 Katie M. Moynihan
Katie M. Moynihan Lisa S. Taylor
Lisa S. Taylor Bryan Siegel1,2
Bryan Siegel1,2 Efrat Lelkes
Efrat Lelkes Wynne Morrison
Wynne Morrison
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Pediatr., 11 January 2024
Sec. Pediatric Critical Care
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1325207
This article is part of the Research TopicWomen in Pediatric Critical Care: 2023View all 14 articles
Introduction: Advances in medical technology have led to both clinical and philosophical challenges in defining death. Highly publicized cases have occurred when families or communities challenge a determination of death by the irreversible cessation of neurologic function (brain death). Parallels can be drawn in cases where an irreversible cessation of cardiopulmonary function exists, in which cases patients are supported by extracorporeal cardiopulmonary support, such as extracorporeal membrane oxygenation (ECMO).
Analysis: Two cases and an ethical analysis are presented which compare and contrast contested neurologic determinations of death and refusal to accept the irreversibility of an imminent death by cardiopulmonary standards. Ambiguities in the Uniform Determination of Death Act are highlighted, as it can be clear, when supported by ECMO, that a patient could have suffered the irreversible cessation of cardiopulmonary function yet still be alive (e.g., responsive and interactive). Parallel challenges with communication with families around the limits of medical technology are discussed.
Discussion: Cases that lead to conflict around the removal of technology considered not clinically beneficial are likely to increase. Reframing our goals when death is inevitable is important for both families and the medical team. Building relationships and trust between all parties will help families and teams navigate these situations. All parties may require support for moral distress. Suggested approaches are discussed.
“Death is the one great certainty. The subject of powerful social and religious rituals and moving literature, it is contemplated by philosophers, probed by biologists and combated by physician”. Morris B. Abram 1981 (1)
“If one subject in health law and bioethics can be said to be at once well settled and persistently unresolved, it is how to determine that death has occurred”. Alexander Capron 2001 (2)
While death is “the one great certainty” of humanity, controversies exist surrounding accepted medical standards to define death (1–6). Biologically, somatic death is a gradual process whereby entropy overwhelms homeostasis as tissues variably endure oxygen deprivation (7). But rather than the state of isolated cells, societal death relates to the fate of a “person,” and “certainty that the process has become irreversible” has much greater clinical relevance (8, 9). The World Medical Assembly and the Uniform Determination of Death Act (UDDA) define death as having occurred when: “an individual … has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem” (4, 8, 9). Death by cardiopulmonary criteria is widely accepted due to the obvious bodily changes which occur after cessation of circulation. It is assumed that, when circulatory death occurs, neurological death will follow. Declaring death by neurologic criteria (DNC) can lead to controversy as the reverse is not always immediately true; some physiological processes, such as cardiac function, can continue if ventilator support is maintained. Numerous authors have argued that DNC is a social construct or legal fiction not synonymous with human death (3–6, 10–13), and some US states allow conscientious objection to DNC (14). Notwithstanding these and other challenges, empiric establishment of uniform standards of DNC (4, 13, 15) provided a societal definition for death of an individual which (1) offered closure for families, (2) provided a path to discontinue non-beneficial care to prevent overwhelming healthcare systems, (3) afforded legal protection for physicians, and (4) facilitated organ donation.
Extracorporeal Membrane Oxygenation (ECMO) is a highly technologic, invasive intervention that is often emergently instituted to temporarily replace pulmonary and cardiac function. Thus, this technology could contradict strict interpretation of the UDDA definition that complete, irreversible failure of the native heart or respiratory system functions constitutes death. A person who still has neurologic function (even if heavily sedated) is clearly neither intuitively or clinically dead, highlighting the challenges of the UDDA definition in light of modern technology (16–18). Though death during the hospitalization is certain as indefinite support is not feasible, arguably despite irreversible cardiorespiratory failure they are living on ECMO (19)—essential processes are maintained by a machine. The most recent update to the DNC Consensus Guideline has begun to acknowledge that some UDDA language may need updating or clarification, noting in the terminology section that they choose to use “permanence” rather than “irreversibility” in their language, and adding that medical interventions will not be used to attempt restoration of function (20).
In this paper, we describe and analyze cases where ECMO raises ethical issues after a disease process has led to total, irreversible loss of patient cardiopulmonary function and draw parallels with the evolution of DNC definitions (21). Both sets of circumstances highlight the difficulties—in both terminology and societal consensus—that occur with defining death as our technologic ability to support patients expands. ECMO support will inevitably result in some cases where the only thing ECMO achieves is delaying death, so considering such cases will be important in clinical care (16). We argue that lessons learned from DNC may apply in these ECMO cases and warrant a stakeholder-approved approach to exploring the novel use of therapies in children such as ECMO in the setting of irreversible cardiorespiratory failure that cannot be managed by means such as transplant or assist devices.
Baby TL was born with complex congenital heart disease. The blood supply to the heart relied entirely on pressure within a hypoplastic, dysfunctional right ventricle chamber. Survival was possible only with heart transplant, so he was listed immediately for cardiac transplantation. He deteriorated despite exhaustive attempts to medically manage his challenging circulation, and was emergently cannulated for extracorporeal membrane oxygenation (ECMO) for cardio-respiratory failure. Immediately following ECMO initiation, the right ventricle chamber was decompressed resulting in inadequate coronary blood flow, thus his heart infarcted. Baby TL remained asystolic with no cardiac electrical activity or pulsatility, i.e irreversible heart death, with no chance of recovery. The ECMO machine maintained circulation to his body, so he was warm and initiated some breaths on the ventilator, but required high doses of sedatives and was minimally interactive. The initial goal for ECMO was as a bridge to heart transplant, but he suffered kidney injury and was no longer a transplant candidate. Thus, baby TL had irreversible, permanent circulatory failure.
SB was a 16 year old girl with cystic fibrosis diagnosed in infancy. In adolescence, she developed progressive pancreatic insufficiency and did not adhere to medications, often presenting with diabetic ketoacidosis and developing significant malnutrition. SB also had recurrent pulmonary infections requiring frequent hospitalizations, and her pulmonary function tests indicated severe disease. A viral infection led to endotracheal intubation. With worsening hypoxemia and hypercarbia, she was urgently cannulated onto ECMO. Because of prior non-adherence and poor nutritional status, SB was deemed to not be a lung transplant candidate. Attempts to reduce sedation failed with symptomatic breathlessness despite continued invasive ventilation, although SB was occasionally able to interact with her family and friends. She continued to require ECMO for refractory hypoxemia, with no ability to wean support and no recovery seen after six weeks. Thus, SB had irreversible, permanent respiratory failure.
Many challenges associated with ECMO discontinuation for children with irreversible cardio-respiratory failure and no destination options parallel those in unilateral decision-making in DNC (Table 1). In this section we discuss how, although there is ethical justification for withdrawing non-beneficial ECMO support when all stakeholders are in agreement, if surrogates insist on continuation or value continued biological life, discontinuation of support over their objection is more ethically complex.
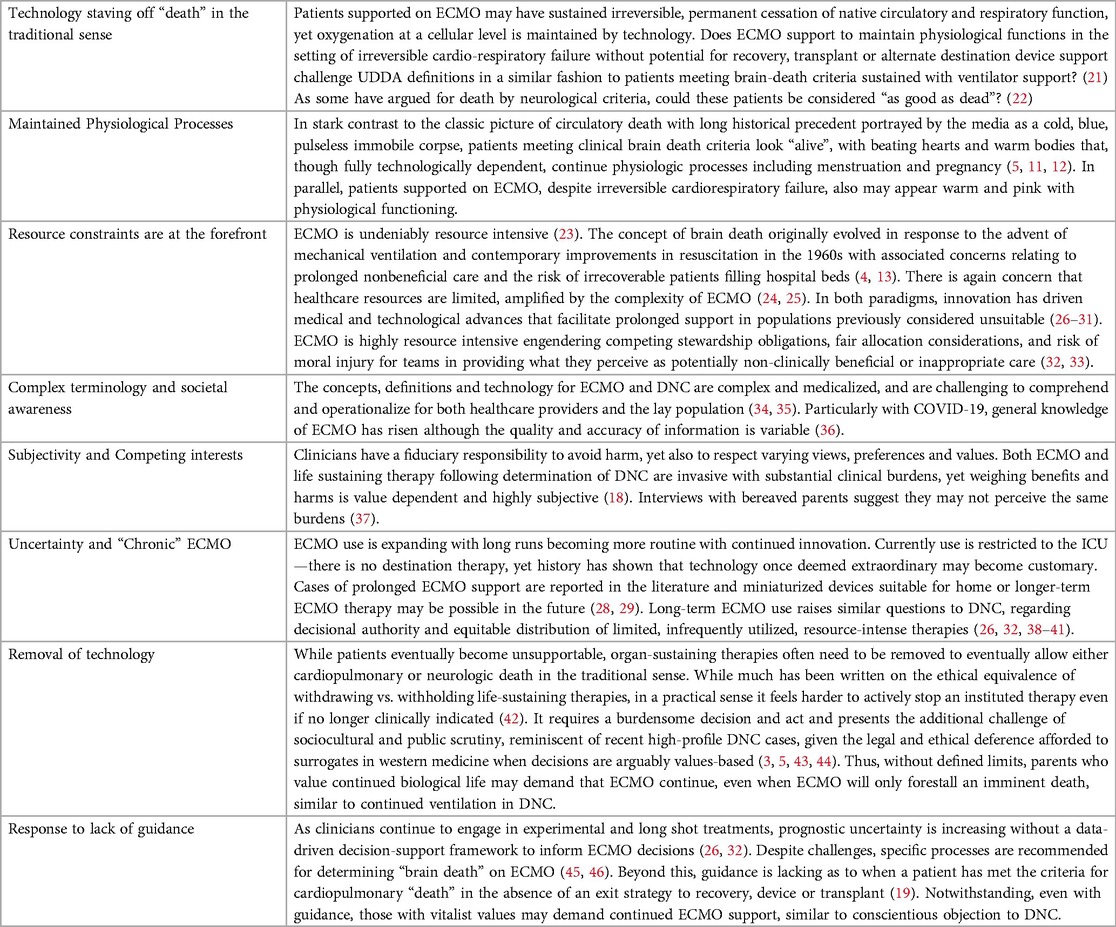
Table 1. Parallels between ECMO and ambiguity surrounding death by neurological criteria.
Traditionally, there are four potential goals for ECMO use: as a bridge to recovery, device, or transplant, or as a bridge to decision regarding one of these alternatives (47–49). Outside these parameters, continuing ECMO leads to death in the ICU within days to months, so is felt to be a prolongation of support that has no clinically beneficial outcome (16, 19, 26, 47, 50, 51). In current practice, with no long-term or home “destination” therapies yet available, it has often been referred to as a “bridge to nowhere” (21, 52–55). Defining acceptable ECMO use in children with irreversible cardio-respiratory failure and no bridging options is challenging at baseline with limited published guidance (26, 32), but is especially difficult when patients are neurologically intact (16, 17, 19, 56). As a pluralistic society, there are multiple ethically reasonable ways to approach a given situation. Recent ethical analyses focus on withdrawal of ECMO in awake adolescents/adults over their dissent which is uncommon in pediatric ECMO (16–19, 56). A comprehensive exploration of pediatric ethical issues using varying ethical frameworks and lenses is critical to ensure that rationales for decisions are robustly constructed (17, 18, 23, 55–57).
There are strong ethical arguments that clincians should not initiate or continue medically inappropriate therapies (33, 51, 56). However discontinuing technology is especially challenging in pediatrics, when it involves overriding patient/surrogate/parent's objections (50). Parental decision-making is generally given the utmost respect, unless the decisions are harming the child (18). Whether (and how much) ongoing, highly invasive support that only prolongs the dying process causes harm to the child is an important question and may be case-specific (58). ECMO support is often emergently initiated without time for fully informed conversations with a decision-maker (59) based on clinician judgment as to whether ECMO has a chance of leading to a good outcome. ECMO is a high-risk, high-cost, high-reward therapy at the intersection of standard ICU care and innovative therapy. So, if clinicians prognosticate with a high degree of certainty that the patient's organs will not recover, and the patient is not a transplant candidate, can prolonging death in this way be considered beneficial? For some, delaying death, even for a short while, may have value (a consequentialist, vitalist argument). A patient, or surrogate, may express a desire to be maintained on ECMO, and it may be physiologically feasible. Does a demand for a therapy to avoid death outweigh all else? The relative weight of benefits vs. burdens and what constitutes a good outcome or best interests are highly subjective (60, 61). Clinicians and surrogates may legitimately have different views of what is in the best interests of the patient (62, 63). The best interest standard is also applied differently internationally; in the US, clinicians typically override parental authority only if parental decisions cause substantial/significant harm to the child, while in some countries medical authority is given more priority (62, 64, 65). Resource limitations, however, may change this calculus as the impacts on other potential patients or the healthcare system affect what it is appropriate to provide for any individual (23). When death is unavoidable and proximate, does discontinuation of circulatory support fall within the zone of parental discretion or harm? (17, 56, 58, 66).
There are other ethical frameworks/reasoning that support clinician and institutional interests in establishing standardized indications for ECMO cannulation/discontinuation (18, 56). If the compassionate act, when death is inevitable, is to take the burden of end of life decision-making away from a family, the virtues of discernment, altruism, beneficence, honesty and integrity might justify allowing the medical team to determine that decannulation is appropriate. One could also consider the professional duties of a physician through a deontological model. It would not be possible, or desirable, to support every dying child with invasive technology to gain limited additional time, so the categorical imperative would argue that there is no moral obligation to continue ECMO when the therapy is not clinically beneficial. This also aligns with the professional medical ethics model of decision making (51, 67, 68). There is also a duty to be truthful—regarding prognosis, imminent death and false hope, especially in cases with little uncertainty about the outcome, such as with irreversible and permanent dependence on ECMO. Unfortunately, medical certainty does not always lead to trust in authority, and fear of litigation, social media responses, and ratings of physicians and hospitals have created a culture in which some clinicians are conflict averse. Healthcare professionals also have a duty to society. The extensive resources utilized in ECMO—beds, personnel, blood, medication, finances—are limited (23). ECMO is also a therapy with inequitable access (69, 70). When perceived to be not clinically beneficial, when death is imminent, continued utilization of ECMO then becomes unjust in a society where healthcare is a finite resource (23, 26). Providers have stewardship obligations—to be judicious in the use of these therapies, and thus discontinue ECMO when death is inevitable (26). Reductionists would reason, when death is inevitable, it should be respected as a biological truth. Judicious use of ECMO under standard care conditions in this way differs from resource limitation settings (or “crisis” standards of care) when the ethical weight of individual benefit vs. population utility shifts, requiring specific processes for procedural fairness (71).
In contrast to frameworks that support discontinuation of ECMO despite parental wishes, other approaches center on deference to parents or other surrogate decision-makers in deciding if and when these supports should be discontinued. As long as a patient is not suffering or being substantially harmed (highly subjective determinations) (72), a care ethics perspective suggests that the relationship between parent and child is sacred and that parents are uniquely situated to determine what is best for their child (73). Thus, even if the medical team determines that continuation of ECMO is inappropriate, the family may have a moral argument for continuing (74). Virtue ethics also requires humility; clinical judgment can be imprecise and flawed, and hubris in circumstances of uncertainty can damage the therapeutic alliance. In these situations, narrative ethics—understanding the patient/family's story, understanding how we arrived at this scenario, and similarly giving room to the narrative of all stakeholders—may mitigate some of the friction and moral distress. If the medical team does proceed with removal of ECMO, narrative ethics may provide a basis for much-needed discourse and support of the family. Contemporary medical advances mean it is also possible to be awake, interactive, and walking on ECMO which could be reasonably perceived as quality of life. But what if the only purpose of ECMO is sustaining perfusion without these other benefits? Vitalist values argue that mere biological function should be respected, and further complexity arises when patients, families or team members perceive any life to be of value in spite of dependence on technological support (19).
In all scenarios in the care of a patient with irreversible cardiorespiratory failure and permanent dependence on ECMO, all ethical frameworks are relevant; none are dispositive (50). Further, as with DNC, unilateral decision-making around ECMO over parents' values-based objections may be ethically fraught, warranting collaborative communication and shared decision-making approaches (75).
Just as opposition to DNC has evolved, we anticipate objections to ECMO discontinuation in children when used outside the four “bridges” to increase in the future. In this section we offer actionable practice changes. Ideally preemptive conversations both within teams and with patients/families can avoid conflict (57). Such discussions may help avoid escalating to advanced technologies in cases where there is little hope of benefit. However now more than ever there is abundant misinformation and unrealistic media portrayals as well as great scrutiny on medical decision-making and societal mistrust (34–36). Unjustified bias in healthcare decisions is well described, requiring medical providers to endeavor to re-establish societal trust in decision-making as well as advocate for accurate media representation (76–78). At the same time we are at a moment of great distress within the medical profession, with an epidemic of burnout, mental health crises, and colleagues leaving medicine (79). While rebuilding societal trust, we must also support our teams. Variability in practice and frequent conflict suggests no all-encompassing principle or theory will resolve all cases (50) and much ongoing collaborative, conceptual work is required to forge a path toward defining the appropriate use of ECMO in children. The goal is to avoid relying on conclusory definitions of death or candidacy limitations that might have the benefit of expedience for providers but are in conflict with patient and family values while also avoiding simply continuing a resource intensive, invasive therapy due to fear of conflict (26, 27).
We need to reframe our language to make clear that we are not burdening a family with a life/death decision but rather supporting them through an impossibly challenging situation. Death is often seen as a failure in our culture and medical practice, and has become highly medicalized (80). If we ask patients or their surrogates to decide to discontinue life-sustaining therapies, it is akin to asking them to choose if they or their loved one will die. This framing of discontinuation as optional unfairly burdens our patients and their families, and may be harmful (43, 81–83). Though input from patients and their surrogates is important in end-of-life decision making, connoting that death is a result of that choice is a fallacy. Our communication has to change when faced with decisions between two tragic options. In these situations, more than most, words matter. Death is a result of the underlying disease process, not decisions of the medical team, patient or family. To state otherwise unjustly burdens decision-makers by unfairly suggesting that outcomes depend on the decision. In the literature and when we approach our patients and their surrogates to discuss therapies such as ECMO or ventilation we use the term life-sustaining therapy or “extracorporeal life support” indicating that our emphasis is on life and death. This term is flawed, and we would be more accurate to discuss organ-sustaining therapies as is applied for or organ-replacing therapies such as “renal replacement therapy”. A change in our language would potentially allow us to advance our conversations and avoid implying that patients, surrogates or patients/carers and clinicians are “choosing” death.
We need to reframe our focus from fighting death at all costs to encouraging acceptance when it is inevitable (on the part of patients, families, and healthcare teams) (80, 84). Death indeed is the one great certainty, yet in modern medicine, survival is expected (80). Our fixation with avoiding mortality, preoccupation with quantity rather than quality of time, and the need for certainty may fail those patients that die and their families (84). We live in a pluralistic society with differing values and perspectives as to what is a life worth living, as well as emphasis on respecting values that many would consider idiosyncratic. With contemporary critique of DNC, our consideration of somatic death also needs to be reframed in response to evolving technological developments. Complete consensus in defining life and death is not feasible. Framing what the extent of disease process means for the patient as a person may be enough, in most circumstances, to reach agreement regarding compassionate ECMO discontinuation (21, 57). Communication guides suggest using clear language (e.g., “die” rather than ambiguous terms such as “pass away”) and describing the child as dying in spite of the support to ensure clarity and encouraging honest and courageous conversations about what is or is not possible with ECMO (59). Life and death scenarios are commonplace in the ICU. Transparent, open communication with families and team members, trust and alliance with families, and listening and understanding their stories are all crucial elements. While parents generally desire equal medical team input in shared decision-making for big picture decisions, such communication should be personalized (57, 85, 86). Religious or cultural contexts may also be a strong influence on surrogate or parent/caregiver's conceptualization of technology discontinuation. For some families using strong medical recommendations and working with respected community leaders are key steps (43, 87). For others, particularly when there is distrust in the medical team and perceived unfair treatment, parents may want to retain decision-making authority and resist directive approaches—which makes addressing the trust issues a priority. Finally, one must consider the potential for disparities in who is offered ongoing time on ECMO, particularly with known institutional, regional and individual provider variability in ECMO support (88). It is essential to ensure processes are in place to mitigate any potential for bias, and research is also warranted to follow if differential approaches are used for populations with different levels of resources, education, representation.
Disagreements related to continued ECMO indication may be some of the hardest we currently face in the ICU. The toll on the family and on the medical team may be immense. In circumstances where values based conflict is anticipated, we ought to use all tools at our disposal as early as possible to avoid relational harm and reach an ethically supportable resolution that mitigates provider moral distress (50). Paticulary with misrepresentation with the media (34, 35), as with DNC public perception and understanding of invasive organ support at the end of life is challenging and consensus on strategies to mitigate harm are important. This includes involvement of trusted persons, primary teams, or religious authorities, and consultation of both ethics and of pediatric palliative care may be invaluable for the patient, family, and team (32, 89–92). Striving for alignment with patients and their family during this time is crucial, and managing disagreements without abandoning patients and families is key. We must proceed with integrity, maintain patient dignity, and aggressively treat symptoms at end of life. A thoughtful, compassionate, patient/family-centered approach to providing a “good death” with ECMO discontinuation is a moral imperative (57, 93, 94). Moral distress for the medical team should be anticipated and may be particularly heightened when caring for alert patients. Though withdrawal and withholding are considered ethically equivalent (42), for some, active participation in the death of a patient who can communicate may be contrary to their personal beliefs. Our duties then extend to supporting the medical team through conversation, ethics consultation and involvement of palliative care providers.
In both cases ECMO was discontinued after significant, lengthy conversations with the patients' families (in Case 2, the patient chose not to be involved in discussions), the patients' primary teams, the ICU teams, palliative care team and ethics consultants. Primary bedside nurses and family supports, which included spiritual care and extended families, were able to join multiple family meetings. The medical team approached discussions emphasizing that death was inevitable rather than a decision to be made. Proceeding with removal of ECMO support thus was presented as the recommended next step. Neither family dissented. Timing of discontinuation was a collaborative decision with the family, allowing for specific hopes—the baby to have his first Christmas, and the teenager to say goodbye to loved ones (59). Discontinuation of support was planned in detail to prepare the team and the family with child-life services, music therapy, and palliative care supporting the family, patient, and team throughout this process (93). For both patients, their deaths appeared peaceful.
ECMO technologies can sustain physiological processes with a machine despite irreversible cardio-respiratory failure. Examining parallels with continued physiologic support after DNC and controversies that arise can be informative. We advocate that attention to semantics, societal education, and reframing the meaning of the disease for the individual child's life and therapy are needed. This requires proactive implementation of a systematic approach to decision-making. This will reduce decision-making burdens on families, minimize conflict around decannulation, enhance appropriate utilization of ECMO and intentionally focus on compassionate, value-centered, end of life care for patients on ECMO and their families.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
KM: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. LT: Conceptualization, Formal Analysis, Writing – review & editing. BS: Conceptualization, Formal Analysis, Writing – review & editing. NN: Writing – review & editing. EL: Conceptualization, Formal Analysis, Writing – review & editing. WM: Conceptualization, Formal Analysis, Funding acquisition, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
Publication was supported by the Justin Michael Ingerman Center for Palliative Care, Children's Hospital of Philadelphia to WM.
WM time is supported by the Justin Michael Ingerman Endowed Chair in Palliative Care.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1Details of both cases have been altered to preserve confidentiality.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Defining death: a report on the medical, legal and ethical issues in the determination of death. Washington, DC: President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research (1981).
2. Capron AM. Brain death—well settled yet still unresolved. N Engl J Med. (2001) 344(16):1244–6. doi: 10.1056/NEJM200104193441611
3. Truog RD. Defining death-making sense of the case of Jahi McMath. JAMA. (2018) 319(18):1859–60. doi: 10.1001/jama.2018.3441
4. Truog RD, Berlinger N, Zacharias RL, Solomon MZ. Brain death at fifty: exploring consensus. Controversy, and contexts. Hastings Cent Rep. (2018) 48(S4):S2–5. doi: doi: 10.1002/hast.942
5. Truog RD. Defining death: lessons from the case of Jahi McMath. Pediatrics. (2020) 146(Suppl 1):S75–80. doi: 10.1542/peds.2020-0818O
6. Truog RD, Krishnamurthy K, Tasker RC. Brain death—moving beyond consistency in the diagnostic criteria. JAMA. (2020) 324(11):1045–7. doi: 10.1001/jama.2020.11665
7. Hershey D, Lee WE III. Entropy, aging and death. Syst Res. (1987) 4(4):269–81. doi: 10.1002/sres.3850040406
8. Machado C, Korein J, Ferrer Y, Portela L, García Mde L, Chinchilla M, et al. The declaration of Sydney on human death. J Med Ethics. (2007) 33(12):699–703. doi: 10.1136/jme.2007.020685
9. Gilder SS. Twenty-second world medical assembly. Br Med J. (1968) 3(5616):493–4. doi: 10.1136/bmj.3.5616.493
10. Shewmon DA. Chronic “brain death”: meta-analysis and conceptual consequences. Neurology. (1998) 51(6):1538–45. doi: 10.1212/wnl.51.6.1538
11. Said A, Amer AJ, Masood UR, Dirar A, Faris C. A brain-dead pregnant woman with prolonged somatic support and successful neonatal outcome: a grand rounds case with a detailed review of literature and ethical considerations. Int J Crit Illn Inj Sci. (2013) 3(3):220–4. doi: 10.4103/2229-5151.119205
12. Staff L, Nash M. Brain death during pregnancy and prolonged corporeal support of the body: a critical discussion. Women Birth. (2017) 30(5):354–60. doi: 10.1016/j.wombi.2017.01.009
13. A definition of irreversible coma: report of the ad hoc committee of the harvard medical school to examine the definition of brain death. JAMA. (1968) 205(6):337–40. doi: 10.1001/jama.1968.03140320031009
14. Lewis A, Greer D. Current controversies in brain death determination. Nat Rev Neurol. (2017) 13(8):505–9. doi: 10.1038/nrneurol.2017.72
15. Lewis A, Bernat J, editors Death Determination by Neurologic Criteria: Areas of Consensus and Controversy (Advances in Neuroethics). 1st ed. Switzerland: Springer Nature (2022).
16. Childress A, Bibler T, Moore B, Nelson RH, Robertson-Preidler J, Schuman O, et al. From bridge to destination? Ethical considerations related to withdrawal of ECMO support over the objections of capacitated patients. Am J Bioeth. (2023) 23(6):5–17. doi: 10.1080/15265161.2022.2075959
17. Kingsley J, Berkman ER, Derrington SF. Battle of the bridge: ethical considerations related to withdrawal of ECMO support for pediatric patients over family objections. Am J Bioeth. (2023) 23(6):32–5. doi: 10.1080/15265161.2023.2201237
18. Wilkinson D, Fraser J, Suen J, Suzuki MK, Savulescu J. Ethical withdrawal of ECMO support over the objections of competent patients. Am J Bioeth. (2023) 23(6):27–30. doi: 10.1080/15265161.2023.2201194
19. Truog RD, Thiagarajan RR, Harrison CH. Ethical dilemmas with the use of ECMO as a bridge to transplantation. Lancet Respir Med. (2015) 3(8):597–8. doi: 10.1016/S2213-2600(15)00233-7
20. Greer DM, Kirschen MP, Lewis A, Gronseth GS, Rae-Grant A, Ashwal S, et al. Pediatric and adult brain death/death by neurologic criteria consensus guideline: report of the AAN guidelines subcommittee, AAP, CNS, and SCCM. Neurology. (2023). doi: 10.1212/wnl.0000000000207740. [Epub ahead of print]
21. Doernberg SN, Soled DR, Truog RD. Ethical issues in the transition to ECMO as a destination therapy. Am J Bioeth. (2023) 23(6):18–20. doi: 10.1080/15265161.2023.2201193
22. Kilcullen JK. “As good as dead” and is that good enough? Public attitudes toward brain death. J Crit Care. (2014) 29(5):872–4. doi: 10.1016/j.jcrc.2014.06.018
23. Andrist E. Fairly distributing the distributive justice argument permits stopping ECMO. Am J Bioeth. (2023) 23(6):65–7. doi: 10.1080/15265161.2023.2201226
24. Badulak J, Antonini MV, Stead CM, Shekerdemian L, Raman L, Paden ML, et al. Extracorporeal membrane oxygenation for COVID-19: updated 2021 guidelines from the extracorporeal life support organization. ASAIO J. (2021) 67(5):485–95. doi: 10.1097/MAT.0000000000001422
25. Ramanathan K, Antognini D, Combes A, Paden M, Zakhary B, Ogino M, et al. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir Med. (2020) 8(5):518–26. doi: 10.1016/S2213-2600(20)30121-1
26. Moynihan KM, Jansen M, Siegel BD, Taylor LS, Kirsch RE. Extracorporeal membrane oxygenation candidacy decisions: an argument for a process-based longitudinal approach. Pediatr Crit Care Med. (2022) 23(9):e434–9. doi: 10.1097/PCC.0000000000002991
27. Moynihan KM, Basu S, Kirsch R. Discretion over discrimination: toward good decisions for extracorporeal membrane oxygenation use in patients with neurological comorbidities. Pediatr Crit Care Med. (2022) 23(11):943–6. doi: 10.1097/PCC.0000000000003078
28. Dreier E, Malfertheiner MV, Dienemann T, Fisser C, Foltan M, Geismann F, et al. ECMO in COVID-19-prolonged therapy needed? A retrospective analysis of outcome and prognostic factors. Perfusion. (2021) 36(6):582–91. doi: 10.1177/0267659121995997
29. Raza T. 300 plus days on ECMO—lessons learned. Qatar Med J. (2017) 2017(1):49. doi: 10.5339/qmj.2017.swacelso.49
30. Coleman RD, Goldman J, Moffett B, Guffey D, Loftis L, Thomas J, et al. Extracorporeal membrane oxygenation mortality in high-risk populations: an analysis of the pediatric health information system database. ASAIO J. (2020) 66(3):327–31. doi: 10.1097/MAT.0000000000001002
31. Burgos CM, Frenckner B, Broman LM. Premature and extracorporeal life support: is it time? A systematic review. ASAIO J. (2022) 68(5):633–45. doi: 10.1097/MAT.0000000000001555
32. Moynihan KM, Dorste A, Seigel BD, Rabinowitz EJ, McReynolds A, October TW. Decision-making, ethics and end-of-life care in pediatric extracorporeal membrane oxygenation: a comprehensive narrative review. Pediatr Crit Care Med. (2021) 22(9):806–12. doi: 10.1097/pcc.0000000000002766
33. Bosslet GT, Pope TM, Rubenfeld GD, Lo B, Truog RD, Rushton CH, et al. An official ATS/AACN/ACCP/ESICM/SCCM policy statement: responding to requests for potentially inappropriate treatments in intensive care units. Am J Respir Crit Care Med. (2015) 191(11):1318–30. doi: 10.1164/rccm.201505-0924ST
34. Fernando SM, Mathew R, Slutsky AS, Rochwerg B, Kyeremanteng K, Combes A, et al. Media portrayals of outcomes after extracorporeal membrane oxygenation. JAMA Intern Med. (2021) 181(3):391–4. doi: 10.1001/jamainternmed.2020.6094
35. Holtzman JN, Dhruva SS. Media portrayals of extracorporeal membrane oxygenation: the unforeseen harm of unfounded optimism. JAMA Intern Med. (2021) 181(3):394–5. doi: 10.1001/jamainternmed.2020.6091
36. Fleck LM. ECMO: what would a deliberative public judge? Am J Bioeth. (2023) 23(6):46–8. doi: 10.1080/15265161.2023.2201197
37. Curley MAQ, Meyer EC. Parental experience of highly technical therapy: survivors and nonsurvivors of extracorporeal membrane oxygenation support. Pediatr Crit Care Med. (2003) 4(2):214–9. doi: 10.1097/01.PCC.0000043915.79848.8D
38. Schou A, Mølgaard J, Andersen LW, Holm S, Sørensen M. Ethics in extracorporeal life support: a narrative review. Crit Care. (2021) 25(1):256. doi: 10.1186/s13054-021-03689-0
39. Meltzer EC, Ivascu NS, Stark M, Orfanos AV, Acres CA, Christos PJ, et al. A survey of physicians’ attitudes toward decision-making authority for initiating and withdrawing VA-ECMO: results and ethical implications for shared decision making. J Clin Ethics. (2016) 27(4):281–9. doi: 10.1086/JCE2016274281
40. Chapman RL, Peterec SM, Bizzarro MJ, Mercurio MR. Patient selection for neonatal extracorporeal membrane oxygenation: beyond severity of illness. J Perinatol. (2009) 29(9 PG-606-11):606–11. doi: 10.1038/jp.2009.57
41. Kuo K, Barbaro R, Gadepalli S, Davis M, Bartlett R, Odetola F. Should extracorporeal membrane oxygenation be offered? An international survey. Crit Care Med. (2016) 44(12 PG-216):216. doi: 10.1097/01.ccm.0000509238.50003.b9
42. Wilkinson D, Butcherine E, Savulescu J. Withdrawal aversion and the equivalence test. Am J Bioeth. (2019) 19(3):21–8. doi: 10.1080/15265161.2019.1574465
43. Moynihan KM, Jansen MA, Liaw SN, Alexander PMA, Truog RD. An ethical claim for providing medical recommendations in pediatric intensive care. Pediatr Crit Care Med. (2018) 19(8):e433–7. doi: 10.1097/PCC.0000000000001591
44. Lantos JD. The tragic case of charlie gard. JAMA Pediatr. (2017) 171(10):935–6. doi: 10.1001/jamapediatrics.2017.3079
45. Bein T, Müller T, Citerio G. Determination of brain death under extracorporeal life support. Intensive Care Med. (2019) 45(3):364–6. doi: 10.1007/s00134-018-05510-z
46. Taran S, Steel A, Healey A, Fan E, Singh JM. Organ donation in patients on extracorporeal membrane oxygenation: considerations for determination of death and withdrawal of life support. Can J Anesth. (2020) 67(8):1035–43. doi: 10.1007/s12630-020-01714-4
47. Abrams DC, Prager K, Blinderman CD, Burkart KM, Brodie D. Ethical dilemmas encountered with the use of extracorporeal membrane oxygenation in adults. Chest. (2014) 145(4):876–82. doi: 10.1378/chest.13-1138
48. Kirsch R, Munson D. Ethical and end of life considerations for neonates requiring ECMO support. Semin Perinatol. (2018) 42(2):129–37. doi: 10.1053/j.semperi.2017.12.009
49. Bein T, Brodie D. Understanding ethical decisions for patients on extracorporeal life support. Intensive Care Med. (2017) 43(10):1510–1. doi: 10.1007/s00134-017-4781-5
50. Lantos JD. Best interest, harm, god’s will. Parental discretion, or utility. Am J Bioeth. (2018) 18(8):7–8. doi: 10.1080/15265161.2018.1504502
51. Brett AS, Mccullough LB. Addressing requests by patients for nonbeneficial interventions. JAMA. (2012) 307(2):149–50. doi: 10.1001/jama.2011.1999
52. Mehra MR, Cleveland JCJ, Uriel N, Cowger JA, Hall S, Horstmanshof D, et al. Primary results of long-term outcomes in the MOMENTUM 3 pivotal trial and continued access protocol study phase: a study of 2200 HeartMate 3 left ventricular assist device implants. Eur J Heart Fail. (2021) 23(8):1392–400. doi: 10.1002/ejhf.2211
53. Goldstein DJ, Naka Y, Horstmanshof D, Ravichandran AK, Schroder J, Ransom J, et al. Association of clinical outcomes with left ventricular assist device use by bridge to transplant or destination therapy intent: the multicenter study of MagLev technology in patients undergoing mechanical circulatory support therapy with HeartMate 3 (MOM). JAMA Cardiol. (2020) 5(4):411–9. doi: 10.1001/jamacardio.2019.5323
54. Mehra MR, Salerno C, Cleveland JC, Pinney S, Yuzefpolskaya M, Milano CA, et al. Healthcare resource use and cost implications in the MOMENTUM 3 long-term outcome study. Circulation. (2018) 138(18):1923–34. doi: 10.1161/CIRCULATIONAHA.118.035722
55. Kirsch RE. The divergence of technical and human teleology. Am J Bioeth. (2023) 23(6):38–41. doi: 10.1080/15265161.2023.2201213
56. Kon AA. Withdrawal of ECMO support over the objections of a capacitated patient can be appropriate. Am J Bioeth. (2023) 23(6):30–2. doi: 10.1080/15265161.2023.2201218
57. Morrison W, Moynihan K. Personalizing care and communication at the limits of technology. Am J Bioeth. (2023) 23(6):41–3. doi: 10.1080/15265161.2023.2201207
58. Lantos J. To whom do children belong? Am J Bioeth. (2017) 17(11):4–5. doi: 10.1080/15265161.2017.1388032
59. Moynihan KM, Purol N, Alexander PMAP, Wolfe J, October TW. A communication guide for pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med. (2021) 22(9):832–41. doi: 10.1097/pcc.0000000000002758
60. Friedman Ross L. Better than best (interest standard) in pediatric decision making. J Clin Ethics. (2019) 30(3):183–95. doi: 10.1086/JCE2019303183
61. Bester JC. The best interest standard is the best we have: why the harm principle and constrained parental autonomy cannot replace the best interest standard in pediatric ethics. J Clin Ethics. (2019) 30(3):223–31. doi: 10.1086/JCE2019303223
62. Ross LF. Reflections on charlie gard and the best interests standard from both sides of the Atlantic Ocean. Pediatrics. (2020) 146(August):S60–5. doi: 10.1542/peds.2020-0818l
63. Diekema D. When parents and providers disagree. Pediatr Ethicsc. (2020) 31(2). https://pediatricethicscope.org/article/when-parents-and-providers-disagree/
64. Gillam L. The zone of parental discretion: an ethical tool for dealing with disagreement between parents and doctors about medical treatment for a child. Clin Ethics. (2016) 11(1):1–8. doi: 10.1177/1477750915622033
65. Katz AL, Webb SA, Committee on Bioethics. Informed consent in decision-making in pediatric practice. Pediatrics. (2016) 138(2):e20161485. doi: 10.1542/peds.2016-1485
66. Gillam L. Children’s bioethics and the zone of parental discretion. Monash Bioeth Rev. (2010) 20(2):1–3. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22032018
67. Hursthouse R, Pettigrove G. Virtue ethics. In: Zalta EN, Nodelman U, editors. The Stanford Encyclopedia of Philosophy. Fall 2023 edn. Stanford, CA: Metaphysics Research Lab, Stanford University (2018).
68. McCullough LB. The professional medical ethics model of decision making under conditions of clinical uncertainty. Med Care Res Rev. (2013) 70(1 Suppl):141S–158S. doi: 10.1177/1077558712461952
69. Wallace DJ, Angus DC, Seymour CW, Yealy DM, Carr BG, Kurland K, et al. Geographic access to high capability severe acute respiratory failure centers in the United States. PLoS One. (2014) 9(4):e94057. doi: 10.1371/journal.pone.0094057
70. Farr BJ, McEvoy LTCS, Ross-Li D, Rice-Townsend SE, Ricca RL. Geographic distance to extracorporeal life support centers for pediatric patients within the continental United States. Pediatr Crit Care Med. (2021) 22(11):e594–8. doi: 10.1097/PCC.0000000000002795
71. Saunders B. Accountability for reasonableness or equality of resources? Am J Bioeth. (2018) 18(3):49–50. doi: 10.1080/15265161.2017.1418934
72. Tate T. Pediatric suffering and the burden of proof. Pediatrics. (2020) 146(Suppl 1):S70–4. doi: 10.1542/peds.2020-0818N
73. Schuchter P, Heller A. The care dialog: the “ethics of care” approach and its importance for clinical ethics consultation. Med Health Care Philos. (2018) 21(1):51–62. doi: 10.1007/s11019-017-9784-z
74. Wightman A, Kett J, Campelia G, Wilfond BS. The relational potential standard: rethinking the ethical justification for life-sustaining treatment for children with profound cognitive disabilities. Hastings Cent Rep. (2019) 49(3):18–25. doi: 10.1002/hast.1003
75. Weiss EM, Fiester A. From “longshot” to “fantasy”: obligations to pediatric patients and families when last-ditch medical efforts fail. Am J Bioeth. (2018) 18(1):3–11. doi: 10.1080/15265161.2017.1401157
76. FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics. (2017) 18(1):19. doi: 10.1186/s12910-017-0179-8
77. Wilkinson DJC, Truog RD. The luck of the draw: physician-related variability in end-of-life decision-making in intensive care. Intensive Care Med. (2013) 39(6):1128–32. doi: 10.1007/s00134-013-2871-6
78. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. (2013) 28(11):1504–10. doi: 10.1007/s11606-013-2441-1
79. National Academies of Sciences, Engineering, and Medicine. Taking Action Against Clinician burNout: A Systems Approach to Professional Well-Being. Washington, DC: The National Academies Press (2019). doi: 10.17226/25521
80. Sallnow L, Smith R, Ahmedzai SH, Bhadelia A, Chamberlain C, Cong Y, et al. Report of the lancet commission on the value of death: bringing death back into life. Lancet. (2022) 399(10327):837–84. doi: 10.1016/S0140-6736(21)02314-X
81. White DB, Evans LR, Bautista CA, Luce JM, Lo B. Are physicians’ recommendations to limit life support beneficial or burdensome? Bringing empirical data to the debate. Am J Respir Crit Care Med. (2009) 180(4):320–5. doi: 10.1164/rccm.200811-1776OC
82. Sarela AI. Stop sitting on the fence: recommendations are essential to informed decision making. Br Med J. (2013) 347:f7600. doi: 10.1136/bmj.f7600
83. Jacobsen J, Blinderman C, Alexander Cole C, Jackson V. “I’d recommend …” how to incorporate your recommendation into shared decision making for patients with serious illness. J Pain Symptom Manage. (2018) 55(4):1224–30. doi: 10.1016/j.jpainsymman.2017.12.488
84. Moynihan KM, Lelkes E, Kumar RK, DeCourcey DD. Is this as good as it gets? Implications of an asymptotic mortality decline and approaching the nadir in pediatric intensive care. Eur J Pediatr. (2022) 181(2):479–87. doi: 10.1007/s00431-021-04277-8
85. Siegel B, Moynihan K. Precision decisions: tailoring decision-sharing in contemporary paediatric healthcare. Arch Dis Child. (2023) 108(8):593–4. doi: 10.1136/archdischild-2023-325367
86. Tadros HJ, Saidi A, Rawlinson AR, Cattier C, Black EW, Rackley J, et al. Assessment of parental decision making in congenital heart disease, cardiomyopathy and heart transplantation: an observational study analysing decisional characteristics and preferences. Arch Dis Child. (2023) 108(8):641–6. doi: 10.1136/archdischild-2022-324373
87. Morrison W, Clark JD, Lewis-Newby M, Kon AA. Titrating clinician directiveness in serious pediatric illness. Pediatrics. (2018) 142(November):S178–86. doi: 10.1542/peds.2018-0516I
88. Moynihan KM, Dorste A, Alizadeh F, Phelps K, Barreto JA, Kolwaite AR, et al. Health disparities in extracorporeal membrane oxygenation utilization and outcomes: a scoping review and methodologic critique of the literature. Crit Care Med. (2023) 51(7):843–60. doi: 10.1097/CCM.0000000000005866
89. Wirpsa MJ, Carabini LM, Neely KJ, Kroll C, Wocial LD. Mitigating ethical conflict and moral distress in the care of patients on ECMO: impact of an automatic ethics consultation protocol. J Med Ethics. (2021):1–7. doi: 10.1136/medethics-2020-106881
90. Doorenbos AZ, Starks H, Bourget E, McMullan DM, Lewis-Newby M, Rue TC, et al. Examining palliative care team involvement in automatic consultations for children on extracorporeal life support in the pediatric intensive care unit. J Palliat Med. (2013) 16(5):492–5. doi: 10.1089/jpm.2012.0536
91. Courtwright AM, Robinson EM, Feins K, Carr-Loveland J, Donahue V, Roy N, et al. Ethics committee consultation and extracorporeal membrane oxygenation. Ann Am Thorac Soc. (2016) 13(9):1553–8. doi: 10.1513/AnnalsATS.201511-757OC
92. Grant JK, Vincent L, Ebner B, Singh H, Maning J, Olorunfemi O, et al. In-hospital utilization and outcomes of palliative care consultation in patients with advanced heart failure complicated by cardiogenic shock requiring mechanical circulatory support. Am J Cardiol. (2021) 148:94–101. doi: 10.1016/j.amjcard.2021.02.024
Keywords: extracorporeal membrane oxygenation (ECMO), ethics, communication, death & dying, pediatric
Citation: Moynihan KM, Taylor LS, Siegel B, Nassar N, Lelkes E and Morrison W (2024) “Death as the One Great Certainty”: ethical implications of children with irreversible cardiorespiratory failure and dependence on extracorporeal membrane oxygenation. Front. Pediatr. 11:1325207. doi: 10.3389/fped.2023.1325207
Received: 20 October 2023; Accepted: 22 December 2023;
Published: 11 January 2024.
Edited by:
Michael-Alice Moga, University of Toronto, CanadaReviewed by:
Andrew Helmers, University of Toronto, Canada© 2024 Moynihan, Taylor, Siegel, Nassar, Lelkes and Morrison. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katie M. Moynihan a2F0aWUubW95bmloYW5AY2FyZGlvLmNoYm9zdG9uLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.