapediatrics.2015.2401
61. Chawla S, Natarajan G, Shankaran S, Carper B, Brion LP, Keszler M, et al. Markers of successful extubation in extremely preterm infants, and morbidity after failed extubation. J Pediatr. (2017) 189:113–119.e2. doi: 10.1016/j.jpeds.2017.04.050
62. Shalish W, Keszler M, Kovacs L, Chawla S, Latremouille S, Beltempo M, et al. Age at first extubation attempt and death or respiratory morbidities in extremely preterm infants. J Pediatr. (2023) 252:124–130.e3. doi: 10.1016/j.jpeds.2022.08.025
63. Normon M, Jonsson B, Soderling J, Bjorklund LJ, Hakansson S. Patterns of respiratory support by gestational age in very preterm infants. Neonatology. (2023) 120:142–52. doi: 10.1159/000527641
64. A predictive model for extubation readiness in extremely preterm infants. J Perinatol. (2019) 39:1663–9. doi: 10.1038/s41372-019-0475-x
65. Assessment of Extubation Readiness Using Spontaneous Breathing Trials in Extremely Preterm Neonates | Critical Care Medicine | JAMA Pediatrics | JAMA Network. (Cited May 10, 2023). Available online at: https://jamanetwork.com/journals/jamapediatrics/fullarticle/2757363
66. Mueller M, Wagner CC, Stanislaus R, Almeida JS. Machine learning to predict extubation outcome in premature infants. IEEE Conference publication, IEEE Xplore. (Cited May 10, 2023). Available online at: https://ieeexplore-ieee-org.libproxy.uthscsa.edu/document/6707058
67. Natarajan A, Lam G, Liu J, Beam AL, Beam KS, Levin JC. Prediction of extubation failure among low birthweight neonates using machine learning. J Perinatol Off J Calif Perinat Assoc. (2023) 43(2):209–14. doi: 10.1038/s41372-022-01591-3
68. Kanbar LJ, Shalish W, Onu CC, Latremouille S, Kovacs L, Keszler M, et al. Automated prediction of extubation success in extremely preterm infants: the APEX multicenter study. Pediatr Res. (2023) 93(4):1041–9. doi: 10.1038/s41390-022-02210-9
69. Dryer RA, Salem A, Saroha V, Greenberg RG, Rysavy MA, Chawla S, et al. Evaluation and validation of a prediction model for extubation success in very preterm infants. J Perinatol Off J Calif Perinat Assoc. (2022) 42(12):1674–9. doi: 10.1038/s41372-022-01517-z
70. Cristea AI, Tracy MC, Bauer SE, Guaman MC, Welty SE, Baker CD, et al. Approaches to interdisciplinary care for infants with severe bronchopulmonary dysplasia: a survey of the bronchopulmonary dysplasia collaborative. Am J Perinatol. (2022). doi: 10.1055/s-0042-1755589
71. El Faleh I, Faouzi M, Adams M, Gerull R, Chnayna J, Giannoni E, et al. Bronchopulmonary dysplasia: a predictive scoring system for very low birth weight infants. A diagnostic accuracy study with prospective data collection. Eur J Pediatr. (2021) 180(8):2453–61. doi: 10.1007/s00431-021-04045-8
72. Ochab M, Wajs W. Expert system supporting an early prediction of the bronchopulmonary dysplasia. Comput Biol Med. (2016) 69:236–44. doi: 10.1016/j.compbiomed.2015.08.016
73. Peng HB, Zhan YL, Chen Y, Jin ZC, Liu F, Wang B, et al. Prediction models for bronchopulmonary dysplasia in preterm infants: a systematic review. Front Pediatr. (2022) 10:1–12. doi: 10.3389/fped.2022.856159
74. Jassem-Bobowicz JM, Klasa-Mazurkiewicz D, Żawrocki A, Stefańska K, Domżalska-Popadiuk I, Kwiatkowski S, et al. Prediction model for bronchopulmonary dysplasia in preterm newborns. Child Basel Switz. (2021) 8(10):886. doi: 10.3390/children8100886
75. Gao Y, Liu D, Guo Y, Cao M. Risk prediction of bronchopulmonary dysplasia in preterm infants by the nomogram model. Front Pediatr. (2023) 11:1117142. doi: 10.3389/fped.2023.1117142
76. Ou W, Lei K, Wang H, Ma H, Deng X, He P, et al. Development of a blood proteins-based model for bronchopulmonary dysplasia prediction in premature infants. BMC Pediatr. (2023) 23(1):304. doi: 10.1186/s12887-023-04065-3
77. Romijn M, Dhiman P, Finken MJJ, van Kaam AH, Katz TA, Rotteveel J, et al. Prediction models for bronchopulmonary dysplasia in preterm infants: a systematic review and meta-analysis. J Pediatr. (2023) 258:113370. doi: 10.1016/j.jpeds.2023.01.024
78. Laughon MM, Langer JC, Bose CL, Smith PB, Ambalavanan N, Kennedy KA, et al. Prediction of bronchopulmonary dysplasia by postnatal age in extremely premature infants. Am J Respir Crit Care Med. (2011) 183(12):1715–22. doi: 10.1164/rccm.201101-0055OC
79. Jensen EA, Dysart K, Gantz MG, McDonald S, Bamat NA, Keszler M, et al. The diagnosis of bronchopulmonary dysplasia in very preterm infants. An evidence-based approach. Am J Respir Crit Care Med. (2019) 200(6):751–9. doi: 10.1164/rccm.201812-2348OC
80. Greenberg RG, McDonald SA, Laughon MM, Tanaka D, Jensen E, Van Meurs K, et al. Online clinical tool to estimate risk of bronchopulmonary dysplasia in extremely preterm infants. Arch Dis Child Fetal Neonatal Ed. (2022) 107(6):638–43. doi: 10.1136/archdischild-2021-323573
81. Álvarez-Fuente M, Moreno L, Mitchell JA, Reiss IK, Lopez P, Elorza D, et al. Preventing bronchopulmonary dysplasia: new tools for an old challenge. Pediatr Res. (2019) 85(4):432–41. doi: 10.1038/s41390-018-0228-0
82. NCI-MATCH Precision Medicine Clinical Trial—NCI. (2015). (Cited January 8, 2024). Available online at: https://www.cancer.gov/about-cancer/treatment/nci-supported/nci-match
83. Pollard TJ, Johnson AEW, Raffa JD, Celi LA, Mark RG, Badawi O. The eICU collaborative research database, a freely available multi-center database for critical care research. Sci Data. (2018) 5(1):180178. doi: 10.1038/sdata.2018.178
84. Leigh RM, Pham A, Rao SS, Vora FM, Hou G, Kent C, et al. Machine learning for prediction of bronchopulmonary dysplasia-free survival among very preterm infants. BMC Pediatr. (2022) 22(1):542. doi: 10.1186/s12887-022-03602-w
85. Sun S, Ji W, Tang L, Zhang X, Zhang Y, Feng R. An interpretable causal approach for bronchopulmonary dysplasia prediction. 2022 IEEE International Conference on Bioinformatics and Biomedicine (BIBM) (2022):1193–200. (Cited January 8, 2024). Available online at: https://ieeexplore.ieee.org/document/9995412
86. Shepherd EG, De Luca D. New imaging tools allow bronchopulmonary dysplasia to enter the age of precision medicine. Am J Respir Crit Care Med. (2020) 202(7):924–6. doi: 10.1164/rccm.202005-2067ED
87. Palma JP, Benitz WE, Tarczy-Hornoch P, Butte AJ, Longhurst CA. Neonatal informatics: transforming neonatal care through translational bioinformatics. NeoReviews. (2012) 13(5):e281–4. doi: 10.1542/neo.13-5-e281
88. Stevenson AG, Tooke L, Edwards EM, Mangiza M, Horn D, Heys M, et al. The use of data in resource limited settings to improve quality of care. Semin Fetal Neonatal Med. (2021) 26(1):101204. doi: 10.1016/j.siny.2021.101204
89. Fang JL, Chuo J. Using telehealth to support pediatricians in newborn care. Curr Probl Pediatr Adolesc Health Care. (2021) 51(1):100952. doi: 10.1016/j.cppeds.2021.100952
90. Coppersmith NA, Sarkar IN, Chen ES. Quality informatics: the convergence of healthcare data, analytics, and clinical excellence. Appl Clin Inform. (2019) 10(2):272–7. doi: 10.1055/s-0039-1685221
91. Leung K, Lu-McLean D, Kuziemsky C, Booth RG, Collins Rossetti S, Borycki E, et al. Using patient and family engagement strategies to improve outcomes of health information technology initiatives: scoping review. J Med Internet Res. (2019) 21(10):e14683. doi: 10.2196/14683
92. NICHD Neonatal Research Network. Generic database: a survey of morbidity and mortality in very low birth weight infants. Report no.: NCT00063063. (2023). (Cited May 8, 2023). Available online at: https://clinicaltrials.gov/ct2/show/NCT00063063
93. Shah PS, Lee SK, Lui K, Sjörs G, Mori R, Reichman B, et al. The international network for evaluating outcomes of very low birth weight, very preterm neonates (iNeo): a protocol for collaborative comparisons of international health services for quality improvement in neonatal care. BMC Pediatr. (2014) 14:1–11.doi: 10.1186/1471-2431-14-110
94. Hei M, Li X, Shi Y, Cao Y, Sun J, Wu H, et al. Chinese neonatal network: a national protocol for collaborative research and quality improvement in neonatal care. BMJ Open. (2022) 12(5):e051175. doi: 10.1136/bmjopen-2021-051175
95. Modi N. Information technology infrastructure, quality improvement and research: the UK national neonatal research database. Transl Pediatr. (2019) 8(3):193–8. doi: 10.21037/tp.2019.07.08
96. Data Collection: Swiss Society of Neonatology. (Cited May 10, 2023). Available online at: https://www.neonet.ch/swissneonet/data-collection
98. Sarkar IN, Chen ES, Rosenau PT, Storer MB, Anderson B, Horbar JD. Using arden syntax to identify registry-eligible very low birth weight neonates from the electronic health record. AMIA Annu Symp Proc AMIA Symp. (2014) 2014:1028–36.25954412
99. Battersby C, Statnikov Y, Santhakumaran S, Gray D, Modi N, Costeloe K. The United Kingdom national neonatal research database: a validation study. PLoS One. (2018) 13:1–19. doi: 10.1371/journal.pone.0201815
100. Guaman MC, Pishevar N, Abman SH, Keszler M, Truog WE, Panitch H, et al. Invasive mechanical ventilation at 36 weeks post-menstrual age, adverse outcomes with a comparison of recent definitions of bronchopulmonary dysplasia. J Perinatol Off J Calif Perinat Assoc. (2021) 41(8):1936–42. doi: 10.1038/s41372-021-01102-w
101. Collaco JM, Agarwal A, Austin ED, Hayden LP, Lai K, Levin J, et al. Characteristics of infants or children presenting to outpatient bronchopulmonary dysplasia clinics in the United States. Pediatr Pulmonol. (2021) 56(6):1617–25. doi: 10.1002/ppul.25332
102. Guaman MC, Gien J, Baker CD, Zhang H, Austin ED, Collaco JM. Point prevalence, clinical characteristics, and treatment variation for infants with severe bronchopulmonary dysplasia. Am J Perinatol. (2015) 32(10):960–7. doi: 10.1055/s-0035-1547326
103. Lavilla OC, Aziz KB, Lure AC, Gipson D, de la Cruz D, Wynn JL. Hourly kinetics of critical organ dysfunction in extremely preterm infants. Am J Respir Crit Care Med. (2022) 205(1):75–87. doi: 10.1164/rccm.202106-1359OC
104. OHDSI—Observational Health Data Sciences and Informatics. (Cited January 8, 2024). Available online at: https://www.ohdsi.org/
105. Data Standardization—OHDSI. (Cited January 8, 2024). Available online at: https://www.ohdsi.org/data-standardization/
106. Onland W, Debray TP, Laughon MM, Miedema M, Cools F, Askie LM, et al. Clinical prediction models for bronchopulmonary dysplasia: a systematic review and external validation study. BMC Pediatr. (2013) 13:207. doi: 10.1186/1471-2431-13-207
107. Wells AH. Systematized nomenclature of pathology. Conversion to the computer language of medicine. Minn Med. (1972) 55(6):585–90.5033048
108. Forrey AW, McDonald CJ, DeMoor G, Huff SM, Leavelle D, Leland D, et al. Logical observation identifier names and codes (LOINC) database: a public use set of codes and names for electronic reporting of clinical laboratory test results. Clin Chem. (1996) 42(1):81–90. doi: 10.1093/clinchem/42.1.81
Keywords: informatics, bronchopulmonary dysplasia, chronic lung disease, premature neonate, clinical decision
Citation: Moreira AG, Husain A, Knake LA, Aziz K, Simek K, Valadie CT, Pandillapalli NR, Trivino V and Barry JS (2024) A clinical informatics approach to bronchopulmonary dysplasia: current barriers and future possibilities. Front. Pediatr. 12:1221863. doi: 10.3389/fped.2024.1221863
Received: 13 May 2023; Accepted: 23 January 2024;
Published: 12 February 2024.
Edited by:
Minesh Khashu, University Hospitals Dorset NHS Foundation Trust, United KingdomReviewed by:
Enrique Gomez-Pomar, University of Kentucky, United States© 2024 Moreira, Husain, Knake, Aziz, Simek, Valadie, Pandillapalli, Trivino and Barry. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alvaro G. Moreira bW9yZWlyYWFAdXRoc2NzYS5lZHU=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.