 Roberto Debbag1*
Roberto Debbag1* Jaime R. Torres2
Jaime R. Torres2 Luiza H. Falleiros-Arlant3
Luiza H. Falleiros-Arlant3 Maria L. Avila-Aguero4,5Jose Brea-del Castillo6
Maria L. Avila-Aguero4,5Jose Brea-del Castillo6 Angela Gentile7
Angela Gentile7 Xavier Saez-Llorens8Abiel Mascarenas9
Xavier Saez-Llorens8Abiel Mascarenas9 Flor M. Munoz10
Flor M. Munoz10 Juan P. Torres11Liliana Vazquez12Marco A. Safadi13
Juan P. Torres11Liliana Vazquez12Marco A. Safadi13 Carlos Espinal14
Carlos Espinal14 Rolando Ulloa-Gutierrez4
Rolando Ulloa-Gutierrez4 Monica Pujadas15Pio Lopez16
Monica Pujadas15Pio Lopez16 Eduardo López-Medina17Octavio Ramilo18
Eduardo López-Medina17Octavio Ramilo18
- 1President of Sociedad Latinoamericana de Infectología Pediátrica, SLIPE, Buenos Aires, Argentina
- 2Infectious Diseases Section, Tropical Medicine Institute, Universidad Central De Venezuela, Caracas, Venezuela
- 3Department of Children’s Health, Faculdade De Medicina, Universidade Metropolitana De Santos, Santos, Brazil
- 4Infectious Diseases Service, Hospital Nacional De Niños “Dr. Carlos Sáenz Herrera”, Caja Costarricense De Seguro Social (CCSS), San José, Costa Rica
- 5Affiliated Researcher Center for Infectious Disease Modeling and Analysis (CIDMA) at Yale University, New Haven, CT, United States
- 6Associated Researcher, Investigador Asociado Hospital Dr. Hugo Mendoza, Santo Domingo, Republic Dominicana
- 7Epidemiology Department, Hospital de Niños “Ricardo Gutiérrez”, Buenos Aires University, Buenos Aires, Argentina
- 8Head of Infectious Diseases and Director of Clinical Research, Hospital del Niño “Dr. José Renán Esquivel”, Panama City, Panama
- 9Department of Pediatric Infectious Diseases, Hospital Universitario “José E. Gonzalez”, Universidad Autónoma De Nuevo León, Nuevo Leon, México
- 10Department of Pediatrics, Baylor College of Medicine, Houston, TX, United States
- 11Department of Pediatrics and Children Surgery, Universidad de Chile, Santiago, Chile
- 12Pediatric Infectious Diseases, Clinica y Maternidad Suizo Argentina, Sanatorio Finochietto, Buenos Aires, Argentina
- 13Department of Pediatrics, Faculda de de Ciências Médicas da Santa Casa de São Paulo, Sao Paulo, Brazil
- 14Global Health Consortium, Robert Stempel College of Public Health & Social Work, Florida International University, Miami, FL, United States
- 15Department of Epidemiology and Pediatric Infectious Diseases, Centro Hospitalario Pereira Rossell, Faculty of Medicine, Universidad de la República, Montevideo, Uruguay
- 16Department of Pediatrics, Hospital Universitario del Valle, Cali, Colombia
- 17Centro de Estudios en Infectología Pediátrica CEIP, Department of Pediatrics, Universidad del Valle, Clinica Imbanaco Grupo Quironsalud, Cali, Colombia
- 18Department of Infectious Diseases, St. Jude Children’s Research Hospital, Memphis, TN, United States
While the first 1,000 days of life are a critical period in child's development, limited information on the main determinants affecting this period in the Latin America and the Caribbean (LAC) region is available. Therefore, the Latin American Pediatric Infectious Diseases Society (SLIPE) held an ad hoc workshop in May 2022 with an expert panel designed to analyze the main factors impacting the development of childhood in the region during this period and the main causes of maternal infant morbimortality. The aim was to identify priorities, generate recommendations, and advise practical actions to improve this situation. Considerations were made about the challenges involved in bridging the gap that separates the region from more developed countries regarding an optimal early childhood and maternal care. Extensive discussion was conducted to reach consensus recommendations on general strategies intended to reduce maternal and infant mortality associated with infections and immune-preventable diseases during the first 1,000 days of life in LAC.
1. Introduction
The first 1,000 days of life—the time spanning between the moment a woman becomes pregnant and her child's second birthday—is a unique window of opportunity where foundations for children growth, ability to learn, and health are built (1, 2). This period is considered the phase where brain begins its development, and the base of future health and neurodevelopment. It also represents a time of vulnerability. For example, nutrition of the mother during pregnancy and the one a child receives in the first two years of life, is a crucial determinant of health (1–3). In low-income countries (LIC), poverty often debilitates access to proper food, causing mortality, significant morbidities, and a substantial loss of neurodevelopmental potential (2, 3).
During the last decades, plentiful research in the fields of neuroscience, biology, and early childhood development provided powerful insights into how interaction between nutrition and environments in these 1,000 days shape future outcomes.
The first 1,000 days are characterized by rapid rates of neuronal proliferation, growth and differentiation, myelination, and generation of synapses. This is also a time of brain vulnerability to any nutrient deficit, infectious diseases, detrimental living conditions, or vaccination status among others.
Nutrition plays a fundamental role in child's development. Poor nutrition in the first 1,000 days and its sequelae can cause irreversible damage to a children's growing brain, affecting proper education, and making it harder for them and their families to rise from poverty. It can also be later translated in obesity, diabetes, and other chronic diseases and a lifetime of health issues (1–5).
Current global estimates suggest that about 10.6 million children under the age of five die annually. Of those, 3.8 million die in the first four weeks of life, with 75% occurring in the first week after birth. Neonates account for 38% of deaths in children with a similar number of stillborn (6). Most deaths occur in LIC with an estimated mortality of 33/1,000 live births, while the remaining occur in high-income countries with a clear lower rate (4/1,000 live births) (6).
Infections are the predominant cause of mortality in this vulnerable group. Major categories of neonatal deaths in poor communities include preterm birth (28%), sepsis/pneumonia (26%), tetanus (7%), diarrhea (3%), complications of asphyxia (23%), or congenital abnormalities (7%) (6). It has been described that the risk of neonatal death secondary to infections in countries with a very high-mortality is about 11-fold higher than in low-mortality countries. According to the 2020 report of the United Nations Children's Fund (UNICEF), World Health Organization (WHO), World Bank Group, and Population Division of the Department of Economic and Social Affairs of the United Nations, nearly 2 million fetal deaths occur in the world every year: with one death every 16 s, almost 4 every minute, more than 200 per hour, almost 5,400 every day, and about 164,000 every month.
In 2019, 39 countries had a higher fetal mortality rate than neonatal deaths, and 15 countries had a higher number of stillbirths than children under one year of age. Nearly 40% of global fetal deaths occur during childbirth due to poor quality of care during pregnancy and delivery (7). It is expected that an additional excess of stillbirths in low-middle income countries (LMIC) will occur due to the COVID-19 pandemic. The major social determinants affecting the under 5 years' morbidity and mortality include poverty, malnutrition, inequity, lack of education, failure to implement breast-feeding or complementary feeding programs, complications of labor and low birth weight, infections, and inadequate health-related social practices (6).
Little information is available on the aspects affecting this critical period of life in the region. Therefore, the Latin American Pediatric Infectious Diseases Society (SLIPE) convened a panel of experts to analyze the context and main barriers negatively impacting adequate development of childhood during the first 1,000 days of life and the maternal infant morbidity and mortality in LAC.
2. Current state of early pediatric mortality in the region
By 2020, LAC had a population of about 30,150,000 children under 2 years of age and an infant mortality rate of 14.8/1,000 live births. This means that in our region, 115,816 children under the age of one die (7). The corresponding infant mortality rates by LAC subregions, Mexico and Brazil are shown in Table 1.
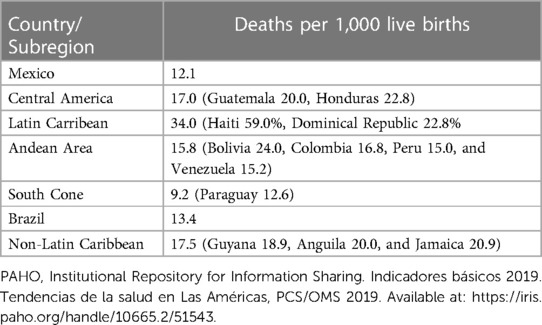
Table 1. Infant mortality rates by Latin American subregion, Mexico, and Brazil, and (in parenthesis) specific countries with values above the regional average.
The neonatal mortality rate for the region of the Americas by 2019 was 7.7/1,000 live births, and 9.3/1,000 children aged less than 28 days for the LAC region. While the neonatal mortality rate in LAC has experienced a steady decline (23 in 1990 to 9/1,000 in 2020), the global mortality in children under five years of age has fell more rapidly than the one observed in neonates (Figure 1). An estimate of 92,000 stillbirths were reported that year in LAC, that varies by country in the region: from 13.1/1,000 in Guyana, to 12.7/1,000 in Guatemala, 4.5/1,000 in Costa Rica, and 3.1/1,000 in Chile (8).

Figure 1. Comparative level and trends in pediatric death rates by age group (less than 5 year-old, neonates and 1 to 59 months). In Latin America and the Caribbean from 1990 to 2021. Source: Reliefweb. Levels & Trends in Child Mortality: Report 2022. Estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation. https://reliefweb.int/report/world/levels-trends-child-mortality-report-2022.
The first cause of neonatal death in the region is premature birth, followed by congenital defects, neonatal asphyxia, and trauma. Also sexually transmitted infections (STI), or respiratory tract infections account as causes of neonatal demise. During the first 28 days of life one fifth (20,000) of them are due to congenital defects (8, 9). More than half deaths before the age of five occur during pregnancy, birth, or the first four weeks of life (8, 9).
3. Development of immune system in early infancy
Infectious diseases represent the most frequent cause of death among infants and young children (10–16). Susceptibility to invasive pathogens is related to the fact that immune response in infants is generally less competent than in adults (17–25). Elucidating why infant immune responses to microbes and vaccines are less protective than the one observed in adults, has major implications for developing improved vaccines.
Infants display cytokine response patterns to Toll-like receptors (TLRs) stimulation that are different from those of older children and adults (26). The recent availability of system analysis tools has facilitated in depth analysis of immune responses in individuals with acute infections and in response to vaccinations. Those studies have described “immune signatures” that can let the identification of early gene expression patterns and cell populations that correlate with, or even predict, the development of protective immune responses (27–31).
Increasing evidence indicates that the initial encounter with a specific antigen or pathogen, whether it is in the context of infection or vaccination, has profound implications for future immune responses. The best-known example is influenza virus where initial exposure to the virus via infection and/or vaccination shapes the establishment of B cell memory and the responses to subsequent infections and vaccinations, a process known as the “original antigenic sin” (32). It has been proposed that this phenomenon of “immune imprinting” in not unique to influenza virus and that it may also occur in the context of other viral infections such as coronaviruses or dengue virus (33, 34).
There is a concept that infants have predominantly naïve B and T cells, and the numbers of memory B and T cells increase progressively as they get exposed to different pathogens and vaccines. For this reason, in the initial months of life infants rely mostly on maternal antibodies and the innate immune responses. However, these notions are being challenged by recent data. Analysis of young infants infected with Respiratory Syncytial Virus (RSV) showed that the innate immune response, and more specifically, the antiviral interferon response is not very effective during the first 6 months of life (34, 35). Indeed, this inadequate interferon response has been associated with poorer clinical outcomes, which may explain in part why RSV causes such severe disease, especially in the first months of life (36).
Animal studies suggest a potential role of the microbiome composition in modulating responses to vaccines (37). A recent retrospective study provided evidence that young children to 24 months of age who were prescribed antibiotics had a higher frequency of vaccine-induced antibody titers below the levels of protection compared with children with no antibiotic prescriptions. Furthermore, investigators observed a dose-effect as the total antibiotic exposure was associated to lower antibody titers. The authors proposed that antibiotic treatment in early life modified the gut microbiome, which in turn altered immune responses to routine vaccines (38). Despite the limitations of the study design, these provocative observations clearly deserve future prospective studies as their findings could have major repercussions for the immunization programs (39).
These are a few examples of how the unique features of the infant immune system significantly impact childhood health and have long-term consequences for establishing protective immunity. For these reasons, and despite the challenges involved in conducting clinical studies in young children, it is essential we dedicate renewed efforts to improve our understanding of early life immunity to further develop more effective vaccines and therapies for children.
4. Determinants that affect child's health from preconception to two years of life
4.1. Maternal health
An essential element of the first 1,000 days of life is the health condition of the pregnant woman, not only along pregnancy, but also during childbirth and puerperium. High maternal mortality rates may be related to poor reproductive health, including lack of access to proper care during pregnancy and childbirth, and availability of safe abortion whether legal or not. Poverty, low economic status, lack of education, poor nutrition, heavy workloads, and violence may increase the risks of poor outcomes during pregnancy and childbirth (40). According to the State of the World's Children 2023 report from UNICEF, they all are strongly associated with poor vaccination coverage rates in the region (40).
Maternal mortality is defined as the death of a woman during pregnancy, childbirth, or the first 42 days after delivery. In the last decade, LAC have shown modest reduction in maternal mortality, however, the COVID-19 pandemic, has increased the number of deaths reported (41). The greatest risk of maternal mortality is age, and it includes adolescents under the age of 15 in most developing countries. Severe hemorrhages, infections, complicated hypertension (preeclampsia and eclampsia), and dangerous abortions account for 75% of maternal deaths (41).
LAC reported a maternal mortality rate of 74/100,000 live births in 2017, and by 2020, it decreased to 67.2/100,000. According to the Sustainable Development Goal (SDG), this rate should be lower than 70/100,000 live births for 2030 (41, 42), but there are still several countries in the region with higher mortality index.
4.2. Food security and nutrition
The 2021 United Nations report on regional food and nutrition security reported that LAC experienced a 30% increase in hunger between 2019 and 2020. About 4.8 million boys and girls under five years of age in the region are affected by chronic malnutrition (43). Over one year, in the context of the COVID-19 pandemic, the number of people living with hunger increased by 13.8 million, reaching a total of 59.7 million people (43).
The prevalence of hunger in LAC is currently 9.1%, the highest of the last 15 years. It has been estimated that four out of ten people in the region (about 267 million) experienced moderate to severe food insecurity in 2020; that is, 60 million more than in 2019, mainly in Mesoamerica (43, 44). By 2020, the malnourished population reached 16.1% in the Caribbean, 10.6% in Mesoamerica, and 7.8% in South America (43, 44).
Maternal food deprivement is also related to other conditions. The region has not shown significant progress in reducing the prevalence of anemia in women of reproductive age, that by 2019 reached 17.2%. There is a goal set by the SDG-2 to reduce anemia in 50% by 2030, not yet accomplished in LAC. Nowadays anemia affects 14.6% of women in reproductive age in Mesoamerica, 17.3% in South America, and 29.2% in the Caribbean. Countries with the highest prevalence in the region are Haiti (47.7%), Guyana (31.7%), and Dominican Republic (26.4%), in contrast with countries such as Chile (8.7%) and Guatemala (7.4%) (43).
Regional rate of exclusive breastfeeding during the first six months of life is 33.4%, much lower than the world's average (44%) (45). This may be related with children under five years of age with failure to thrive in LAC, an indicator of disease, poor health, and malnutrition, that ranges between 7.3%–12.6% in 2019 (46). All these factors increase the risk of complicated infections and death during the first 1,000 days of life.
4.3. Exposure to toxins, pollutants, and infectious agents
Exposure to toxic chemicals can lead to chronic and often irreversible health disorders, including birth defects, neurodevelopmental delay, and endocrine disrupted diseases. Chemical hazards, such as exposure to pesticides, lead, and mercury, tend to disproportionately affect children and pregnant women. Pediatric population, especially young children, are exposed to continuous pollutants, increasing the risk of premature deaths and diseases related to multiple sources of contamination.
In the Americas, about 847,000 deaths per year (13%) are attributable to environmental risks. Air pollution is the main public health hazard in the Americas, where more than 150 million people in LAC live in cities that exceed the WHO Air Quality Guidelines. Consequently, 320,000 preventable deaths in the Americas result from air pollution (47).
Water pollution is also an important problem. Twenty-eight million people in the region lack potable water access, and 83 million lack adequate basic sanitation services and facilities, causing nearly 30,000 preventable infectious related deaths. Approximately 7,600 children under five years of age die annually from acute diarrhea in the region. Haiti (23%), Guatemala (10%), Bolivia (7%), and Venezuela (5%) have the highest rates of mortality (8).
Children are particularly susceptible to the harmful effects of the environment. The impact of heavy metals such as lead and mercury on the pregnant woman and the newborn brings harmful consequences for children development, cognitive capacity, and growth. Those under five years of age are particularly vulnerable because depending on the source of contamination, they absorb 4–5 times more lead than adults (48, 49). Harmful effects of lead include premature birth, low birth weight, developmental delay, learning difficulties, and growth retardation in young children. These effects are more common in risk exposures from the mother or the baby (49, 50).
It is estimated that in LAC 49,107,507 children between 0 and 9 years of age have blood levels of lead above 5 ug/dl. Elevated lead levels in children have been reported in Mexico, Colombia, Peru, and Brazil (50). Countries of the Amazon basin (Brazil, Colombia, Peru, Ecuador, Venezuela, and Bolivia) have reported high concentrations of mercury in children, including newborns, detected in the umbilical cord and breast milk (49). In Latin America, more than 4.5 million people are chronically exposed to arsenic levels in drinking water, more than 200 times higher than the WHO limit (10 μg/L). In a systematic review conducted by Heng et al., it was shown that postnatal exposure to lead and manganese is associated with neurodevelopmental delay (48, 49).
Exposure to lesser common toxins is also a health menace. More than 80 million people still depend on polluting fuels such as solid fuels or kerosene for lighting, cooking, and heating (47).
As mentioned before, infectious disease account for an important risk factor of death in the first 1,000 years of life. According to recent data, it is estimated that approximately 3% of the deaths in young children are caused by meningitis (51). The most common bacteria causing meningitis include Streptococcus agalactiae, enteric bacilli, occasionally Listeria monocytogenes during the first two months of life, Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae, but their relative contribution differs over time, region, and age group (52, 53). In Latin America, as well as in other LMIC countries, tuberculosis is also a relevant cause of meningitis in young children (51).
Most of the clinical burden of acute gastroenteritis occurs in young children, mainly in developing countries (54). Studies carried out in our region have revealed the etiological importance of rotavirus and norovirus, that represent almost half of hospitalizations during early childhood. Other organisms described are Shigella sp., Giardia sp., Campylobacter sp., and pathogenic strains of Escherichia coli (55, 56).
Acute respiratory infections are also a leading causes of child morbidity and mortality, causing close to one third of deaths in children under five years of age in LIC (57, 58). In the WHO Region of the Americas report, pneumonia and influenza accounted for 11.5% of all deaths in children 0–4 years of age in 2007. Typical bacterial pathogens that cause community acquired pneumonia are S. pneumoniae, H. influenzae (both vaccine-preventable infections), Mycoplasma pneumoniae, and S. aureus. In Latin America, the predominant infections are caused by S. pneumoniae, H. Influenzae type b, Respiratory Syncytial Virus, Influenza virus, and recently, SARS-CoV-2 (57, 58).
4.4. Migration and climate change
Migrant children and pregnant women are affected by social and health inequities. This vulnerable population is also exposed to violence, sexual exploitation, and sexually transmitted diseases. Venezuelan migration within the Americas has accounted for 3.9 million people moving from their country, where 24% were children (59, 60).
Vulnerable groups are disproportionately at risk from increased frequency and severity of extreme weather conditions (60). Climate-related factors have an impact on health and well-being of population because they disrupt the world's physical, biological, and ecological systems. Health effects may include, but are not limited to, increased respiratory and cardiovascular diseases, injuries and premature deaths related to extreme weather events, food insecurity and air pollution, threats to mental health, and changing patterns of vector-borne diseases transmission and climate-sensitive infections (60).
The SDGs for 2030 Agenda addresses the environmental determinants of health and contribute directly and indirectly to SDG-3 pertaining “Good Health and Well-being” to ensure healthy lives and promote well-being for all. Issues include water supply, sanitation and hygiene, air quality, chemical safety, and climate action (61).
5. SLIPE advisory group recommendations
The Advisory Group of SLIPE has defined ten general strategies aimed to reduce the maternal and infant mortality associated with infections and immune preventable diseases during the first 1,000 days of life in LAC.
5.1. Problem awareness
It is necessary to increase awareness in the medical and public community about the determinants of maternal and infant morbidity and mortality in the region. Provide universal access to medical care with a focus on vulnerable populations in LAC, such as mothers and children, is essential. Health policies are necessary to reduce this burden, and improve food and nutritional security, reduce the exposure to infectious agents, and provide adequate healthcare to populations are affected by natural phenomena caused by climate change.
5.2. Universal access to mother's health
One of the most effective means to improve maternal health is to invest in primary health care and improve health systems to ensure availability and professional care at all levels. Family planning services, prevention of unplanned pregnancies, and access to safe abortion and post-abortion care services may significantly impact maternal deaths and morbidities (40).
Preventive health assessments for women before and during pregnancy play a crucial role in reducing the risk of adverse health effects for both the women and their infants. While prenatal care is generally elevated in LAC (62), several other aspects of health require attention. These include the management of chronic conditions, the appropriate use of prescribed and non-prescribed medications, nutrition evaluation, screening for violence, assessing security and living conditions, ensuring adequate support postpartum, and addressing mental health. In some settings, these aspects are not always prioritized for pregnant women (63).
It's important to recognize that safeguarding the health of newborns begins with the health of pregnant women, and assessing vaccination status during prenatal care should be a standard practice in every health intervention (63).
5.3. Prevention of climate change and environmental impact on health
Environmental public health programs must assess health issues attributable to climate factors trough the development of inclusive and equitable policies to protect people from environmental hazards. This is achieved through pragmatic, intersectoral, multisectoral, subnational, national, and supranational approaches. It is important that public health programs foster an environmentally responsible and resilient health sector.
To reduce the burden of disease and health inequity attributable to environmental determinants of health in the region is necessary to increase the capacity of health actors and to address the environmental determinants of health, emphasizing air quality, safety of chemical substances, factors associated with climate and water, sanitation, and hygiene, prioritizing populations living in vulnerable situations.
Actions must be focus on improvement of public health programs, environmental public health surveillance, and promotion of responsible and resilient health sector.
5.4. Access to food security and nutrition in LAC
Optimal physiological, cognitive, and emotional development in children requires access to food of quality and in quantity at this critical period. Unfortunately, according to the United Nations report “Overview of Food Security and Nutrition 2022”, hunger in LAC reached 56.5 million in 2021, with the Caribbean as the most affected area (64). By 2021, 40.6% of population experienced moderate to severe food insecurity, compared to 29.3% worldwide (64).
A worrisome amount of 131.3 million people in the region were not able to afford a healthy diet in 2020, largely due to costs as compared to other regions. This situation affects more severely vulnerable populations such as small farmers and women in rural areas, as well as indigenous and Afro-descendant populations. The average cost of a daily healthy diet in the Caribbean has been estimated in USD 4.23, followed by USD 3.61 in South America, and USD 3.47 in Mesoamerica (64). While no individual policy can solve this problem, regional governments need to develop public policies that guarantee adequate nutrition and availability of nutritious food at affordable prices, in addition to nutritional counseling, in vulnerable communities.
Food insecurity may be both a driver and an effect of migration. While incidental evidence indicates that it is common to identify food insecurity in migrants, is not well documented. Both migration and food security are complex events, and migration presents both challenges and opportunities in food security, as they are heavily influenced by local conflicts, natural threats or disasters, climate change, and poverty, but they are also a vital component of the work force of the food processing industry and contribute to food security through agricultural labor (65).
5.5. Implementation of general measures to promote a healthy parenthood: availability of adequate infectious diseases evaluation at pre-conception and during pregnancy. Specialized care during childbirth, adoption of infection prevention practices during pregnancy and early postpartum
Elimination of mother-to-child transmitted diseases is a priority in the region of the Americas. Work should begin prior to pregnancy among adolescents and women of childbearing age, with special focus on the most vulnerable segments of the population, through counseling, prevention of sexually transmitted infections, contraception, comprehensive sexual health clinics, and counseling on pre- and post-exposure HIV prophylaxis.
Difficulties accessing health services and vulnerabilities of groups are fundamental factors conditioning the analysis of the interventions to be carried out. Emphasis must be placed in avoiding unplanned pregnancies and the implementation of measures to improve health conditions of each woman prior to the beginning of pregnancy.
Access to appropriate prenatal care, with specialized attention to childbirth and immediate postpartum should be guaranteed, including measures aimed to generate practices to prevent infections during pregnancy and in a hospital setting. Infections acquired prior to pregnancy, during pregnancy or peripartum, can affect maternal health, cause pregnancy loss, intrauterine growth restriction, neonatal deaths, and a wide variety of sequelae that can manifest throughout life.
Investigation of asymptomatic infections and identification of risk situations will allow the application of preventive or therapeutic measures to reduce maternal, fetal, and neonatal morbidity and mortality.
Strategies aimed to the community and hospitalized women of child-bearing age are necessary to encourage responsible procreation, prevention of sexually transmitted infections, and infections associated with health care. Joint work of obstetricians, pediatricians, neonatologists, biochemists, nurses, infectious diseases specialists, and health agents is vital.
5.6. Appropriate fulfillment of maternal immunization schedules before and during pregnancy
During pregnancy, up-to-date routine immunizations should be guaranteed, and previous immunization schedules should be reviewed, as some vaccines cannot be offered in a gestated woman, but disease may cause severe birth defects (66–68). Everyone in the household must be up to date with their immunizations, lowering the chance of vaccine preventable diseases in pregnant woman.
5.6.1. Recommended vaccines for pregnant women
Pregnant women are advised to receive influenza vaccine at any time during pregnancy, pertussis-containing vaccines (Tdap) between second and third trimester (Table 2). SARS-CoV-2 infection during pregnancy has been associated with a higher risk of preterm birth and stillbirth. Therefore, health authorities in LAC and North America recommend COVID-19 vaccination for everyone aged 6 months and older, including people who are pregnant, breastfeeding, or might become pregnant in the future. This recommendation includes getting boosters as recommended (69).
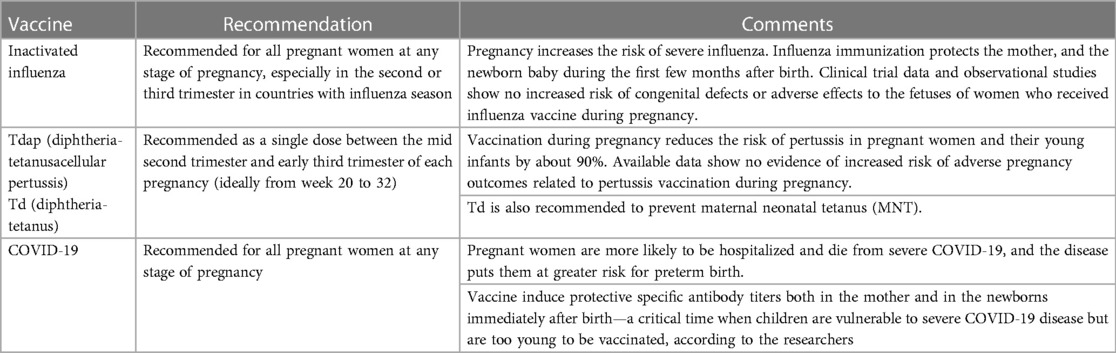
Table 2. Recommended vaccines for pregnant women.
Pregnant women can recieve Td or Tdap vaccines for the prevention of maternal-neonatal tetanus, or to manage tetanus-prone wounds. Also, they can receive rabies vaccine if required for post-exposure prophylaxis, with a significant risk of exposure (related to occupation or travel), or if there has been a potential exposure to rabies virus or another bat lyssavirus (70, 71).
Live attenuated vaccines are generally contraindicated in pregnant women due to a hypothetical risk of harm if the vaccine pathogen replicates in the fetus (66–68). Although pregnant women are not recommended to receive yellow fever vaccine, travel to a country with risk of yellow fever transmission, or to endemic areas may be unavoidable. In this case, risks and benefits of yellow fever vaccination must be weighted, and other strategies to reduce risk of infection should be contemplated (66–68).
5.6.2. Immunization of breastfeeding women
Vaccination is rarely contraindicated in breastfeeding women. For most vaccines, an infant's immune response to vaccination in relation to breastfeeding has been considered. In general, breastfeeding does not adversely affect immunization, and is not a contraindication for any vaccines recommended in infants.
Breastfeeding women should not receive yellow fever vaccine unless the mother has a high risk of acquiring yellow fever or cannot avoid or postpone travel. Although extremely rare, there have been case reports of probable transmission of the yellow fever vaccine virus to infants through breast milk (72, 73).
5.7. Completion of vaccine calendars during the first and second year of life, according to national vaccination programs
Vaccines in children from the neonatal period until the age of 24 months helps to protect them from serious and life-threatening diseases. Early vaccination can help ensure children's protection when they are most at risk. Additionally, it may help prevent the spread of these diseases within communities, providing protection not only for the vaccinated child but also for those who are too young or unable to receive vaccines themselves through herd immunity.
Recommended vaccines from birth to 24 months of age may vary in every region. Globally, twenty-five new vaccine introductions were recorded in 2021 (not including COVID-19 vaccine). Although this is an increase from 2020, it is well below the number of introductions of any year in the past two decades prior to 2020. This slowdown is likely to continue as countries focus on ongoing efforts to control COVID-19 pandemic (74).
While immunizations have been one of the most successful interventions to reduce or eliminate the incidence of vaccine-preventable diseases, vaccination coverage has decreased over the years, even before COVID-19 (75). While the pandemic did cause a frightening drop in coverage due to intrinsic conditions of social isolation widely discussed in different publications, regional trends in vaccination coverage in Latin America had already experienced a progressive reduction that intensified in 2020 (76).
In 2021, more than 2.7 million children under one year of age in the Americas (19.7%) did not receive all their shots, leaving them susceptible to diseases such as polio, tetanus, measles, and diphtheria. Two years into the pandemic, health services have not yet fully recovered (75, 76).
As seen in Figure 2, regional vaccination coverage rates for children have shown a steady percentual decline since 2016, including MMR (17.08%), polio (7.06%), DPT (11.09%), PCV (4.77%), rotavirus (3.85%), and hepatitis B (10.53%) (74–76).
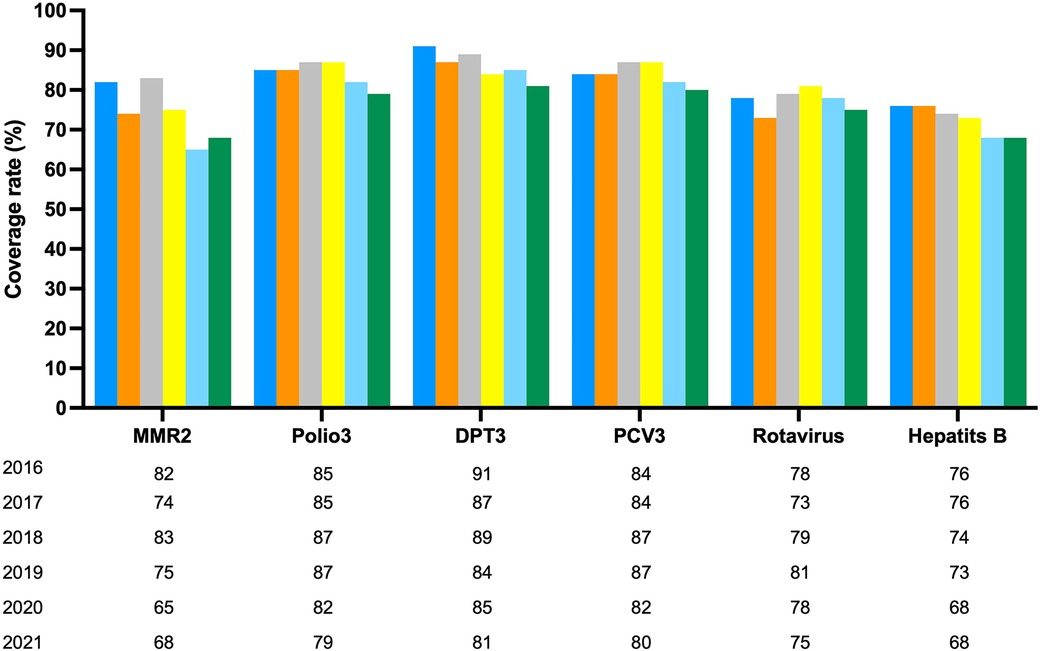
Figure 2. Vaccination coverage of selected vaccines in region of the Americas, 2016–2021. Country reports through the PAHO-WHO/UNICEF Joint Reporting. Source: IRF and country submissions of the electronic. PAHO-WHO/UNICEF Joint reporting From (e.IRF). Preliminary data as of 04 August 2022.
Over the last decade, overall vaccination rates for children in the continent fell from 93% to barely 75%, which places LAC below the world average (81%) with regions such as the East and Southern Africa (74%). Moreover, by 2023, more than 1.7 million children in the region had not received any dose of any vaccine, a phenomenon known as “zero children”. The most affected countries are Brazil (700,000), Mexico (316,000), and Venezuela (120,000). These three countries account for more than 60% of unimmunized minors in the region. Brazil and Mexico also appear on the list of the 20 countries with the higher number of unvaccinated children. Main causes include migration, natural disasters, political instability, and violence. Children in situation of poverty are three times more likely to be in this group. This vulnerable population is increasing in number, partially because immunization is lower on the list of priorities for families and countries (74–76).
Vaccine hesitancy has been stable in the region until the beginning of the pandemic, that negatively impacted vaccination coverage rates (77). Rejection has been mainly identified towards mRNA vaccines, most importantly in the group below 5 years of age. COVID-19 brought a negative impact on national vaccination programs secondary to a decrease in the demand during confinement, decrease capacity for epidemiological surveillance, and weakness of health systems around the region (77).
Despite progress in vaccination, collective efforts have fallen short. While new vaccines are being developed or are in the pipeline, achieving sufficient coverage remains a challenge. Ensuring the right of all children to be immunized involves comprehensive programs with adequate infrastructure and resources, education of healthcare workers and communities about the importance of immunization, and collaboration with national entities and international organizations (40).
Countries need to strengthen their national health systems to provide universal coverage, making all available vaccines accessible to every child. Despite the rapid development of vaccines during the pandemic, global distribution and uptake remained inadequate (78).
Equity in immunization should be a priority, viewing it as a lifesaving intervention. The goal is to vaccinate every child, everywhere, build confidence in vaccination, invest in vaccines, and fortifying national immunization programs through resilient strategies. This approach aligns with the principle that access to vaccines is a fundamental right for every child, regardless of geographical location or socio-economic status (40).
5.8. Prompt clinical evaluation of newborns with suspicion of congenital infection under standardized diagnostic and treatment guidelines
LAC is a region with high prevalence of syphilis and HIV. The elimination of Mother-To-Child Transmission (MTCT) of these diseases is a priority in the region (62). A 10% maternal transmission rate of HIV, and 2 cases of congenital syphilis (CS) per 1,000 live births are estimated, with important differences between different countries (0–6.5/1,000 live births in 2015). Significant progress has been made towards the goal of disease eradication, and eight countries in the region have achieved certification of dual elimination of HIV and CS. Nevertheless, increased efforts are needed to achieve greater accessibility in the evaluation in pregnant women and their partners including optimization of the frequency and quality of follow up appointments during pregnancy, accessible education for sexually transmitted diseases prevention, adequate treatment for the pregnant woman and her/his/their partners, and improved epidemiological reporting systems to achieve sustained control of these infections (79).
In September 2010, the PAHO/WHO approved the strategy and Plan of Action for the elimination of MTCT of HIV and CS, with the goal of reducing MTCT of HIV to 2% or less, and the incidence of CS to 0.5 cases (including stillbirths) or less per 1,000 live births by the year 2015 (80). This commitment was renewed and expanded in 2016, when the member states approved the “Action Plan for the Prevention and Control of HIV Infection and Sexually Transmitted Infections (STIs) 2016–2021” or ETMI-Plus incorporating Hepatitis B and Chagas into the disease eradication strategy (79).
Streptococcus agalactiae or beta-hemolytic Group B (SGB) continues to be one of the main pathogens of early neonatal sepsis (ENS). The detection of the maternal colonization by SGB and the intrapartum antibiotic prophylaxis have managed to reduce by nearly 75% cases of ENS. It's key to implement in our countries policies that allow the identification of pregnant women through vaginal and rectal cultures to search for SGB after 35 weeks of gestational age (81).
There are no worldwide standardized recommendations over the prevention of congenital toxoplasmosis. In Latin America, Colombia, Argentina, Uruguay, Paraguay, Brazil, Panama, and other countries there is a proposal for a screening program, but this isn't the case in other countries like Chile, Peru, Mexico, and Ecuador. Several studies have been performed in both France and Colombia that show that cost benefit of screening, even in locations with few cases (82, 83).
The introduction of an investigation protocol (before conception and labor), the diagnosis, the timely treatment during pregnancy, and the evaluation and monitoring of newborns has diminished cases of children with severe sequelae due to congenital toxoplasmosis (84, 85).
Cytomegalovirus (CMV) is the most frequent reason for congenital infections. The fetal infection can occur due to a primary maternal infection during pregnancy or secondarily through a viral reactivation or reinfection. Hearing loss is the main consequence of congenital CMV and the leading cause of non-genetic deafness among children (86). There are no recommendations of serological studies for CMV nor of effective treatments for pregnant women with a primary infection or reinfection. Several screening programs for newborns are currently undergoing with the goal of diagnosing and treating congenital infection at an early stage and prevent the main hearing and neurological consequences that might develop (87).
The main source of infection for CMV during pregnancy is contact with children under five years old which are in the early stages of their education. Apart from the serological results for CMV, pregnant women must be warned and educated about the potential risk of infection that contact with the saliva and urine of children brings, and they must be reminded of how important it is to wash their hands (88).
All newborns, regardless of their clinical condition, must be evaluated to rule out congenital infections. The evaluation of both the mother and child in the first days of neonatal life offers the opportunity to analyze the maternal clinical history during pregnancy, establish epidemiological determinants of risk, and review compliance and results of the serological tests recommended in each region. If testing is incomplete, this approach provides the opportunity to complete them prior to discharge.
Children who present with clinical stigmata suspicious for congenital infections should be evaluated by first reviewing maternal history and serological results, ranking the most frequent infections.
5.8.1. Need to elaborate consensus guidelines to detect risks in children with fever in the first year of life
Fever represents one of the main reasons for pediatric consultation in the first 1,000 days of life. For different reasons children have a greater susceptibility to viral and bacterial infections, which favors the use of antibiotics.
To prevent the excessive use of antibiotics without neglecting the possibility of a serious hidden bacterial infection, risk criteria and diagnostic algorithms for the clinical management of febrile children have been established (89, 90). In addition, with the universal introduction in many sites of effective conjugate vaccines and the incorporation of new molecular tests into the laboratory, documenting a viral etiology has become particularly relevant, especially in the era of antibiotic resistance.
The neonatal period is certainly one of the most important in the management of the pediatric patient with fever and the one with the highest risk for serious bacterial infections. The febrile neonate must be carefully evaluated and, except in very rare cases, must be hospitalized and treated with antibiotics while the pertinent tests are performed to rule out early or late onset sepsis. Ideally, the mother should have been screened for the presence of vaginal and/or rectal colonization by Streptococcus agalactiae (Group B) during pregnancy (89–91).
Beyond the neonatal period and during the first 1,000 days, other risk factors for severe infection become significant, such as protein-calorie malnutrition, lack of breastfeeding, incomplete vaccination schedule, immunosuppressive treatment or immunodeficiency, environmental health conditions, and the presence of infections in the child's home environment (89, 90).
Because of the widespread use of conjugate vaccines, the febrile child is much less likely to have an invasive bacterial infection from the encapsulated pneumococcus, meningococcus, and Haemophilus influenzae type b (90). Escherichia coli urinary tract infections or staphylococcal infections tend to prevail. To guarantee the well-being of young children, it is important to implement clear diagnosis and treatment guidelines in our region to detect viral pathogens, as well as to suspect the presence of serious infections and guarantee the adequate use of antibiotics (10, 89, 90). This would contribute to reduce antimicrobial resistance, a growing problem that must be faced wisely and responsibly.
The coexistence of differing clinical strategies for the management of young febrile infants from various national professional societies or organizations with broad representation, underlies the need for an evidence-based guideline adapted to the realities of our region.
5.9. Encouragement of optimal breastfeeding practices to decrease child death and contribute to the long-term health of children
Multiple studies have shown that breast milk decreases infant mortality. Non-breastfed infants may suffer from more frequent and severe infectious diseases, with a risk of hospitalization up to seven times higher than those receiving breastfeeding (92). Breast milk has all the necessary nutrients for the first months of life: fats, carbohydrates, proteins, vitamins, and minerals. It also contains bioactive factors such as enzymes, hormones, immunomodulatory factors, and bifidogenic components that, in combination with leukocytes, prevent the adherence infectious agents in the neonate and infant. In addition to other nutritious, immunological and emotional advantages, the WHO recommends exclusive breastfeeding until 6 months and supplemented until 2 years of age (92). Unfortunately, the data available from the LAC region reveal that only 50% of newborns are breastfed within the first hour of birth and only 37% maintain continuous breastfeeding during the first 6 months (92, 93).
Breastfeeding allows transfer of immunocompetence to the newborn and the subsequent maturation of the immune system for protection against microbes (94). Human milk also contains lactoferrin, a substance with antimicrobial properties and the ability to modulate the innate and adaptive immune response (95). Its antimicrobial capacity is based on the chelating action of iron necessary for pathogens, which provides bacteriostatic and bactericidal power. The hydrolysis of lactoferrin by pepsin gives rise to peptides called lactoferrin H and B that have greater antimicrobial potency than the predecessor molecule. Other peptides with antimicrobial action are components derived from lactalbumin, lactoperoxidase, lysozyme, milk mucins, tenascin (glycoprotein), and bioactive peptides capable of inhibiting viral growth or suppressing microbial replication (96–98).
Studies have shown a variety of benefits of breastfeeding, of which the decrease in necrotizing enterocolitis, late sepsis, retinopathy of prematurity, and rehospitalization in the first year of life, stand out. More recently, studies have delved into the composition of human breastfeed, and have also established differences between mothers of premature and term infants. In addition, lactoferrin is higher in premature mothers and more concentrated in colostrum (8, 9).
A review to determine the impact of breastfeeding on the rate of hospitalizations in healthy, full-term infants younger than 8 months of age, showed that exclusive and prolonged breastfeeding is a protective factor for hospital admission due to diarrhea or lower respiratory tract infection. However, the protective effect of breastfeeding disappears as time progresses (8). In a prospective cohort study conducted in Turkey to analyze the impact of breastfeeding on frequent pediatric infections, a significant decrease in otitis media and gastroenteritis during the first five years of life with breastfeeding for more than 12 months, was found. These infections were significantly lower in children who had an exclusive breastfeeding for 6 months (40).
Another potential protective effect of breastfeeding is the stimulation of growth of non-pathogenic flora, which reduces colonization by enteropathogens, improves the development of mucosal barriers, and facilitates passage of immune cells, proteins, and anti-infectious enzymes (99). The microbiota present in milk also has peptides and lipids with antimicrobial activity (100).
Protection against some pathogens in the neonatal period can be obtained with the passive acquisition of maternal antibodies. It is well known that the secretory antibodies of human milk from vaccinated pregnant women, such as IgA, the immunoglobin predominant in human milk, protect against influenza (101, 102). The transfer of antibodies into the breast milk of lactating women one week after the initial dose of COVID-19 mRNA vaccine has been demonstrated, suggesting the possibility of passive protection for the infant after maternal vaccination (103).
It has been proposed that exclusive breastfeeding for the first 6 months of life, is the preventive intervention that has the greatest potential impact on infant mortality (104). It does not only provide the necessary and unique nutrients for growth and development, but also becomes the first immunization for the infant (105).
5.10. Rationale and prudent use of antibiotics
Antimicrobial resistance is one of the greatest public health challenges of our time since few treatment options exist for people infected with drug-resistant bacteria. Whereas antibiotics may be lifesavers, they can also be associate with unnecessary adverse events and contribute to the occurrence of antimicrobial resistance.
Animal studies suggest a potential role of the microbiome composition in modulating responses to vaccines (37). A recent retrospective study provided evidence that young children to 24 months of age who were prescribed antibiotics, had a higher frequency of vaccine-induced antibody titers below the levels of protection compared with children with no antibiotic prescriptions. Furthermore, investigators observed a dose-effect between total antibiotic exposure and lower antibody titers. Antibiotic treatment in early life might modify gut microbiome, alter immune responses, and affect vaccine effect (38). These provocative observations clearly deserve future prospective studies as their findings could have major repercussions for immunization programs (39).
Smart use of antibiotics is a key part of best care. Prescribing antibiotics only when needed helps fight antibiotic resistance, and ensures that these life-saving drugs, will be available for future generations (106).
6. Conclusions
LAC still faces immense challenges to overcome the barriers that negatively impact the early and healthy development of children during the first 1,000 days of life. Infectious diseases are a relevant cause of morbidity, associated with significant maternal and infant mortality in the region. Health policy makers from health organization that generate influence in Latin American governments need to be aware and plan strategies within health policies directed to reduce maternal and infant death.
The ten strategies presented by the Advisory Group of SLIPE focus on the current gaps and obstacles identified in the region that negatively affect this vital phase of life. Feasible strategies are provided gradually overcome these barriers. However, to carry out these recommendations, countries of the region need proper planification to accomplish these measures. Suitable venues to facilitate implementation of specific plans, needs to be part of a comprehensive program to optimize attention during this critical period of child's development.
Author contributions
RD: Writing – original draft, Writing – review & editing. JT: Writing – original draft, Writing – review & editing. LF: Writing – original draft, Writing – review & editing. MA: Writing – original draft, Writing – review & editing. JB: Writing – original draft, Writing – review & editing. AG: Writing – original draft, Writing – review & editing. XS: Writing – original draft, Writing – review & editing. AM: Writing – original draft, Writing – review & editing. FM: Writing – original draft, Writing – review & editing. JT: Writing – original draft, Writing – review & editing. LV: Writing – original draft, Writing – review & editing. MS: Writing – original draft, Writing – review & editing. CE: Writing – original draft, Writing – review & editing. RU: Writing – original draft, Writing – review & editing. MP: Writing – original draft, Writing – review & editing. PL: Writing – original draft, Writing – review & editing. EL: Writing – original draft, Writing – review & editing. OR: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors are grateful to Helena Brenes for editing the manuscript and to Silvia Enrique (Essentia-Medical) for program development and logistics support organizing the workshop.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Scott JA. The first 1000 days: a critical period of nutritional opportunity and vulnerability. Nutr Diet. (2020) 77(3):295–7. doi: 10.1111/1747-0080.12617
2. Lake A. The first 1,000 days of a child’s life are the most important to their development—and our economic success. World Economic Forum Annual Meeting (2017). Available at: https://www.weforum.org/agenda/2017/01/the-first-1-000-days-of-a-childs-life-are-the-most-important-to-their-development-and-our-economic-success/
3. Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, et al. Child development: risk factors for adverse outcomes in developing countries. Lancet. (2007) 369(9556):145–57. doi: 10.1016/S0140-6736(07)60076-2
4. Chang S, Zeng L, Brouwer ID, Kok FJ, Yan H. Effect of iron deficiency Anemia in pregnancy on child mental development in rural China. Pediatrics. (2013) 131(3):e755–63. doi: 10.1542/peds.2011-3513
5. Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. (2008) 371(9608):243–60. doi: 10.1016/S0140-6736(07)61690-0
6. Bhutta ZAS. M. A. Childhood infectious diseases: overview. Int Encycl Public Health. (2008):620–40. doi: 10.1016/B978-012373960-5.00568-2
7. UNICEF. A neglected tragedy. the global burden of stillbirths (2020). Available at: https://data.unicef.org/resources/a-neglected-tragedy-stillbirth-estimates-report/
8. Organización Panamericana de la Salud. Indicadores Básicos 2019. Tendencias De La Salud En Las Américas (2019). Available at: http://www.bvs.hn/docum/ops/IndicadoresBasicos2019_spa.pdf
9. Banco Mundial. Tasa De Mortalidad, Neonatal (Por Cada 1.000 Nacidos Vivos)—Latin America & Caribbean (2021). Available at: https://datos.bancomundial.org/indicador/SH.DYN.NMRT?locations=ZJ
10. Global Health Observatory, World Health Organization. Causes of child mortality for the year 2010 Who, Geneva: (2021). Available at: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/child-mortality-and-causes-of-death
11. Chopra M, Mason E, Borrazzo J, Campbell H, Rudan I, Liu L, et al. Ending of preventable deaths from pneumonia and diarrhoea: an achievable goal. Lancet. (2013) 381(9876):1499–506. doi: 10.1016/S0140-6736(13)60319-0
12. Nair H, Simoes EA, Rudan I, Gessner BD, Azziz-Baumgartner E, Zhang JSF, et al. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet. (2013) 381(9875):1380–90. doi: 10.1016/S0140-6736(12)61901-1
13. Rudan I, Nair H, Marusic A, Campbell H. Reducing mortality from childhood pneumonia and diarrhoea: the leading priority is also the greatest opportunity. J Glob Health. (2013) 3(1):010101. doi: 10.7189/jogh.03.010101
14. Rudan I, O'Brien KL, Nair H, Liu L, Theodoratou E, Qazi S, et al. Epidemiology and etiology of childhood pneumonia in 2010: estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J Glob Health. (2013) 3(1):010401. doi: 10.7189/jogh.03.010401
15. Walker CLF, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta ZA, et al. Global burden of childhood pneumonia and diarrhoea. Lancet. (2013) 381(9875):1405–16. doi: 10.1016/S0140-6736(13)60222-6
16. World Health Organization. Regional Update Ew 39, 2013: Influenza and Other Respiratory Viruses (2013). Available at: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiX29HW056BAxWCQzABHbagAwgQFnoECBYQAQ&url=https%3A%2F%2Fwww.paho.org%2Fes%2Ffile%2F36171%2Fdownload%3Ftoken%3DZxaiKn_7&usg=AOvVaw3UWDOuq8btw0ru5VT7XlyQ&opi=89978449
17. Wilson CB, Kollmann TR. Induction of antigen-specific immunity in human neonates and infants. Nestle Nutr Workshop Ser Pediatr Program. (2008) 61:183–95. doi: 10.1159/000113493
18. Corbett NP, Blimkie D, Ho KC, Cai B, Sutherland DP, Kallos A, et al. Ontogeny of toll-like receptor mediated cytokine responses of human blood mononuclear cells. PLoS One. (2010) 5(11):e15041. doi: 10.1371/journal.pone.0015041
19. PrabhuDas M, Adkins B, Gans H, King C, Levy O, Ramilo O, et al. Challenges in infant immunity: implications for responses to infection and vaccines. Nat Immunol. (2011) 12(3):189–94. doi: 10.1038/ni0311-189
20. Kollmann TR, Crabtree J, Rein-Weston A, Blimkie D, Thommai F, Wang XY, et al. Neonatal innate Tlr-mediated responses are distinct from those of adults. J Immunol. (2009) 183(11):7150–60. doi: 10.4049/jimmunol.0901481
21. Halasa NB, O’Shea A, Shi JR, LaFleur BJ, Edwards KM. Poor immune responses to a birth dose of diphtheria, tetanus, and acellular pertussis vaccine. J Pediatr. (2008) 153(3):327–32. doi: 10.1016/j.jpeds.2008.03.011
22. Knuf M, Schmitt HJ, Jacquet JM, Collard A, Kieninger D, Meyer CU, et al. Booster vaccination after neonatal priming with acellular pertussis vaccine. J Pediatr. (2010) 156(4):675–8. doi: 10.1016/j.jpeds.2009.12.019
23. Cuenca AG, Wynn JL, Moldawer LL, Levy O. Role of innate immunity in neonatal infection. Am J Perinatol. (2013) 30(2):105–12. doi: 10.1055/s-0032-1333412
24. Dowling DJ, Levy O. Ontogeny of early life immunity. Trends Immunol. (2014) 35(7):299–310. doi: 10.1016/j.it.2014.04.007
25. Kollmann TR, Levy O, Hanekom W. Vaccine-induced immunity in early life. Vaccine. (2013) 31(21):2481–2. doi: 10.1016/j.vaccine.2013.04.025
26. Pantell RH, Roberts KB, Adams WG, Dreyer BP, Kuppermann N, O'Leary ST, et al. Evaluation and management of well-appearing febrile infants 8 to 60 days old. Pediatrics. (2021) 148(2):e2021052228. doi: 10.1542/peds.2021-052228
27. Nakaya HI, Wrammert J, Lee EK, Racioppi L, Marie-Kunze S, Haining WN, et al. Systems biology of vaccination for seasonal influenza in humans. Nat Immunol. (2011) 12(8):786–95. doi: 10.1038/ni.2067
28. Querec T, Bennouna S, Alkan S, Laouar Y, Gorden K, Flavell R, et al. Yellow fever Vaccine Yf-17d activates multiple dendritic cell subsets via Tlr2, 7, 8, and 9 to stimulate polyvalent immunity. J Exp Med. (2006) 203(2):413–24. doi: 10.1084/jem.20051720
29. Obermoser G, Presnell S, Domico K, Xu H, Wang Y, Anguiano E, et al. Systems scale interactive exploration reveals quantitative and qualitative differences in response to influenza and pneumococcal vaccines. Immunity. (2013) 38(4):831–44. doi: 10.1016/j.immuni.2012.12.008
30. Furman D, Davis MM. New approaches to understanding the immune response to vaccination and infection. Vaccine. (2015) 33(40):5271–81. doi: 10.1016/j.vaccine.2015.06.117
31. Furman D, Jojic V, Sharma S, Shen-Orr SS, Angel CJ, Onengut-Gumuscu S, et al. Cytomegalovirus infection enhances the immune response to influenza. Sci Transl Med. (2015) 7(281):281ra43. doi: 10.1126/scitranslmed.aaa2293
32. de St G F, Webster RG. Disquisitions of original antigenic sin. I. Evidence in man. J Exp Med. (1966) 124(3):331–45. doi: 10.1084/jem.124.3.331
33. Roltgen K, Nielsen SCA, Silva O, Younes SF, Zaslavsky M, Costales C, et al. Immune imprinting, breadth of variant recognition, and germinal center response in human Sars-Cov-2 infection and vaccination. Cell. (2022) 185(6):1025–40 e14. doi: 10.1016/j.cell.2022.01.018
34. Rothman AL. Immunity to dengue virus: a tale of original antigenic sin and tropical cytokine storms. Nat Rev Immunol. (2011) 11(8):532–43. doi: 10.1038/nri3014
35. Mejias A, Dimo B, Suarez NM, Garcia C, Suarez-Arrabal MC, Jartti T, et al. Whole blood gene expression profiles to assess pathogenesis and disease severity in infants with respiratory syncytial virus infection. PLoS Med. (2013) 10(11):e1001549. doi: 10.1371/journal.pmed.1001549
36. Hall CB, Weinberg GA, Iwane MK, Blumkin AK, Edwards KM, Staat MA, et al. The burden of respiratory syncytial virus infection in young children. N Engl J Med. (2009) 360(6):588–98. doi: 10.1056/NEJMoa0804877
37. Belkaid Y, Harrison OJ. Homeostatic immunity and the microbiota. Immunity. (2017) 46(4):562–76. doi: 10.1016/j.immuni.2017.04.008
38. Chapman TJ, Pham M, Bajorski P, Pichichero ME. Antibiotic use and vaccine antibody levels. Pediatrics. (2022) 149(5):e2021052061. doi: 10.1542/peds.2021-052061
39. Ramilo O, Mejias A. Antibiotics and immunizations: a complex interaction. Pediatrics. (2022) 149(5):e2021055610. doi: 10.1542/peds.2021-055610
40. UNICEF. The state of the world’s children 2023. for every child, vaccination (2023). Available at: https://www.unicef.org/reports/state-worlds-children-2023
41. Organización Mundial de la Salud. Maternal mortality (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality
42. Castro A. Maternal and child mortality worsens in Latin America and the Caribbean. Lancet. (2020) 396(10262):e85. doi: 10.1016/S0140-6736(20)32142-5
43. FAO, FIDA, OPS, WFP, UNICEF. América Latina Y el caribe—panorama regional De la seguridad Alimentaria Y nutricional 2021: EstadíSticas Y tendencias. United States: FAO, FIDA, OPS, WFP y UNICEF (2021). Available at: https://www.fao.org/3/cb7497es/cb7497es.pdf
44. Organización Panamerica de la Salud. Nuevo Informe De La Onu: El Hambre En América Latina Y El Caribe Aumentó En 13,8 Millones De Personas En Solo Un Año (2021). Available at: https://www.paho.org/es/noticias/30-11-2021-nuevo-informe-onu-hambre-america-latina-caribe-aumento-138-millones-personas
45. Meira CAR, Buccini G, Azeredo CM, Conde WL, Rinaldi AEM. Evolution of breastfeeding indicators and early introduction of foods in Latin American and Caribbean countries in the decades of 1990, 2000 and 2010. Int Breastfeed J. (2022) 17(1):32. doi: 10.1186/s13006-022-00477-6
46. UNICEF. Unicef-who-the world bank: joint child malnutrition estimates — levels and trends—2020 edition (2020). Available at: https://data.unicef.org/resources/jme-report-2020/
47. Serie Derechos Humanos Y Salud. Medio ambiente Y cambio climático: un enfoque basado en los derechos humanos. United States: Organización Panamerica de la Salud (2022). Available at: https://iris.paho.org/bitstream/handle/10665.2/55293/OPSLEGDHdhs7210001_spa.pdf?sequence=4&isAllowed=y
48. Heng YY, Asad I, Coleman B, Menard L, Benki-Nugent S, Hussein Were F, et al. Heavy metals and neurodevelopment of children in low and middle-income countries: a systematic review. PLoS One. (2022) 17(3):e0265536. doi: 10.1371/journal.pone.0265536
49. Olivero-Verbel JA-O N, Alcala-Orozco M, Caballero-Gallardo K. Population exposure to lead and mercury in Latin America. Curr Opinion Toxicol. (2021) 27(5):27–37. doi: 10.1016/j.cotox.2021.06.002
50. Olympio KP, Goncalves CG, Salles FJ, Ferreira AP, Soares AS, Buzalaf MA, et al. What are the blood lead levels of children living in Latin America and the Caribbean? Environ Int. (2017) 101:46–58. doi: 10.1016/j.envint.2016.12.022
51. Wright C, Blake N, Glennie L, Smith V, Bender R, Kyu H, et al. The global burden of meningitis in children: challenges with interpreting global health estimates. Microorganisms. (2021) 9(2):377. doi: 10.3390/microorganisms9020377
52. Le Govic Y, Demey B, Cassereau J, Bahn YS, Papon N. Pathogens infecting the central nervous system. PLoS Pathog. (2022) 18(2):e1010234. doi: 10.1371/journal.ppat.1010234
53. Bottomley MJ, Serruto D, Safadi MA, Klugman KP. Future challenges in the elimination of bacterial meningitis. Vaccine. (2012) 30(Suppl 2):B78–86. doi: 10.1016/j.vaccine.2011.12.099
54. Collaborators GBDDD. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: a systematic analysis for the global burden of disease study 2015. Lancet Infect Dis. (2017) 17(9):909–48. doi: 10.1016/S1473-3099(17)30276-1
55. Lopez-Medina E, Parra B, Davalos DM, Lopez P, Villamarin E, Pelaez M. Acute gastroenteritis in a pediatric population from cali, Colombia in the post rotavirus vaccine era. Int J Infect Dis. (2018) 73:52–9. doi: 10.1016/j.ijid.2018.06.006
56. Foster YY, Correoso Guevara JD, Nuñez-Ortega JM. Factores de riesgo de enfermedad diarreica aguda en menores de 5 años. Revista Médico Científica. (2021) 34(1):1–8. doi: 10.37416/rmc.v34i1.573
57. Gentile A, Bardach A, Ciapponi A, Garcia-Marti S, Aruj P, Glujovsky D, et al. Epidemiology of community-acquired pneumonia in children of Latin America and the Caribbean: a systematic review and meta-analysis. Int J Infect Dis. (2012) 16(1):e5–15. doi: 10.1016/j.ijid.2011.09.013
58. Comite de N, Comite de I, Comite de Medicina Interna P, Comite de Pediatria Ambulatoria y C, Comite de Pediatria A. Recommendations for the management of acute lower respiratory infections in children under 2 years of age. Update 2021. Arch Argent Pediatr. (2021) 119(4):S171–S97. doi: 10.5546/aap.2021.S171
59. UNHCR. Global trends report 2021: the un refugee agency (2021). Available at: https://www.unhcr.org/media/global-trends-report-2021
60. Council On Environmental H. Global climate change and children’s health. Pediatrics. (2015) 136(5):992–7. doi: 10.1542/peds.2015-3232
61. United Nations Development Programme. Sustainable development goals—Sdgs and the 2030 Agenda (2023). Available at: https://www.undp.org/sustainable-development-goals?utm_source=EN&utm_medium=GSR&utm_content=US_UNDP_PaidSearch_Brand_English&utm_campaign=CENTRAL&c_src=CENTRAL&c_src2=GSR&gclid=Cj0KCQjwwtWgBhDhARIsAEMcxeDLCCG0Q5jp81irPm0ZxvAchGd-97OKdggu9jNQ3zep3IhJO76FsKAaAipwEALw_wcB
62. Pan American Health Organization. Iniciativa Regional Para La Eliminación De La Transmisión Maternoinfantil Del Vih Y De La Sífilis Congénita En América Latina Y El Caribe: Documento Conceptual (2009). Available at: https://iris.paho.org/handle/10665.2/49406
63. . . Acog committee opinion No. 762: prepregnancy counseling. Obstet Gynecol. (2019) 133(1):e78–89. doi: 10.1097/AOG.0000000000003013
64. FAO; IFAD; UNICEF; PAHO; WFP. Regional overview of food security and nutrition in latin america and the caribbean: towards improving affordability of healthy diets (2023). Available at: https://www.fao.org/documents/card/en/c/cc3859en
65. Orjuela-Grimm M, Deschak C, Aragon Gama CA, Bhatt Carreno S, Hoyos L, Mundo V, et al. Migrants on the move and food (in) security: a call for research. J Immigr Minor Health. (2022) 24(5):1318–27. doi: 10.1007/s10903-021-01276-7
66. Centers for Disease C. Rubella vaccination during pregnancy—United States, 1971–1988. MMWR Morb Mortal Wkly Rep. (1989) 38(17):289–93.2496289
67. Hamkar R, Jalilvand S, Abdolbaghi MH, Esteghamati AR, Hagh-Goo A, Jelyani KN, et al. Inadvertent Rubella vaccination of pregnant women: evaluation of possible transplacental infection with Rubella vaccine. Vaccine. (2006) 24(17):3558–63. doi: 10.1016/j.vaccine.2006.02.001
68. Bar-Oz B, Levichek Z, Moretti ME, Mah C, Andreou S, Koren G. Pregnancy outcome following Rubella vaccination: a prospective controlled study. Am J Med Genet A. (2004) 130A(1):52–4. doi: 10.1002/ajmg.a.30225
69. Center for Disease Control and Prevention. Covid-19 vaccines while pregnant or breastfeeding (2022). Available at: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html#:∼:text=CDC%20recommends%20COVID%2D19%20vaccines,become%20pregnant%20in%20the%20future
70. Sudarshan MK, Giri MS, Mahendra BJ, Venkatesh GM, Sanjay TV, Narayana DH, et al. Assessing the safety of post-exposure rabies immunization in pregnancy. Hum Vaccin. (2007) 3(3):87–9. doi: 10.4161/hv.3.3.4010
71. Manning SE, Rupprecht CE, Fishbein D, Hanlon CA, Lumlertdacha B, Guerra M, et al. Human rabies prevention--United States, 2008: recommendations of the advisory committee on immunization practices. MMWR Recomm Rep. (2008) 57(RR-3):1–28.18496505
72. Cavalcanti DP, Salomao MA, Lopez-Camelo J, Pessoto MA, Campinas Group of Yellow Fever Immunization during P. Early exposure to yellow fever vaccine during pregnancy. Trop Med Int Health. (2007) 12(7):833–7. doi: 10.1111/j.1365-3156.2007.01851.x
73. World Health Organization. Vaccines and vaccination against yellow fever. Who position paper—June 2013. Wkly Epidemiol Rec. (2013) 88(27):269–83.23909008
74. World Health Organization. Immunization coverage (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage
75. Pan American Health Organization. Immunization in the Americas: 2022 summary (2022). Available at: https://www.paho.org/en/documents/immunization-americas-2022-summary
76. Castrejon MM, Leal I, de Jesus Pereira Pinto T, Guzman-Holst A. The impact of COVID-19 and catch-up strategies on routine childhood vaccine coverage trends in Latin America: a systematic literature review and database analysis. Hum Vaccin Immunother. (2022) 18(6):2102353. doi: 10.1080/21645515.2022.2102353
77. Aguero ML A, Castillo JBD, Falleiros-Arlant LH, Berezin E, de Moraes JC, Torres-Martinez C, et al. Risks of low vaccination coverage and strategies to prevent the resurgence of vaccine-preventable diseases in infants in the COVID-19 pandemic scenario: recommendations for Latin America and the Caribbean by the group of experts on infant immunization for Latin America. Expert Rev Vac. (2023) 22(1):1091–101. doi: 10.1080/14760584.2023.2271057
78. Sachs JD, Karim SSA, Aknin L, Allen J, Brosbol K, Colombo F, et al. The lancet commission on lessons for the future from the COVID-19 pandemic. Lancet. (2022) 400(10359):1224–80. doi: 10.1016/S0140-6736(22)01585-9
79. Castellanos LGG, Kurtis H, Mello MB, Perez F, Ropero AM, Salvatella R, et al. Etmi Plus—Marco Para La Eliminación De La Transmisión Maternoinfantil Del Vih, La Sífilis, La Hepatitis Y La Enfermedad De Chagas (2017). Available at: www.paho.org/hq/dmdocuments/2017/2017-cha-etmi-plus-marco-vihhep-chagas.pdf
80. Pan American Health Organization. Epidemiological review of Syphilis in the Americas (2021). Available at: https://www.paho.org/en/documents/epidemiological-review-syphilis-americas-december-2021
81. Verani JR, McGee L, Schrag SJ. Division of bacterial diseases NCfI, respiratory diseases CfDC, prevention. prevention of perinatal group B streptococcal disease-revised guidelines from Cdc, 2010. MMWR Recomm Rep. (2010) 59(RR-10):1–36.21088663
82. Stillwaggon E, Carrier CS, Sautter M, McLeod R. Maternal serologic screening to prevent congenital toxoplasmosis: a decision-analytic economic model. PLoS Negl Trop Dis. (2011) 5(9):e1333. doi: 10.1371/journal.pntd.0001333
83. Lappalainen M, Sintonen H, Koskiniemi M, Hedman K, Hiilesmaa V, Ammala P, et al. Cost-benefit analysis of screening for toxoplasmosis during pregnancy. Scand J Infect Dis. (1995) 27(3):265–72. doi: 10.3109/00365549509019020
84. Foulon W, Naessens A, Ho-Yen D. Prevention of congenital toxoplasmosis. J Perinat Med. (2000) 28(5):337–45. doi: 10.1515/JPM.2000.043
85. Group SS, Thiebaut R, Leproust S, Chene G, Gilbert R. Effectiveness of prenatal treatment for congenital toxoplasmosis: a meta-analysis of individual patients’ data. Lancet. (2007) 369(9556):115–22. doi: 10.1016/S0140-6736(07)60072-5
86. Manicklal S, Emery VC, Lazzarotto T, Boppana SB, Gupta RK. The "silent" global burden of congenital cytomegalovirus. Clin Microbiol Rev. (2013) 26(1):86–102. doi: 10.1128/CMR.00062-12
87. Morton CC, Nance WE. Newborn hearing screening-a silent revolution. N Engl J Med. (2006) 354(20):2151–64. doi: 10.1056/NEJMra050700
88. Adler SP, Marshall B. Cytomegalovirus infections. Pediatr Rev. (2007) 28(3):92–100. doi: 10.1542/pir.28-3-92
89. Orfanos I, Elfving K, Sotoca Fernandez J, Wennlund L, Weiber S, Eklund EA, et al. Management and outcome of febrile infants </=60 days, with emphasis on infants </=21 days old, in Swedish pediatric emergency departments. Pediatr Infect Dis J. (2022) 41(7):537–43. doi: 10.1097/INF.0000000000003542
90. Byington CL, Enriquez FR, Hoff C, Tuohy R, Taggart EW, Hillyard DR, et al. Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. (2004) 113(6):1662–6. doi: 10.1542/peds.113.6.1662
91. Furfaro LL, Chang BJ, Payne MS. Perinatal streptococcus agalactiae epidemiology and surveillance targets. Clin Microbiol Rev. (2018) 31(4):e00049–18. doi: 10.1128/CMR.00049-18
92. Cruz-Hernandez MG-G, Garcia Garcia JJ, Cruz-Martinez O, Mintegi-Raso S, Moreno-Villares JM. Manual De pediatría. Spain: Ergon (2019). Available at: https://dialnet.unirioja.es/servlet/libro?codigo=831916
93. Picciano MF. Human milk: nutritional aspects of a dynamic food. Biol Neonate. (1998) 74(2):84–93. doi: 10.1159/000014015
94. Field CJ. The immunological components of human milk and their effect on immune development in infants. J Nutr. (2005) 135(1):1–4. doi: 10.1093/jn/135.1.1
95. Legrand D. Overview of lactoferrin as a natural immune modulator. J Pediatr. (2016) 173:Suppl:S10-5. doi: 10.1016/j.jpeds.2016.02.071
96. Wada Y, Lonnerdal B. Bioactive peptides derived from human milk proteins-mechanisms of action. J Nutr Biochem. (2014) 25(5):503–14. doi: 10.1016/j.jnutbio.2013.10.012
97. Ng TB, Cheung RC, Wong JH, Wang Y, Ip DT, Wan DC, et al. Antiviral activities of whey proteins. Appl Microbiol Biotechnol. (2015) 99(17):6997–7008. doi: 10.1007/s00253-015-6818-4
98. Drago-Serrano ME, Campos-Rodriguez R, Carrero JC, de la Garza M. Lactoferrin: balancing ups and downs of inflammation due to microbial infections. Int J Mol Sci. (2017) 18(3):501. doi: 10.3390/ijms18030501
99. Brandtzaeg P. The mucosal immune system and its integration with the mammary glands. J Pediatr. (2010) 156(2 Suppl):S8–15. doi: 10.1016/j.jpeds.2009.11.014
100. Fernandez L, Langa S, Martin V, Maldonado A, Jimenez E, Martin R, et al. The human milk Microbiota: origin and potential roles in health and disease. Pharmacol Res. (2013) 69(1):1–10. doi: 10.1016/j.phrs.2012.09.001
101. Henkle E, Steinhoff MC, Omer SB, Roy E, Arifeen SE, Raqib R, et al. The effect of exclusive breast-feeding on respiratory illness in young infants in a maternal immunization trial in Bangladesh. Pediatr Infect Dis J. (2013) 32(5):431–5. doi: 10.1097/INF.0b013e318281e34f
102. Schlaudecker EP, Steinhoff MC, Omer SB, McNeal MM, Roy E, Arifeen SE, et al. Iga and neutralizing antibodies to influenza a virus in human milk: a randomized trial of antenatal influenza immunization. PLoS One. (2013) 8(8):e70867. doi: 10.1371/journal.pone.0070867
103. Baird JK, Jensen SM, Urba WJ, Fox BA, Baird JR. Sars-Cov-2 antibodies detected in mother’s milk post-vaccination. J Hum Lact. (2021) 37(3):492–8. doi: 10.1177/08903344211030168
104. Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS. Bellagio child survival study G. How many child deaths can we prevent this year? Lancet. (2003) 362(9377):65–71. doi: 10.1016/S0140-6736(03)13811-1
105. Horta BLV, Victora CG. Long-Term effects of breastfeeding: a systematic review. United States: World Health Organization (2013). Available at: https://apps.who.int/iris/bitstream/handle/10665/79198/9789241505307_eng.pdf;jsessionid=04B821DB34FBCA65AC93879FF0AA5978?sequence=1
106. Centers for Disease Control and Prevention. Antibiotic prescribing and use (2023). Available at: https://www.cdc.gov/antibiotic-use/index.html
Keywords: first 1,000 days of life, pregnancy immunization, infant immunization, pediatric, social determinants of health
Citation: Debbag R, Torres JR, Falleiros-Arlant LH, Avila-Aguero ML, Brea-del Castillo J, Gentile A, Saez-Llorens X, Mascarenas A, Munoz FM, Torres JP, Vazquez L, Safadi MA, Espinal C, Ulloa-Gutierrez R, Pujadas M, Lopez P, López-Medina E and Ramilo O (2023) Are the first 1,000 days of life a neglected vital period to prevent the impact on maternal and infant morbimortality of infectious diseases in Latin America? proceedings of a workshop of experts from the Latin American pediatric infectious diseases society, SLIPE. Front. Pediatr. 11:1297177. doi: 10.3389/fped.2023.1297177
Received: 19 September 2023; Accepted: 15 November 2023;
Published: 30 November 2023.
Edited by:
George A. Syrogiannopoulos, University of Thessaly, GreeceReviewed by:
Fani Ladomenou, University of Crete, GreeceBenhur Sirvan Cetin, Erciyes University, Türkiye
Jussi Mertsola, University of Turku, Finland
© 2023 Debbag, Torres, Falleiros-Arlant, Avila-Aguero, Brea-del Castillo, Gentile, Saez-Llorens, Mascarenas, Munoz, Torres, Vazquez, Safadi, Espinal, Ulloa-Gutierrez, Pujadas, Lopez, López-Medina and Ramilo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberto Debbag cmRlYmJhZ0Bob3RtYWlsLmNvbQ==