 Tomáš Seeman1,2,3*†
Tomáš Seeman1,2,3*† Jiří Dušek2
Jiří Dušek2
- 1Department of Pediatrics, University Hospital Ostrava, Ostrava, Czechia
- 2Department of Pediatrics, 2nd Medical Faculty, Charles University Prague, Prague, Czechia
- 3Faculty of Mediciny, University of Ostrava. Ostrava, Czechia
Background: It is not known whether withdrawal of angiotensin-converting enzyme inhibitors (ACEIs) in children with advanced chronic kidney disease (CKD) is beneficial similar to adults. We report a case series of children with advanced CKD whose ACEIs were stopped.
Methods: In the last 5 years, we stopped ACEIs in seven consecutive children on ACEI therapy with rapidly declining CKD stage 4–5. The median age was 12.5 years (range 6.8–17.6); the median estimated glomerular filtration rate (eGFR) at stopping ACEIs was 12.5 ml/min/1.73 m2 (range 8.8–19.9).
Results: Six to twelve months after stopping ACEIs, the eGFR increased in five children (71%). The median absolute increase of eGFR was 5.0 ml/min/1.73 m2 (range −2.3 to +20.0) and relative increase of eGFR was 30% (range −34 to +99). The median follow-up after stopping ACEIs was 2.7 (range 0.5–5.0) years, either until the start of dialysis (n = 5) or until the last follow-up without dialysis (n = 2).
Conclusions: This case series showed that withdrawal of ACEIs in children with CKD stage 4–5 and rapidly declining kidney function may lead to an increase in eGFR.
section-at-acceptancePediatric NephrologyIntroduction
Treatment of children with chronic kidney disease (CKD) with renin–angiotensin–aldosterone system inhibitors (RAASi) is the cornerstone of conservative therapy due to their antihypertensive, antiproteinuric, and renoprotective effects. Recently, van den Belt et al. (1) published a retrospective study on the effects of discontinuation of RAASi in children with advanced CKD. Withdrawal of RAASi led to a more rapid estimated glomerular filtration rate (eGFR) decline than before discontinuation. This finding was in sharp contrast to several previous similar trials in adults. These studies showed that stopping of RAASi leads to improvement of eGFR in the majority of patients (2–4). In the largest adult study, Ahmed et al. demonstrated increased eGFR in 60% of adults with advanced CKD and undoubtedly delayed onset of kidney replacement therapy (KRT) in the majority of patients after stopping inhibitors of the RAASi (2). The reasons for the discrepancy between the result of pediatric and adult studies are not fully clear and need further analyses.
We aimed to present a case series of seven children from our tertiary pediatric nephrology center with CKD stage 4–5 (CKD5) and rapidly declining GFR with stopping angiotensin-converting enzyme inhibitors (ACEIs). Our case series is unique as no pediatric study has yet shown that, in contrary to adults, withdrawal of ACEIs in children with CKD5 can be beneficial in terms of kidney function.
Case description
In the last 5 years, we stopped ACEIs in all seven consecutive children on therapy with RAASi who had rapidly declining GFR toward CKD stage 5 and have been not yet indicated for KRT with the aim to win time for preparation of KRT. We did it after reading the positive results of stopping ACEI in adults with advanced CKD (2–4) in hope to delay onset of KRT.
The median age of the patients was 12.5 years (range 6.8–17.6); the primary kidney diseases were mainly congenital anomalies of kidneys and urinary tract. Five children received ramipril (median dose 2.3 mg/m2/day) and two received enalapril (0.1 and 0.2 mg/kg/day). The indication for ACEI was hypertension (n = 5) and hypertension with proteinuria (n = 2). The median eGFR [Schwartz formula (5)] at stopping ACEI was 12.5 ml/min/1.73 m2 (range 8.8–19.9), and six children were already in CKD stage 5. The median eGFR slope 6–12 months before stopping ACEI was −9.8 ml/min/1.73 m2/year (range from −4.0 to −19.5). All children had declining eGFR at least in the last two assessments before stopping ACEI and had no acute infection or dehydration. The blood pressure index was calculated as patients’ blood pressure (BP) divided by the 95th percentile. Formal statistical analysis was not performed due to the low number of cases.
Diagnostic assessment and therapeutic intervention
Kidney function
Six to twelve months after stopping ACEIs, the eGFR increased in five of seven children (71%). The median absolute increase of eGFR was 5.0 ml/min/1.73 m2 (range −2.3 to +20.0) and relative increase of eGFR was 30% (range from −34 to +99). Improvement of eGFR >25% from baseline value [a parameter used by Ahmed et al. in their study (2)] occurred in 57% of children. The eGFR slope in all individual patients is given in Figure 1. The median follow-up after stopping ACEI was 2.7 (range 0.5–5.0) years, until the start of KRT (n = 5) or until the last follow-up without KRT (n = 2). The prognosis of these children improved as the time without the need for KRT (dialysis/transplantation) was prolonged.
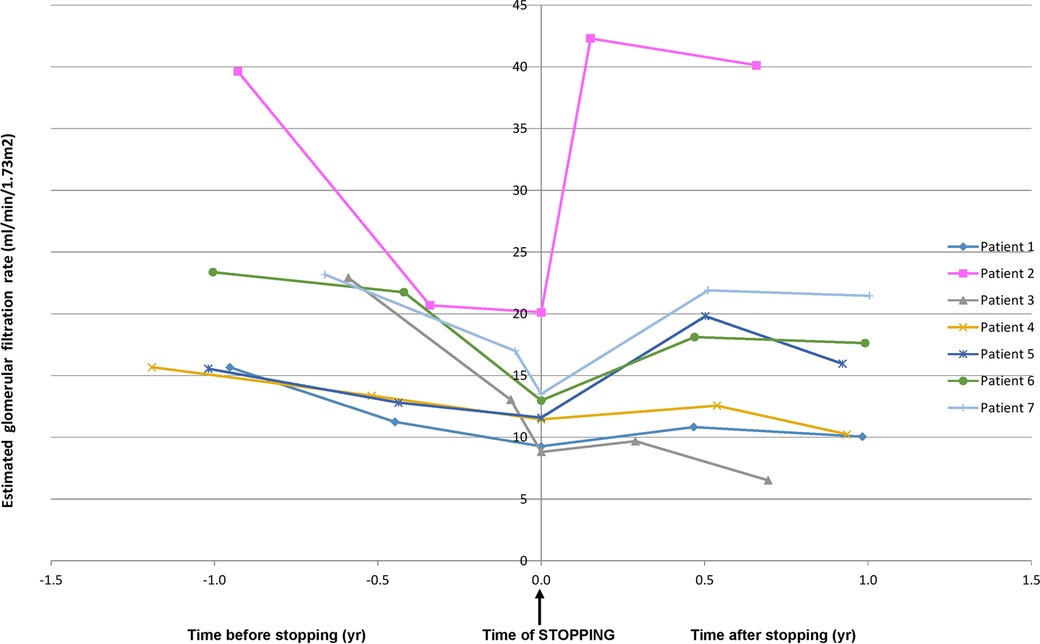
Figure 1. Glomerular filtration rate slope in all individual patients before and after stopping ACEIs. ACEIs, angiotensin-converting enzyme inhibitors.
Blood pressure, proteinuria, and serum potassium
The median BP and proteinuria at the time of stopping ACEI were 107/68 mmHg (BP index 0.93) and 28 mg/mmol creatinine (range 13–41), respectively, and they increased to 121/80 mmHg (BP index 0.97) and 138 mg/mmol creatinine (range 43–209) after stopping, respectively. The median serum potassium was 5.3 mmol/L (range 4.9–6.7) at the time of stopping ACEI and 4.8 mmol/L (range 4.4–5.2) after stopping. Patient and laboratory characteristic in all individual patients is given in Table 1.
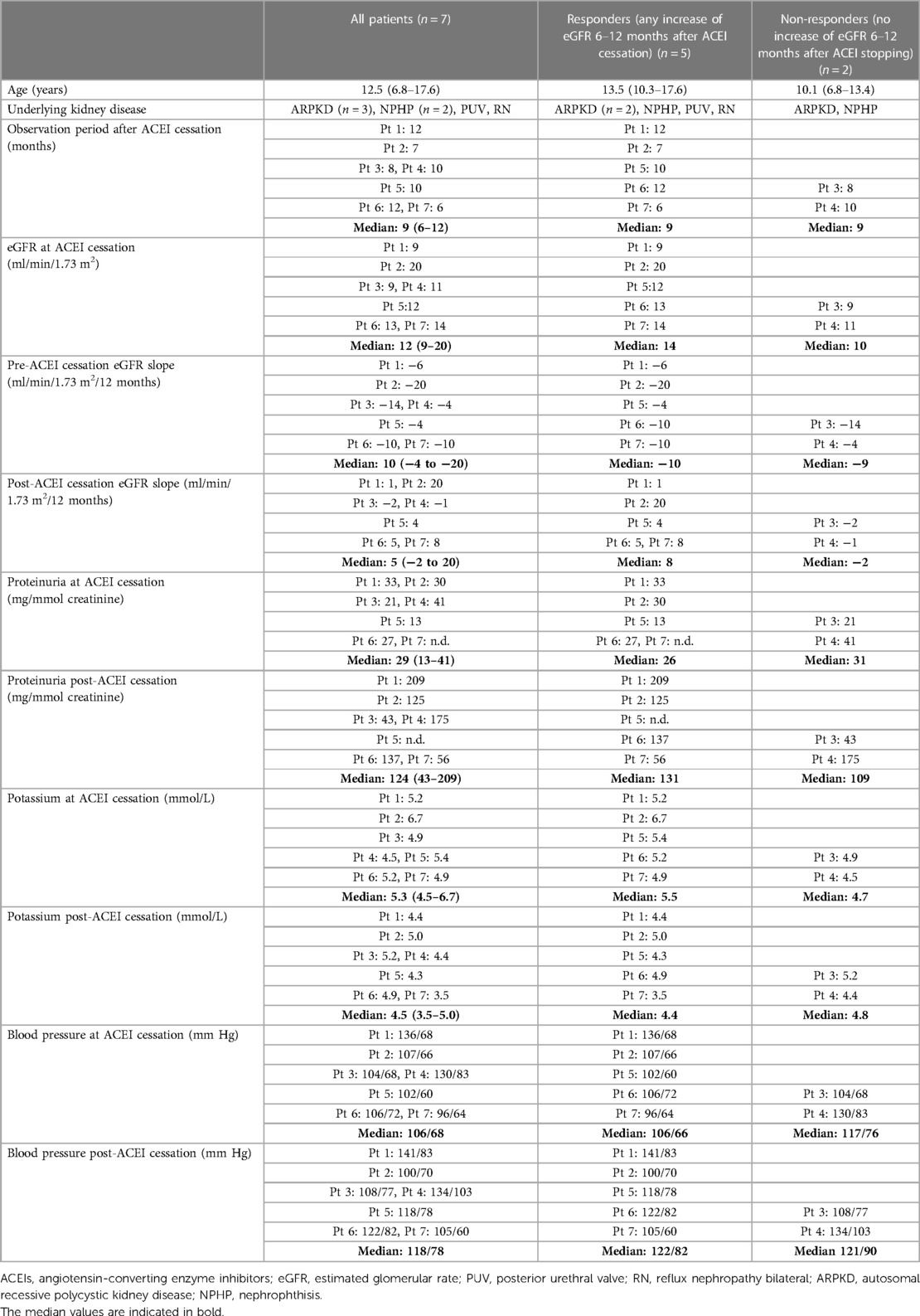
Table 1. Patient and laboratory characteristics in all individual patients before and after stopping ACEIs.
Discussion
In this small case series from our center, we compare the kidney function before and after withdrawal of ACEI in children with rapidly declining CKD stages 4–5. We could demonstrate that kidney function, similarly to the adults, improved also in children by approximately 70%.
There are at least three adult studies showing that the withdrawal of ACEI in CKD patients leads to improved GFR (2–4). Ahmed et al. demonstrated in an adult study that eGFR increased in 60% of patients with advanced CKD and undoubtedly delayed the onset of KRT in the majority of patients after stopping inhibitors of the RAAS (2). Hansen et al. observed increased GFR 1 month after withdrawal of long-term antihypertensive treatment, mainly ACEI, in 42 patients with diabetic nephropathy and CKD stages 1–2 (3). Onuigbo and Onuigbo demonstrated in their prospective study on 100 consecutive patients with advanced CKD stage 4 (mean GFR at stopping 22 ml/min) who presented with >25% increase in baseline that serum creatinine before enrollment (rapid progressors) that withdrawal of RAAS blockers lead to increase in GFR in 74% of patients (4). The median percentage of GFR improvement in the responders was 64%, again similar to the study done by Ahmed et al. However, Hsu et al. showed in their population-based observational study from Taiwan that the use of RAAS blockers in predialysis CKD stage 5 adult patients was associated with 6% lower risk for long-term dialysis (6).
On the contrary to the three adult studies that stopped ACEIs, the only pediatric study published recently by van den Belt et al. (1) showed in a retrospective design that discontinuation of RAASi in children with advanced CKD led to more rapid eGFR decline than before RAASi discontinuation. This finding is in sharp contrast to previous similar trials in adults.
The reasons for discrepant results in the study by van den Belt et al. (1) and others (2–4) and our case series could be several: eGFR at stopping of ACEIs, rate of the progression of CKD, reasons for stopping, BP, proteinuria, or type of study. In our patients and in the study by Ahmed et al., the eGFR at stopping ACEI was considerably lower than in the study by van den Belt et al. (12 and 16 vs. 27 ml/min/1.73 m2) (1, 2). Moreover, the eGFR slope before stopping ACEI was 4–7 times faster in our patients and the study by Ahmed et al. than in the study by van den Belt et al. (10 and 6 vs. 1.5 ml/min/1.73 m2/year) (1, 2). The children from the latter study would, therefore, progress to CKD stage 5 (GFR <15 ml/min/1.73 m2) very slowly and as late as in 8 years.
The eGFR slope after stopping ACEI in our study was +5 ml/min/1.73 m2/year (ranging −2 to 20, Table 1), which is in contrast to the results in the study by van Belt et al. where the eGFR slope increased from −1.5 to −3.9 ml/min/1.73 m2/year. The reasons for the different results in these two studies can be similar to that discussed earlier.
The reason for stopping ACEI was always the rapid decline of GFR toward CKD stage 5 in both studies with improvement of GFR after stopping. On the contrary, in the study by van den Belt et al., increase of serum creatinine was the reason for discontinuation in only 33% of patients; the remaining 67% had other reasons such as hyperkalemia (1). It would be interesting to know whether this subgroup of 33% children with increase of serum creatinine as the indication for discontinuation of RAASi did better than the whole group. Chan et al. hypothesized in their educational review on this topic that the study done by van den Belt et al. is limited by its observational nature and selection bias (7).
In another pediatric study, Abraham et al. (8) showed in children with CKD from the CKiD study that the use of RAASi was found to reduce the risk of KRT by 21% in comparison to nonusers. However, the median eGFR in discontinuers was much higher (26 ml/min/1.73 m2 with no patient <15 ml/min/1.73 m2) than in our case series (12 ml/min/1.73 m2), and the reasons for RAASi discontinuation were not specified. Furthermore the authors stated that “our results suggest that clinicians choose to maintain residual kidney function by discontinuing ACEi/ARBs.”
We speculate that the different results between our case series, adult studies, and those by van den Belt et al. and Abraham et al. are mainly due to different GFR at ACEI stopping (lower in the adult studies and our patients) and GFR slope before stopping (faster in the adult studies and our patients). We hypothesize, that highly selected patients with very low GFR at CKD stage 5 (10–15 ml/min/1.73 m2) being prepared for the start of KRT with a rapid declining GFR slope might potentially profit from stopping ACEI with subsequent improvement of GFR as it has been shown in adults and in our pediatric cases.
Our case series has strengths and limitations. The main strength is the fact that it is only the second pediatric study dealing with kidney effects of withdrawal of ACEIs in patients with advanced CKD. There are several limitations, especially very small number of cases, the retrospective design, and the lack of a control group of patients without ACEI withdrawal.
In a most recent article on the topic of stopping ACEIs in advanced CKD, Chan et al. recommended cessation of RAASi if patients develop rapidly declining kidney function progressing to CKD stage 5 (7). Nevertheless, only the results of the ongoing randomized controlled trial of RAAS blockers’ withdrawal in advanced renal disease (ongoing STOP-ACEi trial), will answer the question whether stopping ACEI in patients with advanced CKD is beneficial (9).
Conclusion
Our case series suggests that in some children with advanced CKD stage 5 and rapidly deteriorating kidney function, stopping ACEIs may lead to an increase in eGFR in some patients.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
TS made the conception and design of the study and drafted the article. JD made acquisition and interpretation of data. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors thank to the patients, their parents, and renal nurses for their cooperation and Karel Vondrak for collecting data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ACEI, angiotensin-converting enzyme inhibitor; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; KRT, kidney replacement therapy.
References
1. van den Belt SM, Heerspink HJL, Kirchner M, Gracchi V, Thurn-Valsassina D, Bayazit AK, et al. Discontinuation of RAAS inhibition in children with advanced CKD. Clin J Am Soc Nephrol. (2020) 15:625–32. doi: 10.2215/CJN.09750819
2. Ahmed AK, Kamath NS, El Kossi M, El Nahas AM. The impact of stopping inhibitors of the renin-angiotensin system in patients with advanced chronic kidney disease. Nephrol Dial Transplant. (2010) 25:3977–82. doi: 10.1093/ndt/gfp511
3. Hansen HP, Rossing P, Tarnow L, Nielsen FS, Jensen BR, Parving HH. Increased glomerular filtration rate after withdrawal of long-term antihypertensive treatment in diabetic nephropathy. Kidney Int. (1995) 47:1726–31. doi: 10.1038/ki.1995.238
4. Onuigbo MA, Onuigbo NT. Late-onset renal failure from angiotensin blockade (LORFFAB) in 100 CKD patients. Int Urol Nephrol. (2008) 40:233–9. doi: 10.1007/s11255-007-9299-2
5. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. (2009) 20:629–37. doi: 10.1681/ASN.2008030287
6. Hsu TW, Liu JS, Hung SC, Kuo KL, Chang YK, Chen YC, et al. Renoprotective effect of renin-angiotensin-aldosterone system blockade in patients with predialysis advanced chronic kidney disease, hypertension, and anemia. JAMA Intern Med. (2014) 174:347–54. doi: 10.1001/jamainternmed.2013.12700
7. Chan EY, Ma AL, Tullus K. When should we start and stop ACEi/ARB in paediatric chronic kidney disease? Pediatr Nephrol. (2021) 36:1751–64. doi: 10.1007/s00467-020-04788-w
8. Abraham AG, Betoko A, Fadrowski JJ, Pierce C, Furth S, Warady BA, et al. Renin-angiotensin II-aldosterone system blockers and time to renal replacement therapy in children with CKD. Pediatr Nephrol. (2017) 32:643–9. doi: 10.1007/s00467-016-3512-4
9. Bhandari S, Ives N, Brettell EA, Valente M, Cockwell P, Topham PS, et al. Multicentre randomized controlled trial of angiotensin-converting enzyme inhibitor/angiotensin receptor blocker withdrawal in advanced renal disease: the STOP-ACEi trial. Nephrol Dial Transplant. (2016) 31:255–61. doi: 10.1093/ndt/gfv346
Keywords: estimated glomerular filtration rate (eGFR), blood pressure (BP), proteinuria, case report, chronic kidney disease
Citation: Seeman T and Dušek J (2023) Case report: Withdrawal of angiotensin-converting enzyme inhibitors in children with advanced chronic kidney disease and rapidly declining kidney function. Front. Pediatr. 11:1172567. doi: 10.3389/fped.2023.1172567
Received: 23 February 2023; Accepted: 4 April 2023;
Published: 4 May 2023.
Edited by:
Rainer Büscher, Essen University Hospital, GermanyReviewed by:
Julia Thumfart, Charité University Medicine Berlin, GermanyDagmara Borzych-Duzalka, Medical University of Gdansk, Poland
© 2023 Seeman and Dušek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomáš Seeman dG9tYXMuc2VlbWFuQGxmbW90b2wuY3VuaS5jeg==
†ORCID Tomáš Seeman orcid.org/0000-0003-1371-3096