
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 22 August 2023
Sec. Pediatric Immunology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1137051
This article is part of the Research Topic Multisystem Inflammatory Syndrome in Children View all 10 articles
 Francesco Licciardi1
Francesco Licciardi1 Carlotta Covizzi1*
Carlotta Covizzi1* Marta Dellepiane1
Marta Dellepiane1 Nicole Olivini2
Nicole Olivini2 Maria Vincenza Mastrolia3Andrea Lo Vecchio4Viviana Monno5Maria Tardi6
Maria Vincenza Mastrolia3Andrea Lo Vecchio4Viviana Monno5Maria Tardi6 Angela Mauro7Maria Alessio4
Angela Mauro7Maria Alessio4 Giovanni Filocamo8
Giovanni Filocamo8 Marco Cattalini9
Marco Cattalini9 Andrea Taddio10
Andrea Taddio10 Roberta Caorsi11
Roberta Caorsi11 Gian Luigi Marseglia12
Gian Luigi Marseglia12 Francesco La Torre5
Francesco La Torre5 Andrea Campana2
Andrea Campana2 Gabriele Simonini3
Gabriele Simonini3 Angelo Ravelli11
Angelo Ravelli11 Davide Montin1
Davide Montin1
Background: The treatment of multisystem inflammatory syndrome in children unresponsive to first-line therapies (IVIG and/or steroids) is challenging. The effectiveness of IL-1 receptor antagonist, anakinra, is debated.
Patients and methods: We conducted an anonymous retrospective multicenter study on MIS-C patients treated with anakinra in Italy from January 2020 to February 2021. Our study outcomes included the percentage of patients who required further therapeutic step-up, the percentage of patients who experienced fever resolution within 24 h and a reduction of CRP by half within 48 h, and the percentage of patients who developed Coronary Artery Anomalies (CAA) during follow-up.
Results: 35 cases of MIS-C were treated in 10 hospitals. Of these, 13 patients started anakinra while in the ICU, and 22 patients started anakinra in other wards. 25 patients (71.4%) were treated with corticosteroids at a starting dose 2–30 mg/Kg/day plus IVIG (2 g/Kg), 10 patients (28.6%) received only corticosteroids without IVIG. Anakinra was administered intravenously to all patients in Group A (mean dose 8 mg/Kg/day), and subcutaneously in Group B (mean dose 4 mg/Kg/day). Only two patients required further treatment step-up and no patients developed CAA after receiving anakinra. The most commonly observed side effect was an increase in ALT, occurring in 17.1% of patients.
Conclusions: In this retrospective cohort of severe MIS-C patients treated with anakinra we report favorable clinical outcomes with a low incidence of side effects. The simultaneous use of steroids ± IVIG in these patients hinders definitive conclusions regarding the need of IL-1 inhibition in MIS-C treatment.
MIS-C is a severe complication of SARS-CoV2 infection in children, it often results in high rates of ICU admission, mainly due to acute cardiac insufficiency. Although most patients do not develop sequelae, in the acute phase MIS-C can be a life-threatening disease, making timely and appropriate treatment critical (1). Currently, the primary treatment options for MIS-C are IVIG and steroids. Numerous studies have established that MIS-C results from a cytokine storm involving various cytokines (2, 3). Therefore, biologic drugs, particularly the IL-1 receptor antagonist (anakinra), have shown promise in treating MIS-C, as evidenced by small case series. However, data on the overall efficacy and safety of anakinra in MIS-C treatment is still lacking (4–9).
We conducted an anonymous retrospective multicenter study on patients who met the criteria for MIS-C and were treated with anakinra in Italy from January 4th, 2020 to February 28th, 2021. We included patients who met the WHO preliminary case definition (10) with recent biological evidence of SARS-CoV2 infection, either through serology or positive RT-PCR swab tests within six weeks prior to admission. The patients were divided into two groups: Group A included those who began anakinra treatment in the ICU, while Group B included patients treated in non-ICU pediatric wards. We collected clinical data at symptom onset, at the start of anakinra treatment, previous and concurrent treatments, along with reasons why anakinra was prescribed, dosage, and route of administration. The reasons for starting anakinra, according to the prescriber, included: worsening of cardiac dysfunction (defined as a reduction of EF to less than 50% or persistent hypotension requiring inotrope support), persistent clinical symptoms (persistence of fever with or without persistent mucocutaneous manifestations), or abnormal laboratory results (failure to reduce CRP or progressive increase of ferritin 24–36 h) despite treatment with steroid ± IVIG. We considered as outcomes the percentage of patients who required further therapeutic step-up, the percentage of patients with fever resolution within 24 h and CRP reduction by half within 48 h, and the percentage of patients with Coronary Artery Anomalies (CAA) during follow-up. We defined CAA based on the 2017 AHA Guidelines for Kawasaki Disease (11). The presence of CAA was screened at anakinra start, 2 weeks and 6–8 weeks after disease onset. In addition, we calculated the halving time of pro-BNP/BNP and CRP for each patient.
Overall, 35 cases of MIS-C were treated in 10 hospitals throughout Italy and met the inclusion criteria, with 13 in Group A and 22 in Group B. Table 1 displays baseline clinical and laboratory features, while Table 2 provides information on first-line therapies and dosing, timing and reasons for anakinra initiation, anakinra dose, and method of administration. 25 patients were treated with corticosteroids at a starting dose 2–30 mg/Kg/day plus IVIG (2 g/Kg), 10 patients received only corticosteroids without IVIG. In Group A, cardiac function deterioration was the most common reason for starting anakinra (76.9%), while in Group B, anakinra was mostly started due to persistent clinical symptoms that were unresponsive to IVIG and/or steroids (54.5%). Of the 13 cases in Group A, 11 were admitted to ICU and initiated anakinra within 48 h of hospitalization. In all these patients anakinra was started less then 36 h after the start of steroid and/or IVIG. Anakinra was administered intravenously to all patients in Group A, with a mean dose of 8 mg/Kg/day. Meanwhile, the majority of patients in Group B (72.7%) received the drug via subcutaneous route, with a mean dose of 4 mg/Kg/day. Table 3 outlines the outcomes and side effects experienced by these patients. In summary, only two patients required further treatment step-up: one patient in Group A needed an increase in methylprednisolone dose, while another patient in Group B required IVIG. No patients developed CAA after receiving anakinra. The most commonly observed side effect was an increase in ALT with 30.8% of Group A patients and 9.1% of Group B patients experiencing this effect. Only one patient in the study experienced an injection site reaction.
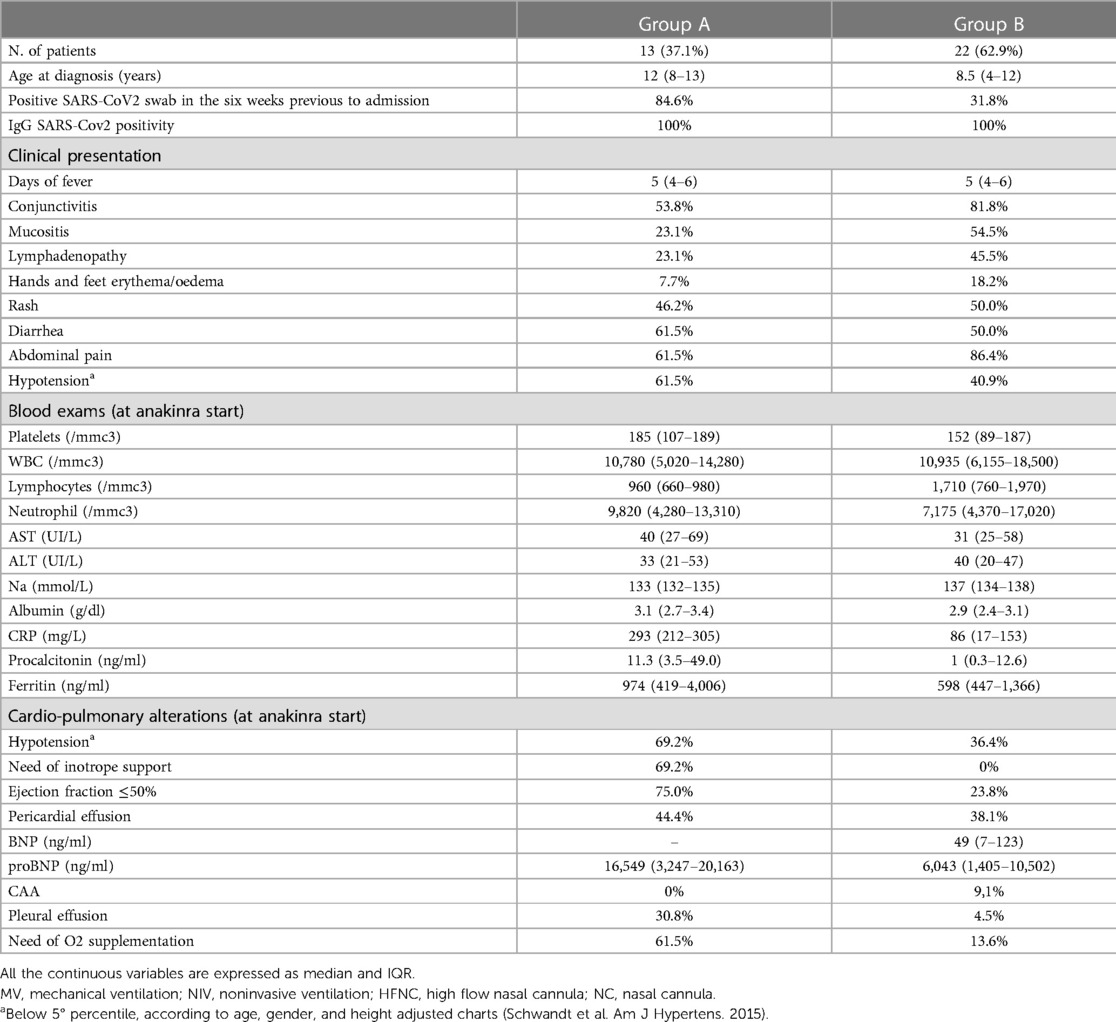
Table 1. Baseline clinical and laboratory features.
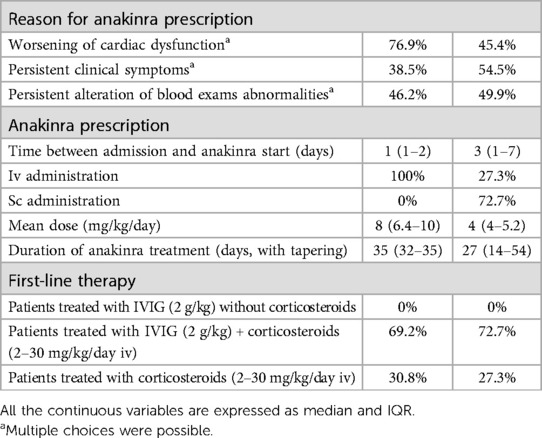
Table 2. Reasons for anakinra start, anakinra dose and route of administration.
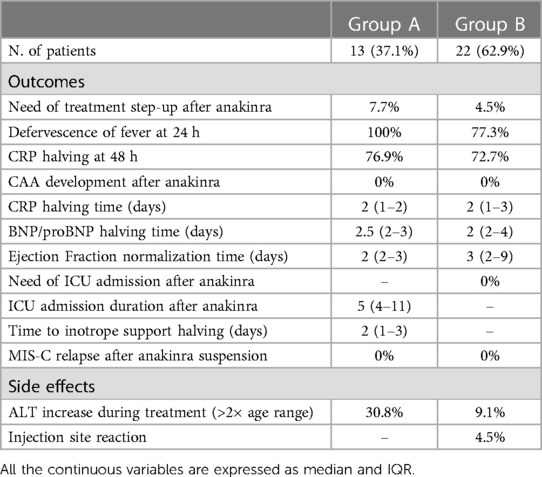
Table 3. Outcomes and side effects.
MIS-C is a life-threatening late complication of SARS-COV2 infection in children. The treatment of MIS-C has been extensively debated over the past few years and is mainly based on the use of IVIG and/or glucocorticoids. According to most international recommendations, (12, 13) anakinra is suggested as a second-line therapy in patients resistant to conventional therapy. These recommendations are based mainly on individual case or small case series. A recent revision by Mastrolia et al. of these published cases found an efficacy of anakinra in 85/87 (97.7%) patients, nevertheless this result is burdened by publication bias and the outcome measures are extremely heterogenous (14). In this report, we describe the outcomes of a large multicenter cohort of MIS-C patients treated with anakinra. In both Italy and the US, anakinra is considered a second-line therapy for MIS-C (12, 13). Therefore, our retrospective cohort includes patients who either had very severe MIS-C at onset or were unresponsive to first-line therapy. Despite this selection bias, the majority of our patients achieved positive clinical and laboratory outcomes. Specifically, 85.7% of patients experienced fever remission within 24 h, while the median CRP and pro-BNP halving time was 2 days. Recently, Çaǧlayan et al. published a retrospective study of 82 MIS-C patients treated with anakinra. Of them, 89.1% were discharged without sequelae, but seven patients died (8.5%). In contrast, none of the patients in our study died. The lower mortality in our cohort may be due to several possible factors, such as a different ethnic background and a higher mean dose of anakinra (5.5 mg/Kg/day vs. 2.7 mg/Kg/day in Çaǧlayan et al.) (9). Our study confirms that anakinra may have a role as a second line treatment after glucocorticoids and/or IVIG. In Group B, only one patient (4.5%) required further therapeutic intervention after starting anakinra, none required admission to the ICU or vasopressor support. The majority experienced rapid fever resolution (77.3% at +24 h) and normalization of EF within an average of three days. It should be highlighted that 10 patients did not receive IVIG prior to or during anakinra treatment. Of these patients, 90% achieved fever remission within 24 h and halved their CRP levels within 48 h when treated with a combination of anakinra and intravenous methylprednisolone, only 1 patient required further therapeutic step-up with IVIG. This suggests that the anakinra and intravenous methylprednisolone combination may be effective even without IVIG. After the first revision of our manuscript, Chang et al. published a multicenter retrospective study analyzing the effect of anakinra therapy in the early phase of MIS-C treatment. The authors compared 121 MIS-C patients treated with anakinra plus IVIG and/or glucocorticoids to 389 propensity-score matched MIS-C patients treated without anakinra, and found that the treatment with anakinra was not associated with significant differences in vasopressor requirement, ventricular dysfunction, or C-reactive protein reduction (15). The results of this recently published paper are partially comparable with ours, in fact Chang et al. only included patients who received anakinra on days 0 or 1 after diagnosis, which matches with only 11 patients in our cohort who were treated early with anakinra in the ICU setting. When comparing this similar subgroup of patients our outcomes were overall better than Chang's. For instance, the mean time to EF recovery was considerably shorter in our cohort (2 vs. 3 days). A possible explanation for this different outcome could be the higher mean dose of anakinra in our cohort (8 vs. 4 mg/Kg/day). It is worth mentioning that anti-IL1Ra autoantibodies have been described in small groups of children with MIS-C, and although their role in MIS-C pathogenesis is still debated, they can reduce free IL1-Ra, thereby possibly antagonizing anakinra and increasing the need for anakinra in MIS-C treatment (16). In accordance with this hypothesis, previous papers report the efficacy of high doses of anakinra in MIS-C (up to 10 mg/Kg/day) (5, 17). With regards to vasopressor support, the outcome considered in the aforementioned paper (% of patients needing vasopressor support at day 3) might not have been sensitive enough to detect the benefit of anakinra. In fact, in our experience, anakinra had a benefit in terms of vasopressor tapering (mean time for halving vasopressor dose was 48 h), but not in terms of early suspension. Finally, it should be highlighted that the incidence of CAA in MIS-C worldwide is between 10%–20%. In 2020, an Italian multicenter survey reported an incidence of 13.2% (12, 18). Interestingly, none of the patients in our cohort developed CAA after receiving anakinra, possibly indicating a protective role of IL-1 inhibition on coronary arteries during the acute phase of the disease, similar to that observed in KD (19).
This study has some limitations. Firstly, the data were collected retrospectively and there was no shared protocol between centers on when and how starting anakinra. The lack of a protocol led to a heterogeneity in timing and dosing between different hospitals. Additionally, the absence of a control group hinders the ability to draw a firm conclusion regarding the benefits of anakinra, particularly at disease onset when anti-IL1 is initiated shortly after steroid use.
In summary, in this retrospective cohort of patients treated with anakinra, we have observed favorable clinical outcomes with a low incidence of side effects, mainly transient ALT elevation. However, it is crucial to note that anakinra was administered in combination with other therapies, primarily steroids, which makes it difficult to draw definitive conclusions about the role of IL-1 inhibition in MIS-C treatment. Our data is not conclusive, especially in the ICU setting where anakinra was used simultaneously with IVIG and steroids.
Prospective randomized trials should be conducted to confirm our findings and determine the optimal timing and dose of anakinra for MIS-C treatment. Additionally, the development of a first-line therapies resistance score, similar to the Kobayashi score for IVIG resistance in Kawasaki Disease, might help identify which patients might benefit from prompt IL-1 inhibition.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Comitato etico interaziendale AOU Città della Salute e della Scienza di Torino—AO Mauriziano—ASL Città di Torino. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
FL: conception and design of the work; analysis and interpretation of data; writing of the manuscript. CC: conception and design of the work; analysis and data collection; writing of the manuscript. MD: analysis and data collection; writing of the manuscript. NO: data collection and critical reviewing of the manuscript. MVM: data collection and critical reviewing of the manuscript. ALV: data collection and critical reviewing of the manuscript. VM: data collection and critical reviewing of the manuscript. MT: data collection and critical reviewing of the manuscript. AM: data collection and critical reviewing of the manuscript. MA: data collection and critical reviewing of the manuscript. GF: data collection and critical reviewing of the manuscript. MC: data collection and critical reviewing of the manuscript. AT: data collection and critical reviewing of the manuscript. RC: data collection and critical reviewing of the manuscript. GLM: data collection and critical reviewing of the manuscript. FLT: data collection and critical reviewing of the manuscript. AC: data collection and critical reviewing of the manuscript. GS: data collection and critical reviewing of the manuscript. AR: data collection and critical reviewing of the manuscript. DM: conception and design of the work; analysis and interpretation of data; critical reviewing of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that this study received funding from SOBI as economic support for the submission; the funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
GF is a consultant for SOBI, GS and MM received an unrestricted educational Grant from SOBI, for a project not related to MIS-C.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Licciardi F, Pruccoli G, Denina M, Parodi E, Taglietto M, Rosati S, et al. SARS-CoV-2-induced Kawasaki-like hyperinflammatory syndrome: a novel COVID phenotype in children. Pediatrics. (2020) 146(2):e20201711. doi: 10.1542/peds.2020-1711
2. Sacco K, Castagnoli R, Vakkilainen S, Liu C, Delmonte OM, Oguz C, et al. Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19. Nat Med. (2022) 28(5):1050–62. doi: 10.1038/s41591-022-01724-3
3. Consiglio CR, Cotugno N, Sardh F, Pou C, Amodio D, Rodriguez L, et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell. (2020) 183(4):968–81.e7. doi: 10.1016/j.cell.2020.09.016
4. Della Paolera S, Valencic E, Piscianz E, Moressa V, Tommasini A, Sagredini R, et al. Case report: use of anakinra in multisystem inflammatory syndrome during COVID-19 pandemic. Front Pediatr. (2020) 8:624248. doi: 10.3389/fped.2020.624248
5. Mastrolia MV, Marrani E, Calabri GB, L’Erario M, Maccora I, Favilli S, et al. Fast recovery of cardiac function in PIMS-TS patients early using intravenous anti-IL-1 treatment. Crit Care Lond Engl. (2021) 25(1):131. doi: 10.1186/s13054-021-03548-y
6. Carducci FIC, De Ioris MA, Agrati C, Carsetti R, Perrotta D, D’Argenio P, et al. Hyperinflammation in two severe acute respiratory syndrome coronavirus 2-infected adolescents successfully treated with the interleukin-1 inhibitor anakinra and glucocorticoids. Front Pediatr. (2020) 8:576912. doi: 10.3389/fped.2020.576912
7. Fouriki A, Fougère Y, De Camaret C, Blanchard Rohner G, Grazioli S, Wagner N, et al. Case report: case series of children with multisystem inflammatory syndrome following SARS-CoV-2 infection in Switzerland. Front Pediatr. (2020) 8:594127. doi: 10.3389/fped.2020.594127
8. Chiotos K, Bassiri H, Behrens EM, Blatz AM, Chang J, Diorio C, et al. Multisystem inflammatory syndrome in children during the coronavirus 2019 pandemic: a case series. J Pediatr Infect Dis Soc. (2020) 9(3):393–8. doi: 10.1093/jpids/piaa069
9. Çaǧlayan Ş, Sönmez HE, Otar Yener G, Baǧlan E, Öztürk K, Ulu K, et al. Anakinra treatment in multisystemic inflammatory syndrome in children (MIS-C) associated with COVID-19. Front Pediatr. (2022) 10:942455. doi: 10.3389/fped.2022.942455
10. Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19. Available at: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescentswith-covid-19
11. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American heart association. Circulation. (2017) 135(17):e927–99. doi: 10.1161/CIR.0000000000000484
12. Cattalini M, Taddio A, Bracaglia C, Cimaz R, Paolera SD, Filocamo G, et al. Childhood multisystem inflammatory syndrome associated with COVID-19 (MIS-C): a diagnostic and treatment guidance from the rheumatology study group of the Italian society of pediatrics. Ital J Pediatr. (2021) 47(1):24. doi: 10.1186/s13052-021-00980-2
13. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 3. Arthritis Rheumatol Hoboken NJ. (2022) 74(4):e1–20. doi: 10.1002/art.42062.
14. Mastrolia MV, Marrani E, Maccora I, Pagnini I, Simonini G. The role of anti-IL-1 treatment in MIS-C patients. Expert Opin Biol Ther. (2022) 22(1):1–5. doi: 10.1080/14712598.2022.2006631
15. Chang JC, Young CC, Muscal E, Sexson Tejtel SK, Newhams MM, Kucukak S, et al. Variation in early anakinra use and short-term outcomes in multisystem inflammatory syndrome in children. Arthritis Rheumatol. (2023) 75(8):1466–76. doi: 10.1002/art.42495
16. Pfeifer J, Thurner B, Kessel C, Fadle N, Kheiroddin P, Regitz E, et al. Autoantibodies against interleukin-1 receptor antagonist in multisystem inflammatory syndrome in children: a multicentre, retrospective, cohort study. Lancet Rheumatol. (2022) 4(5):e329–37. doi: 10.1016/S2665-9913(22)00064-9
17. Brisca G, Consolaro A, Caorsi R, Pirlo D, Tuo G, Campanello C, et al. Timely recognition and early multi-step antinflammatory therapy may prevent ICU admission of patients with MIS-C: proposal for a severity score. Front Pediatr. (2021) 9:783745. doi: 10.3389/fped.2021.783745
Keywords: MIS-C, multisystem inflammatory syndrome, pediatrics, COVID-19, SARS-CoV2
Citation: Licciardi F, Covizzi C, Dellepiane M, Olivini N, Mastrolia MV, Lo Vecchio A, Monno V, Tardi M, Mauro A, Alessio M, Filocamo G, Cattalini M, Taddio A, Caorsi R, Marseglia GL, La Torre F, Campana A, Simonini G, Ravelli A and Montin D (2023) Outcomes of MIS-C patients treated with anakinra: a retrospective multicenter national study. Front. Pediatr. 11:1137051. doi: 10.3389/fped.2023.1137051
Received: 3 January 2023; Accepted: 27 July 2023;
Published: 22 August 2023.
Edited by:
Masafumi Onodera, National Center for Child Health and Development (NCCHD), JapanReviewed by:
Hidetoshi Takada, University of Tsukuba, Japan© 2023 Licciardi, Covizzi, Dellepiane, Olivini, Mastrolia, Lo Vecchio, Monno, Tardi, Mauro, Alessio, Filocamo, Cattalini, Taddio, Caorsi, Marseglia, LaTorre, Campana, Simonini, Ravelli and Montin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlotta Covizzi Y2FybG90dGFAZnJhbmNvY292aXp6aS5pdA==
Abbreviations: MIS-C, multisystem inflammatory syndrome in children; ICU, intensive care unit; IVIG, intravenous immunoglobulin; CAA, coronary artery anomalies (CAA); AHA, American heart association; CRP, C-reactive protein; Pro-BNP, pro-brain natriuretic peptide; EF, ejection fraction.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.