
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 09 May 2023
Sec. Children and Health
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1135415
This article is part of the Research Topic Assessing Health-related Quality of Life of Children View all 23 articles
 Hannah Schillok1,2
Hannah Schillok1,2 Michaela Coenen1,2
Michaela Coenen1,2 Eva A. Rehfuess1,2
Eva A. Rehfuess1,2 Pia H. Kuhlmann3
Pia H. Kuhlmann3 Stefan Matl3Hannah Kindermann3Nicole Maison3,4,5
Stefan Matl3Hannah Kindermann3Nicole Maison3,4,5 Jana Eckert3
Jana Eckert3 Ulrich von Both3,6Uta Behrends7
Ulrich von Both3,6Uta Behrends7 Michael C. Frühwald8
Michael C. Frühwald8 Antje Neubert9
Antje Neubert9 Joachim Woelfle9Michael Melter10
Joachim Woelfle9Michael Melter10 Johannes Liese11Johannes Hübner3
Johannes Liese11Johannes Hübner3 Christoph Klein3Anna Kern3,†
Christoph Klein3Anna Kern3,† Caroline Jung-Sievers1,2*†
Caroline Jung-Sievers1,2*†
Introduction: The COVID-19 pandemic with its containment measures such as closures of schools and daycare facilities led to numerous restrictions in daily life, putting developmental opportunities and health-related quality of life in children at risk. However, studies show that not every family was impacted equally by the pandemic and that this exceptional health and societal situation reinforced pre-existing health inequalities among the vulnerable. Our study aimed at analyzing changes in behavior and health-related quality of life of children attending elementary schools and daycare facilities in Bavaria, Germany in spring 2021. We also sought to identify associated factors contributing to inequalities in quality of life.
Methods: Data from a multi-center, open cohort study (“COVID Kids Bavaria”) conducted in 101 childcare facilities and 69 elementary schools across all electoral districts of Bavaria were analyzed. Children attending these educational settings (aged 3-10 years) were eligible for participation in a survey on changes in behavior and health-related quality of life. The KINDLR questionnaire (based on children’s self-report and parental report) was administered about one year after the onset of the pandemic (spring 2021). Descriptive and logistic regression analyses and comparisons to pre-pandemic KiGGS (German Health Interview and Examination Survey for Children and Adolescents) data were undertaken.
Results: Among respondents, a high percentage of parents reported changes in their children's eating and sleeping behavior, sports and outdoor activities as well as altered screen time. Health-related quality of life in KINDLR analyses compared to pre-pandemic population averages were lower in all age groups (for 3–6-year-old KINDLR-total score: COVID Kids Bavaria MD 74.78 ± 10.57 vs KiGGS data 80.0 ± 8.1; 7-10 years-old KINDLR-total score: COVID Kids Bavaria MD 73.88 ± 12.03 vs KiGGS data 79.30 ± 9.0). No significant differences were detected with regard to associated factors, namely type of institution, sex of the child, migration background, household size and parental education.
Conclusion: These findings suggest a relevant impact of the COVID-19 pandemic on children’s behavior and health-related quality of life one year after the onset of the pandemic. Further analyses in large-scale longitudinal studies are needed to determine the effects of specific pandemic or crisis associated factors contributing to health inequalities.
The global spread of the SARS-CoV-2 virus can be seen as a worldwide stress test for populations around the world, but especially for vulnerable groups. Even if children are only mildly affected by a SARS-CoV-2 infection in general, they represent a particularly vulnerable group with regards to the consequences of mitigation measures taken against the spread of the virus during different stages of the pandemic (1, 2). Being in a critical developmental phase, they were at times deprived of educational opportunities and social contacts by the closure or reduced services of schools and childcare institutions. At the same time, they were confronted with stressors such as isolation, stressed parents due to potentially insecure social and economic situations, and loss of daily structure through restricted leisure activities. In addition, they may have had less resilience capacity due to their lack of life experience compared to adults.
During the pandemic, the mental health of children has been compromised as demonstrated by many international studies and systematic reviews (3–10). A meta-analysis of studies on the prevalence of depressive and anxiety symptoms in children and adolescents during the pandemic demonstrates a two-fold increase in these symptoms (4). Certain groups, such as children with preexisting (chronic) physical or mental health conditions and lower socioeconomic family resources suffer disproportionately (11).
After a rapid increase in the first phase of the pandemic, stress and psychosocial symptoms have remained at high and relatively stable levels throughout the pandemic. Ravens-Sieberer et al. reported in the COPSY (longitudinal COVID-19 and Psychological Health) study that two-thirds of children and adolescents were highly burdened by the COVID-19 pandemic with lower health-related quality of life (QoL), more mental health problems and worsened behavior compared to pre-pandemic times. However, levels of mental health problems between the first wave in spring 2020 and the second wave in winter 2020/2021 did not differ significantly (12–16). Analyses of the German serial cross-sectional “Corona Snapshot Monitoring” (COSMO) study showed that about a third of children suffered from mental health problems according to the Strengths and Difficulties Questionnaire (SDQ) proxy-report by their parents (17). This was again higher than pre-pandemic levels while no significant differences were observed between different waves.
An additional stressing factor for children during the pandemic might stem from their parents, who themselves have been highly burdened at the same time, posing another risk factor for children's wellbeing (18). The mental health of parents and of their children are closely intertwined and the risk of violence against children increases through a burdened family environment (19). Against this backdrop, it is particularly important to monitor children's health-related QoL and psychological status and to identify how they can be strengthened and protected during the present and future crises.
Our study, a sub-study embedded in the larger COVID Kids Bavaria study, thus sought to analyze changes in behavior and health-related quality of life of children attending elementary schools and daycare facilities in Bavaria, Germany in spring 2021. More specifically, we investigated the following aspects: (a) behavior change during the pandemic compared to pre-pandemic behavior, (b) health-related QoL compared to pre-pandemic reference values among a nationally representative sample of healthy children, (c) health-related QoL comparing children's self-assessment with their parents' assessment, (d) determining factors for health inequalities in children during the pandemic, depicted as differences in QoL.
We hypothesized that children in our sample would demonstrate decreased health-related QoL as well as altered, presumably negatively, changed behavior patterns. We also hypothesized that children of different socioeconomic backgrounds would be differentially affected. The COVID Kids Bavaria main study question investigated the occurrence of asymptomatic cases of SARS-CoV-2 infections among children and staff in daycare facilities and elementary schools in Bavaria. Results of this SARS-CoV-2 infection surveillance were previously published (20).
COVID Kids Bavaria is a multi-center, open cohort study covering every electoral district in Bavaria, Germany. It was registered with the German Clinical Trials Register (http://www.drks.de/DRKS00022380) and approved by six local ethics committees. Methods described in this report focus on the survey component of the COVID Kids Bavaria study, whereas methods of the SARS-CoV-2 infection surveillance component of the study are reported elsewhere (20).
Six study centers (Augsburg, Erlangen, Regensburg, Würzburg, Technische Universität München, Ludwig-Maximilians-Universität München) collected data in all 46 Bavarian electoral districts with selected facilities evenly distributed among them (20). Initially 149 facilities were enrolled (101 childcare facilities and 49 elementary schools) in September 2020. 147 facilities were visited by study teams. Towards the end of the study additional 20 elementary schools were recruited for administering questionnaires to further increase the study population. The regional distribution of the participating institutions is displayed in Supplementary Figure S1.
Participating families were eligible for enrollment if they met the following inclusion criteria: child attending the enrolled schools or daycare facilities (aged between 1 and 10 years) and written informed consent provided by parents or legal representatives. Potential participants were approached from September 2020 up to May 2021 in three consecutive phases. Eligibility to participate in the QoL KINDLR questionnaire was granted for the age group of 3 years and older.
At selected elementary schools and childcare facilities, an information letter about the study was distributed to all families. After providing written informed consent, parents received a personal access link to the web-based, electronic questionnaire via email. Online forms were pseudonymized during data entry.
Great care was taken by the consortium to ensure the comprehensibility of the questionnaire. Thus, the focus was put on the use of simple language for lay participants with the aim to generate understandable information material. Also, the questionnaire offered free field comments to point out unclear aspects of the survey. In addition, a pilot phase was conducted in July 2020 in which the questionnaire was tested and adapted accordingly. The KINDLR represents a validated questionnaire, previously tested for comprehensibility in the respective target groups.
Extrapolating from the size and number of enrolled facilities, we expected 15 827 families with school children and 8,586 families with preschool children to be eligible. Of these, 3,166 families with children (1,891 families with school children and 1,275 families with preschool children) consented to participate in the study and to fill in an online questionnaire.
The questionnaire contained socioeconomic variables, demographics, measures taken in regard to hygiene and mitigation, behavior change, the parent or caretaker situation and external contextual factors.
The customized database for electronic data capture was programmed with the Castor software that is compliant with regulations such as ICH E6 Good Clinical Practice, GDPR, HIPAA, FDA 21 CFR Part 11, ISO 27001, and ISO 9001 [Castor Electronic Data Capture (Castor EDC, Amsterdam, the Netherlands)].
We assessed person-related covariates, such as the children's sex and the type of institution (elementary school, kindergarten, nursery, combined institution). Type of institution was used as an indicator for the child's age group as proxy. We defined migration background as either the child itself or at least one parent indicating a country of origin other than Germany. The family structure as well as the number of children living in the household were directly reported by the parents. Parental education was assessed based on years of education of whichever parent answered the questionnaire and then categorized into three groups (≤9 years, ≤12 years, >12 years). In addition, the children's parents were divided into system-relevant and non-system-relevant “workers”, with system-relevant professions regarded as essential for the continuation of essential services, such as supermarkets, schools and healthcare settings.
Changes in behavior were assessed by parents' report on the following topics: eating behavior, sleeping behavior, sports, outdoor activities, meeting friends offline, meeting friends online, screen time (leisure), screen time (education). Parents rated the changes in behaviour (more than in pre-pandemic times, equal, less than in pre-pandemic times) for each of the topics by comparing the one-year time period after the onset of the pandemic to pre-pandemic times.
Health-related QoL was assessed using the KINDLR questionnaire. It can be answered either by the children themselves (self-report) or by their parent or caretaker (parental assessment). Depending on the children's age and developmental stage, up to four Likert-scaled questions are asked across each of six dimensions of subjective well-being (physical well-being, emotional well-being, self-esteem, family, friends, and school). The items are answered using up to five-level response categories.
The KINDLR was developed by Ravens-Sieberer & Bullinger and is publicly available (https://www.kindl.org/) (21, 22). It has been used in different international health contexts including by the nationally representative KiGGS/BELLA study (the mental health module of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) initiated by the Robert Koch Institute (RKI)) (21, 23–30). Three versions of the KINDLR are available comprising 12 or 24 questions (as self-report and parental proxy-report), depending on the children's age. In this study, the Kiddy KINDLR version for children was used for children aged 3–6 years, as well as the Kid KINDLR version for children aged 7–10 years. Parents answered the corresponding KINDLR caretaker version. It should be noted, however, that the child-assessed Kiddy KINDLR is validated only for the age group 4–6 years, whereas the parent-assessed version is validated for the age group 3–6 years. While the parent-assessed (proxy) versions are identical for both KINDLR versions and together with the self-reported Kid KINDLR consist of 24 items that can be translated into 6 sub-scores and one total score, the Kiddy KINDLR version differs in its structure. Due to the challenge of interviewing very young children, the self-reported version's total score has only 12 items, 2 items for each of the 6 dimensions. Therefore, it is not possible to calculate any sub-scores for this KINDLR version. Another difference of this version lies in the three-level response categories, which range from 1 = “never“ to 3 = “quite often“ in contrast to five-level response categories for children aged 7–10 (1 = “never” to 5 = “always”). A visual overview of the different KINDLR versions as well as their respective sub-scores and dimensions used in this report can be found in the appendix (Supplementary Figure S2).
According to the KINDLR manual the total score and six sub-scores are calculated independently for the KINDLR and the Kid KINDLR (31). The responses per scale are added up, whereby certain items need to be negatively recoded and pooled beforehand, creating a mean value substitution (“sum score”). Any scale can only be evaluated if no more than 30% of its items are missing (corresponding to max. 7 for the total score and 1 for any sub-scale, respectively). The resulting scores are then transformed onto a scale ranging from 0 to 100, representing the respective health-related QoL in any given dimension (e.g., Family, Friends, School, or Total score), with a higher value indicating a better QoL (see Supplementary Figure S2).
Parent-reported KINDLR scores were additionally analysed in relation to reported changes in behavior.
For our analysis, we included data of questionnaires completed from April to May 2021 one year after the onset of the COVID-19 pandemic in Germany. A respective flowchart depicts the inclusion of participants (Supplementary Figure S3).
Descriptive statistics include the person-related key characteristics described above (age and sex of children, household size and migration background of family) as well as behavior change during the COVID-19 pandemic compared to pre-pandemic times. Missing values were kept as missing.
For the health-related QoL in children, means and standard deviation of the KINDLR total and sub-scores were compared to pre-pandemic values using population averages from the German KiGGS/BELLA study. For this part, we distinguished between the age groups 3–6 years and 7–10 years.
Logistic regressions were undertaken to identify factors affecting children's health-related QoL during the COVID-19 pandemic. The outcome variable was defined as a lower total score on the KINDLR questionnaire compared to the median of the respective population averages (median split). For the univariate as well as the multivariate regression, the two parent-assessed KINDLR reports (age categories 3–6 and 7–10) were dichotomized (via median split) and then pooled (“health-related QoL better than median” vs. “health-related QoL worse than median”). The same pooling strategy was applied to the child-assessed KINDLR reports of both age categories. The covariates are shown in Table 1 and describe the socioeconomic background of the families, the daily life of the children during the pandemic, and information regarding the parents' occupation.
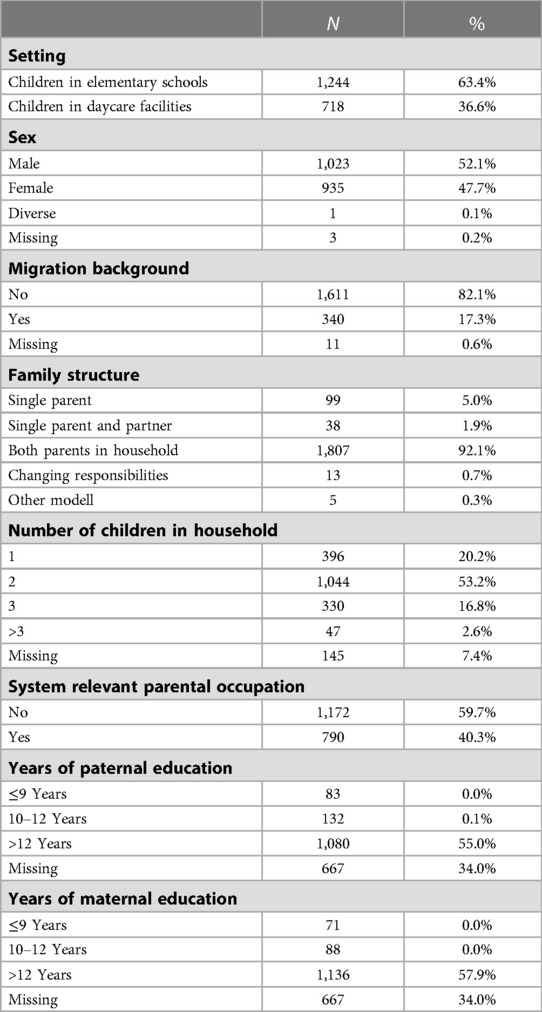
Table 1. Characteristics of the analyzed COVID Kids Bavaria study sample one year after the onset of the pandemic in spring 2021 (N = 1,962).
Children's self-assessed KINDLR scores were contrasted with parent-assessed KINDLR scores via a t-test for paired samples and Cohen's kappa to test the inter-rater reliability of the two assessments.
As an exploratory approach to observe the effect of various adaptive behavior patterns during the pandemic, we descriptively compared the KINDLR scores (means and standard deviations) stratified by the different types of behavior change.
Univariate logistic regression analyses with pooled KINDLR scores as outcome variables (median split) were performed and corresponding ORs (odds ratios) and 95% CIs (confidence intervals) were reported.
All analyses were undertaken in IBM SPSS Statistics 27.
Comparing the expected number of participants with the actual number of participants shows a response rate of 12.9% (11.9% for school children, 14.8% for pre-schoolers) over the entire study period. We included 1962 child-parent-pairs with completed questionnaires (Table 1). Participants and non-participants were shown to be similar with regards to demographics and educational level, as reported in the main study paper by Kern et al. (20).
The majority of children attended Bavarian elementary schools (n = 1244, 63.4%) while 36.6% of the children (n = 718) attended childcare centers. Sex distribution was balanced (boys 52.1% vs. girls 47.7%, with one child specified as diverse). 17.3% of children had at least one parent born outside of Germany and 40.3% of children had a parent engaged in a profession considered “system relevant” during the COVID-19 pandemic. A detailed overview of the distribution concerning the children's living conditions and family-related covariates can be found in Table 1.
In addition, we used variables to assess the family impact of the COVID-19 pandemic. Thus, our data showed that 4.5% of the respondents themselves and 2.3% of their partners were no longer working due to the pandemic. Regarding healthcare access during the pandemic, 5.4% of parents reported refraining from visiting a doctor with their child due to the pandemic. While 65.5% of all parents reported that all medical appointments took place, 6.2% reported that their children's medical appointments were cancelled during these times.
Concerning attitudes toward vaccination, 71.7% expressed interest in COVID-19 vaccination for their children which was not available at the time of questionnaire distribution. In total, 87.5% of included children were fully vaccinated against childhood infectious diseases according to the German Standing Committee on Vaccination (STIKO) recommendations while 3.7% were not fully vaccinated. In comparison to previously published vaccination rates, the rates in our sample are high (32).
Parents were asked to judge their children's behavior patterns compared to pre-pandemic times. Regarding sport/ physical activity, the majority reported that their child did less sport. General screen time for leisure and education purposes increased, while time with friends was also reportedly to shift towards more online time. Parents also observed considerable changes concerning the eating and sleeping behavior of their children, with changes in both directions, indicating maladaptive coping strategies in each case. A detailed overview is displayed in Table 2.
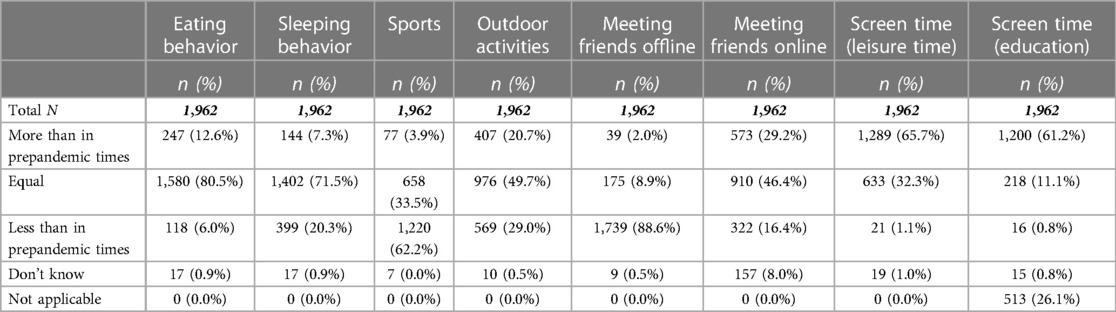
Table 2. Subjective changes in behavior one year after the onset of the pandemic compared to pre-pandemic times assessed by parents (N = 1,962).
Comparing the parent-assessed KINDLR scores associated with different changes in behavior, we observed that results were similar for both age categories. Therefore, for the sake of clarity, this paragraph will always refer to the KINDLR total score of the 7–10-year-olds. All results for all age categories are displayed in Supplementary Table A1.
Eating more and eating less than before the pandemic were both associated with worse KINDLR total scores (eating more: MD 67.40 ± 12.76); eating less: MD 64.05 ± 13.18) compared to children whose eating behavior had not changed during the pandemic according to their parents' judgement (MD 76.04 ± 10.87). Similarly, for sleep behavior, the children who experienced changes in behavior (more or less sleep than before the pandemic) also had a clearly worse KINDLR total score than their peers whose sleep behavior had remained the same (MD 76.56 ± 10.62), with the children who slept less than before having even worse KINDLR scores (MD 66.91 ± 12.97) than the children who slept more than before (MD 73.34 ± 11.70). Although few in number (n = 77), children who did more sport during the pandemic showed a higher KINDLR score (MD 80.93 ± 9.11) than children with unchanged sports behavior (MD 78.93 (±10.49) and especially children who played less sports during the pandemic (MD 72.13 ± 12.05). Children whose leisure time remained unchanged compared to pre-pandemic times reported better KINDLR scores (MD 78.00 ± 10.94) than children who spent more time in front of a screen during the pandemic (MD 72.16 ± 12.07). This would also apply to children whose screen time decreased during the pandemic, but numbers were small (n = 16).
We compared the parent-assessed KINDLR of the COVID Kids Bavaria cohort one year after the onset of the pandemic to pre-pandemic reference values provided by the German KiGGS/BELLA cohort, a longitudinal study on the health of children and adolescents in Germany conducted between 2003 and 2006 (Table 3) (30, 33).
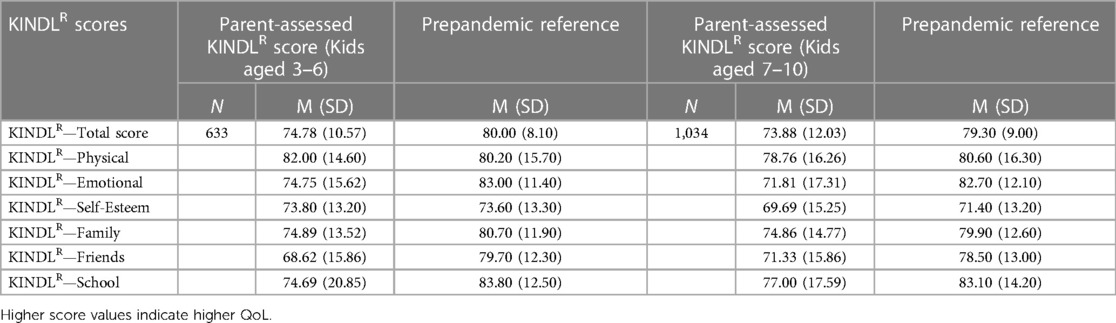
Table 3. Health-related quality of life (QoL) measured with the KINDLR one year after the onset of the pandemic compared to reference data in healthy population (30, 33).
In general, we observed lower total scores in all KINDLR analyses in the COVID Kids Bavaria cohort compared to pre-pandemic population averages across all age groups (for 3–6-year-old KINDLR-total score: COVID Kids Bavaria MD 74.78 ± 10.57 vs. KiGGS data 80.0 ± 8.1; 7–10 years-old KINDLR-total score: COVID Kids Bavaria MD 73.88 ± 12.03 vs. KiGGS data 79.30 ± 9.0).
Regarding the KINDLR sub-scores, Emotional Well-Being, Family, Friends, and School, the KINDLR scores for all age groups were lower one year after the onset of the pandemic compared to pre-pandemic population averages. Also, in the dimensions of Physical Well-Being (COVID Kids Bavaria MD 78.76 ± 16.26 vs. KiGGS data 80.60 ± 16.3) and Self-Esteem (COVID Kids Bavaria MD 69.69 ± 15.25 vs. KiGGS data 71.40 ± 13.2) lower KINDLR values were found for the 7–10-year-olds. In contrast, the values for the 3–6-year-olds were slightly above pre-pandemic population averages in these dimensions (Physical Well-Being: COVID Kids Bavaria MD 82.00 ± 14.6 vs. KiGGS data 80.20 ± 15.7; Self-esteem: COVID Kids Bavaria MD 73.80 ± 13.2 vs. KiGGS 73.60 ± 13.3).
Comparing the parent-assessed KINDLR scores to the children's self-reports, our results indicate that they do not correspond well, with the t-test also indicating a significant difference between parental and child assessment (Supplementary Table A2, A3). The kappa-values for interrater-reliability shown in these tables generally translate to no more than a slight strength of agreement (34).
Across all age groups, children's self-report on health-related QoL was significantly higher than the parent-assessed QoL, indicating that children consistently assessed their situation more positively than their parents, with only one exception for self-esteem, where the 7–10 year old children rated their QoL slightly worse than their parents. Our findings seem to be stable over time, as they align with the KINDLR scores of 2068 children assessed from November 2020 – March 2021 who display similar KINDLR outcomes compared to the time period analyzed by us (April-May 2021) (Supplementary Table A4).
We sought to identify subgroups that may be especially vulnerable to a worsening of health-related QoL during the pandemic, thereby indicating a health disadvantage. To do so we performed binary univariate regression analyses with a pooled outcome variable of the KINDLR score, combining all age categories into a dichotomized median split.
As shown in Table 4, we did not find any differences between those children with a high or low health-related QoL (median split) for the covariates type of institution, sex, migration background, family structure, household size, system relevant parental occupation and parental education, for the parent-assessed KINDLR report for children aged 3–10 years. However, with the children-assessed KINDLR report, our results indicate that boys were less likely to report a KINDLR total score above the sample's median compared to girls (OR: 0.82 [0.68; 0.99]). Regarding the family concept, children living with both parents in one household were more likely to experience an above-median health-related QoL (KINDLR total score) compared to children living with a single parent (OR: 1.62 [1.03; 2.55]).
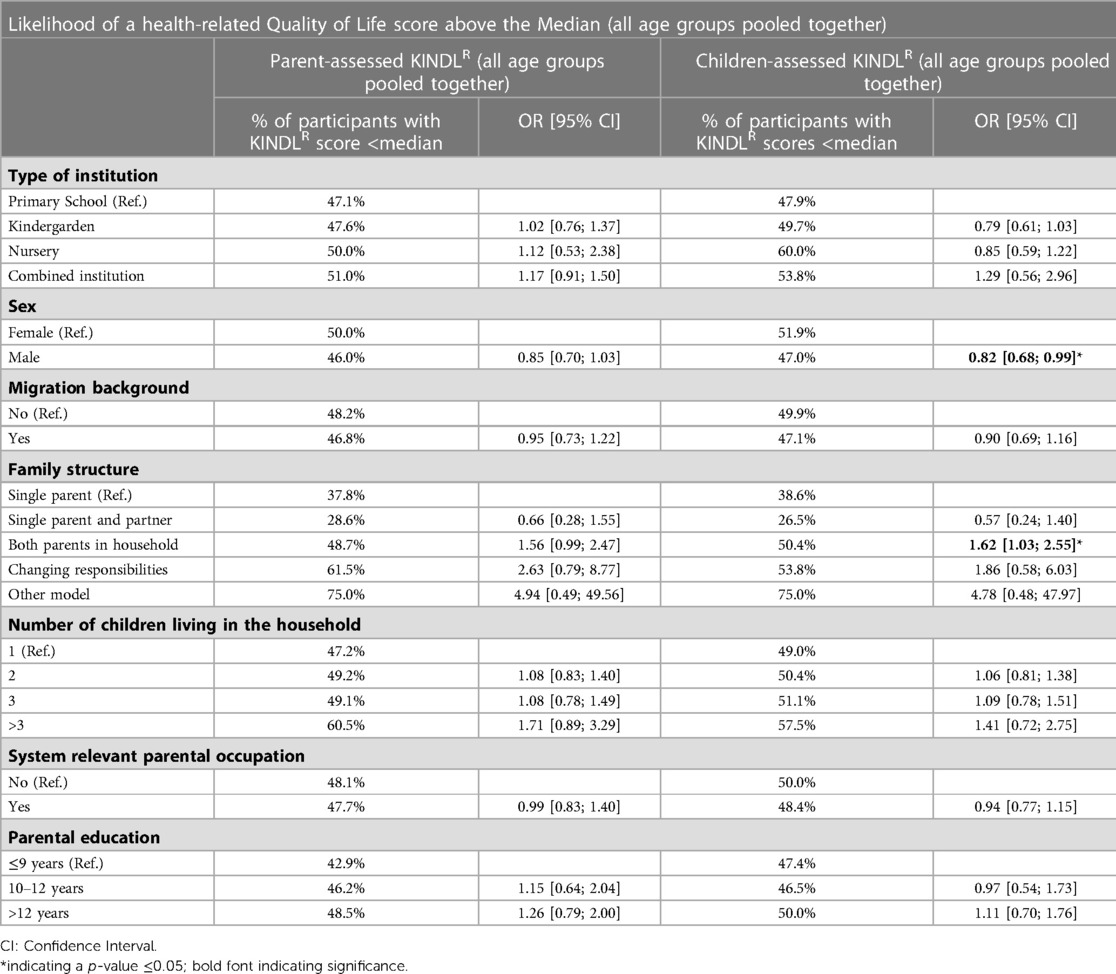
Table 4. Univariate logistic regression (median split of parent-assessed and children-assessed health-related quality of life) for children aged 3–10.
Under the same assumptions, we ran multivariate binary regressions for both the pooled parent-assessed outcome and the child-assessed outcome (Table 5). For both KINDLR outcomes, we could not detect any significant differences between the children aged 3–10 years with above-median or below-median health-related QoL considering the mostly socio-economic covariates described above.
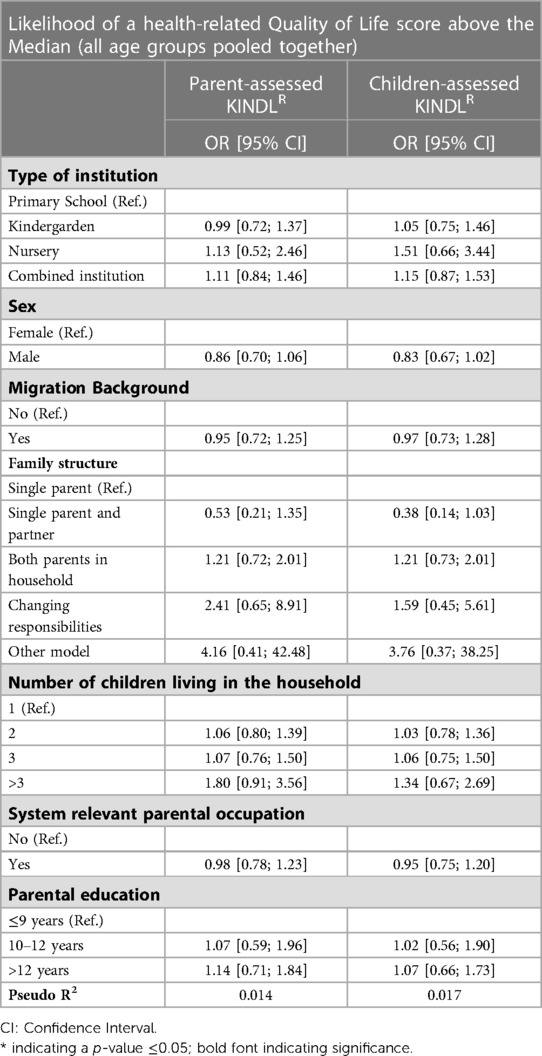
Table 5. Multivariate logistic regression with health-related QoL outcome (median split) for children aged 3–10.
The COVID Kids Bavaria study assessed the incidence of SARS-CoV-2 and its ramifications in healthy children attending elementary schools and day care facilities in different phases of the COVID-19 pandemic. Herein, we investigated health-related QoL and changes in behavior of children with a focus on the time point one year after the onset of the COVID-19 pandemic.
Main results were that a high percentage of parents reported pronounced changes in behaviour in their children, which were found to be associated with reduced health-related QoL. Children's health-related QoL was lower one year after the onset of the pandemic compared to pre-pandemic levels while children still had a more positive QoL perception than their parents.
These findings are in line with other studies reporting a deterioration in wellbeing and mental health among the youngest during the COVID-19 pandemic nationally (15) and internationally (35–40). Prior to the pandemic, in 2017, 17.2% of children and adolescents aged 3 to 17 years in the German BELLA cohort study showed psychosocial problems measured with the SDQ (41). Similarly, a meta-analysis from 2012 reported that about one in five children were at risk of mental health problems (42) while recent publications now report one in three children to be at risk (17). With regard to KINDLR-specific values, a German study from 2016 showed that the KINDLR scores and therefore the health-related QoL perception of children and parents alike had increased consistently over the past 10 years before the start of the COVID-19 pandemic (43). This would point towards an even higher difference compared to pre-pandemic values.
Overall, children aged 3–10 years in our cohort had much more positive perception of their current QoL than their parents, with children generally reporting higher KINDLR total scores and sub-scores. This, however, is in contrast to pre-pandemic studies comparing parents' and children's KINDLR reports, where the picture is less consistent. In a German study comparing parents' and children's KINDLR reports stemming from the KiGGS study (from 2003 to 2006), parents significantly overestimated their children's health-related QoL, both in the KINDLR total score and in the sub-scores for the dimensions Physical Well-Being, Self-esteem, and School. At the same time, they underestimated the sub-scores Emotional Well-Being and Family (24, 44). For a direct interpretation, however, it is important to know that the children considered in the KiGGS cohort were older than in our sample, namely 11–17 years old. Similar results were also reported in a Norwegian study from 1999, in which parents generally reported significantly more positive KINDLR scores than their 9–16-year-old children (45). Overall, our results suggest that the COVID-19 pandemic might have exacerbated pre-existing discrepancies in the perceptions of children's QoL, making it even more difficult for parents to assess their children's actual situation. Alternatively, due to the high stress levels during this situation (18), parents could have tried to compensate this by being especially concerned about their children, resulting in evaluating their QoL worse than it actually was. The QoL tends to deteriorate with the age of the children. One could also deduce that especially younger age groups in our sample perceive the threatening situation differently from their parents.
Regarding changes in behavior, nearly 20% of this selected cohort ate either more or less than before the pandemic, 30% changed their sleeping behavior, 60% of children engaged in fewer sports activities than before, and 65% of children spent more leisure time in front of a screen. These results are in line with other international studies. Thus, trajectories in psychosocial aspects have already been described in the literature, all of them reported changes in children's and adolescents' sleeping behavior, reductions in physical activity and increases in screen time (46–51). On this basis, a 2020 US study recognized the positive association between higher levels of physical activity or less screen time and better mental health outcomes during the pandemic, as measured by the SDQ (52). Furthermore, a Turkish study of children during the pandemic showed the association between increased Internet use and worsened KINDLR scores (48).
A systematic review also stressed the association of poor mental health with sleeping problems, which could lead to a downward trajectory during the COVID-19 pandemic and could partially explain the study results (53). Screen time also tends to be related to sleeping problems and sleeping deviations, which—as shown by our data—has increased during the COVID-19 pandemic, both school-related and during leisure time. Thus, the observed changes in behavior and associated KINDLR scores may also be interdependent to some extent.
Univariate analyses of the children self-reported KINDLR revealed that being male was a risk factor for a below-median health-related QoL, whereas living in a household with both parents increased the likelihood of an above-median QoL. However, based on our multivariate analyses of parent-assessed and children-assessed KINDLR outcomes, we were not able to identify any predicting factor for above- or below-median health-related QoL that could indicate a specific vulnerability for health inequalities during the pandemic.
In contrast, published evidence often reports female sex as a risk factor for poor mental health during the COVID-19 pandemic, as it is also considered a risk factor for depression in general (54–58).
The overall low response rate limits the external validity of the study with a high likelihood for systematic bias. The results shown here should thus be interpreted with caution due to the high probability of a selection and non-responder bias in our study sample. Thus, data cannot be considered to be representative of Bavarian children as a whole. Our study cohort rather provides information about which population groups and segments are willing to participate in a questionnaire-based study in a school setting during a pandemic crisis.
Based on a non-responder analysis for COVID Kids Bavaria (20), the characteristics of the responders of this convenience sample shows that a systematic middle-class bias is likely to be present. For instance, 17.3% of all children in our cohort have a migration background, whereas the Bavaria-wide share of families with a migration background was 34.2% in 2019 and is thus strongly underrepresented in our sample and may explain why our covariate analysis for migration background did not reveal any differences for a high or low health-related QoL (median split) (59). The situation is similar for single parent status: while 15.1% of all families across Bavaria were single parents in 2019 (59), the share in our cohort is only 6.9%. The number of children per household in our sample also differs from the Bavarian average: in 2019, 49.5% of households with children had one child, 39.1% had two children, and 11.4% had three or more children (59). Our sample overestimates the number of households with two children (53.0% instead of 39.1%) and underestimates the number of one-child households (20.0% instead of 49.5%).
Consequently, the families in our sample have less migration background, are more likely to be married and less likely to be single parents, and are more likely to have two children. Notably, these factors were also found to be generally protective against health inequalities, potentially leading to distortions in our data that may mask determinants of health disadvantage.
Based on the characteristics of our sample and the comparison with the Bavarian general population, our participants seem to come from the rather well-off middle class milieu and are therefore not representative for Bavaria as a whole. Other possible homogeneities in the cohort, such as common beliefs or motivation, may not be traceable at all. A particularly strong bias is also evident in the years of parental education: for both fathers and mothers, 34.0% did not indicate any answer. While the percentage of missing values was relatively low for most variables, the variables for paternal and maternal education both showed 34.0% of missing values, which could very likely distort the picture. Thus, our results have only a limited external validity and are therefore only transferable to Bavarian primary school and daycare facility children to some extent.
Self-assessment may represent another source of bias, potentially leading to recall bias, optimism bias, or social-desirability bias. However, as results point in a similar direction as parental external assessments and evidence from other studies, we believe that this effect should not be overestimated.
A growing body of evidence shows that children suffer from significant psychosocial consequences during this pandemic. However, it remains a challenge to differentiate the effects of acute and chronic somatic, psychological and social sequelae of COVID-19 and its mitigation measures in individual children and pediatric populations as a whole. Therefore, further analyses in large-scale longitudinal studies and surveillance data are needed to understand how the various factors affect quality of life, changes in behavior and mental health in children. For future crises and pandemics, policymakers, researchers and clinicians should prioritize the wellbeing, psychosocial monitoring and mental health right from the beginning to identify and protect vulnerable groups, to identify targets for interventions for those at risk and to promote mental health and resilience. As it now became evident that the pandemic affects all areas of children's lives, these efforts should not only be limited to mitigation measures but also other pandemic aspects. The approach of the German Wü-KiTa-CoV-Project on the feasibility of SARS-CoV-2 testing in daycare centers gives an example of how the situation of children could not only be well monitored, but also of how to include the children's perspective through qualitative work and how to test different models for improvement through intervention studies (60–62).
In terms of policies and practice, widespread awareness, research and implementation of evidence based (mental) health protection and promotion efforts in children during crises should be undertaken. While at the same time inequalities should be balanced through focus on the disadvantaged by drawing on international and national guidance (63, 64).
Inquiries regarding the raw data supporting the conclusions of this study can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ethikkommission der Medizinischen Fakultät der LMU (Ethics committee of the Medical Faculty of the University of Munich, LMU). Processing number: 20–538. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
The COVID Kids Bavaria study team (herein represented by AK, PHK, SM, HK, NM, JE, UvB, UB, MCF, AN, JW, MM, JL, JH, and CK) were responsible for the overall COVID Kids Bavaria study design, organization and conduct. HS, MC, EAR and CJ-S were responsible for the choice of survey instruments and analysis of data presented in this study including the interpretation of findings and manuscript preparation. All authors contributed to the article and approved the submitted version.
We thank all children and parents for their participation and schools, the school authorities and the teachers for their constructive support.
The study COVID Kids Bavaria was financed by the Bavarian Ministry of Research and Art. CK reports support from the Care-for-Rare Foundation. CJS reports involvement with other COVID-19 related studies such as the COSMO study, COVerCHILD (NUM) and others. ER reports involvement with other COVID-19 related studies, notably COVerCHILD, and having co-coordinated the German evidence- and consensus-based S3 guideline on schooling during COVID-19 as well as being a member of the WHO Technical Advisory Group on Schooling during COVID-19. HS is a doctoral candidate in the Research Training Group “PrediktOren und Klinische Ergebnisse bei depressiven ErkrAnkungen in der hausärztLichen Versorgung (POKAL, DFG-GRK 2621)” (Predictors and Clinical Outcomes of Depressive Disorders in Primary Care) POKAL, a member of the German Research Foundation (DFG). UB is employed by the Department of Pediatrics, Kinderklinik München Schwabing, StKM GmbH und Klinikum Rechts der Isar, Technische Universität München, Germany. NM is employed by the Institute for Asthma- and Allergy Prevention (IAP), Helmholtz Center Munich, German Research Center for Environmental Health (GmbH), Munich, Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1135415/full#supplementary-material.
1. Kratzer S, Pfadenhauer LM, Biallas RL, Featherstone R, Klinger C, Movsisyan A, et al. Unintended consequences of measures implemented in the school setting to contain the COVID-19 pandemic: a scoping review. Cochrane Database Syst Rev. (2022) 6(6):CD015397. doi: 10.1002/14651858.CD015397
2. Krishnaratne S, Littlecott H, Sell K, Burns J, Rabe JE, Stratil JM, et al. Measures implemented in the school setting to contain the COVID-19 pandemic. Cochrane Database Syst Rev. (2022) 1:CD015029. doi: 10.1002/14651858.CD015029
3. Fong V, Iarocci G. Child and family outcomes following pandemics: a systematic review and recommendations on COVID-19 policies. J Pediatr Psychol. (2020) 45(10):1124–43. doi: 10.1093/jpepsy/jsaa092
4. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. (2021) 175(11):1142–50. doi: 10.1001/jamapediatrics.2021.2482
5. Imran N, Aamer I, Sharif MI, Bodla ZH, Naveed S. Psychological burden of quarantine in children and adolescents: a rapid systematic review and proposed solutions. Pak J Med Sci. (2020) 36(5):1106–16. doi: 10.12669/pjms.36.5.3088
6. Panda P, Gupta J, Chowdhury S, Kumar R, Meena A, Madaan P, et al. Psychological and behavioral impact of lockdown and quarantine measures for COVID-19 pandemic on children, adolescents and caregivers: a systematic review and meta-analysis. J Trop Pediatr. (2021) 67(1)fmaa122. doi: 10.1093/tropej/fmaa122
7. Meherali S, Punjani N, Louie-Poon S, Rahim KA, Das JK, Salam RA, et al. Mental health of children and adolescents amidst COVID-19 and past pandemics: a rapid systematic review. Int J Environ Res Public Health. (2021) 18(7):3432. doi: 10.3390/ijerph18073432
8. Singh S, Roy D, Sinha K, Parveen S, Sharma G, Joshi G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/j.psychres.2020.113429
9. Loades ME, Chatburn E, Higson-Sweeney N, Reynolds S, Shafran R, Brigden A, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. (2020) 59(11):1218. doi: 10.1016/j.jaac.2020.05.009
10. Ravens-Sieberer U, Erhart M, Devine J, Gilbert M, Reiss F, Barkmann C, et al. Child and adolescent mental health during the COVID-19 pandemic: results of the three-wave longitudinal COPSY study. J Adolesc Health. (2022) 71(5):570–78. doi: 10.1016/j.jadohealth.2022.06.022
11. Reiss F, Meyrose AK, Otto C, Lampert T, Klasen F, Ravens-Sieberer U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: results of the German BELLA cohort-study. PLoS One. (2019) 14(3):e0213700. doi: 10.1371/journal.pone.0213700
12. Skoda EM, Spura A, de Bock F, Schweda A, Dörrie N, Fink M, et al. [Change in psychological burden during the COVID-19 pandemic in Germany: fears, individual behavior, and the relevance of information and trust in governmental institutions]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2021) 64(3):322–33. doi: 10.1007/s00103-021-03278-0
13. Ravens-Sieberer U, Kaman A, Erhart M, Devine J, Schlack R, Otto C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur Child Adolesc Psychiatry. (2021) 31:879–89. doi: 10.1007/s00787-021-01726-5
14. Ravens-Sieberer U, Kaman A, Erhart M, Otto C, Devine J, Löffler C, et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: results of a two-wave nationwide population-based study. Eur Child Adolesc Psychiatry. (2021) 1–14. doi: 10.1007/s00787-021-01889-1
15. Ravens-Sieberer U, Kaman A, Otto C, Adedeji A, Devine J, Erhart M, et al. Mental health and quality of life in children and adolescents during the COVID-19 pandemic—results of the copsy study. Dtsch Arztebl Int. (2020) 117:828–9. doi: 10.3238/arztebl.2020.0828
16. Ravens-Sieberer U, Kaman A, Otto C, Adedeji A, Napp AK, Becker M, et al. Mental health and psychological burden of children and adolescents during the first wave of the COVID-19 pandemic—results of the COPSY study. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2021) 64:1–10. doi: 10.1007/s00103-021-03291-3
17. Rathgeb C, Schillok H, Voss S, Coenen M, Schulte-Körne G, Merkel C, et al. Emotional situation of children and adolescents during the COVID-19 pandemic in Germany: results from the COVID-19 snapshot monitoring study (COSMO). Int J Environ Res Public Health. (2022) 19(5):2698. doi: 10.3390/ijerph19052698
18. Rabe JE, Schillok H, Merkel C, Voss S, Coenen M, de Bock F, et al. [Burden in parents of school-aged children during different phases of the COVID-19 pandemic in Germany: an analysis within the COVID-19 snapshot monitoring (COSMO) study]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2021) 64(12):1500–11. doi: 10.1007/s00103-021-03453-3
19. Bhatia A, Fabbri C, Cerna-Turoff I, Turner E, Lokot M, Warria A, et al. Violence against children during the COVID-19 pandemic. Bull World Health Organ. (2021) 99(10):730–8. doi: 10.2471/BLT.20.283051
20. Kern A, Kuhlmann PH, Matl S, Ege M, Maison N, Eckert J, et al. Surveillance of acute SARS-CoV-2 infections in elementary schools and daycare facilities in bavaria, Germany (09/2020–03/2021). Front Pediatr. (2022) 10:1019. doi: 10.3389/fped.2022.888498
21. Ravens-Sieberer U, Bullinger M. Assessing health-related quality of life in chronically ill children with the German KINDL: first psychometric and content analytical results. Qual Life Res. (1998) 7(5):399–407. doi: 10.1023/A:1008853819715
22. Ravens-Sieberer U, Bullinger M. News from the KINDL-questionnaire—a new version for adolescents. Qual Life Res. (1998) 7:653. doi: 10.1023/A:1008853819715
23. Bullinger M, Brütt AL, Erhart M, Ravens-Sieberer U. Psychometric properties of the KINDL-R questionnaire: results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17(Suppl 1):125–32. doi: 10.1007/s00787-008-1014-z
24. Erhart M, Ellert U, Kurth BM, Ravens-Sieberer U. Measuring adolescents’ HRQoL via self reports and parent proxy reports: an evaluation of the psychometric properties of both versions of the KINDL-R instrument. Health Qual Life Outcomes. (2009) 7(1):77. doi: 10.1186/1477-7525-7-77
25. Eser E, Yüksel H, Baydur H, Erhart M, Saatli G, Ozyurt BC, et al. [The psychometric properties of the new Turkish generic health-related quality of life questionnaire for children (kid-KINDL)]. Turk Psikiyatri Derg. (2008) 19(4):409–17. PMID: 19110983.19110983
26. Essaddam L, ben Mansour A, ben Amor A, Ravens-Sieberer U, Klein TM, ben Becher S. Validation of the Arabic and Tunisian Arabic version of the KINDL questionnaires for children with diabetes type 1. Libyan J Med. (2019) 14(1):1–7. doi: 10.1080/19932820.2018.1537457
27. Fernández-López JA, Fernández Fidalgo M, Cieza A, Ravens-Sieberer U. [Measuring health-related quality of life in children and adolescents: preliminary validation and reliability of the Spanish version of the KINDL questionnaire]. Aten Primaria. (2004) 33(8):434–42. doi: 10.1016/S0212-6567(04)79429-9
28. Rajmil L, Serra-Sutton V, Fernandez-Lopez JA, Berra S, Aymerich M, Cieza A, et al. [The Spanish version of the German health-related quality of life questionnaire for children and adolescents: the Kindl]. An Pediatr (Barc). (2004) 60(6):514–21. doi: 10.1016/S1695-4033(04)78320-4
29. Bullinger M, Schmidt S, Petersen C, Erhart M, Ravens-Sieberer U. [Methodological challenges and potentials of health-related quality of life evaluation in children with chronic health conditions under medical health care]. Med Klin (Munich). (2007) 102(9):734–45. doi: 10.1007/s00063-007-1092-6
30. Ravens-Sieberer U, Ellert U, Erhart M. Gesundheitsbezogene Lebensqualität von Kindern und Jugendlichen in Deutschland. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2007 May 1) 50(5–6):810–8. doi: 10.1007/s00103-007-0244-4
31. Ravens-Sieberer U, Bullinger M. Manual—kindl.org. (2000). Available from: https://www.kindl.org/english/manual/ (cited January 9, 2022).
32. Krankenkasse T, Egert-Schmidt A-M, Holtz S, Kaufmann-Kolle P, Neubert A, Spelly C, et al. Kinder und Arzneimittel – Verordnungsreport (2022).
33. Ravens-Sieberer U, Erhart M, Wille N, Bullinger M, BELLA study group. Health-related quality of life in children and adolescents in Germany: results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17(Suppl 1):148–56. doi: 10.1007/s00787-008-1016-x
34. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33(1):159. doi: 10.2307/2529310
35. Mahase E. COVID-19: children’s mental health services in England are “nowhere near sufficient,” says commissioner. Br Med J. (2021) 372:n258. doi: 10.1136/bmj.n258
36. Cost KT, Crosbie J, Anagnostou E, Birken CS, Charach A, Monga S, et al. Mostly worse, occasionally better: impact of COVID-19 pandemic on the mental health of Canadian children and adolescents. Eur Child Adolesc Psychiatry. (2022) 31(4):671–84. doi: 10.1007/s00787-021-01744-3
37. Saurabh K, Ranjan S. Compliance and psychological impact of quarantine in children and adolescents due to COVID-19 pandemic. Indian J Pediatr. (2020) 87(7):532–6. doi: 10.1007/s12098-020-03347-3
38. Patrick SW, Henkhaus LE, Zickafoose JS, Lovell K, Halvorson A, Loch S, et al. Well-being of parents and children during the COVID-19 pandemic: a national survey. Pediatrics. (2020) 146(4):e2020016824. doi: 10.1542/peds.2020-016824
39. Xie X, Xue Q, Zhou Y, Zhu K, Liu Q, Zhang J, et al. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei province, China. JAMA Pediatr. (2020) 174(9):898–900. doi: 10.1001/jamapediatrics.2020.1619
40. Orgilés M, Morales A, Delvecchio E, Mazzeschi C, Espada JP. Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Front Psychol. (2020) 11:2986. doi: 10.3389/fpsyg.2020.579038
41. Klasen F, Meyrose AK, Otto C, Reiss F, Ravens-Sieberer U. Leitthema Psychische Auffälligkeiten von Kindern und Jugendlichen in Deutschland Ergebnisse der BELLA-Studie. Monatsschr Kinderheilkd. (2017) 5(165):402–7. doi: 10.1007/s00112-017-0270-8
42. Barkmann C, Schulte-Markwort M. Prevalence of emotional and behavioural disorders in German children and adolescents: a meta-analysis. J Epidemiol Community Health (1978). (2012) 66(3):194–203. doi: 10.1136/jech.2009.102467
43. Meyer M, Oberhoffer R, Hock J, Giegerich T, Müller J. Health-related quality of life in children and adolescents: current normative data, determinants and reliability on proxy-report. J Paediatr Child Health. (2016) 52(6):628–31. doi: 10.1111/jpc.13166
44. Ellert U, Ravens-Sieberer U, Erhart M, Kurth BM. Determinants of agreement between self-reported and parent-assessed quality of life for children in Germany-results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). (2011). Available from: http://www.hqlo.com/content/9/1/102 (cited January 9,2022).
45. Jozefiak T, Larsson B, Wichstrøm L, Mattejat F, Ravens-Sieberer U. Quality of life as reported by school children and their parents: a cross-sectional survey. Health Qual Life Outcomes. (2008) 6(1):1–11. doi: 10.1186/1477-7525-6-34
46. Liu Z, Tang H, Jin Q, Wang G, Yang Z, Chen H, et al. Sleep of preschoolers during the coronavirus disease 2019 (COVID-19) outbreak. J Sleep Res. (2021) 30(1):e13142. doi: 10.1111/jsr.13142
47. López-Bueno R, López-Sánchez GF, Casajús JA, Calatayud J, Gil-Salmerón A, Grabovac I, et al. Health-related behaviors among school-aged children and adolescents during the spanish COVID-19 confinement. Front Pediatr. (2020) 8:573. doi: 10.3389/fped.2020.00573
48. Adıbelli D, Sümen A. The effect of the coronavirus (COVID-19) pandemic on health-related quality of life in children. Child Youth Serv Rev. (2020) 119:105595. doi: 10.1016/j.childyouth.2020.105595
49. Francisco R, Pedro M, Delvecchio E, Espada JP, Morales A, Mazzeschi C, et al. Psychological symptoms and behavioral changes in children and adolescents during the early phase of COVID-19 quarantine in three European countries. Front Psychiatry. (2020) 11:1329. doi: 10.3389/fpsyt.2020.570164
50. Aguilar-Farias N, Toledo-Vargas M, Miranda-Marquez S, Cortinez-O’ryan A, Cristi-Montero C, Rodriguez-Rodriguez F, et al. Sociodemographic predictors of changes in physical activity, screen time, and sleep among toddlers and preschoolers in Chile during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 18(1):1–13. doi: 10.3390/ijerph18010176
51. Medrano M, Cadenas-Sanchez C, Oses M, Arenaza L, Amasene M, Labayen I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: a longitudinal analysis from the MUGI project. Pediatr Obes. (2021) 16(4):e12731. doi: 10.1111/ijpo.12731
52. Tandon PS, Zhou C, Johnson AM, Gonzalez ES, Kroshus E. Association of children’s physical activity and screen time with mental health during the COVID-19 pandemic. JAMA Netw Open. (2021) 4(10):e2127892. doi: 10.1001/jamanetworkopen.2021.27892
53. Palacio-Ortiz JD, Londoño-Herrera JP, Nanclares-Márquez A, Robledo-Rengifo P, Quintero-Cadavid CP. Psychiatric disorders in children and adolescents during the COVID-19 pandemic. Rev Colomb Psiquiatr (Engl Ed). (2020) 49(4):279.33328021
54. Panchal U, Salazar de Pablo G, Franco M, Moreno C, Parellada M, Arango C, et al. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur Child Adolesc Psychiatry. (2021) 1:1–27. doi: 10.1007/s00787-021-01856-w
55. Chen F, Zheng D, Liu J, Gong Y, Guan Z, Lou D. Depression and anxiety among adolescents during COVID-19: a cross-sectional study. Brain Behav Immun. (2020) 88:36–8. doi: 10.1016/j.bbi.2020.05.061
56. Chen S, Cheng Z, Wu J. Risk factors for adolescents’ mental health during the COVID-19 pandemic: a comparison between Wuhan and other urban areas in China. Global Health. (2020) 16(1):1–11. doi: 10.1186/s12992-019-0531-5
57. Magson NR, Freeman JYA, Rapee RM, Richardson CE, Oar EL, Fardouly J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J Youth Adolesc. (2021) 50(1):44–57. doi: 10.1007/s10964-020-01332-9
58. Smirni P, Lavanco G, Smirni D. Anxiety in older adolescents at the time of COVID-19. J Clin Med. (2020) 9(10):1–10. doi: 10.3390/jcm9103064
59. Bayerisches Landesamt für Gesundheit und Lebensmittelsicherheit (LGL). Gesundheitsatlas Bayern.Available from: https://www.lgl.bayern.de/gesundheit/gesundheitsberichterstattung/gesundheitsatlas/ia_report/atlas.html (cited March 4, 2022).
60. Gierszewski D, Kurotschka PK, Krauthausen M, Fröhlich W, Forster J, Pietsch F, et al. Parents’ and childcare workers’ perspectives toward SARS-CoV-2 test and surveillance protocols in Pre-school children day care centers: a qualitative study within the German Wü-KiTa-CoV project. Front Med (Lausanne). (2022) 9:1251.
61. Engels G, Forster J, Streng A, Rücker V, Rudolph P, Pietsch F, et al. Acceptance of different self-sampling methods for semiweekly SARS-CoV-2 testing in asymptomatic children and childcare workers at German day care centers: a nonrandomized controlled trial. JAMA Netw Open. (2022) 5(9):e2231798. doi: 10.1001/jamanetworkopen.2022.31798
62. Forster J, Streng A, Rudolph P, Rücker V, Wallstabe J, Timme S, et al. Feasibility of SARS-CoV-2 surveillance testing among children and childcare workers at German day care centers: a nonrandomized controlled trial. JAMA Netw Open. (2022) 5(1):e2142057. doi: 10.1001/jamanetworkopen.2021.42057
63. Deutsche Gesellschaft für Epidemiologie (DGEpi), Deutsche Gesellschaft für Public Health (DGPH), Deutsche Gesellschaft für, Kinder- und Jugendmedizin (DGKJ), Deutsche Gesellschaft für pädiatrische Infektiologie (DGPI), Gesellschaft für Hygieneet al.S3-Leitlinie – Maßnahmen zur Prävention und Kontrolle der SARS-CoV-2- Übertragung in Schulen – Lebende Leitlinie, Langfassung Version 1.1 2021. Available from: https://www.awmf.org/leitlinien/detail/ll/027-076.html (cited 2022 Jan 9).
64. RAND Mental Health Systems Initiative | RAND. Available from: https://www.rand.org/health-care/key-topics/mental-health/initiative.html (cited 2022 Jan 9).
Keywords: COVID-19, pandemic, mental health—related quality of life, behavior change, health-related quality of life (HRQL), health inequalities in children
Citation: Schillok H, Coenen M, Rehfuess EA, Kuhlmann PH, Matl S, Kindermann H, Maison N, Eckert J, von Both U, Behrends U, Frühwald MC, Neubert A, Woelfle J, Melter M, Liese J, Hübner J, Klein C, Kern A and Jung-Sievers C (2023) Changes in behavior and quality of life in German young children during the COVID-19 pandemic—results from the COVID kids bavaria study. Front. Pediatr. 11:1135415. doi: 10.3389/fped.2023.1135415
Received: 31 December 2022; Accepted: 29 March 2023;
Published: 9 May 2023.
Edited by:
Tim S. Nawrot, University of Hasselt, BelgiumReviewed by:
Doina Anca Plesca, Carol Davila University of Medicine and Pharmacy, Romania© 2023 Schillok, Coenen, Rehfuess, Kuhlmann, Matl, Kindermann, Maison, Eckert, von Both, Behrends, Früehwald, Neubert, Woelfle, Melter, Liese, Hübner, Klein, Kern and Jung-Sievers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Jung-Sievers Y2p1bmdzaWV2ZXJzQGliZS5tZWQudW5pLW11ZW5jaGVuLmRl
†These authors share last authorship
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.