 Emilie Raaum Closs
Emilie Raaum Closs Karl Mårild2,3
Karl Mårild2,3 Ketil Størdal
Ketil Størdal- 1Faculty of Medicine, University of Oslo, Oslo, Norway
- 2Department of Pediatrics, Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden
- 3Department of Pediatric Gastroenterology, Queen Silvia Children's hospital, Gothenburg, Sweden
- 4Hans Christian Andersen Children's Hospital, Odense University Hospital, Odense, Denmark
- 5Department of Pediatric Research, University of Oslo, Oslo, Norway
- 6Division of Pediatric and Adolescent Medicine, Oslo University Hospital, Oslo, Norway
Aims: To examine the use of proton pump inhibitors (PPIs) in Scandinavian children with focus on the geographical variation, temporal changes and possible contributing factors to observed changes.
Methods: An observational population-based study of children and adolescents (1-17 years) in Norway, Sweden, and Denmark during the period 2007-2020. Information concerning dispensed PPIs was obtained from the national prescription databases of each country and presented as means per 1,000 children for each country and calendar year in four age categories (1-4, 5-9, 10-13 and 14-17 years).
Results: In 2007, the PPI use in children was similar across Scandinavian countries. An increased PPI use was observed in all countries during the study period, with gradually increasing differences between the countries. In general, Norway showed both the largest total increase and the largest increase in each age category compared to Sweden and Denmark. In 2020 Norwegian children showed, on average, a 59% higher PPI use compared to Swedish children and a more than double the overall dispensation rate than Denmark. In Denmark there was a 19% reduction in dispensed PPIs from 2015 to 2020.
Conclusion: Despite being countries with similar health care systems and without indications of increased incidence of gastroesophageal reflux disease (GERD), we observed considerable geographical variation and temporal changes of PPI use in children. Although this study did not contain data on the indication for PPI use, these large differences across countries and time may indicate a current overtreatment.
Introduction
Gastroesophageal reflux (GER) is defined as “passage of stomach contents into the esophagus with or without accompanied regurgitation and vomiting”.(1) Gastroesophageal reflux disease (GERD) is first established when the reflux is causing troublesome symptoms or leads to medical complications.(1) GER is physiologic, but the transition to GERD is not clearly defined and depends on clinical judgement. The prevalence of GERD in childhood varies between 2%–8%, depending on its definition, study design and age group (2, 3).
Proton pump inhibitors (PPIs) are considered first-line medical treatment for GERD (4). PPIs are a class of medications that selectively inhibit the gastric proton pump in the parietal cell, leading to reduced acid secretion and thereby increasing the pH (5). Prior to the emergence of PPIs, H2-receptor antagonists (H2As) were the main medical treatment for GERD. These drugs lower gastric acidity by competitively inhibiting histamine from binding to H2-receptors on parietal cells (5). Although rapid onset, they are considered overall less effective than PPIs (6, 7).
Over the last decades, there has been a development in both the diagnostic approach to and the use of PPIs to control symptoms of GERD due to several factors discussed later. Among these, changes of the 2009 to 2018 edition of the European and North American Societies of Gastroenterology, Hepatology and Nutrition (NASPGHAN/ESPGHAN) guidelines with a tendency to a more liberal use of time limited PPI trials as a diagnostic tool for children above 1 year, are likely of major importance (8, 9). While generally considered a safe drug, there are increasing concerns that PPI use, in particular long-term treatment, may increase the risk of several adverse effects including changes in the gut microbiome, infections and fractures (10–12).
The aim of this study is to examine the use of PPIs in children and adolescents (aged 1-17 years) in the Scandinavian countries during the period 2007-2020 with focus on the geographical variation and temporal changes in PPI use.
Methods
This is an observational study covering the PPIs dispensed in the Scandinavian countries Norway, Sweden, and Denmark, during the period 2007-2020 and ages 1-17 years. The Anatomical Therapeutic Chemical code (ATC) for PPIs is ATCA02BC and ATCA02BA for H2As. These drugs are available for these age groups by prescription only, and therefore registered in the nation-wide prescription registries. The use of PPIs in infants (<1 year) is in general not recommended by the international guidelines (4, 8), and not approved for use before 1 year in the Scandinavian countries and European Union (13–16). For those reasons, infant PPI use was not examined in this study, but dealt with in another separate study (17).
Prescription data
A formal approval was granted from the national prescription databases of Norway (18), Sweden (19), and Denmark (20) to gain access to relevant aggregated data concerning the use of PPIs among children and adolescents. All registers contain information concerning all prescription drugs sold in each specific country. Information about H2A- use was collected based on publicly available data obtained from the same sources for Norway and Sweden. Corresponding material was not available for Denmark. Although not fully equivalent concerning age groups (0-19 years for H2A), these data were considered useful for comparing temporal trends. In addition, population data was obtained from Statistics Norway (21) because this information was not included in the original data set.
Analysis
All data sets were based on dispensed prescriptions at pharmacies and were calculated as the number of prescriptions per 1,000 children for each country and calendar year. The data for each country concerning PPIs, were then divided into four age categories (1-4, 5-9, 10-13 and 14-17 years) and presented as prescriptions per 1,000 children per year. The use of H2As per 1,000 children per year were also obtained at the start and end of observation (2007 and 2020) and compared with the use of PPIs.
Ethics
Because this study was based on aggregated, anonymous data that could not be linked to any individual, no ethical approval or informed consent was needed (22).
Results
In 2007 (first year of data capture), the use of PPIs was similar in the three countries at around 10-11 dispenses per 1,000 children per year. The use of PPIs increased in all three countries during the period 2007-2020 (Table 1), but there were major differences in the time trend across countries.
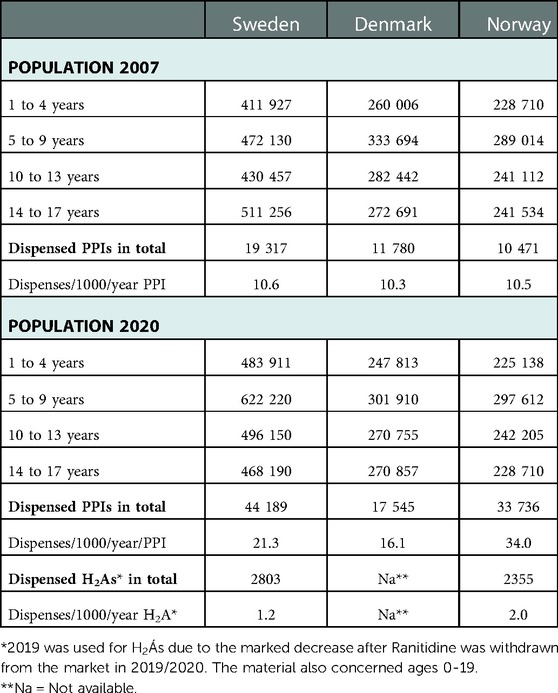
Table 1. Population and dispensed proton pump inhibitors and H2-receptor antagonists for the period 2007-2020 by age and country.
During the study period, Norway had the largest total increase compared to Sweden and Denmark, with dispenses increasing from 10.5 to 34.0/1000/year. In Sweden childhood PPI use increased steadily from 10.6 to 21.3 per 1,000 children/year and in Denmark from 10.3 to 16.1 per 1,000 children/year. In 2020, Norway had a 59% higher overall dispensation rate than Sweden and a more than double the overall dispensation rate than Denmark. As shown in Figures 1A–C, Denmark was the only country where we noted a decrease in childhood PPI use in later years. The use increased until 2015, but from 2015 to 2020, the overall dispensation rate decreased by 19%. In the same period, the total number of dispensations of PPIs continued to increase by 39% in Norway and 18% in Sweden.
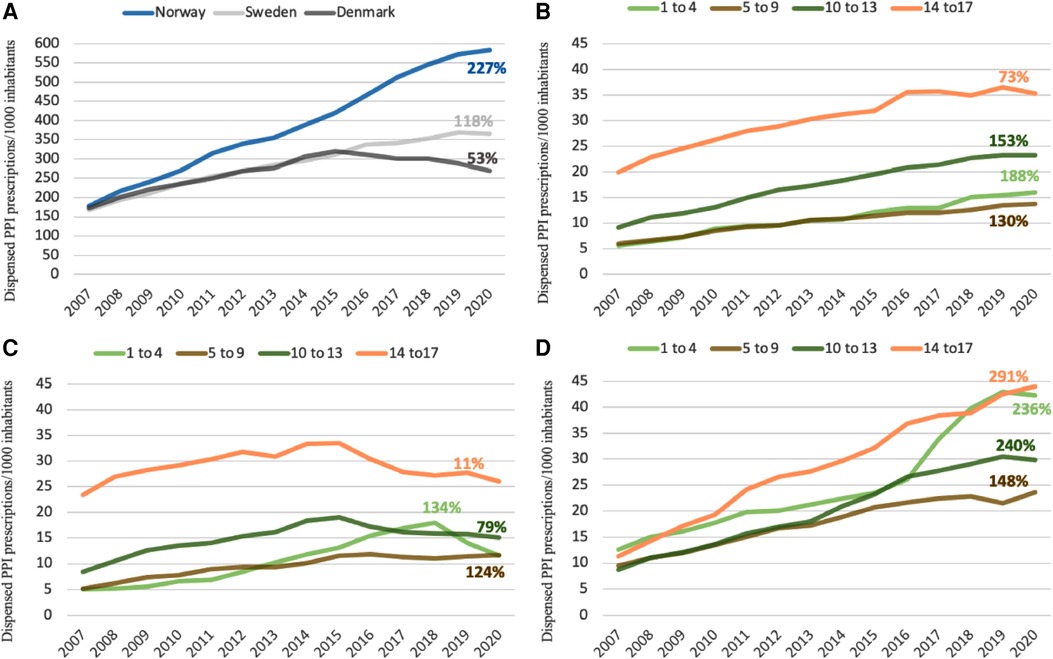
Figure 1. (A–D): temporal changes of PPIs by age and country. Percentages showing the increase in dispensations of PPIs for each age group and each country from 2007 to 2020. A = All countries, B = Sweden, C = Denmark, D = Norway.
For comparison, from 2007 to 2020, the use of H2A decreased from 2.9 to 1.2 dispensations per 1,000 children/year in Sweden and was largely unchanged in Norway (1.8 and 2.0 dispensations per 1,000 children/year, respectively) (Table 1).
Between 2007 and 2015, we noted an even increase in PPI use across all age groups in all three countries (Figures 1B–D). However, since 2015, we noted a considerable decrease in PPI use in Danish adolescents (14-17 years of age) and, in contrast, a marked increased PPI use in Norwegian children aged 1-4 years reaching the same rate as Norwegian children aged 14-17 years (2020: 42 and 44 per 1,000 children, respectively). In Denmark and Sweden, the number of dispensations was highest in the oldest age group during the whole study period.
Discussion
The main findings in this study were a marked increase in the number of dispensations of PPIs in all the Scandinavian countries from 2007 until 2020. However, while childhood PPI use showed a steady increase in Norway and Sweden during this time period, there was a noticeable reduction in Denmark from 2015 until 2020. The most considerable increase was found in Norway.
The causes behind an increase in the number of dispensations of a specific group of pharmaceutical agents such as PPIs is likely multifactorial rather than caused by one single factor. There are no data indicating a rise in GERD in Scandinavian children over the past two decades that could explain our findings. Also, there are to our knowledge no reasons to believe there is a true difference in the prevalence of childhood GERD across Scandinavian countries. Access to the relevant medication and formulations suitable for children is likely of major importance. Since 2014, Norwegian children may be prescribed subsidized PPIs by any physician (rather than by pediatricians only) and without any required specific diagnostic procedures (23). PPIs as a granulate formulation was licensed in 2008, These changes in access might partly explain the particular increased PPI dispensations in the age group of 1-4 years after 2015.
A concomitant reduction in the number of dispensations of H2As was observed in Sweden but not in Norway. The reduction in dispensed H2A was too limited to explain the marked increase in PPI dispenses.
There is increasing evidence of potential adverse effects with particularly long-term PPI use, illustrating the importance of weighing potential benefit against harms when prescribing PPIs to children. Children exposed to PPIs have been reported to have changes in the microbiome and increased risk of gastrointestinal infections including Cl. Difficile (12). Furthermore, an increased risk of allergic diseases and obesity after exposures the first two years of life are of concern (24). Reduced absorption of minerals may also impact on bone health by similar mechanisms as in adults (11). Furthermore, it has been reported that use of PPIs over several weeks increase the risk of rebound hyperacidity. This is thought to be due to a reflective increase in gastrin secretion secondary to the PPI induced hypoacidity (25, 26). Rebound hyperacidity may cause dyspeptic symptoms itself, which may lead to the reinstitution of medication and thereby a vicious cycle that prevents stopping PPI treatment. In addition, hypergastrinemia might be associated with an increased risk of developing gastric neuroendocrine tumors (NET) (27). The clinical relevance of these tumors in young people and the strength of the associations are however controversial.
To the best of our knowledge, our study is the first to examine the use of PPIs for the purpose of comparison across children of several countries over time. A major strength in our study is therefore the opportunity to evaluate similarities, differences, and trends between countries. In Table 2 we summarize studies of PPI use in single countries. These studies indicate increasing use of PPIs over time.
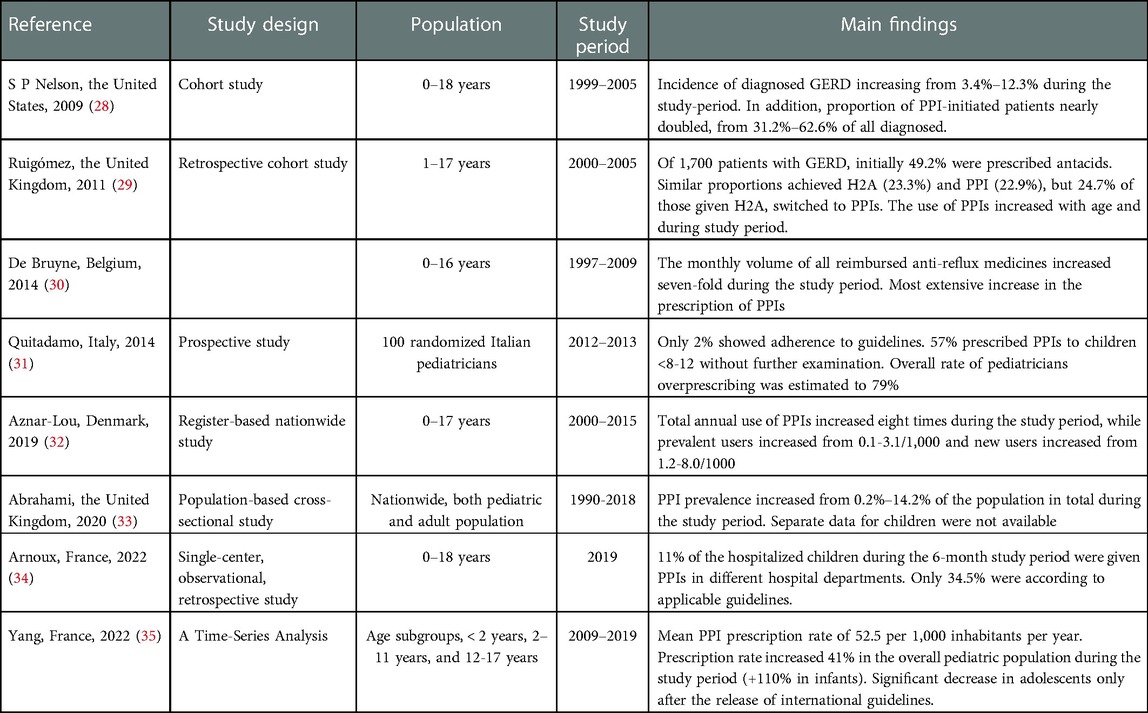
Table 2. Studies concerning the trends in the use of PPIs in children and adolescents.
Another strength is that the data sets are large and comprehensive based on nation-wide population-based registers avoiding any selection bias. Available data from three countries with similar populations and public health care, made it possible to study unexplained variation in prescription practice. The study period 2007-2020 is interesting in itself due to the extensive research concerning the use and possible side effects of PPIs among children and adolescents. In the same period, NASPGHAN/ESPGHAN published the first guidelines for the handling of GERD in children and adolescent in 2009, which were revised 2018 (8, 9). Our study also has limitations.
We lacked data on defined daily doses of PPI. To obtain such information, individual data are required after legal approvals, and would be strengthened by linkage to patient registers for diagnoses and procedure codes. The material does not contain information concerning patient´s adherence to the pharmacological treatment dispensed. As a result, our data gives information concerning the number of dispenses, but not whether the patients take their medicines or not. Although adherence to prescriptions might have changed some during the study period, and maybe across borders, this is not likely to be a main cause of any changes observed in the number of dispenses of PPI. Another limitation to our study is that we are not able to describe whether the size of each prescription has changed, which might have an impact on how we would interpret our results. In addition, the data sets do not distinguish between different PPIs approved for children and adolescents or give any option to distinguish on potential sex differences.
It would also add important information to examine to what extent PPIs are prescribed by non-specialists compared to pediatricians. Without supplementary investigations that are available only in specialized care, it may be difficult to differentiate between GER and GERD. This differentiation may be even more challenging if the examining doctor meets children with suggestive symptoms quite infrequently. Reflux is physiologic in infants and occurs frequently also in older children and adolescents (2). Without any pathognomonic symptoms or gold standard diagnostic tool, it is challenging to strictly differentiate normal physiology from disease. Lack of precise diagnostic criteria is likely to open for large variation in clinical practice and may lead to overdiagnosis and overtreatment. In our study covering Scandinavian countries with similar health care systems, the marked differences in childhood PPIs use over time and geography noted in this study, is likely to be a sign of overtreatment (i.e., unsubstantiated use).
PPIs are also use for other conditions than suspected GERD. Functional dyspepsia is frequent in older children and adolescents. Based upon clinical examination alone, differentiating GERD from functional dyspepsia may be difficult. As a definitive diagnosis may require invasive procedures as gastroscopy, esophageal biopsies and 24 h pH metry with or without impedance, the application of a “treat” instead of “test” strategy may partly explain increasing PPI use in older children. Information regarding diagnostic procedures was not available from our datasets, and beyond the scope of this study.
In typical cases with symptoms like regurgitation, heartburn and pain in the chest or upper abdomen, a preliminary diagnosis is based on history and clinical examination alone. Despite this, neither the 2009 nor the 2018 editions of the NASPGHAN/ESPGHAN guidelines recommend long-term use of PPIs without further examination. Nevertheless, there are some differences important to be aware of. The 2009 guidelines recommended a “time-limited” trial of maximum 4 weeks for older children and adolescents, without any specific age limit downwards. The 2018 guidelines recommend a 4–8-week trial for children and adolescents with typical symptoms, but makes a clearer recommendation against empiric use in infants (8, 9). The 2018 recommendation of a prolonged (from 4 to 4-8 weeks) use of PPIs is parallel to our findings of marked increase in the number of dispensations in the youngest age group over the last years of study.
It is important to acknowledge that untreated GERD will affect children and adolescents in negative ways, both short-term and long-term. Frequent regurgitation, and accompanying symptoms like abdominal pain, heartburn, halitosis, and persistent coughing may reduce the quality of life for those affected. If the reflux is severe and left untreated for a long time, it might result in esophagitis and secondary strictures. A dreaded complication of chronic (>5 years) or frequent (>1 weekly) GERD is the development of Barret´s esophagus, a risk factor for esophageal cancer in late adulthood (36). The balance in clinical practice will always be to avoid missing the diagnosis of GERD and at the same time to avoid unnecessary long term use of PPIs in children without a defined diagnosis.
Conclusion
In Scandinavian children aged 1-17 years PPI use has increased considerably from 2007 to 2020. We observed marked geographical variation and temporal changes of PPI use in children in three neighboring countries with similar health care system and without indications of differences in incidence of gastroesophageal reflux disease (GERD). Although factors such as more use of time-limited PPI trials as a diagnostic tool for children may contribute, the marked differences across countries and time may indicate a current overtreatment.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets were provided by the national prescription databases and are available from the data owners. Requests to access these datasets should be directed to; https://www.reseptregisteret.no, https://www.socialstyrelsen.se/en/statistics-and-data/registers/national-prescribed-drug-register/, https//sundhedsdatastyrelsen.dk/da/registre-og-services/om-de-nationale-sundhedsregistre/sygedomme-laegemidler-og-behandlinger/Laegemiddelstatistikregisteret.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
Closs had primary responsiblity for data analysis and writing the manuscript. Mårild and Nielsen contributed to the writing of the manuscript. Professor Størdal supervised the design and execution of the study, supervised the data analyses and contributed to the writing of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Baird DC, Harker DJ, Karmes AS. Diagnosis and treatment of gastroesophageal reflux in infants and children. Am Fam Physician. (2015) 92(8):705–14. PMID: 26554410
2. Mousa H, Hassan M. Gastroesophageal reflux disease. Pediatr Clin North Am. (2017) 64(3):487–505. doi: 10.1016/j.pcl.2017.01.003
3. Richter JE, Rubenstein JH. Presentation and epidemiology of gastroesophageal reflux disease. Gastroenterology. (2018) 154(2):267–76. doi: 10.1053/j.gastro.2017.07.045
4. Orel R, Benninga MA, Broekaert IJ, Gottrand F, Papadopoulou A, Ribes-Koninckx C, et al. Drugs in focus: proton pump inhibitors. J Pediatr Gastroenterol Nutr. (2021) 72(5):645–53. doi: 10.1097/MPG.0000000000003063
5. Helgadottir H, Bjornsson ES. Problems associated with deprescribing of proton pump inhibitors. Int J Mol Sci. (2019) 20(21):5469. doi: 10.3390/ijms20215469
6. van Pinxteren B, Sigterman KE, Bonis P, Lau J, Numans ME. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev. (2010) (11):Cd002095. doi: 10.1002/14651858.CD002095.pub4
7. Berardi RR. A critical evaluation of proton pump inhibitors in the treatment of gastroesophageal reflux disease. Am J Manag Care. (2000) 6(9 Suppl):S491–505. PMID: 10977489
8. Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the north American society for pediatric gastroenterology, hepatology, and nutrition and the European society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. (2018) 66(3):516–54. doi: 10.1097/MPG.0000000000001889
9. Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the north American society for pediatric gastroenterology, hepatology, and nutrition (NASPGHAN) and the European society for pediatric gastroenterology, hepatology, and nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr. (2009) 49(4):498–547. doi: 10.1097/MPG.0b013e3181b7f563
10. van der Sande L, Jöbsis Q, Bannier M, van de Garde EMW, Coremans JJM, de Vries F, et al. The risk of community-acquired pneumonia in children using gastric acid suppressants. Eur Respir J. (2021) 58(4):2003229. doi: 10.1183/13993003.03229-2020
11. Tavares M, Amil-Dias J. Proton-Pump inhibitors: do children break a leg by using them? J Pediatr Gastroenterol Nutr. (2021) 73(6):665–9. doi: 10.1097/MPG.0000000000003246
12. Levy EI, Hoang DM, Vandenplas Y. The effects of proton pump inhibitors on the microbiome in young children. Acta Paediatr. (2020) 109(8):1531–8. doi: 10.1111/apa.15213
13. https://www.legemiddelsok.no/_layouts/15/Preparatomtaler/Spc/20-13340.pdf Legemiddelsøk Esomeprazol dosegranulat 2021. Available at: https://www.legemiddelsok.no/_layouts/15/Preparatomtaler/Spc/20-13340.pdf
14. https://docetp.mpa.se/LMF/Esomeprazole%20Orifarm%20gastro-resistant%20granules%20for%20oral%20suspension%20in%20sachet%20SmPC_09001bee81882053.pdf Läkemedelsverket esomeprazol dosegranulat 2010.
15. http://produktresume.dk/AppBuilder/search?button=Søg&id=&page=1&q=esomeprazol&type=&utf8=✓ Lægemiddelstyrelsen esomeprazol dosegranulat 2022.
16. https://relis.no/sporsmal_og_svar/4-5693?source=relisdb Proton Pump Inhibotors to Children 2015.
17. Lyamouri M, Mårild K, Nielsen RG, Størdal K. Proton pump inhibitors for infants in three scandinavian countries increased from 2007 to 2020 despite international recommendations. Acta Paediatr. (2022) 11:2222–8. doi: 10.1111/apa.16491
18. Furu K, Wettermark B, Andersen M, Martikainen JE, Almarsdottir AB, Sørensen HT. The nordic countries as a cohort for pharmacoepidemiological research. Basic Clin Pharmacol Toxicol. (2010) 106(2):86–94. doi: 10.1111/j.1742-7843.2009.00494.x
19. Wettermark B, Hammar N, Fored CM, Leimanis A, Otterblad Olausson P, Bergman U, et al. The new Swedish prescribed drug register–opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf. (2007) 16(7):726–35. doi: 10.1002/pds.1294
20. Kildemoes HW, Sørensen HT, Hallas J. The danish national prescription registry. Scand J Public Health. (2011) 39(7 Suppl):38–41. doi: 10.1177/1403494810394717
21. https://www.ssb.no Statistics Norway, SSB2022. Available from: https://www.ssb.no
22. Ludvigsson JF, Håberg SE, Knudsen GP, Lafolie P, Zoega H, Sarkkola C, et al. Ethical aspects of registry-based research in the nordic countries. Clin Epidemiol. (2015) 7:491–508. doi: 10.2147/CLEP.S90589
23. https://tidsskriftet.no/2015/05/nyheter-fra-statens-legemiddelverk/nytt-om-legemidler-0# News about drugs from The Norwegian Medicines Agency2015. Available from: https://tidsskriftet.no/2015/05/nyheter-fra-statens-legemiddelverk/nytt-om-legemidler-0#
24. Mitre E, Susi A, Kropp LE, Schwartz DJ, Gorman GH, Nylund CM. Association between use of acid-suppressive medications and antibiotics during infancy and allergic diseases in early childhood. JAMA Pediatr. (2018) 172(6):e180315. doi: 10.1001/jamapediatrics.2018.0315
25. Waldum HL, Arnestad JS, Brenna E, Eide I, Syversen U, Sandvik AK. Marked increase in gastric acid secretory capacity after omeprazole treatment. Gut. (1996) 39(5):649–53. doi: 10.1136/gut.39.5.649
26. Fossmark R, Johnsen G, Johanessen E, Waldum HL. Rebound acid hypersecretion after long-term inhibition of gastric acid secretion. Aliment Pharmacol Ther. (2005) 21(2):149–54. doi: 10.1111/j.1365-2036.2004.02271.x
27. Fossmark R, Martinsen TC, Waldum HL. Adverse effects of proton pump inhibitors-evidence and plausibility. Int J Mol Sci. (2019) 20(20):5203. doi: 10.3390/ijms20205203
28. Nelson SP, Kothari S, Wu EQ, Beaulieu N, McHale JM, Dabbous OH. Pediatric gastroesophageal reflux disease and acid-related conditions: trends in incidence of diagnosis and acid suppression therapy. J Med Econ. (2009) 12(4):348–55. doi: 10.3111/13696990903378680
29. Ruigómez A, Hungin AP, Lundborg P, Johansson S, Wallander MA, García Rodríguez LA. Treatment patterns in paediatric patients with a new diagnosis of gastroesophageal reflux disease. Eur J Gastroenterol Hepatol. (2011) 23(3):232–7. doi: 10.1097/MEG.0b013e328343b06e
30. De Bruyne P, Christiaens T, Vander Stichele R, Van Winckel M. Changes in prescription patterns of acid-suppressant medications by Belgian pediatricians: analysis of the national database, [1997-2009]. J Pediatr Gastroenterol Nutr. (2014) 58(2):220–5. doi: 10.1097/MPG.0b013e3182a3b04e
31. Quitadamo P, Miele E, Alongi A, Brunese FP, Di Cosimo ME, Ferrara D, et al. Italian Survey on general pediatricians’ approach to children with gastroesophageal reflux symptoms. Eur J Pediatr. (2015) 174(1):91–6. doi: 10.1007/s00431-014-2369-4
32. Aznar-Lou I, Reilev M, Lødrup AB, Rubio-Valera M, Haastrup PF, Pottegård A. Use of proton pump inhibitors among danish children: a 16-year register-based nationwide study. Basic Clin Pharmacol Toxicol. (2019) 124(6):704–10. doi: 10.1111/bcpt.13191
33. Abrahami D, McDonald EG, Schnitzer M, Azoulay L. Trends in acid suppressant drug prescriptions in primary care in the UK: a population-based cross-sectional study. BMJ Open. (2020) 10(12):e041529. doi: 10.1136/bmjopen-2020-041529
34. Arnoux A, Bailhache M, Tetard C, Rebouissoux L, Clouzeau H, Lamireau T, et al. Proton pump inhibitors are still overprescribed for hospitalized children. Arch Pediatr. (2022) 29(4):258–62. doi: 10.1016/j.arcped.2022.02.004
35. Yang S, Trinh NTH, Chalumeau M, Kaguelidou F, Ruemmele FM, Milic D, et al. Pediatric prescriptions of proton pump inhibitors in France (2009-2019): a time-series analysis of trends and practice guidelines impact. J Pediatr. (2022) 245:158–64.e4. doi: 10.1016/j.jpeds.2022.01.041
Keywords: gastroesophageal reflux disease, children, PPI, overtreatment, temporal changes, adolescents
Citation: Closs ER, Mårild K, Nielsen RG and Størdal K (2023) Use of proton pump inhibitors in scandinavian children and adolescents: An observational study. Front. Pediatr. 11:1052978. doi: 10.3389/fped.2023.1052978
Received: 24 September 2022; Accepted: 20 January 2023;
Published: 16 February 2023.
Edited by:
Ron Shaoul, Rambam Health Care Campus, IsraelReviewed by:
Helge Waldum, Norwegian University of Science and Technology, NorwayJanet Sultana, Mater Dei Hospital, Malta
Reidar Fossmark, Norwegian University of Science and Technology, Norway
© 2023 Closs, Mårild, Nielsen and Størdal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ketil Størdal a2V0aWwuc3RvcmRhbEBtZWRpc2luLnVpby5ubw==
†ORCID Ketil Størdal orcid.org/0000-0002-2620-7646
Specialty Section: This article was submitted to Pediatric Gastroenterology, Hepatology and Nutrition, a section of the journal Frontiers in Pediatrics