 Zakaria Ahmed Mohamed
Zakaria Ahmed Mohamed Chunjiao Tang1
Chunjiao Tang1 Youping Deng
Youping Deng Jingyi Fan
Jingyi Fan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 17 August 2023
Sec. Pediatric Infectious Diseases
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1226403
Background: The Omicron variant of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is less likely to cause severe disease in children than the other variants but has become an increasing cause of febrile seizures (FS) among children. In this case-control study, we aimed to examine the risk factors associated with FS in children infected with the COVID-19 Omicron variant and related treatment modalities.
Methods: This retrospective case-control study includes 113 subjects infected with the COVID-19 Omicron variant, grouped into 45 cases (those with FS) and 68 controls (those without FS). Data on clinical features, laboratory parameters, and treatment modalities were collected and analyzed.
Results: Approximately 5.74% of COVID-19 infected children developed COVID-19-associated FS. Children with COVID-19 and high body temperatures [RR 1.474; (95% CI: 1.196–1.818), p < 0.001], previous history of FS [RR 1.421; (95% CI: 1.088–1.855), p = 0.010], high procalcitonin levels [RR 1.140; (95% CI: 1.043–1.246), p = 0.048] and high neutrophil counts [RR 1.015; (95% CI: 1.000–1.029), p = 0.048] were more likely to experience FS than the controls. In contrast, children with COVID-19 and low eosinophil counts, low hemoglobin levels, and cough had a lower risk of developing FS [RR 0.494; (95% CI: 0.311–0.783), p = 0.003], [RR 0.979; (95% CI: 0.959–0.999), p = 0.044]; and [RR 0.473 (95% CI 0.252–0.890), p = 0.020]; respectively. Children with FS received more anti-flu medications than those without.
Conclusion: A significant increase in FS was observed in children with Omicron SARS-CoV-2 infection. A higher body temperature, a history of FS, a higher procalcitonin level, and a high neutrophil count were all associated with an increased risk of FS in children with COVID-19. The risk of developing FS was lower in children with COVID-19 and low eosinophil counts and hemoglobin levels than in those without.
On December 7, 2022, China abruptly amended its COVID-19 containment policy, ending the almost three-year-long zero Covid policy. This sudden shift in approach led to a surge in COVID-19 outbreaks countrywide, with the mutated Omicron variant as the dominant variant (1). Unlike its predecessor, the delta variant, Omicron was particularly associated with significantly increased pediatric admissions in China (2–4) and abroad (5–9). It further impacted other pediatric illnesses; for instance, several US investigators noticed a sharp rise in the incidence of Croup, a clinically diagnosed pediatric disease caused by virus-induced subglottic airway inflammation or laryngotracheobronchitis (10–13). Recent publications from Korea (14), Japan (15), and the USA (16) have all demonstrated an association between the Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Omicron variant and increased incidence of febrile seizures among children compared to the pre-Omicron stage. While emerging evidence clarifies this association, the clinical characteristics of these children and other associated factors are still largely undescribed.
Febrile seizure (FS) is a common neurological disorder affecting 2%–4% of children <5 years old who do not have any intracranial infections (17). Although its exact etiology is still unclear, it's strongly associated with the elevation of body temperature, certain vaccinations, previous history and family history of FS, maternal alcohol exposure, iron deficiency, and viral infections (18–20). Among the published viral causes of FS, adenoviruses, human herpesvirus-6, influenza, and rhinoviruses are the standout culprits (21, 22); for instance, evidence suggests that 15%–20% of children hospitalized with influenza A virus develop FS (23). In Wuhan City, the Omicron strains BA.1, BA.2, BA.5, and BF.7 were the dominant strains that significantly drove up pediatric admissions at our hospital in February 2023.
Given the reported association between the Omicron variant and increased incidence of FS, coupled with the paucity of studies on the risk factors associated with febrile seizures among children infected with the SARS-CoV-2 Omicron variant, we sought to evaluate SARS-CoV-2-Omicron infected children to ascertain their risks for developing febrile seizures and related treatment modalities.
This study was a retrospective case-control design conducted at the pediatrics department of Zhongnan Hospital of Wuhan University, Wuhan, China, using medical records of pediatric patients below 14 years of age who were admitted due to COVID-19 in December 2022. The cases had febrile seizures, while the controls were febrile children without seizures. Febrile seizures were diagnosed based on the International Classification of Disease (ICD)-10 code of R56.0 (febrile seizure), while COVID-19 was diagnosed using polymerase chain reaction (PCR) or antigen test. Cases were children aged 0 months to 12 years presenting with febrile seizures as per the American Academy of Pediatrics (AAP) guidelines (24), while controls were children aged 0 months to 13 years presenting with fever but no seizures. Children with afebrile seizures, chronic neurodevelopmental problems, metabolic abnormalities, central nervous system infections, and diagnosed cases of other hematologic issues, those on an iron supplement, chronic systemic diseases, and very sick children were excluded from the study. Consecutive cases and concurrent controls were selected from the same setting in a ratio of 1:1. We defined a simple febrile seizure as a generalized tonic-clonic seizure lasting less than 15 min, occurring only once in 24 h in a child between 6 months and 5 years of age with a fever of 38°C. A seizure lasting more than 15 min in a child under 6 months or more than 5 years of age and occurring more than once in 24 h is a complex febrile seizure. Febrile status epilepticus is any prolonged or recurrent seizure lasting more than 30 min without returning to full consciousness.
Data collected on both cases and controls were: Clinical history, physical examination, relevant laboratory investigations, and treatment. Clinical characteristics include; age (in months), sex, underlying disease, previous febrile seizure history, and family history. Seizure features included; underlying disease, previous febrile seizure history, family history, seizure duration (in minutes), total seizure number in 24 h, and peak body temperature. Treatment provided included; anticonvulsant therapy, antipyretics, and other medications used.
The Statistical Package for Social Sciences, SPSS (Version 27, IBM, Inc.), was used for the data analysis. Statistical analysis included descriptive statistics and a multivariate Poisson regression model to determine the adjusted risk ratio and independent risk factors for febrile seizures in children.
In December 2022, 1,289 pediatric patients were diagnosed with COVID-19 in our outpatient department. Among these patients, 74 (5.74%) were diagnosed with febrile seizures, of which 45 (60.8%) were hospitalized. The majority of the patients 29 (64.4%), had simple febrile seizures, whereas 16 (35.6%) suffered from complex febrile seizures (Figure 1).
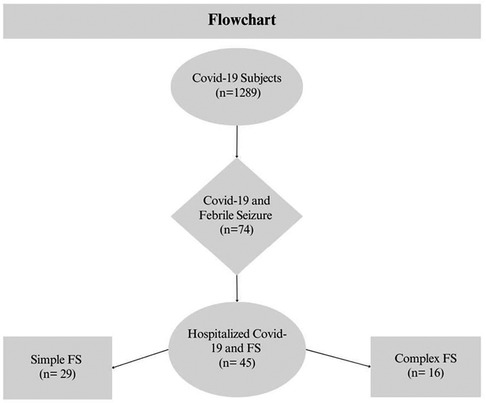
Figure 1. Database cohort overview flowchart.
The two groups of patients did not differ in age, gender, underlying disease, number of days of hospitalization, and poor sanity (all p > 0.05). However, we observed significant differences regarding previous history of FS, family history of FS, and maximum body temperature (all p < 0.05). Concerning COVID-19 associated clinical symptoms, cases did not differ from controls with regards to a stuffy nose, runny nose, headache, vomiting, diarrhea, non-consciousness, pulse rate, and SPO2 (all p > 0.05) but differed significantly in terms of cough, expectoration, dry rales, wet rales, and respiration rate (all p < 0.05). Detailed information is summarized in Table 1.
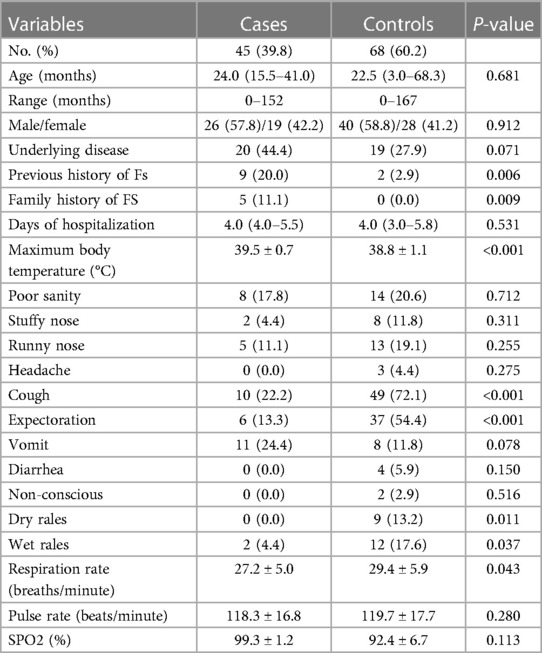
Table 1. Clinical characteristics of the patients.
There were no statistically significant differences between the two groups in terms of C-reactive protein, interleukin 6, carbon dioxide, myoglobin, high-sensitivity troponin, and creatine kinase MB (all p > 0.05). Similar results were obtained for respiratory syncytial virus, influenza A and B, mycoplasma pneumonia, Epstein-Barr virus capsid antigen IgM, and cytomegalovirus IgM. In contrast, erythrocyte sedimentation rate, procalcitonin, and bacterial infection rates differed significantly (p < 0.05). Procalcitonin levels and bacterial infection rates were higher in cases than in controls, while ESR was lower in cases. Analysis of hematological parameters revealed that hemoglobin, platelets, lymphocytes, and eosinophils were significantly lower in cases than in controls (all p < 0.05). At the same time, neutrophil counts were significantly higher in cases than in controls (p < 0.05). However, there were no significant differences between the two groups regarding white blood cell counts, red blood cell counts, and monocyte counts (all p > 0.05). Liver, renal function tests and electrolyte levels showed no difference between cases and controls in terms of the levels of alanine transaminase, aspartate aminotransferase, total protein, albumin, globulin, creatinine, potassium, sodium, chloride, and calcium levels (all p > 0.05), while, blood urea nitrogen levels were significantly higher in cases than control (all p < 0.05). Detailed information is presented in Table 2.
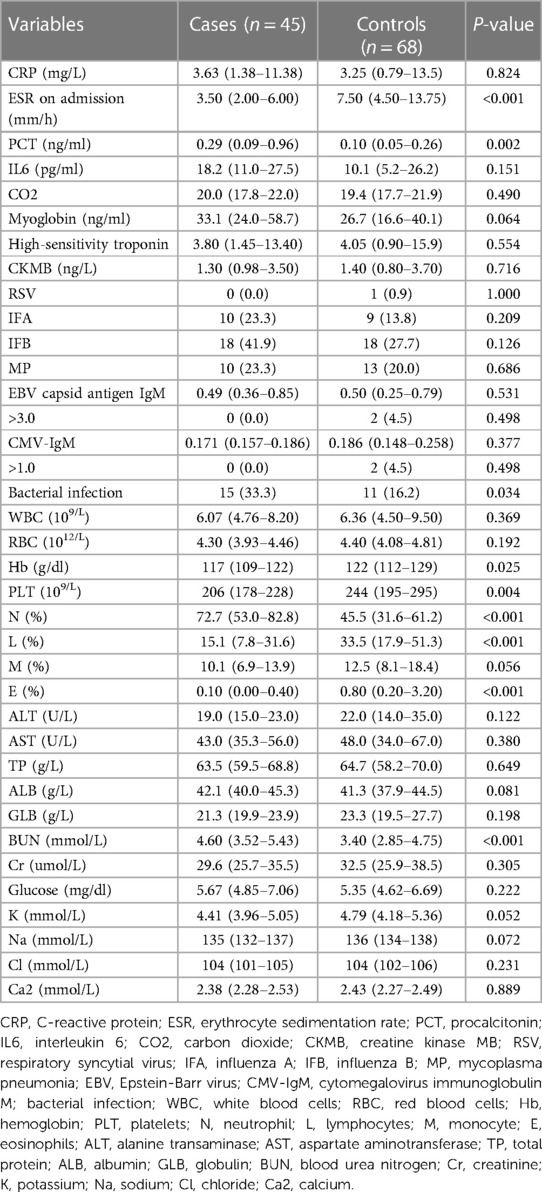
Table 2. Comprehensive laboratory investigations.
There was no difference in the prescription of piperacillin, tazobactam, azithromycin, clindamycin, ceftriaxone, cefoperazone, sulbactam, ribavirin, and ganciclovir between cases and controls (all p > 0.05). In contrast, more children in the case group were prescribed antiflu medications than those in the control group (p < 0.05). Additionally, we did not observe any significant differences between case and control with regards to intravenous corticosteroids, such as hydrocortisone, dexamethasone, or nebulizers, including beclomethasone dipropionate inhalation, ipratropium bromide inhalation, albuterol inhalation, acetylcysteine inhalation or expectorants such as ambroxol oral medicine, oral montelukast sodium, non-invasive breathing, oxygen with a mask or nasal cannula, invasive breathing (all p > 0.05). In contrast, fewer children in the case group were given methylprednisolone, sodium succinate injection, budesonide inhalation, and ambroxol injection than those in the control group (p < 0.05). Detailed information is presented in Table 3.

Table 3. Medications used.
Lastly, we conducted a Poisson regression analysis to determine factors that can predict the development of febrile seizures in children infected with COVID-19. We adjusted for cough, maximum body temperature, history of previous seizures, eosinophil count, hemoglobin levels, procalcitonin levels, neutrophil count, platelet count, and blood urea nitrogen.
In a minimally adjusted model (model 1), children with COVID-19 and cough were less likely to experience FS than their controls, adjusted [RR 0.309; (95% CI: 0.170–0.564), p < 0.001], while those with high body temperatures and previous history of febrile seizures were more likely to experience febrile seizures than their controls, adjusted [RR 1.474; (95% CI: 1.196–1.818), p < 0.001], and [RR 1.421; (95% CI: 1.088–1.855), p = 0.010], respectively.
Using the moderately adjusted model (model 2), which was adjusted for eosinophil count, hemoglobin level, neutrophil count, platelet count, and blood urea nitrogen, children with low eosinophil counts and hemoglobin levels had a lower risk of developing FS [RR 0.494; (95% CI: 0.311–0.783), p = 0.003] and [RR 0.979 (95% CI: 0.959–0.999), p = 0.044], respectively. In comparison, those with higher procalcitonin levels and neutrophil counts had a higher risk of experiencing FS than those without [RR 1.140; (95% CI: 1.043–1.246), p = 0.048], and [RR 1.015; (95% CI: 1.000–1.029), p = 0.048], respectively.
After adjusting for all these factors in (model 3), children with COVID-19 with low eosinophil counts [RR 0.428 (95% CI: 0.275–0.666), p < 0.001], low hemoglobin levels [RR 0.978 (95% CI: 0.960–0.996), p = 0.015], and cough [RR 0.473 (95% CI: 0.252–0.890), p = 0.020], had a lower risk of developing FS. Meanwhile, children with COVID-19 with higher procalcitonin levels [RR 1.140 (95% CI: 1.043–1.246), p = 0.004] and neutrophil counts [RR 1.017 (95% CI: 1.003–1.031), p = 0.015] had a higher risk of experiencing FS than those without (Table 4).
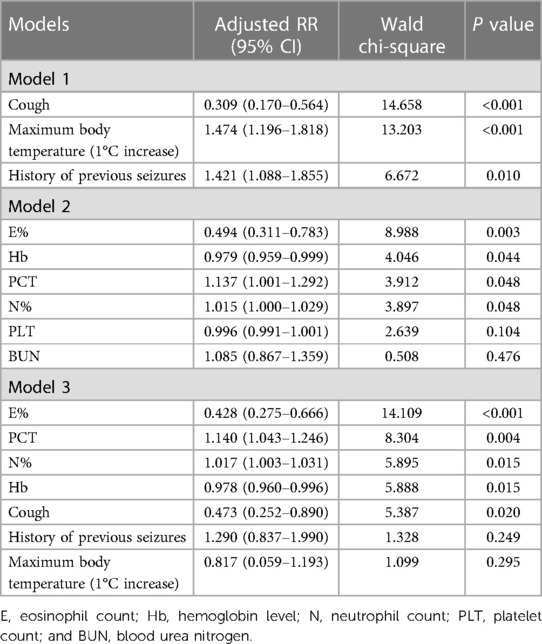
Table 4. Adjusted poisson regression models for predicting febrile seizures.
In this case-control study, we examined the incidence of febrile seizure among SARS-CoV-2-Omicron-infected children, their admission rate, risk factors associated with febrile seizures among the infected children, and their treatment modalities. Our findings revealed that 5.74% of the children had febrile seizures, and approximately 60.8% were hospitalized. These findings suggest that both COVID-19 associated OPD visits and the incidence of febrile seizures among the COVID-19-infected children rapidly increased during the Omicron period. Our results are consistent with those of Cloete et al., who reported a rapid rise in pediatric COVID-19 hospitalizations in the early stages of the Omicron wave in South Africa (25). Furthermore, a Korean study by Joung et al. demonstrated that 7.0% of COVID-19 infected Korean children developed COVID-19-associated febrile seizures during the Omicron period (26).
In August 2021, during the highly transmissible “delta variant” wave, the Chinese government adopted the “Dynamic zero-COVID” policy to stem the spread of the disease (27). During that period, pediatric seizure-related hospitalizations dropped drastically. For instance, a study in Hong Kong demonstrated a significant reduction in seizure-related emergency department visits in 2020 [RR 0.39 (95% CI: 0.174–0.526), p = 0.001]. Furthermore, the rate of febrile seizure-related admissions for children aged 0–6 decreased by more than 20% from the previous year (28). However, on December 7, 2022, China abruptly abandoned its zero-COVID policy, leading to a surge in COVID-19 outbreaks nationwide, with the mutated Omicron variant as the predominant strain (1). Since then, there has been a significant increase in pediatric infections with the SARS-CoV-2 Omicron variant and subsequently increased incidence of febrile seizures (2).
This study had no statistical difference in the ages of cases and controls (p > 0.05). However, children with febrile seizures had a slightly higher median (IQR) age than the controls, 24.0 (15.5–41.0) vs. 22.5 (3.0–68.3) months, respectively. Our findings are supported by Juong et al., who also found that children with COVID-19 and febrile seizures were generally older than those without febrile seizures; median (IQR) age 33.0 (22.0–60.0) and 23.0 (14.5–31.5) months, although their control group was COVID-19 negative children (26). In addition, evidence suggests that sex can influence the differentiation and maintenance of virus-driven T cells and antiviral immune response in tissues (29). This study had no statistical difference between the groups regarding sex distribution. Similarly, the underlying disease, number of days of hospitalization, and poor sanity of both groups did not statistically differ.
Published literature alludes to genetic predispositions for FS. For instance, Veisani et al.'s meta-analysis concluded that family history is strongly associated with febrile seizure (30). In this study, we observed a previous history of FS and a family history of FS in 20.0% and 11.1% of the cases and only 2.9% and 0% of the controls, respectively. Based on these findings, genetic factors and shared environmental exposures may play an essential role in the development of FS.
According to Taytard and colleagues, children infected with the Omicron variant have significantly higher body temperatures than those infected with the Delta variant (30). The higher peak body temperature caused by SARS-CoV-2 infection during the Omicron period may have contributed to increased febrile seizures. Despite both cases and controls in our study being positive for the Omicron variant, the cases had significantly higher body temperatures than the controls; mean (±SD) body temperature, 39.5 ± 0.7°C and 38.8 ± 1.1°C, respectively. These findings are consistent with those of Margaretha et al. (31), who found mean temperatures of 39.01 ± 0.56°C and 38.64 ± 0.45°C for children with and without FS, respectively (31). Meanwhile, Leung et al. observed that FS tended to occur when body temperatures exceeded 39°C (32).
Other clinical symptoms associated with COVID-19 were not significantly different between cases and controls, except for cough, expectoration, dry rales, wet rales, and respiration rate, which were significantly higher in controls. In most cases, COVID-19 affects children in a mild form. Fever, dry cough, and fatigue are some of the common symptoms experienced by children (33). In previous studies, the cough has been associated with high intrathoracic pressure, which can result in cough-induced syncope and fainting (34). However, our study found that cough was associated with a lower risk of febrile seizures [RR 0.473 (95% CI: 0.252–0.890), p = 0.020]. Children with COVID-19 and cough were less likely to experience febrile seizures than controls, whereas those who had a high fever were more likely to experience febrile seizures. This suggests that fever is more closely associated with FS than respiratory symptoms.
Regarding the laboratory results, bacterial infection rates were higher in cases than in controls. Bacterial infection was observed in 33.3% of children with FS and 16.2% of controls. Our findings are consistent with Jarrett et al. (35), who found a higher prevalence of bacterial infection in cases than thin e control. Similarly, procalcitonin levels (PCT) were higher in cases than in controls, with median PCT levels of 0.29 ng/ml in cases ag/ml in controls. A similar finding was found by Murakami et al. (36) who found increased levels of PCT in convulsion patients. Increased levels of procalcitonin were first observed in 1993 in patients with sepsis, and today it is a widely used biomarker for serious bacterial infections (37). PCT is a natural prohormone of calcitonin synthesized by C-cells of the thyroid glands (38). Its production increases in patients with septicemia and infections caused by gram-negative bacteria due to inflammatory cytokines, such as tumor necrosis factor-alpha and interleukin-6 (IL-6) (39). This study observed gram-negative mycoplasma pneumonia co-infections in 23.3% of cases compared to 20% of controls. Furthermore, the erythrocyte sedimentation rate was significantly lower in cases than in controls, which corresponds with the findings of Abbasi et al. (40).
According to a study by Pisacane et al., children with FS had significantly higher rates of iron deficiency anaemia than their non-FS counterparts (41). Interestingly, Talebian et al. revealed that anaemic children had a reduced incidence of febrile seizure compared to children without anaemia (42). In support of this finding, Yousefichaijan and colleagues found that iron deficiency prevents febrile convulsions in children and likely increases the threshold of neuronal excitation during fevers (43). In line with these studies, our findings revealed that cases had lower haemoglobin levels than controls and had a lower risk of developing FS [RR, (0.979; 95% CI: 0.959–0.999), p = 0.044]. Similarly, children with low eosinophil counts had a lower risk of developing FS [RR 0.494; (95% CI: 0.311–0.783), p = 0.003] than the controls. Eosinophils play an essential role in allergic inflammation, but no evidence has been found linking them to FS (44).
Moreover, in a recent study by Romanowska et al., the platelet and lymphocyte count of children with FS were significantly lower than those of controls. In contrast, the neutrophil counts were significantly higher (45). In line with the study, our study found that the platelet and lymphocyte counts were significantly lower in cases than in controls. Meanwhile, neutrophil counts were significantly higher in cases than in controls. It has been determined that neutrophil-lymphocyte ratio and mean platelet volume are novel inflammatory biomarkers associated with the development of FS in children (44).
Regarding liver and renal function tests and serum electrolytes, there was no significant difference between cases and controls, other than blood urea nitrogen level, which was significantly higher in cases than in controls. This finding is supported by Abbasi et al., who also found that patients with febrile seizures had substantially higher levels of BUN and creatinine than those without febrile seizures (40). It has been shown that patients with a history of illnesses, such as vomiting and diarrhea or signs of dehydration, may affect their renal function tests (46). In this study, 24.4% of the cases and 11.8% of the controls reported vomiting during admission. While it has been shown that hyponatremia is associated with febrile seizures (47), another study by Yousefichaija et al. has found that children with febrile seizures have normal electrolyte levels. And therefore, it is not necessary to routinely test the electrolyte levels of all patients with simple febrile seizures (48). This study found no differences between cases and controls in electrolyte levels.
The prescription of antibiotics and antivirals was not significantly different between the two groups, except for the antiflu medications, where cases got more than the controls. In contrast, fewer children in the case group were given corticosteroids and expectorants than controls. The increasing use of antiflu medications could be attributed to SARS-CoV-2 co-infection with influenza A and B viruses. A meta-analysis by Masoud Dadashi et al. showed that influenza infection was 0.8% in patients with confirmed COVID-19, while the frequency of influenza virus co-infection among patients with COVID-19 was 4.5% in Asia and 0.4% in North America (49). In line with these findings, we observed a higher incidence of influenza A; 23.3% vs. 13.8%, and influenza B; 41.9% vs. 27.7% among cases than controls, respectively.
Strengths and limitations: This study had a few distinct advantages worth highlighting: (1) It was the first study to examine the incidence of febrile seizures in children infected with the SARS-CoV-2-Omicron variant in Hubei, China. (2) It further examined detailed clinical presentations and risk factors associated with febrile seizures in children infected with the SARS-CoV-2-Omicron variant. However, the following limitations existed: (1) Sample size was rather small and this could limit the study's power. (2) The study was retrospectively conducted thus it carried the inevitable disadvantages of retrospective studies such as recall bias and missing information. (3) The study was a single-center study, so the findings cannot be generalized to make inferences on the incidence of FS among children infected with COVID-19 across the country.
In summary, a significant increase in febrile seizures was observed in children with SARS-CoV-2-Omicron infection. Approximately 5.74% of participants with COVID-19 suffered febrile seizures. A higher body temperature, a history of FS, a higher procalcitonin level and a higher neutrophil count were all associated with an increased risk of FS in children with COVID-19. The risk of developing FS was lower in children with COVID-19 who had low eosinophil counts, and low hemoglobin levels. More children in the case were prescribed antiflu medications than those in the control group. In contrast, fewer children in the case group were given corticosteroids and expectorants than those in the control group.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
This study was approved by the Ethics Committee of Zhongnan Hospital of Wuhan University, following Helsinki instructions and guidelines for medical research on children. Parents of all eligible children gave their informed consent for inclusion before they participated in the study. The confidentiality of the patients was ensured throughout the study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
The author's ZM and ET conducted manuscript drafting. CT conducted data collection and analysis. YD and JF conceived and supervised the entire study process. All authors contributed to the article and approved the submitted version.
This work was supported by the Scientific and Technological Innovation Nurturing Grant of Zhongnan Hospital of Wuhan University. Grant number: 2022CGZH-MS001.
The authors would like to thank Feng Shuwen, Zhu Zhiqiang, Yu Yuchen, Wang Xinfu, Li Wenjie, Chen Lin, Yang Dong, Tang Xiong Zhizi, Chen Zhiqiang, Zhao Wenxuan, and Liu Yu for their assistance during the data collection process.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Zheng L, Liu S, Lu F. Impact of national omicron outbreak at the end of 2022 on the future outlook of COVID-19 in China. Emerg Microbes Infect. (2023) 12(1):2191738. doi: 10.1080/22221751.2023.2191738
2. Shen N, Wu YF, Chen YW, Fang XY, Zhou M, Wang WY, et al. Clinical characteristics of pediatric cases infected with the SARS-CoV-2 Omicron variant in a tertiary children’s medical centre in Shanghai, China. World J Pediatr. (2023) 19(1):87–95. doi: 10.1007/s12519-022-00621-6
3. Zhou JG, Lu YM, Wang LB, Yu H, Zhang T, Chen YW, et al. Pediatric patients in the new wave of SARS-CoV-2 infection in Shanghai, China. World J Pediatr. (2022) 18(9):579–81. doi: 10.1007/s12519-022-00570-0
4. Li Y-C, Ma Z, Zhong H-Y, You H-L. Clinical characteristics of children with Omicron SARS-CoV-2 infection in Changchun, China from March to April 2022: a retrospective study. Front Pediatr. (2022) 10:990944. doi: 10.3389/fped.2022.990944
5. Bahl A, Mielke N, Johnson S, Desai A, Qu L. Severe COVID-19 outcomes in pediatrics: an observational cohort analysis comparing alpha, Delta, and Omicron variants. Lancet Reg Health Am. (2023) 18:100405. doi: 10.1016/j.lana.2022.100405
6. Cloete J, Kruger A, Masha M, du Plessis NM, Mawela D, Tshukudu M, et al. Paediatric hospitalisations due to COVID-19 during the first SARS-CoV-2 Omicron (B.1.1.529) variant wave in South Africa: a multicentre observational study. Lancet Child Adolesc Health. (2022) 6(5):294–302. doi: 10.1016/S2352-4642(22)00027-X
7. Khemiri H, Ayouni K, Triki H, Haddad-Boubaker S. SARS-CoV-2 infection in pediatric population before and during the Delta (B.1.617.2) and Omicron (B.1.1.529) variants era. Virol J. (2022) 19(1):144. doi: 10.1186/s12985-022-01873-4
8. Standard B. Covid cases in children rose in Omicron wave in Europe, shows data. (2022). Available at: https://www.business-standard.com/article/international/covid-cases-in-children-rose-in-omicron-wave-in-europe-shows-data-122031701297_1.html (Cited Apr 17, 2023).
9. Acker KP, Levine DA, Varghese M, Nash KA, RoyChoudhury A, Abramson EL, et al. Indications for hospitalization in children with SARS-CoV-2 infection during the Omicron wave in New York City. Children. (2022) 9(7):1043. doi: 10.3390/children9071043
10. Brewster RC, Parsons C, Laird-Gion J, Hilker S, Irwin M, Sommerschield A, et al. COVID-19-associated croup in children. Pediatrics. (2022) 149(6):e2022056492. doi: 10.1542/peds.2022-056492
11. Choi YY, Kim YS, Lee SY, Sim J, Choe YJ, Han MS. Croup as a manifestation of SARS-CoV-2 Omicron variant infection in young children. J Korean Med Sci. (2022) 37(20):e140. doi: 10.3346/jkms.2022.37.e140
12. Sharma S, Agha B, Delgado C, Walson K, Woods C, Gonzalez MD, et al. Croup associated with SARS-CoV-2: pediatric laryngotracheitis during the Omicron surge. J Pediatr Infect Dis Soc. (2022) 11(8):371–4. doi: 10.1093/jpids/piac032
13. Tunҫ EM, Koid Jia Shin C, Usoro E, Thomas-Smith SE, Trehan I, Migita RT, et al. Croup during the coronavirus disease 2019 Omicron variant surge. J Pediatr. (2022) 247:147–9. doi: 10.1016/j.jpeds.2022.05.006
14. Han MJ, Heo JH, Hwang JS, Jang YT, Lee M, Kim SJ. Incidence of febrile seizures in children with COVID-19. J Clin Med. (2023) 12(3):1076. doi: 10.3390/jcm12031076
15. Iijima H, Kubota M, Ogimi C. Change in seizure incidence in febrile children with COVID-19 in the era of Omicron variant of concern. J Pediatr Infect Dis Soc. (2022) 11(11):514–7. doi: 10.1093/jpids/piac085
16. Cadet K, Boegner J, Ceneviva GD, Thomas NJ, Krawiec C. Evaluation of febrile seizure diagnoses associated with COVID-19. J Child Neurol. (2022) 37(5):410–5. doi: 10.1177/08830738221086863
17. Leung AK, Hon KL, Leung TN. Febrile seizures: an overview. Drugs Context. (2018) 7:212536. doi: 10.7573/dic.212536
18. Delpisheh A, Veisani Y, Sayehmiri K, Fayyazi A. Febrile seizures: etiology, prevalence, and geographical variation. Iran J Child Neurol. (2014) 8(3):30–7.25143771
19. Kaputu Kalala Malu C, Mafuta Musalu E, Dubru JM, Leroy P, Tomat AM, Misson JP. Epidemiology and characteristics of febrile seizures in children. Rev Med Liege. (2013) 68(4):180–5.23755708
20. Berg AT, Shinnar S, Shapiro ED, Salomon ME, Crain EF, Hauser WA. Risk factors for a first febrile seizure: a matched case-control study. Epilepsia. (1995) 36(4):334–41. doi: 10.1111/j.1528-1157.1995.tb01006.x
21. Chung B, Wong V. Relationship between five common viruses and febrile seizure in children. Arch Dis Child. (2007) 92(7):589–93. doi: 10.1136/adc.2006.110221
22. Carman KB, Calik M, Karal Y, Isikay S, Kocak O, Ozcelik A, et al. Viral etiological causes of febrile seizures for respiratory pathogens (EFES study). Hum Vaccines Immunother. (2019) 15(2):496–502. doi: 10.1080/21645515.2018.1526588
23. Kukuruzovic M. 391 Febrile convulsions and influenza A or B- are there differences? Arch Dis Child. (2021) 106(Suppl 2):A164. doi: 10.1136/archdischild-2021-europaediatrics.391
24. Subcommittee on Febrile Seizures, American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. (2011) 127(2):389–94. doi: 10.1542/peds.2010-3318
25. Cloete J, Kruger A, Masha M, du Plessis NM, Mawela D, Tshukudu M, et al. Rapid rise in paediatric COVID-19 hospitalisations during the early stages of the omicron wave, Tshwane District, South Africa. medRxiv (2021). s2352-4642(22)00027-x:2021.12.21.21268108. doi: 10.1101/2021.12.21.21268108 Available at: https://www.medrxiv.org/content/10.1101/2021.12.21.21268108v1 (Cited April 26, 2023).
26. Joung J, Yang H, Choi YJ, Lee J, Ko Y. The impact of Omicron wave on pediatric febrile seizure. J Korean Med Sci. (2022) 38(3):e18. doi: 10.3346/jkms.2023.38.e18
27. Liu J, Liu M, Liang W. The dynamic COVID-zero strategy in China. China CDC Wkly. (2022) 4(4):74–5. doi: 10.46234/ccdcw2022.015
28. Chiu TGA, Leung WCY, Zhang Q, Lau EHY, Ho RWH, Chan HSS, et al. Changes in pediatric seizure-related emergency department attendances during COVID-19—a territory-wide observational study. J Formos Med Assoc. (2021) 120(8):1647–51. doi: 10.1016/j.jfma.2020.11.006
29. Poon MML, Byington E, Meng W, Kubota M, Matsumoto R, Grifoni A, et al. Heterogeneity of human anti-viral immunity shaped by virus, tissue, age, and sex. Cell Rep. (2021) 37(9):110071. doi: 10.1016/j.celrep.2021.110071
30. Taytard J, Prevost B, Schnuriger A, Aubertin G, Berdah L, Bitton L, et al. SARS-CoV-2 B.1.1.529 (Omicron) variant causes an unprecedented surge in children hospitalizations and distinct clinical presentation compared to the SARS-CoV-2 B.1.617.2 (Delta) variant. Front Pediatr. (2022) 10:932170. doi: 10.3389/fped.2022.932170
31. Margaretha L, Masloman N. Correlation between serum zinc level and simple febrile seizure in children. Paediatr Indones. (2010) 50(6):326–30. doi: 10.14238/pi50.6.2010.326-30
32. Leung AK, Robson WL. Febrile convulsions. How dangerous are they? Postgrad Med. (1991) 89(5):217–8. 221–2, 224. doi: 10.1080/00325481.1991.11700905
33. Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020 109(6):1088–95. doi: 10.1111/apa.15270
34. Waldmann V, Combes N, Narayanan K, Sharifzadehgan A, Bouzeman A, Beganton F, et al. Cough syncope. Am J Med. (2017) 130(7):e295–6. doi: 10.1016/j.amjmed.2017.01.050
35. Jarrett OO, Fatunde OJ, Osinusi K, Lagunju IA. Prevalence of bacteraemia amongst children with febrile seizures at the University College Hospital, Ibadan. Ann Ib Postgrad Med. 2018 16(2):170–3.31217776
36. Murakami H, Naraba H, Gondo T, Mochizuki M, Nakano H, Takahashi Y, et al. Diagnostic value of serum procalcitonin in patients with convulsion in emergency department, an observational study. Antibiotics. (2020) 9(10):683. doi: 10.3390/antibiotics9100683
37. Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet Lond Engl. (1993) 341(8844):515–8. doi: 10.1016/0140-6736(93)90277-N
38. Maruna P, Nedelníková K, Gürlich R. Physiology and genetics of procalcitonin. Physiol Res. (2000) 49(Suppl 1):S57–61.10984072
39. Dandona P, Nix D, Wilson MF, Aljada A, Love J, Assicot M, et al. Procalcitonin increase after endotoxin injection in normal subjects. J Clin Endocrinol Metab. (1994) 79(6):1605–8. doi: 10.1210/jcem.79.6.7989463
40. Abbasi E, Ghazavi A, Firoozi A. Comparison of laboratory parameters in children admitted with febrile seizures and fever without localized sign in Urmia Motahari Hospital, Iran, 2015 until 2020. Med J Tabriz Univ Med Sci. (2022) 44(1):47–54. doi: 10.34172/mj.2022.013
41. Pisacane A, Sansone R, Impagliazzo N, Coppola A, Rolando P, D'Apuzzo A, et al. Iron deficiency anaemia and febrile convulsions: case-control study in children under 2 years. BMJ. (1996) 313(7053):343. doi: 10.1136/bmj.313.7053.343
43. Yousefichaijan P, Eghbali A, Rafeie M, Sharafkhah M, Zolfi M, Firouzifar M. The relationship between iron deficiency anemia and simple febrile convulsion in children. J Pediatr Neurosci. (2014) 9(2):110–4. doi: 10.4103/1817-1745.139276
44. Liu Z, Li X, Zhang M, Huang X, Bai J, Pan Z, et al. The role of mean platelet volume/platelet count ratio and neutrophil to lymphocyte ratio on the risk of febrile seizure. Sci Rep. (2018) 8:15123. doi: 10.1038/s41598-018-33373-3
45. Gontko-Romanowska K, Żaba Z, Panieński P, Steinborn B, Szemień M, Łukasik-Głębocka M, et al. The assessment of laboratory parameters in children with fever and febrile seizures. Brain Behav. (2017) 7(7):e00720. doi: 10.1002/brb3.720
46. Taylor K, Jones EB. Adult dehydration. StatPearls. Treasure Island, FL: StatPearls Publishing (2023). Available at: http://www.ncbi.nlm.nih.gov/books/NBK555956/ (Cited April 29, 2023).
47. Miyagi Y, Sasano T, Kato H, Kin K. Hyponatremia and recurrent febrile seizures during febrile episodes: a meta-analysis. Cureus. (2022) 14(4):e24398. doi: 10.7759/cureus.24398
48. Yousefichaijan P, Dorreh F, Abbasian L, Pakniyat AG. Assessing the prevalence distribution of abnormal laboratory tests in patients with simple febrile seizure. J Pediatr Neurosci. (2015) 10(2):93–7. doi: 10.4103/1817-1745.159180
Keywords: febrile seizure, SARS-CoV-2, children, Omicron variant, COVID policy
Citation: Mohamed ZA, Tang C, Thokerunga E, Deng Y and Fan J (2023) Pediatric infection with the Omicron variant increases the risks of febrile seizures among COVID-19 infected children. Front. Pediatr. 11:1226403. doi: 10.3389/fped.2023.1226403
Received: 23 May 2023; Accepted: 7 August 2023;
Published: 17 August 2023.
Edited by:
Cristina Calvo, Hospital Infantil La Paz, SpainReviewed by:
Fatih Akın, Necmettin Erbakan University, Türkiye© 2023 Mohamed, Tang, Thokerunga, Deng and Fan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Youping Deng ZGVuZ3lwQHdodS5lZHUuY24= Jingyi Fan amZhbkB3aHUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.