 Ya-Ju Ju
Ya-Ju Ju Yi-Chun Du
Yi-Chun Du Hsien-Chun Huang4
Hsien-Chun Huang4 Rong-Ju Cherng
Rong-Ju Cherng- 1Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan
- 2Department of Biomedical Engineering, College of Engineering, National Cheng Kung University, Tainan, Taiwan
- 3Medical Device Innovation Center, National Cheng Kung University, Tainan, Taiwan
- 4Department of Product Engineering Division, Voltafield Technology Corporation, Hsinchu, Taiwan
- 5Department of Physical Medicine and Rehabilitation, Landseed International Hospital, Taoyuan, Taiwan
- 6Department of Physical Therapy, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Introduction: Developmental coordination disorder (DCD) is a neurodevelopmental disorder characterized by motor skill deficits. Such deficits often limit children's participation in physical activities, further affecting their overall health, including through reduced cardiopulmonary fitness. Because virtual reality (VR) devices offer interactive games and activities that require various movements and coordination, they can serve as motivating and enjoyable means for children to perform physical exercise. In this study, we developed a VR-based exergaming system and tested its ability to enhance the cardiopulmonary fitness of children with DCD.
Materials and methods: A total of 13 children with DCD and 10 young adults were recruited in phase I to examine the test–retest reliability and concurrent validity of our system (including a custom-made heart rate monitor) with a commercial heart rate device. In phase II, we included an additional 13 children with DCD to test the feasibility of the system. We tested the outcomes using the enjoyment rating scale, intrinsic motivation inventory (IMI), and 20-m shuttle run test (20mSRT).
Results: In phase I, test–retest reliability was good to excellent in the static task and moderate to good in the dynamic task. Concurrent validity was excellent in both tasks. In phase II, more than half of the children (18 out of 26) assigned the maximum rating for their enjoyment of the game; they also had high average scores on the IMI. Furthermore, after the 8-week training using the VR program, the average running distance of the 26 children in the 20mSRT had increased significantly from 129.23 m to 176.92 m (p < 0.001).
Conclusion: Our VR-based exergaming program can serve as an alternative intervention for enhancing cardiopulmonary fitness in children with DCD.
1. Introduction
Developmental coordination disorder (DCD) is a neurodevelopmental disorder characterized by motor skill deficits. These deficits experienced by individuals with DCD often limit their performance of and participation in physical activities, further harming their overall health through, for example, reduced cardiopulmonary fitness. A systematic review indicated that the oxygen consumption at peak physical exertion (⩒O2max) of typical children and adolescents aged 8–19 years is 35–47 ml/kg/min during cardiopulmonary endurance exercise (1). However, the ⩒O2max in children with DCD is much lower, only 33.5–34.4 ml/kg/min on average (2). In addition, a longitudinal study revealed that the difference in cardiopulmonary endurance between children with DCD and typical children increased with age (3).
The American College of Sports Medicine indicates that cardiopulmonary fitness is promoted by aerobic exercise, especially exercise that increases the heart rate to 65%–75% of its maximum. Aerobic exercise can improve cardiopulmonary fitness, muscle power, body composition, cognition, and inhibitory control (4–8). Lau et al. also demonstrated that aerobic exercise and moderate-to-vigorous physical activity from 19.2 to 29.33 ml/kg/min could improve cardiopulmonary fitness through increased ⩒O2max (9). Although studies have demonstrated the benefits of traditional aerobic exercise, children often regard this exercise as boring or difficult.
In virtual reality (VR), multimedia technology and an interface between the human body and a computer enable people to experience a virtual environment and the objects in it as they do in the real world. Because VR offers interactive games and activities requiring various movements and coordination, it represents a motivating and enjoyable approach to physical exercise. VR technology is thus highly suitable for combining exercise with gaming (exergaming). Studies have indicated that individuals using VR training outperformed those using traditional training programs in the Fugl–Meyer assessment, Berg balance scale, timed up-and-go test, functional reach test, and 10-m walking test (10–12). Moreover, individuals with cerebral palsy or Down syndrome exhibited marked improvements in their motor coordination, balance, and ambulatory function after undergoing weekly 1-h VR training sessions, highlighting the efficacy of this training for improving physical capabilities (13, 14). Many scholars have reported improved motor control in patients undergoing VR training, but the results have been inconsistent. Moreover, studies have yet to examine the effect of VR training in children with DCD.
2. Method
2.1. Participants
A total of 10 young adults (age: 25.9 ± 4.3 years; 3 men and 7 women) and 13 school-age children with DCD (average age: 8.8 ± 0.9 years; 7 boys and 6 girls) participated in our phase I study to examine the test–retest reliability and concurrent validity of the system and program that we developed with a customer. In our phase II feasibility study, a further 13 children with DCD joined the original 13 children with DCD, leading to a total of 26 participants (age: 8.3 ± 1.0 years, 16 boys and 10 girls). These children completed an 8-week program with our VR device. The young adults were recruited from a university for convenience. Individuals with a neurological, musculoskeletal, or cardiopulmonary condition were excluded. Children with DCD were screened and referred by teachers from local primary schools. DCD diagnosis was based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. We used the Movement Assessment Battery for Children, Second Edition (MABC-2) to confirm the children's motor skill deficits. Motor difficulty was indicated by a total score at or below the 16th percentile of the age norm. This study was approved by the ethics committee of our university, and the participants provided informed consent prior to their participation, in accordance with the Declaration of Helsinki.
Table 1 presents the demographic characteristics of the participants. All of the children with DCD in the phase I and II studies had total MABC-2 scores that were below the 16th percentile. Their subtest scores also revealed motor difficulties in aiming, catching, and balance.
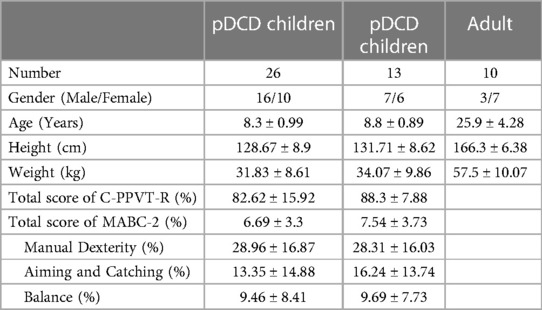
Table 1. The demographic characteristics of phase I and II participants.
2.2. Equipment and apparatus
2.2.1. Hardware
ProComp5 Infiniti encoder (SA7525, Thought Technology Ltd., 2007, Canada.)
The ProComp5 Infiniti™ (SA7525, Thought Technology Ltd., 2007, Canada.) is encased in an ergonomically designed housing, requiring only a USB port for seamless connectivity to the computer. With two sensor channels, it ensures optimal signal fidelity, providing a high sampling rate of 2,048 samples per second for observing raw heart rate signals.
2.2.1.1. VIVE pro (HTC Corporation, Taiwan)
To develop our VR-based exergaming program, we used the VIVE pro (HTC Corporation, Taiwan) as our application programming interface. The VIVE pro is a portable and convenient VR system that includes a head monitor and four sensors, two each for the hands and feet. The head monitor has a 110° field of view, a resolution of 1,080 × 1,200 pixels per eye, and a refresh rate of 90 Hz. We added a custom-made heart rate monitor to this system. The sensor was attached to the pulp of the index finger of the non-dominant hand and fixed at the wrist by a wire. Figure 1 demonstrates the experimental setting.
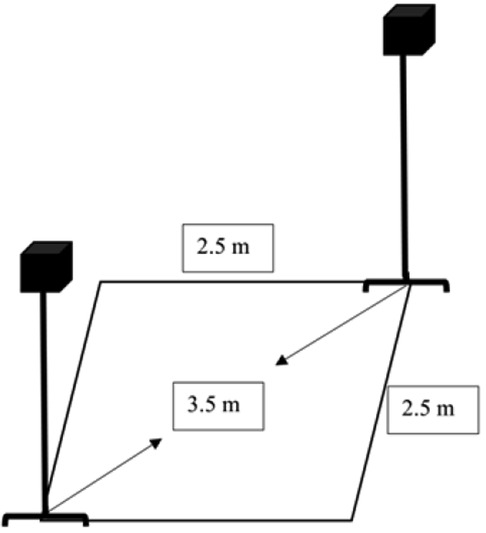
Figure 1. The experiment setting. In the virtual reality environment setup, cameras are placed at diagonal corners with a spacing of 3.5 m, forming a rectangular frame measuring 2.5 m in length and width. Children will perform action training within this area.
2.2.2. Software
We designed an exergaming program named “Animal Escape” by using Unity software (Unity 5.0, Unity-Technologies, 2004, San Francisco, California, USA; Figure 2). The game content was task oriented, with a focus on repetitive practice of real-life functional tasks.

Figure 2. The VR exergaming program. The virtual reality system creates a cardiorespiratory fitness exercise game with the background of small animals escaping from a farm. Children are required to help the farmer catch the small animals and bring them back to the farm.
Consistent with the principles of aerobic exercise training, the game is structured as follows: first, a 5-min warm-up stretching activity, then 20 min of training activities, and finally, a 5-min cool-down activity (15). The game involves returning escaped animals to their farm. Different animals appear one after another and hide in random locations. As soon as one appears, the player must catch it. The interval between the appearance of animals is 1 s during the warm-up and cool-down stages but 0.5 s or 0.25 s during the training stage. Players receive a coin reward after having caught 100 animals.
2.2.3. Movement assessment battery for children-second edition (MABC-2)
The MABC-2 is a norm-referenced motor test for children aged 3–16 years (16).
The test is divided into three age bands (3–6, 7–10, and 11–16 years) and consists of three subtests (manual dexterity, aiming and catching, and balance). The total score on the three subtests is used to diagnose motor difficulties in children. A total score at or below the 5th percentile denotes a significant movement difficulty, whereas scores between the 5th and 15th percentiles indicate the child is at risk of having movement difficulties (16). The MABC-2 test has been widely used in hospitals and research because of its good-to-excellent test–retest reliability and validity (17). In this study, children with a total MABC-2 score lower than the 16th percentile were regarded as having DCD.
2.3. Outcome measurement
2.3.1. Enjoyment rating scale
After the whole training session, we used the enjoyment rating scale (Table 2) to measure how much the children enjoyed the exergaming program. We used a 5-point Likert scale (0: no fun at all, 1: boring, 2: a bit of fun, 3: fun, and 4: super fun) (18, 19).
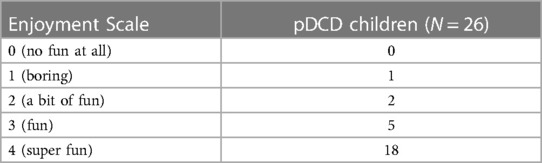
Table 2. The results of the enjoyment scale.
2.3.2. Intrinsic motivation inventory scale (IMI scale)
The intrinsic motivation inventory (IMI), a multidimensional measurement device that is grounded in self-determination theory, is intended to assess participants' subjective experiences related to a target activity. There are seven subscales of IMI. However, we only used the following three subscales of the IMI: interest/enjoyment (seven items), perceived competence (six items), and effort/importance (six items; Table 3). Each item is scored from 1 to 7 points, with more points indicating more favorable performance. The IMI has been applied in healthy adults, athletes, patients with schizophrenia, and patients with stroke (20–23). This scale has favorable test–retest reliability (intraclass correlation r = 0.77) (20).
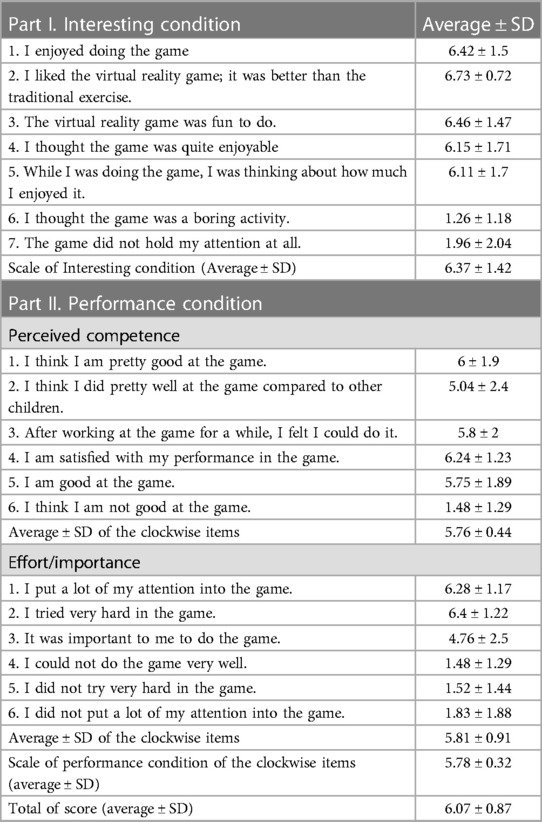
Table 3. The results of the IMI score.
2.3.3. Twenty-meter shuttle run test
The 20-m shuttle run test (20mSRT) is a common field test for measuring cardiorespiratory fitness and has favorable test–retest reliability (r = 0.89) (24, 25). In the test, a participant must run back and forth between two lines before a beep sounds. The test ends when the child fails to reach the line before the designated time. The total distance ran represents the test performance.
2.4. Procedure
A total of 10 young adults and 13 children with DCD participated in phase I of our study, in which we examined the test–retest and concurrent validity of our custom-designed heart rate device. We measured the participants' heart rate under static and dynamic conditions. In the static condition, a participant was asked to sit quietly and relax on a chair with its height adjusted to their leg length to ensure hip and knee flexion of 90° and that their feet were flat on the floor. The participant's hands were naturally placed on their thighs. The examiner twice recorded the participant's heart rate for 1 min, with the interval between measurements being 30 min. Subsequently, for the dynamic task, the participant performed a modified stepping test; the adults and children used 35 cm and 20 cm steps, respectively. The task involved 24 up-and-down cycles per minute for 2 min, yielding 96 steps. Immediately after the test, the participant sat on a chair in the same manner as previously described, and their heart rate was measured for 1 min; the measurement was repeated after 30 min. In our phase II study for measuring the feasibility of the system, another 13 children with DCD joined the original 13 children for an 8-week exergaming program using our VR device. After the 8-week program, all participants completed the enjoyment rating scale, IMI, and 20mSRT (26). All participants completed the enjoyment rating scale and IMI after the physical fitness game.
2.5. Statistical analysis
The participants' demographic data and their scores on the enjoyment rating scale and IMI are presented as means and standard deviations. We examined the test–retest reliability and concurrent validity of our device by using Pearson correlation analysis (i.e., calculating the intraclass correlation coefficient, ICC; SPSS version 20; Chicago, IL, USA). Pearson correlation coefficients of <0.5, 0.5–0.75, and >0.75 indicate no correlation, moderate-to-good correlation, and excellent correlation, respectively.
3. Results
3.1. The test–retest reliability and concurrent validity with self-developed heart rate monitor device
In the static task, the device exhibited good-to-excellent test–retest reliability (adult group ICC = 0.946, p = 0.000; children group ICC = 0.768, p = 0.001) and concurrent validity (adult group r = 0.992, p = .000; children group r = 0.943, p = .000). In the dynamic task, the device exhibited moderate-to-good test–retest reliability (adult group ICC = 0.93, p = 0.000; children group ICC = 0.913, p = 0.000) and excellent concurrent validity (adult group r = 0.98, p = .000; children group r = 0.967, p = .000).
3.2. Feasibility of the VR-based training system
The average rating on the enjoyment rating scale was 3.6 ± 0.8 points (maximum = 4; Table 2). In terms of the IMI, the average scores were 6.4 ± 1.4 and 5.8 ± 0.3 points for the interest and performance subdimensions, respectively (Table 3). After 8 weeks of training with the VR-based exergame, the children with DCD exhibited a significant improvement in the distance they ran in the 20mSRT from 129.23 m to 176.92 m (p < 0.001). However, their ⩒O2max was not significantly better after the training program.
4. Discussion
In this study, we examined the test–retest reliability, concurrent validity, and feasibility of an exergame system aimed at improving cardiopulmonary fitness. In the feasibility test, we considered the participants' enjoyment, intrinsic motivation, and performance on the 20mSRT after 8 weeks of training. Our results indicated that the concurrent validity of the heart rate device was good to excellent and that the participants enjoyed using the system. They also had high scores for the interest and performance subdimensions of the IMI.
4.1. High reliability and validity of the heart rate device
Our heart rate device exhibited good-to-excellent test–retest reliability and concurrent validity. Individuals with gross motor deficits have consistently been found to have lower cardiopulmonary fitness and reduced anaerobic exercise capacity (27, 28). Cardiopulmonary fitness is commonly assessed using heart rate and ⩒O2max. In our study, the average resting heart rate in the healthy adults was 80–83 beats per min, consistent with findings from previous studies (29, 30). In addition, the children with DCD in our sample had higher resting heart rates than typically developing children, ranging from 90 to 97 beats per min. This can be attributed to their engagement in static activities for prolonged periods and limited participation in moderate-to-vigorous-intensity exercise (31). We employed static and dynamic tasks to observe changes in heart rate. During the dynamic task, our heart rate device exhibited slightly lower test–retest reliability than a commercial heart rate device with cable transmission. However, our heart rate device remains viable because of its portability and wireless transmission capability (contingent on a stable wireless connection).
4.2. Change in fitness level after VR training
4.2.1. Objective change
The 20mSRT is a widely recognized measurement tool for assessing ⩒O2max in children and adults. Numerous studies have reported that children with DCD tend to cover a shorter distance during the 20mSRT than do typically developing children, indicating lower cardiorespiratory fitness in children with DCD (28). Furthermore, the 20mSRT has been proven effective in detecting changes in fitness following training interventions. After our participants used our VR fitness program, the distance they covered in the 20mSRT was significantly higher than that before. However, we discovered no significant change in their ⩒O2max. The VR game helped improve the participants' cardiopulmonary fitness because they could run longer distances than before playing the game. Other research has also demonstrated that physical fitness programs can improve muscle power and endurance (32). Leger et al. reported that for estimating the ⩒O2max of children aged 6–18 years, data from the multistage 20mSRT had good reliability. Additionally, relative to a treadmill test, the 20mSRT was discovered to have moderate reliability for estimating ⩒O2max in children aged 6–10 years (33). Although the estimated ⩒O2max derived from the multistage 20mSRT is a useful option for estimating cardiorespiratory fitness, it may yield more accurate results in adults than in children (34). Notably, discrepancies may have arisen between the distance covered during the 20mSRT and the estimated ⩒O2max, potentially leading to inconsistent performance rankings in our study. We conducted the test outdoors to provide a natural environment for the children. Additionally, some of the children may have felt hot and tired during the outdoor testing, and these factors may have affected their motivation and performance.
4.2.2. Perceived change
We used the enjoyment rating scale, which has favorable reliability (35, 36), to measure the children's motivation. The children in our study comprehended the scale's meaning and provided responses accordingly. Most of the children reported having fun while playing our game. However, three children expressed boredom or less enjoyment and perceived the game as too easy, leading to low motivation. To assess our participants' abilities, performance, and mental engagement, we used the IMI (37). The children understood the scale items and could thus accurately answer them. The children's answers on the IMI prior to playing the game indicated that most of them had high expectations. Moreover, we observed that the children concentrated and exerted considerable effort during the game because they believed that maintaining their motivation was crucial given the perceived difficulty level. After playing the game, most of the children reported liking it and had increased confidence because their abilities and physical fitness had improved. Additionally, the VR game fostered closer relationships between the children and their classmates.
4.3. Study limitation
Because of the unstable wireless connection of the heart rate device during the dynamic task, only moderate test–retest reliability was discovered for this task. Moreover, the estimated ⩒O2max of our 26 participants, measured using the multistage 20mSRT, was not improved after our VR training program. We recognize that this test may not be the most accurate for measuring ⩒O2max changes, but it was the only one we employed. Three children provided low enjoyment scores, suggesting room for improvement in the game's content to make it more challenging and interesting. In addition, the small sample size affects the study's generalizability and application.
4.4. Future study
We aim to adopt a higher-quality wireless transmission module to improve our heart rate device performance. To enhance the children's enjoyment of the game, we plan to introduce different game levels to challenge the children appropriately in accordance with their abilities.
5. Conclusion
Our device has good reliability and validity. Additionally, we obtained preliminary evidence that our VR game can improve physical fitness, but further research with a larger sample size is necessary. The VR game and heart rate device that we have designed may be useful for physical fitness interventions in the future.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by National Cheng Kung University Governance Framework for Human Research Ethics. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
Totally, five researchers completed the study together, such as R-JC and students, Y-JJ and P-SH, designed the game program and performed this study project. Y-CD and his student, H-CH, wrote the programming of heart rate device and virtual reality system. All authors contributed to the article and approved the submitted version.
Funding
This study was partially funded by grants from the National Science and Technology Council, Taiwan, ROC: MOST 107-2221-E-006 -066 -MY2 supported by MOST 107-2221-E-006 -066 -MY2.
Acknowledgment
We would like to thank all the participants and their family. This study was partially funded by grants from the National Science and Technology Council, Taiwan, ROC.
Conflict of interest
H-CH was employed by the company Voltafield Technology Corporation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ruiz JR, Cavero-Redondo I, Ortega FB, Welk GJ, Andersen LB, Martinez-Vizcaino V. Cardiorespiratory fitness cut points to avoid cardiovascular disease risk in children and adolescents; what level of fitness should raise a red flag? A systematic review and metaanalysis. Br J Sports Med. (2016) 50(23):1451–8. doi: 10.1136/bjsports-2015-095903
2. Cairney J, Hay J, Veldhuizen S, Faught B. Comparison of VO2 maximum obtained from 20 m shuttle run and cycle ergometer in children with and without developmental coordination disorder. Res Dev Disabil. (2010) 31(6):1332–9. doi: 10.1016/j.ridd.2010.07.008
3. Cairney J, Veldhuizen S, King-Dowling S, Faught BE, Hay J. Tracking cardiorespiratory fitness and physical activity in children with and without motor coordination problems. J Sci Med Sport. (2017) 20(4):380–5. doi: 10.1016/j.jsams.2016.08.025
4. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. (2003) 14(2):125–30. doi: 10.1111/1467-9280.t01-1-01430
5. Young J, Angevaren M, Rusted J, Tabet N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev. (2015) 4:Cd005381. doi: 10.1002/14651858.CD005381.pub4
6. Ludyga S, Gerber M, Mücke M, Brand S, Weber P, Brotzmann M, et al. The acute effects of aerobic exercise on cognitive flexibility and task-related heart rate variability in children with ADHD and healthy controls. J Atten Disord. (2020) 24(5):693–703. doi: 10.1177/1087054718757647
7. Watts K, Jones TW, Davis EA, Green D. Exercise training in obese children and adolescents: current concepts. Sports Med. (2005) 35(5):375–92. doi: 10.2165/00007256-200535050-00002
8. Pollock ML, Wenger NK. Physical activity and exercise training in the elderly: a position paper from the society of geriatric cardiology. Am J Geriatr Cardiol. (1998) 7(4):45–6. PMID: 1141646511416465
9. Lau PW, Wang JJ, Maddison R. A randomized-controlled trial of school-based active videogame intervention on Chinese children’s aerobic fitness, physical activity level, and psychological correlates. Games Health J. (2016) 5(6):405–12. doi: 10.1089/g4h.2016.0057
10. Shin JH, Kim MY, Lee JY, Jeon YJ, Kim S, Lee S, et al. Effects of virtual reality-based rehabilitation on distal upper extremity function and health-related quality of life: a single-blinded, randomized controlled trial. J Neuroeng Rehabil. (2016) 13:17. doi: 10.1186/s12984-016-0125-x
11. Thielbar KO, Lord TJ, Fischer HC, Lazzaro EC, Barth KC, Stoykov ME, et al. Training finger individuation with a mechatronic-virtual reality system leads to improved fine motor control post-stroke. J Neuroeng Rehabil. (2014) 11:171. doi: 10.1186/1743-0003-11-171
12. Zondervan DK, Friedman N, Chang E, Zhao X, Augsburger R, Reinkensmeyer DJ, et al. Home-based hand rehabilitation after chronic stroke: randomized, controlled single-blind trial comparing the MusicGlove with a conventional exercise program. J Rehabil Res Dev. (2016) 53(4):457–72. doi: 10.1682/jrrd.2015.04.0057
13. Lopes JBP, Duarte NAC, Lazzari RD, Oliveira CS. Virtual reality in the rehabilitation process for individuals with cerebral palsy and down syndrome: a systematic review. J Bodyw Mov Ther. (2020) 24(4):479–83. doi: 10.1016/j.jbmt.2018.06.006
14. Warnier N, Lambregts S, Port IV. Effect of virtual reality therapy on balance and walking in children with cerebral palsy: a systematic review. Dev Neurorehabil. (2020) 23(8):502–18. doi: 10.1080/17518423.2019.1683907
15. Obrusnikova I, Firkin CJ, Farquhar WB. A systematic review and meta-analysis of the effects of aerobic exercise interventions on cardiorespiratory fitness in adults with intellectual disability. Disabil Health J. (2022) 15(1):101185. doi: 10.1016/j.dhjo.2021.101185
16. Henderson S, Sugden D, Barnett A. Movement assessment battery for children. 2nd ed. London, England: Harcourt Assessment (2007).
17. Schoemaker MM, Niemeijer AS, Flapper BC, Smits-Engelsman BC. Validity and reliability of the movement assessment battery for children-2 checklist for children with and without motor impairments. Dev Med Child Neurol. (2012) 54(4):368–75. doi: 10.1111/j.1469-8749.2012.04226.x
18. Smits-Engelsman BC, Jelsma LD, Ferguson GD, Geuze RH. Motor learning: an analysis of 100 trials of a ski slalom game in children with and without developmental coordination disorder. PLoS One. (2015) 10(10):e0140470. doi: 10.1371/journal.pone.0140470
19. Jelsma D, Geuze RH, Mombarg R, Smits-Engelsman BC. The impact of wii fit intervention on dynamic balance control in children with probable developmental coordination disorder and balance problems. Hum Mov Sci. (2014) 33:404–18. doi: 10.1016/j.humov.2013.12.007
20. Alexandris K, Tsorbatzoudis C, Grouios G. Perceived constraints on recreational sport participation: investigating their relationship with intrinsic motivation, extrinsic motivation and amotivation. J Leis Res. (2002) 34(3):233–52. doi: 10.1080/00222216.2002.11949970
21. Lloréns R, Noé E, Colomer C, Alcañiz M. Effectiveness, usability, and cost- benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke: a randomized controlled trial. Arch Phys Med Rehabil. (2015) 96(3):418–25.e2. doi: 10.1016/j.apmr.2014.10.019
22. McAuley E, Duncan T, Tammen VV. Psychometric properties of the intrinsic motivation inventory in a competitive sport setting: a confirmatory factor analysis. Res Q Exerc Sport. (1989) 60(1):48–58. doi: 10.1080/02701367.1989.10607413
23. Choi J, Mogami T, Medalia A. Intrinsic motivation inventory: an adapted measure for schizophrenia research. Schizophr Bull. (2010) 36(5):966–76. doi: 10.1093/schbul/sbp030
24. Léger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. (1988) 6(2):93–101. doi: 10.1080/02640418808729800
25. Pitetti K, Fernhall B, Figoni S. Comparing two regression formulas that predict ⩒O2peak using the 20-M shuttle run for children and adolescents. Pediatr Exerc Sci. (2002) 14:125–34. doi: 10.1123/pes.14.2.125
26. George AM, Rohr LE, Byrne J. Impact of nintendo wii games on physical literacy in children: motor skills, physical fitness, activity behaviors, and knowledge. Sports. (2016) 4(1):3. doi: 10.3390/sports4010003
27. O’Beirne C, Larkin D, Cable T. Coordination problems and anaerobic performance in children. Adapt Phys Activ Q. (1994) 11:141–9. doi: 10.1123/apaq.11.2.141
28. Cairney J, Hay JA, Faught BE, Flouris A, Klentrou P. Developmental coordination disorder and cardiorespiratory fitness in children. Pediatr Exerc Sci. (2007) 19(1):20–8. doi: 10.1123/pes.19.1.20
29. Fleming S, Thompson M, Stevens R, Heneghan C, Plüddemann A, Maconochie I, et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet. (2011) 377(9770): 1011–8. doi: 10.1016/S0140-6736(10)62226-X
30. Colasante T, Malti T. Resting heart rate, guilt, and sympathy: a developmental psychophysiological study of physical aggression. Psychophysiology. (2017) 54(11):1770–81. doi: 10.1111/psyp.12915
31. Chen FC, Tsai CL, Biltz GR, Stoffregen TA, Wade MG. Variations in cognitive demand affect heart rate in typically developing children and children at risk for developmental coordination disorder. Res Dev Disabil. (2015) 38:362–71. doi: 10.1016/j.ridd.2014.12.002
32. Chambers TL, Burnett TR, Raue U, Lee GA, Finch WH, Graham BM, et al. Skeletal muscle size, function, and adiposity with lifelong aerobic exercise. J Appl Physiol. (2020) 128(2):368–78. doi: 10.1152/japplphysiol.00426.2019
33. Arsa G, Lanza FC, Cambri LT, Antonio EL, Murad N, de Mello MT, et al. Predicted equation for VO2 based on a 20-meter multistage shuttle run test for children. Int J Sports Med. (2018) 39(14):1049–54. doi: 10.1055/a-0665-4700
34. Mayorga-Vega D, Aguilar-Soto P, Viciana J. Criterion-related validity of the 20-M shuttle run test for estimating cardiorespiratory fitness: a meta-analysis. J Sports Sci Med. (2015) 14(3):536–47. PMID: 26336340; PMCID: PMC454111726336340
35. Burford K, Gillespie K, Jowers EM, Bartholomew JB. Children’s enjoyment, perceived competency, and vigorous physical activity during high-intensity interval training in physical education. Res Q Exerc Sport. (2022) 93(4):835–44. doi: 10.1080/02701367.2021.192520734806941
36. Timo J, Sami YP, Anthony W, Jarmo L. Perceived physical competence towards physical activity, and motivation and enjoyment in physical education as longitudinal predictors of adolescents’ self-reported physical activity. J Sci Med Sport. (2016) 19(9):750–4. doi: 10.1016/j.jsams.2015.11.003
Keywords: developmental coordination disorder, cardiopulmonary fitness, exergame, virtual reality, motor skill deficit
Citation: Ju Y-J, Du Y-C, Huang H-C, Hu Kao P-S and Cherng R-J (2023) Development and feasibility of a virtual reality-based exergaming program to enhance cardiopulmonary fitness in children with developmental coordination disorder. Front. Pediatr. 11:1238471. doi: 10.3389/fped.2023.1238471
Received: 11 June 2023; Accepted: 1 December 2023;
Published: 20 December 2023.
Edited by:
Michelle Plusquin, University of Hasselt, BelgiumReviewed by:
Barbara Lombardo, University of Naples Federico II, ItalyOlga Scudiero, University of Naples Federico II, Italy
Rossella Alfano, University of Hasselt, Belgium
© 2023 Ju, Du, Huang, Hu Kao and Cherng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rong-Ju Cherng cmpjNDdAbWFpbC5uY2t1LmVkdS50dw==