 Blandine Aubert†
Blandine Aubert† Manon Cadoux
Manon Cadoux Cyril Sahyoun
Cyril Sahyoun
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr., 30 May 2023
Sec. General Pediatrics and Pediatric Emergency Care
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1182899
Background: Subgaleal hematoma is a well-known life-threatening complication of instrumentation at birth. Even though most cases of subgaleal hematomas occur in the neonatal period, older children and adults are also at risk for subgaleal hematomas and their complications, following head trauma.
Objective: We hereby report the case of a 14-year-old boy who presented with a traumatic subgaleal hematoma requiring drainage and review the relevant literature regarding potential complications and indications for surgical intervention.
Results: Infection, airway compression, orbital compartment syndrome and anemia requiring transfusion are potential complications of subgaleal hematomas. Although rare, surgical drainage and embolization are occasionally required interventions.
Conclusion: Subgaleal hematomas following head trauma can occur in children beyond the neonatal period. Large hematomas may require drainage to relieve pain or when compressive or infectious complications are suspected. Although usually not life-threatening, physicians taking care of children must be cognizant of this entity when caring for a patient with a large hematoma following head trauma and in severe cases, consider a multidisciplinary approach.
Subgaleal hematomas occurs when blood accumulates between the periosteum and the aponeurosis due to the tearing of emissary veins. It is a known complication of instrumentation at birth, and neonates can have up to 50% of the body blood volume accumulate in the space, leading to hemorrhagic shock and death (1, 2). Even though most cases of subgaleal hematomas occur in the neonatal period, older children and adults are also at-risk following head trauma. In this report, and we hereby report the case of a 14-year-old child who presented with a traumatic subgaleal hematoma with worsening headache and without hemodynamic instability, requiring drainage and review the available literature on the topic.
A 14-year-old otherwise healthy boy was brought to the pediatric emergency department (PED) of a tertiary care urban medical center by his parents 3 days after sustaining a skateboarding injury. The patient reports falling directly on his head from his height, striking the top of his head on the halfpipe cement structure of the skatepark, while not wearing a helmet. He denies loss of consciousness, nausea, vomiting, abnormal behavior, or any other injury at the time and did not seek medical consultation. He has however since complained of a progressively worsening headache when moving his head from side to side and felt a lump on the frontoparietal part of his head. With the headache becoming severe, the patient and his family decided to seek care in the PED.
Vital signs revealed a normal heart rate of 80 beats per min, a slightly elevated blood pressure of 133/90 mmHg, a normal respiratory rate of 16 per min, normal oxygen saturation at 98% in ambient air, and no fever. The patient appeared well, was alert, interactive and conversive, he complained of mild discomfort at rest but pain that is difficult to tolerate when ambulating, particularly when moving his head from side to side. On inspection, a large area of fluctuant swelling on the right frontoparietal region of the scalp was noted, which was painful to palpation. The remainder of the examination including the neurological examination showed no abnormalities.
Given the suspicion for an underlying skull fracture and given the severity of the headache, the decision was made to obtain a non-contrast computed tomography (CT) of the head. CT revealed no evidence of intracranial hemorrhage, intracranial hypertension, or skull fracture, and confirmed the diagnosis of a right voluminous frontoparietal subgaleal hematoma extending to the left frontal region (Figure 1).
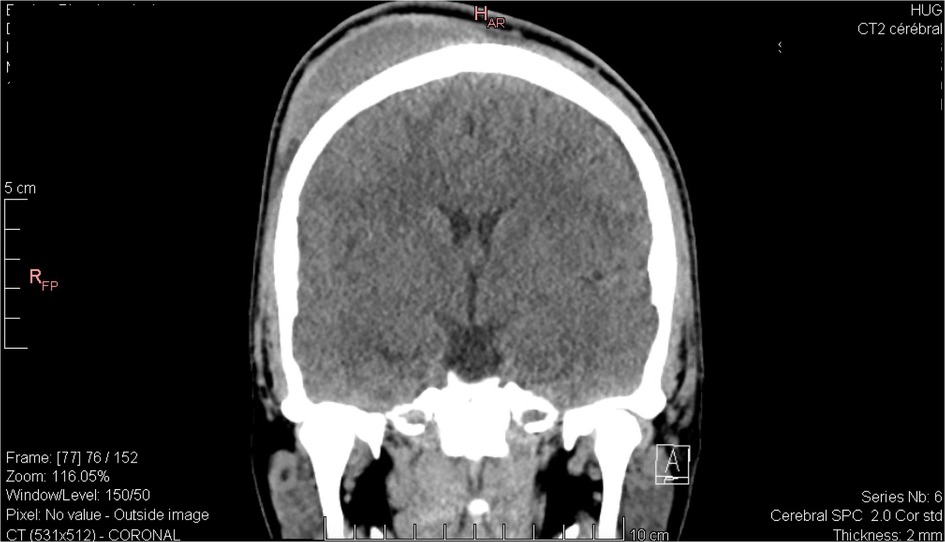
Figure 1. Coronal view of the head computed tomography scan revealing a large right-sided subgaleal hematoma.
Laboratory examination showed normal coagulation studies and no thrombocytopenia. Neurosurgical consultation was obtained to help guide management, and given the severity of the headache, the decision was made to drain the collection. Bedside needle drainage was performed by the neurosurgeon in the PED, with insertion of a butterfly needle in sterile conditions and aspiration of 100 cc of blood, followed by application of a compression bandage. The patient was subsequently discharged from the PED with a follow up appointment with his pediatrician.
The compression bandage was kept for 48 h, and headaches resolved in that timeframe. There were no other symptoms in the days and weeks following his admission to the PED. No further analgesia was needed, and the swelling progressively decreased then completely resolved over the course of 3 weeks, as documented by a telephone conversation with the patient and his family.
Subgaleal hematoma is a complication known to pediatricians attending the delivery room. The condition is much rarer in older children. The patient described above presented with severe pain from a traumatic subgaleal hematoma, improved with needle drainage, and had no further complications.
We searched PubMed for articles published in the last forty years in English with the title containing “subgaleal hematoma,” with available abstracts and accessible full-texts, and retained only the ones involving otherwise healthy children outside of the neonatal period. Our literature review reveals that the main reasons for subgaleal hematomas in children are minor head injury, hair pulling or braiding and trauma leading to a skull fracture. Reports of child abuse with hair pulling, hair braiding or corporal punishment leading to subgaleal hematoma are also described (Table 1).
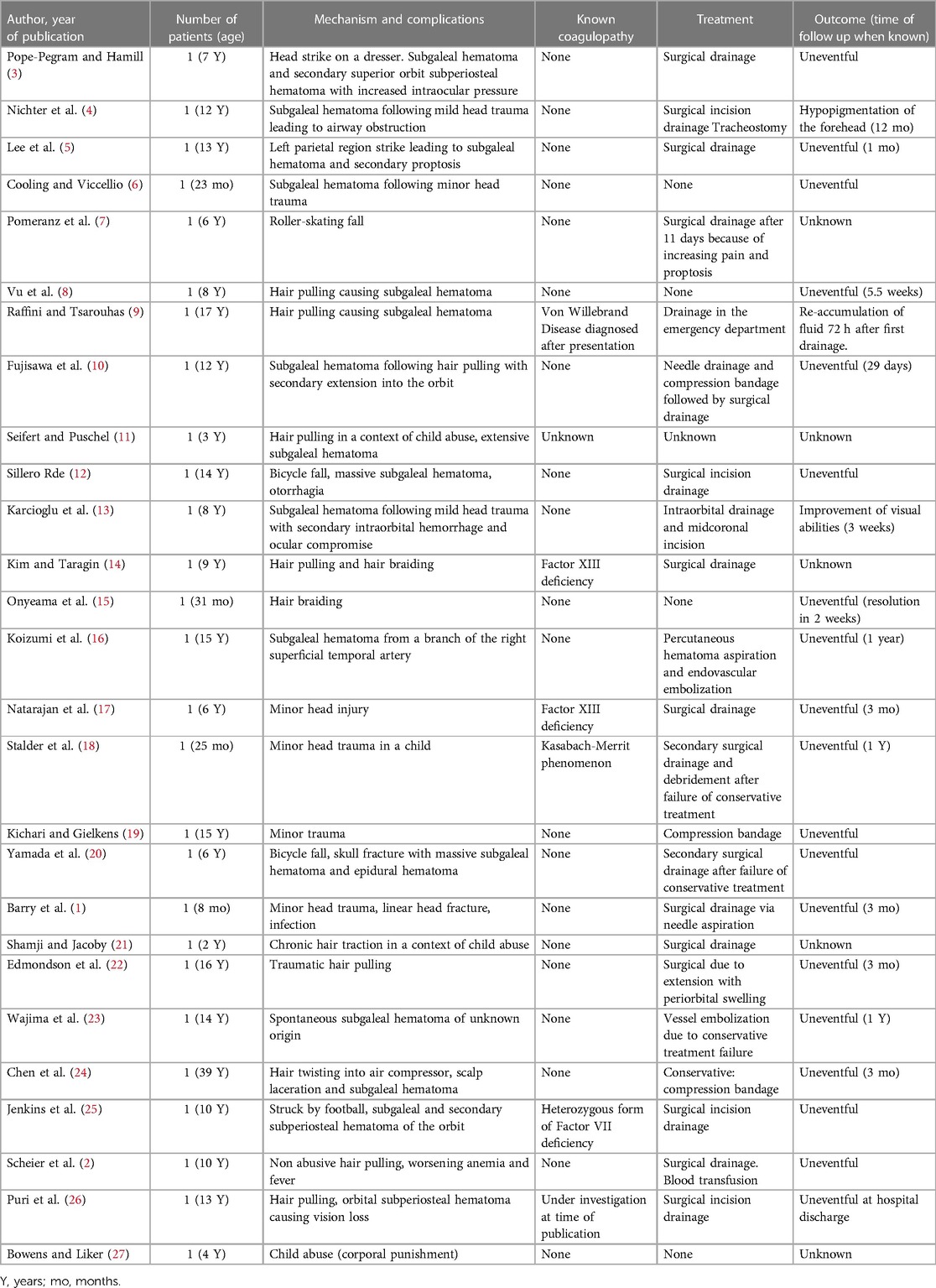
Table 1. Literature review and outcome summary of relevant publications related to pediatric subgaleal hematoma.
Intervening on a subgaleal hematoma is rarely needed in children. The symptoms of pain and swelling usually resolve within a few days to weeks after the injury and drainage is rarely necessary. The usual work up performed includes complete blood count looking for thrombocytopenia and coagulation profiles looking for a bleeding diathesis (9, 14, 17, 25).
We hereby discuss the potential complications of traumatic subgaleal hematomas and related interventions.
Airway compression is a rare complication of a traumatic subgaleal hematoma. Nichter et al. describe a 12-year-old healthy child who suffered a mild blow to the head leading to a massive hematoma of the head and neck resulting in airway compression. Emergency tracheostomy and surgical drainage was required, with concern for impending skin necrosis (4). In their report, the mechanism leading to the massive swelling remained unclear, but the hypothesis was that the attachment of the galea to the zygomatic arch can be delicate and a large hematoma could cross this boundary. The patient described in their report had a favorable outcome at twelve months follow up with only spotty hypopigmentation in the forehead region.
Orbital compartment syndrome has also been described as a complication of subgaleal hematoma, with extension of the hematoma to the orbital subperiosteum (3, 5, 7, 10, 13, 19, 25, 26). Patients usually present with a history of head trauma and progressive exophthalmia, blurred vision, ptosis, and pain. In such cases, prompt surgical drainage of the hematoma may be required, as blindness secondary to increased intraocular pressure is a possible outcome of untreated orbital compartment syndrome.
Infection of subgaleal hematomas secondary to a scalp laceration during instrumented delivery has been well described in the neonatal period (1). In older children, subgaleal hematomas can also get infected through local spread of bacteria, but hematogenous dissemination during an upper respiratory infection has also been reported: Barry et al. report a healthy 8-month-old girl who presented with an infected subgaleal hematoma following a minor fall. Physical examination revealed no scalp laceration, yet cultures of the hematoma grew Streptococcus pneumoniae. The origin of the infection was hypothesized to be hematogenous spread of S. pneumoniae colonizing the nasopharynx, through one of the anastomoses of the facial vascular system. The patient underwent four weeks of intravenous antibiotics regimen before hospital discharge. In the articles reviewed in this study, no prophylactic antibiotics were used after drainage in non-infected subgaleal hematoma.
It is worth noting that even though the relative volume of blood in traumatic hematomas is usually less important than in newborns, transfusion might be needed in some cases (2). In addition to the case reported by Nichter et al. and mentioned above where a transfusion was required after a liter of blood was drained from the patient's subgaleal hematoma, Scheier et al. also describe a case requiring a blood transfusion; a 10-year-old girl presented with a subgaleal hematoma following non accidental hair pulling. The patient underwent surgical drainage (250 ml of blood), and a transfusion was required for a hemoglobin nadir of 7.1 g/L, associated with tachycardia and fatigue. The outpatient follow-up showed no coagulopathy and no recurrence of the hematoma.
When the above complications are suspected, surgical drainage may be necessary. Drainage however carries a risk of complications, particularly iatrogenic infection, as emissary veins communicate with the dural sinuses.
In the patient described in this case report, drainage was deemed appropriate to relieve the discomfort of the patient, after weighing the risks and benefits of the procedure.
Subgaleal hematomas might also lead to calcification, motivating drainage to avoid such complications. In rare cases, calcifications can indeed lead to cranial deformation requiring reconstructive surgery, especially in patients with hematologic disease such as Kasabach-Merrit phenomenon, whereby a vascular lesion causes platelet and coagulation factor consumption (18). Concern for potential development of calcifications is however not a criterion for drainage, as calcifications are not prevalent, particularly in patients with no underlying disease. The decision to surgically treat hence depends on patient risk factors, symptoms intensity and evolution, and complications. A similar approach is also described in adult studies and reports (24).
When calcifications or complications are present, however, surgical drainage and evacuation may be warranted. Edmondson et al. report a case of a 16-year-old boy who presented with a large subgaleal hematoma following hair braiding 10 days prior, with magnetic resonance imaging revealing areas of calcification (22). There were no arguments for an underlying vascular malformation, however, because of hematoma extension to the periorbital space, the patient underwent drainage of calcified clots via multiple small incisions.
Embolization has also been described after subgaleal hematoma (16, 23). Wajima et al. report an otherwise healthy adolescent presenting to the emergency department with two days of headache and no recall of head injury. Swelling of the scalp was noted and a head CT confirmed a subgaleal hematoma. He was drained on initial presentation and returned two weeks later with further scalp swelling and pain. Because of the recurrence of the hematoma, the patient underwent embolization. The outcome was favorable with no recurrence of the hematoma.
Although rare, physicians must be cognizant of the complications above and the indications for intervention, when presented with a subgaleal hematoma in a pediatric patient.
Although rare, subgaleal hematomas can occur in children beyond the neonatal period and are mostly associated with trauma, at times as benign as a minor fall, hair-braiding or hair pulling. While it is rare, voluminous subgaleal hematomas may require drainage to relieve pain or when compressive or infectious complications are suspected, especially in a patient with a known coagulopathy. Although usually not life-threatening unlike in the neonatal period, physicians taking care of children must be cognizant of this entity when caring for a patient with a large hematoma following head trauma, anticipate potential complications and consider a multidisciplinary approach with neurosurgery and hematology consultation if the presentation or evolution is atypical.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Open access funding by University of Geneva.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Barry J, Fridley J, Sayama C, Lam S. Infected subgaleal hematoma following blunt head trauma in a child: case report and review of the literature. Pediatr Neurosurg. (2015) 50(4):223–8. doi: 10.1159/000433442
2. Scheier E, Ben-Ami T, Guri A, Balla U. Subgaleal hematoma from a carnival costume. Isr Med Assoc J. (2019) 21(6):422–3.31280516
3. Pope-Pegram LD, Hamill MB. Post-traumatic subgaleal hematoma with subperiosteal orbital extension. Surv Ophthalmol. (1986) 30(4):258–62. doi: 10.1016/0039-6257(86)90122-0
4. Nichter LS, Bolton LL, Reinisch JF, Sloan GM. Massive subgaleal hematoma resulting in skin compromise and airway obstruction. J Trauma. (1988) 28(12):1681–3. doi: 10.1097/00005373-198812000-00014
5. Lee KS, Bae HG, Yun IG. Bilateral proptosis from a subgaleal hematoma. Case report. J Neurosurg. (1988) 69(5):770–1. doi: 10.3171/jns.1988.69.5.0770
6. Cooling DS, Viccellio P. Massive subgaleal hematoma following minor head trauma. J Emerg Med. (1991) 9(Suppl 1):33–5. doi: 10.1016/0736-4679(91)90585-4
7. Pomeranz AJ, Ruttum MS, Harris GJ. Subgaleal hematoma with delayed proptosis and corneal ulceration. Ann Emerg Med. (1995) 26(6):752–4. doi: 10.1016/S0196-0644(95)70051-X
8. Vu TT, Guerrera MF, Hamburger EK, Klein BL. Subgaleal hematoma from hair braiding: case report and literature review. Pediatr Emerg Care. (2004) 20(12):821–3. doi: 10.1097/01.pec.0000148031.99339.b7
9. Raffini L, Tsarouhas N. Subgaleal hematoma from hair braiding leads to the diagnosis of von Willebrand disease. Pediatr Emerg Care. (2004) 20(5):316–8. doi: 10.1097/01.pec.0000125661.50937.fc
10. Fujisawa H, Yonaha H, Oka Y, Uehara M, Nagata Y, Kajiwara K, et al. A marked exophthalmos and corneal ulceration caused by delayed massive expansion of a subgaleal hematoma. Childs Nerv Syst. (2005) 21(6):489–92. doi: 10.1007/s00381-004-1054-8
11. Seifert D, Puschel K. Subgaleal hematoma in child abuse. Forensic Sci Int. (2006) 157(2–3):131–3. doi: 10.1016/j.forsciint.2005.03.023
12. Sillero Rde O. Massive subgaleal hematoma. J Trauma. (2008) 65(4):963. doi: 10.1097/TA.0b013e31809ff3ce
13. Karcioglu ZA, Hoehn ME, Lin YP, Walsh J. Ocular involvement after subgaleal hematoma. J Pediatr Ophthalmol Strabismus. (2008) 12(5):521–3. doi: 10.1016/j.jaapos.2008.03.004
14. Kim D, Taragin B. Subgaleal hematoma presenting as a manifestation of factor XIII deficiency. Pediatr Radiol. (2009) 39(6):622–4. doi: 10.1007/s00247-009-1176-y
15. Onyeama CO, Lotke M, Edelstein B. Subgaleal hematoma secondary to hair braiding in a 31-month-old child. Pediatr Emerg Care. (2009) 25(1):40–1. doi: 10.1097/PEC.0b013e318191db98
16. Koizumi K, Suzuki S, Utsuki S, Nakahara K, Niki J, Mabuchi I, et al. A case of non-traumatic subgaleal hematoma effectively treated with endovascular surgery. Interv Neuroradiol. (2010) 16(3):317–21. doi: 10.1177/159101991001600315
17. Natarajan MS, Prabhu K, Braganza A, Chacko AG. Posttraumatic subgaleal and orbital hematoma due to factor XIII deficiency. J Neurosurg Pediatr. (2011) 7(2):213–7. doi: 10.3171/2010.11.PEDS10486
18. Stalder MW, Dorafshar AH, Redett RJ. Calcified subgaleal hematoma with secondary cranial deformity in a patient with Kasabach-Merritt phenomenon. J Craniofac Surg. (2011) 22(1):208–11. doi: 10.1097/SCS.0b013e3181f753d6
19. Kichari JR, Gielkens H. Massive traumatic subgaleal haematoma. Emerg Med J. (2013) 30(4):344. doi: 10.1136/emermed-2012-201729
20. Yamada SM, Tomita Y, Murakami H, Nakane M. Delayed post-traumatic large subgaleal hematoma caused by diastasis of rhomboid skull suture on the transverse sinus. Childs Nerv Syst. (2015) 31(4):621–4. doi: 10.1007/s00381-014-2531-3
21. Shamji S, Jacoby JL. Massive subgaleal hematoma and clinical suspicion of child abuse. J Am Osteopath Assoc. (2015) 115(1):58; quiz 9–60. doi: 10.7556/jaoa.2015.014
22. Edmondson SJ, Ramman S, Hachach-Haram N, Bisarya K, Fu B, Ong J, et al. Hair today; scalped tomorrow: massive subgaleal haematoma following sudden hair pulling in an adolescent in the absence of haematological abnormality or skull fracture. J Craniofac Surg. (2016) 27(5):1261–2. doi: 10.1097/SCS.0000000000002710
23. Wajima D, Nakagawa I, Kotani Y, Wada T, Yokota H, Park YS, et al. A case of refractory subgaleal hematoma in adolescence treated with aspiration and endovascular surgery. Acta Neurochir (Wien). (2017) 159(8):1565–9. doi: 10.1007/s00701-017-3207-z
24. Chen CE, Liao ZZ, Lee YH, Liu CC, Tang CK, Chen YR. Subgaleal hematoma at the contralateral side of scalp trauma in an adult. J Emerg Med. (2017) 53(5):e85–e8. doi: 10.1016/j.jemermed.2017.06.007
25. Jenkins TL, Zheng CX, Murchison AP, Bilyk JR. Orbital compartment syndrome following post-traumatic subgaleal hematoma. Ophthalmic Plast Reconstr Surg. (2017) 33(2):e33–6. doi: 10.1097/IOP.0000000000000684
26. Puri S, Duff SM, Mueller B, Prendes M, Clark J. Hairpulling causing vision loss: a case report. Orbit. (2019) 38(2):162–5. doi: 10.1080/01676830.2018.1459739
Keywords: pediatric, drainage, head trauma, subgaleal hematoma, trauma
Citation: Aubert B, Cadoux M and Sahyoun C (2023) Traumatic subgaleal hematoma drainage in an adolescent: a case report and review of the literature. Front. Pediatr. 11:1182899. doi: 10.3389/fped.2023.1182899
Received: 9 March 2023; Accepted: 15 May 2023;
Published: 30 May 2023.
Edited by:
Jean-Christophe Mercier, Université de Paris, FranceReviewed by:
Danielle S. Wendling-Keim, Ludwig Maximilian University of Munich, Germany© 2023 Aubert, Cadoux and Sahyoun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manon Cadoux bWFub24uY2Fkb3V4QGhjdWdlLmNo
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.