 Olga Gómez1,2,3*
Olga Gómez1,2,3* Laura Nogué1,2Iris Soveral1,4Laura Guirado1Nora Izquierdo1Miriam Pérez-Cruz1,5,6Narcís Masoller1,2María Clara Escobar5,7
Laura Nogué1,2Iris Soveral1,4Laura Guirado1Nora Izquierdo1Miriam Pérez-Cruz1,5,6Narcís Masoller1,2María Clara Escobar5,7 Joan Sanchez-de-Toledo5,7Josep Maria Martínez-Crespo1,2,3
Joan Sanchez-de-Toledo5,7Josep Maria Martínez-Crespo1,2,3 Mar Bennasar1,2,†Fàtima Crispi1,2,3,†
Mar Bennasar1,2,†Fàtima Crispi1,2,3,†
- 1BCNatal Fetal Medicine Research Center, Sant Joan de Déu Hospital, Barcelona, Spain
- 2August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain
- 3Fetal Medicine Department, Centro de Investigación Biomédica en Red de Enfermedades Raras (CIBERER), Madrid, Spain
- 4Department of Obstetrics, Hospital General de Hospitalet, Barcelona, Spain
- 5Sant Joan de Déu Research Institute (IRSJD), Barcelona, Spain
- 6Primary Care Interventions to Prevent Maternal and Child Chronic Diseases of Perinatal and Developmental Origin Network, Carlos III Health Institute, Madrid, Spain
- 7Pediatric Cardiology Department, Sant Joan de Déu Hospital, Esplugues de Llobregat, Barcelona, Spain
Previous reports suggest that cord blood biomarkers could serve as a prognostic tool for conotruncal congenital heart defects (CHD). We aimed to describe the cord blood profile of different cardiovascular biomarkers in a prospective series of fetuses with tetralogy of Fallot (ToF) and D-transposition of great arteries (D-TGA) and to explore their correlation with fetal echocardiography and perinatal outcome.
Methods: A prospective cohort study (2014–2019), including fetuses with isolated ToF and D-TGA and healthy controls, was conducted at two tertiary referral centers for CHD in Barcelona. Obstetric ultrasound and fetal echocardiography were performed in the third trimester and cord blood was obtained at delivery. Cord blood concentrations of N-terminal precursor of B-type natriuretic peptide, Troponin I, transforming growth factorβ (TGFβ), placental growth factor, and soluble fms-like tyrosine kinase-1 were determined.
Results: Thirty-four fetuses with conotruncal-CHD (22 ToF and 12 D-TGA) and 36 controls were included. ToF-fetuses showed markedly increased cord blood TGFβ (24.9 ng/ml (15.6–45.3) vs. normal heart 15.7 ng/ml (7.2–24.3) vs. D-TGA 12.6 ng/ml (8.7–37.9); P = 0.012). These results remained statistically significant even after adjusting for maternal body mass index, birth weight and mode of delivery. TGFß levels showed a negative correlation with the pulmonary valve diameter z-score at fetal echocardiography (r = −0.576, P = 0.039). No other differences were found in the rest of cord blood biomarkers among the study populations. Likewise, no other significant correlations were identified between cardiovascular biomarkers, fetal echocardiography and perinatal outcome.
Conclusions: This study newly describes increased cord blood TGFβ concentrations in ToF compared to D-TGA and normal fetuses. We also demonstrate that TGFβ levels correlate with the severity of right ventricle outflow obstruction. These novel findings open a window of research opportunities on new prognostic and potential preventive strategies.
1. Introduction
Conotruncal anomalies are a common group of congenital heart defects (CHD) involving the outflow tracts and great vessels. The inclusion of the outflow tracts views into fetal heart screening ultrasound (1) has greatly improved the prenatal detection of conotruncal anomalies, particularly tetralogy of Fallot (ToF) and D-transposition of great arteries (D-TGA), the two most commonly prenatally diagnosed cyanotic CHD (2). Multidisciplinary care from fetal life has also contributed to greatly increase neonatal survival (3). Therefore, fetal cardiology is now focused on improving medium- and long-term prognostic evaluation.
Several blood cardiovascular biomarkers have been proposed as potential prognostic factors. Previous reports suggest altered circulating concentrations of angiogenic factors in fetuses with CHD. Placental growth factor (PlGF) is a glycoprotein mainly produced in placental trophoblast to promote endothelial growth but also expressed by cardiomyocytes in response to stress (4). The soluble form of fms-like tyrosine kinase-1 (sFlt-1) is a potent antagonist of PlGF that prevents its interaction with cell receptors (5). However, only a few studies have evaluated the pattern of these biomarkers in fetuses with CHD showing controversial results. An antiangiogenic imbalance, with significantly increased cord blood sFlt-1 levels, was firstly described in a mixed group of CHD (6). Recently, a proangiogenic profile with drastically reduced cord blood sFlt1 concentrations, has been reported in a group of left univentricular CHD including hypoplastic left heart syndrome, severe aortic stenosis and Shone syndrome (7). Nonetheless, the role of PlGF and sFlt1 in different types of CHD and their correlation with cardiac dysfunction and perinatal outcome has been insufficiently studied to date.
Additional biomarkers with a potential role in CHD are B-type natriuretic peptide (BNP) and its N-terminal precursor (NT-proBNP). They are released from ventricular myocytes in response to pressure/volume overload or hypoxia, and are clinically useful for CHD screening in neonatal stage (8). Moreover, increased cord blood levels of NT-proBNP and Troponin I, a specific marker of myocardial damage (9), have been described in fetuses with single ventricle (7, 10). Nonetheless, elevated cord blood levels of NT-proBNP and Troponin I have also been reported in neonates with acidosis (11) and intrauterine growth restriction (12).
Lastly, transforming growth factor β1 (TGFβ) is a cytokine produced by different cells with an essential role in the development of heart remodeling and fibrosis (13). Several studies describe elevated plasmatic concentrations of TGFβ in adolescents and young adults with repaired ToF, indicating altered TGFβ signaling in ToF correlating with aortic root dilation (14, 15). To our knowledge, only one study has evaluated this biomarker in fetal life, demonstrating a significant elevation in aortic coarctation, aortic stenosis and Shone syndrome with biventricular outcome (7).
Thus, the study of these biomarkers in a series specifically composed of common conotruncal anomalies could be of interest to preliminary define its cardiac biomarker profile from fetal life, evaluating its potential clinical applicability in subsequent studies. We aimed to first describe the cord blood levels of PlGF, sFlt1, BNP, Troponin I and TGFβ in a prospective series of fetuses with ToF and D-TGA and to explore their correlation with fetal echocardiography and perinatal outcome.
2. Materials and methods
2.1. Study population
A prospective cohort study was conducted between January 2014 and December 2019, including fetuses diagnosed with ToF and D-TGA at the Fetal Cardiology Unit of BCNatal, which groups two tertiary referral centers for CHD in Barcelona (Clínic and Sant Joan de Déu hospitals). Fetuses with structurally normal hearts were also recruited from low-risk pregnancies attended at BCNatal and included as a control group. Pregnancies of women older than 18 years with accurate gestational age (GA) calculated by first-trimester crown-rump length (16) were considered eligible. Fetal ultrasound and echocardiography were performed in the third trimester, cord blood was obtained at delivery and perinatal results and cardiovascular outcome data were collected postnatally. The study was approved by the institutional Ethics Committee (Reg. HCB/2019/0540). Written consent was obtained from all pregnant women.
ToF was defined by the combination of a subaortic ventricular septal defect with an overriding aorta and infundibular pulmonary obstruction. ToF-cases were sub-classified as ToF with pulmonary stenosis or atresia, based on the presence or absence of anterograde flow through the pulmonary valve, respectively. To obtain a homogeneous group, infrequent cases of TOF with absent pulmonary valve or with major aortopulmonary collaterals were not considered eligible for the study. D-TGA was defined based on the presence a discordant ventricular arterial connection and it was later subdivided into two categories: simple-D-TGA and complex-D-TGA (in the presence of a ventricular septal defect, pulmonary stenosis and/or coarctation of the aorta). All fetuses underwent prenatal genetic testing with microarray analysis and complete extracardiac anatomical ultrasound at diagnosis and during follow-up. Fetuses with pre or postnatal diagnosis of additional major cardiac defects, major extracardiac malformations and/or chromosomal abnormalities were excluded from the study.
Control fetuses were recruited from singleton, spontaneously conceived and low-risk pregnancies attended at the maternal-fetal Medicine Department at BCNatal. Control fetuses were matched for GA (±2 weeks) at delivery with conotruncal-CHD fetuses. Exclusion criteria for controls were pre or postnatal diagnosis of CHD, major extracardiac malformations, chromosomal abnormalities and/or those conditions potentially affecting cord blood biomarkers such as intrauterine growth restriction (12, 17–19), macrosomia (20), pregestational diabetes (20, 21), pregestational hypertension or exposure to toxics (22).
2.2. Baseline, perinatal characteristics and cardiovascular outcome
Maternal age, body mass index, ethnicity, smoking status, pre-gestational medical conditions and parity were collected from medical records. Pregnancy outcome, including the presence of intrauterine growth restriction, preeclampsia, pregnancy induced hypertension, gestational diabetes and prematurity below 37 weeks and perinatal characteristics as GA at delivery, mode of delivery, birthweight, neonatal height and head circumference, umbilical artery pH and Apgar score were also recorded. Intrauterine growth restriction was defined as EFW and birthweight below the 3rd centile or below the 10th centile with abnormal uterine, umbilical or middle cerebral artery Doppler values (23). In all cases, CHD subtype was confirmed by postnatal echocardiography and clinical outcome was obtained from medical records at least one year after birth and reevaluated yearly if necessary.
2.3. Fetal ultrasound and echocardiography
Fetal ultrasound and echocardiography were performed using a Siemens Sonoline Antares (Siemens Medical Systems, Malvern; PA, USA) or Voluson E10 (General Electric, Zipf, Austria) using a curved-array 2–6 MHz transducer. Structural fetal ultrasound encompassed a detailed extra-cardiac and cardiac examination, following recommended guidelines (24, 25).
Third trimester standard obstetric ultrasound comprised estimation of fetal weight, measurement of mean uterine arteries pulsatility index (PI), umbilical artery PI, middle cerebral artery PI, aortic isthmus PI (26) and ductus venosus PI (27). Estimated fetal weight (EFW) was calculated according to the method of Hadlock et al. (28). EFW centile was calculated using institutional reference curves (29). The cerebroplacental ratio was calculated by dividing the middle cerebral artery PI by the umbilical artery PI (30).
Following the echocardiographic protocol of our center in CHD, in fetuses with ToF and D-TGA, a detailed study of cardiac morphometry and functionalism was performed including measurement of cardiac area, cardiothoracic ratio, ventricular widths, lengths, right-to-left and sphericity indices (SI) and septal thickness from an apical or transverse four-chamber view at end-diastole (31, 32). Aortic and pulmonary valve diameters at mid-systole and aortic-to-pulmonary valve ratio were also obtained Aortic and pulmonary valve size were normalized for gestational age and the z-scores were calculated (33).Cardiac function evaluation included aortic and pulmonary peak systolic velocities, mitral (MAPSE) and tricuspid annular-plane systolic excursion (TAPSE) (34).
2.4. Cord blood biomarkers
Cord blood samples were obtained from the umbilical vein after cord clamping at birth. Plasma was separated from ethylenediaminetetraacetic acid-treated blood using centrifugation at 1,400× g for 10 min at 4°C. Serum was separated using centrifugation at 2,000× g for 10 min at room temperature. Sample aliquots were immediately stored at −80°C until assayed.
Cord blood biomarkers were measured as previously described (7). Briefly, concentrations of PlGF and sFlt1 were determined in serum by the fully automated Elecsys assays on an electrochemiluminescence immunoassay platform Cobas analyzer (Roche Diagnostics, Mannheim, Germany). NT-proBNP and Troponin I concentrations were measured in plasma by electrochemiluminescence immunoassay using Siemens Atellica IM NT-proBNP and High Sensitivity Troponin I (sensitivity of the technique: 0.0025 pg/ml), respectively (Siemens Healthcare, Erlangen, Germany). TGFβ was measured in serum by conventional ELISA assay Quantikine Human TGF-beta1 (R&D Systems, Minneapolis, MN, USA). Concentrations of cord concentrations of PlGF, sFlt1, NT-proBNP and TGFβ are presented as continuous variables. Given the different behavior of troponin I (acute increase in response to ischemia or hypoxia), Troponin I was treated as dichotomous variable: concentrations above 0.0093 pg/ml (which corresponds to the 75th centile of the troponin level among the control group), were considered to be high.
2.5. Statistical analysis
IBM SPSS Statistics version 25 statistical package (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Kolmogorov-Smirnov test of normality was performed in all continuous variables. Measurements were expressed as mean ± standard deviation or as median (range) for continuous variables as appropriate, and frequencies with percentages for categorical variables. Differences between study groups were examined using parametric analysis of variance (one-way ANOVA) followed by post hoc Bonferroni tests for pairwise comparison for normally distributed variables, Kruskal–Wallis one-way ANOVA followed by post-hoc pairwise comparisons using the Dunn–Bonferroni approach for non-normally distributed variables and χ2 test for categorical variables.
Baseline variables were analyzed to identify possible confounders including maternal age, maternal body mass index (BMI), nulliparity, smoking, pregestational diabetes, gestational diabetes, preeclampsia, GA at delivery, birth weight, gender and mode of delivery. Potentially confounders factors such as maternal BMI, birth weight and mode of delivery were significantly different between groups, therefore were adjusted in the model. Spearman correlation coefficient to compare associations between biomarkers and the previously described standard obstetric ultrasound and echocardiographic parameters was used in the ToF and D-TGA groups. For all analyses, P-values <0.05 were considered statistically significant.
3. Results
3.1. Study population and obstetric standard ultrasound
From the original cohort of 84 ToF and D-TGA fetuses, 18 pregnant women elected for termination of pregnancy. We excluded from the analysis 6 cases with ToF: 1 case with absent pulmonary valve, 1 case with major aorto-pulmonary collateral arteries (MAPCAs), 1 case with intrauterine fetal demise, 1 monochorionic twin pregnancy, 1 case with a chromosomal abnormality and a last case with an associated multicystic kidney disease. We didn't obtain cord blood at delivery in 23 cases, 1 patient was lost to follow-up and 2 refused to participate. The final study population consisted of 34 fetuses with conotruncal CHD (22 ToF and 12 D-TGA cases) and 36 controls.
As shown in Figure 1, the ToF group included 19 fetuses with pulmonary stenosis and 3 cases with pulmonary atresia. Only one case of ToF with pulmonary stenosis presented retrograde flow at the ductus arteriosus, with the remaining cases presenting forward flow until birth. Blalock-Taussig shunt was required prior to the ToF corrective surgery only in the 3 cases with pulmonary atresia.
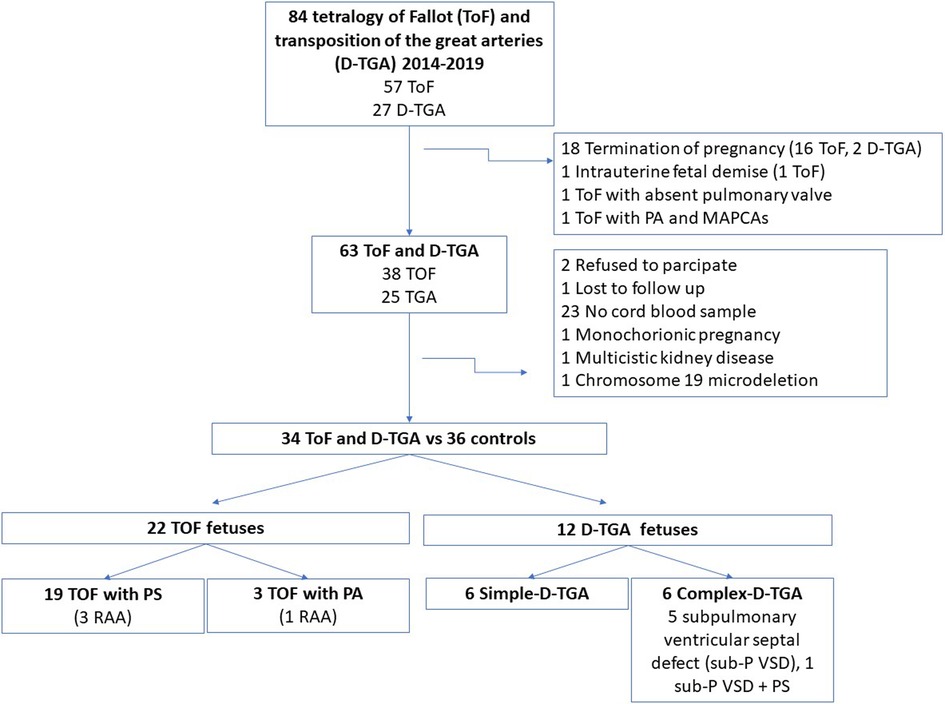
Figure 1. Flow chart of fetuses with conotruncal congenital heart defects included in the study. ToF, tetralogy of fallot, D-TGA, transposition of the great arteries; PA, pulmonary atresia; MAPCAs, major aortopulmonary collateral arteries; RAA, right aortic arch; sub-P VSD, subpulmonary ventricular septal defect; PS, pulmonary stenosis.
The D-TGA-group included 6 fetuses with a simple-D-TGA, 5 cases with a subpulmonary ventricular septal defect and one fetus with an associated pulmonary stenosis (complex-D-TGA group). Rashkind atrioseptostomy was performed prior to arterial switch procedure in 58.3% of the D-TGA fetuses (7/12). The cardiovascular outcome was favorable in all conotruncal CHD cases, with no significant postnatal complications and with a median follow-up of 46 months (interquartile range 28.0–50.5).
Maternal baseline characteristics and perinatal results are shown in Table 1. Most baseline characteristics were similar in the three study populations; however, BMI was significantly higher in pregnant women with ToF-fetuses compared to the other two groups. Additionally, the prevalence of small for GA fetuses was higher in the ToF group [31.8% (7/22)] and cesarean section was more frequently performed in the ToF and D-TGA groups compared to controls. Additional perinatal outcomes such as GA at delivery was similar across groups and there were no differences in the five-minute Apgar score and umbilical artery pH. No cases of fetal acidosis were found. Regarding biometrics at birth, ToF-fetuses had a significantly lower birth weight compared to D-TGA and control groups, with only 2 ToF cases with pulmonary stenosis presenting a birth weight below the 3th percentile. The head circumference at birth was also significantly reduced in both conotruncal CHD groups as compared to controls. As shown in Table 1, birth length did not significantly differ between the three groups.
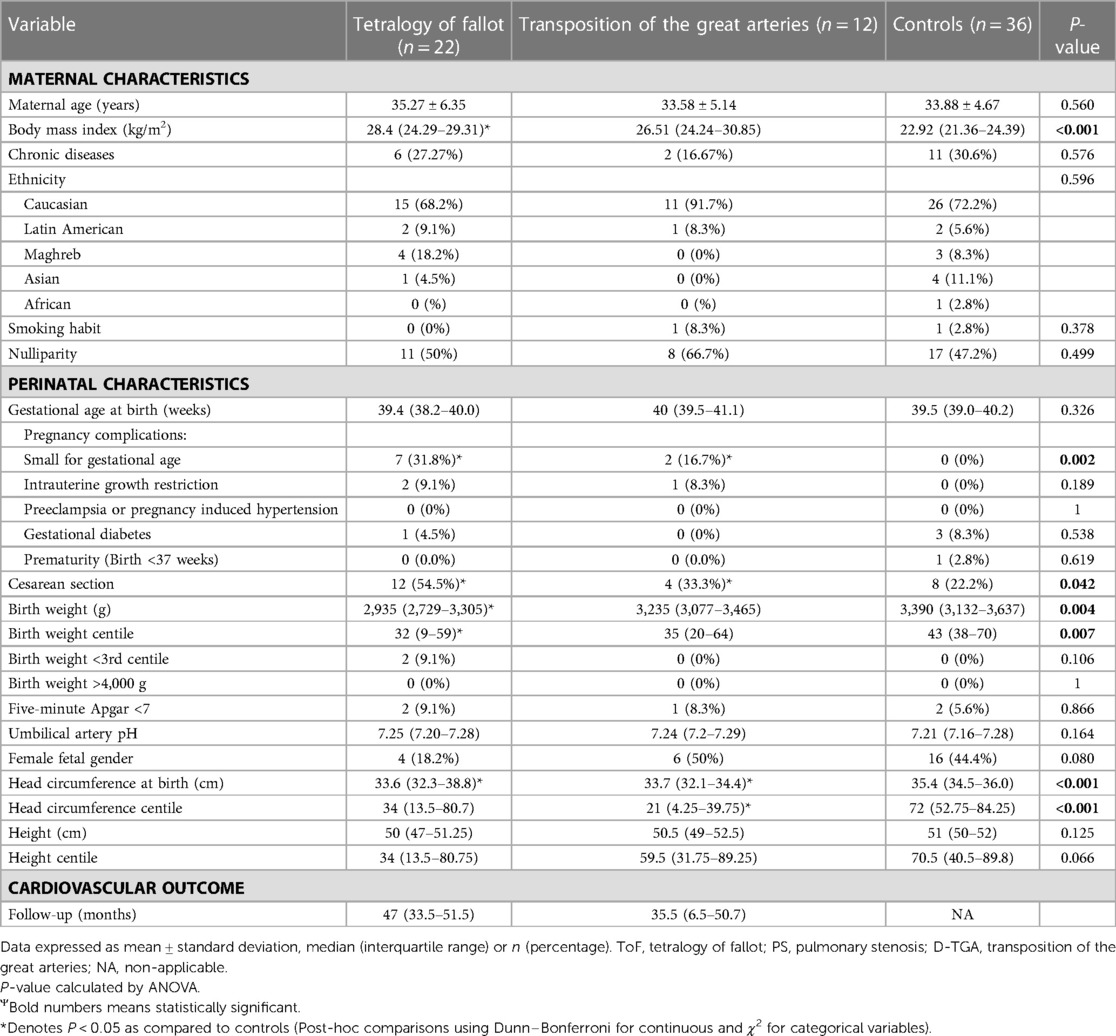
Table 1. Maternal characteristics and perinatal outcome in the study populations.
Table 2 details the results of fetal ultrasound in the study populations. Interestingly, there were no significant differences in estimated fetal weight or head circumference at the time of ultrasound. There were also no differences in uterine or umbilical-fetal and ductus venosus Doppler between the three groups.
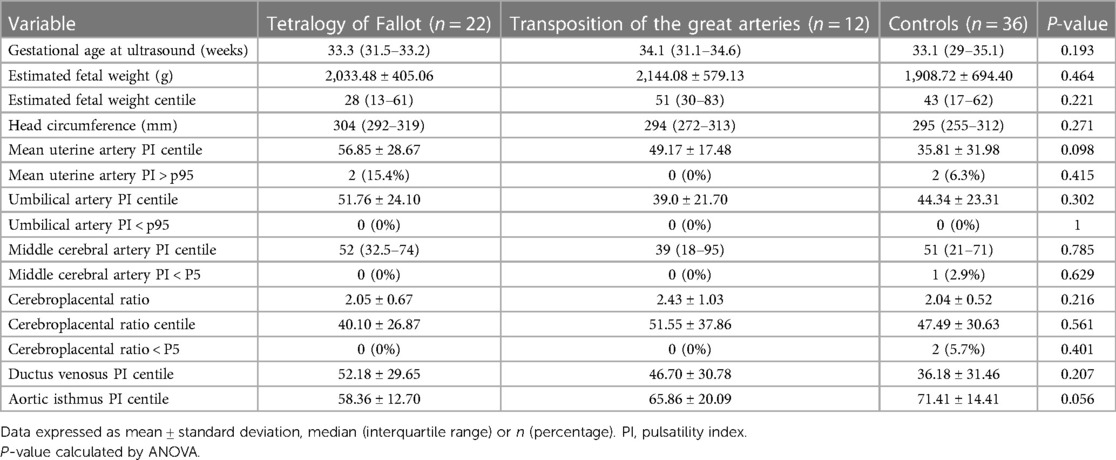
Table 2. Feto-placental ultrasound in the study populations.
3.2. Cord blood biomarkers
Results of cord blood biomarkers in ToF, D-TGA and control-groups are presented in Table 3 and Figure 2. Concentrations of cord blood angiogenic factors including PlGF, sFlt1 and sFlt1/PlGF ratio, did not show significant differences among the study populations. Compared with the controls, ToF fetuses presented a marked increase in cord blood concentrations of TGFβ. Troponin showed a non-significant tendency to higher concentrations in the D-TGA group (Figure 2).
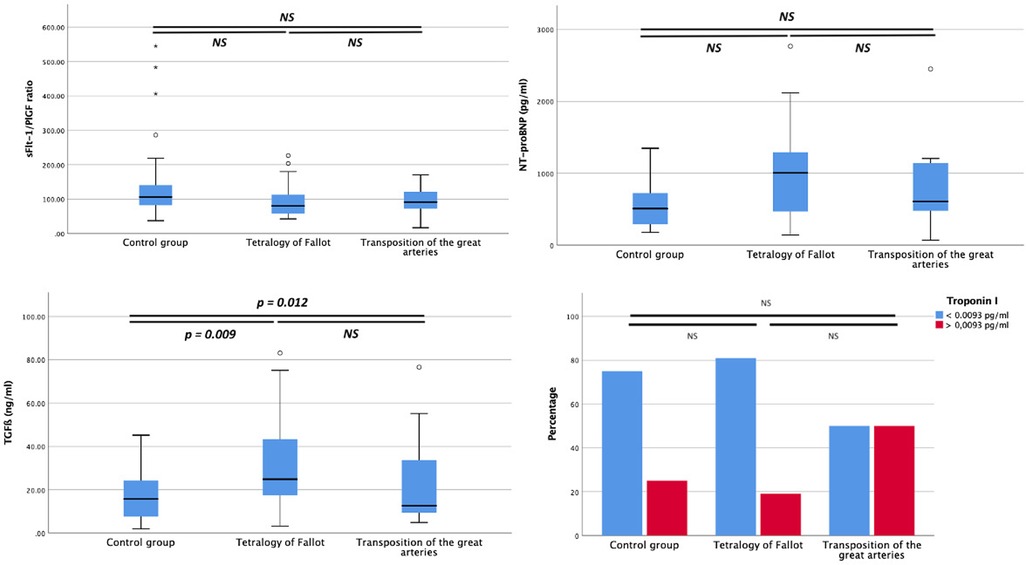
Figure 2. Umbilical cord concentrations of tyrosine kinase-1/placental growth factor (sFlt-1/PlGF) ratio, N-terminal precursor of B-type natriuretic peptide, transforming growth factor ß (TGFß) and percentage of fetuses with troponin I positive (considered positive if concentration >0.0093 pg/ml which represents 75th centile in the control population), in fetuses with tetralogy of fallot, transposition of the great arteries and in normal fetuses. P < 0.05 is considered statistically significant. NS: not significant.

Table 3. Concentrations of biomarkers in cord blood the study populations.
Cord blood biomarkers were not correlated with any obstetric ultrasound parameter, such us umbilical artery, middle cerebral artery and aortic isthmus PI, nor with any perinatal outcome including mode of delivery, estimated fetal weight, head circumference, umbilical artery pH and 5 min Apgar score.
Finally, and as shown in Figure 3, cord blood levels of TGFβ showed a negative correlation with the pulmonary valve diameter z-score (r = −0.576, P = 0.039) and positive correlation with aortic/pulmonary valve ratio (r = 0.611, P = 0.026) in ToF fetuses. No additional correlations were found between cord blood biomarkers and the rest of morphometric and functional echocardiographic parameters evaluated in ToF and D-TGA fetuses, including aortic peak systolic velocity.
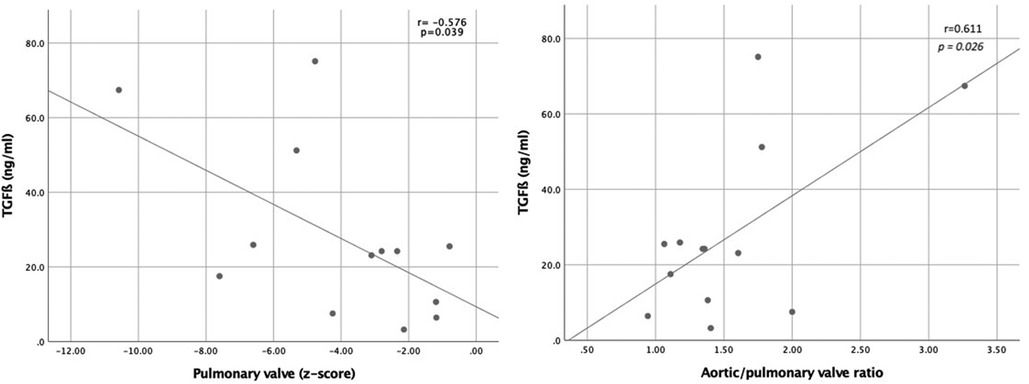
Figure 3. Relationship between umbilical cord concentration of transforming growth factor ß (TGFß) and pulmonary valve diameter z-scoress (left graphic) and aorta/pulmonary ratio (right graphic).
4. Discussion
This study first describes the pattern of different cord blood biomarkers in a cohort of fetuses diagnosed with isolated ToF and D-TGA. Our main findings are: (1) TGFβ is significantly increased in ToF from fetal stage and (2) cord blood TGFβ levels correlate with the severity of the prenatal right ventricular outflow tract obstruction. Only a few prior studies have evaluated cord blood cardiovascular biomarkers in fetuses with CHD with conflicting results. Differences in the CHD groups included among the studies, together with their small sample size, precludes direct comparison of results. A series of 39 fetuses with a mixed group of CHD, which included some cases with conotruncal anomalies reported an anti-angiogenic pattern with increased cord blood sFlt-1 levels (6). On the contrary, a prior study by our group, evaluating 45 fetuses with left-CHD, found only modestly decreased PlGF in the left-CHD group compared to normal fetuses, and markedly decreased sFlt1 only in fetuses with univentricular left-CHD conferring a proangiogenic profile of PlGF and SFlt1 in the poor prognostic group (7). In our study, no differences were found in cord blood levels of PlGF and sFlt1 among the study groups. Given that sFlt1 is downregulated by hypoxia (35), our results in conotruncal CHD suggest that there is little ventricular hypoxic damage in utero in these cyanotic CHD. Further studies are needed to better define which groups of CHD are related to abnormal angiogenesis at the cardiac level and its possible relationship with a concomitant deficient placental angiogenesis (36).
Several studies have reported cord blood NT-proBNP to be elevated in CHD, including 10 cases with mixed CHD (12), 15 fetuses with functional single ventricle associated to neonatal death (10), 16 fetuses with univentricular left-CHD (7) and 6 cases with non-immune hydrops of cardiac origin (10). Although these studies group a limited number of cases, the results are consistent with prior data reporting elevated NT-proBNP in pediatric patients (37) with heart failure, indicating that NT-proBNP is a useful predictor in the setting of severe cardiac anomalies. In our study, NT-proBNP was slightly elevated in the ToF group and preserved in D-TGA cases, which is in accordance with the favorable biventricular outcome and lack of major postnatal complications of our series.
Finally, there is very limited data on Troponin I behavior in fetuses with CHD. We previously reported positive cord blood Troponin I to be more frequent in the group of fetuses with left-CHD with favorable cardiac outcome (7). In the present study, a higher proportion of fetuses with D-TGA presented positive values above the 75th centile (Figure 2), but this difference was not significant possibly due to the limited number of cases. Troponin I is a very sensitive biomarker for endocardial hypoxia and myocardial damage. It has also been found to be elevated in newborns requiring NICU admission (38), in neonates with acidemia (39) and in fetuses with intrauterine growth restriction (40). Thus, larger populations studies are needed to better describe the profile of all these biomarkers not only in different groups of CHD but also in clinical conditions associated with cardiac dysfunction.
4.1. Increased cord blood TGFß in ToF compared with D-TGA
This is the first prenatal report of increased cord blood TGFβ concentrations in ToF. This increase may be explained by different mechanisms. First, TGFβ has been identified as a primary factor responsible for cardiovascular fibrosis (41) and upregulation of TGFβ signaling has been shown to be associated with pro-fibrotic molecular signaling in cardiac pressure overload (42). In this regard, limited data is available on blood flow mechanics and its effect on biventricular remodeling in fetal ToF (43). Nonetheless, a recent computational model evaluating fluid dynamics in fetuses with ToF has shown that although biventricular pressure is equalized by the presence of the ventricular septal defect, biventricular pressure is globally elevated in ToF compared to normal hearts leading to mild right ventricle hypertrophy in fetal life (44). These findings could plausibly explain the higher levels of TGFβ in the ToF group. Furthermore, the ventricular walls around the ventricular septal defect consistently experienced high stress due to a shear flow effect, a mechanism which has also been described to induce cardiovascular tissue growth and remodeling (45).
Secondly, in normal fetal circulation there is a preferential shunting across the foramen ovale that comprises 30% of the cardiac output (46). However, tricuspid flow has been described to be increased in ToF (44), as a lower resistance alternative to the foramen ovale. As such, some of the right atrial flow is derived through the right ventricle and the ventricular septal defect instead of flowing through the foramen ovale, further contributing to the increased endothelial shear stress at the ventricular septal defect.
Finally, TGFβ has also a central role in vascular morphogenesis and extracellular matrix homeostasis, thus there is a growing interest to better understand its contribution to vascular remodeling. Altered TGFβ signaling has been reported in bicuspid aortopathy as a key component in the pathogenesis of thoracic aneurysms (47) as well as in Marfan syndrome, in which circulating levels of TGFβ are correlated with aortic root dilation (48). Moreover, overexpression of TGFβ in the ascending aorta has been described in patients with ToF, tricuspid atresia and double-outlet right ventricle in association with abnormal elastic fibers. Interestingly, increased TGFβ levels have been recently found in a study evaluating adolescents and young adults with TOF after surgery in comparison with controls (14). TGFβ was also slightly elevated after atrial switch operation in corrected TGA and Fontan procedures but was preserved after arterial switch surgery in D-TGA. These data suggest that different mechanisms may be involved in the neo-aortic root dilation that progressively occurs in repaired D-TGA compared to other CHD. Our data, showing similar results in fetuses with ToF and D-TGA, reinforce the hypothesis that an underlying lesion of the aorta may already be present in ToF from very early stages of development. In fact, a decreased aortic compliance, evaluated by fetal echocardiography, has already been reported in fetuses with Marfan syndrome and ToF compared to normal fetuses (49). Therefore, future studies evaluating fetal aortic characteristics in different CHD are warrantied.
4.2. TGFß correlates with the severity of the right ventricle obstruction in ToF
Prior studies have demonstrated a positive correlation between circulating levels of TGFβ and aortic sinus dimension in patients with repaired-ToF (14). Moreover, TGFβ levels have also been correlated with the aortic stiffness evaluated by echocardiography in patients with ToF before the surgical repair (15). Our data are consistent with these findings. As shown in Figure 3, TGFβ concentration showed a negative correlation with the pulmonary valve diameter and a positive correlation with aortic/pulmonary valve ratio in ToF fetuses. Thus, we could hypothesize that increasing right ventricular obstruction severity results in progressive aortic volume overload, which may be associated with a more pronounced deleterious hemodynamic effect and higher TGFβ levels. However, we could not demonstrate any correlation between TGFβ levels and fetal right ventricular morphometry and functionalism, assessed by the sphericity index and tricuspid annular-plane systolic excursion, respectively; nor with peak pulmonary/aortic systolic velocity, findings that require to be conformation with a larger number of cases.
In agreement with previous reports, ToF-newborns had a significantly lower birth weight compared to D-TGA and control groups (50). Additionally, head circumference perimeter at birth was also significantly reduced in both conotruncal CHD groups (51). However, cord blood biomarkers were neither correlated with any ultrasound parameter and perinatal outcome. Likewise, no cord blood biomarker was correlated with any echocardiographic parameter in the D-TGA and control groups. However, these results may be limited by the small sample size of our study.
4.3. Strengths and limitations
To our knowledge, this is the first study to perform a comprehensive assessment of cord blood cardiac biomarkers profile in a specific series of fetuses diagnosed with conotruncal anomalies. It is also the first study to identify increased cord blood TGFβ concentrations in ToF and its correlation with the severity of right ventricular outflow tract obstruction.
However, this is an exploratory study and, therefore, future studies are necessary to confirm our findings and subsequently evaluate the potential clinical applicability of TGFβ in the prognostic evaluation of ToF. The main limitation of our study is the limited number of cases, especially in the D-TGA group. However, the group of ToF is quite homogeneous since most of the cases correspond to ToF with pulmonary stenosis. Although cord blood biomarkers concentrations were analyzed after adjustment for identified confounders we recognize that additional confounders might exist. Finally, we are aware that we have neither the weight of the placenta at birth nor a placental biopsy, which could also provide relevant information.
5. Conclusions
This study newly describes increased cord blood TGFβ concentrations in ToF compared to D-TGA and normal fetuses. Moreover, we demonstrate that TGFβ levels correlate with the severity of right ventricle outflow obstruction. These novel findings open a window of research opportunities into new prognostic and potential preventive strategies. For this, larger multicenter studies, including enough cases in each category of conotruncal anomalies and other groups of CHD, both in fetal and postnatal stages, are warranted. Additionally, the study of these cardiovascular biomarkers in maternal blood and as well as in the amniotic fluid would allow to expand their potential clinical applicability to earlier stages of gestation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee Hospital Clínic de Barcelona (Reg. HCB/2019/0540). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, IS, OG, MB and FC; methodology, IS, LN, OG and FC; software, LN; validation, IS and LG; formal analysis, LN, IS, OG and FC; investigation, OG, LN, IS, LG, NI, MP, NM, MCE, JST, JMM, MB and FC; resources OG, LN, IS, LG, NI, MP, NM, MCE, JST, JMM, MB and FC; data curation, LN, IS; writing—original draft preparation, OG; writing—review and editing, OG, LN, IS, LG, NI, MP, NM, MCE, JST, JMM, MB and FC; visualization, LN; supervision, OG, MB and FC; project administration, OG, MB and FC; funding acquisition, LN, OG, JMM, MB and FC. All authors contributed to the article and approved the submitted version.
Funding
The research leading to these results has received funding from Hospital Clinic de Barcelona (Ajut Josep Font 2015 and Premi Emili Letang 2019, Barcelona, Spain), Instituto de Salud Carlos III (ISCIII) (PI15/00263, PI17/00675, PI20/00246, INT21/00027) co-funded by the European Union, Cerebra Foundation for the Brain Injured Child (Carmarthen, Wales, UK), Fundació La Marató de TV3 (Ref 202016-30-31), and the Maternal and Child Health and Development Network (SAMID), RD16/0022/0015. Additionally, we would like to thank the Fundació Jesús Serra of the Grup Catalana Occident for the Fundació Jesús Serra Research Prize in the Clinical category awarded to the Researcher Fatima Crispi in its 4th edition for the project titled “Cardiovascular prevention from fetal life: benefits of Mediterranean diet during gestation”.
Acknowledgments
We would like to thank Biobanks of Clínic-IDIBAPS and Fundació Sant Joan de Déu for the valuable management of samples.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. International Society of Ultrasound in Obstetrics and Gynecology null, Carvalho JS, Allan LD, Chaoui R, Copel JA, DeVore GR, Hecher K, et al. ISUOG practice guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol. (2013) 41(3):348–59. doi: 10.1002/uog.12403
2. Shinebourne EA, Babu-Narayan SV, Carvalho JS. Tetralogy of fallot: from fetus to adult. Heart. (2006) 92(9):1353–9. doi: 10.1136/hrt.2005.061143
3. Donofrio MT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American heart association. Circulation. (2014) 129(21):2183–242. doi: 10.1161/01.cir.0000437597.44550.5d
4. Iwama H, Uemura S, Naya N, Imagawa KI, Takemoto Y, Asai O, et al. Cardiac expression of placental growth factor predicts the improvement of chronic phase left ventricular function in patients with acute myocardial infarction. J Am Coll Cardiol. (2006) 47(8):1559–67. doi: 10.1016/j.jacc.2005.11.064
5. Maglione D, Guerriero V, Viglietto G, Delli-Bovi P, Persico MG. Isolation of a human placenta cDNA coding for a protein related to the vascular permeability factor. Proc Natl Acad Sci U S A. (1991) 88(20):9267–71. doi: 10.1073/pnas.88.20.9267
6. Llurba E, Sánchez O, Ferrer Q, Nicolaides KH, Ruíz A, Domínguez C, et al. Maternal and foetal angiogenic imbalance in congenital heart defects. Eur Heart J. (2014) 35(11):701–7. doi: 10.1093/eurheartj/eht389
7. Soveral I, Guirado L, Escobar-Diaz MC, Alcaide MJ, Martínez JM, Rodríguez-Sureda V, et al. Cord blood cardiovascular biomarkers in left-sided congenital heart disease. J Clin Med. (2022) 11(23):7119. doi: 10.3390/jcm11237119
8. Mitchell ME, Sander TL, Klinkner DB, Tomita-Mitchell A. The molecular basis of congenital heart disease. Semin Thorac Cardiovasc Surg. (2007) 19(3):228–37. doi: 10.1053/j.semtcvs.2007.07.013
9. Agewall S, Giannitsis E, Jernberg T, Katus H. Troponin elevation in coronary vs. non-coronary disease. Eur Heart J. (2011) 32(4):404–11. doi: 10.1093/eurheartj/ehq456
10. Lee SM, Kwon JE, Song SH, Kim GB, Park JY, Kim BJ, et al. Prenatal prediction of neonatal death in single ventricle congenital heart disease. Prenat Diagn. (2016) 36(4):346–52. doi: 10.1002/pd.4787
11. Irmak K, Tüten N, Karaoglu G, Madazli R, Tüten A, Malik E, et al. Evaluation of cord blood creatine kinase (CK), cardiac troponin T (cTnT), N-terminal-pro-B-type natriuretic peptide (NT-proBNP), and s100B levels in nonreassuring foetal heart rate. J Matern Fetal Neonatal Med. (2021) 34(8):1249–54. doi: 10.1080/14767058.2019.1632285
12. Kocylowski RD, Dubiel M, Gudmundsson S, Sieg I, Fritzer E, Alkasi O, et al. Biochemical tissue-specific injury markers of the heart and brain in postpartum cord blood. Am J Obstet Gynecol. (2009) 200(3):273.e1–25. doi: 10.1016/j.ajog.2008.10.009
13. Ren LL, Li XJ, Duan TT, Li ZH, Yang JZ, Zhang YM, et al. Transforming growth factor-β signaling: from tissue fibrosis to therapeutic opportunities. Chem Biol Interact. (2023) 369:110289. doi: 10.1016/j.cbi.2022.110289
14. Cheung YF, Chow PC, So EKF, Chan KW. Circulating transforming growth factor-β and aortic dilation in patients with repaired congenital heart disease. Sci Rep. (2019) 9(1):162. doi: 10.1038/s41598-018-36458-1
15. Seki M, Kurishima C, Saiki H, Masutani S, Arakawa H, Tamura M, et al. Progressive aortic dilation and aortic stiffness in children with repaired tetralogy of fallot. Heart Vessels. (2014) 29(1):83–7. doi: 10.1007/s00380-013-0326-1
16. Robinson HP, Sweet EM, Adam AH. The accuracy of radiological estimates of gestational age using early fetal crown-rump length measurements by ultrasound as a basis for comparison. Br J Obstet Gynaecol. (1979) 86(7):525–8. doi: 10.1111/j.1471-0528.1979.tb10804.x
17. Rodríguez-López M, Cruz-Lemini M, Valenzuela-Alcaraz B, Garcia-Otero L, Sitges M, Bijnens B, et al. Descriptive analysis of different phenotypes of cardiac remodeling in fetal growth restriction. Ultrasound Obstet Gynecol. (2017) 50(2):207–14. doi: 10.1002/uog.17365
18. Crispi F, Bijnens B, Figueras F, Bartrons J, Eixarch E, Le Noble F, et al. Fetal growth restriction results in remodeled and less efficient hearts in children. Circulation. (2010) 121(22):2427–36. doi: 10.1161/CIRCULATIONAHA.110.937995
19. Barker DJP. Adult consequences of fetal growth restriction. Clin Obstet Gynecol. (2006) 49(2):270–83. doi: 10.1097/00003081-200606000-00009
20. Mert MK, Satar M, Özbarlas N, Yaman A, Özgünen FT, Asker HS, et al. Troponin T and NT ProBNP levels in gestational, type 1 and type 2 diabetic mothers and macrosomic infants. Pediatr Cardiol. (2016) 37(1):76–83. doi: 10.1007/s00246-015-1242-1
21. Patey O, Carvalho JS, Thilaganathan B. Perinatal changes in fetal cardiac geometry and function in diabetic pregnancy at term. Ultrasound Obstet Gynecol. (2019) 54(5):634–42. doi: 10.1002/uog.20187
22. García-Otero L, López M, Gómez O, Goncé A, Bennasar M, Martínez JM, et al. Zidovudine treatment in HIV-infected pregnant women is associated with fetal cardiac remodelling. AIDS. (2016) 30(9):1393–401. doi: 10.1097/QAD.0000000000001066
23. Figueras F, Gratacós E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn Ther. (2014) 36(2):86–98. doi: 10.1159/000357592
24. Yagel S, Cohen SM, Achiron R. Examination of the fetal heart by five short-axis views: a proposed screening method for comprehensive cardiac evaluation. Ultrasound Obstet Gynecol. (2001) 17(5):367–9. doi: 10.1046/j.1469-0705.2001.00414.x
25. Lee W, Carvalho JS, Chaoui R, Copel J, Hecher K, Paladini D. Cardiac screening examination of the fetus: guidelines for performing the “basic” and “extended basic” cardiac scan. Ultrasound Obstet Gynecol. (2006) 27(1):107–13. doi: 10.1002/uog.2677
26. Bhide A, Acharya G, Bilardo CM, Brezinka C, Cafici D, Hernandez-Andrade E, et al. ISUOG Practice guidelines: use of Doppler ultrasonography in obstetrics. Ultrasound Obstet Gynecol. (2013) 41(2):233–9. doi: 10.1002/uog.12396
27. Hecher K, Campbell S, Snijders R, Nicolaides K. Reference ranges for fetal venous and atrioventricular blood flow parameters. Ultrasound Obstet Gynecol. (1994) 4(5):381–90. doi: 10.1046/j.1469-0705.1994.04050381.x
28. Hadlock FP, Harrist RB, Shah YP, King DE, Park SK, Sharman RS. Estimating fetal age using multiple parameters: a prospective evaluation in a racially mixed population. Am J Obstet Gynecol. (1987) 156(4):955–7. doi: 10.1016/0002-9378(87)90365-6
29. Figueras F, Meler E, Iraola A, Eixarch E, Coll O, Figueras J, et al. Customized birthweight standards for a Spanish population. Eur J Obstet Gynecol Reprod Biol. (2008) 136(1):20–4. doi: 10.1016/j.ejogrb.2006.12.015
30. Baschat AA, Gembruch U. The cerebroplacental Doppler ratio revisited. Ultrasound Obstet Gynecol. (2003) 21(2):124–7. doi: 10.1002/uog.20
31. García-Otero L, Soveral I, Sepúlveda-Martínez Á, Rodriguez-López M, Torres X, Guirado L, et al. Reference ranges for fetal cardiac, ventricular and atrial relative size, sphericity, ventricular dominance, wall asymmetry and relative wall thickness from 18 to 41 gestational weeks. Ultrasound Obstet Gynecol. (2021) 58(3):388–97. doi: 10.1002/uog.23127
32. García-Otero L, Gómez O, Rodriguez-López M, Torres X, Soveral I, Sepúlveda-Martínez Á, et al. Nomograms of fetal cardiac dimensions at 18–41 weeks of gestation. Fetal Diagn Ther. (2020) 47(5):387–98. doi: 10.1159/000494838
33. Schneider C, McCrindle BW, Carvalho JS, Hornberger LK, McCarthy KP, Daubeney PEF. Development of z-scores for fetal cardiac dimensions from echocardiography. Ultrasound Obstet Gynecol. (2005) 26(6):599–605. doi: 10.1002/uog.2597
34. Cruz-Lemini M, Crispi F, Valenzuela-Alcaraz B, Figueras F, Sitges M, Gómez O, et al. Value of annular M-mode displacement vs tissue Doppler velocities to assess cardiac function in intrauterine growth restriction. Ultrasound Obstet Gynecol. (2013) 42(2):175–81. doi: 10.1002/uog.12374
35. Ikeda T, Sun L, Tsuruoka N, Ishigaki Y, Yoshitomi Y, Yoshitake Y, et al. Hypoxia down-regulates sFlt-1 (sVEGFR-1) expression in human microvascular endothelial cells by a mechanism involving mRNA alternative processing. Biochem J. (2011) 436(2):399–407. doi: 10.1042/BJ20101490
36. Snoep MC, Aliasi M, van der Meeren LE, Jongbloed MRM, DeRuiter MC, Haak MC. Placenta morphology and biomarkers in pregnancies with congenital heart disease - A systematic review. Placenta. (2021) 112:189–96. doi: 10.1016/j.placenta.2021.07.297
37. Di Angelantonio E, Chowdhury R, Sarwar N, Ray KK, Gobin R, Saleheen D, et al. B-type natriuretic peptides and cardiovascular risk: systematic review and meta-analysis of 40 prospective studies. Circulation. (2009) 120(22):2177–87. doi: 10.1161/CIRCULATIONAHA.109.884866
38. Mondal T, Ryan PM, Gupta K, Radovanovic G, Pugh E, Chan AKC, et al. Cord-blood high-sensitivity troponin-I reference interval and association with early neonatal outcomes. Am J Perinatol. (2022) 29(14):1548–54. doi: 10.1055/s-0041-1722944
39. Alexandre SM, D’Almeida V, Guinsburg R, Nakamura MU, Tufik S, Moron A. Cord blood cardiac troponin I, fetal Doppler velocimetry, and acid base status at birth. Int J Gynaecol Obstet. (2008) 100(2):136–40. doi: 10.1016/j.ijgo.2007.08.007
40. Perez-Cruz M, Crispi F, Fernández MT, Parra JA, Valls A, Gomez Roig MD, et al. Cord blood biomarkers of cardiac dysfunction and damage in term growth-restricted fetuses classified by severity criteria. Fetal Diagn Ther. (2018) 44(4):271–6. doi: 10.1159/000484315
41. Goumans MJ, Liu Z, ten Dijke P. TGF-beta signaling in vascular biology and dysfunction. Cell Res. (2009) 19(1):116–27. doi: 10.1038/cr.2008.326
42. Dobaczewski M, Chen W, Frangogiannis NG. Transforming growth factor (TGF)-β signaling in cardiac remodeling. J Mol Cell Cardiol. (2011) 51(4):600–6. doi: 10.1016/j.yjmcc.2010.10.033
43. Jatavan P, Tongprasert F, Srisupundit K, Luewan S, Traisrisilp K, Tongsong T. Quantitative cardiac assessment in fetal tetralogy of fallot. J Ultrasound Med. (2016) 35(7):1481–8. doi: 10.7863/ultra.15.08017
44. Wiputra H, Chen CK, Talbi E, Lim GL, Soomar SM, Biswas A, et al. Human fetal hearts with tetralogy of fallot have altered fluid dynamics and forces. Am J Physiol Heart Circ Physiol. (2018) 315(6):H1649–59. doi: 10.1152/ajpheart.00235.2018
45. Groenendijk BCW, Hierck BP, Gittenberger-De Groot AC, Poelmann RE. Development-related changes in the expression of shear stress responsive genes KLF-2, ET-1, and NOS-3 in the developing cardiovascular system of chicken embryos. Dev Dyn. (2004) 230(1):57–68. doi: 10.1002/dvdy.20029
46. Sun L, van Amerom JFP, Marini D, Portnoy S, Lee FT, Saini BS, et al. MRI Characterization of hemodynamic patterns of human fetuses with cyanotic congenital heart disease. Ultrasound Obstet Gynecol. (2021) 58(6):824–36. doi: 10.1002/uog.23707
47. El-Hamamsy I, Yacoub MH. Cellular and molecular mechanisms of thoracic aortic aneurysms. Nat Rev Cardiol. (2009) 6(12):771–86. doi: 10.1038/nrcardio.2009.191
48. Franken R, den Hartog AW, de Waard V, Engele L, Radonic T, Lutter R, et al. Circulating transforming growth factor-β as a prognostic biomarker in Marfan syndrome. Int J Cardiol. (2013) 168(3):2441–6. doi: 10.1016/j.ijcard.2013.03.033
49. Taketazu M, Sugimoto M, Saiki H, Ishido H, Masutani S, Senzaki H. Developmental changes in aortic mechanical properties in normal fetuses and fetuses with cardiovascular disease. Pediatr Neonatol. (2017) 58(3):245–50. doi: 10.1016/j.pedneo.2016.05.004
50. Ghanchi A, Rahshenas M, Bonnet D, Derridj N, LeLong N, Salomon LJ, et al. Prevalence of growth restriction at birth for newborns with congenital heart defects: a population-based prospective cohort study EPICARD. Front Pediatr. (2021) 9:676994. doi: 10.3389/fped.2021.676994
51. Escobar-Diaz MC, Pérez-Cruz M, Arráez M, Cascant-Vilaplana MM, Albiach-Delgado A, Kuligowski J, et al. Brain oxygen perfusion and oxidative stress biomarkers in fetuses with congenital heart disease-A retrospective, case-control pilot study. Antioxidants. (2022) 11(2):299. doi: 10.3390/antiox11020299
Keywords: transforming growth factor beta, Troponin I, angiogenic factors, congenital heart disease, fetal echocardiography, NT-pro-brain natriuretic peptide, tetralogy of fallot, transposition of the great arteries
Citation: Gómez O, Nogué L, Soveral I, Guirado L, Izquierdo N, Pérez-Cruz M, Masoller N, Escobar MC, Sanchez-de-Toledo J, Martínez-Crespo JM, Bennasar M and Crispi F (2023) Cord blood cardiovascular biomarkers in tetralogy of fallot and D-transposition of great arteries. Front. Pediatr. 11:1151814. doi: 10.3389/fped.2023.1151814
Received: 26 January 2023; Accepted: 10 April 2023;
Published: 28 April 2023.
Edited by:
Biagio Castaldi, University of Padua, ItalyReviewed by:
John Simpson, Guy’s and St Thomas’ NHS Foundation Trust, United KingdomMonique Haak, Leiden University Medical Center (LUMC), Netherlands
© 2023 Gómez, Nogué, Soveral, Guirado, Izquierdo, Pérez-Cruz, Masoller, Escobar, Sanchez-de-Toledo, Martínez-Crespo, Bennasar and Crispi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Olga Gómez b2dvbWV6QGNsaW5pYy5jYXQ=
†These authors share last authorship