 Teng Wan1,2,†
Teng Wan1,2,† Biao Li
Biao Li Xudong Wang
Xudong Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 23 March 2023
Sec. Pediatric Surgery
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1133456
Virtual reality (VR) has been proven an important supplement for surgical education in medical students. However, studies on immersive VR (iVR) simulation in orthognathic surgical education are limited. This study aimed to assess the validity of the iVR surgical training system for orthognathic surgery. Participants completed questionnaires at the end of the course to assess the validity of the training system. The questionnaires included questions on the experience of using the iVR system and surgical authenticity. Seven experienced surgeons and seven inexperienced students were recruited in this study to use our self-developed iVR training system for orthognathic surgery. The participants showed strong agreement to the fidelity of our training system (4.35 out of 5), including the virtual environment, instruments, anatomy structures, and surgical procedures. The participants also strongly agreed that the iVR technique was essential in imparting surgical education. However, most of the participants experienced some degree of dizziness or fatigue after 1 h of using the system. The iVR training system is a new method for imparting education about orthognathic surgery. The iVR training system can act as a supplement and potential substitute of the traditional surgical training method.
Surgical residents commonly acquire new procedure knowledge through a combination of reading technique guides and watching surgical procedure videos (1, 2).
In recent years, significant advancements in computer sciences have enabled the development of innovative training tools in the medical field, which has enhanced the knowledge and technical skills acquired by surgical trainees (3).
Virtual reality (VR) simulator training has enabled trainees to learn surgical skills in a risk-free environment while also increasing their technical proficiency, improving their operating performance, and decreasing the operation time.
The use of virtual reality (VR) and immersive VR (iVR) in surgical training has become increasingly popular due to the advancements in technology (4, 5).
iVR provides a more realistic and immersive experience compared to conventional VR, allowing trainees to simulate surgical procedures in a more realistic operating room environment.
This technology has been shown to improve technical proficiency, decrease operation time, and increase the attractiveness and degree of participation in surgical training (6–8).
Consequently, this system can provide an immersive surgical experience that enhances the knowledge and skills required for a given surgical procedure.
iVR has the advantages of conventional VR and operates on low-cost, portable, and commercially available hardware. Unlike conventional VR, immersion in iVR is provided as an uninterrupted, scaled environment capable of simulating the full magnitude of sensory stimuli present in the OR (5).
With the COVID-19 pandemic and physical distancing, VR may play a crucial role in providing surgical education to medical students whose regular clerkship experiences have been suspended (9).
Previous studies have demonstrated the use of VR as an advantageous tool in anatomy education and residency training for medical students (10–13).
The development of iVR training systems for orthognathic surgery is particularly important given the challenges of this type of surgery, including complex anatomical structures, limited surgical field of intraoral approach, and the use of various surgical instruments.
While previous studies have focused on specific procedures, such as the application of a reciprocating saw in Le Fort I osteotomy, the use of iVR for double jaw orthognathic surgery has not been explored extensively.
Therefore, we developed an iVR training system for double jaw orthognathic surgery. We assessed the validity of this system and explored the possibility of using it as an additional training tool for orthognathic surgery.
Seven senior surgeons (experts) and seven fifth-year medical students (novices) were enrolled from our hospital after obtaining institutional review board approval and written informed consent for participation.
Each participant completed a pretest questionnaire reporting their age, sex, and prior exposure (cases observed) and experience (cases performed) with orthognathic surgery as well as any previous experience with VR devices.
All participants tested the iVR system for approximately 1 h, completing the training mode and assessment mode of bimaxillary orthognathic surgical procedure.
During their first VR session, each participant completed a tutorial on general orientation in the VR space (Figures 1, 2).
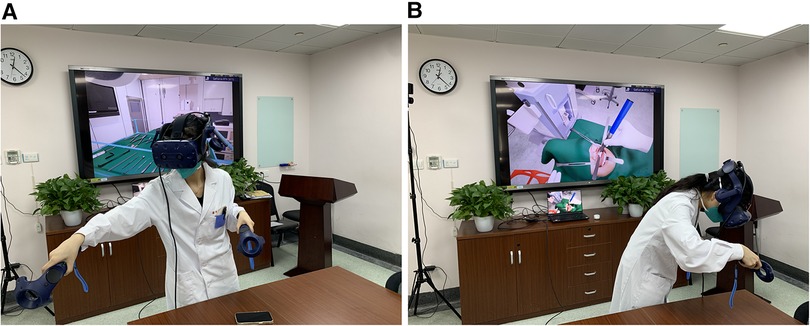
Figure 1. (A) the trainee is picking instrument from the table. (B) The trainee is doing the osteotomy with reciprocating saw.
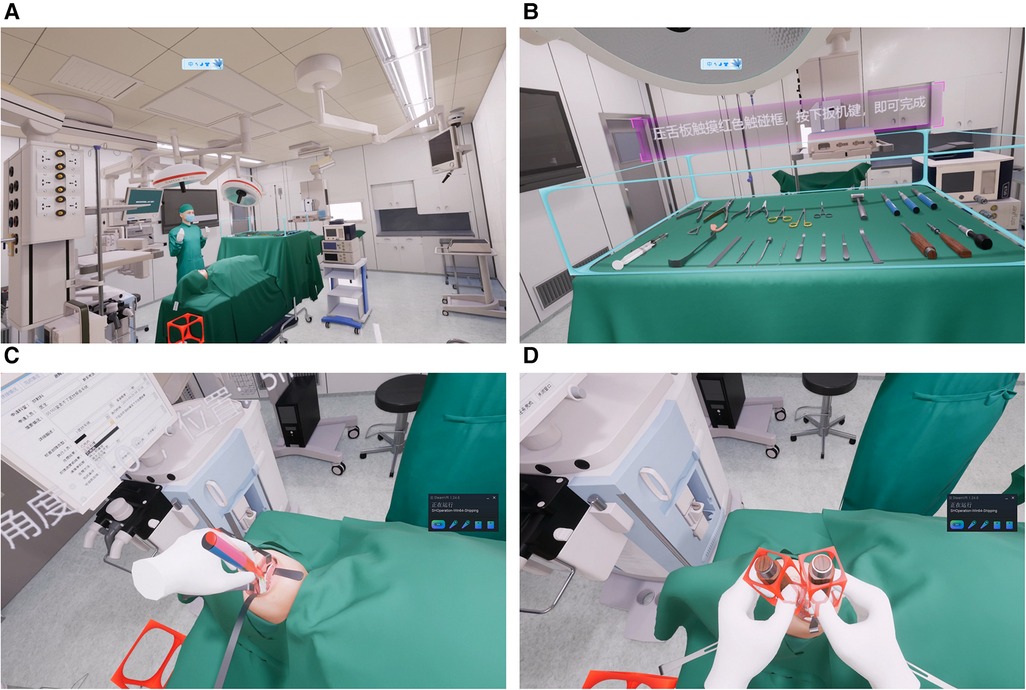
Figure 2. (A) the simulated operating room. (B) Instrument table. (C) Le Fort I osteotomy. (D) BSSRO.
A survey of user experience was administered at the end of the course (Table 1).
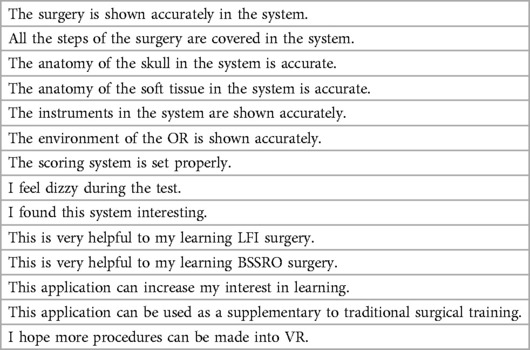
Table 1. The content of the questionaire.
The survey included 14 questions asking participants to rank their level of agreement regarding the use of VR on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree).
The questionnaire consisted of two sections. The first section focused on the experience and application of the VR system. The second section focused on the surgical content, including anatomical accuracy, integrity of the surgical procedure, and fidelity of the OR and surgical instruments.
We developed an iVR orthognathic surgical training system that places operators in a virtual OR and allows them to use surgical instruments on a virtual patient to perform bimaxillary orthognathic surgery.
The HMD device used in this study was HTC VIVE Pro 2 (HTC Corporation, Taiwan). The virtual operation room was created based on a real OR captured using a 360° camera.
Virtual models of the surgical instruments required in our clinical practice were generated using obverse design. The patient model was generated based on the computed tomography (CT) data and optical scan of dental casts of a real patient with skeletal class III malocclusion.
Subsequently, the entire surgical procedure was scripted using Unreal Engine 4 (Epic Games, Inc. NC, USA) to generate the operation flow of the VR training system.
The maxillary surgical procedures included incision, Le Fort I osteotomy, intermaxillary fixation with the intermediate splint, and maxilla fixation. The mandibular surgical procedures included incision, bilateral SSRO, intermaxillary fixation with the final splint, and mandible fixation.
We developed two modes in this system: training and assessment. The training mode involved VR guidance to demonstrate the next surgical step or instrument and the correct instrument positions to the trainee. Voice prompts of the surgical procedures were integrated in the system.
In each step, a virtual assistant would hand out the required surgical instrument to the trainee, and the placement of each instrument was depicted as a phantom for further guidance.
In the assessment mode, the surgical instruments were placed on the instrument table. The trainee was required to select the appropriate instruments required and place them correctly to initiate the next surgical step without any guidance.
The following four measures were used to evaluate the operator performance in the iVR training system: procedural duration (minutes), number of instrument selection errors, instrument position and angular errors, and number of prompts required to progress to the next step (triggered by the operator). The assessment record was available to the trainee at the end of the virtual procedure.
All 14 participants completed the test and questionnaire. The mean age of the experts and novices was 38.6 years and 22.1 years, respectively. The expert group comprised six men and one woman, whereas the novice group comprised two men and five women. The experts had a mean orthognathic surgical experience of 7.3 years, with 371 cases observed and 187 cases performed, whereas the novices had no previous orthognathic experience, with an average of 4.4 cases observed. The medical students observed at least one bimaxillary orthognathic surgery before completing the questionnaire. One expert and one novice had prior experience with VR devices.
The mean score of the first section was 4.35 out of 5, demonstrating strong agreement to the fidelity of the system. The answers to each question are shown in Figure 3.
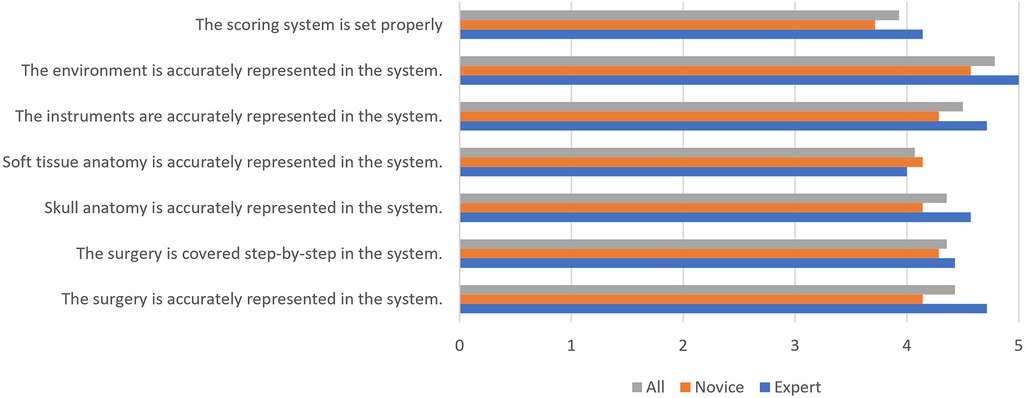
Figure 3. The first section of the questionnaire.
The mean score of the second section was 4.40 out of 5. The answers to each question are shown in Figure 4. Most participants experienced some degree of dizziness or fatigue after the 1-h test. All novice participants strongly agreed that this application was helpful to their learning of the surgical technique (5 out of 5).
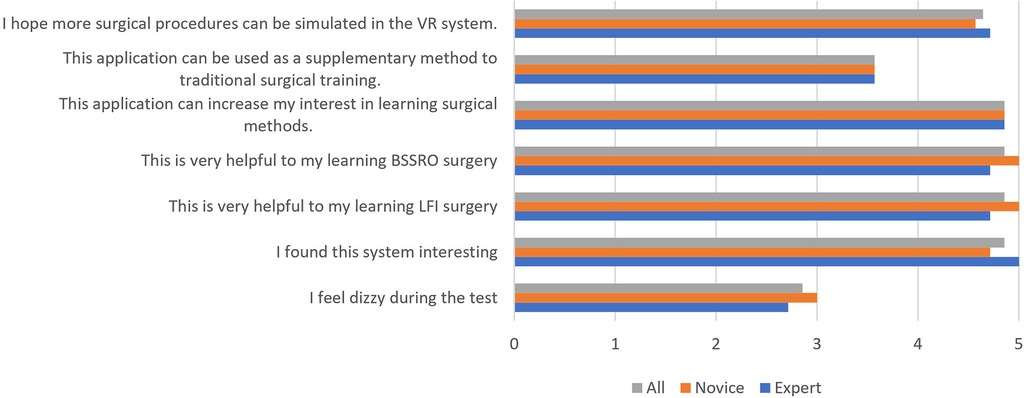
Figure 4. The second section of the questionnaire.
In general, learners initially go through a cognitive stage to become acquainted with the task and learn the prerequisite steps. Subsequently, in the integrative stage, the specific tasks become familiar. Finally, in the autonomous stage, the overall task performance becomes smooth and efficient (14).
Junior surgical residents often prepare themselves for surgical procedures by studying technical guides and watching videos of the procedure (1). The results of this study demonstrated that iVR was realistic and useful in orthognathic surgical training.
Most participants agreed that our iVR training system was a useful learning tool, which could enhance their understanding of surgical procedures and interest in orthognathic surgery.
Dizziness was the main complaint regarding the iVR system. In this study, participants experienced no (36%), slight (28%), and moderate (36%) motion sickness.
The goal of VR is to replace the physical world with a virtual world and render the 3D environment immersive, semi-immersive, or no immersive.
In an immersion system, users find themselves in a complete virtual environment through its sensory output devices, which may be visual (HMD), audio, or haptic. HMD is more widely used because this application is more flexible and requires a smaller space than audio or haptic devices.
The essential points of VR surgery are the 360° experience, close-up stereoscopic visualization, and 3D interaction (15, 16).
VR may offer a useful adjunct to conventional training methods, which may help residents learn the procedural workflow and specific application of surgical instruments to perform surgical procedures.
The application of VR technology in clinical surgery enables users to efficiently learn surgical procedures that can be subsequently applied safely at any point throughout the training process, and it is especially useful before performing an operation for the first time. The implementation of VR for clerkship preparation or as a supplement to surgical rotation can improve students' knowledge and clinical skills (17).
As a common maxillofacial surgical procedure, orthognathic surgery involves a complex interplay of cognitive (maxillofacial anatomy and surgical instrument application), combined (instrument placement and surgical process), and technical (saw control and soft tissue handling) skills.
However, the intraoral approach greatly reduces intraoperative observation due to the limited surgical field. Thus, orthognathic surgery is an appropriate example of a complex and highly skillful surgical procedure, where there is an opportunity to demonstrate the effectiveness of assistive technology on surgical performance.
Several previous studies have explored the feasibility of using VR techniques to train inexperienced oral maxillofacial surgeons. For instance, Pulijala et al. developed a VR training tool for orthognathic surgery based on 360° and stereoscopic videos of orthognathic surgery (18, 19). However, the surgical procedures were mainly presented using stereoscopic videos instead of virtual model interaction.
Wu et al. presented a VR-based training system primarily used for application in Le Fort I osteotomy by reconstructing virtual models from CT data and using virtual instruments built from laser scanning data (20). The system mainly focused on the haptic force feedback simulation rather than on complete surgical steps and procedures.
Arikatla et al. presented methods to simulate bone drilling and cutting with low computational cost and high-fidelity haptic feedback in BSSO (21).
Furthermore, virtual rigid skull and jaw models without soft tissues have been commonly used in OMFS simulators (22). However, most of the abovementioned studies focused on the haptic feedback algorithm of bone drilling and cutting. Therefore, the VR training system used in those studies could not provide an immersive simulation of the entire surgical procedure and operation environment.
VR applications, such as Touch Surgery (Kinosis, London, United Kingdom) and CIVA (BioDigital, New York, USA), have been used to teach surgical procedures using the cognitive task analysis theory. The entire surgical procedure could be divided into a series of cognitive steps, such as decision making, problem solving, memory, attention, and judgment. Consequently, trainees can increase their familiarity with surgical tools and anatomical landmarks as well as become accustomed to the most common errors committed during any given surgical procedure (23, 24). However, the immersive experience and interaction with virtual objects in these web-based applications remains limited.
Therefore, we developed an iVR surgical learning system for orthognathic surgery, aiming to integrate the entire procedure of orthognathic surgery into the system with high fidelity. The operation room in our iVR system was created with rich details based on a real OR to provide the operator with an immersive learning environment.
Virtual models of all surgical instruments required during real-world operation were generated and could be freely selected and applied. The correct position and angle of several specific instruments were marked and recorded into the system.
There is a distinct gap between isolated skill training and performing the entire surgical procedure in the OR. Our procedural VR system helps the trainee combine each of these little steps simultaneously and complete the complex orthognathic procedure efficiently.
However, there are also limitations and challenges that need to be addressed. The iVR system's simulation was primarily focused on visual details, haptic feedback and physical interaction experiences are still lacking. VR dizziness and resolution ratio of HMD were the most common complaints by the participants, which could be improved in the future with continuous development of the iVR technique and commercial VR devices.
Additionally, there were also limitations of this study. The study had a limited sample size, and it lacked a control group for comparison.
Additional research is necessary, utilizing randomized controlled trials with a more substantial sample size. Future studies should evaluate the utility of VR training at various levels of surgical education and residency training.
iVR technology has the potential to revolutionize surgical training and education by providing standardized and cost-effective training, objective assessment, and multi-user capabilities. As the technology continues to develop and improve, it may become an increasingly valuable tool in surgical training and education.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
TW: contributed to data curation, statistical analysis and drafting of the manuscript. KL: contributed to data curation. BL: contributed to the development of the iVR training system and reviewing the manuscript. XW: contributed to reviewing and editing of the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by National Natural Science Foundation of China [grant number 81901066]; and Clinical Research Plan of Shanghai Hospital Development Center [grant number SHDC12019103].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rapp AK, Healy MG, Charlton ME, Keith JN, Rosenbaum ME, Kapadia MR. YouTube Is the most frequently used educational video source for surgical preparation. J Surg Educ. (2016) 73:1072–6. doi: 10.1016/j.jsurg.2016.04.024
2. Theelen L, Bischoff C, Grimm B, Heyligers IC. Current practice of orthopaedic surgical skills training raises performance of supervised residents in total knee arthroplasty to levels equal to those of orthopaedic surgeons. Perspect Med Educ. (2018) 7:126–32. doi: 10.1007/S40037-018-0408-Y
3. Khor WS, Baker B, Amin K, Chan A, Patel K, Wong J. Augmented and virtual reality in surgery-the digital surgical environment: applications, limitations and legal pitfalls. Ann Transl Med. (2016) 4:454. doi: 10.21037/atm.2016.12.23
4. Luca A, Giorgino R, Gesualdo L, Peretti GM, Belkhou A, Banfi G, et al. Innovative educational pathways in spine surgery: advanced virtual reality-based training. World Neurosurg. (2020) 140:674–80. doi: 10.1016/j.wneu.2020.04.102
5. Moorthy K, Munz Y, Adams S, Pandey V, Darzi A. A human factors analysis of technical and team skills among surgical trainees during procedural simulations in a simulated operating theatre. Ann Surg. (2005) 242:631–9. doi: 10.1097/01.sla.0000186298.79308.a8
6. Mao RQ, Lan L, Kay J, Lohre R, Ayeni OR, Goel DP, et al. Immersive virtual reality for surgical training: a systematic review. J Surg Res. (2021) 268:40–58. doi: 10.1016/j.jss.2021.06.045
7. van Merrienboer JJ, Sweller J. Cognitive load theory in health professional education: design principles and strategies. Med Educ. (2010) 44:85–93. doi: 10.1111/j.1365-2923.2009.03498.x
8. Su Z, Liu Y, Zhao W, Bai Y, Jiang N, Zhu S. Digital technology for orthognathic surgery training promotion: a randomized comparative study. PeerJ. (2022) 10:e13810. doi: 10.7717/peerj.13810
9. Atli K, Selman W, Ray A. A comprehensive multicomponent neurosurgical course with use of virtual reality: modernizing the medical classroom. J Surg Educ. (2021) 78:1350–6. doi: 10.1016/j.jsurg.2020.11.003
10. Seymour NE, Gallagher AG, Roman SA, O'Brien MK, Bansal VK, Andersen DK, et al. Virtual reality training improves operating room performance: results of a randomized, double-blinded study. Ann Surg. (2002) 236:458–63. discussion 63–4. doi: 10.1097/00000658-200210000-00008
11. Grantcharov TP, Kristiansen VB, Bendix J, Bardram L, Rosenberg J, Funch-Jensen P. Randomized clinical trial of virtual reality simulation for laparoscopic skills training. Br J Surg. (2004) 91:146–50. doi: 10.1002/bjs.4407
12. Dayal R, Faries PL, Lin SC, Bernheim J, Hollenbeck S, DeRubertis B, et al. Computer simulation as a component of catheter-based training. J Vasc Surg. (2004) 40:1112–7. doi: 10.1016/j.jvs.2004.09.028
13. Saratzis A, Calderbank T, Sidloff D, Bown MJ, Davies RS. Role of simulation in endovascular aneurysm repair (EVAR) training: a preliminary study. Eur J Vasc Endovasc Surg. (2017) 53:193–8. doi: 10.1016/j.ejvs.2016.11.016
14. Lu J, Cuff RF, Mansour MA. Simulation in surgical education. Am J Surg. (2021) 221:509–14. doi: 10.1016/j.amjsurg.2020.12.016
15. Grall P, Ferri J, Nicot R. Surgical training 2.0: a systematic approach reviewing the literature focusing on oral maxillofacial surgery—part I. J Stomatol Oral Maxillofac Surg. (2021) 122:411–22. doi: 10.1016/j.jormas.2021.01.006
16. Grall P, Ferri J, Nicot R. Surgical training 2.0: a systematic approach reviewing the literature focusing on oral maxillofacial surgery—part II. J Stomatol Oral Maxillofac Surg. (2021) 122:423–33. doi: 10.1016/j.jormas.2020.11.010
17. Orland MD, Patetta MJ, Wieser M, Kayupov E, Gonzalez MH. Does virtual reality improve procedural completion and accuracy in an intramedullary tibial nail procedure? A randomized control trial. Clin Orthop Relat Res. (2020) 478:2170–7. doi: 10.1097/CORR.0000000000001362
18. Pulijala Y, Ma M, Pears M, Peebles D, Ayoub A. An innovative virtual reality training tool for orthognathic surgery. Int J Oral Maxillofac Surg. (2018) 47:1199–205. doi: 10.1016/j.ijom.2018.01.005
19. Pulijala Y, Ma M, Pears M, Peebles D, Ayoub A. Effectiveness of immersive virtual reality in surgical training-A randomized control trial. J Oral Maxillofac Surg. (2018) 76:1065–72. doi: 10.1016/j.joms.2017.10.002
20. Wu F, Chen X, Lin Y, Wang C, Wang X, Shen G, et al. A virtual training system for maxillofacial surgery using advanced haptic feedback and immersive workbench. Int J Med Robot. (2014) 10:78–87. doi: 10.1002/rcs.1514
21. Arikatla VS, Tyagi M, Enquobahrie A, Nguyen T, Blakey GH, White R, et al. High fidelity virtual reality orthognathic surgery simulator. Proc SPIE Int Soc Opt Eng. (2018) 10576:1057612. doi: 10.1117/12.2293690
22. Chen X, Hu J. A review of haptic simulator for oral and maxillofacial surgery based on virtual reality. Expert Rev Med Devices. (2018) 15:435–44. doi: 10.1080/17434440.2018.1484727
23. Diaz-Siso JR, Plana NM, Stranix JT, Cutting CB, McCarthy JG, Flores RL. Computer simulation and digital resources for plastic surgery psychomotor education. Plast Reconstr Surg. (2016) 138:730e–8e. doi: 10.1097/PRS.0000000000002558
Keywords: immersive virtual reality, orthognathic surgery, surgery training, validity, surgical education and training
Citation: Wan T, Liu K, Li B and Wang X (2023) Validity of an immersive virtual reality training system for orthognathic surgical education. Front. Pediatr. 11:1133456. doi: 10.3389/fped.2023.1133456
Received: 29 December 2022; Accepted: 6 March 2023;
Published: 23 March 2023.
Edited by:
Songsong Zhu, Sichuan University, ChinaReviewed by:
Anand Marya, University of Puthisastra, Cambodia© 2023 Wan, Liu, Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xudong Wang eHVkb25nd2FuZzcwQGhvdG1haWwuY29t Biao Li YmVubGVleEBmb3htYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Pediatric Surgery, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.