
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 02 September 2022
Sec. Pediatric Gastroenterology, Hepatology and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.983717
 Elodie Privat1
Elodie Privat1 Madeleine Aumar1,2Delphine Ley1,2
Madeleine Aumar1,2Delphine Ley1,2 Léa Chantal Tran2Stéphanie Coopman1Dominique Guimber1Dominique Turck1,2Frédéric Gottrand1,2*
Léa Chantal Tran2Stéphanie Coopman1Dominique Guimber1Dominique Turck1,2Frédéric Gottrand1,2*Objectives: Malnutrition is common in children with biliary atresia (BA) awaiting liver transplantation (LT). Few studies have evaluated the effectiveness of enteral nutrition (EN) in these patients. The objective of this work was to assess the efficacy and tolerance of EN in children with BA awaiting LT.
Methods: A total of 31 patients with BA followed between 1995 and 2018 were retrospectively included. Anthropometric indicators (weight, length, and head circumference) and adverse effects of EN were noted at the start (T0) and the end (T1) of EN. The z-scores for anthropometric indicators were compared between T0 and T1.
Results: The median age at T0 was 7 months (interquartile range [IQR] 5–9), and the median duration of EN was 9 months (IQR 3–17). The z-scores for anthropometric variables improved from T0 to T1: –1.6 (IQR –2.5 to –1.0) to –0.5 (IQR –1.8 to 0.3) for median weight for age; –1.3 (IQR –2.4 to 0) to –0.4 (IQR –2.0 to 0.7) for length for age; –0.9 (IQR –2.3 to –0.3) to –0.3 (IQR –1.2 to 0.1) for weight for length; and –1.2 (IQR –2.1 to –0.6) to –0.2 (IQR –1.6 to 0.4) for body mass index (p < 0.05 for all comparisons). Nearly all (94%) of the patients had a weight-for-length z-score > –2 at the end of EN; 23% had adverse effects and 10% had complications leading to the cessation of EN.
Conclusion: EN is effective and well tolerated in infants with BA awaiting LT.
Biliary atresia (BA) is the most common cause of neonatal cholestasis and the leading indication for liver transplantation (LT) in children (1, 2). The incidence of BA in France is 1 in 18,400 births, or about 41 children per year (2). BA involves the progressive fibrosis of the intra- and extrahepatic bile ducts and leads to obstruction (3, 4). Surgical treatment comprises the restoration of bile drainage using Kasai portoenterostomy (KPE).
A total of 70–80% of patients who undergo an operation for BA progress to biliary cirrhosis requiring LT (2, 5–7). Malnutrition is a common complication of cholestatic and end-stage liver diseases (8–11) and is related mainly to low-energy intake, altered nutrient metabolism (increased energy expenditure, insulin resistance, and abnormal oxidation of macronutrients), and malabsorption/maldigestion (1, 4, 12–14). Malnutrition is associated with increased morbidity and mortality following LT (1, 8, 12, 15–17) and with compromised neurocognitive development (12, 15, 18, 19). Nutritional management of children awaiting LT is therefore essential.
Due to the high energy needs in children with cholestasis, energy intake should be increased to 130–150% of the dietary reference values (DRVs) (1, 12). This objective is difficult to achieve through oral feeding alone (20). The use of enteral nutrition (EN) may help to ensure good nutritional status and therefore improve post-LT survival and neurocognitive development (12, 14, 21–23). Few studies have evaluated the efficacy of EN in patients with BA awaiting LT (12, 18, 20). The objective of this study was to assess the efficacy and tolerance of EN in children with BA awaiting LT.
We conducted a retrospective, observational, and monocentric study. We analyzed data for patients who were operated on for BA in our tertiary hospital in Lille, France, between 1995 and 2018.
Every child operated on for BA between 1995 and 2018 in the Lille University Hospital who was awaiting LT and who received EN were included. The feed was started as soon as growth was faltering and was given overnight. Children who received parenteral nutrition (PN) as first-line treatment and children who were still receiving EN at the time of the study were not included.
The primary study end point was the success rate of EN defined a priori as a weight-for-length (W/L) or weight-for-height (W/H) z-score > –2 at the end of EN and a decrease of < 0.5 standard deviation (SD) between the start (T0) and end (T1) of EN. The secondary study end points were z-scores for the evolution of weight for age, height, or length for age, W/L or W/H, head circumference (HC), mid-upper arm circumference (MUAC), body mass index (BMI) at T0 and T1, and tolerance of EN.
Data were extracted from the national register for BA. The data were collected during medical consultations, assessments by dietitians, hospitalizations, and during home visits by the Home Artificial Nutrition Unit. The Home Artificial Nutrition Unit is a department of the Lille University Hospital that ensures the management of EN at home through a quarterly visit by a dietitian, who performs anthropometric measurements and evaluates energy intake and EN tolerance. The following information was collected:
– Date of birth, sex, weight (considered apart from ascites or edema conditions), length, and HC at birth, prematurity, and intrauterine growth retardation.
– Age at surgery and complications of surgery.
– T0 and T1 for EN, and reason(s) for stopping EN.
– Complications of EN, including vomiting, diarrhea, abdominal pain, inhalation, ascites, hemorrhage, or refeeding syndrome, and major complications of EN such as complications leading to the cessation of EN.
Clinical and biological parameters were collected at T0 and T1. Anthropometric parameters included weight, length, or height, W/L or W/H, BMI, HC, and MUAC. The following parameters were collected:
– Weight was measured without clothes, to the nearest 10 g.
– The length was measured in the supine position with a tape measure before 2 years of age.
– Height was measured while standing after age 2 years. HC was measured by encircling the supraorbital ridges and occipital protuberance.
– Microcrania was defined as an HC > 2 SD below the mean for sex and age.
Anthropometric parameters were expressed as z-scores according to the French reference growth charts of Sempé and Pédron (24). BMI was expressed as a z-score according to the French reference charts of Rolland-Cachera (25).
The following other information was also collected:
– Laboratory values such as conjugated bilirubin (μmol/L), prothrombin (%), albumin (g/L), and γ-glutamyl transferase (GGT) (U/L).
– Diuretic treatments.
– EN formula and daily caloric intake by EN and oral feeding as a percentage of the DRVs for age and sex (26).
– Presence of portal hypertension (splenomegaly, leukopenia, thrombocytopenia, and esophageal varices), edema of the lower limbs, or ascites (clinically and/or on ultrasound).
Qualitative data are presented by frequency and percentage. Quantitative data are expressed as mean and SD and/or median and interquartile range (IQR). Anthropometric data were compared between T0 and T1 using the non-parametric matched Wilcoxon test. A p-value of < 0.05 was considered to be significant. Statistical analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC, United States) by the Biostatistics Unit of Lille University Hospital.
In accordance with French laws, because this study was retrospective and observational, formal informed consent from the patients/parents and ethical committee approval were not required. All data were anonymized.
A total of 94 patients with BA were followed up at the Lille University Hospital between 1995 and 2018. A total of 41 patients were successfully operated on and did not require LT (Figure 1). A total of 34 (36%) patients with BA received EN while awaiting LT: three were still receiving EN at the time of the study and were excluded from the analysis. Finally, 31 patients who received EN before LT were included. Most were girls (sex ratio 0.72). The number of patients included every year in the program (1–2 per year) did not change over the study period as well as the age when EN was started (7.5 months ± 2.3 SD vs. 6.2 months ± 3.1 SD, comparing the first 16 patients from 2008 to 2010, to the last 15 patients from the more recent period, p = 0.18). Only one patient had intrauterine growth retardation. The mean age at KPE was 56 days (± 19). Two patients were not operated on because of a delayed diagnosis.
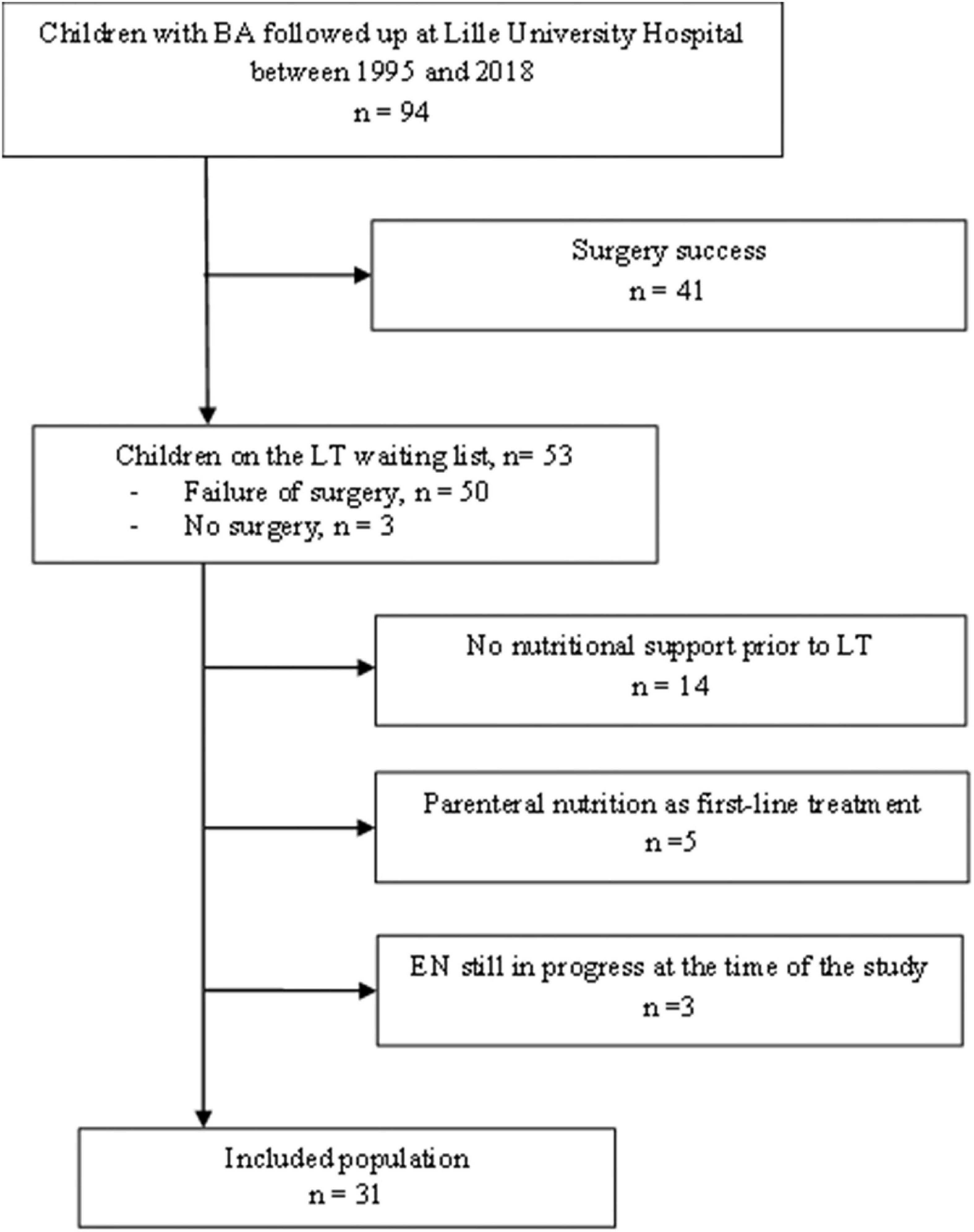
Figure 1. Study flow-chart. BA, biliary atresia; LT, liver transplantation.
The median age at T0 was 7 months (IQR 5–9). EN was started after the age of 1 year in only two patients. The median W/L or W/H z-score at T0 was –0.9 (IQR –2.3 to –0.3) and improved up to 0.3 at T1 (IQR –1.2 to 0.1). Notably, nine (29%) patients had a W/L or W/H z-score < –2, and ten (32%) patients had growth retardation (length- or height-for-age z-score < –2). All patients received semi-elemental formula except for one patient who received an amino acid-based formula because of an immunoglobulin E-mediated cow’s milk protein allergy that was resistant to hydrolyzed formula. The semi-elemental formula (Peptamen Junior, produced by Nestlé, Vevey, Switzerland) was isocaloric (1 kcal/ml) or hypercaloric (1.5 kcal/ml) with 60% of medium-chain triglycerides (MCTs) according to volume tolerance. The mean intake of protein/kg of body weight was 1.5 ± 0.7 SD. None of the patients had dextrin maltose or protein added to the formula. We chose to systematically start EN for a night administration for patient’s comfort and affect as less as possible their oral feeding intake during the day. When calculating the energy supply by EN, we anticipated a 10% reduction in the patient’s oral intake. Finally, we also adapted the caloric intake according to the evolution of their oral intake and their weight gain, which often ends in prolonging EN duration.
All patients had portal hypertension. A total of 14 (45%) patients received diuretic treatment (furosemide or spironolactone). The mean albumin concentration was 33 g/L (SD, 4), mean prothrombin time was 81% (SD ± 15), mean conjugated bilirubin was 234 μmol/L (SD, 104), and mean GGT concentration was 365 U/L (SD, 288).
Of 31 patients, 29 had a W/H or W/L z-score > –2 at T1, and EN failed in two patients, which meant that EN was successful in 94% of the patients. The first patient with EN failure had intrauterine growth retardation. He underwent a KPE at 48 days of age. EN was started 15 days after surgery because of poor oral intake but was not well tolerated, as shown by vomiting and bloating. Small-bowel X-ray showed a dilatation, which led to the suspicion of the subocclusive syndrome. However, the patient’s EN tolerance was not ameliorated after adhesiolysis, and EN was stopped at the age of 4 months and PN was started. The W/L z-score at T1 was –2.2. The second patient with EN failure had a syndromic BA involving interatrial communication, anomalous pulmonary venous return, and intestinal malrotation. He underwent heart surgery at the age of 4 months. EN was stopped at 6 months because of insufficient weight gain and PN was started. The patient’s W/L z-score at T1 was –2.1. This patient died at the age of 7.5 months from respiratory failure related to hepatopulmonary syndrome while awaiting LT.
The median duration of EN was 9 months (IQR 3–17), and the median age at T1 was 18 months (IQR 9–26). The z-score for weight, length, or height, W/L or W/H, and BMI improved significantly between T0 and T1 (p < 0.05) (Figure 2). The percentages of patients with a z-score < –2 decreased between T0 and T1 for weight, length, or height, HC, and W/L or W/H. The difference was significant for W/L or W/H (Figure 3). The evolution of MUAC between T0 and T1 could not be analyzed because of the extent of missing data at T1 (20/31 patients, 65% of patients with missing data).
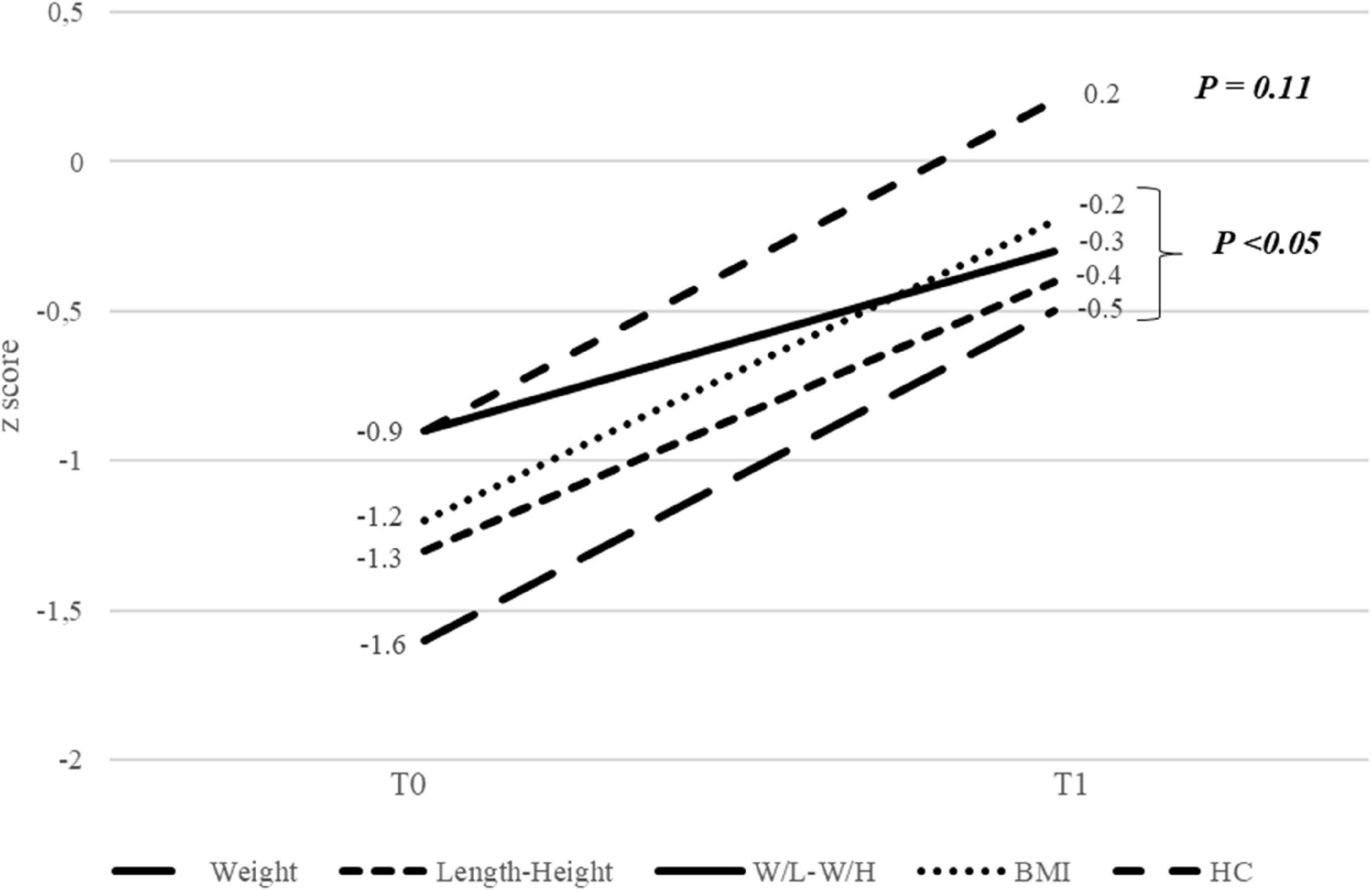
Figure 2. Evolution of anthropometric parameters between the start (T0) and end (T1) of enteral nutrition. W/L, weight for length; W/H, weight for height; BMI, body mass index; HC, head circumference.
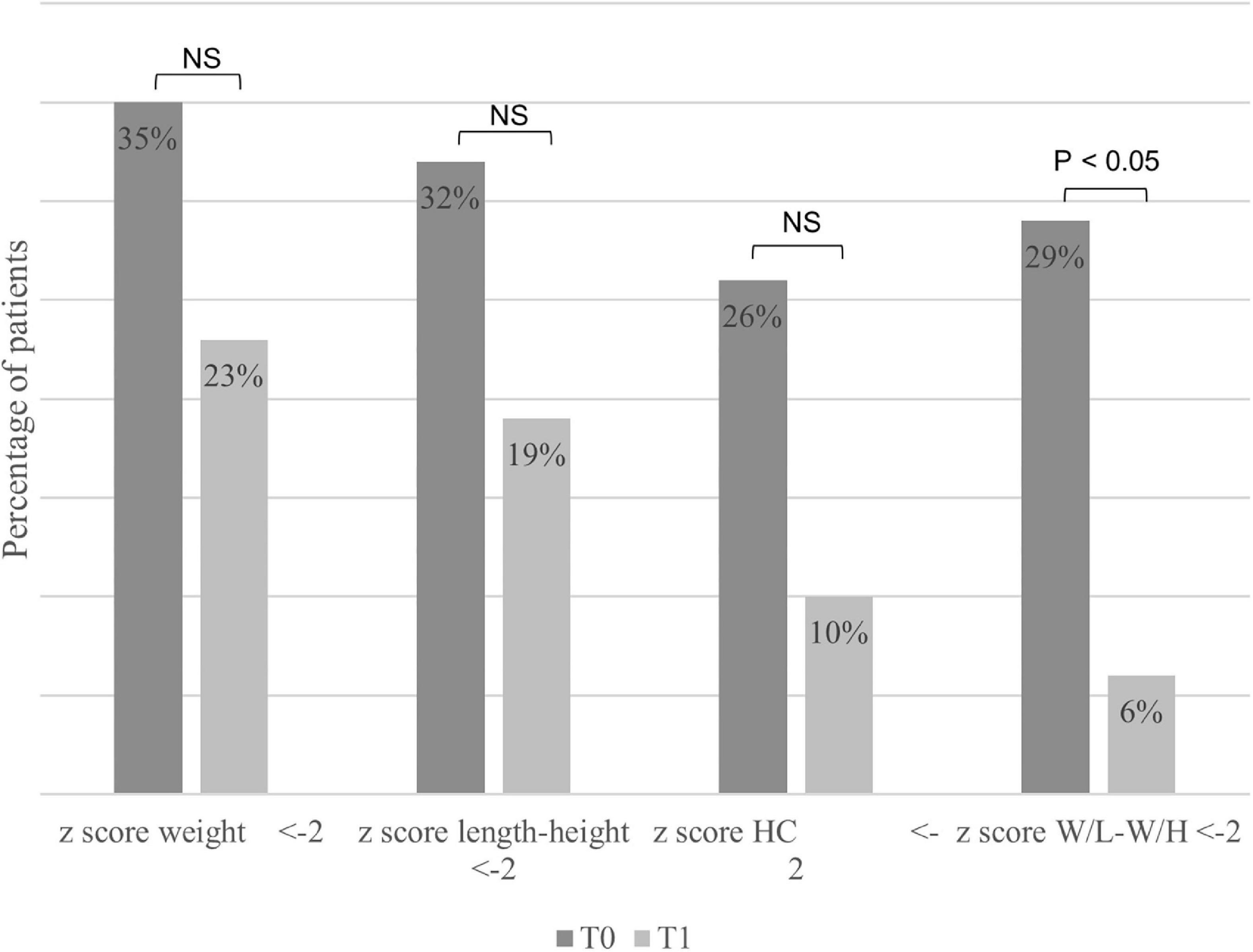
Figure 3. Percentage of patients with a z score < –2 for anthropometric parameters at the start (T0) and the end (T1) of enteral nutrition. HC, head circumference; W/L, weight for length; W/H, weight for height; NS, not significant.
At T0, the mean oral caloric intake was 101% of the DRVs, and the mean total caloric intake (oral + enteral) was 186% of the DRVs. Between T0 and T1, oral intake decreased from 101% to 68% of the DRVs, and enteral intake increased from 85 to 91% of the DRVs. At T1, the mean total caloric intake was 159% of the DRVs.
Of the patients, seven (23%) had complications; each patient could have several complications (Table 1). Of note, four (13%) patients had nausea or vomiting, two (6%) patients had diarrhea, and three (10%) patients frequently removed their nasogastric tubes. These complications occurred mainly at the start of EN and improved within a few weeks. In one patient with diarrhea and vomiting, the diagnosis of cow’s milk protein allergy was confirmed, and the symptoms regressed after the introduction of amino acid-based formula. In addition, three (10%) patients had major complications that led to the cessation of EN and the switch to PN, two (6%) patients had recurrent vomiting with bloating and discomfort, and one patient had fluid overload with respiratory distress; this patient had severe congenital anomalies associated with BA such as interatrial communication, ventricular septal defect, and bridging bronchus.
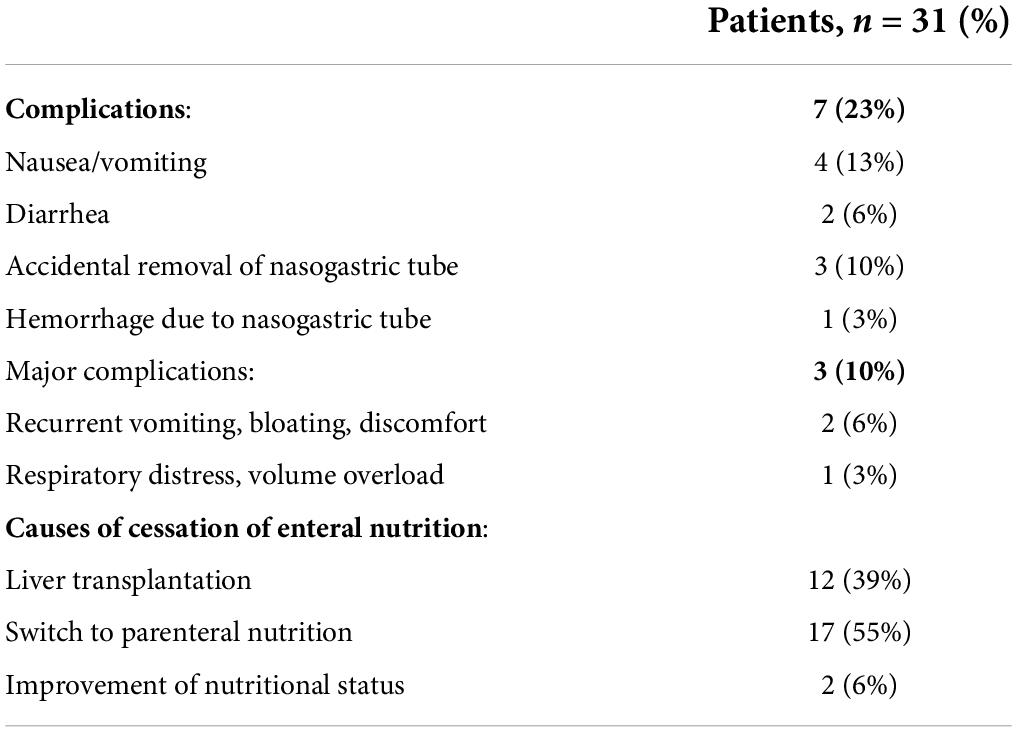
Table 1. Complications and reasons for cessation of enteral nutrition.
No death caused by EN or refeeding syndrome was reported. EN was continued until LT in 12 (39%) patients. A switch to PN was necessary in 17 (55%) patients because of insufficient weight gain (n = 6), ascites (n = 5), hematemesis (n = 2), respiratory distress (n = 2), protein-losing enteropathy (n = 1), or recurrent cholangitis (n = 1). For two patients, EN was stopped because their nutritional status improved and they returned to full oral feeding until LT.
Our study found significant improvements in weight, length, or height, BMI, and W/L or W/H z-score between the start (T0) and end (T1) of EN in patients with BA awaiting LT. Most patients had a W/L or W/H z-score > –2 when EN was stopped. EN was generally well tolerated, and only 10% of patients had major complications that led to the cessation of EN.
Our study confirms the main findings of a previous study by Macías-Rosales et al. that compared the effectiveness of EN vs. oral nutrition for 12 weeks in 15 infants with BA (20). In the EN group, the z-scores for length and HC remained stable from T0 to T1: –2.4 to –2.2 (p = 0.697) and –1.9 to –2.1 (p = 0.650), respectively. These values decreased significantly in the oral nutrition group: –2.4 to –3.2 (p < 0.001) for length and –1.5 to –2.1 (p < 0.001) for HC (20). In a case series of five patients with chronic cholestasis who underwent percutaneous endoscopic gastrostomy, one boy with BA showed a weight gain of 3.1 kg after 10 months but also developed ascites and needed PN (27). Holt et al. showed that the linear growth and anthropometric measurements of 33 children with BA and failure to thrive improved after 3–7 months of nasogastric feeding (28). Yuksekkaya et al. found an improvement in MUAC after 2 months of EN in 38 children (median age 5.6 months ± 3.2) with neonatal cholestasis, including nine children with BA (15). Similarly, Charlton et al. reported significant improvements in the z-scores for weight and MUAC after 8 weeks of EN in 10 children with advanced cirrhosis, 6 of whom had BA (18).
Interestingly, 55% of our cohort finally required conversion to PN because of poor weight gain or ascites. This finding shows that PN may be an alternative in some patients and shows benefits by improving children’s nutritional status as reported by Wendel et al. (29). Sullivan et al. (30) also demonstrated better anthropometric outcomes when comparing 25 patients with BA who had PN and 22 patients without PN, with a mean duration of PN of 2.9 months, after a same mean duration of EN. Using PN is also recommended in case of EN failure by the 2019 guidelines published by Mouzaki et al. (12), as well as a recent review by Boster et al., who advised first using oral feeds, second nasogastric tube feeding when oral intake is insufficient, and third PN in case of poor growth despite NG feeds (31). Our results reinforce the importance to set up an early EN prior to transplantation in order to prevent the onset of malnutrition and consequences of advanced chronic liver diseases and avoid the use of PEN.
A new finding of our study is that, although not statistically significant, the rate of children with microcrania decreased from 26 to 10% from T0 to T1. This suggests a positive effect of improving nutrition on brain growth in these children. Infancy and early childhood (from birth to 24 months) are critical periods for neurodevelopment because of the rapid growth and differentiation of brain regions (32, 33). As the young brain accounts for 60% of the body’s energy consumption, malnutrition during early childhood may compromise neurodevelopment (32). Language and motor skills are impaired in children with BA awaiting LT, although the roles of chronic liver disease and prolonged hospitalization in these children are not clearly understood (34). Growth retardation before LT is an independent risk factor for long-term cognitive deficit (34–40).
In addition to being effective, EN was well tolerated. Most of the complications were transient and resolved quickly except in two patients. In the study by Macías-Rosales et al., diarrhea was experienced more often by patients in the EN group than in the oral nutrition group, but the rates of respiratory infections, vomiting, and abdominal distension did not differ between groups (20). Charlton et al. reported good tolerance to EN. During the 8 weeks of that study, all children tolerated a daily caloric intake of 140% of the DRVs (18).
As previously reported, our study found a high prevalence of malnutrition in children with BA despite optimized oral intake. All of our patients were under the care of a dietitian and received high-calorie formula (0.8–1.2 kcal/ml) before the start of EN. This prompted us to choose semi-elemental formulas enriched in MCT for most patients. In fact, in France, chronic liver disease-specific formulas enriched with branched-chain amino acids are not available. We were fully aware that children with an advanced BA should benefit from these formulas that were designed for cholestatic infants, as stated in the 2007 nutritional guidelines by Baker et al. (21). The only way to add MCT, which are necessary due to cholestasis and long-chain fatty acid malabsorption, was to use semi-elemental formulas that contain 60% of MCT. However, even with this fortified diet, the mean oral caloric intake was only 101% of the DRVs at T0. Macías-Rosales et al. found similar results (20). Shepherd et al. reported that oral caloric intake was 63% of the DRVs at the time of acceptance for LT (41). These findings indicate that appropriate caloric intake (130–150% of the DRVs) cannot always be achieved by optimizing the oral diet (1, 12, 21). EN made it possible to achieve the high caloric intake recommended in patients with BA (> 130% of the caloric requirements for age). Moreover, growth retardation occurs early. In this study, 32% of children had chronic malnutrition (length z-score < –2 SD) at a median age of 7 months.
The North American and European Societies for Pediatric, Gastroenterology, Hepatology and Nutrition recently proposed a practical approach to the nutritional support of children with the end-stage liver disease through the early onset of EN (12). EN on a nasogastric or nasojejunal tube is recommended in cases of poor tolerance or poor evolution of anthropometric parameters after 2–4 weeks of an optimized oral diet (e.g., fortified diet, use of medium-chain triglyceride-enriched formula, and smaller volumes more frequently) (12). These recommendations should lead to an earlier introduction of EN. Utterson et al. reported that only 16% of the 755 children awaiting LT had EN but that > 40% had growth failure (16). The early introduction of EN should help to improve the nutritional status before LT and, therefore, reduce the risk of morbidity and mortality following LT and improve brain development (8, 16, 17).
This study has both strengths and limitations. The strengths are the homogeneous population and follow-up of a large series of patients with BA. The limitations are the retrospective design and the missing data for MUAC at the follow-up. The study protocol, retrospective and over a long time period, does not allow to replicate our results. We, however, checked that there were no changes over time in the number of patients and the age of patients when starting EN. In fact, we included a mean of 1–2 patients per year over 23 years, and the age at T0 between the first 16 included patients (from 1999 to 2010) and the last 15 patients (from 2011 to 2018) was not statistically different (7.5 months ± 2.3 SD vs. 6.2 months ± 3.1 SD, p = 0.18). In patients with BA, weight measurement may be distorted by ascites, fluid overload, and/or organomegaly, which may lead to underestimation of malnutrition. We only recorded the presence/absence of ascites without grading its severity at T0 and T1. We, unfortunately, lack the INR values to calculate the PELD score, as well as MUAC values, for which we had 20 missing data, hindering us to use this parameter. In this context, MUAC is useful because it is less likely to be affected by fluid overload and is sensitive to short-term changes in nutritional status (12). We also did not collect EN modalities. In fact, recording the hours of EN administration is particularly relevant when the spontaneous oral intake tends to decrease over time in BA as in other chronic liver diseases.
Enteral nutrition is effective and well tolerated in children with BA awaiting LT when commenced earlier. However, PN might still be required and then should be started without delay. EN significantly improves the z-score for weight, length, or height, W/L or W/H, and BMI. EN should be started early to prevent morbidity and mortality following LT and improve neurological development.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants or their legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
EP contributed substantially to the design of the work, the acquisition, analysis, and interpretation of data, wrote the draft, approved the final version of the manuscript, and agreed to be responsible for all aspects of the work by ensuring that the issues related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MA, DL, LT, SC, DG, DT, and FG contributed substantially to the design of the work, the analysis and interpretation of data, revised the manuscript critically, approved the final version of the manuscript, and agreed to be responsible for all aspects of the work by ensuring that the issues related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Young S, Kwarta E, Azzam R, Sentongo T. Nutrition assessment and support in children with end-stage liver disease. Nutr Clin Pract. (2013) 28:31729. doi: 10.1177/0884533612474043
2. Chardot C, Buet C, Serinet MO, Golmard JL, Lachaux A, Roquelaure B, et al. Improving outcomes of biliary atresia: French national series 1986-2009. J Hepatol. (2013) 58:120917. doi: 10.1016/j.jhep.2013.01.040
3. Sanchez-Valle A, Kassira N, Varela VC, Radu SC, Paidas C, Kirby RS. Biliary atresia: epidemiology, genetics, clinical update, and public health perspective. Adv Pediatr. (2017) 64:285305. doi: 10.1016/j.yapd.2017.03.012
4. Kilgore A, Mack CL. Update on investigations pertaining to the pathogenesis of biliary atresia. Pediatr Surg Int. (2017) 33:123341. doi: 10.1007/s00383-017-4172-6
5. Ramos-Gonzalez G, Elisofon S, Dee EC, Staffa SJ, Medford S, Lillehei C, et al. Predictors of need for liver transplantation in children undergoing hepatoportoenterostomy for biliary atresia. J Pediatr Surg. (2019) 54:112731. doi: 10.1016/j.jpedsurg.2019.02.051
6. Nio M. Japanese biliary atresia registry. Pediatr Surg Int. (2017) 33:131925. doi: 10.1007/s00383-017-4160-x
7. Kasahara M, Umeshita K, Sakamoto S, Fukuda A, Furukawa H, Uemoto S. Liver transplantation for biliary atresia: a systematic review. Pediatr Surg Int. (2017) 33:128995. doi: 10.1007/s00383-017-4173-5
8. DeRusso PA, Ye W, Shepherd R, Haber BA, Shneider BL, Whitington PF, et al. Growth failure and outcomes in infants with biliary atresia: a report from the Biliary Atresia Research Consortium. Hepatol Baltim Md. (2007) 46:16328. doi: 10.1002/hep.21923
9. da Silva FV, Ferri PM, Nascentes Queiroz TC, de Souza Haueisen Barbosa P, Cassiano de Oliveira MC, de Melo Pereira LJ, et al. Nutritional evaluation of children with chronic cholestatic disease. J Pediatr (Rio J). (2016) 92:197205. doi: 10.1016/j.jped.2015.07.006
10. Cywes C, Millar AJ. Assessment of the nutritional status of infants and children with biliary atresia. South Afr Med J. (1990) 77:1315.
11. Zamberlan P, Leone C, Tannuri U, Carvalho WB, de Delgado AF. Nutritional risk and anthropometric evaluation in pediatric liver transplantation. Clin Sao Paulo Braz. (2012) 67:138792. doi: 10.6061/clinics/2012(12)07
12. Mouzaki M, Bronsky J, Gupte G, Hojsak I, Jahnel J, Pai N, et al. Nutrition support of children with chronic liver diseases: a joint position paper of the north american society for pediatric gastroenterology, hepatology, and nutrition and the european society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. (2019) 69:498–511. doi: 10.1097/MPG.0000000000002443
13. Sundaram SS, Mack CL, Feldman AG, Sokol RJ. Biliary atresia: Indications and timing of liver transplantation and optimization of pretransplant care. Liver Transplant. (2017) 23:96109. doi: 10.1002/lt.24640
14. Yang CH, Perumpail BJ, Yoo ER, Ahmed A, Kerner JA. Nutritional needs and support for children with chronic liver disease. Nutrients. (2017) 9:1127. doi: 10.3390/nu9101127
15. Yuksekkaya HA, Cakir M, Tumgor G, Baran M, Arikan C, Yagci RV, et al. Nutritional status of infants with neonatal cholestasis. Dig Dis Sci. (2008) 53:8038. doi: 10.1007/s10620-007-9917-y
16. Utterson EC, Shepherd RW, Sokol RJ, Bucuvalas J, Magee JC, McDiarmid SV, et al. Biliary atresia: clinical profiles, risk factors, and outcomes of 755 patients listed for liver transplantation. J Pediatr. (2005) 147:1805.
17. Barshes NR, Chang IF, Karpen SJ, Carter BA, Goss JA. Impact of pretransplant growth retardation in pediatric liver transplantation. J Pediatr Gastroenterol Nutr. (2006) 43:8994. doi: 10.1097/01.mpg.0000226378.03247.1f
18. Charlton CP, Buchanan E, Holden CE, Preece MA, Green A, Booth IW, et al. Intensive enteral feeding in advanced cirrhosis: reversal of malnutrition without precipitation of hepatic encephalopathy. Arch Dis Child. (1992) 67:6037. doi: 10.1136/adc.67.5.603
19. Black MM, Pérez-Escamilla R, Rao SF. Integrating nutrition and child development interventions: scientific basis, evidence of impact, and implementation considerations. Adv Nutr Bethesda Md. (2015) 6:8529. doi: 10.3945/an.115.010348
20. Macías-Rosales R, Larrosa-Haro A, Ortíz-Gabriel G, Trujillo-Hernández B. Effectiveness of enteral versus oral nutrition with a medium-chain triglyceride formula to prevent malnutrition and growth impairment in infants with biliary atresia. J Pediatr Gastroenterol Nutr. (2016) 62:1019. doi: 10.1097/MPG.0000000000000909
21. Baker A, Stevenson R, Dhawan A, Goncalves I, Socha P, Sokal E. Guidelines for nutritional care for infants with cholestatic liver disease before liver transplantation. Pediatr Transplant. (2007) 11:82534. doi: 10.1111/j.1399-3046.2007.00792.x
22. Nightingale S, Ng VL. Optimizing nutritional management in children with chronic liver disease. Pediatr Clin North Am. (2009) 56:116183. doi: 10.1016/j.pcl.2009.06.005
23. Cleghorn G. The role of basic nutritional research in pediatric liver disease: an historical perspective. J Gastroenterol Hepatol. (2009) 24(Suppl 3):S93–6. doi: 10.1111/j.1440-1746.2009.06078.x
24. Sempé (M). — Auxologie, méthode et séquences. (Vol. 7). Paris: Bull Mém Société Anthropol (1980). 77 p.
25. Rolland-Cachera MF, Cole TJ, Sempé M, Tichet J, Rossignol C, Charraud A. Body Mass Index variations: centiles from birth to 87 years. Eur J Clin Nutr. (1991) 45:1321.
26. Actualisation des repères du Pnns: élaboration des références nutritionnelles. Avis de l’Anses. Rapports d’expertise Collective. (2016). Available online at: https://www.anses.fr/fr/system/files/NUT2012SA0103Ra-2.pdf (accessed December 12, 2016).
27. Duché M, Habès D, Lababidi A, Chardot C, Wenz J, Bernard O. Percutaneous endoscopic gastrostomy for continuous feeding in children with chronic cholestasis. J Pediatr Gastroenterol Nutr. (1999) 29:425. doi: 10.1097/00005176-199907000-00012
28. Holt RI, Miell JP, Jones JS, Mieli-Vergani G, Baker AJ. Nasogastric feeding enhances nutritional status in paediatric liver disease but does not alter circulating levels of IGF-I and IGF binding proteins. Clin Endocrinol (Oxf). (2000) 52:21724. doi: 10.1046/j.1365-2265.2000.00934.x
29. Wendel D, Mortensen M, Harmeson A, Shaffer ML, Hsu E, Horslen S. Resolving malnutrition with parenteral nutrition before liver transplant in biliary atresia. J Pediatr Gastroenterol Nutr. (2018) 66:2127. doi: 10.1097/MPG.0000000000001798
30. Sullivan JS, Sundaram SS, Pan Z, Sokol RJ. Parenteral nutrition supplementation in biliary atresia patients listed for liver transplantation. Liver Transplant. (2012) 18:1208. doi: 10.1002/lt.22444
31. Boster JM, Feldman AG, Mack CL, Sokol RJ, Sundaram SS. Malnutrition in biliary atresia: assessment, management, and outcomes. Liver Transplant. (2022) 28:48392. doi: 10.1002/lt.26339
32. Krebs NF, Lozoff B, Georgieff MK. Neurodevelopment: the impact of nutrition and inflammation during infancy in low-resource settings. Pediatrics. (2017) 139(Suppl 1):S508. doi: 10.1542/peds.2016-2828G
33. Rodijk LH, den Heijer AE, Hulscher JBF, Verkade HJ, de Kleine RHJ, Bruggink JLM. Neurodevelopmental outcomes in children with liver diseases: a systematic review. J Pediatr Gastroenterol Nutr. (2018) 67:15768. doi: 10.1097/MPG.0000000000001981
34. Caudle SE, Katzenstein JM, Karpen SJ, McLin VA. Language and motor skills are impaired in infants with biliary atresia before transplantation. J Pediatr. (2010) 156:936–40. doi: 10.1016/j.jpeds.2009.12.014
35. Caudle SE, Katzenstein JM, Karpen S, McLin V. Developmental assessment of infants with biliary atresia: differences between boys and girls. J Pediatr Gastroenterol Nutr. (2012) 55:3849. doi: 10.1097/MPG.0b013e318259ed20
36. Sorensen LG, Neighbors K, Martz K, Zelko F, Bucuvalas JC, Alonso EM, et al. Longitudinal study of cognitive and academic outcomes after pediatric liver transplantation. J Pediatr. (2014) 165:65–72. doi: 10.1016/j.jpeds.2014.03.032
37. Kaller T, Langguth N, Petermann F, Ganschow R, Nashan B, Schulz KH. Cognitive performance in pediatric liver transplant recipients. Am J Transplant. (2013) 13:2956–65. doi: 10.1111/ajt.12408
38. Gilmour S, Adkins R, Liddell GA, Jhangri G, Robertson CM. Assessment of psychoeducational outcomes after pediatric liver transplant. Am J Transplant. (2009) 9:294–300. doi: 10.1111/j.1600-6143.2008.02480.x
39. van Mourik ID, Beath SV, Brook GA, Cash AJ, Mayer AD, Buckels JA, et al. Long-term nutritional and neurodevelopmental outcome of liver transplantation in infants aged less than 12 months. J Pediatr Gastroenterol Nutr. (2000) 30:26975.
40. Talcott JB, Beath SV, Patel T, Griffiths G, Kelly DA. Long-term effects of cholestatic liver disease in childhood on neuropsychological outcomes and neurochemistry. J Pediatr Gastroenterol Nutr. (2019) 69:145–51. doi: 10.1097/MPG.0000000000002380
Keywords: biliary atresia, enteral nutrition, nasogastric tube, stunted growth, malnutrition
Citation: Privat E, Aumar M, Ley D, Tran LC, Coopman S, Guimber D, Turck D and Gottrand F (2022) Efficacy and tolerance of enteral nutrition in children with biliary atresia awaiting liver transplantation. Front. Pediatr. 10:983717. doi: 10.3389/fped.2022.983717
Received: 01 July 2022; Accepted: 01 August 2022;
Published: 02 September 2022.
Edited by:
Pietro Vajro, University of Salerno, ItalyReviewed by:
Andrea Pietrobattista, Bambino Gesù Children’s Hospital (IRCCS), ItalyCopyright © 2022 Privat, Aumar, Ley, Tran, Coopman, Guimber, Turck and Gottrand. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frédéric Gottrand, ZnJlZGVyaWMuZ290dHJhbmRAY2h1LWxpbGxlLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.