 Marie Aline Charles1,2*
Marie Aline Charles1,2* Pierre-Yves Ancel2Thierry Simeon1
Pierre-Yves Ancel2Thierry Simeon1 Laetitia Marchand-Martin2Cécile Zaros1Marie-Noelle Dufourg1Valérie Benhamou2Hélène Blanché3Jean-François Deleuze3Delphine Rahib4Nathalie Lydie4Xavier de Lamballerie5Fabrice Carrat6,7
Laetitia Marchand-Martin2Cécile Zaros1Marie-Noelle Dufourg1Valérie Benhamou2Hélène Blanché3Jean-François Deleuze3Delphine Rahib4Nathalie Lydie4Xavier de Lamballerie5Fabrice Carrat6,7
- 1UMS Elfe, Ined, Inserm, EFS, Aubervilliers, France
- 2Center for Research in Epidemiology and Statistics, Paris Cité University, INSERM, INRAE, Paris, France
- 3Fondation Jean Dausset-Centre d’Etude du Polymorphisme Humain, CEPH-Biobank, Paris, France
- 4Health Prevention and Promotion Department, Santé Publique France, Saint-Maurice, France
- 5Unité des Virus Emergents, Aix Marseille University, IRD, INSERM, IHU Méditerranée Infection, Marseille, France
- 6Institut Pierre-Louis d'Epidémiologie et de Santé Publique, Sorbonne Université, Inserm, Paris, France
- 7Département de Santé Publique, Hôpital Saint-Antoine, APHP, Paris, France
Introduction: Children have been significantly less affected by COVID-19 than adults and presented with milder and less symptomatic forms of the disease. However, there has been suggestion that children older than 10 years and adolescents exhibits features closer to that of young adults. Most studies combine children in different age-groups and lack sufficient numbers to explore in detail age specificities. We report data on a population-based sample of 2,555 children at the pivotal age of 9 years.
Methods: In April 2020, the participants in two French nationwide cohorts of children, Elfe and Epipage2, were invited to take part into an online survey about Covid related symptoms and family life during the lockdown. A second questionnaire was sent on May 5. This questionnaire also proposed to the child included in the cohort and to one of his/her parents to take part into a capillary blood collection for Covid serology. Families who agreed to the serological survey were sent kits for dried blood spots self-sampling (DBS) with instructions. Samples were processed with a commercial Elisa test (Euroimmun®, Lübeck, Germany) to detect anti-SARS-CoV-2 antibodies (IgG) directed against the S1 domain of the spike protein of the virus.
Results: Children's acceptance rate for the serological survey was around 60%. 2,555 serological results were analyzed. The weighted prevalence of a positive Elisa Spike serology was 2.8% in 9 yr-old children (95% CI: 1.7%–4.0%). Positive serology was found in 8.6% (7.4%–9.7%) of parents who provided blood. There was a significant association (p < 0.001) between serology of the child and parent from the same household with an odds ratio of 13.8 (7.9–24.2).
Discussion: We have shown that 9-yr old children had a lower susceptibility to SARS-Cov2 infection than adults with the initial Chinese strain, similar to younger children and estimated that around 3% of them have developed antibodies against SARS-Cov2 in France after the first wave of the Covid-19 epidemics.
Introduction
At the beginning of the COVID-19 epidemic, initial data from China indicated that children were significantly less affected by COVID-19 than adults and more frequently presented with mild and asymptomatic forms of the disease than adults (1). This has been later confirmed by many other publications and by seroprevalence studies from different parts of the world (2, 3). However, there has been a suggestion that children older than 10 years and adolescents exhibit features closer to that of young adults (2). In the USA, the weekly incidence of COVID-19 cases among adolescents aged 12–17 years was approximately twice compared with that of children aged 5–11 years between March and September 2020 (4). Evidence demonstrated that the SARS-CoV-2 viral-specific antibody response profiles vary with age and differ between younger children, adolescents, and young adults (5).
Most studies combine children in different age groups and lack sufficient numbers to explore them in detail age specificities. Here, we report data on a population-based sample of 2,555 children at the pivotal age of 9 years to gain more insight into the transition between younger and older child-type responses to SARS-CoV-2 infection.
The data originated from the child cohorts of the SAPRIS (“SAnté, Perception, pratiques, Relations et Inégalités Sociales en population générale pendant la crise COVID-19”) project, a consortium of prospective French cohort studies involving three general population-based adult cohorts, aside from the two child cohorts (6). The goal of the present analysis is to describe (1) the symptoms compatible with a SARS-CoV-2 infection in the two involved cohorts of children born in 2011 during or right after the first lockdown in France (from 17 March 2020 to 11 May 2020) and (2) the prevalence of SARS-CoV-2 ELISA Spike seropositivity in children and one of their parents.
Population
In April 2020, the participants in two French nationwide cohorts of children, namely, Elfe and Epipage2, were invited to take part in an online survey about COVID-19-related symptoms and family life during the lockdown.
Both cohorts had enrolled children at birth in 2011. Children born at term, moderate preterm, or late preterm (after 33 weeks of gestation) were participants in the Elfe cohort and enrolled on 25 selected days over 2011, from a random sample of 320 maternity units in mainland France (7). Children born extremely preterm (below 35 weeks) were participants in the Epipage2 cohort. All maternity units in French mainland regions (but one) and in overseas regions were involved in the Epipage2 inclusion phase over periods that lasted from 5 weeks to 8 months according to three gestational age strata (8).
All families who had not withdrawn from the cohorts and had an email address known by the management teams were eligible for the COVID-19 survey.
Elfe children born before 35 weeks of gestation were excluded from the present analyses as these preterm children are best represented by the Epipage2 cohort.
Methods
Data collection
The first online questionnaire was sent on 16 April 2020 and remained accessible until May 4.
For the index child, symptoms compatible with a COVID-19 infection (see list in Table 1) were reported if they had been present at least once in the last 14 days. If a symptom had been, but was no longer present when the questionnaire was completed, the duration was noted on a scale (less than 1, 1–3, 4–7, 8–14, >14 days). Finally, a question enquired about the total time (in days) between the onset of the first symptoms and the date of the questionnaire filling, but too many missing data for correct exploitation were noted. For other members of the household, only cough and/or fever in the last 14 days were reported. Additional questions included the socioeconomic and employment status of the parents, dwelling type and household composition, recurse to care for the child, preventive measures against COVID-19, familial relationship, school, and leisure-related activities of the child during the lockdown (9).
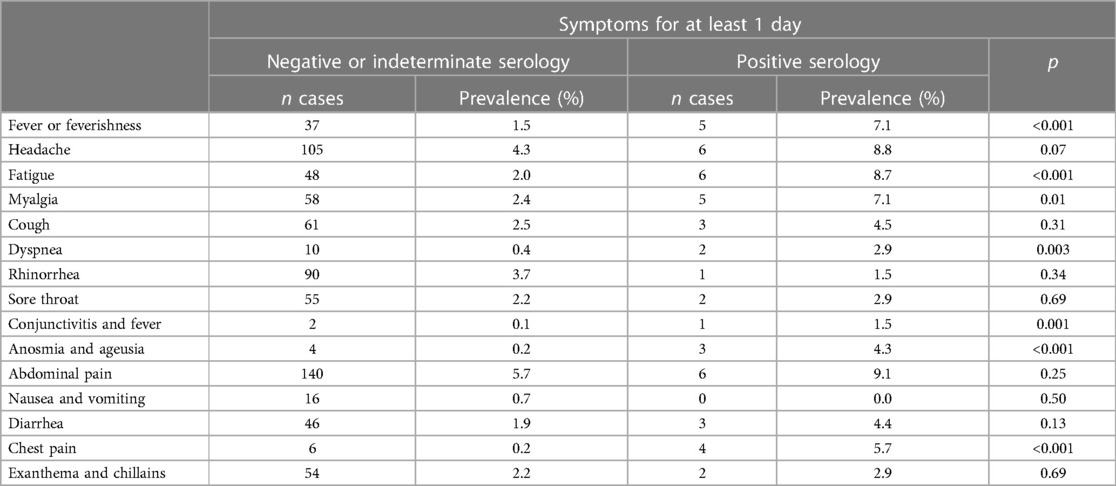
Table 1. Prevalence of clinical symptoms lasting at least 1 day during the lockdown according to ELISA Spike serology.
The second questionnaire was sent on May 5 and remained available until June 29. It included the same questions as the first questionnaire and additional questions on family life and mental health. This questionnaire also proposed to the child included in the cohort and to one of his/her parents to take part in a capillary blood collection for COVID-19 serology.
Serological tests
Families who agreed to the serological survey were sent kits with instructions for the self-sampling of dried blood spots (DBS). The cards for the parent and the child were pre-labeled. The participants added their first names and the date of sampling on the card. Before the sampling, they had to fill out an online consent and a short questionnaire about COVID-19-related symptoms in the three previous weeks and about positive PCR test(s) since the completion of the second online survey questionnaire.
After sampling, the DBS were sent in a padded pre-stamped and pre-addressed envelope to a Central Biobank (CEPH Biobank, Paris, France). On receipt, after a visual assessment of the blood spots and registration, four discs of 4.7 mm for adults and one to four discs for children were punched from the spots on a Panthera™ (PerkinElmer) and stored in 2D FluidX 96-Format 0.5 ml tubes (Brooks) at room temperature. They were sent to the virology laboratory (Unité des Virus Émergents, Marseille, France) for serological analyses.
Samples were processed with a commercial ELISA test (Euroimmun®, Lübeck, Germany) to detect anti-SARS-CoV-2 antibodies (IgG) directed against the S1 domain of the spike protein of the virus (ELISA S). The volume of eluate used corresponded to the amount of serum and dilution recommended by the manufacturer. According to the recommendation of the manufacturer, a test with an optical density ratio of ≥1.1 is ELISA-positive; if it is between 0.8 and 1.1, it is ELISA-indeterminate; and if it is <0.8, it is ELISA-negative.
Due to the low availability of serological tests at this time, kits were sent only to families living in three regions of France, from May 15 to July 6: the two regions with the highest reported cumulated rates of COVID-19, namely, Grand Est (GE) and Ile-de-France (IDF), and a region with a low reported rate, Nouvelle Aquitaine (NA) (French Public Health Agency, COVID-19 Epidemiologic Situation, 14 May 2020). From July 7, all other families who had volunteered were sent a kit. Most of the sampling were completed in the last 2 weeks of May (27%) and the first 3 weeks of July (44%), but the last kits received dated from early November.
Ethical approval
The SAPRIS survey was approved by the Inserm Ethics Committee (approval #20–672 dated 30 March 2020). The SAPRIS-SERO study was approved by the Sud-Mediterranée III ethics committee (approval #20.04.22.74247). A specific information letter was addressed to the child in addition to the letter to the parents. Electronic consents were given by the parents for themselves and their child.
Statistical analysis
The prevalence of SARS-CoV-2 ELISA Spike seropositivity was weighted to take into account the initial sampling plan, enrollment rate in the two cohorts, and response rate to the current survey. The weights for the two cohorts were combined to represent the target population of children born in 2011 in mainland France (Supplementary Material S1).
According to the European Centre for Disease Prevention and Control, a possible COVID-19 was defined as at least one of the following symptoms: fever, cough, dyspnea, a sudden onset of anosmia, ageusia, or dysgeusia (10). As symptoms are milder in children than those in adults, they were significantly considered as soon as they lasted for at least 1 day.
The weighted seroprevalence is presented in the total sample and according to a four-category region variable (IDF, GE, NA, and other regions).
The association between the serologies of the parent and the child was tested using the chi-square test. The odds ratio has been computed to quantify the strength of the association. The associations between the child serology and clinical symptoms were also tested using the chi-square test.
Results
Eligible participants for the COVID-19 survey were 12,814 and 2,922 in the Elfe and Epipage2 cohorts, respectively. Among them, 3,894 (30%) and 841 (29%), respectively, responded to the second survey questionnaire and were proposed to participate in the serological survey. The acceptance rate of children for the serological survey was approximately 60% (n = 2,358 and 498, respectively), which was similar for the two cohorts. A total of 2,828 DBS from children were received at the Biobank. Among them, 2,680 (95%) could be punched and were sent for analysis, and 2,642 serological results were returned. After the exclusion of the missing values of the sampling date and children that could not be included in the weighing procedure, data collected from 2,555 children were included in the statistical analysis. Among 2,400, one parent had also provided a DBS that could be analyzed.
The crude and weighted characteristics of the children are presented in Table 2. The crude prevalence of a positive ELISA Spike serology was not statistically different in the preterm children of the Epipage2 cohort (2.4%) and the term children of the Elfe cohort (1.7%, p = 0.40); therefore, results were given for the pooled sample.
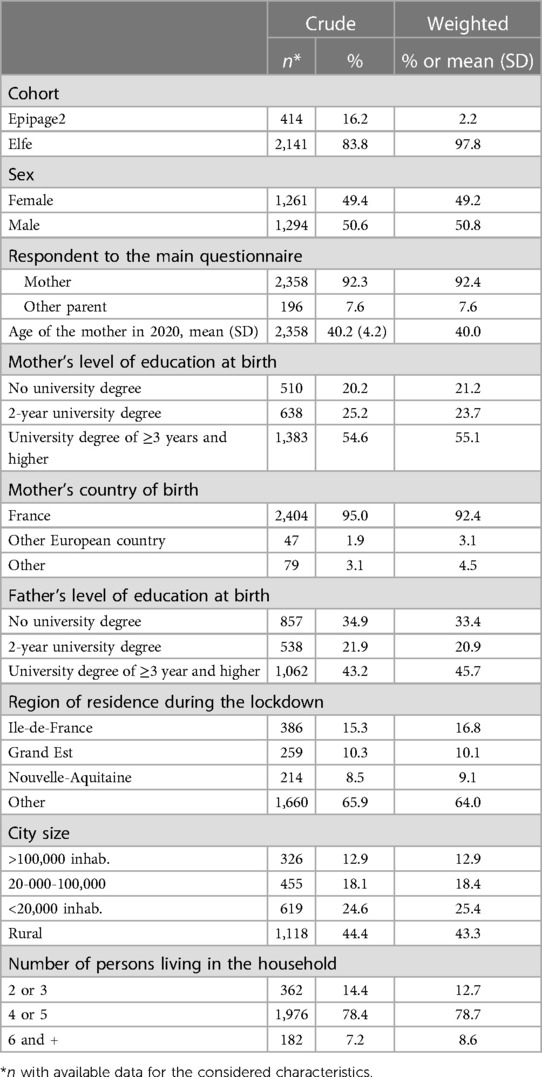
Table 2. Characteristics of the participant child.
The weighted prevalence of a positive ELISA Spike serology was 2.8% in 9-year-old children (95% CI: 1.7%–4.0%). It showed the expected gradient according to the regional viral contamination rates before the lockdown, ranging from 6.9% (2.4%–11.4%) in Grand Est to 0.1% (0.0%–0.3%) in Nouvelle Aquitaine (Table 3). In the whole sample, a positive serology was found in 8.6% (7.4%–9.7%) of parents who provided blood (the mother in 76% and the father in 24% of cases), which was more than three times higher than that in their children.
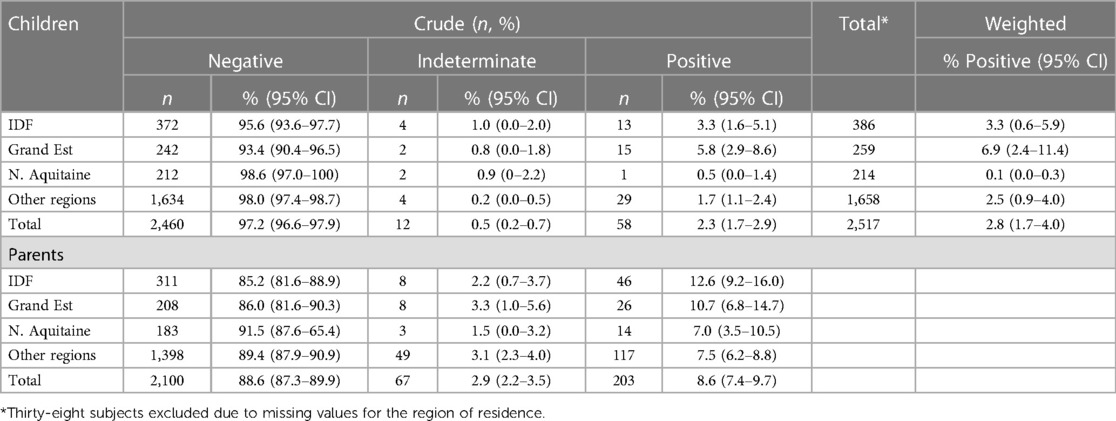
Table 3. Crude and weighted ELISA Spike serology according to region of residence.
Table 4 shows a significant association (p < 0.001) between the serologies of the child and the parent from the same household with an odds ratio of 13.8 (7.9–24.2).
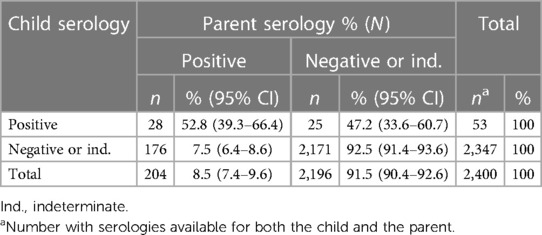
Table 4. Association between ELISA Spike serologies of a 9-year-old child and a parent from the same household.
The clinical symptoms of the “possible COVID-19” definition that lasted for at least 1 day had been more frequently declared (13.4%) during the lockdown when ELISA Spike serology was positive than when it was negative or indeterminate (3.8%, p = 0.02).
Among the symptoms proposed in the questionnaire, those that lasted for at least 1 day and had been significantly more frequently declared in case of positive serology were anosmia/ageusia, fever, fatigue, dyspnea, and chest pain (Table 1).
Of the children with positive serology, 74% (43/58) (CI: 63%–86%) reported no symptoms in the past 14 days (i.e., during the lockdown), and of them, 71% (CI: 58%–83%) reported no fever nor cough earlier in the year.
Discussion
From this sample and according to ELISA Spike serology, it is estimated that 2.8% (95% CI: 1.7–4.0) of 9-year-old children born in France in 2011 had produced antibodies against the SARS-CoV-2 spike protein before the summer of 2020 in France, which is three times less than that of the parents living in the same household. In the presence of one infected parent in the household, only 14% of children had a positive serology.
In France, schools closed from 16 March 2020 to June, except for children of first-line workers. Reopening took place on 22 June 2020 for the whole country but started on May 11 in districts with low SARS-CoV-2 circulation. After the first lockdown, the incidence rate of COVID-19 as assessed by positive PCR tests in the 7 previous days decreased to below 5/100,000 inhab (11), before rising again at the end of the summer. We can assume that in our study a majority of the children and their parents with positive SARS-CoV-2 serology had been contaminated before or during the first weeks of the lockdown as most DBS were performed before the end of July.
Serological data on children after the first COVID-19 wave are scarce in France, and none has a national scope. To the best of our knowledge, only two are population-based. The first study was performed in the city north of Paris where the first COVID-19 outbreak in schools was recognized in France at the beginning of the epidemic. A serological survey performed in schools in the Haut de France region in March–April 2020 before any protection measure was taken found that 35% of 664 children aged 12–17 years who participated in the study were seropositive in high school where the outbreak occurred and only 9% of 1,340 children in primary schools of the city (12).
The second study was undertaken in the city of Nancy in a random sample of households drawn from the electoral list. It yielded a SARS-CoV-2 seropositivity prevalence of 1% (95% CI: 0.1–3.5) in 5–19-year-old children (n 203) in June 2020 (13). Two other studies were performed in clinical settings. In a study based on the serum samples collected from children requiring hospital admission in North Eastern France for other causes than COVID-19 between February and August 2020, seropositivity was estimated at 4.0% in 1,400 children aged ≤19 years (14). In the Ile-de-France region, 27 ambulatory pediatric practices participated in a fingerstick serological survey in April–May 2020. Data were collected from 605 children at a mean age of 5 years, of whom 204 were asymptomatic, 118 had COVID-19-compatible symptoms between 7 days and 2 months before enrollment, and 283 were symptomatic. SARS-CoV-2 seropositivity was 6.4% (95% CI: 3.4–10.7), 23.7% (16.4–32.7), and 8.5% (5.5–12.5), respectively (15). Although all these studies used different methods for SARS-CoV-2 serology, they are coherent with our regional estimates in 9-year-old children that rank from 0.1% to 6.9% in the general population depending on the intensity of SARS-CoV-2 circulation.
A number of studies have found that the seroprevalence rate is lower in children and, for some studies, in adolescents than that in adults (2). We confirmed this result in 9-year-old children and adults sharing the same household. In a household transmission survey in Geneva (16), compared with 20–49-year olds, 5–9-year olds had less than half the odds ratio of seropositivity in the presence of a positive household member, which confirms their low susceptibility to SARS-CoV-2 infections. On the other hand, in our study, parental seropositivity was seven times higher (53%) when their child was seropositive compared with negative or indeterminate. A similar finding was found in the Haut de France survey for primary school pupils in contrast to high school pupils (12). Closer contacts between young children and their parents than between adolescents and their parents has been hypothesized to explain this finding, and, in that matter, 9-year-olds seem to behave as younger children. Although we cannot determine who was the index case in the household, it was more likely the parent or another adult member of the household, given the differences in the infection rates between children and adults. This suggests that close contacts with an infected adult explained a substantial proportion of infections with the initial SARS-CoV-2 variant in 9-year-old children and therefore the high frequency of infected adults in their surroundings.
However, children have a more robust innate and/or mucosal immune response to SARS-CoV-2 than adults, which translates into the absence of adaptive immune solicitation and antibody production. The difference in seroconversion between children and adults may also be due in part to a difference in cellular immune responses (T and B cells) (17). Therefore, the absence of ELISA Spike seropositivity may not always indicate an absence of infection. In addition, our estimates are based only on ELISA Spike seropositivity, which does not have 100% specificity and sensibility, which may induce some misclassification.
The clinical symptoms associated with seropositivity in our study are in accordance with those described in other studies in children (3, 12, 18, 19) except for gastro-intestinal symptoms that were not statistically different between seropositive children and the others, although in the expected direction. Most seropositive children reported no symptoms in the first 2 weeks of the lockdown or earlier in the year. In contrast to the SAPRIS study performed in adult cohorts, only 19% of seropositive adults reported no symptoms (20), pointing again to the difference in the immune response between 9-year-old children and adults.
To conclude, we have shown that 9-year-old children had a lower susceptibility to SARS-CoV-2 infection than adults with the initial Chinese strain, similar to younger children, and estimated that approximately 3% of them have developed antibodies against SARS-CoV-2 in France after the first wave of the COVID-19 epidemics.
Data availability statement
Personal data of children from the ELFE and EPIPAGE2 cohorts cannot be made publicly available for ethical reasons. They are available upon reasonable request from the authors under data-security conditions.
Ethics statement
This study involving humans was approved by the Ethics Committee of Sud-Mediterran III. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
MC: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – original draft. PA: Conceptualization, Funding acquisition, Writing – review & editing. TS: Data curation, Formal analysis, Methodology, Writing – review & editing. LM: Data curation, Formal analysis, Methodology, Writing – review & editing. CZ: Investigation, Writing – review & editing. MD: Investigation, Writing – review & editing. VB: Investigation, Writing – review & editing. HB: Investigation, Writing – review & editing. JD: Investigation, Writing – review & editing. DR: Investigation, Writing – review & editing. NL: Investigation, Writing – review & editing. XdL: Formal analysis, Methodology, Writing – review & editing. FC: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by the ANR (Agence Nationale de la Recherche ANR-20-COVI-000), Fondation pour la Recherche Médicale 20RR052-00, and Inserm (Institut National de la Santé et de la Recherche Médicale C20-26) and Elfe and Epipage2 cohorts were funded by the ANR “Investissements d'avenir” programs (ANR-11-EQPX-0038, ANR-19-COHO-0001).
Acknowledgments
The authors warmly thank the parents and children from the Elfe and Epipage2 cohorts who participated in this COVID-19 survey and all the members of the Elfe and Epipage2 coordination teams who actively contributed in a short time to the data collection during the first COVID-19 wave. The authors acknowledge the contribution of SAPRIS-SERO study group for the initiation and collaboration in studying COVID-19 in French cohorts, namely, Fabrice Carrat, Pierre-Yves Ancel, Marie-Aline Charles, Gianluca Severi, Mathilde Touvier, and Marie Zins (SAPRIS-SERO investigators); Nathalie Bajos, Fabrice Carrat, Pierre-Yves Ancel, Marie-Aline Charles, Florence Jusot, Claude Martin, Laurence Meyer, Ariane Pailhé, Alexandra Rouquette, Gianluca Severi, Alexis Spire, Mathilde Touvier, and Marie Zins (SAPRIS questionnaires); Sofiane Kab, Adeline Renuy, Stephane Le-Got, Celine Ribet, Emmanuel Wiernik, Marcel Goldberg, Mireille Pellicer, and Marie Zins (Constances cohort); Fanny Artaud, Pascale Gerbouin-Rérolle, Mélody Enguix, Camille Laplanche, Roselyn Gomes-Rima, Lyan Hoang, Emmanuelle Correia, Alpha Amadou Barry, Nadège Senina, and Gianluca Severi (E3N-E4N cohort); Julien Allegre, Fabien Szabo de Edelenyi, Nathalie Druesne-Pecollo, Younes Esseddik, Serge Hercberg, Mélanie Deschasaux, and Mathilde Touvier (NutriNet-Santé cohort); Marie-Aline Charles, Pierre-Yves Ancel, Valérie Benhammou, Anass Ritmi, Laetitia Marchand, Cecile Zaros, Elodie Lordmi, Adriana Candea, Sophie de Visme, Thierry Simeon, Xavier Thierry, Bertrand Geay, Marie-Noelle Dufourg, and Karen Milcent (Epipage2 and Elfe child cohorts); Delphine Rahib and Nathalie Lydie (Santé Publique France); Clovis Lusivika-Nzinga, Gregory Pannetier, Nathanael Lapidus, Isabelle Goderel, Céline Dorival, Jérôme Nicol, Olivier Robineau, and Fabrice Carrat (IPLESP – methodology and coordinating data center); Cindy Lai, Liza Belhadji, Hélène Esperou, and Sandrine Couffin-Cadiergues (Inserm); Jean-Marie Gagliolo (Institut de Santé Publique); Hélène Blanché, Jean-Marc Sebaoun, Jean-Christophe Beaudoin, Laetitia Gressin, Valérie Morel, Ouissam Ouili, and Jean-François Deleuze (CEPH-Biobank); and Laetitia Ninove, Stéphane Priet, Paola Mariela Saba Villarroel, Toscane Fourié, Souand Mohamed Ali, Abdenour Amroun, Morgan Seston, Nazli Ayhan, Boris Pastorino, and Xavier de Lamballerie (Unité des Virus Emergents).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles 10.3389/fped.2023.1274113/full#supplementary-material
References
1. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiology of COVID-19 among children in China. Pediatrics. (2020) 145(6):e20200702. doi: 10.1542/peds.2020-0702
2. Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. (2021) 175(2):143–56. doi: 10.1001/jamapediatrics.2020.4573
3. Waterfield T, Watson C, Moore R, Ferris K, Tonry C, Watt A, et al. Seroprevalence of SARS-CoV-2 antibodies in children: a prospective multicentre cohort study. Arch Dis Child. (2021) 106(7):680–6. doi: 10.1136/archdischild-2020-320558
4. Leeb R, Price S, Sliwa S, Kimball A, Szucs L, Caruso E, et al. COVID-19 trends among school-aged children—United States, 1 March–19 September 2020. MMWR Morb Mortal Wkly Rep. (2020) 69(39):1410–5. doi: 10.15585/mmwr.mm6939e2
5. Yang HS, Costa V, Racine-Brzostek SE, Acker KP, Yee J, Chen Z, et al. Association of age with SARS-CoV-2 antibody response. JAMA Netw Open. (2021) 4(3):e214302. doi: 10.1001/jamanetworkopen.2021.4302
6. Carrat F, Touvier M, Severi G, Meyer L, Jusot F, Lapidus N, et al. Incidence and risk factors of COVID-19-like symptoms in the French general population during the lockdown period: a multi-cohort study. BMC Infect Dis. (2021) 21(1):169. doi: 10.1186/s12879-021-05864-8
7. Charles MA, Thierry X, Lanoe JL, Bois C, Dufourg MN, Popa R, et al. Cohort profile: the French national cohort of children (ELFE)—birth to 5 years. Int J Epidemiol. (2020) 49(2):368–9j. doi: 10.1093/ije/dyz227
8. Lorthe E, Benhammou V, Marchand-Martin L, Pierrat V, Lebeaux C, Durox M, et al. Cohort profile: the etude epidemiologique sur les petits ages gestationnels-2 (EPIPAGE-2) preterm birth cohort. Int J Epidemiol. (2021) 50(5):1428–9. doi: 10.1093/ije/dyaa282
9. Pailhé A, Panico L, Solaz A. Children’s well-being and intra-household family relationships during the first COVID-19 lockdown in France. J Famliy Research. (2021) 34(1):249–80. doi: 10.20377/jfr-718
10. European Center for Diseases Control. Case definition for coronavirus disease 2019 (COVID-19), as of 29 May 2020, Available at: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (Accessed June 15, 2020).
11. Santé publique France. Available at: https://geodes.santepubliquefrance.fr/#c=indicator&i=sp_ti_tp_7j.tx_pe_gliss&s=2021-10-24-2021-10-30&t=a01&view=map2. (Accessed June 15, 2020)
12. Fontanet A, Tondeur L, Grant R, Temmam S, Madec Y, Bigot T, et al. SARS-CoV-2 infection in schools in a northern French city: a retrospective serological cohort study in an area of high transmission, France, January to April 2020. Euro Surveill. (2021) 26(15):2001695. doi: 10.2807/1560-7917
13. Gegout Petit A, Jeulin H, Legrand K, Jay N, Bochnakian A, Vallois P, et al. Seroprevalence of SARS-CoV-2, symptom profiles and sero-neutralization in a suburban area, France. Viruses. (2021) 13(6):1076. doi: 10.3390/v13061076
14. Woudenberg T, Pelleau S, Anna F, Attia M, Donnadieu F, Gravet A, et al. Humoral immunity to SARS-CoV-2 and seasonal coronaviruses in children and adults in north-eastern France. EBioMedicine. (2021) 70:103495. doi: 10.1016/j.ebiom.2021.103495
15. Cohen R, Jung C, Ouldali N, Sellam A, Batard C, Cahn-Sellem F, et al. Assessment of SARS-CoV-2 infection by reverse transcription-PCR and serology in the Paris area: a cross-sectional study. BMJ Paediatr Open. (2020) 4(1):e000887. doi: 10.1136/bmjpo-2020-000887
16. Bi Q, Lessler J, Eckerle I, Lauer SA, Kaiser L, Vuilleumier N, et al. Insights into household transmission of SARS-CoV-2 from a population-based serological survey. Nat Commun. (2021) 12(1):3643. doi: 10.1038/s41467-021-23733-5
17. Toh ZQ, Anderson J, Mazarakis N, Neeland M, Higgins RA, Rautenbacher K, et al. Comparison of seroconversion in children and adults with mild COVID-19. JAMA Netw Open. (2022) 5(3):e221313. doi: 10.1001/jamanetworkopen.2022.1313
18. Tonshoff B, Muller B, Elling R, Renk H, Meissner P, Hengel H, et al. Prevalence of SARS-CoV-2 infection in children and their parents in southwest Germany. JAMA Pediatr. (2021) 175(6):586–93. doi: 10.1001/jamapediatrics.2021.0001
19. Blankenberger J, Haile SR, Puhan MA, Berger C, Radtke T, Kriemler S, et al. Prediction of past SARS-CoV-2 infections: a prospective cohort study among Swiss schoolchildren. Front Pediatr. (2021) 9:710785. doi: 10.3389/fped.2021.710785
20. Carrat F, de Lamballerie X, Rahib D, Blanche H, Lapidus N, Artaud F, et al. Antibody status and cumulative incidence of SARS-CoV-2 infection among adults in three regions of France following the first lockdown and associated risk factors: a multicohort study. Int J Epidemiol. (2021) 50(5):1458–72. doi: 10.1093/ije/dyab110
Keywords: COVID-19, serology, children, France, household
Citation: Charles MA, Ancel P-Y, Simeon T, Marchand-Martin L, Zaros C, Dufourg M-N, Benhamou V, Blanché H, Deleuze J-F, Rahib D, Lydie N, de Lamballerie X and Carrat F (2023) SARS-CoV-2 seroprevalence in French 9-year-old children and their parents after the first lockdown in 2020. Front. Pediatr. 11:1274113. doi: 10.3389/fped.2023.1274113
Received: 7 August 2023; Accepted: 2 October 2023;
Published: 25 October 2023.
Edited by:
Maurizio Aricò, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, ItalyReviewed by:
Desiree Caselli, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, ItalyAssathiany Rémy, Private Practitioner, France
© 2023 Charles, Ancel, Simeon, Marchand-Martin, Zaros, Dufourg, Benhammou, Blanché, Deleuze, Rahib, Lydie, de Lamballerie and Carrat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Aline Charles bWFyaWUtYWxpbmUuY2hhcmxlc0BpbnNlcm0uZnI=