
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 13 June 2023
Sec. Genetics of Common and Rare Diseases
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1184529
This article is part of the Research TopicInsights in Genetics of Common and Rare Diseases: 2022View all 14 articles
 Vega-Hanna Lourdes1
Vega-Hanna Lourdes1 Sanz-Cuesta Mario2Casas-Alba Didac3,4Bolasell Mercè3Martorell Loreto3Pías Leticia3,4Feller Ana Lucia5Antonio Federico Martínez-Monseny3*Serrano Mercedes4,6
Sanz-Cuesta Mario2Casas-Alba Didac3,4Bolasell Mercè3Martorell Loreto3Pías Leticia3,4Feller Ana Lucia5Antonio Federico Martínez-Monseny3*Serrano Mercedes4,6
Introduction: Sotos Syndrome (SS, OMIM#117550) is a heterogeneous genetic condition, recognized by three main clinical features present in most cases: overgrowth with macrocephaly, typical facial appearance and different degrees of intellectual disability. Three different types are described caused by variants or deletions/duplications in NSD1, NFIX and APC2 genes. We aimed to describe a cohort of pediatric patients reporting the typical and unexpected findings in order to expand the phenotype of this syndrome and trying to find genotype-phenotype correlations.
Methods: In our referral center, we collected and analyzed clinical and genetic data of 31-patients cohort diagnosed with SS.
Results: All of them presented with overgrowth, typical dysmorphic features and different degree of developmental delay. Although structural cardiac defects have been reported in SS, non-structural diseases such as pericarditis were outstanding in our cohort. Moreover, we described here novel oncological malignancies not previously linked to SS such as splenic hamartoma, retinal melanocytoma and acute lymphocytic leukemia. Finally, five patients suffered from recurrent onychocryptosis that required surgical procedures, as an unreported prevalent medical condition.
Discussion: This is the first study focusing on multiple atypical symptoms in SS at the time that revisits the spectrum of clinical and molecular basis of this heterogeneous entity trying to unravel a genotype-phenotype correlation.
Sotos Syndrome (SS, OMIM#117550) is a heterogeneous genetic condition, recognized by three main clinical features present in most cases: overgrowth, defined as height and/or head circumference at least two standard deviations above the mean; typical facial appearance and different degrees of intellectual disability. Indeed, SS is the most frequent genetic cause of overgrowth, with an estimated incidence of 1/14.000 live births (1–3).
More than 90% of the patients present an autosomal dominant deletion or variant in the Nuclear Receptor SET Domain–containing protein 1 (NSD1) gene, located at chromosome 5q35, encodes a histone methyltransferase that catalyzes the transfer of methyl groups to lysine residues of histone tails: more specifically lysine residue 36 of histone H3 (H3K36) and less frequently lysine residue 20 of histone H4 (H4K20) (4). These methylation marks are most frequently associated with transcriptional activation but can be associated with repression depending on the cellular context (5). Loss of function experiments in animal models revealed that NSD1 is essential for normal development and has been confirmed to also play an important role in human developmental syndromes, such as SS, as well as in different types of malignancies (6–10).
Other causes may correspond to variants in the recently described NFIX or APC2 genes (located on chromosome 19p13) that explain SS type two (also called Malan syndrome) and SS type three (11–13). There are also other syndromes characterized by overgrowth, mainly Tatton-Brown-Rahman Syndrome, Weaver Syndrome, or Sotos-like Syndrome, caused by variants in DNMT3A, EZH2, and SETD2 genes, respectively (14, 15).
The typical overgrowth pattern of SS starts prenatally, where patients may have higher mean birth length, weight, and head circumference, but contrarily, many reach adulthood with a height within the upper normal range. Hypotonia, feeding difficulties, hypoglycemia, and neonatal jaundice are also commonly found during the perinatal period (16–18).
SS dysmorphic features include macrocephaly and dolichocephaly, frontal bossing, high anterior hairline, down-slanted palpebral fissures, high arched palate, pointed and triangular chin, and large hands and feet. Clinically, SS patients may present neurodevelopmental delays associated with learning and behavior problems, attention deficit with hyperactivity, and socialization disturbances with autistic traits (19–23). Other complications include epilepsy, impaired vision and hearing, cardiac, urinary, and orthopedic defects, recurrent infections, and increased oncological risk (5, 24).
In this work, we aimed to describe a cohort of pediatric patients diagnosed with SS, focusing on the unreported medical complications, and expanding the clinical and genetic profile of the syndrome. We reevaluate the possibility of un-described phenotype-genotype correlations.
We conducted a descriptive, observational, and ambispective study. We included patients according to the following criteria: pediatric patients (between 2 and 18 years at the time of diagnosis) with a confirmed molecular diagnosis of SS attended at a tertiary hospital [Hospital Sant Joan de Déu (HSJD), Barcelona Spain] between January 2012 and July 2020.
We analyzed the medical records of a total of 31 pediatric patients. Information on clinical characteristics and complementary exams was analyzed. Adolescence was considered between 10 and 19 years of age, according to the World Health Organization definition.
Parents or legal representatives gave their written informed consent, and children/adolescents gave their assent. Blood samples were obtained in accordance with the Declaration of Helsinki revised in 2013.
In most patients (particularly the older individuals who underwent previous study protocols), genetic screening was performed using either Multiple Ligation Probe Assay (MLPA) or Array-CGH to search Deletions/Duplications of NSD1 and NFIX genes. In many patients (with negative MLPA/Array-CGH or those more recently enrolled) Sanger studies or clinical exome sequencing and subsequent confirmation and segregation of variants with Sanger sequencing was performed. All variants resulted de novo.
SALSA MLPA Probemix P026-E2 Sotos (MRC-Holland) has one probe for each one of the 23 exons from NSD1 and the 10 exons of NFIX genes and allowed us to detect any alteration at the exon level.
Array-CGH analysis was performed using a comparative genomic hybridization oligonucleotide microarray (qChipCM, 8 × 60 K; qGenomics). The submitted sample was hybridized against a commercial reference DNA of the same sex (Agilent Technologies). The quality of the data obtained was evaluated following the manufacturer's recommendations.
Primers used for sanger sequencing were designed with Primer3 program (httP://bioinfo.ut.ee/primer3/ analysis was performed by comparison with the reference sequence for NSD1 (NM_0022455.5).
Exome sequencing of the coding regions (exons, and 25 bp intronic regions flanking the exon) of 6,710 genes associated with pathology according to the Human Gene Mutation Database (HGMD), GeneTest.org, and the Online Mendelian Inheritance in Man catalog (OMIM) was performed. Next-generation sequencing (NGS) techniques were employed using enrichment by hybridization in solution with an Illumina design kit (TruSight One Sequencing Panel) and subsequent sequencing on an Illumina NextSeq500 sequencer. The bioinformatic analysis for the exome data was carried out using a pipeline developed in the bioinformatics unit within our hospital.
Once the SS diagnosis is established, the follow up of these patients consists of a once per year visit in a multidisciplinary visit including genetics and neuropediatrics. During these follow-ups, a detailed physical examination is performed, which includes anthropometric measurements, dysmorphologic descriptions, and back examinations for scoliosis. Additionally, endocrinology visits are appointed biannually, and oncological assessments are performed by specialists when the genetic diagnostic is confirmed. All the families have the contact of a patient manager, in case any health complication or necessity appears.
Since other comorbidities need to be ruled out at the time of diagnosis and during the follow up, an echocardiogram and renal ultrasound tests are routinely performed. Individuals are also systematically, referred for an audiology assessment.
Descriptive analyses were performed using univariate (Chi squared tests corrected by Pearson and Fisher's exact tests). Two-sided tests yielding a p < 0.05 was considered statistically significant. SPSS statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA) was used to perform all statistical analysis.
The study protocol was reviewed and approved by the Research & Ethics Committee of the Hospital Sant Joan de Déu, Barcelona, Spain (Project Internal Code PIC-08-19). The study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practices, and applicable regulatory requirements. All parents and adult patients provided written informed consent, and adolescent patients able to understand the procedure gave their assent prior to patient enrollment.
We analyzed 31 patients (16 males and 15 females) between 2 and 25 years of age (12.9 ± 5.9) in the last evaluation. The mean age at diagnosis was 8.0 (±5.9) years with a mean follow up time of 8.8 (±5.3) years. The clinical data of our cohort is described in Table 1 and Supplementary Table S1.
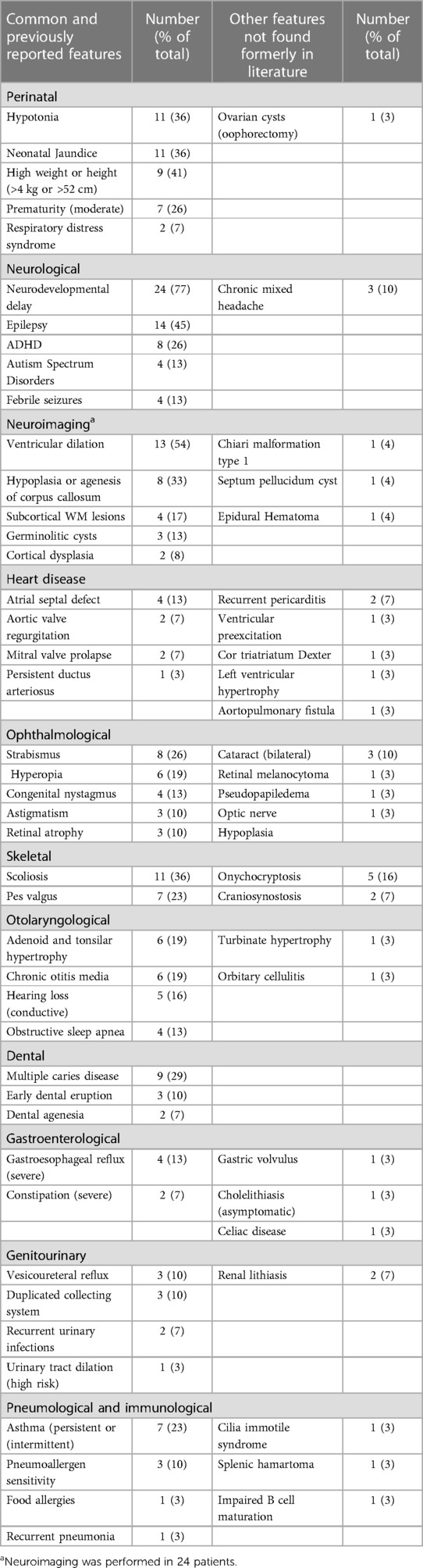
Table 1. Common features and other features not found in literature.
Out of all patients, 27 (87%) corresponded to variants of the NSD1 gene, with 18 point variants (5 missense and 13 truncating), 7 deletions, and 2 duplications (Figure 1). There were 4 patients who presented variants of the NFX1 gene, with 2 missense variants, 1 deletion, and 1 duplication. The description of the genetic variants identified in each patient are stated in Table 2.
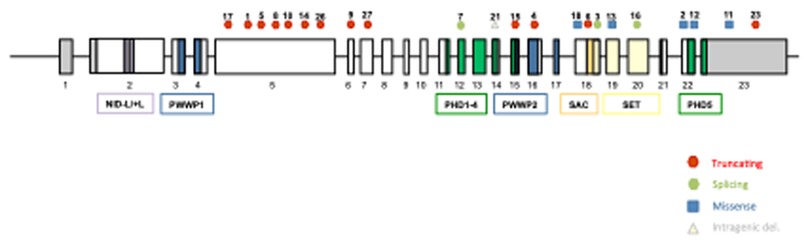
Figure 1. Schematic representation of NSD1 gene, showing the localization of the variants described in our cohort. All 23 exons of NSD1 are presented by boxes and introns are represented by lines. The domains of NSD1 are represented with different colored boxes. NSD1 contain two nuclear receptor interacting domains (NID), two proline-tryptophan-tryptophan-proline (PWWP), five plant homeodomain zinc fingers (PHD), the catalytic Su(var)3–9, enhancer-of-zeste, Trithorax (SET) and the C-terminal C5HCH (Cys-His) domain (SAC). Missense variants are represented with blue squares, truncating variants with red circles, intragenic deletions with yellow triangles and splicing variants with green circles.
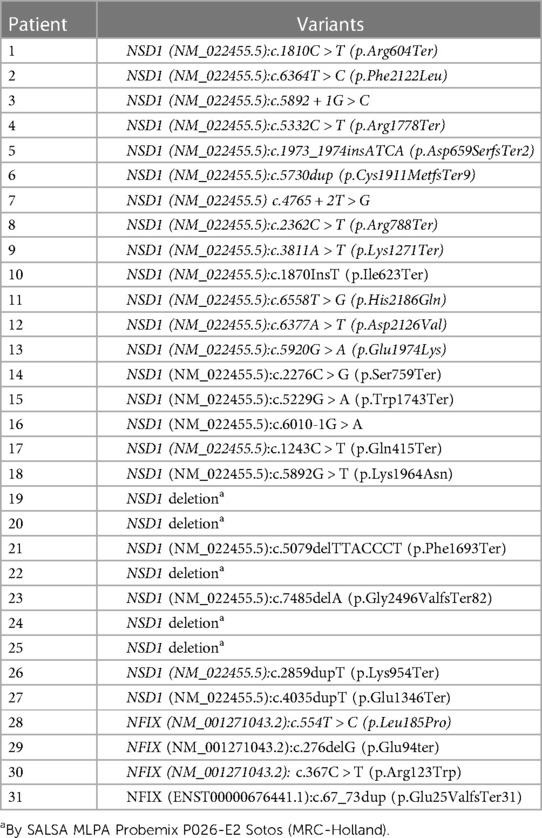
Table 2. Description of the genetic variants identified in each patient.
Hypotonia and neonatal jaundice were observed in a third of the individuals, showing a significant difference in those premature patients (p = 0.049 and p = 0.003 respectively). Only 12.9% presented feeding difficulties, being more prevalent in females (p = 0.043) and in patients with NFIX variants (p = 0.003). Seven subjects were born moderately preterm (Table 1).
High birth length (>52 cm) and weight (>4 Kg) was observed in 40.9% of the patients. A pronounced subsequent postnatal growth (at least 2 SD above the mean) was maintained in almost half of the patients. Macrocephaly (at least 2 SD above the mean) was present in 50% of the patients.
A characteristic facial appearance consisting of a high and broad forehead, sparse frontotemporal hair, downslanted palpebral fissures, malar flushing, and a pointed chin was present in all patients. Three patients presented microretrognathia and one patient presented facial asymmetry.
Psychomotor delay and a varying range of intellectual disability were observed in most patients (77.4%). As neurological comorbidities, epileptic seizures were found in almost half of the sample (45.2%), of which nine patients required medical treatment: valproic acid (VPA) in three patients; levetiracetam (LEV) and topiramate (TPM) both in one patient each; and associations of VPA plus LEV and VPA plus vigabatrin (VGB), both in two patients, respectively. Two patients suffered from simple febrile seizures, not followed by epilepsy.
In terms of behavioral disorders, attention-deficit hyperactivity disorder (ADHD) was diagnosed in eight patients (25.8%) and socialization difficulties were evident in seven patients (22.6%), including four with severe autism spectrum disorder (ASD) (12.9%). This last diagnosis was more prevalent in male patients (p = 0.05).
Meanwhile, other comorbidities such as impulsive behavior and anxiety disorder were diagnosed in 11 patients (35.5%), being the latter more prevalent in teenagers and young adults (p = 0.01).
No genetic correlations were identified between variants, affected genes, and the presence of epilepsy or behavioral disorders.
Regarding heart disease, 13 patients (41.9%) were diagnosed with some form of it. Cardiac structural defects were the most frequent (38.7%) (Table 1), and patients with hypotonia at birth were at increased risk of developing them (p = 0.042). These included atrial septal defects and persistent ductus arteriosus, observed in four patients, one of which was a preterm baby. Other findings included the diagnosis of mitral valve prolapse, cor triatriatum dexter, and left ventricle hypertrophy.
Two patients presented recurrent pericarditis with pericardial effusion (Figure 2). Clinical presentation started with a viral infection as a trigger leading to pericarditis without positive evidence of infectious or rheumatic etiology. These patients underwent multiple relapses and ended up depending on chronic immunosuppressant therapy (corticosteroid therapy). Both cases of pericarditis were detected in patients with NSD1 affectations. One of them presented an NSD1 deletion, and the other one a nonsense variant in the same gene NSD1:c.3811A > T (p.Lys1271Ter).
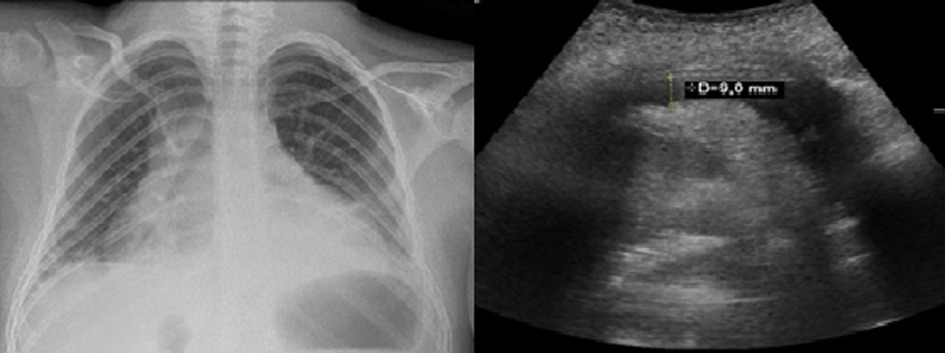
Figure 2. Pericardial effusion. Left: Thorax radiography showing cardiomegaly. Right: echocardiogram of patient with pericardial effusion of 9 mm.
Arrhythmia was detected in one patient, which was further diagnosed with ventricular preexcitation without paroxysmal tachycardia. There was no statistically significant correlation between the presence of heart disease (structural or not) and molecular findings.
Twenty-two patients (71%) presented ophthalmological disorders, including strabismus (eight patients) and refractive defects (hyperopia in six patients and astigmatism in three patients) as the most prevalent. Congenital nystagmus affected four patients. Moreover, three patients showed bilateral cataracts that needed surgery during the first months of life, and three developed retinal atrophy. One subject presented a retinal melanocytoma, explained in the oncological findings section.
Chronic otitis media leading to conductive hearing loss and adenoid and tonsil hypertrophy were the most prevalent diseases, both in six patients. Four of the subjects suffered from apnea-hypopnea syndrome, due to adenoid and tonsil hypertrophy or microretrognathia, plus the hypotonic muscle tone. Two patients presented cholesteatoma, one of them associated with hypoacusis. Both patients required surgical intervention.
The most frequent skeletal finding in our cohort was scoliosis, present in 11 patients (35.5%), two of them required surgical intervention. Pes valgus was observed in seven patients (22.6%). Five patients (16.1%) suffered from recurrent onychocryptosis needing surgical procedures due to the lack of improvement with conservative treatment.
Eight patients (25.8%) suffered from genitourinary pathology including urinary tract dilation, duplicated collecting system, renal dysplasia/hypoplasia, or renal agenesis. Unilateral cryptorchidism was reported in two patients. One child suffered from hydrocele testicle and needed surgical treatment. One boy presented idiopathic precocious puberty without abnormalities at the sellar and suprasellar regions in neuroimaging.
Within our cohort, we identified three different oncological presentations. One case of splenic hamartoma (Figure 3), diagnosed at seven years of age, in a routine study that remained stable in subsequent controls; one case of retinal melanocytoma, diagnosed at one year of age, showing spontaneous involution; and one case of acute lymphocytic leukemia diagnosed at 14 years of age, to whom chemotherapy treatment is currently ongoing. Missense variants in the NSD1 gene were drivers of increased oncological malignancies compared to NFIX alterations (p = 0.049) in our cohort.
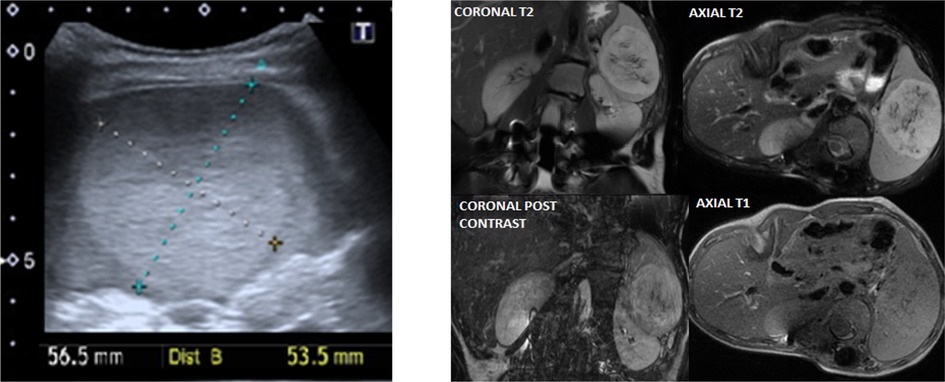
Figure 3. Splenic hamartoma clinical imaging. Left panel: Ultrasound of a patient with well-defined splenic solid mass, 5.7 × 5.4 centimeters, isoechoic, with calcifications dotted inside. Right panel: MRI imaging of the same patient that shows stable mass of 7.2 × 5.9 × 6.9 cm, hyperintense in T2, isointense in T1, without fat, with enhancement in small hemorrhagic areas.
SS is a rare genetic disorder characterized by a range of features, which have mainly been described in adult populations and small pediatric cohorts with overgrowth syndromes. In this study, we aim to provide a comprehensive description of the typical and atypical findings in a large cohort of pediatric patients with SS, all followed in the same center.
Regarding the conventional and extensively documented observations, the prevailing feature observed in all patients was the distinct facial appearance. While macrocephaly is commonly regarded as a hallmark symptom of SS, it was only detected in half of our patient cohort. Nonetheless, the particular skull shape was also observed in the non-macrocephalic subjects, pointing towards SS as a potential diagnosis.
There were no specific remarkable perinatal findings. Mild prematurity, neonatal jaundice, and perinatal global hypotonia are frequently found in SS individuals and may rise the suspicion of a genetic condition. Contrarily, hypoglycemia was not as frequent as expected.
As for neurological assessment, neurodevelopment delay was present in 77.4% of the sample. Classically, SS patients reported in the literature always presented with intellectual disability. For example, some studies found that 5q35 microdeletions are linked with lower scores in cognitive, adaptive functioning, and behavioral domains (25). However, other studies are starting to show a varying range of cognitive ability and some patients can be found within a normal cognitive range (18, 21).
In our sample, the range of intellectual difficulties is also wide, with many patients attending normal schooling with some subject adaptations. ADHD has been reported as a very prevalent neurodevelopmental disorder in this population (19) and probably is underdiagnosed in our cohort since the coexistence of intellectual disability and ADHD traits may complicate the diagnosis.
The present study reveals a notable prevalence of ASD traits in our sample, despite not meeting all of the classical criteria for ASD. This finding is consistent with previous reports in the literature (19–22). Again, the coexistence of a typical behavioral phenotype with traits of other neurodevelopmental conditions (perhaps not fulfilling the classical criteria), complicates the diagnosis. However, particular recognition and correct management of ADHD and ASD may have a relevant impact on the patient's development, including academic achievements, social inclusion, but also the quality of their home life.
Regarding behavioral issues, tantrums and anxiety were found to be the most prevalent. The behavioral disturbances observed may be attributed, in part, to the characteristics of ADHD and ASD, such as impulsiveness, rigidity, and social difficulties. In view of our results and the impact on patients' and families' wellbeing, guidelines need to include mental health experts (both psychologists and psychiatrists) implied in the assessment and follow-up of this group of patients. Regarding epilepsy, in concordance with the literature (5, 26), presented in half of our patients and was well controlled with antiepileptic drugs, mostly in monotherapy. None of the patients presented neurological regression due to uncontrolled epilepsy. The presence of febrile seizures was not related to subsequent epilepsy.
In our study, we wanted to take a holistic view of SS by considering a wide array of comorbidities and make an exhaustive analysis to expand the clinical phenotype. Subsequently, we have identified a series of characteristics linked to SS in our cohort, rarely described in the literature. One such characteristic is the presence of recurrent pericarditis or arrhythmias.
According to established studies, between 20% and 50% of SS patients may present with cardiac defects (27), but these usually include septal or valvular defects.
In our cohort, two patients exhibited recurring pericarditis, which manifested at comparable ages (nine and ten years old) and with similar clinical presentations (associated with viral infection triggers, multiple relapses, and dependence on corticosteroid treatment). Despite the patients' similar presentations, infectious and rheumatologic etiologies were ruled out. Recently, one study reported pericarditis in a patient with SS, which was observed in the context of SARS-CoV-2 infection, highlighting SS as a potential risk factor for this condition during viral infections (28). Therefore, the possibility of recurrent idiopathic pericarditis and the benefit of corticosteroid treatment should be considered in SS patients.
In addition, there have been infrequent reports of arrhythmogenic mechanisms. In a study by Segreti et al., a Brugada syndrome was identified in a patient with SS (29). Similarly, Sharma et al. reported a case of overgrowth and dysmorphic features in a patient with Wolff Parkinson White Syndrome (WPWS) in 2003, even though no genetic findings were reported, and SS was not formally diagnosed (30). In our own cohort, we have also observed a comparable form of arrhythmia, suggesting a potential underlying mechanism that warrants further investigation in future studies.
The increased oncological risks afflicting SS patients are of great concern to geneticists, pediatricians, oncologists, and families. Somatic variants affecting NSD1 have been identified in various types of tumors, suggesting a potential tumor suppressing role (31). Tauchmann et al. recently reviewed the role and molecular functions of NSD1, in which it is shown to be widely expressed in different tissues, playing an important role in human developmental syndromes, such as SS, as well as in different types of malignancies (32, 33).
Indeed, the genetic profile of SS has great repercussions on the clinical presentation of these patients. In our study, we found a correlation between oncological risk and missense NSD1. Future studies to understand the functional involvement of these variants and the role of NSD1 would be of great interest. Most of the reported malignancies in SS have been solid tumors, such as Wilms tumor, hepatocarcinoma, neuroectodermal tumor, small cell lung carcinoma, teratomas, and neuroblastoma. However, other malignancies, including lymphoproliferative disorders such as acute lymphoblastic leukemia, B-cell lymphoblastic lymphoma, and other non-Hodgkin lymphomas, have also been reported (34, 35).
In our cohort, two patients presented solid tumors: one of them corresponds to a stable splenic hamartoma, and another one presented a retinal melanocytoma as a finding on ocular examination, asymptomatic at the time of diagnosis. None of these tumors had been previously described in SS.
Interestingly, although with less involvement in the severity of the disease but potentially very afflictive, five patients presented onychocryptosis, not previously associated with this pathological entity. Particular nail care may be useful to prevent this outstanding complication in our cohort, probably explained by distal phalanx or nail malformations or connective tissue anomalies.
Since it is difficult to determine if these atypical findings are sporadic or clearly secondary to SS, we recommend increasing awareness among physicians, annotating and reporting them. Associating these new phenotypes with the wider SS clinical spectrum should be considered.
Future descriptions are needed on this issue in order to expand the specific follow-up protocols. What does seem mandatory is the need for a multidisciplinary approach to patients with SS.
This study deepens in the already known phenotype but also considers multiple atypical findings that may have been not described but are probably frequent and relevant in SS. Remarkably recurrent pericarditis, onychocryptosis, and unusual malignancies were found in our large pediatric sample indicating that multidisciplinary and comprehensive follow-up recommendations are needed. The clinical and molecular spectrum of SS in this sample is described in detail, highlighting the importance of continuously revisiting and expanding the phenotype and genotype of rare diseases, as well as, exploring the possible correlations among them. Unfortunately, we were not able to establish a clear correlation between phenotype and genotype. However, we found that ASD is more frequently diagnosed in males than in females; contrarily feeding disorders are more prevalent in females. NFIX patients had more prevalent feeding disorders but fewer malignancies than NSD1 patients. The findings of this study can aid in directing follow-up, screening for associated comorbidities, and assessing newly described health complications. Overall, this study emphasizes the need for continued research into rare diseases to better understand their clinical and molecular characteristics, revisit and redesign follow-up guidelines, and, as a final goal, improve patients' and families’ outcomes and wellbeing.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Research & Ethics Committee of the Hospital Sant Joan de Déu, Barcelona, Spain (the internat evaluation code PIC-08-19). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
V-HL visited patients, coordinated and contributed to the data extraction, wrote mostly the manuscript and provided feedback on the report. S-CM contributed to data extraction, helped write the manuscript and provided feedback on the report. C-AD, BM, PL, and FL visited patients, helped write the manuscript and provided feedback on the report. ML contributed to molecular studies. AM and SM visited patients, designed the study, coordinated the data extraction, helped write the manuscript and coordinated the manuscript revisions. All authors contributed to the article and approved the submitted version.
We thank the patients and families for their active participation in this study and the clinicians that recruited them.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1184529/full#supplementary-material
2. Cole TR, Hughes HE. Sotos syndrome: a study of the diagnostic criteria and natural history. J Med Genet. (1994) 31(1):20–32. doi: 10.1136/jmg.31.1.20
3. Ko JM. Genetic syndromes associated with overgrowth in childhood. Ann Pediatr Endocrinol Metab. (2013) 18(3):101–5. doi: 10.6065/apem.2013.18.3.101
4. Rayasam GV, Wendling O, Angrand PO, Mark M, Niederreither K, Song L, et al. NSD1 Is essential for early post-implantation development and has a catalytically active SET domain. EMBO J. (2003) 22(12):3153–63. doi: 10.1093/emboj/cdg288
5. Foster A, Zachariou A, Loveday C, Ashraf T, Blair E, Clayton-Smith J, et al. The phenotype of sotos syndrome in adulthood: a review of 44 individuals. Am J Med Genet C Semin Med Genet. (2019) 181(4):502–8. doi: 10.1002/ajmg.c.31738
6. Rio M, Clech L, Amiel J, Faivre L, Lyonnet S, Le Merrer M, et al. Spectrum of NSD1 mutations in sotos and weaver syndromes. J Med Genet. (2003) 40(6):436–40. doi: 10.1136/jmg.40.6.436
7. Waggoner DJ, Raca G, Welch K, Dempsey M, Anderes E, Ostrovnaya I, et al. NSD1 Analysis for sotos syndrome: insights and perspectives from the clinical laboratory. Genet Med. (2005) 7(8):524–33. doi: 10.1097/01.GIM.0000178503.15559.d3
8. Ha K, Anand P, Lee JA, Jones JR, Kim CA, Bertola DR, et al. Steric clash in the SET domain of histone methyltransferase NSD1 as a cause of sotos syndrome and its genetic heterogeneity in a Brazilian cohort. Genes (Basel). (2016) 7(11):96. doi: 10.3390/genes7110096
9. Berdasco M, Esteller M. Genetic syndromes caused by mutations in epigenetic genes. Hum Genet. (2013) 132(4):359–83. doi: 10.1007/s00439-013-1271-x
10. Choufani S, Cytrynbaum C, Chung BH, Turinsky AL, Grafodatskaya D, Chen YA, et al. NSD1 Mutations generate a genome-wide DNA methylation signature. Nat Commun. (2015) 6:10207. doi: 10.1038/ncomms10207
11. Türkmen S, Gillessen-Kaesbach G, Meinecke P, Albrecht B, Neumann LM, Hesse V, et al. Mutations in NSD1 are responsible for sotos syndrome, but are not a frequent finding in other overgrowth phenotypes. Eur J Hum Genet. (2003) 11(11):858–65. doi: 10.1038/sj.ejhg.5201050
12. Cecconi M, Forzano F, Milani D, Cavani S, Baldo C, Selicorni A, et al. Mutation analysis of the NSD1 gene in a group of 59 patients with congenital overgrowth. Am J Med Genet A. (2005) 134(3):247–53. doi: 10.1002/ajmg.a.30492
13. Tatton-Brown K, Douglas J, Coleman K, Baujat G, Chandler K, Clarke A, et al. Multiple mechanisms are implicated in the generation of 5q35 microdeletions in sotos syndrome. J Med Genet. (2005) 42(4):307–13. doi: 10.1136/jmg.2004.027755
14. Tatton-Brown K, Seal S, Ruark E, Harmer J, Ramsay E, Del Vecchio Duarte S, et al. Mutations in the DNA methyltransferase gene DNMT3A cause an overgrowth syndrome with intellectual disability. Nat Genet. (2014) 46(4):385–8. doi: 10.1038/ng.2917
15. Marzin P, Rondeau S, Aldinger KA, Alessandri JL, Isidor B, Heron D, et al. SETD2 Related overgrowth syndrome: presentation of four new patients and review of the literature. Am J Med Genet C Semin Med Genet. (2019) 181(4):509–18. doi: 10.1002/ajmg.c.31746
16. Douglas J, Tatton-Brown K, Coleman K, Guerrero S, Berg J, Cole TR, et al. Partial NSD1 deletions cause 5% of sotos syndrome and are readily identifiable by multiplex ligation dependent probe amplification. J Med Genet. (2005) 42(9):e56. doi: 10.1136/jmg.2005.031930
17. Priolo M, Schanze D, Tatton-Brown K, Mulder PA, Tenorio J, Kooblall K, et al. Further delineation of malan syndrome. Hum Mutat. (2018) 39(9):1226–37. doi: 10.1002/humu.23563
18. Tatton-Brown K, Rahman N. Clinical features of NSD1-positive sotos syndrome. Clin Dysmorphol. (2004) 13(4):199–204. doi: 10.1097/00019605-200410000-00001
19. Lane C, Milne E, Freeth M. Cognition and behaviour in sotos syndrome: a systematic review. PLoS One. (2016) 11(2):e0149189. doi: 10.1371/journal.pone.0149189
20. Harris JR, Fahrner JA. Disrupted epigenetics in the sotos syndrome neurobehavioral phenotype. Curr Opin Psychiatry. (2019) 32(2):55–9. doi: 10.1097/YCO.0000000000000481
21. Lane C, Milne E, Freeth M. The cognitive profile of sotos syndrome. J Neuropsychol. (2019) 13(2):240–52. doi: 10.1111/jnp.12146
22. Lane C, Milne E, Freeth M. Characteristics of autism spectrum disorder in sotos syndrome. J Autism Dev Disord. (2017) 47(1):135–43. doi: 10.1007/s10803-016-2941-z
23. Ball LJ, Sullivan MD, Dulany S, Stading K, Schaefer GB. Speech-language characteristics of children with sotos syndrome. Am J Med Genet A. (2005) 136A(4):363–7. doi: 10.1002/ajmg.a.30799
24. van Haelst MM, Hoogeboom JJ, Baujat G, Brüggenwirth HT, Van de Laar I, Coleman K, et al. Familial gigantism caused by an NSD1 mutation. Am J Med Genet A. (2005) 139(1):40–4. doi: 10.1002/ajmg.a.30973
25. Siracusano M, Riccioni A, Frattale I, Arturi L, Dante C, Galasso C, et al. Cognitive, adaptive and behavioral profile in sotos syndrome children with 5q35 microdeletion or intragenic variants. Am J Med Genet A. (2023). doi: 10.1002/ajmg.a.63211
26. Nicita F, Ruggieri M, Polizzi A, Mauceri L, Salpietro V, Briuglia S, et al. Seizures and epilepsy in sotos syndrome: analysis of 19 Caucasian patients with long-term follow-up. Epilepsia. (2012) 53(6):e102–5. doi: 10.1111/j.1528-1167.2012.03418.x
27. Letter to the Editor Congenital Heart Defects in Sotos Syndrome To the Editor. (1999) 172(November 1998):9670810.
28. Citoni B, Digilio MC, Capolino R, Gagliardi MG, Campana A, Drago F, et al. SARS-CoV-2 and pre-tamponade pericardial effusion. Could sotos syndrome be a major risk factor? Genes (Basel). (2021) 12(11):1782. doi: 10.3390/genes12111782
29. Segreti A, Piccirillo F, Crispino SP, Cocchia F, Martucciello A, Calabrese V, et al. Simultaneous presence of Brugada and overgrowth syndromes. Monaldi Arch Chest Dis. (2023). doi: 10.4081/monaldi.2023.2521
30. Sharma PP, Vidaillet H, Dietz J. Patient with sotos syndrome, Wolff-Parkinson-White pattern on electrocardiogram, and two right-sided accessory bypass tracts. Am J Med Genet A. (2003) 116A(4):372–5. doi: 10.1002/ajmg.a.10022
31. Villani A, Greer MC, Kalish JM, Nakagawara A, Nathanson KL, Pajtler KW, et al. Recommendations for cancer surveillance in individuals with RASopathies and other rare genetic conditions with increased cancer risk. Clin Cancer Res. (2017) 23(12):e83–e90. doi: 10.1158/1078-0432.CCR-17-0631
32. Brioude F, Toutain A, Giabicani E, Cottereau E, Cormier-Daire V, Netchine I. Overgrowth syndromes—clinical and molecular aspects and tumour risk. Nat Rev Endocrinol. (2019) 15(5):299–311. doi: 10.1038/s41574-019-0180-z
33. Tauchmann S, Schwaller J. NSD1: a lysine methyltransferase between developmental disorders and cancer. Life (Basel). (2021) 11(9):877. doi: 10.3390/life11090877
34. Al-Mulla N, Belgaumi AF, Teebi A. Cancer in sotos syndrome: report of a patient with acute myelocytic leukemia and review of the literature. J Pediatr Hematol Oncol. (2004) 26(3):204–8. doi: 10.1097/00043426-200403000-00013
Keywords: sotos syndrome, phenotype, overgrowth, NSD1, NFIX, APC2
Citation: Lourdes V-H, Mario S-C, Didac C-A, Mercè B, Loreto M, Leticia P, Lucia FA, Martínez-Monseny AF and Mercedes S (2023) Beyond the known phenotype of sotos syndrome: a 31-individuals cohort study. Front. Pediatr. 11:1184529. doi: 10.3389/fped.2023.1184529
Received: 11 March 2023; Accepted: 15 May 2023;
Published: 13 June 2023.
Edited by:
Jordi Pérez-Tur, Spanish National Research Council (CSIC), SpainReviewed by:
Aldesia Provenzano, University of Florence, Italy© 2023 Lourdes, Mario, Didac, Mercè, Loreto, Leticia, Lucia, Martínez-Monseny and Mercedes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Federico Martínez-Monseny YW50b25pb2ZlZGVyaWNvLm1hcnRpbmV6QHNqZC5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.