 Christina H. Wolfsberger1,2*
Christina H. Wolfsberger1,2* Nina Höller1,2
Nina Höller1,2 Nariae Baik-Schneditz1,2
Nariae Baik-Schneditz1,2 Bernhard Schwaberger1,2
Bernhard Schwaberger1,2 Ena Suppan1,2
Ena Suppan1,2 Lukas Mileder1,2
Lukas Mileder1,2 Alexander Avian3
Alexander Avian3 Berndt Urlesberger1,2
Berndt Urlesberger1,2 Gerhard Pichler1,2
Gerhard Pichler1,2
- 1Division of Neonatology, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria
- 2Research Unit for Neonatal Micro- and Macrocirculation, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria
- 3Institute for Medical Informatics, Statistics and Documentation, Medical University of Graz, Graz, Austria
Background: Peripheral muscle fractional tissue oxygen extraction (pFTOE) represents the relative extraction of oxygen from the arterial to venous compartment, providing information about dynamic changes of oxygen delivery and oxygen consumption. The aim of the present study was to establish reference values of pFTOE during the first 24 h after birth in stable term and late preterm neonates.
Methods: The present study is a post-hoc analysis of secondary outcome parameters of prospective observational studies. Only stable neonates without infection, asphyxia and any medical support were eligible for our analysis to obtain normal values. For measurements of peripheral muscle tissue oxygenation index (pTOI) during the first 24 h after birth in term and preterm neonates, the NIRO200/NIRO200NX was used. Arterial oxygen saturation (SpO2) was obtained by pulse oximetry. pFTOE was calculated out of pTOI and SpO2: pFTOE = (SpO2-pTOI)/SpO2. Measurements of neonates were stratified into four groups according to their respective measurement time point (6 h periods) after birth. Term and preterm neonates were analyzed separately. Mean values of measurements during the first time period (0–6 h after birth) were compared to measurements of the following time periods (second = 7–12 h, third = 13–18 h, fourth = 19–24 h after birth).
Results: Two-hundred-fourty neonates (55 term and 185 late preterm neonates) had at least one peripheral muscle NIRS measurements within the first 24 h after birth. Mean gestational age and birth weight were 39.4 ± 1.1 weeks and 3360 (2860–3680)g in term neonates and 34.0 ± 1.4 weeks and 2060 (1750–2350)g in preterm neonates, respectively. In term neonates pFTOE was 0.264 (0.229–0.300), 0.228 (0.192–0.264), 0.237 (0.200–0.274) and 0.220 (0.186–0.254) in the first, second, third and fourth time period. In preterm neonates pFTOE was 0.229 (0.213–0.246), 0.225 (0.209–0.240), 0.226 (0.210–0.242) and 0.238 (0.222–0.255) in the first, second, third and fourth time period. pFTOE did not show any significant changes between the time periods, neither in term nor in preterm neonates.
Conclusion: We provide reference values of pFTOE for stable term and late preterm neonates within the first 24 h after birth, which were stable when comparing four 6-h periods. These normal values are of great need for interpreting pFTOE in scientific context as well as for potential future clinical applications.
Introduction
Peripheral muscle oxygenation, may serve as a sensitive early marker of sepsis or shock in neonates due to disturbances in microcirculation, as described in several studies within the last decades (1, 2). Peripheral muscle oxygenation can be monitored continuously and non-invasively using near-infrared spectroscopy (NIRS), which measures oxygenated hemoglobin (O2Hb) and deoxygenated hemoglobin (HHb) in venous (70%), capillary (20%) and arteriolar (10%) compartments (3, 4). When combining peripheral muscle NIRS monitoring with the venous occlusion method, information about oxygenation, perfusion, oxygen consumption and oxygen delivery can be obtained by different calculations based on changes in O2Hb and HHb during the occlusion (5, 6). One parameter obtained by this method is peripheral muscle fractional oxygen extraction (pFOE). pFOE represents the relative extraction from the arterial to venous compartment and is calculated out of peripheral muscle oxygen consumption (pVO2) and peripheral muscle oxygen delivery (pDO2) (5, 6): pFOE = pVO2/pDO2. Another parameter which can be obtained by peripheral muscle measurements is peripheral muscle fractional tissue oxygen extraction (pFTOE). pFTOE represents the relative oxygen extraction from arterial compartments to compartments of smaller arterial and venous vessels and capillaries. For calculation of this parameter, measurement of peripheral muscle tissue oxygenation index (pTOI) is necessary. pTOI is obtained by NIRS, using the spatially resolved method, which enables a non-invasive continuous measurement without venous occlusions. Using pTOI and arterial oxygen saturation (SpO2) pFTOE can be calculated using the following equation: pFTOE = (SpO2-pTOI)/SpO2 (7).
pFTOE has been described in several studies in preterm neonates during the first 24 h after birth (8–10). A possible comparability of pFOE and pFTOE was investigated by Hoeller et al. (11). This study described that pFOE and pFTOE show the same trend but cannot be equated, as pFOE values were found to be higher compared to pFTOE values.
As venous occlusions have some limitations including the susceptibility to movement artefacts and the limited applicability in clinical routine due to time constraints (4, 12), pFTOE is a value that might be implemented in clinical routine much easier than pFOE. However, up to now only studies on pFOE during the first 24 h after birth have been published (13). Thus, reference values of pFTOE during the first 24 h after birth are missing, which would be essential for future clinical applications of pFTOE measurements.
Therefore, the aim of the present study was to establish reference values of pFTOE during the first 24 h after birth in stable term and late preterm neonates.
Methods
Study design and analyses
In this post-hoc analysis, secondary outcome parameters obtained in five prospective observational studies with peripheral muscle oxygenation measurements during the first 24 h after birth were analyzed (10, 14, 15). These studies were conducted between January 2008 and December 2022 at the Division of Neonatology, Medical University of Graz, Austria. All studies were approved by the Regional Committee on Biomedical Research Ethics (EC numbers: 19–291 ex 07/08, 21–149 ex 09/10, 23–402 ex 10/11, 25–237 ex 12/13 and 33–161 ex 20/21). Written parental consent was obtained prior to patient inclusion in all studies.
To establish reference values for pFTOE during the first 24 h after birth, four time periods were defined according to the time-point of measurements of peripheral muscle oxygenation: 0–6 h after birth (starting after the first 15 min after birth) (“first time period”), 7–12 h after birth (“second time period”), 13–18 h after birth (“third time period”) and 19–24 h after birth (“fourth time period”). Mean pFTOE values of each time period were calculated for term and for preterm neonates. Values of the first “6 h period” were compared to the following measurement periods.
Patients
Only stable neonates after admission to the neonatal intensive care unit (NICU) with available pFTOE values were included into our analysis to define normal values. Neonates with intensive medical (inotropes or vasopressors) or invasive and non-invasive respiratory support, perinatal asphyxia (defined as an umbilical artery pH below 7.00) or severe congenital malformations were excluded. Furthermore, neonates with clinical signs of infection, defined as C-reactive protein values higher than 10 mg/L, leucocyte counts above 34000 /µl, immature-to-total neutrophil ratio > 0.20 or positive blood cultures during the first 24 h after birth were excluded.
Study protocols of included prospective observational studies
In one (EC number: 33–161 ex 20/21) out of the five included studies with pFTOE measurements, peripheral muscle measurements were performed within the first six hours after birth by five short reapplications. The mean pFTOE value of these reapplications was calculated for further analysis.
Peripheral muscle oxygenation measurements in the other four prospective observational studies were performed continuously for a varying time period within the first 24 h after birth. Out of these measurements, the mean pFTOE for each “6 h time period” was calculated and used for further analysis.
Medical history
Demographic data including sex, birth weight, gestational age, Apgar scores, umbilical artery pH and mode of delivery were documented.
Measurements during the first 24 h after birth
Peripheral muscle oxygenation monitoring with NIRS, as mentioned above, were conducted when the term or preterm neonate were in a stable condition at the NICU, at least 15 min after birth. Measurements of pTOI were performed either with continuous measurements during the first 24 h after birth, with a fixed NIRS probe on the right forearm, or with five reapplications, according to the study protocol. For reapplications, the NIRS probe was held gently by the examiner on the neonates’ right forearm for approximately 30 s and was then removed for a 10 s period. After that, the sensor was reapplied for further four times in the same position. The mean value of the five peripheral muscle measurements was documented.
In all prospective observational studies, peripheral muscle oxygenation measurements with NIRS were performed according to already published quality criteria and recommendations (12), using the NIRO 200 or NIRO 200NX device (Hamamatsu Photonics, Hamamatsu, Shizuoka, Japan). The interoptode distance for peripheral muscle oxygenation measurements was chosen in accordance to the birth weight of the neonate: 3.0 cm in neonates with a birth weight >1500 g and 2.0 cm in preterm neonates with a birth weight <1500 g. The thickness of the subcutaneous fat tissue and the diameter of the forearm were evaluated by ultrasound using the GE Logiq S8 (GE Health Care, Chicago, United States). Routine monitoring parameters including SpO2 and heart rate (HR) were continuously measured with pulse oximetry using either the IntelliVue MP50 or MX750 monitor (Philips, Eindhoven, The Netherlands). Non-invasively measured mean arterial blood pressure (MABP) was documented at least once in a stable condition at the NICU within the first 24 h after birth, using either the IntelliVue MP50 or MX750 monitor (Philips, Eindhoven, The Netherlands). Peripheral and rectal body temperature were measured using a skin and rectal probe, respectively. All monitoring data were stored in the polygraphic system “alpha-trace digital MM” (B.E.S.T Medical Systems, Vienna, Austria) for subsequent analysis.
Peripheral muscle fractional tissue oxygen extraction (pFTOE)
pFTOE was calculated out of SpO2 and pTOI using the following equation (7):
Statistical analysis
Demographic data were described as absolute and relative numbers, mean ± SD or median IQR, as appropriate. Courses of pFTOE, pTOI, SpO2 and HR within the first 24 h after birth were analysed using a linear mixed model with fixed effects for time and group (term vs preterm neonates). A first order autoregressive covariance structure was used. Post hoc analysis for group differences at each time period was performed. Results according to this analysis are presented as estimated means and 95% confidence intervals. A p value < 0.05 was considered statistically significant. The statistical analyses were performed using IBM SPSS Statistics 28.0.1 (IBM Corporation; Armonk, USA).
Results
Seven-hundred-twenty-five term and late preterm neonates were included in the five prospective observational studies. For the present study, we excluded 357 neonates receiving respiratory support, 101 neonates with clinical and/or laboratory signs of infection, 17 neonates with an umbilical artery pH of <7.00 and ten neonates receiving inotropes or vasopressors. Finally, 240 neonates, 55 term and 185 late preterm neonates, were eligible for the final analysis (Figure 1). Demographic data of the included term and preterm neonates are presented in Table 1. Preterm neonates were admitted to the NICU due to gestational age <34 weeks and/or a birth weight <2000 g (n = 58).
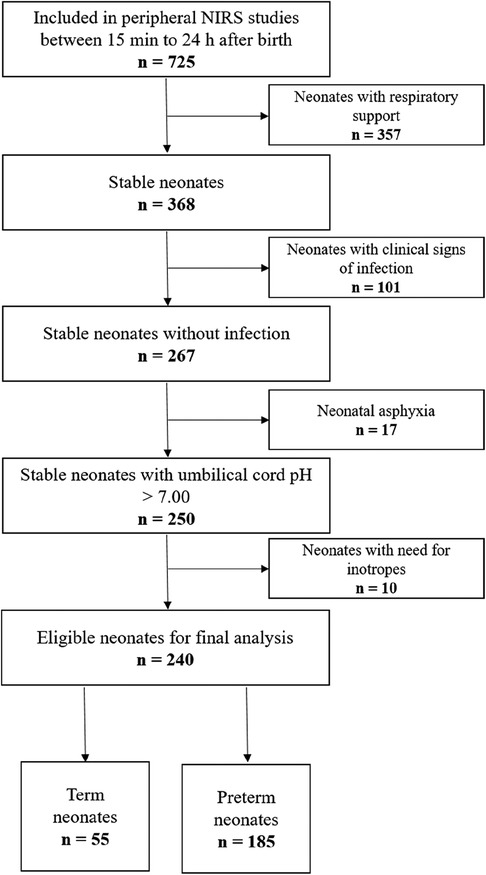
Figure 1. Study flow chart of term and preterm neonates with pFTOE measurements after admission to the neonatal intensive care unit during the first 24 h after birth.
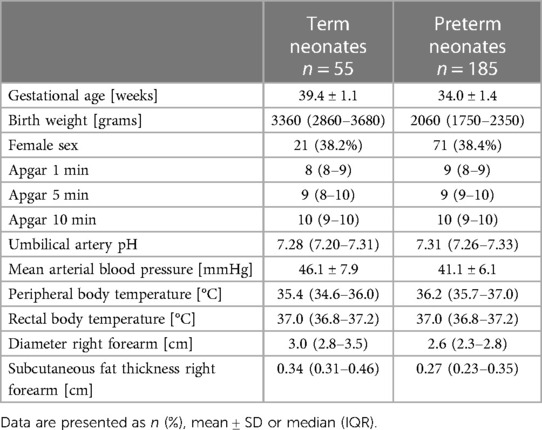
Table 1. Demographic data of term and preterm neonates with pFTOE measurements during the first 24 h after birth.
pFTOE and pTOI as well as routine monitoring variables are presented in Table 2. pFTOE did not differ between term and preterm during the first 24 h after birth (Table 2, Figure 2) (p = 0.591). Furthermore, there were no significant differences between all four time periods in term and preterm neonates (p = 0.303) and courses of pFTOE were similar between term and preterm neonates (p = 0.137). According to the model the highest value of pFTOE in term neonates was observed in the first time period [estimated mean: 0.264 (95% CI: 0.029–0.300)], whereas in preterm neonates the highest pFTOE value [0.238 (0.222–0.255)] was observed in the fourth time period. Looking on each time period, also no differences in pFTOE between term and preterm neonates could be observed: “first time period” [p = 0.080], “second time period” [p = 0.866]), “third time period” [p = 0.597] and “fourth time period” [p = 0.342]) (Table 2). pTOI also showed no differences between term and preterm neonates (p = 0.705), no changes over time (p = 0.423) and comparable courses of groups (p = 0.125) (Figure 3).
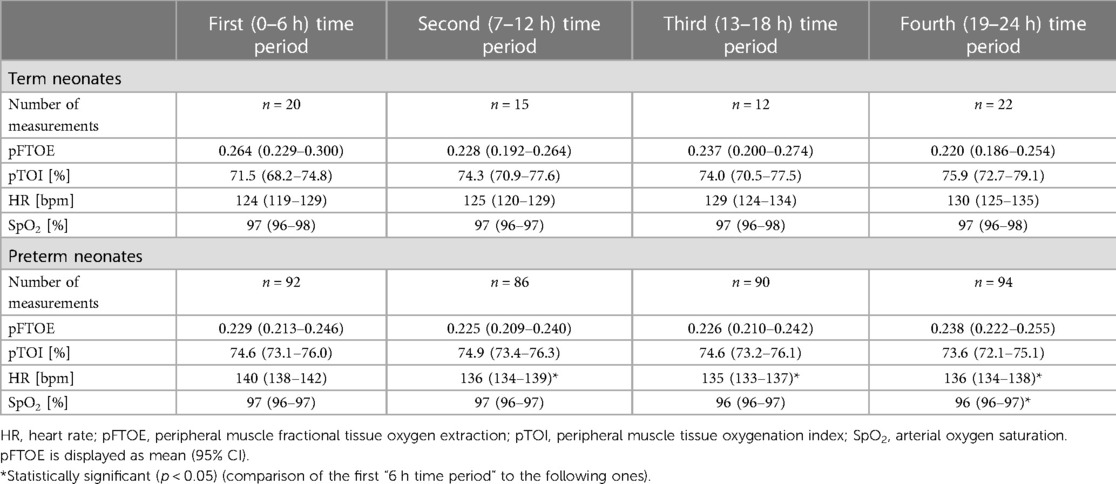
Table 2. Peripheral muscle oxygenation parameters (pFTOE and pTOI) and routine monitoring parameters of stable term and preterm neonates with peripheral muscle oxygenation measurements during the first 24 h after birth.
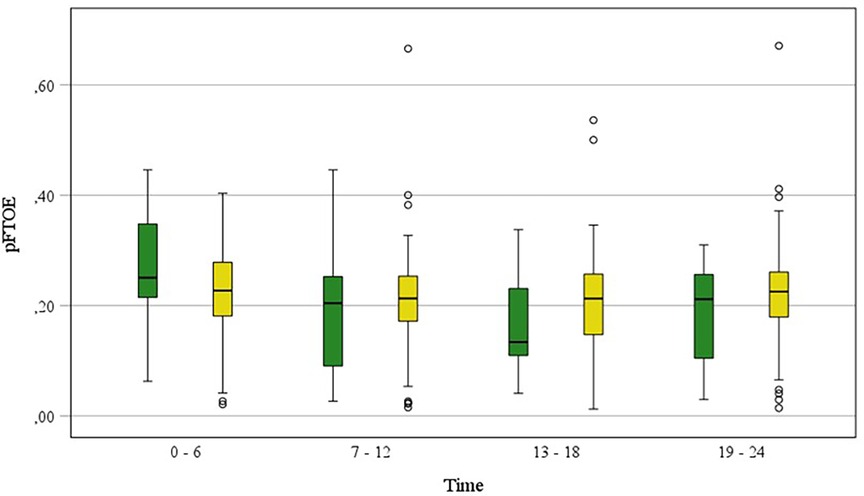
Figure 2. pFTOE measured with NIRS in stable term and preterm neonates during the first 24 h after birth, grouped in “6 h time periods” (“0–6 h”, “7–12 h”, “13–18 h”, “19–24 h”). Term neonates are displayed in green blots and preterm neonates in yellow blots. Values are presented as median (IQR).
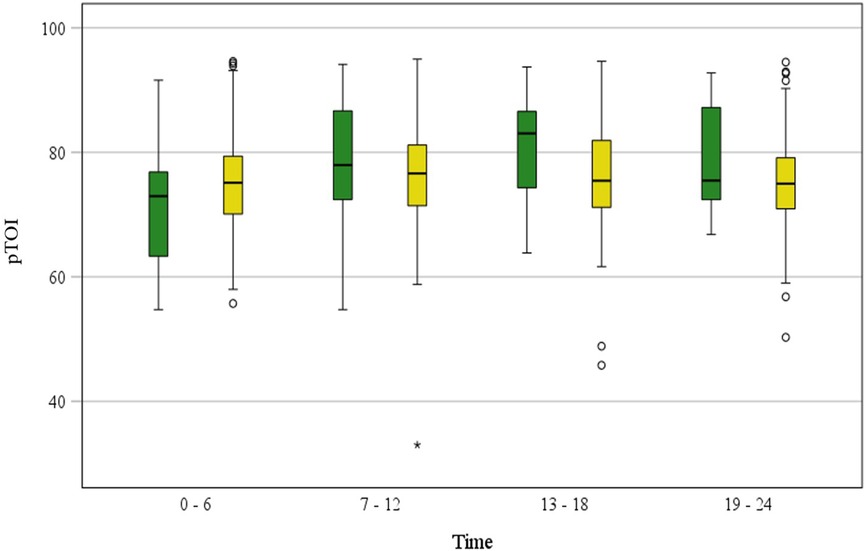
Figure 3. pTOI measured with NIRS in stable term and preterm neonates during the first 24 h after birth, grouped in “6 h time periods” (“0–6 h”, “7–12 h”, “13–18 h”, “19–24 h”). Term neonates are displayed in green blots and preterm neonates in yellow blots. Values are presented as median (IQR).
In HR significant differences between term and preterm neonates (p < 0.001) with higher values in preterm neonates and differences in the course of HR (p = 0.010) between term and preterm neonates could be observed. While in term neonates HR did not change over time, in preterm neonates HR decreased significantly from the first to the second (p < 0.001), to the third (p < 0.001) and to the fourth time period (p = 0.002). Although SpO2 showed no significant change over time (p = 0.309), difference between groups (p = 0.138) and comparable courses of groups (p = 0.260), in post hoc analysis a statistically significant change in SpO2 of preterm neonates comparing the first time period to the fourth time period (p = 0.031) was observed (Table 2).
Discussion
This is the first study describing reference values of pFTOE during the first 24 h after birth in stable term and late preterm neonates. Besides the identification of reference values, we found no changes in pFTOE behaviour over the four defined “6 h time periods”.
The pFTOE value of 0.264 during the first period in stable term neonates is comparable to already published data by Pichler et al. (16). Timing of the measurement, however, was different from ours (mean of 106 h after birth) (16). Furthermore, in the study by Pichler et al. (16), term and moderate-to-late preterm neonates with respiratory and medical support were also included, too. Comparing, however, pFTOE values in the fourth time period of term (0.220) and preterm neonates (0.238) of our present study with the work published by Pichler et al. (16), differences between the two studies can be observed. This observation may be based on the above mentioned differences in gestational age, need for medical/respiratory support and/or the postnatal age at measurement.
Fujioka et al. (17) presented pFTOE data during the first 72 h after birth of 0.25 ± 0.06 in term neonates and of 0.25 ± 0.06 in preterm neonates measured with the time resolved NIRS technique. Although, the measurement period, the utilized NIRS device/technique and the study cohort of neonates with and without need for medical and respiratory support, stated in the study by Fujioka et al., were different from ours, pFTOE values are still comparable. This may be explained by minimal changes of pFTOE after the initial fetal-to-neonatal transition period, with stable pFTOE values in later periods. Furthermore, it may be assumed that in neonates with appropriate medical support, no differences in oxygen supply to and/or consumption of peripheral muscle can be detected.
In contrast to our present pFTOE within the first time period, Bruckner et al. (18) published pFTOE values of median (IQR) 0.08 (0.04–0.15) in term and preterm neonates with a mean gestational age of 34 weeks within the first four to six hours after birth. These values were noticeably lower compared with pFTOE in our study [0.26 (95%CI 0.229–0.300)]. This observed discrepancy may be based on the fact, that peripheral regional oxygen saturation was clearly higher in the study by Bruckner et al. [87% (80–92)] compared to the pTOI in our study (term neonates 71.5% [68.2–74.8]; preterm neonates 74.6% [73.1–76.0]). The differences in peripheral muscle oxygen saturation and consequently in pFTOE between Bruckner et al.’s study (18) and our work may be explained by the different NIRS devices used (INVOS versus NIRO 200/NIRO 200NX), since the INVOS device shows higher tissue oxygen saturation compared to NIRO devices (19, 20). Direct comparisons of these two devices have revealed a difference of up to ten percent, especially with increasing tissue oxygen saturation (20).
Another study presenting pFTOE values was published by Ergenekon et al. (21) with median pFTOE values of 0.34 (0.19–0.47) before exchange transfusion and of 0.36 (0.23–0.48) after exchange transfusion in term neonates with polycythemia within 24 h after birth. Higher values of pFTOE were observed by Ergenekon et al. (21) compared to our results for term neonates. This discrepancy may be explained by different factors. Firstly, polycythemia influences viscosity and leading to a potential influence on oxygen extraction from the tissue. Secondly, Ergenekon et al. (21) performed measurements on the calf, whereby in our present study, measurements were performed on the forearm of the neonate. Thirdly, the interoptode distance used by Ergenekon et al. (21) was 4.0 cm, which is also higher than in our present study with an interoptode distance of 3.0 cm in neonates with a birth weight >1500 g. Fourthly, only 15 neonates were included and analyzed by Ergenekon et al. (21). As the number of included neonates is 16 times higher in our study and quality criteria to increase reproducibility, published by Pichler et al. (12), were taken into account for all measurements, we assume that our data are more representative as normal values.
pFTOE did not show any significant changes when comparing the first “6 h time period” to the following time periods within the first 24 h after birth in our study. In preterm neonates pFTOE remained almost stable during the first three time periods, with a slight increase in pFTOE afterwards. Similarly, Wolfsberger et al. (13) observed changes of pFOE in stable preterm neonates during the first 24 h after birth, comparing the first “6 h time period” to the following ones. They described a decrease of pFOE from the first to the third time period and afterwards a significant increase comparing the first to the fourth time period. However, when comparing pFTOE of our present study [0.229 (0.213–0.246)] during the first “6 h time period” to pFOE (13) [0.35 (0.29–0.40)] at the same time period, higher values were observed for pFOE. Differences between and comparability of pFTOE and pFOE have already been investigated by Hoeller et al. (11), who described the same trend of lower pFTOE values compared to pFOE values within the first few days after birth. This emphasizes that, even though both parameters describe the estimation of oxygen extraction in the tissue, pFTOE and pFOE cannot be used interchangeably. While pFOE reflects the oxygen extraction from the arterial to venous compartment, pFTOE reflects a mixed saturation compartment (venules, arterioles and capillaries).
Possible relevance for pFTOE in clinical practice and therefore the need for reference values have been described in associations between pFTOE and cardiac function (18), partial exchange transfusion (21), ventilator modes (22), and carbon dioxide (CO2) (23).
The potential influence of respiratory support on pFTOE during initial fetal-to-neonatal transition in neonates has already been described (24). After initial fetal-to-neonatal transition period, Ericksen et al. (22) investigated the influence of changes in mode of invasive and non-invasive ventilation at a median of 14.6 days after birth in preterm neonates, without any statistically significance of these changes on pFTOE. Unfortunately, pFTOE values were not provided in the same form as they are in our present study. Nevertheless, pFTOE values displayed in the figure by Ericksen et al. (22), can be compared to our values presented in this work. Besides respiratory support, hematocrit can also influence pFTOE. Therefore, changes of pFTOE in neonates with polycythemia and need for partial exchange transfusion were investigated before and after transfusion (21), showing an increase in cerebral oxygenation and a decrease in pFTOE during the first 24 h after birth in 15 term neonates.
The potential effect of changes in CO2 levels, measured by a transcutaneous probe, on pFTOE has been observed in 13 neonates with a birth weight below 1500 g (23). Twenty-three measurements were performed during the first three days after birth and a significant negative correlation of CO2 and pFTOE, independent of MABP, was observed. In this study, 23 individual pFTOE values were described from each single measurement, including five measurements during the first 24 h after birth. These pFTOE values proved to be comparable to our results of preterm neonates.
Strengths and limitations
The strengths of the study are that we focused on a homogeneous population, i.e., stable neonates without respiratory or cardio-circulatory support, and that the sample size, especially of preterm neonates, was large. The first limitation is that in term neonates the sample size was lower, however being still representative in comparison to previous studies. The second limitation is that less than 40% of the included infants were female, whereby this is below the rate of admitted female neonates (∼48%) to the NICU (25). The third limitation is that pFTOE was not calculated in all of the included term and preterm neonates in each “6 h period” during the first 24 h after birth. Therefore, changes in pFTOE over time should be interpreted with caution.
Conclusion
Reference values of pFTOE during the first 24 h after birth for four “6 h time periods” were defined in this study. Furthermore, pFTOE measured during the first 24 h after birth, showed no statistically significant changes over time during the first 24 h after birth. These normal values of pFTOE are of great need for interpreting pFTOE in scientific context as well as for potential future clinical applications.
Data availability statement
The dataset generated and analysed during the current study are not publicly available due to their containing information that could compromise the privacy of research participants, but are available from the corresponding author on reasonable request.
Ethics statement
The studies involving humans were approved by Regional Committee on Biomedical Research Ethics, Medical University of Graz. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CW: Conceptualization, Investigation, Methodology, Project administration, Writing – original draft, Writing – review and editing. NH: Writing – review and editing. NB: Writing – review and editing. BS: Writing – review and editing. ES: Writing – review and editing. LM: Writing – review and editing. AA: Writing – review and editing. BU: Writing – review and editing. GP: Conceptualization, Methodology, Project administration, Supervision, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
This study was performed as part of a doctoral thesis in the Doctoral School “Sustainable Health Research” at the Medical University of Graz. The authors want to thank Evelyn Ziehenberger for her valuable technical support during performance of study measurements.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Crookes BA, Cohn SM, Bloch S, Amortegui J, Manning R, Li P, et al. Can near-infrared spectroscopy identify the severity of shock in trauma patients? J Trauma. (2005) 58(4):806–13. doi: 10.1097/01.ta.0000158269.68409.1c
2. Ikossi DG, Knudson MM, Morabito DJ, Cohen MJ, Wan JJ, Khaw L, et al. Continuous muscle tissue oxygenation in critically injured patients: a prospective observational study. J Trauma. (2006) 61(4):780–8. doi: 10.1097/01.ta.0000239500.71419.58
3. Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bülow J, Kjaer M. Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand J Med Sci Sports. (2001) 11(4):213–22. doi: 10.1034/j.1600-0838.2001.110404.x
4. Pichler G, Grossauer K, Peichl E, Gaster A, Berghold A, Schwantzer G, et al. Combination of different noninvasive measuring techniques: a new approach to increase accuracy of peripheral near infrared spectroscopy. J Biomed Opt. (2009) 14(1):014014. doi: 10.1117/1.3076193
5. Yoxall CW, Weindling AM. The measurement of peripheral venous oxyhemoglobin saturation in newborn infants by near infrared spectroscopy with venous occlusion. Pediatr Res. (1996) 39(6):1103–6. doi: 10.1203/00006450-199606000-00028
6. Yoxall CW, Weindling AM. Measurement of venous oxyhaemoglobin saturation in the adult human forearm by near infrared spectroscopy with venous occlusion. Med Biol Eng Comput. (1997) 35(4):331–6. doi: 10.1007/BF02534086
7. Naulaers G, Meyns B, Miserez M, Leunens V, Van Huffel S, Casaer P, et al. Use of tissue oxygenation index and fractional tissue oxygen extraction as non-invasive parameters for cerebral oxygenation. A validation study in piglets. Neonatology. (2007) 92(2):120–6. doi: 10.1159/000101063
8. Bruckner M, Mileder LP, Richter A, Baik-Schneditz N, Schwaberger B, Binder-Heschl C, et al. Association between regional tissue oxygenation and body temperature in term and preterm infants born by caesarean section. Children (Basel). (2020) 7(11):205. doi: 10.3390/children7110205
9. Urlesberger B, Brandner A, Pocivalnik M, Koestenberger M, Morris N, Pichler G. A left-to-right shunt via the ductus arteriosus is associated with increased regional cerebral oxygen saturation during neonatal transition. Neonatology. (2013) 103(4):259–63. doi: 10.1159/000346384
10. Urlesberger B, Grossauer K, Pocivalnik M, Avian A, Müller W, Pichler G. Regional oxygen saturation of the brain and peripheral tissue during birth transition of term infants. J Pediatr. (2010) 157(5):740–4. doi: 10.1016/j.jpeds.2010.05.013
11. Hoeller N, Wolfsberger CH, Pfurtscheller D, Binder-Heschl C, Schwaberger B, Urlesberger B, et al. pFOE or pFTOE as an early marker for impaired peripheral microcirculation in neonates. Children (Basel). (2022) 9(6):898. doi: 10.3390/children9060898
12. Pichler G, Wolf M, Roll C, Weindling MA, Greisen G, Wardle SP, et al. Recommendations to increase the validity and comparability of peripheral measurements by near infrared spectroscopy in neonates. ‘round table’, section of haematology, oxygen transport and microcirculation, 48th annual meeting of ESPR, Prague 2007. Neonatology. (2008) 94(4):320–2. doi: 10.1159/000151655
13. Wolfsberger C, Baik-Schneditz N, Schwaberger B, Binder-Heschl C, Nina H, Mileder L, et al. Changes in peripheral muscle oxygenation measured with near-infrared spectroscopy in preterm neonates within the first 24 h after birth. Physiol Meas. (2020) 41(7):075003. doi: 10.1088/1361-6579/ab998b
14. Pichler G, Höller N, Baik-Schneditz N, Schwaberger B, Mileder L, Stadler J, et al. Avoiding arterial hypotension in preterm neonates (AHIP)-a single center randomised controlled study investigating simultaneous near infrared spectroscopy measurements of cerebral and peripheral regional tissue oxygenation and dedicated interventions. Front Pediatr. (2018) 6:15. doi: 10.3389/fped.2018.00015
15. Binder C, Urlesberger B, Riedl R, Morris N, Schwaberger B, Pichler G. Leukocytes influence peripheral tissue oxygenation and perfusion in neonates. Signa Vitae. (2013) 8(2):20–3. doi: 10.22514/SV82.102013.3
16. Pichler G, Pocivalnik M, Riedl R, Pichler-Stachl E, Morris N, Zotter H, et al. ‘Multi-associations’: predisposed to misinterpretation of peripheral tissue oxygenation and circulation in neonates. Physiol Meas. (2011) 32(8):1025–34. doi: 10.1088/0967-3334/32/8/003
17. Fujioka T, Takami T, Ishii H, Kondo A, Sunohara D, Kawashima H. Difference in cerebral and peripheral hemodynamics among term and preterm infants during the first three days of life. Neonatology. (2014) 106(3):181–7. doi: 10.1159/000362152
18. Bruckner M, Binder-Heschl C, Schwaberger B, Mileder LP, Baik-Schneditz N, Koestenberger M, et al. Cerebral and peripheral tissue oxygenation in stable neonates: absent influence of cardiac function. Acta Paediatr. (2020) 109(8):1560–9. doi: 10.1111/apa.15172
19. Schneider A, Minnich B, Hofstätter E, Weisser C, Hattinger-Jürgenssen E, Wald M. Comparison of four near-infrared spectroscopy devices shows that they are only suitable for monitoring cerebral oxygenation trends in preterm infants. Acta Paediatr. (2014) 103(9):934–8. doi: 10.1111/apa.12698
20. Kleiser S, Ostojic D, Andresen B, Nasseri N, Isler H, Scholkmann F, et al. Comparison of tissue oximeters on a liquid phantom with adjustable optical properties: an extension. Biomed Opt Express. (2017) 9(1):86–101. doi: 10.1364/BOE.9.000086
21. Ergenekon E, Hirfanoglu IM, Turan O, Beken S, Gucuyener K, Atalay Y. Partial exchange transfusion results in increased cerebral oxygenation and faster peripheral microcirculation in newborns with polycythemia. Acta Paediatr. (2011) 100(11):1432–6. doi: 10.1111/j.1651-2227.2011.02358.x
22. Ericksen K, Alpan G, La Gamma EF. Effect of ventilator modes on neonatal cerebral and peripheral oxygenation using near-infrared spectroscopy. Acta Paediatr. (2021) 110(4):1151–6. doi: 10.1111/apa.15600
23. Vanderhaegen J, Naulaers G, Vanhole C, De Smet D, Van Huffel S, Vanhaesebrouck S, et al. The effect of changes in tPCO2 on the fractional tissue oxygen extraction–as measured by near-infrared spectroscopy–in neonates during the first days of life. Eur J Paediatr Neurol. (2009) 13(2):128–34. doi: 10.1016/j.ejpn.2008.02.012
24. Schwaberger B, Pichler G, Binder C, Avian A, Pocivalnik M, Urlesberger B. Even mild respiratory distress alters tissue oxygenation significantly in preterm infants during neonatal transition. Physiol Meas. (2014) 35(10):2085–99. doi: 10.1088/0967-3334/35/10/2085
Keywords: pFTOE, neonate, muscle oxygenation, reference values, near-infrared spectroscopy
Citation: Wolfsberger CH, Höller N, Baik-Schneditz N, Schwaberger B, Suppan E, Mileder L, Avian A, Urlesberger B and Pichler G (2023) Peripheral muscle fractional tissue oxygen extraction in stable term and preterm neonates during the first 24 h after birth. Front. Pediatr. 11:1276769. doi: 10.3389/fped.2023.1276769
Received: 13 August 2023; Accepted: 1 November 2023;
Published: 15 November 2023.
Edited by:
Burkhard Simma, Landeskrankenhaus Feldkirch, AustriaReviewed by:
Subhabrata Mitra, University College London, United KingdomPeter Krcho, Louis Pasteur University Hospital Košice, Slovakia
© 2023 Wolfsberger, Höller, Baik-Schneditz, Schwaberger, Suppan, Mileder, Avian, Urlesberger and Pichler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina H. Wolfsberger Y2hyaXN0aW5hLndvbGZzYmVyZ2VyQG1lZHVuaWdyYXouYXQ=