
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 28 April 2023
Sec. General Pediatrics and Pediatric Emergency Care
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.970867
 Hairong Gong1,†
Hairong Gong1,† Yuan Wang2,†
Yuan Wang2,† Yongzhen Li3
Yongzhen Li3 Pengpeng Ye2
Pengpeng Ye2 Li Xie4
Li Xie4 Guoping Lu1
Guoping Lu1 Jing Liu1
Jing Liu1 Jun Song1
Jun Song1 Xiaowen Zhai1
Xiaowen Zhai1 Hong Xu1*Leilei Duan2*
Hong Xu1*Leilei Duan2*
Background: Understanding the occurrence and severity of child injuries is the cornerstone of preventing child injuries. Currently, there is no standardized child injury surveillance dataset in China.
Methods: Multistage consultation by a panel of Chinese experts in child injury to determine items to include in the core dataset (CDS) was performed. The experts participated in two rounds of the modified Delphi method comprising a consultation questionnaire investigation (Round 1) and a face-to-face panel discussion (Round 2). Final consensus was established based on the opinions of the experts regarding the modified CDS information collection items. Enthusiasm and authority exhibited by the experts were evaluated by the response rate and using the expert authority coefficient, respectively.
Results: The expert panel included 16 experts in Round 1 and 15 experts in Round 2. The experts during both rounds had a high degree of authority, with an average authority coefficient of 0.86. The enthusiasm of the experts was 94.12%, and the proportion of suggestions reached 81.25% in Round 1 of the modified Delphi method. The draft CDS evaluated in Round 1 included 24 items, and expert panelists could submit recommendations to add items. Based on findings in Round 1, four additional items, including nationality, residence, type of family residence, and primary caregiver were added to the draft of the CDS for Round 2. After Round 2, consensus was reached on 32 items arranged into four domains—general demographic information, injury characteristics, clinical diagnosis and treatment, and injury outcome—to include in the final CDS.
Conclusion: The development of a child injury surveillance CDS could contribute to standardized data collection, collation, and analysis. The CDS developed here could be used to identify actionable characteristics of child injury to assist health policymakers in designing evidence-based injury prevention interventions.
Child injury is the main cause of childhood hospitalization and death worldwide and has become an increasingly severe public health problem globally (1). More than 98% of child injury deaths occur in developing countries (2). In China, mortality for children under 18 years old was 11.42/100,000 in 2019 (3), driven by injury-related deaths, which are the leading cause of death for children under 6 years of age (1).
To effectively and systematically prevent child injuries, the first fundamental step is to understand factors surrounding their occurrence as well as factors that influence their severity (4, 5). The Injury Surveillance Systems help determine injury patterns and severity through continuous and systematic data collection, analysis, interpretation, and dissemination, as well as by providing necessary evidence to prescribe preventive measures. Although the National Injury Surveillance System (NISS) had been established in China since 2003, the all-age-grouped dataset lacks clinical characteristics and child growth and development information. Furthermore, most previous studies are either from non-tertiary hospitals focusing on the basic epidemiological characteristics of injury (6–8) or from general hospitals focusing on the disease burden collected in the all-age-grouped database (9–11). It is known that distinct behaviors and growth patterns in children cause the characteristics of injuries in children to be quite different from those in adults (12), creating an urgent need for the development of a standardized core dataset (CDS) for child injury surveillance. Establishing a more practical and routinely applied surveillance CDS for emergency departments is therefore essential for the collection of high-quality data on child injuries (13).
This study developed a surveillance CDS that is better suited to the characteristics and patterns of child injury and is more cohesive with emergency medical practice to provide insight into child injury prevention toward developing targeted strategies to control child injury.
A modified Delphi study is a structured, questionnaire-based method for converting the opinions of multiple experts into a consensus. Recently, the modified Delphi method has gained popularity in medical research. In this study, a core study group designed a two-round modified Delphi study, which was conducted between June 2020 and January 2021, to achieve consensus on a CDS for child injury surveillance (Figure 1). The core study group comprised five members involved in this project who were not among the experts who served as panelists for the modified Delphi study.
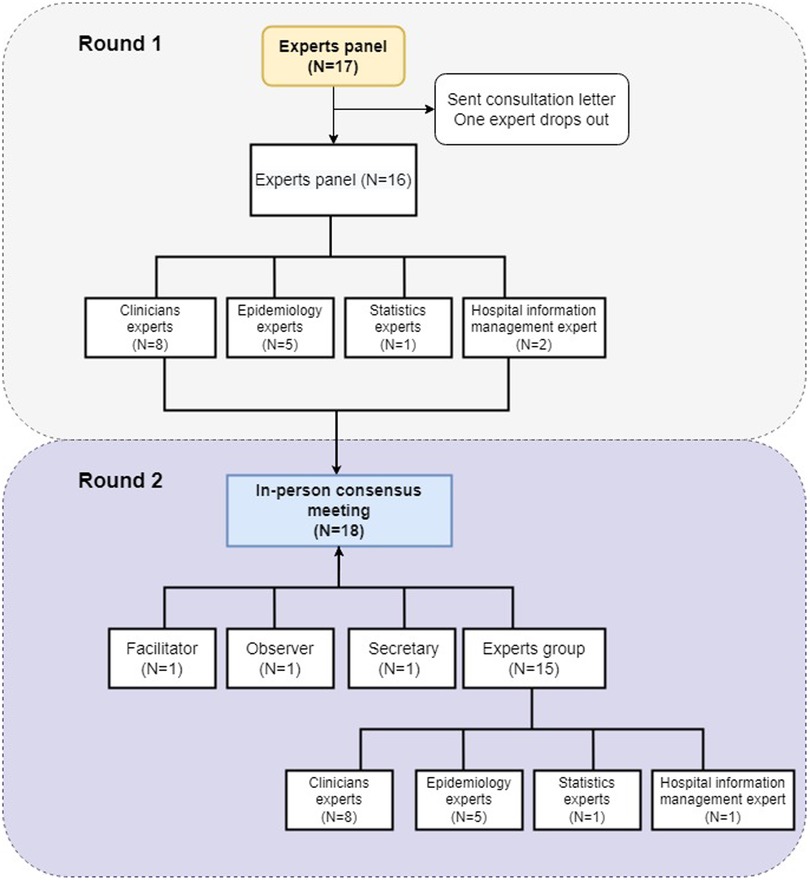
Figure 1. Flow chart of the modified Delphi method used to develop the Child Injury Surveillance CDS. Gray and purple indicate Round 1 and Round 2 of the Modified Delphi study, respectively.
A multidisciplinary expert panel to develop the CDS was recruited using an academic reputation-based snowball sampling method. The inclusion criteria for members of the expert panel were (1) clinicians whose work had been related to the child injury disease field for >5 years and who were familiar with the clinical characteristics and prognoses of child injuries; (2) researchers who engaged in epidemiological research of child injury or in research related to prevention and control of injuries for the Center for Disease Control and Prevention Bureau; (3) biostatisticians with ≥5 years of experience in public health; or (4) information technology engineers with >5 years of experience managing Hospital Information Systems.
Creation of the injury surveillance CDS involved three main steps: (1) collect and determine candidate items that could be included in the CDS of child injury surveillance; (2) validate the chosen items by collecting expert opinions using a questionnaire (Round 1); and (3) convene a meeting of experts to discuss the revised surveillance CDS and determine the final CDS items (Round 2). During conduction of this study, we followed the basic principles of the Delphi method: anonymous rating, multiple rounds of consultation, and providing feedback to participants before starting the next round of consultation.
The core study group used information from a literature review (14–18) and from combing of the current NISS dataset in China early during the project (19) and combined this with the epidemiological and clinical characteristics of child injury to create a first draft of items to include in the CDS for the Delphi expert consultation questionnaire. In accordance with the World Health Organization (WHO) and Center for Disease Control Injury Surveillance Guidelines, fundamental characteristics of an injury surveillance system, such as simplicity, flexibility, acceptability, reliability, utility, sustainability, and timeliness, were thoroughly considered when creating the draft (20).
A consultation questionnaire was sent to the panel of experts between October 2020 and November 2020 via email. Expert consultants were given project guidance and asked to complete the consultation questionnaire. The project guidance presented the context, objective, scope, and significance of the project and consultation as well as provided a concise explanation of the significance and value of expert opinions. The consultation questionnaire contained the fundamental information of experts, drafted questions for capturing child injury surveillance items in the CDS, and self-evaluations of experts' familiarity with consulting problems and evaluation criteria. Experts' familiarity was rated on a five-level scale, and the evaluation was based on seven factors, including epidemiology, clinic, statistics, and monitoring systems with varying quantitative values. The importance of each item in the consultation questionnaire was rated on a 5-point Likert scale, where 5 = very important, 4 = important, 3 = moderately important, 2 = unimportant, and 1 = very unimportant. Meanwhile, opinion boxes were set under each item for experts to write in suggestions regarding the items.
Before Round 2, the core group modified the items in the draft CDS according to the opinions collected from the expert group in Round 1, and the new draft CDS was provided to the expert panel for discussion during an in-person meeting held in January 2021. The final CDS items reflect the votes of the expert panel.
Demographic characteristics of the expert panelists were collected and analyzed. The frequencies, percentages, interquartile ranges, and medians of expert responses from the Round 1 questionnaire were calculated to determine the consistency of the experts on each item. If the collective consistency of adding a new item had a mean importance index >3.75 points (75% of the 5-point Likert scale) or deleting an item had a mean importance index <3.75 points, the opinion was accepted and the corresponding item was modified before Round 2. The expert positivity index was calculated as the response rate on the expert consultation questionnaire, and >70% response rate was interpreted as high motivation. The authoritative indicators of the experts were expressed by the coefficient of reliability (Cr), which was represented by the results of the self-evaluations of the experts. Cr was determined using the coefficient of adjudication (Ca) and coefficient of sense (Cs), which reflect the familiarity of the experts with the consulting content, using the equation Cr = (Ca + Cs)/2. Cr values ≥0.7 were considered acceptable (21, 22). The coefficient of adjudication (Ca) was composed of four coefficients: research evidence, practical experience, clinical guidelines, and instinct. Different weighting scales were assigned to each item according to its influence intensity. All statistical analyses were performed using Stata 13.0 software (Stata Corporation, College Station, TX, United States). GraphPad Prism 8.0.1 (GraphPad Software, San Diego, CA, United States) was used to plot the data.
We invited 18 experts to participate in two rounds of the Delphi method as part of an expert panel. In Round 1, 16 experts participated, and 15 experts participated in Round 2. Clinicians, injury epidemiologists, health statisticians, and information technology engineers were all represented on the expert panel during both rounds. Members in the expert panel were from a wide range of provinces in China, including Beijing, Shanghai, Guangdong, Zhejiang, and Shaanxi, with relatively equal numbers of men and women (Supplementary Table S1). All of the experts had at least a master's degree, and 56.3% (9/16) and 66.7% (10/15) of the experts in Round 1 and Round 2, respectively, had a doctoral degree. The number of years of work experience of the experts ranged from 5 to 30 years, with 18.3 and 21.1 average working years of experience among the experts in Round 1 and 2, respectively. Table 1 and Supplementary Table S1 present the demographic characteristics of the expert panelists during both rounds of the modified Delphi study.
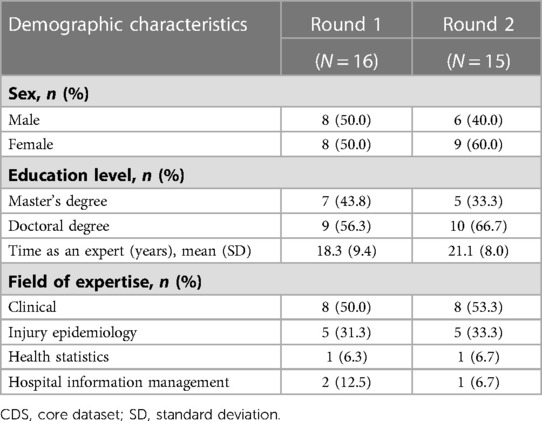
Table 1. Demographic characteristics of modified Delphi expert panelists who participated in developing the child injury surveillance CDS.
An implementation and reliability analysis was conducted by evaluating the authority of experts (Supplementary Tables S2, S3). Overall, 17 questionnaires were sent out and 16 were collected at the end of Round 1, yielding an overall response rate of 94.11%. Among the experts who returned the questionnaires, 13 (81.25%) experts provided additional suggestions. The authority coefficient of each expert was calculated by assigning different-weight coefficients to academic degree held by the expert. The Cr of the experts in this study ranged from 0.625–1.0, and the mean Cr of the 16 experts who participated in Round 1 was 0.86 (SD = 0.10) (Table 2), indicating a high degree of authority among the expert panel.
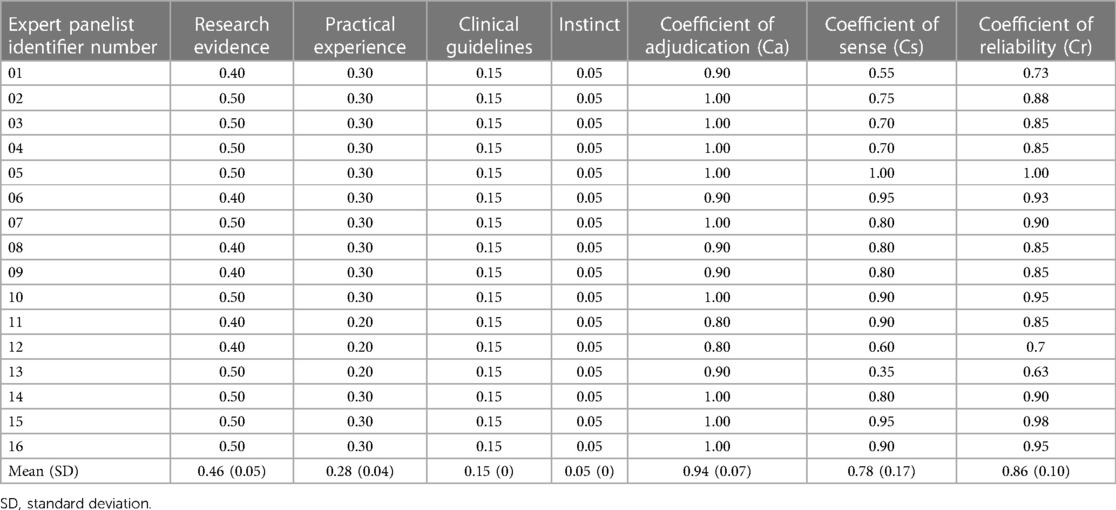
Table 2. Quantitative assessment of familiarity of modified Delphi study panelists with child injury.
A draft CDS of Child Injury Surveillance was created by integrating data mined by the core study group to create a four-part document that included a total of 24 items. Part I collected eight items regarding general demographic information of the children and their parents or guardians, including (1) outpatient admission number, (2) sex, (3) date of birth, (4) weight, (5) height, (6) residence, (7) nationality, and (8) parent education level. Part II collected eight items regarding the characteristics of the injury, including (1) time of injury, (2) time of hospital visit, (3) mechanism of injury, (4) location of injury, (5) activity at the time of the injury, (6) intention of the injury, (7) caregiver type, and (8) caregiver status. Part III collected four items regarding clinical diagnosis and treatment of the injury, including (1) nature of the injury, (2) body parts affected by injuries, (3) body systems affected by injury, and (4) the Pediatric Trauma Score (PTS), which can easily, quickly, and accurately identify the severity of traumatic injuries in children. Part IV collected four items regarding the outcome of the injury, including (1) severity of the injury, (2) clinical diagnosis, (3) injury outcome, and (4) date of injury outcome. Meanwhile, four additional administrative items were collected, including (1) the monitoring hospital number, (2) report card number, (3) reporter, and (4) date.
A flow chart depicting the modified Delphi method used in this study is provided in Figure 1. The expert panel comprehensively evaluated the importance and rationality of each of the 28 items in the draft CDS and provided detailed suggestions regarding the deletion and improvement of items. For Part I, the most highly rated demographic items were sex (81%), date of birth (75%), outpatient admission number (69%), weight (63%), and medical number (63%). The experts suggested that the CDS collects information of child caregiver educational background, age, intellectual development, education level or school status of the child, siblings, current residence, race, etc. In Part II, the panel determined that the most important characteristics of the injury to collect were injury time, reason, location, time of patient's visit, and the activity when the injury occurred, all of which scored >88%. The status of the caregiver at the time of injury also scored highly (75%), followed by the primary family caregiver (63%) and the main caregiver at the time of injury (63%). Whether alcohol use was involved in the injury scored the lowest among the items in Part II (50%). All four of the items in Part III were considered very important or important by the experts, reflecting the high relevance of collecting adequate data regarding the clinical diagnosis and treatment of the injury. In Part IV, the panel determined that the most important items related to injury outcome were severity of injury (94%), outcome of injury (94%), clinical diagnosis of injury (88%), and occurrence date of outcome of injury (69%) (Figure 2). The draft CDS of Child Injury Surveillance was revised based on this feedback from Round 1, which included adding ethnicity, place of residence, family residence type, and child's primary caregiver to patient demographic information.
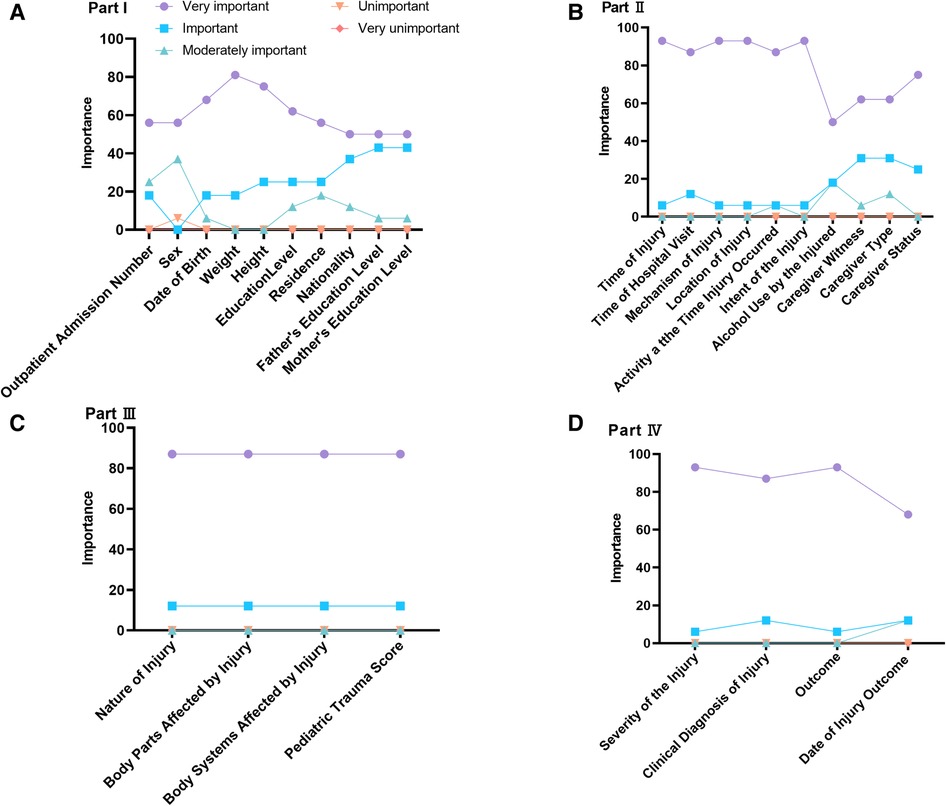
Figure 2. Importance of evaluating items in the draft child injury surveillance CDS based on expert opinion. (A) Part I: General patient information; (B) Part II: Basic injury information; (C) Part III: Clinical injury information; (D) Part IV: Injury outcome information.
Following an interview schedule prepared in advance, we conducted Round 2 of the modified Delphi study as an online, in-person consensus meeting for 3 h in January 2021. An observer and a secretary were present to document the interactions among the expert panel and facilitator. There was no conflict of interest for any of the expert panelists nor for the facilitator, observer, or secretary. At this meeting, 30 proposed items for the CDS were evaluated. After extensive discussion, 32 final core items were included in the CDS of Child Injury Surveillance (Table 3).
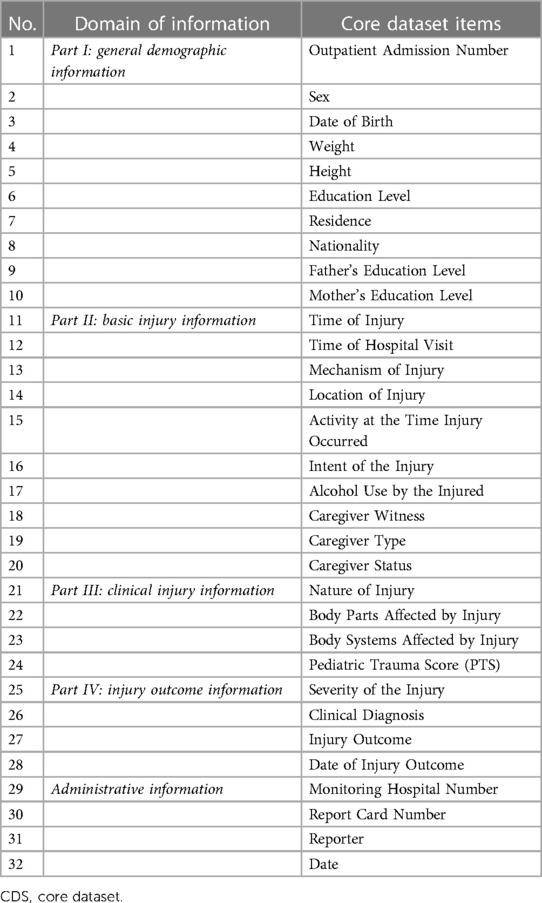
Table 3. Items included in final version of Child Injury Surveillance CDS.
Because injuries to children differ from those in adults, precise information related to child-specific injuries, such as activity at the time of injury, guardian status, and injury characteristics, are needed to develop measures to prevent child injuries. Previous studies have shown that children of different ages are vulnerable to different injury types or injury places, and that the characteristics of injuries also differ according to age (7, 23, 24). For example, children of primary school age are vulnerable to bite injuries, whereas the proportions of traffic injuries or suicide increase between 15 and 17 years of age, and accidental injuries such as falls are more common in infants (25). Therefore, tailored prevention and policy intervention are needed to reduce a wide array of child injuries. Here, we developed a CDS of Child Injury Surveillance by amending a draft CDS on the basis of expert opinions and suggestions that can offer comprehensive and uniform data collection to create a robust dataset that may be used to understand and prevent child injury.
Previous studies have reported that occupation and income level of families are correlated with child injury (26, 27); thus, collecting residence location could reflect socioeconomic status and inform on whether these factors may indeed influence child injury. Studies have also shown that unintentional child injuries may be reduced by parents teaching safety rules (28, 29). Also, the parents' level of education can influence the security of a child's environment, including safety standards and level of supervision, which should be significant in determining child injuries. Therefore, we included the education level of the parents/guardians as relevant demographic information in the final CDS to allow investigating the correlation between the parent educational level and injury characteristics and to promote targeted prevention.
Traditional and modified Delphi methods are often used in medical and health services research (30–32) to facilitate effective decision making in situations where conflicting or inadequate information exists. This study is the first to use the modified Delphi method to develop a child-specific injury surveillance CDS. By improving and refining the system for multidepartment, coordinated data collection regarding child injuries, the CDS provides a systematic, comprehensive, scientific, and accurate mechanism to improve our understanding of the characteristics of child injury to design prevention strategies.
Our study has some limitations. First, the CDS would require additional work from emergency department staff who already have a heavy work load. With this in mind, we meticulously designed and reviewed the CDS items, and the majority of them can be extracted automatically from the electronic health record system. Second, we did not include the specific information that resides within each of the included items, such as expansion of the mechanism (reason, cause) code to the second level of detail, which would enhance the understanding of the problem and thus inform prevention strategies. We intend to introduce additional datasets containing comprehensive information on child injury surveillance in the future. Third, an important study limitation is that the panel only included experts from China, while an international panel would have been preferable. Hence, this may impact the generalizability of the CDS.
Injury is an important public health problem that endangers child health. The surveillance of child injury and various epidemiological studies have contributed to preventing child injury and reducing disease burden. However, retrospective information collected by questionnaires often has recall bias, and memory discrepancies may also result in errors in the recall of guardians or teachers. As treatment of child injury is mainly in the outpatient or emergency settings, establishing this standardized, integrated child injury surveillance dataset and using it in hospital emergency departments can capture demographic and clinical characteristics of child injury. Consequently, the CDS may contribute to tailored intervention strategies to prevent child injury by systematically collating comprehensive, unbiased data to identify at-risk populations.
In conclusion, we developed a child injury surveillance CDS using the modified Delphi method and achieved a multidisciplinary, multiexpert consensus. The child injury surveillance CDS could provide a foundation for establishing standardized and high-quality child injury data collection, collation, and analysis to identify actionable characteristics of child injury that can assist health policymakers in designing evidence-based injury prevention interventions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
HG, YW, LD, and HX conceptualized and designed the study, coordinated and supervised data collection and interpretation, drafted the initial manuscript and reviewed and revised the manuscript. YL, PY, GL, JL, JS, and XZ designed the data collection instruments and collected data. YL and LX carried out the statistical analyses and interpretation. XZ and YW critically reviewed the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
This study was financially supported by the Scientific Project of Shanghai Municipal Health Commission (Grant No. 202140086) and the Scientific Project of Children's Hospital of Fudan University Grant (Grant No. 2020ZBDL12).
We thank Chuyue Shen (The University of Melbourne, Faculty of Science) and Rui Yang (Children's Hospital of Fudan University) for assisting in data manipulation and manuscript elaboration.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.970867/full#supplementary-material.
1. Linnan H, Duan J, Chen X, Yan S. Child injury surveillance that guides interventions: the Beijing primary healthcare experience. Injury Prev. (2011) 17:74–8. doi: 10.1136/ip.2010.026443
2. Fei F, Zhong J, Yu M, Gong W, Wang M, Pan J, et al. Impact of injury-related mortality on life expectancy in Zhejiang, China based on death and population surveillance data. BMC Public Health. (2018) 18:24. doi: 10.1186/s12889-017-4566-3
3. Ji C, Duan L, Lu Z, Ye P, Wang Y, Er Y. Analysis of injury epidemiological characteristics in children aged 6-17 based on data from the national injury surveillance system in China from 2015 to 2018. Chin J Sch Health. (2020) 41:979–82. doi: 10.16835/j.cnki.1000-9817.2020.07.006
4. Schwarz DF. It is time to get serious about childhood injury surveillance in the United States. Am J Prev Med. (1995) 11:134–5. doi: 10.1016/S0749-3797(18)30490-2
5. Jagnoor J, Ponnaiah M, Varghese M, Ivers R, Kumar R, Prinja S, et al. Potential for establishing an injury surveillance system in India: a review of data sources and reporting systems. BMC Public Health. (2020) 20:1909. doi: 10.1186/s12889-020-09992-9
6. Jin Y, Ye PP, Deng X, Wang Y, Er YL, Ji CR, et al. Prevalence of injury among children in 28 counties of 6 provinces in China in 2017. Chin J Epidemiol. (2021) 42:1392–400. doi: 10.3760/cma.j.cn112338-20201112-01325
7. Gong H, Lu G, Ma J, Zheng J, Hu F, Liu J, et al. Causes and characteristics of children unintentional injuries in emergency department and its implications for prevention. Front Public Health. (2021) 9:669125. doi: 10.3389/fpubh.2021.669125
8. Cheng P, Wang L, Ning P, Yin P, Schwebel DC, Liu J, et al. Unintentional falls mortality in China, 2006-2016. J Glob Health. (2019) 9(1):010603. doi: 10.7189/jogh.09.010603
9. Cai P, Wu X, Liu Z, Deng Y, Chen X, Yi G, et al. Analysis of the burden and trend of injury in Sichuan, China, from 2006 to 2015: results from the national injury surveillance system. BMJ Open. (2019) 9:e031184. doi: 10.1136/bmjopen-2019-031184
10. Fadel SA, Boschi-Pinto C, Yu S, Reynales-Shigematsu LM, Menon GR, Newcombe L, et al. Trends in cause-specific mortality among children aged 5–14 years from 2005 to 2016 in India, China, Brazil, and Mexico: an analysis of nationally representative mortality studies. Lancet. (2019) 393:1119–27. doi: 10.1016/S0140-6736(19)30220-X
11. Li Y, Pu M, Wang Y, Feng T, Jiang C. Analysis of the reduction in injury mortality disparity between urban and rural areas in developing China from 2010 to 2016. BMC Public Health. (2020) 20(1):903. doi: 10.1186/s12889-020-09027-3
12. Yin X, Li D, Zhu K, Liang X, Peng S, Tan A, et al. Comparison of intentional and unintentional injuries among Chinese children and adolescents. J Epidemiol. (2020) 30:529–36. doi: 10.2188/jea.JE20190152
13. Magnus D, Bhatta S, Mytton J, Joshi E, Bird EL, Bhatta S, et al. Establishing injury surveillance in emergency departments in Nepal: protocol for mixed methods prospective study. BMC Health Serv Res. (2020) 20:433. doi: 10.1186/s12913-020-05280-9
14. Mirani N, Ayatollahi H, Khorasani-Zavareh D. Injury surveillance information system: a review of the system requirements. Chin J Traumatol. (2020) 23:168–75. doi: 10.1016/j.cjtee.2020.04.001
15. McClure RJ, Mack K. Injury surveillance as a distributed system of systems. Inj Prev. (2016) 22(Suppl 1):i1–2. doi: 10.1136/injuryprev-2015-041788
16. Kirkwood G, Hughes TC, Pollock AM. Injury surveillance in Europe and the UK. BMJ. (2014) 349:g5337. doi: 10.1136/bmj.g5337
17. Horan JM, Mallonee S. Injury surveillance. Epidemiol Rev. (2003) 25:24–42. doi: 10.1093/epirev/mxg010
18. Mitchell RJ, Williamson AM, O'Connor R. The development of an evaluation framework for injury surveillance systems. BMC Public Health. (2009) 9:260. doi: 10.1186/1471-2458-9-260
19. Duan L, Deng X, Wang Y, Wu C, Jiang W, He S, et al. The national injury surveillance system in China: a six-year review. Injury. (2015) 46:572–9. doi: 10.1016/j.injury.2014.12.013
21. Zhao ZG, Cheng JQ, Xu SL, Hou WL, Richardus JH. A quality assessment index framework for public health services: a Delphi study. Public Health. (2015) 129:43–51. doi: 10.1016/j.puhe.2014.10.016
22. Sun ZQ, Wang LS. Comprehensive evaluation method and its application in medicine. Beijing: People's Medical Publishing House Co., Ltd (2014).
23. West BA, Rudd RA, Sauber-Schatz EK, Ballesteros MF. Unintentional injury deaths in children and youth, 2010-2019. J Safety Res. (2021) 78:322–30. doi: 10.1016/j.jsr.2021.07.001
24. Yin X, Dai W, Du Y, Li D. The injury mechanisms and injury pyramids among children and adolescents in Zhuhai city, China. BMC Public Health. (2021) 21:436. doi: 10.1186/s12889-021-10425-4
25. National Bureau of Statistics of China. Final Statistical Monitoring Report on the Implementation of China National Program for Child Development (2011–2020). (2021). Available at: http://www.stats.gov.cn/english/PressRelease/202112/t20211231_1825803.html (Accessed April 19, 2023)
26. Magnus D, Bhatta S, Mytton J, Joshi E, Bhatta S, Manandhar S, et al. Epidemiology of paediatric injuries in Nepal: evidence from emergency department injury surveillance. Arch Dis Child. (2021) 106:1050–5. doi: 10.1136/archdischild-2020-321198
27. Ghebreab L, Kool B, Lee A, Morton S. Risk factors of unintentional injury among children in New Zealand: a systematic review. Aust NZ J Publ Heal. (2021) 45:403–10. doi: 10.1111/1753-6405.13125
28. Zhou H, Fan L, Wu C, Luo A, Mo C, He G, et al. Understanding the associations among parents teaching safety rules to children, safety behaviors and unintentional injuries in Chinese preschool children. Prev Med. (2019) 118:98–103. doi: 10.1016/j.ypmed.2018.10.022
29. Morrongiello BA. Understanding Toddlers’ in-home injuries: II. Examining parental strategies, and their efficacy, for managing child injury risk. J Pediatr Psychol. (2004) 29:433–46. doi: 10.1093/jpepsy/jsh047
30. Maher TM, Whyte MKB, Hoyles RK, Parfrey H, Ochiai Y, Mathieson N, et al. Development of a consensus statement for the definition, diagnosis, and treatment of acute exacerbations of idiopathic pulmonary fibrosis using the Delphi technique. Adv Ther. (2015) 32:929–43. doi: 10.1007/s12325-015-0249-6
31. Gidman W, Shah S, Zhang L, McKendrick J, Cong Z, Cohan D, et al. Clinicians’ perspectives on cure in adult patients with acute lymphoblastic leukemia with minimal residual disease: a Delphi study. Adv Ther. (2019) 36:3017–29. doi: 10.1007/s12325-019-01099-x
Keywords: child injury, injury surveillance, modified Delphi method, core dataset, surveillance tool
Citation: Gong H, Wang Y, Li Y, Ye P, Xie L, Lu G, Liu J, Song J, Zhai X, Xu H and Duan L (2023) Development of a core dataset for child injury surveillance: a modified Delphi study in China. Front. Pediatr. 11:970867. doi: 10.3389/fped.2023.970867
Received: 27 September 2022; Accepted: 11 April 2023;
Published: 28 April 2023.
Edited by:
Raffaele La Russa, University of Foggia, ItalyReviewed by:
Joan Ozanne-Smith, Monash University, Australia© 2023 Gong, Wang, Li, Ye, Xie, Lu, Liu, Song, Zhai, Xu and Duan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Xu aHh1QHNobXUuZWR1LmNu Leilei Duan ZHVhbmxlaWxlaUBuY25jZC5jaGluYWNkYy5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.