 Jeongho Han
Jeongho Han Joowon Lee
Joowon Lee Sujin Choi
Sujin Choi Hyunju Lee
Hyunju Lee Young Hwan Song2
Young Hwan Song2

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr. , 21 November 2022
Sec. Pediatric Cardiology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.995167
This article is part of the Research Topic Case Reports in Pediatric Cardiology: 2022 View all 31 articles
Children with underlying medical conditions potentially develop severe illness from Coronavirus disease 2019 (COVID-19). The use of vaccines against COVID-19 is currently recommended for the pediatric population. The COVID-19 vaccine has a temporal association with the occurrence of myocarditis. Although most patients with COVID-19 vaccination-associated myocarditis (C-VAM) exhibit a mild clinical course and rapid recovery, C-VAM potentially causes electrical instability and sudden cardiac death. Herein, we report the case of a 17-year-old woman who presented with chest pain and syncope following the first dose of the messenger RNA COVID-19 vaccine. The patient's heart function was impaired, and nonsustained ventricular tachycardia was frequent. Cardiac magnetic resonance (CMR) imaging satisfied the criteria for myocarditis. Despite the administration of immunomodulatory drugs, the patient's heart function was not fully restored, and the concentration of cardiac enzymes remained above the normal range. Persistence of late gadolinium enhancement was observed on short-term follow-up CMR imaging. Although most patients with C-VAM exhibit mild symptoms, significant cardiac arrhythmias potentially occur. Furthermore, some patients with C-VAM demonstrate prolonged impaired heart function and sustained late gadolinium enhancement on follow-up CMR imaging. Therefore, monitoring of electrical and functional cardiac abnormalities in patients with C-VAM is crucial and the long-term outcomes and prognosis of patients with C-VAM require further investigation.
Coronavirus disease 2019 (COVID-19) is a worldwide health problem, as it has reached pandemic level and caused multiple outbreaks globally. Although COVID-19 infection in children is typically asymptomatic or mild, it potentially progresses to severe illness in children with underlying medical conditions (1). Multisystem inflammatory syndrome in children, which is associated with high morbidity and mortality, can develop after COVID-19 infection (2). The use of vaccines against COVID-19 has increased among children and adolescents. Both the Pfizer-BioNTech BNT162b2 and Moderna mRNA-1273 vaccines have exhibited excellent efficacy and safety in the pediatric population (3, 4). The Centers for Disease Control and Prevention (CDC) recommended the use of the vaccine for adolescents aged ≥12 years on May 12, 2021, and for children aged 5–11 years on November 2, 2021 (5). The Korea Advisory Committee on Immunization Practices also recommended extending the use of the vaccine to persons aged ≥12 years on August 25, 2021.
Myocarditis and pericarditis are complications that potentially occur after COVID-19 vaccination (6–16). In most cases of COVID-19 vaccination-associated myocarditis (C-VAM) after BNT162b2 or mRNA-1273 vaccination, symptoms developed within a few days after the second vaccine dose, and the clinical course usually appeared mild with resolution of symptoms and signs within 1 week. However, fulminant myocarditis and sudden death after vaccination have also been reported (17, 18).
Herein, we describe the case of a 17-year-old woman with myocarditis after the first dose of the BNT162b2 vaccine. This patient, who presented with syncope and experienced several episodes of polymorphic nonsustained ventricular tachycardia, exhibited a chronic clinical course, which is an uncommon finding in other patients with C-VAM.
A previously healthy 17-year-old woman presented with syncope 7 days after her first BNT162b vaccine dose. The patient was obese, with a body mass index of 26.6 kg/m2 (above the 95 percentile for their age and sex). Two days after the vaccination, the patient started experiencing generalized malaise, headache, chest pain, and dyspnea on exertion. Three days later, the patient experienced palpitations, and the intensity of her chest pain increased. The patient visited the emergency department of our hospital. The patient's electrocardiogram exhibited low voltage in the limb leads, and her troponin I concentration was within the normal range (0.032 ng/ml; normal: 0–0.045 ng/ml). The patient's symptoms were improved slightly, resulting in her subsequent discharge. The next day, the patient lost consciousness for several minutes while sitting in a restaurant.
The patient's vital signs on arrival were as follows: blood pressure, 102/60 mmHg; heart rate, 92 beats/min; respiratory rate, 19 breaths/min; temperature, 37.7 °C; and oxygen saturation, 100%. Physical examination revealed no remarkable findings. Neither audible murmurs nor signs of congestion were observed. Laboratory blood tests revealed myocardial injury without systemic inflammation. The level of high-sensitivity cardiac troponin I was 0.072 ng/ml (normal: 0–0.045 ng/ml). The patient's white blood cell count was elevated (10,960/uL; normal: 4,000–10,000/ul), and eosinophilia was absent. The C-reactive protein concentration (<0.40 mg/dl; normal: 0–0.5 mg/dl) and erythrocyte sedimentation rate (17 mm/h; normal: 0–20 mm/h) were not elevated. The patient's nasopharyngeal polymerase chain reaction (PCR) test result was negative for COVID-19. PCR tests for other viruses using nasopharyngeal swabs, blood, and stool samples were negative. Although serum neutralizing antibody titers against adenovirus types 2 and 5 were 1:180 and 1:256, respectively, nasopharyngeal PCR tests were negative for adenovirus.
Electrocardiography revealed low voltage in the limb leads and premature ventricular contraction (Figure 1). There was no abnormal finding on the chest radiograph. Transthoracic echocardiography revealed left ventricular dilatation with a reduced ejection fraction of 45.1% (biplane Simpson's method). Ambulatory Holter monitoring exhibited repeated episodes of nonsustained polymorphic ventricular tachycardia. Cardiac magnetic resonance (CMR) imaging 2 days after presentation revealed global left ventricular dysfunction with an ejection fraction of 41%, marked hypokinesia, high T2 values in the apical to mid portion of the anterior wall, and diffuse multifocal patchy late gadolinium enhancement (LGE) (Figure 2).
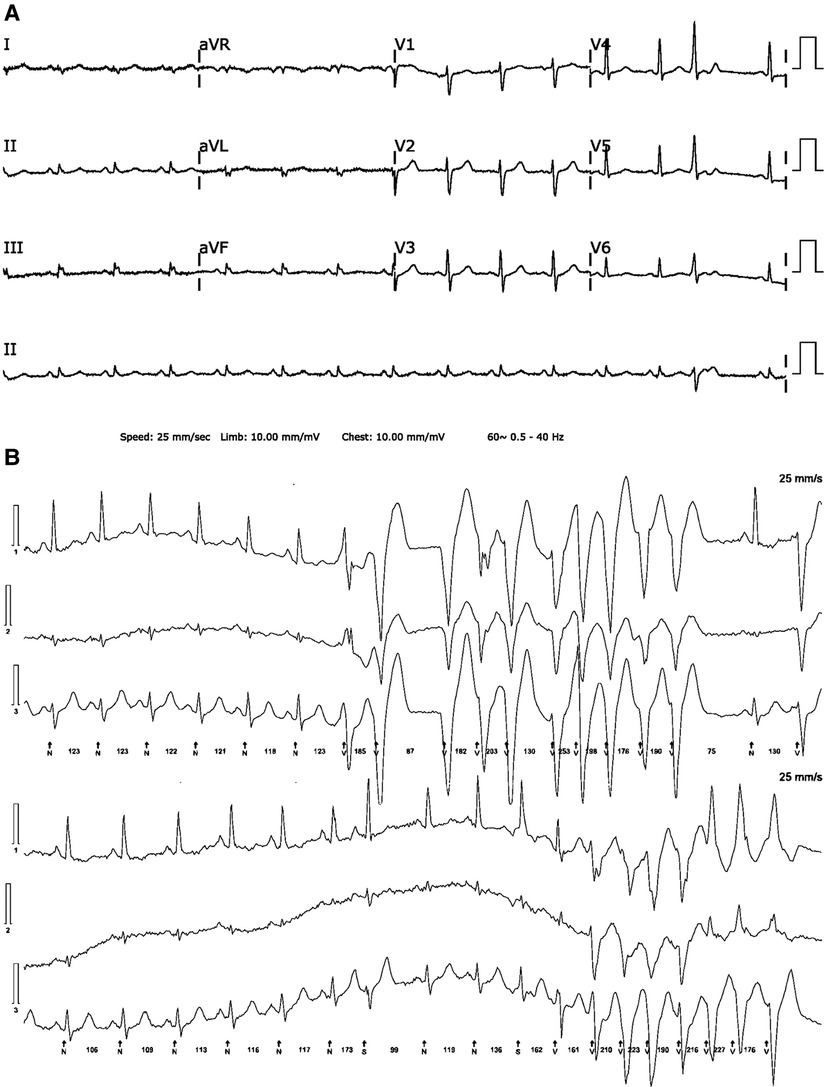
Figure 1. (A) A 12-lead electrocardiogram reveals low QRS voltage in limb leads and isolated ventricular premature beat. (B) Ambulatory 24-hour Holter monitoring reveals several runs of nonsustained polymorphic ventricular tachycardia.
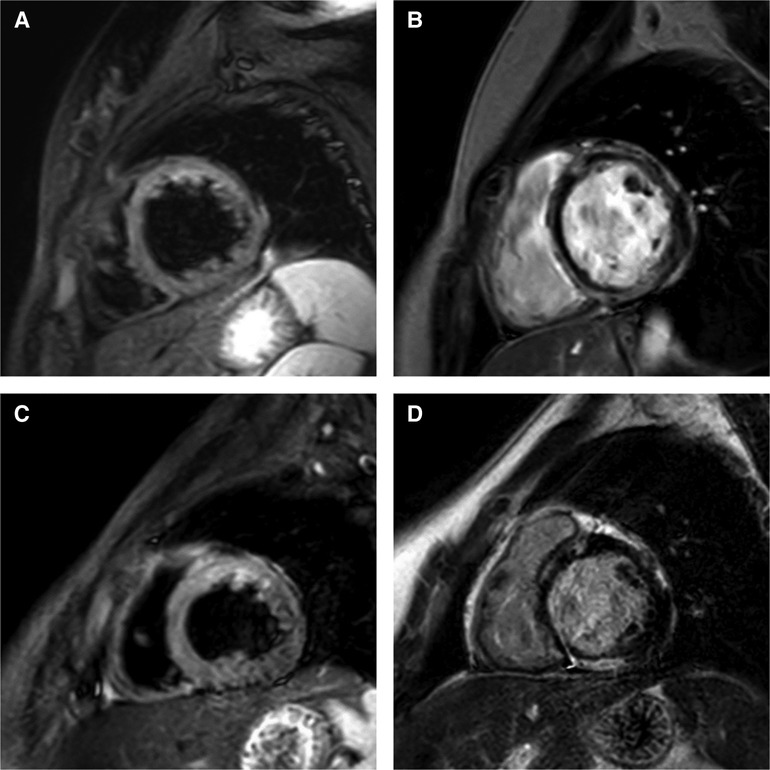
Figure 2. Short-axis cardiac magnetic resonance imaging on days 2 (A,B) and 18 (C,D) after the patient's presentation. (A) High signal intensity in anterior wall of left ventricle on T2-weighted image. (B) Diffuse multifocal patchy late gadolinium enhancement (LGE). (C) Sustained high signal intensity in anterior wall of left ventricle on T2-weighted image. (D) Persistent multifocal patchy LGE.
The patient was admitted to the intensive care unit for the monitoring of hemodynamic and electrical instability and treated with 1 g/kg of intravenous immunoglobulin for two consecutive days as well as 2 mg/kg/day of intravenous methylprednisolone. Ibuprofen use was discontinued after severe myocardial inflammation was identified using CMR imaging. The patient was administered intravenous milrinone and furosemide for a brief period in consideration of the possibility of progressive deterioration of hemodynamic status. Therapy with an angiotensin-converting enzyme inhibitor and beta blocker was initiated after discontinuation of intravenous milrinone.
The troponin I concentration peaked 2 days after presentation (0.689 ng/ml); subsequently, it gradually declined and reached its nadir 9 days after presentation (0.153 ng/ml). Thereafter, it resumed its rising trend, and the patient was administered 1 g/kg of pulsed methylprednisolone therapy for three consecutive days, followed by a planned oral prednisolone taper. CMR imaging 18 days after presentation continued to demonstrate high T2 values in the apical to mid portion of the anterior wall and a slightly decreased extent of diffuse multifocal patchy LGE. A right ventricular endomyocardial biopsy was performed to exclude other etiologies of myocarditis, including giant cell myocarditis. Histological examination of the biopsy specimen revealed focal myocardial degeneration and interstitial edema without significant inflammatory cell infiltration. The patient was discharged 31 days after presentation due to the reduced burden of ventricular tachycardia, improved symptoms, and partial recovery of ventricular function.
Nine days later, the patient was re-hospitalized for Campylobacter colitis and treated with intravenous antibiotics, a stress dose of intravenous hydrocortisone, and an intravenous vasopressor during hospitalization. On follow-up 1 month later, a repeat echocardiography revealed left ventricular dilatation with a reduced ejection fraction of 49.1% (biplane Simpson's method), and the troponin I concentration remained above the normal range (0.137 ng/ml). Follow-up CMR imaging was scheduled two months after hospital discharge (Table 1).
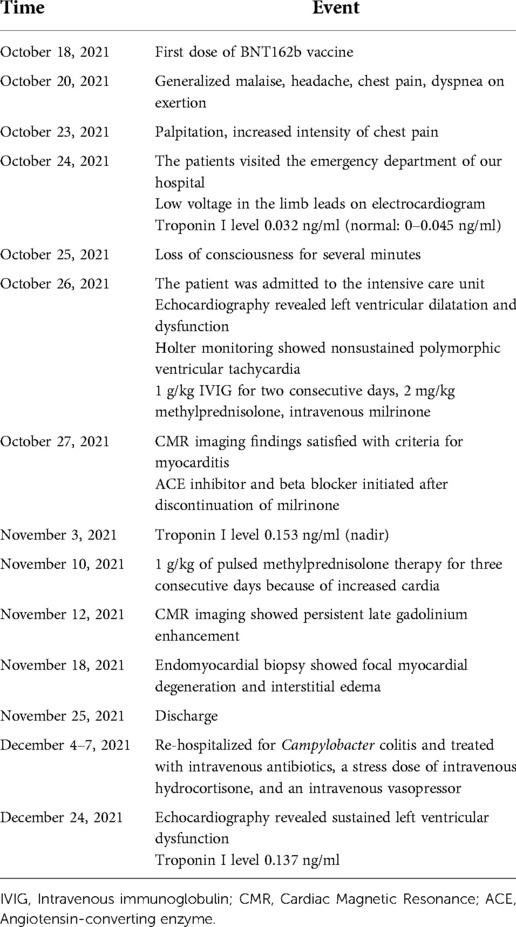
Table 1. Timeline of case.
The patient in this report, who developed myocarditis after the first BNT162b vaccine dose, presented with syncope. Since her ventricular function was impaired, and nonsustained ventricular tachycardia was frequent, the patient required electrical and hemodynamic monitoring in the intensive care unit. The patient's cardiac function did not fully recover, with the persistence of elevated cardiac enzymes and residual LGE on CMR imaging.
A large proportion of patients with myocarditis have experienced cardiac arrhythmia at any stage of the disease. The most serious types of arrhythmias have been ventricular tachycardia and ventricular fibrillation. Ventricular arrhythmia has been associated with poor patient outcomes, including the use of mechanical circulatory support and death (19, 20). This arrhythmia potentially manifests as cardiopulmonary arrest and sudden cardiac death. Therefore, current guidelines recommend mandatory close monitoring of cardiovascular status (including heart rhythm) in the early phase in the management of patients with myocarditis (21, 22). Although no deaths have been attributed to arrhythmia in patients with C-VAM, some patients had nonsustained ventricular tachycardia (Table 2) (7–9, 15, 16). Moreover, a case of sudden cardiac death due to C-VAM have been reported (18). Therefore, electrical monitoring is crucial in the management of pediatric patients with C-VAM.
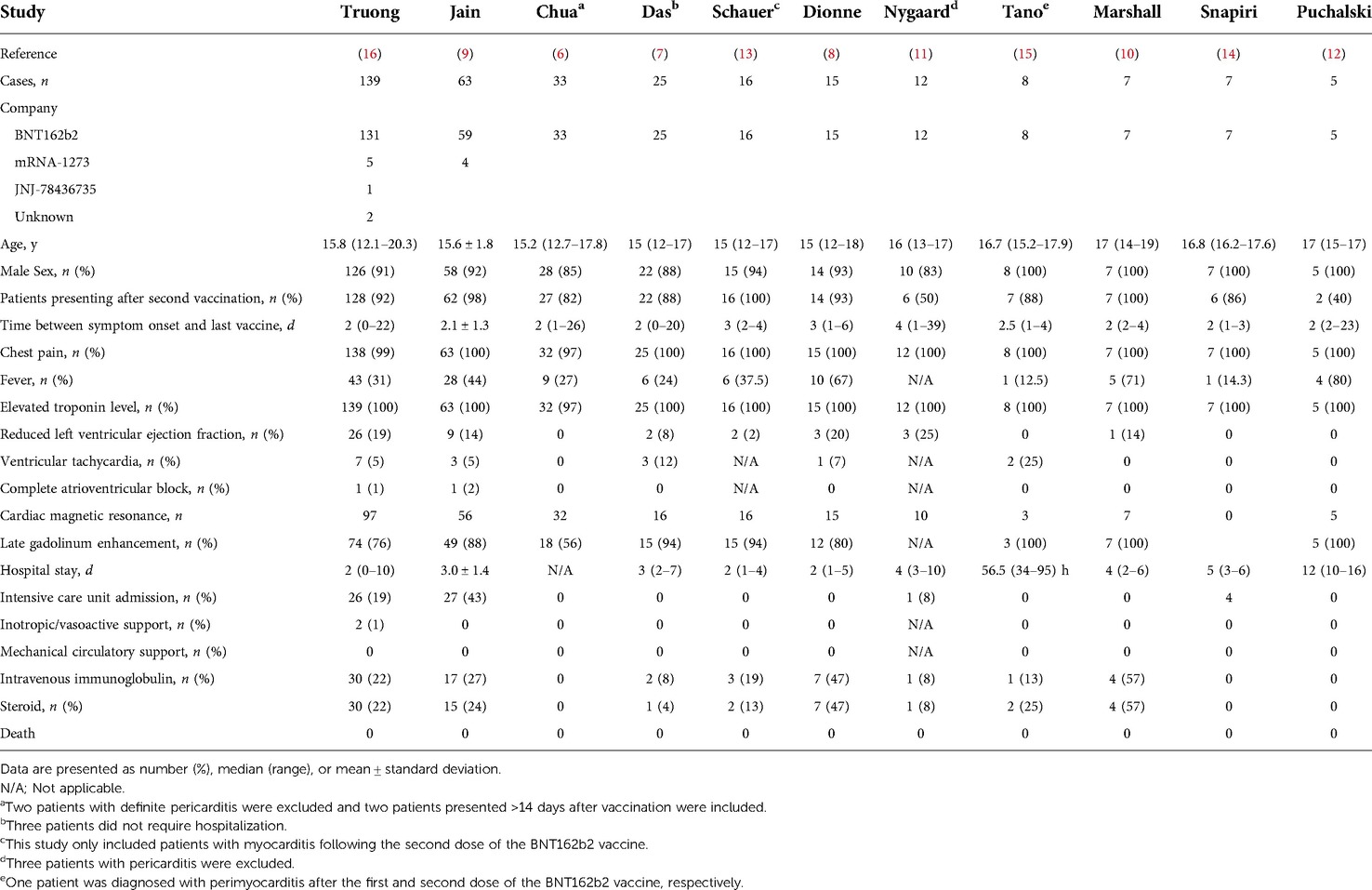
Table 2. Case series and retrospective studies of coronavirus disease 2019 vaccination-associated myocarditis and myopericarditis in children.
Although endomyocardial biopsy (EMB) is the gold standard for the diagnosis of myocarditis, CMR imaging is currently adopted for the confirmation of myocarditis (21). The CMR imaging findings of the patient in this report satisfied the updated Lake Louise criteria, and the patient's condition was consistent with the CDC's definition of confirmed myocarditis. However, the EMB results did not reveal significant inflammatory cell infiltration. These findings possibly resulted from sampling errors associated with the focal distribution of inflammatory infiltrates. The sites of inflammatory infiltrates were sometimes inaccessible to the bioptomes. The false negative rates of EMB were 45% for the left ventricle and 37% for the right ventricle in 38 autopsied hearts with lymphocytic myocarditis (23). The sampling error also occurred due to difference between biopsy sites and involved regions on CMR imaging (24). The biopsy site was usually the right ventricle, while CMR imaging demonstrated predominant left ventricular involvement.
A few case reports and case series showed the histopathologic findings in C-VAM (18, 25–30). The marked inflammatory infiltrates with a predominance of T-cells and macrophages, occasionally admixed with eosinophils, B cells, and plasma cells, and multifocal cardiomyocyte damages were demonstrated in patients with C-VAM (27–30). The autopsied heart with sudden death after COVID-19 vaccination revealed diffuse inflammatory infiltrates predominantly composed of macrophages and neutrophils and the existence of contraction band necrosis (18, 26). However, similar to the findings of the patient in this report, the results of endomyocardial biopsy in patients with C-VAM occasionally demonstrated no inflammatory infiltrates or findings incompatible with classic histopathologic criteria of myocarditis (25, 30–32).
The heart function of the patient in this report was persistently impaired, and LGE was sustained on short-term follow-up CMR imaging. LGE was an independent predictor of mortality and major adverse cardiac events in adult patients with myocarditis (33, 34). The midwall septal pattern of LGE has been associated with late progressive deterioration of left ventricular function (35). Recent studies investigating changes in CMR imaging findings in patients with C-VAM have demonstrated sustained and decreased LGE on follow-up CMR imaging (13, 36, 37). Persistent LGE was observed in a considerable proportion of adult and pediatric patients with myocarditis on follow-up CMR imaging at 3–6 months, even after normalization of inflammatory and cardiac markers (38, 39). Although LGE without edema at 6-month follow-up CMR imaging was associated with a worse outcome in adult patients with acute myocarditis, the clinical significance of LGE and longitudinal changes in heart function in C-VAM require further investigation (40).
We described an adolescent woman with myocarditis after BNT162b2 mRNA vaccination, who exhibited frequent episodes of nonsustained ventricular tachycardia and persistent left ventricular dysfunction with sustained LGE. Monitoring the electrical and functional cardiac abnormalities in patients with C-VAM is crucial. Further studies focusing on the long-term outcomes and prognosis of patients with C-VAM are warranted.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
This report was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-2205-757-701). The requirement for informed consent was waived.
JL and YS contributed to the formation of the research idea. JH and JL collected data and wrote the original draft. JH, JL, SC, HL, and YS participated in patient care, and contributed to manuscript review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CMR, Cardiac magnetic resonance; CDC, Centers for Disease Control and Prevention; COVID-19, Coronavirus disease 2019; C-VAM, COVID-19 vaccination-associated myocarditis; EMB, Endomyocardial biopsy; LGE, Late gadolinium enhancement; PCR, Polymerase chain reaction
1. Preston LE, Chevinsky JR, Kompaniyets L, Lavery AM, Kimball A, Boehmer TK, et al. Characteristics and disease severity of US children and adolescents diagnosed with COVID-19. JAMA Netw Open. (2021) 4(4):e215298. doi: 10.1001/jamanetworkopen.2021.5298
2. Son MBF, Murray N, Friedman K, Young CC, Newhams MM, Feldstein LR, et al. Multisystem inflammatory syndrome in children—initial therapy and outcomes. N Engl J Med. (2021) 385(1):23–34. doi: 10.1056/NEJMoa2102605
3. Creech CB, Anderson E, Berthaud V, Yildirim I, Atz AM, Melendez Baez I, et al. Evaluation of mRNA-1273 COVID-19 vaccine in children 6 to 11 years of age. N Engl J Med. (2022) 386(21):2011–23. doi: 10.1056/NEJMoa2203315
4. Walter EB, Talaat KR, Sabharwal C, Gurtman A, Lockhart S, Paulsen GC, et al. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N Engl J Med. (2022) 386(1):35–46. doi: 10.1056/NEJMoa2116298
5. Woodworth KR, Moulia D, Collins JP, Hadler SC, Jones JM, Reddy SC, et al. The advisory committee on immunization practices’ interim recommendation for use of pfizer-BioNTech COVID-19 vaccine in children aged 5–11 years—United States, november 2021. MMWR Morb Mortal Wkly Rep. (2021) 70(45):1579–83. doi: 10.15585/mmwr.mm7045e1
6. Chua GT, Kwan MYW, Chui CSL, Smith RD, Cheung EC, Tian T, et al. Epidemiology of acute myocarditis/pericarditis in Hong Kong adolescents following comirnaty vaccination. Clin Infect Dis. (2022) 75(4):673–81. doi: 10.1093/cid/ciab989
7. Das BB, Kohli U, Ramachandran P, Nguyen HH, Greil G, Hussain T, et al. Myopericarditis after messenger RNA coronavirus disease 2019 vaccination in adolescents 12 to 18 years of age. J Pediatr. (2021) 238:26–32.e1. doi: 10.1016/j.jpeds.2021.07.044
8. Dionne A, Sperotto F, Chamberlain S, Baker AL, Powell AJ, Prakash A, et al. Association of myocarditis with BNT162b2 messenger RNA COVID-19 vaccine in a case series of children. JAMA Cardiol. (2021) 6(12):1446–50. doi: 10.1001/jamacardio.2021.3471
9. Jain SS, Steele JM, Fonseca B, Huang S, Shah S, Maskatia SA, et al. COVID-19 vaccination-associated myocarditis in adolescents. Pediatrics. (2021) 148(5):e2021053427. doi: 10.1542/peds.2021-053427
10. Marshall M, Ferguson ID, Lewis P, Jaggi P, Gagliardo C, Collins JS, et al. Symptomatic acute myocarditis in 7 adolescents after pfizer-BioNTech COVID-19 vaccination. Pediatrics. (2021) 148(3):e2021052478. doi: 10.1542/peds.2021-052478
11. Nygaard U, Holm M, Bohnstedt C, Chai Q, Schmidt LS, Hartling UB, et al. Population-based incidence of myopericarditis after COVID-19 vaccination in danish adolescents. Pediatr Infect Dis J. (2022) 41(1):e25–e8. doi: 10.1097/INF.0000000000003389
12. Puchalski M, Kaminska H, Bartoszek M, Brzewski M, Werner B. COVID-19-vaccination-induced myocarditis in teenagers: case series with further follow-up. Int J Environ Res Public Health. (2022) 19(6):3456. doi: 10.3390/ijerph19063456
13. Schauer J, Buddhe S, Gulhane A, Sagiv E, Studer M, Colyer J, et al. Persistent cardiac magnetic resonance imaging findings in a cohort of adolescents with post-coronavirus disease 2019 mRNA vaccine myopericarditis. J Pediatr. (2022) 245:233–7. doi: 10.1016/j.jpeds.2022.03.032
14. Snapiri O, Rosenberg Danziger C, Shirman N, Weissbach A, Lowenthal A, Ayalon I, et al. Transient cardiac injury in adolescents receiving the BNT162b2 mRNA COVID-19 vaccine. Pediatr Infect Dis J. (2021) 40(10):e360–e3. doi: 10.1097/INF.0000000000003235
15. Tano E, San Martin S, Girgis S, Martinez-Fernandez Y, Sanchez Vegas C. Perimyocarditis in adolescents after pfizer-BioNTech COVID-19 vaccine. J Pediatric Infect Dis Soc. (2021) 10(10):962–6. doi: 10.1093/jpids/piab060
16. Truong DT, Dionne A, Muniz JC, McHugh KE, Portman MA, Lambert LM, et al. Clinically suspected myocarditis temporally related to COVID-19 vaccination in adolescents and young adults: suspected myocarditis after COVID-19 vaccination. Circulation. (2022) 145(5):345–56. doi: 10.1161/CIRCULATIONAHA.121.056583
17. Abbate A, Gavin J, Madanchi N, Kim C, Shah PR, Klein K, et al. Fulminant myocarditis and systemic hyperinflammation temporally associated with BNT162b2 mRNA COVID-19 vaccination in two patients. Int J Cardiol. (2021) 340:119–21. doi: 10.1016/j.ijcard.2021.08.018
18. Choi S, Lee S, Seo JW, Kim MJ, Jeon YH, Park JH, et al. Myocarditis-induced sudden death after BNT162b2 mRNA COVID-19 vaccination in Korea: case report focusing on histopathological findings. J Korean Med Sci. (2021) 36(40):e286. doi: 10.3346/jkms.2021.36.e286
19. Miyake CY, Teele SA, Chen L, Motonaga KS, Dubin AM, Balasubramanian S, et al. In-hospital arrhythmia development and outcomes in pediatric patients with acute myocarditis. Am J Cardiol. (2014) 113(3):535–40. doi: 10.1016/j.amjcard.2013.10.021
20. Othman HF, Byrnes J, Elsamny E, Hamzah M. Impact of ventricular arrhythmias on outcomes in children with myocarditis. Eur J Pediatr. (2020) 179(11):1779–86. doi: 10.1007/s00431-020-03687-4
21. Law YM, Lal AK, Chen S, Cihakova D, Cooper LT Jr., Deshpande S, et al. Diagnosis and management of myocarditis in children: a scientific statement from the American heart association. Circulation. (2021) 144(6):e123–e35. doi: 10.1161/CIR.0000000000001001
22. Kociol RD, Cooper LT, Fang JC, Moslehi JJ, Pang PS, Sabe MA, et al. Recognition and initial management of fulminant myocarditis: a scientific statement from the American heart association. Circulation. (2020) 141(6):e69–92. doi: 10.1161/CIR.0000000000000745
23. Hauck AJ, Kearney DL, Edwards WD. Evaluation of postmortem endomyocardial biopsy specimens from 38 patients with lymphocytic myocarditis: implications for role of sampling error. Mayo Clin Proc. (1989) 64(10):1235–45. doi: 10.1016/S0025-6196(12)61286-5
24. Chow LH, Radio SJ, Sears TD, McManus BM. Insensitivity of right ventricular endomyocardial biopsy in the diagnosis of myocarditis. J Am Coll Cardiol. (1989) 14(4):915–20. doi: 10.1016/0735-1097(89)90465-8
25. Amemiya K, Kobayashi T, Kataoka Y, Iwai T, Nakagawa S, Morita Y, et al. Myocarditis after COVID-19 mRNA vaccination in three young adult males: significance of biopsy in vaccine-associated myocarditis. Pathol Int. (2022) 72(7):385–7. doi: 10.1111/pin.13234
26. Gill JR, Tashjian R, Duncanson E. Autopsy histopathologic cardiac findings in 2 adolescents following the second COVID-19 vaccine dose. Arch Pathol Lab Med. (2022) 146(8):925–9. doi: 10.5858/arpa.2021-0435-SA
27. Kazama S, Okumura T, Kimura Y, Ito R, Araki T, Mizutani T, et al. Biopsy-proven fulminant myocarditis requiring mechanical circulatory support following COVID-19 mRNA vaccination. CJC Open. (2022) 4(5):501–5. doi: 10.1016/j.cjco.2022.02.004
28. Lim Y, Kim MC, Kim KH, Jeong IS, Cho YS, Choi YD, et al. Case report: acute fulminant myocarditis and cardiogenic shock after messenger RNA coronavirus disease 2019 vaccination requiring extracorporeal cardiopulmonary resuscitation. Front Cardiovasc Med. (2021) 8:758996. doi: 10.3389/fcvm.2021.758996
29. Verma AK, Lavine KJ, Lin CY. Myocarditis after COVID-19 mRNA vaccination. N Engl J Med. (2021) 385(14):1332–4. doi: 10.1056/NEJMc2109975
30. Yamamoto M, Tajiri K, Ayuzawa S, Ieda M. Pathological findings of clinically suspected myocarditis temporally associated with COVID-19 vaccination. Eur J Heart Fail. (2022) 24(6):1132–8. doi: 10.1002/ejhf.2523
31. Larson KF, Ammirati E, Adler ED, Cooper LT Jr., Hong KN, Saponara G, et al. Myocarditis after BNT162b2 and mRNA-1273 vaccination. Circulation. (2021) 144(6):506–8. doi: 10.1161/CIRCULATIONAHA.121.055913
32. Rosner CM, Genovese L, Tehrani BN, Atkins M, Bakhshi H, Chaudhri S, et al. Myocarditis temporally associated with COVID-19 vaccination. Circulation. (2021) 144(6):502–5. doi: 10.1161/CIRCULATIONAHA.121.055891
33. Grun S, Schumm J, Greulich S, Wagner A, Schneider S, Bruder O, et al. Long-term follow-up of biopsy-proven viral myocarditis: predictors of mortality and incomplete recovery. J Am Coll Cardiol. (2012) 59(18):1604–15. doi: 10.1016/j.jacc.2012.01.007
34. Grani C, Eichhorn C, Biere L, Murthy VL, Agarwal V, Kaneko K, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol. (2017) 70(16):1964–76. doi: 10.1016/j.jacc.2017.08.050
35. Aquaro GD, Perfetti M, Camastra G, Monti L, Dellegrottaglie S, Moro C, et al. Cardiac MR with late gadolinium enhancement in acute myocarditis with preserved systolic function: ITAMY study. J Am Coll Cardiol. (2017) 70(16):1977–87. doi: 10.1016/j.jacc.2017.08.044
36. Amir G, Rotstein A, Razon Y, Beyersdorf GB, Barak-Corren Y, Godfrey ME, et al. CMR imaging 6 months after myocarditis associated with the BNT162b2 mRNA COVID-19 vaccine. Pediatr Cardiol. (2022) 43(7):1522–29. doi: 10.1007/s00246-022-02878-0
37. Hadley SM, Prakash A, Baker AL, de Ferranti SD, Newburger JW, Friedman KG, et al. Follow-up cardiac magnetic resonance in children with vaccine-associated myocarditis. Eur J Pediatr. (2022) 181(7):2879–83. doi: 10.1007/s00431-022-04482-z
38. Berg J, Kottwitz J, Baltensperger N, Kissel CK, Lovrinovic M, Mehra T, et al. Cardiac magnetic resonance imaging in myocarditis reveals persistent disease activity despite normalization of cardiac enzymes and inflammatory parameters at 3-month follow-up. Circ Heart Fail. (2017) 10(11):e004262. doi: 10.1161/CIRCHEARTFAILURE.117.004262
39. Dubey S, Agarwal A, Nguyen S, Adebo D. Persistence of late gadolinium enhancement on follow-up CMR imaging in children with acute myocarditis. Pediatr Cardiol. (2020) 41(8):1777–82. doi: 10.1007/s00246-020-02445-5
Keywords: adolescent, myocarditis, COVID-19, vaccine, case report
Citation: Han J, Lee J, Choi S, Lee H and Song YH (2022) Case report: Myocarditis with nonsustained ventricular tachycardia following COVID-19 mRNA vaccination in a female adolescent. Front. Pediatr. 10:995167. doi: 10.3389/fped.2022.995167
Received: 15 July 2022; Accepted: 3 November 2022;
Published: 21 November 2022.
Edited by:
Elena Cervi, Great Ormond Street Hospital for Children NHS Foundation Trust, United KingdomReviewed by:
Tamas Alexy, University of Minnesota Twin Cities, United States© 2022 Han, Lee, Choi, Lee and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joowon Lee andsZWUwNEBnbWFpbC5jb20=
Specialty Section: This article was submitted to Pediatric Cardiology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.