
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 28 April 2023
Sec. Pediatric Urology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1110117
This article is part of the Research Topic Posterior Urethral Valves: Advances in Diagnosis, Management, and Long-Term Follow Up View all 7 articles
 Loes F. M. van der Zanden1*
Loes F. M. van der Zanden1* Sander Groen in ‘t Woud1
Sander Groen in ‘t Woud1 Iris A. L. M. van Rooij1
Iris A. L. M. van Rooij1 Josine S. L. T. Quaedackers2Martijn Steffens3
Josine S. L. T. Quaedackers2Martijn Steffens3 Liesbeth L. L. de Wall4
Liesbeth L. L. de Wall4 Michiel F. Schreuder5,†
Michiel F. Schreuder5,† Wout F. J. Feitz4,†Nel Roeleveld1,†
Wout F. J. Feitz4,†Nel Roeleveld1,†
Introduction: Posterior urethral valves (PUV) is a congenital disorder causing an obstruction of the lower urinary tract that affects approximately 1 in 4,000 male live births. PUV is considered a multifactorial disorder, meaning that both genetic and environmental factors are involved in its development. We investigated maternal risk factors for PUV.
Methods: We included 407 PUV patients and 814 controls matched on year of birth from the AGORA data- and biobank and three participating hospitals. Information on potential risk factors (family history of congenital anomalies of the kidney and urinary tract (CAKUT), season of conception, gravidity, subfertility, and conception using assisted reproductive techniques (ART), plus maternal age, body mass index, diabetes, hypertension, smoking, and use of alcohol and folic acid) was derived from maternal questionnaires. After multiple imputation, adjusted odds ratios (aORs) were estimated using conditional logistic regression corrected for minimally sufficient sets of confounders determined using directed acyclic graphs.
Results: A positive family history and low maternal age (<25 years) were associated with PUV development [aORs: 3.3 and 1.7 with 95% confidence intervals (95% CI) 1.4–7.7 and 1.0–2.8, respectively], whereas higher maternal age (>35 years) was associated with a lower risk (aOR: 0.7 95% CI: 0.4–1.0). Maternal preexisting hypertension seemed to increase PUV risk (aOR: 2.1 95% CI: 0.9–5.1), while gestational hypertension seemed to decrease this risk (aOR: 0.6 95% CI: 0.3–1.0). Concerning use of ART, the aORs for the different techniques were all above one, but with very wide 95% CIs including one. None of the other factors studied were associated with PUV development.
Conclusion: Our study showed that family history of CAKUT, low maternal age, and potentially preexisting hypertension were associated with PUV development, whereas higher maternal age and gestational hypertension seemed to be associated with a lower risk. Maternal age and hypertension as well as the possible role of ART in the development of PUV require further research.
Posterior urethral valves (PUV) is a congenital anomaly of the lower urinary tract in boys that impairs urinary flow. It is a prevalent cause of end-stage kidney disease in children (1) and affects approximately 1 in 4,000 live male births (2). The precise embryological mechanism that results in PUV is uncertain, but the most common theory is that PUVs develop when the mesonephric duct fuses with the cloaca in the 4th or 5th week after conception (which equals week 6 or 7 of pregnancy) (3, 4). PUV is considered to be a multifactorial disorder, meaning that both genetic and environmental factors are involved in its development (5).
Little research has been performed on possible risk factors associated with PUV specifically, as most research so far focused on congenital anomalies of the kidney and urinary tract (CAKUT) as a whole (6). Several studies that focussed on CAKUT in general but included patients with obstructive uropathies (such as PUV) or urethral malformations, found associations between CAKUT and maternal factors, such as age (7), obesity (6, 8, 9), gravidity (7), use of assisted reproductive techniques (ART) (6), and diabetes (6–8, 10). However, other studies were unable to confirm the association with obesity (11). Maternal subfertility (6), hypertension (7), smoking (6, 7, 12), and alcohol use (6, 7) did not seem to be associated with CAKUT, while use of folic acid supplements or folic-acid containing multivitamins was found to be protective (6, 13, 14).
Previous studies showed that separate analyses for different CAKUT phenotypes or for higher vs. lower urinary tract anomalies gave dissimilar results (6, 9). For example, high maternal body mass index (BMI) was associated with upper but not lower urinary tract anomalies. Periconceptional folic acid use was associated with some CAKUT phenotypes but not with PUV, while PUV was the only phenotype associated with gestational diabetes (6, 9). More knowledge on the aetiology of PUV is needed, in order to take preventive measures for PUV, such as adaptation in perinatal care. Therefore, we investigated maternal risk factors for PUV in this study.
AGORA (Aetiologic research into Genetic and Occupational/environmental Risk factors for Anomalies in children) is a large data- and biobank that was initiated in the Radboud university medical center (Radboudumc), Nijmegen, the Netherlands, in which questionnaire data, blood/saliva samples, and phenotypic information are collected from patients with congenital malformations and their parents (15). The AGORA questionnaires are filled out on paper and inquire about demographics, family and pregnancy history, and health and lifestyle in the three months before and during pregnancy.
For the current project, we selected the patients with PUV from the Dutch patient population that we collected for our studies on obstructive uropathy (16). In these studies, we included both patients with ureteropelvic-junction obstruction (UPJO) and PUV who were born in 1981 or later and underwent a pyeloplasty (for UPJO) or valve resection (for PUV) before the age of 18 years from the AGORA data- and biobank. In addition, we searched the medical registry of the Radboudumc to identify more patients born in 1981 or later who underwent a pyeloplasty or valve resection before 18 years of age. We also searched the medical registries of the Isala clinics in Zwolle and the University Medical Center in Groningen (UMCG) where, due to registration issues, we were only able to identify patients treated in 2002 or later. The newly identified patients or their parents (depending on the patients' age) were approached to participate in our obstructive uropathy studies by providing saliva samples and completing the AGORA questionnaires either online or on paper. From all of the participants, only patients who underwent a valve resection were included in the current study.
In 2010–2011, controls were recruited through 39 municipalities, covering the referral areas of the hospitals through which patients were included in AGORA. These villages and cities were asked to provide a random sample of 150 or 300 of their inhabitants in the age range of 0 to 20 years, which was comparable to that of the patient population at time of recruitment. The parents of these children were asked to fill out the same paper questionnaire as the parents of the patients. In 2021, the control population was supplemented with data from children from 28 municipalities born between 2011 and 2021 using a similar approach. In addition, we asked the parents of the patients who completed the questionnaire online to ask parents of a healthy child of similar age to fill out the same online questionnaire. For the current project, we selected only male controls without major structural birth defects as defined by EUROCAT (17).
The Medical Ethics Assessment Committee East Netherlands (METC Oost-Nederland) approved the AGORA data- and biobank (2006-048, 2018-4524 and 2021-13067), while the board of directors of the Isala clinics and the UMCG approved implementation of AGORA in these centers. All participants and/or their parents gave written informed consent for participation in the study.
Information about potential risk factors, variables to be used in imputation, and possible confounders was derived from the questionnaires. We considered the following potential risk factors for PUV: family history of CAKUT, season of conception, gravidity, subfertility and conception using ART, as well as maternal age, BMI, diabetes, hypertension, smoking, alcohol consumption, and use of folic acid or folic-acid containing multivitamins. Several other factors, such as duration of pregnancy, year of birth, birthweight, ethnicity, and education, were abstracted to be used in imputation or as possible confounding variables.
Family history was defined as self-reported maternal or paternal CAKUT. Season of conception was derived from the date of birth and pregnancy duration. Gravidity was categorized into first or subsequent pregnancy. Couples were considered fertile if the parents indicated in the questionnaire not to be subfertile and the time to pregnancy was less than 12 months. Subfertile couples were divided into a subfertile group that conceived the index pregnancy without ART, a group using intra-uterine insemination (IUI) without using hormones, a group using hormonal treatment with or without IUI, and a group using in-vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI). Maternal age was categorized into younger (<25 years), average (25–34 years), and older (≥35 years) age and maternal BMI into underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥ 30.0 kg/m2). Diabetes was considered to be preexisting when women reported it from the start of pregnancy and gestational when it was first diagnosed during the index pregnancy. Preexisting hypertension was defined as any hypertension discovered before the 20th week of gestation, in accordance with guidelines from the American College of Obstetricians and Gynecologists (18), while gestational hypertension appeared from week 20 onwards. For maternal smoking and alcohol use, mothers were divided into a group that smoked or used alcohol during the etiologically relevant period (defined as using before pregnancy and not stopping before the sixth week of pregnancy), a group that smoked or used alcohol prior to the etiologically relevant period (defined as any smoking or alcohol use in the three months before or during the first five weeks of pregnancy only), and a group that did not smoke or use alcohol in the three months before and during pregnancy. For maternal use of folic acid supplements or folic acid-containing multivitamins, mothers were divided into a group that used these supplements as recommended (defined as starting usage before pregnancy and not stopping before the eighth week of pregnancy), a group with suboptimal use (defined as using folic acid supplements or folic-acid containing multivitamins in the four weeks before pregnancy or in the first eight weeks of pregnancy, but not the entire period), and a group that did not use these supplements in this period.
Each patient was matched to two controls born in the same year to account for differences in year of childbirth between patients and controls. Crude odds ratios (ORs) with 95% confidence intervals (CIs) were estimated for the potential risk factors using conditional logistic regression.
For each potential risk factor separately, a minimally sufficient set of confounders was determined using a directed acyclic graph (DAG) created in DAGitty (19). Figure 1 contains the DAG with all our assumptions about causal associations between the potential risk factors and the potential confounders maternal education (divided into low, medium, and high) and ethnicity (defined as European or other). As an example, gravidity was selected as potential risk factor in the DAG in Figure 1, which also shows the minimally sufficient set of confounders for the association between gravidity and PUV.
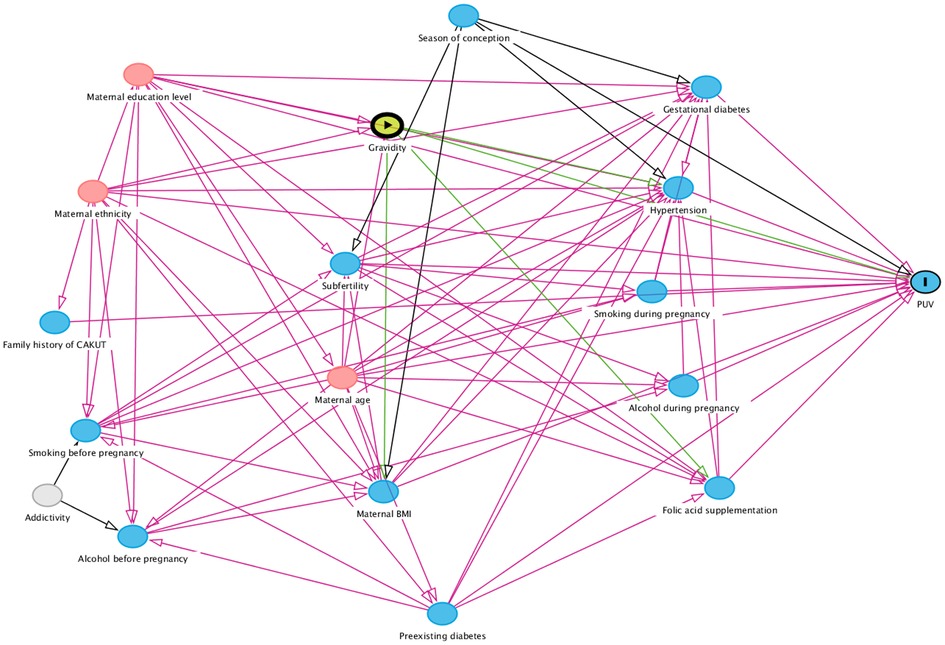
Figure 1. Directed acyclic graph containing all potential risk factors and confounders with their causal relations. Blue circles with black lining: outcome. Blue circles: ancestors of outcome. Pink circles: ancestors of exposure and outcome. Yellow circle: exposure. Grey circle: unobserved variable. BMI, body mass index; CAKUT, congenital anomalies of the kidney and urinary tract; PUV, posterior urethral valves.
We used all patients and controls to perform multiple imputation to generate ten imputed datasets. In the imputation, we used all potential risk factors and confounders as well as the outcome, the duration of pregnancy, birthweight, the time between birth and filling out the questionnaire, whether the questionnaire was completed online or on paper, and year of birth. After imputation, adjusted ORs were estimated in the matched patient-control sets using conditional logistic regression corrected for the relevant minimally sufficient set of confounders, plus a variable indicating whether the questionnaire was completed online or on paper. Adjusted ORs were not estimated when five or fewer patients were exposed. Matching, data imputation, and statistical analyses were performed using IBM SPSS statistics version 27.0.
Figure 2 shows the inclusion and selection of patients and controls. For our studies on obstructive uropathy, 399 eligible patients were included in the AGORA data- and biobank. We identified 247 additional obstructive uropathy patients in the Radboudumc, 131 in the Isala clinics, and 270 in the UMC Groningen. Of these, 143 (53%), 86 (66%) and 161 (60%) patients, respectively, responded positively and participated. We excluded 323 patients who did not have a valve resection, resulting in 466 PUV patients for the current study. A total number of 6,669 and 5,634 control families were asked to fill out the AGORA questionnaires in 2010 and 2021, respectively. Of these, 2,267 (34%) and 1,631 (29%) responded. In addition, the parents of 414 healthy children recruited by parents of patients completed the questionnaire online. We selected the 1,976 male controls without major birth defects for which at least the question about year of childbirth was filled out. Each patient was matched to two controls born in the same year to account for differences in year of childbirth between patients and controls. Therefore, we had to exclude all 35 patients born between 1981 and 1990 and 24 patients born in later years due to a lack of controls from those birth years. As a result, we performed our analyses with 407 PUV patients and 814 male controls. Part of this study population (N = 127 patients) was used in a previous study in which we investigated 562 CAKUT patients, but also performed subgroup analyses for separate phenotypes including PUV (6). Table 1 shows that most patients and controls in the current study were born from 2000 onwards. Mothers of controls reported slightly more often to be highly educated and much more often completed the questionnaire on paper, with only 7% of control parents and 40% of patient parents completing the questionnaire online. Time between childbirth and completion of the questionnaires was similar for patients and controls, and generally 5 years or longer.
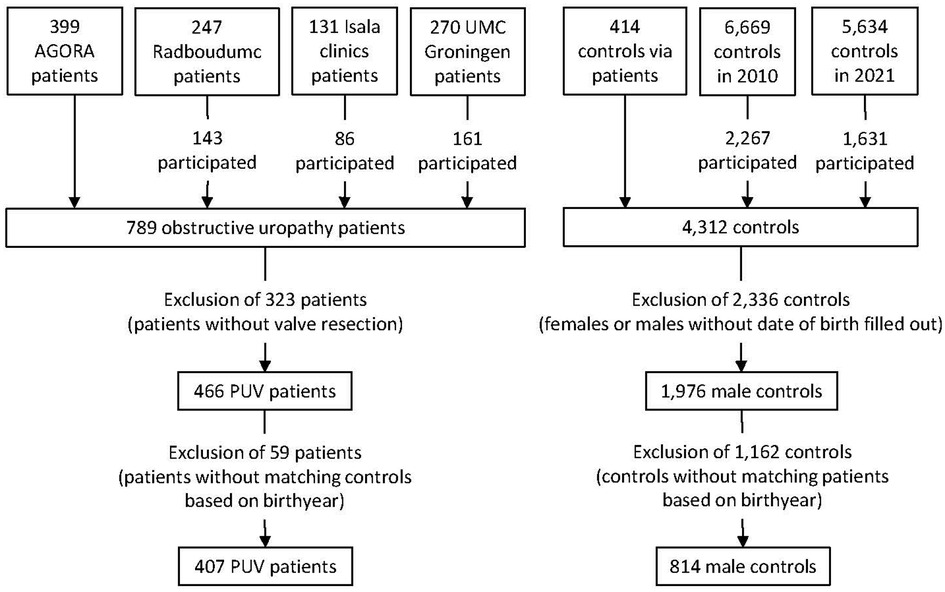
Figure 2. Flowchart showing the selection and in- and exclusion of patients and controls in the current study. PUV, posterior urethral valves.
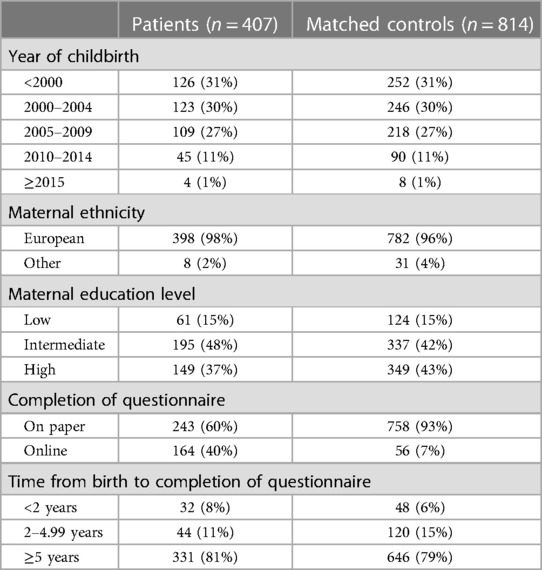
Table 1. Characteristics of patients with posterior urethral valves and healthy population-based controls matched on year of childbirth.
The results of the univariable and multivariable conditional logistic regression analyses are displayed in Table 2. A positive family history of CAKUT and low maternal age (<25 years) were associated with PUV development in both univariable and multivariable analyses (adjusted odds ratios (aOR) 3.3 and 1.7 with 95% confidence intervals (95% CI) 1.4–7.7 and 1.0–2.8, respectively), whereas higher maternal age (≥35 years) was associated with a lower risk (aOR: 0.7 95% CI: 0.4–1.0). Maternal preexisting hypertension seemed to be associated with an increased PUV risk (aOR: 2.1 95% CI: 0.9–5.1), while maternal gestational hypertension seemed to be associated with a decreased risk (aOR: 0.6 95% CI: 0.3–1.0). Concerning use of ART, the aORs for the different techniques were all above 1, ranging from 1.4 to 2.0, but with very wide 95% CIs including one. Slightly increased aORs of 1.4 with 95% CIs including one were also observed for women with underweight, obesity, or gestational diabetes. None of the other factors studied were associated with PUV development.
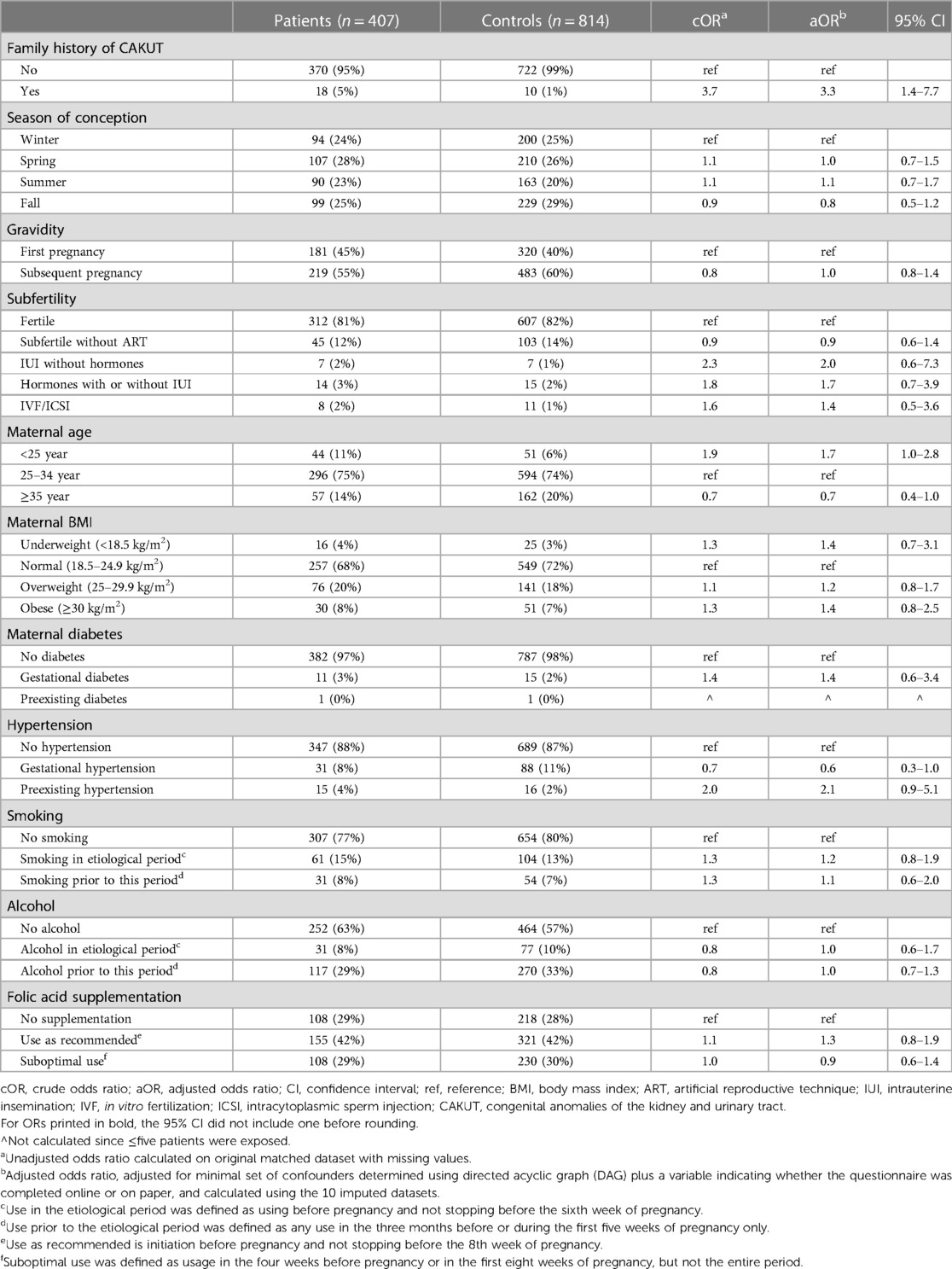
Table 2. Crude and adjusted odds ratios for the associations between potential risk factors and posterior urethral valves.
In the current case-control study with 407 PUV patients and 814 population based-controls, we identified family history of CAKUT and low maternal age as potential risk factors for PUV development, whereas higher maternal age was associated with a lower risk. Maternal preexisting hypertension seemed to increase PUV risk, while gestational hypertension seemed to decrease this risk. Concerning use of ART, the aORs for the different techniques were all above one, but with very wide 95% CIs including one.
This retrospective study included patients and controls born from 1990 onwards. Because several exposures, such as use of folic acid supplements and smoking during pregnancy, changed considerably in the past three decades, we used matching on year of childbirth to prevent confounding by changes over time. A strength of our study is the large number of patients with a well-defined phenotype, in contrast to previous studies that often included a broad range of CAKUT patients. This is especially important as it has been debated whether PUV is part of the CAKUT phenotype spectrum and the possibility of a different underlying cause has been suggested for this specific phenotype (20). Another strength is the availability of information on many potential risk factors and confounders. We used DAGs to select minimally needed sets of confounders for each of the prespecified risk factors, which increases statistical efficiency and avoids overcorrection introducing bias (21). By displaying all possible relations in the DAG, we made the assumptions about causal associations between variables explicit. Despite these strengths, causality cannot be proven with a retrospective observational study like ours.
The time between childbirth and completion of the questionnaire was 5 years or more for ∼80% of the population. Although the time to completion was comparable among mothers of patients and controls, the large time gap may have resulted in some recall errors. The majority of factors that we studied, however, represent maternal or pregnancy characteristics that can easily be retrieved (season of conception, gravidity, subfertility, maternal age, and parental CAKUT) or were clear health conditions (diabetes and hypertension). Therefore, we believe that recall errors for these factors would have been limited and most likely non-differential, only leading to slight underestimation of the odds ratios. The lifestyle habits that we investigated (maternal BMI, smoking, alcohol, and folic acid use) are usually easy to remember in the well-defined period of pregnancy as well, but some differential recall bias cannot be ruled out for these factors. In addition, the way the questionnaire was completed (online or on paper) may have resulted in differential responses. However, the questions were asked exactly the same in both versions and we corrected all of our analyses for the variable indicating online or on paper completion.
PUV is considered to be a multifactorial disorder involving both non-genetic and genetic factors, as familial forms (22) as well as affected sib-pairs have been described (23) and a classical twin study found higher concordance rates among monozygotic compared to dizygotic twin pairs (5). The fact that a family history of CAKUT was the strongest risk factor found in our study supports this hypothesis. Genetic studies previously showed that copy number variants (CNVs) could play a role (24, 25), while associations with common variants have also been reported (26, 27).
We observed an association between PUV and younger maternal age and a protective effect of more advanced maternal age, whereas a previous study that focussed on patients with ureter, bladder, and urethra abnormalities found advanced maternal age to be a risk factor (7). Although the common thought is that advanced maternal age negatively impacts pregnancy outcomes (28), another study showed associations between maternal age and renal agenesis similar to our estimates (29). Therefore, further research into the role of maternal age is warranted.
Our study also points towards an association between PUV and maternal preexisting hypertension, while gestational hypertension seemed to decrease the risk. Gestational hypertension was defined as hypertension detected in the 20th week of pregnancy or later, well after the etiologically relevant period. Therefore, it seems unlikely that gestational hypertension reduces the risk of PUV, although an underlying condition predisposing to gestational hypertension may perhaps play a role. Preexisting hypertension was not associated with ureter, bladder and urethra abnormalities or with other CAKUT phenotypes in most previous studies (7, 30, 31), although the most recent study did find an increased risk (32). Maternal hypertension was consistently associated with hypospadias (33), however, which also is a defect of the urethra and may partly share its' aetiology with PUV. For hypospadias, the association with maternal hypertension was hypothesized to be caused by placental dysfunction in early pregnancy (33). Whether a similar mechanism may be involved in PUV, warrants further research.
Maternal subfertility was not associated with PUV in our study, whereas use of ART may be although the confidence intervals were very wide and included one. An association with ART would be consistent with the results of our previous study (6) and with the slightly elevated risk of urogenital anomalies after ART reported by an Australian registry study (34). ART may lead to congenital defects via the hormonal treatment interfering with the foetal endocrine system, via the in vitro procedures of IVF/ICSI involving a risk of epigenetic defects (35), or via factors underlying the subfertility and the need to use ART.
Weak potential associations were also observed for obesity and gestational diabetes, but again the wide 95% CIs included one. Most previous studies on CAKUT in general but including patients with obstructive uropathy or urethral malformations showed associations with maternal obesity (6, 8, 9) and gestational diabetes (6–8, 10). One study did not find an association with obesity (11) and in two studies the association with obesity disappeared when focussing on patients with lower urinary tract anomalies or PUV only (6, 9). Regarding gestational diabetes, Shnorhavorian et al. found a stronger effect in the phenotypes affecting the kidneys (7), whereas we previously showed that this effect was stronger in PUV patients (6).
We did not find any association with season of conception, smoking, or alcohol use, which is consistent with most previous studies (6, 7, 12). We were unable to confirm the previously reported association with gravidity (7, 32) and the protective effect of the use of folic acid supplements or folic-acid containing multivitamins (6, 13, 14). The latter is consistent with our previous finding of the protective effect of folic acid among CAKUT patients disappearing when focussing on PUV patients only (6).
In conclusion, our study shows that family history of CAKUT and low maternal age are associated with an increased risk of PUV development, while higher maternal age was associated with a lower risk. Maternal preexisting hypertension seemed to be associated with an increased PUV risk as well. Both preexisting and gestational hypertension and maternal age as well as the possible role of ART require further research. We suggest that future studies on the etiology of CAKUT should stratify on different phenotypes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical Ethics Assessment Committee East Netherlands (METC Oost-Nederland). Written informed consent to participate in this study was provided by the participants or their legal guardian/next of kin.
LZ and SG designed and performed the analyses. LZ, SG, IR, JQ, MS, LW, MS, WF, and NR were involved in recruitment of patients and controls. LZ designed the study and wrote the manuscript. MFS, WF and NR oversaw the study. All authors contributed to the article and approved the submitted version.
This research was funded by a Veni grant (91618036) from the Dutch Research Council (NWO) provided to LZ. In addition, LZ and SG are funded by a Consortium Grant of the Dutch Kidney Foundation (20OC002). MFS is funded by a Vidi grant (016.156.454) from the Dutch Research Council (NWO).
We would like to thank everyone involved in data collection, and all patients and parents for their cooperation in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hamilton AJ, Braddon F, Casula A, Inward C, Lewis M, Mallett T, et al. UK renal registry 18th annual report: chapter 4 demography of patients receiving renal replacement therapy in paediatric centres in the UK in 2014. Nephron. (2016) 132(Suppl 1):99–110. doi: 10.1159/000444818
2. Brownlee E, Wragg R, Robb A, Chandran H, Knight M, McCarthy L, et al. Current epidemiology and antenatal presentation of posterior urethral valves: outcome of BAPS CASS national audit. J Pediatr Surg. (2019) 54(2):318–21. doi: 10.1016/j.jpedsurg.2018.10.091
3. Krishnan A, de Souza A, Konijeti R, Baskin LS. The anatomy and embryology of posterior urethral valves. J Urol. (2006) 175(4):1214–20. doi: 10.1016/S0022-5347(05)00642-7
4. Elumalai G, Mdletshe MB. “Posterior urethral valves” embryological basis and its clinical significance. Elixir Embryol. (2017) 103:45661–4. https://www.researchgate.net/publication/313863457_POSTERIOR_URETHRAL_VALVES_EMBRYOLOGICAL_ BASIS_AND_ITS_CLINICAL_SIGNIFICANCE
5. Frese S, Weigert A, Hoppe B, Feldkotter M, Ludwig M, Weber S, et al. A classic twin study of lower urinary tract obstruction: report of 3 cases and literature review. Low Urin Tract Symptoms. (2019) 11(2):O85–O8. doi: 10.1111/lluts.12222
6. Groen In ‘t Woud S, Renkema KY, Schreuder MF, Wijers CH, van der Zanden LF, Knoers NV, et al. Maternal risk factors involved in specific congenital anomalies of the kidney and urinary tract: a case-control study. Birth Defects Res A Clin Mol Teratol. (2016) 106(7):596–603. doi: 10.1002/bdra.23500
7. Shnorhavorian M, Bittner R, Wright JL, Schwartz SM. Maternal risk factors for congenital urinary anomalies: results of a population-based case-control study. Urology. (2011) 78(5):1156–61. doi: 10.1016/j.urology.2011.04.022
8. Hsu CW, Yamamoto KT, Henry RK, De Roos AJ, Flynn JT. Prenatal risk factors for childhood CKD. J Am Soc Nephrol. (2014) 25(9):2105–11. doi: 10.1681/ASN.2013060582
9. Macumber I, Schwartz S, Leca N. Maternal obesity is associated with congenital anomalies of the kidney and urinary tract in offspring. Pediatr Nephrol. (2017) 32(4):635–42. doi: 10.1007/s00467-016-3543-x
10. Banhidy F, Acs N, Puho EH, Czeizel AE. Congenital abnormalities in the offspring of pregnant women with type 1, type 2 and gestational diabetes mellitus: a population-based case-control study. Congenit Anom (Kyoto). (2010) 50(2):115–21. doi: 10.1111/j.1741-4520.2010.00275.x
11. Watkins ML, Rasmussen SA, Honein MA, Botto LD, Moore CA. Maternal obesity and risk for birth defects. Pediatrics. (2003) 111(5 Pt 2):1152–8. doi: 10.1542/peds.111.S1.1152
12. Kallen K. Maternal smoking and urinary organ malformations. Int J Epidemiol. (1997) 26(3):571–4. doi: 10.1093/ije/26.3.571
13. Czeizel AE, Dobo M, Vargha P. Hungarian cohort-controlled trial of periconceptional multivitamin supplementation shows a reduction in certain congenital abnormalities. Birth Defects Res A Clin Mol Teratol. (2004) 70(11):853–61. doi: 10.1002/bdra.20086
14. Werler MM, Hayes C, Louik C, Shapiro S, Mitchell AA. Multivitamin supplementation and risk of birth defects. Am J Epidemiol. (1999) 150(7):675–82. doi: 10.1093/oxfordjournals.aje.a010070
15. van Rooij IA, van der Zanden LF, Bongers EM, Renkema KY, Wijers CH, Thonissen M, et al. AGORA, a data- and biobank for birth defects and childhood cancer. Birth Defects Res A Clin Mol Teratol. (2016) 106(8):675–84. doi: 10.1002/bdra.23512
16. van der Zanden LFM, van Rooij I, Quaedackers J, Nijman RJM, Steffens M, de Wall LLL, et al. CDH12 as a candidate gene for kidney injury in posterior urethral valve cases: a genome-wide association study among patients with obstructive uropathies. Eur Urol Open Sci. (2021) 28:26–35. doi: 10.1016/j.euros.2021.04.001
17. EUROCAT Central Registry UoU. EUROCAT Guide 1.4: Instruction for the registration of congenital anomalies. (2013).
18. Gestational hypertension and preeclampsia: aCOG practice bulletin, number 222. Obstet Gynecol. (2020) 135(6):e237–e60. doi: 10.1097/AOG.0000000000003891
19. Textor J, Hardt J, Knuppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology. (2011) 22(5):745. doi: 10.1097/EDE.0b013e318225c2be
20. Renkema KY, Winyard PJ, Skovorodkin IN, Levtchenko E, Hindryckx A, Jeanpierre C, et al. Novel perspectives for investigating congenital anomalies of the kidney and urinary tract (CAKUT). Nephrol Dial Transplant. (2011) 26(12):3843–51. doi: 10.1093/ndt/gfr655
21. Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. (1999) 10(1):37–48. doi: 10.1097/00001648-199901000-00008
22. Hanlon-Lundberg KM, Verp MS, Loy G. Posterior urethral valves in successive generations. Am J Perinatol. (1994) 11(1):37–9. doi: 10.1055/s-2007-994532
23. Schreuder MF, van der Horst HJ, Bokenkamp A, Beckers GM, van Wijk JA. Posterior urethral valves in three siblings: a case report and review of the literature. Birth Defects Res A Clin Mol Teratol. (2008) 82(4):232–5. doi: 10.1002/bdra.20439
24. Boghossian NS, Sicko RJ, Kay DM, Rigler SL, Caggana M, Tsai MY, et al. Rare copy number variants implicated in posterior urethral valves. Am J Med Genet A. (2016) 170(3):622–33. doi: 10.1002/ajmg.a.37493
25. Caruana G, Wong MN, Walker A, Heloury Y, Webb N, Johnstone L, et al. Copy-number variation associated with congenital anomalies of the kidney and urinary tract. Pediatr Nephrol. (2015) 30(3):487–95. doi: 10.1007/s00467-014-2962-9
26. Laksmi NK, Khullar M, Kaur B, Ahuja M, Mahajan JK, Mittal BR, et al. Association of angiotensin converting enzyme and angiotensin type 2 receptor gene polymorphisms with renal damage in posterior urethral valves. J Pediatr Urol. (2010) 6(6):560–6. doi: 10.1016/j.jpurol.2010.01.002
27. van der Zanden LFM, Maj C, Borisov O, van Rooij I, Quaedackers J, Steffens M, et al. Genome-wide association study in patients with posterior urethral valves. Front Pediatr. (2022) 10:988374. doi: 10.3389/fped.2022.988374
28. Zhang C, Yan L, Qiao J. Effect of advanced parental age on pregnancy outcome and offspring health. J Assist Reprod Genet. (2022) 39(9):1969–86. doi: 10.1007/s10815-022-02533-w
29. Parikh CR, McCall D, Engelman C, Schrier RW. Congenital renal agenesis: case-control analysis of birth characteristics. Am J Kidney Dis. (2002) 39(4):689–94. doi: 10.1053/ajkd.2002.31982
30. Dart AB, Ruth CA, Sellers EA, Au W, Dean HJ. Maternal diabetes mellitus and congenital anomalies of the kidney and urinary tract (CAKUT) in the child. Am J Kidney Dis. (2015) 65(5):684–91. doi: 10.1053/j.ajkd.2014.11.017
31. Nishihama Y, Tatsuta N, Iwai-Shimada M, Nakai K, Arima T, Fujiwara I, et al. The association between gestational use of personal care products and neonatal urological abnormality at birth: the Japan environment and children's study. Reprod Toxicol. (2020) 93:83–8. doi: 10.1016/j.reprotox.2020.01.005
32. van der Zanden LF, van Rooij IA, Feitz WF, Franke B, Knoers NV, Roeleveld N. Aetiology of hypospadias: a systematic review of genes and environment. Hum Reprod Update. (2012) 18(3):260–83. doi: 10.1093/humupd/dms002
33. Boato RT, Aguiar MB, Mak RH, Colosimo EA, Simões E Silva AC, Oliveira EA. Maternal risk factors for congenital anomalies of the kidney and urinary tract: a case-control study. J Pediatr Urol. (2023) 19(2):199.e1-11. doi: 10.1016/j.jpurol.2022.11.025
34. Davies MJ, Moore VM, Willson KJ, Van Essen P, Priest K, Scott H, et al. Reproductive technologies and the risk of birth defects. N Engl J Med. (2012) 366(19):1803–13. doi: 10.1056/NEJMoa1008095
Keywords: environment, exposure, maternal, posterior urethral valves (PUV), risk factors
Citation: van der Zanden LFM, Groen in ‘t Woud S, van Rooij IALM, Quaedackers JSLT, Steffens M, de Wall LLL, Schreuder MF, Feitz WFJ and Roeleveld N (2023) Maternal risk factors for posterior urethral valves. Front. Pediatr. 11:1110117. doi: 10.3389/fped.2023.1110117
Received: 28 November 2022; Accepted: 10 April 2023;
Published: 28 April 2023.
Edited by:
Massimo Garriboli, Guy's and St Thomas’ NHS Foundation Trust, United KingdomReviewed by:
Jaime Restrepo, Valle del Lili Foundation, Colombia© 2023 van der Zanden, Groen In ‘t Woud, van Rooij, Quaedackers, Steffens, de Wall, Schreuder, Feitz and Roeleveld. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Loes F. M. van der Zanden bG9lcy52YW5kZXJ6YW5kZW5AcmFkYm91ZHVtYy5ubA==
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.