 Robert Woroniecki1*
Robert Woroniecki1* Michael L. Moritz2
Michael L. Moritz2
- 1Stony Brook Children’s, Stony Brook University, Stony Brook, NY, United States
- 2UPMC Children’s Hospital of Pittsburgh, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States
Human spirit is an integral part of the medicinal art and science trifecta: body-mind-spirit, and it is contained in the World Health Organization definition of health. Human spirit is defined as our purpose in life, relationships with all living creatures or “Higher Power”, and in general our place on planet Earth. Spirituality is a required part of patient care according to Joint Commission on Accreditation of Health Care Organizations. There is an abundant medical literature that documents discrepancies in the results between studies and populations, and points to the importance of cultural, ethnic, spiritual or religious differences. Validated questionnaires used in research for last several decades demonstrated an association of spirituality with clinical outcomes, coping, and quality of life in different adult chronic diseases. There are also validated scales to measure hope in children based on the premise that children are goal directed and that their goal-related thoughts can be understood, yet their purposefulness, meaning of life and spirit in pediatric nephrology remains mostly unexamined. Although pediatric nephrology has made significant advances in molecular techniques, artificial intelligence, machine learning, and started to address more broad social issues such as racism, health equity, diversity of our work force, etc, it lacks both systematic ways of studying and philosophical approach to fostering human spirit. This mini review examines the place and knowledge gaps in human spirit and spirituality in pediatric nephrology. We review the concept of the human spirit and medical literature pertaining to its role in pediatric nephrology.
Introduction
Kidney disease is fortunately not a common factor contributing to pediatric mortality. The primary causes of death in US American children, adolescent and young adults are fire arms, motor vehicle accidents, neoplasms, suffocation/drowning, drugs, or congenital anomalies (1). Over last few decades, pediatric nephrology has advanced with discoveries of several genetic, epigenetic and molecular mechanisms behind nephron injury and hypertension. Pediatric Nephrologists began recognizing the importance of other external factors that determine “renal health”, such as prematurity, race/ethnicity, socioeconomic factors, poverty, food insecurity, housing, immigration, physical activity, obesity, gender preference, and mental illness. An area that has not been well evaluated is the impact of human spirit in children with kidney disease.
Human spirit
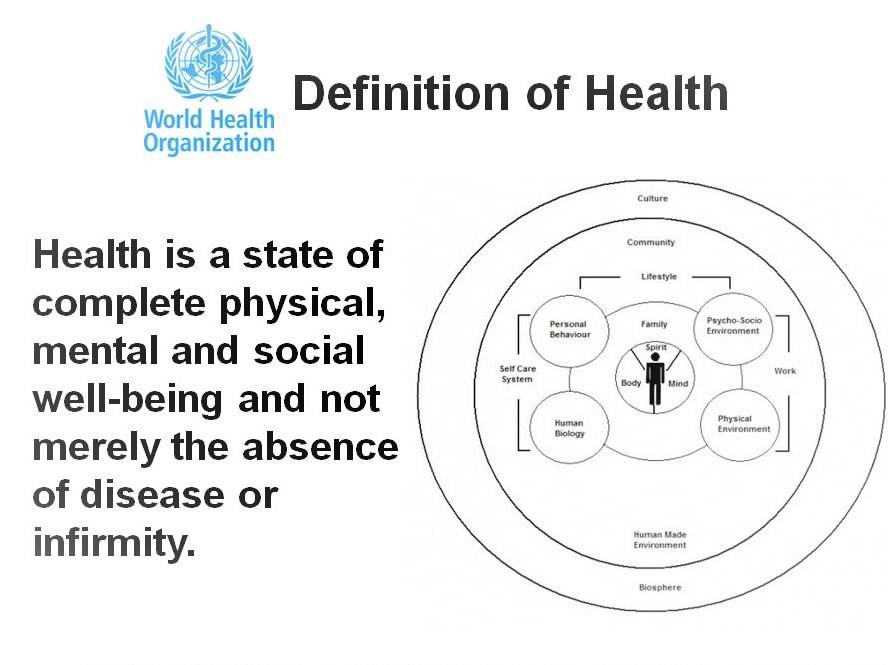
Spirit is a part of the medicinal art and science trifecta: body-mind-spirit. The World Health Organization (WHO) puts spirit at co-existence with body and mind in its definition of health (Figure 1) (2). Spirituality is also an integral part of patient care according to Joint Commission on Accreditation of Health Care Organizations, and specific instructions dealing with it were issued in 2005 and have remained since (3). Spirit has been an essential part of philosophical science throughout history, embracing the study of nature, principles of reality, knowledge, and values based on logic and reasoning (4).
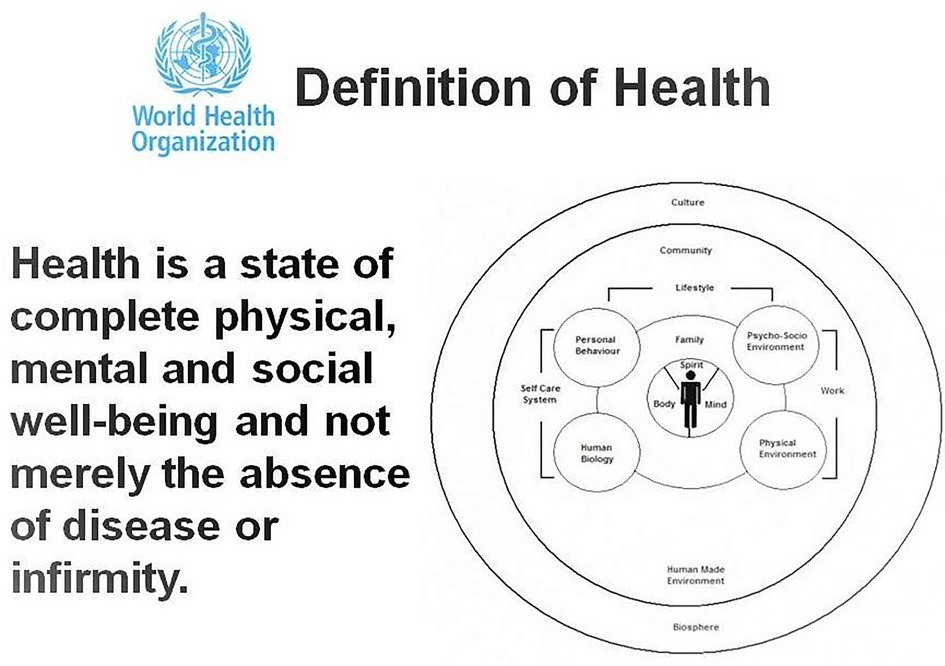
Figure 1. WHO definition of health. https://www.publichealth.com.ng/wp-content/uploads/2019/08/who-definition-of-health-1.jpg.
{kind=link}
Spirit definition
The spirit and soul are not synonymous. They have had distinctive names in ancient cultures: in Hebrew they were called ruach and nephesh, which means “wind” and “breath” in Persian: ahu and urvan, in Buddhist and Hindu: monuhmed and gyan, and in Greek: pneuma and psyche (5). Spirit (“wind”) is the one that connects us to our external life, its purpose, relationship with other humans, animals, nature, or God. It is not our environment but rather a link “air” between the environment and our body and mind. Soul (“breath, psyche, mind”) connects us to the internal life, or our senses, emotions, desires, affections, and appetites, aches, body illness, etc. In Latin, the word spirit is related to the vital process of exchanging air, i.e., spirare means to breathe (6). Indigenous people belief that all nature-made (but not man-made) objects, for example, stone, lake, mountain, have their natural spirits (life purpose) (7). Since ancient times, scientists and philosophers like Aristotle recognized that the basic meaning of life refers to the ability of humans to formulate and implement purposes (8). Purposefulness is at the root of our species dominance allowing us to conquer the Earth, or travel to the Moon. Purposefulness is also one of humanities great shortcomings, allowing us to wage wars, eradicate other species, or other peoples (9). The role of human will was examined by Arthur Schopenhauer who proclaimed; “Man's world is based on man's will and is his idea of the world.” (10). Schopenhauer refers to will as the inner essence of everything: a blind, unconscious, aimless striving devoid of knowledge, outside of space and time, and free of all multiplicity. In his essay on the “free will”, he connects the will and self-consciousness (11). Albert Einstein summarized his philosophy as “a man can do as he will, but not will as he will” (12), and stressed importance of imagination over knowledge in creating solutions and human progress (13). If patients or parents cannot imagine solutions to problems life brings, they will not solve them.
Role of spirit in medical arts
Our current US Healthy People 2030 government programs (14) focus on eliminating health disparities, creating equitable opportunities for people to live healthy lives, to advance health equity, increase health literacy, and address social determinants of health (SDOH). However, it should be noted that SDOH, are not equal to the human spirit, as they do not take into consideration the purpose of individual life. SDOH deal with conditions in the environments where people live, work, develop or age, and those factors are much easier to describe and quantify than individual human spirit formation. Patient economic stability, access to health, transportation, education, job, salary, exposure to violence, racism, etc, although important for health outcomes do not take into consideration individual spirit. SDOH do not define human spirit; do not seek its origin and the ways to foster it. It does not address basic need of human connections with Mother Nature, with human mother, does not specifically support fathers and inter-human relationships. Some peoples with similarly low salaries and similar exposure to stress, discrimination, etc., fare much better than others in terms of their mental and physical health.
One may hypothesize that perseverance of human spirit has a profound role in health outcomes. Those individuals who can “nourish” their spirit, find support, ways to effectively deal with, communicate, reach out, find friends, or simply escape stressful conditions may have better outcomes than those who cannot see or find solution, support, or cannot escape, and then sustain further damage to their spirit. Work of Victor Frankl, a survivor of Nazi concentration camp, revealed that the will to find meaning is the primary motivation in life. Human will, also termed “purpose in life” is associated with favorable health and survival outcomes including protective physiological and cognitive health benefits (15). In fact, logotherapy developed by Frankl (16) is a therapeutic approach focused on the future and on our ability to endure hardship and suffering through a search for purpose.
In adult studies, having purpose in life resulted in 17% less risk for all-cause mortality as well as cardiovascular events, including myocardial infarction, cardiac death, and stroke even after adjustment for sociodemographic, health, and functional status covariates (17).
Sense of purpose has been shown to be a critical factor in human functioning, disability and health. Human spirit could be affected by illness or injury of body or soul. Chronic disease can irreversibly alter purpose of life and human relationships, but human spirit can also affect body response to illness, injury or hardship (18). Higher purpose in life scores in adults predicted better health as measured by biomarkers 10 years later (19). It has been associated with fewer depressive symptoms in elderly (20) and with greater overall life satisfaction (21). The mechanisms underlying those findings include reduced levels of pro-inflammatory cytokines and inflammatory responses to stress (22). Psychological health is an important component of successful aging (23), with children having similar health and aging patterns to those found in their parents (24).
There is a substantial familial component to delayed onset of cardiovascular disease, hypertension, diabetes, and overall lower mortality (25, 26). Recent studies in children linked disorganized parenting and chaotic family life with latter in life cardio-vascular disease (27). We know based on epigenetic experiments that depending on the external experiences one has or does not have; some genes might be, or never be turned on (28). Maternal interpersonal problems are associated with disordered attachment and future relationship issues of the offspring (29). The direct connection of kidney disease with childhood adverse experiences (CAEs) or parental poverty is still lacking.
It is known that both under-nutrition and obesity is associated with childhood HTN, and that both of those conditions are associated with poverty, mental illness, poor relationships (30–33). There is a better mechanistic understanding on how microbiome affects hypertension (34), than how human spirit, social network, or family unit, presence of father and love of mother influence blood pressure regulation or renal outcomes. There are no observational or experimental studies in our field examining those factors.
Purpose in life has been associated with increased likelihood of seeking preventative health measures (35) and avoidance of risk taking behaviors (36).
On the personal and anecdotal level; when we talk to our patients about their complains, their medications, and tell them that most doctors address body and/or mind, and live out spirt, we cannot help but notice their facial and body expressions change, eyes become curious, and the dialog of what is really important to them develops. Patients also frequently thank us after, and say that nobody before talked to them about spirit, or that they “needed it”. Our trainees have a similar reaction.
Studies in pediatric nephrology of how human spirit and spirituality affects day-to-day life of children with chronic kidney disease or hypertension are lacking.
Spirituality, defined as a life oriented toward the spirit has close connection with religion and religious beliefs in kidney disease (37, 38). However, it should be noted that spirituality is distinct from religion understood as institutionally sanctioned beliefs and practices of a defined faith group (39). During evolution, human brain evolved and was able to imagine/meet God and through him/her/them define the individual life purpose, form community and common goals, and bear sacrifices as well as delay gratification. Judaism, the oldest monotheistic religion that has influenced the Christianity, Islam, and in general Western civilization, and addresses the ethical aspects of kidney disease treatment, transplantation, dialysis and end-of life issues (40, 41). Under Jewish written (Torah) and oral (Talmud) laws, with their origin of over 3 thousand years old, a physician is obligated to treat patients, not just to save a life but to restore health as well. According to those ancient laws, physicians have the obligation to prolong life even if a cure is not available, unless patient's suffering outweighs the benefit of life prolongation, and physicians are not allowed to “push away” one life for another (42).
Irrespective of the type of religion, philosophical pastoral care acts as a safeguarding of existence that helps patients to understand life better and to find a viable path in that moment when a person is at a loss (43). That is a way for hope, to find, even to invent, the connections that are so sustainable that it is possible to live in their network and to draw new strength from them, to wish and have confidence, or trust for a particular outcome. As with purposefulness, hope could also have drawbacks and unintended consequences when it becomes “false”, as mirage, and preventative of realistic choices (44).
In adult subjects on dialysis, the existential domain of spirituality had a greater impact on quality of life compared with measures of religiosity (37). However, in the field of pediatric nephrology the role of religion or spirituality or hope has not been well documented.
Spirit measurements
Study and science of the soul/psyche (mind) is scientifically advanced. Soul (mind/psyche) and especially its physical location (brain) can be imaged, probed, stimulated, cut, and examined. Psychiatric disease has its classification and treatment (45). However, the study of the spirit without its physical location is much more difficult to accomplish. Yet, we aim to treat the patient as an individual or as a “whole” person as our field developed a quest for “personalized medicine” (46).
Validated spirituality questionnaires have been used in research for last several decades (47), and purpose of life can be measured in adults using standardized and validated tools (48, 49). Pediatric kidney disease literature focuses on measurements of quality of life (QOL) and does not measure human spirit or spirituality (50). In adults on dialysis, the spirituality measured by validated ESRD Spiritual Beliefs Scale (51) was clinically relevant and had an impact on health related QoL (37).
Although infants do not display characteristics purposeful action toward goals, as it requires learning to identify oneself (52), self-recognition is clearly in place by 12–18 months (53). Young children and adolescent are capable of learning complex abstract and scientific concepts (54, 55). In fact, there are validated scales to measure hope in children based on the premise that children are goal directed and that their goal-related thoughts can be understood according to two components: agency and pathways (56).
As of November 21, 2022 at 11:11AM PubMed search, not limited to English literature, with terms (https://pubmed.ncbi.nlm.nih.gov/?term=spiritual+health%2C+spiritual+well-being+and+children+and+kidney) showed 17 results; Table 1., and review of the subject showed no focus on the spirit/spirituality in children but rather on quality of life, experiences, SDOH, palliative care and religion.
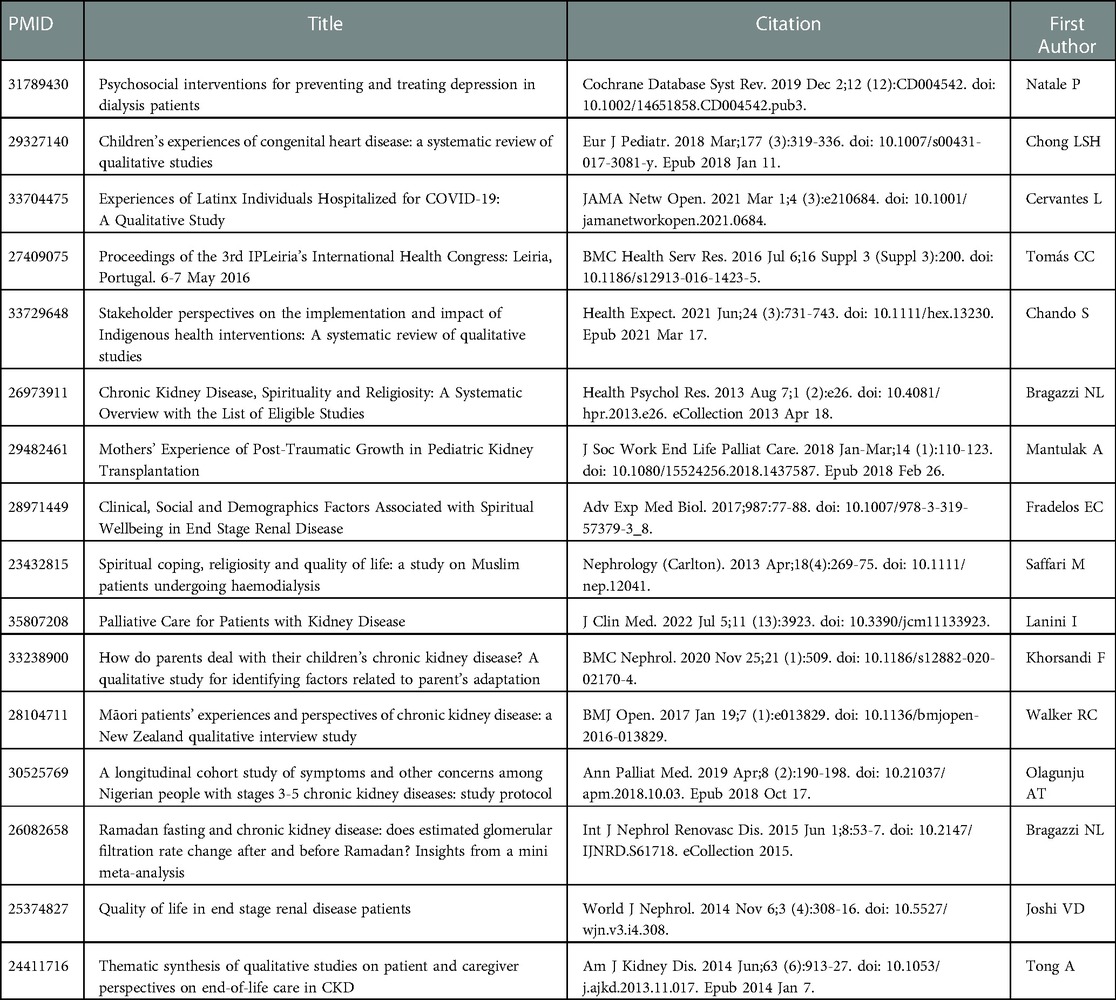
Table 1. November 21, 2022 at 11:11AM pubMed search not limited to English literature with terms (https://pubmed.ncbi.nlm.nih.gov/?term=spiritual+health%2C+spiritual+well-being+and+children+and+kidney).
A recent systematic review of 8,946 articles regarding spirituality and health in adults (57) concluded that the role of spirituality in serious illness and health has not been systematically assessed. This is despite the fact that over 80 medical schools are teaching spirituality and compassionate care in medicine (58).
Conclusions
WHO and JCO recommends addressing human spirit and spirituality in human health and disease Literature on applying this to children with kidney disease is lacking. Although our knowledge has advanced considerably in the field of human body and mind, and social determinants of health, and health equity take top priority in research government programs, human spirit remains under investigated, underappreciated, despite considerable evidence of its role in health outcomes. This mini-review is to raise awareness of the importance of the human spirit and to promote research on human spirit to public in benefit of us all.
Author contributions
RPW contributed to manuscript conceptualization, literature review, writing, editing and finalizing final version. MLM contributed to manuscript conceptualization, literature review, writing, editing and finalizing final version. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Centers for Disease Control and Prevention, National Center for Health Statistics. Mortality 1999–2020 on CDC WONDER Online Database, released in 2021. Available from: http://wonder.cdc.gov/ucd-icd10.html (on Sep 6, 2022 10:12:41 AM).
2. Organization, World Health. World Health Organization (WHO) Definition of Health. (2022). Available from: https://www.publichealth.com.ng/world-health-organizationwho-definition-of-health/
3. Hospital, The Joint Commission Manual: Critical Access. Spiritual Beliefs and Preferences-Evaluating patient’s Spiritual Needs. (2022). Available from: https://www.jointcommission.org/search/#q=spirituality&t=_Tab_All&sort=relevancy
5. Spengler O. The decline of the west. s.l. Arthur H, Helmut W, editor. New York: Oxford university Press (1918).
6. Cambridge, England: Cambridge University Press. dictionary.cambridge.org. (2023). Available from: https://dictionary.cambridge.org/dictionary/italian-english/spirare
7. Kimmerer RW. Braiding sweetgrass: indigenous wisdom, scientific knowledge and the teachings of plants. s.l. Minneapolis: Milkweed Editions (2015).
8. Jones WT. The classical mind: A history of western philosophy. ISBN-10 0155383124. New York City: Harcourt, Brace & World (1969).
9. Jonsen AR. Purposefulness in human life. West J Med. (1976) 125:5–7. PMID: 941450; PMCID: PMC1237170
11. Schopenhauer A. Essay on the freedom of the will. New York: The Liberal Arts Press, Inc (1960) (orginal publication 1841).
13. Einstein A. Einstein on cosmic religion and other opinions and aphorisms. s.l. Mineola, New York: Dover Publication (2009).
14. U.S. Department of Health and Human Services. (2023). Available from: https://health.gov/healthypeople
15. Frankl VE. Man’s search for meaning: an Introduction to logotherapy. s.l. Boston, MA: Beacon Press (1959).
16. Frankl VE. The doctor and the soul: from psychotherapy to logotherapy. s.l. New York City: Random House Digital, Inc (1986).
17. Cohen R, Bavishi C, Rozanski A. Purpose in life and its relationship to all-cause mortality and cardiovascular events: a meta-analysis. Psychosom Med. (2016) 78(2):122–33. doi: 10.1097/PSY.0000000000000274
18. Lee JY, Ready EA, Davis EN, Doyle PC. Purposefulness as a critical factor in functioning, disability and health. Clin Rehabil. (2017) 31(8):1005–18. doi: 10.1177/0269215516672274
19. Zilioli S, Slatcher RB, Ong AD, Gruenewald TL. Purpose in life predicts allostatic load ten years later. J Psychosom Res. (2015) 79(5):451–7. doi: 10.1016/j.jpsychores.2015.09.013
20. Chow EO, Ho HC. The relationship between psychological resources, social resources, and depression: results from older spousal caregivers in Hong Kong. Aging Ment Health. (2012) 16:1016–27. doi: 10.1080/13607863.2012.692769
21. Ardelt M, Edwards CA. Wisdom at the end of life: an analysis of mediating and moderating relations between wisdom and subjective well-being. J Gerontol B Psychol Sci Soc Sci. (2016) 71:502–13. doi: 10.1093/geronb/gbv051
22. Friedman EM, Hayney M, Love GD, Singer BH, Ryff CD. Plasma interleukin-6 and soluble IL-6 receptors are associated with psychological well-being in aging women. Health Psychol. (2007) 26:305–13. doi: 10.1037/0278-6133.26.3.305
23. Phelan EA, Anderson LA, LaCroix AZ, Larson EB. Older adults’ views of “successful aging”—how do they compare with researchers’ definitions? J Am Geriatr Soc. (2004) 52:211–6. doi: 10.1111/j.1532-5415.2004.52056.x
24. Adams ER, Nolan VG, Andersen SL, Perls TT, Terry DF. Centenarian offspring: start healthier and stay healthier. J Am Geriatr Soc. (2008) 56(11):2089–92. doi: 10.1111/j.1532-5415.2008.01949.x
25. Marone S, Bloore K, Sebastiani P, Flynn C, Leonard B, Whitaker K, et al. Purpose in life among centenarian offspring. J Gerontol B Psychol Sci Soc Sci. (2020) 75(2):308–15. doi: 10.1093/geronb/gby023
26. Perls TT, Wilmoth J, Levenson R, Drinkwater M, Cohen M, Bogan H, et al. Life-long sustained mortality advantage of siblings of centenarians. Proc Natl Acad Sci USA. (2002) 99(12):8442–7. doi: 10.1073/pnas.122587599
27. Godoy LC, Frankfurter C, Cooper M, Lay C, Maunder R, Farkouh ME. Association of adverse childhood experiences with cardiovascular disease later in life: A review. JAMA Cardiol. (2021) 6(2):228–35. doi: 10.1001/jamacardio.2020.6050
28. Ghai M, Kader F. A review on epigenetic inheritance of experiences in humans. Biochem Genet. (2022) 60(4):1107–40. doi: 10.1007/s10528-021-10155-7
29. Kerr S, Penner F, Ilagan G, Choi-Kain L, Sharp C. Maternal interpersonal problems and attachment security in adolescent offspring. Borderline Personal Disord Emot Dysregul. (2022) 9:18. doi: 10.1186/s40479-022-00188-8
30. Mphahlele TP, Monyeki KD, Dibakwane WM, Mokgoatšana ST. The relationship between under-nutrition and hypertension among ellisras children and adolescents aged 9 to 17 years. Int J Environ Res Public Health. (2020) 17(23):8926. doi: 10.3390/ijerph17238926
31. Rosner B, Prineas R, Daniels SR, Loggie J. Blood pressure differences between blacks and whites in relation to body size among US children and adolescents. Am J Epidemiol. (2000) 151:1007–19. doi: 10.1093/oxfordjournals.aje.a010129
32. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The relation of overweight to cardiovascular risk factors among children and adolescents: the Bogalusa Heart Study. Pediatrics. (1999) 103:1175–82. doi: 10.1542/peds.103.6.1175
33. Johnson NB, Hayes LD, Brown K, Hoo EC, Ethier KA; Centers for Disease Control and Prevention (CDC). CDC National health report: leading causes of morbidity and mortality and associated behavioral risk and protective factors–United States, 2005-2013. MMWR Surveill Summ. (2014) 63:3–27. PMID: 25356673
34. Avery EG, Bartolomaeus H, Maifeld A, Marko L, Wiig H, Wilck N, et al. The gut microbiome in hypertension, recent advances and future perspectives. Circ Res. (2021) 128(7):934–50. doi: 10.1161/CIRCRESAHA.121.318065
35. Kim ES, Strecher VJ, Ryff CD. Purpose in life and use of preventive health care services. Proc Natl Acad Sci USA. (2014) 111(46):16331–6. doi: 10.1073/pnas.1414826111
36. Konkolÿ Thege B, Bachner YG, Martos T, Kushnir T. Meaning in life: does it play a role in smoking? Substance Use Misuse. (2009) 44(11):1566–77. doi: 10.1080/10826080802495096
37. Davison SN, Jhangri GS. Existential and religious dimensions of spirituality and their relationship with health-related quality of life in chronic kidney disease. Clin J Am Soc Nephrol. (2010) 5(11):1969–76. doi: 10.2215/CJN.01890310
38. Saffari M, Pakpour AH, Naderi MK, Koenig HG, Baldacchino DR, Piper CN. Spiritual coping, religiosity and quality of life: a study on Muslim patients undergoing haemodialysis. Nephrology (Carlton). (2013) 18(4):269–75. doi: 10.1111/nep.12041
39. Koenig HG, McCullough ME, Larson DE. Handbook of religion and health. Oxford: Oxford University Press (2001).
40. Steinberg A. What is it to do good medical ethics? An orthodox Jewish physician and ethicist's perspective. J Med Ethics. (2015) 41(1):125–8. doi: 10.1136/medethics-2014-102296
41. Friedman AN. Medical ethics in nephrology: a Jewish perspective. Rambam Maimonides Med J. (2016) 7(2):e0014. doi: 10.5041/RMMJ.10241
42. Kinzbrunner BM. Jewish Medical ethics and end-of-life care. J Palliat Med. (2004) 7(4):558–73. doi: 10.1089/jpm.2004.7.558
43. Ehrich J, Manemann J, Tasic V, DeSanto NG. The implications of complexity, systems thinking and philosophy for pediatricians. Ital J Pediatr. (2021) 47(1):47–76. doi: 10.1186/s13052-021-01031-6
44. Milona M. Philosophy of hope. In: van den Heuvel SC, editor. Historical and multidisciplinary perspectives on hope. s.l. Cham: Springer (2020). p. 99–116.
45. Association, American Psychiatric. The diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association (2013).
46. Taal MW. Personalized medicine in nephrology a novel approach or just good medicine? Curr Opin Nephrol Hypertens. (2018) 27(6):395–7. doi: 10.1097/MNH.0000000000000448
47. King M, Speck P, Thomas A. The royal free interview for spiritual and religious beliefs: development and validation of a self-report version. Psychol Med. (2001) 31:1015–23. doi: 10.1017/S0033291701004160
48. Smith J, Fisher G, Ryan L, Clarke P, House J, Weir D. Psychosocial and lifestyle questionnaire 2006–2010. Ann Arbor, Michigan: Survey Research Center (2013). Available from: https://hrsonline.isr.umich.edu/sitedocs/userg/HRS2006-2010SAQdoc.pdf
49. Smith J, Ryan L, Fisher G, Sonnega A, Weir D. HRS Psychosocial and lifestyle questionnaire 2006–2016. Ann Arbor, MI: Survey Research Center, Institute for Social Research, University of Michigan (2017).
50. Francis A, Didsbury MS, van Zwieten A, Chen K, James LJ, Kim S, et al. Quality of life of children and adolescents with chronic kidney disease: a cross-sectional study. Arch Dis Child. (2019) 104(2):134–40. doi: 10.1136/archdischild-2018-314934
51. Kimmel PL, Emont SL, Newmann JM, Danko H, Moss AH. ESRD Patient quality of life: symptoms, spiritual beliefs, psychosocial factors, and ethnicity. Am J Kidney Dis. (2003) 42(4):713–21. doi: 10.1016/S0272-6386(03)00907-7
52. Snyder CR. Measuring hope in children. In: Moore KA, Lippman LH, editors. What do children need to flourish? Boston, MA: Springer (2005). p. 37–50.
53. Kaplan L. Oneness and separateness: From infant to individual. s.l. New York City: Simon & Schuster (1978).
54. Nyhout A, Ganea PA. Learning science concepts through prompts to consider alternative possible worlds. J Exp Child Psychol. (2022) 222:105466. doi: 10.1016/j.jecp.2022.105466
55. Goddu MK, Sullivan JN, Walker CM. Toddlers learn and flexibly apply multiple possibilities. Child Dev. (2021) 92(6):2244–51. doi: 10.1111/cdev.13668
56. Snyder CR, Hoza B, Pelham WE, Rapoff J, Ware L, Danovsky M, et al. The development and validation of the children’s hope scale. J Pediatr Psychol. (1997) 22:399–421. doi: 10.1093/jpepsy/22.3.399
57. Balboni TA, VanderWeele TJ, Doan-Soares SD, Long KNG, Ferrell BR, Fitchett G, et al. Spirituality in serious illness and health. JAMA. (2022) 328(2):184–97. doi: 10.1001/jama.2022.11086
Keywords: resilience, spirit, spirituality, social determinants of health, quality of life, religious beliefs, hope
Citation: Woroniecki R and Moritz ML (2023) Investigating the human spirit and spirituality in pediatric patients with kidney disease. Front. Pediatr. 11:1104628. doi: 10.3389/fped.2023.1104628
Received: 21 November 2022; Accepted: 31 January 2023;
Published: 23 February 2023.
Edited by:
Lars Pape, Essen University Hospital, GermanyReviewed by:
Jochen Ehrich, Hannover Medical School, Germany© 2023 Woroniecki and Moritz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert Woroniecki Um9iZXJ0Lndvcm9uaWVja2lAc3Rvbnlicm9va21lZGljaW5lLmVkdQ==
Specialty Section: This article was submitted to Pediatric Nephrology, a section of the journal Frontiers in Pediatrics