
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 15 September 2022
Sec. Pediatric Immunology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.981711
This article is part of the Research TopicMacrophage Activation Syndrome in Children in the Era of COVID-19View all 5 articles
 Piotr Buda1*
Piotr Buda1* Ewa Strauss2†
Ewa Strauss2† Danuta Januszkiewicz-Lewandowska3†
Danuta Januszkiewicz-Lewandowska3† Ewa Czerwinska4
Ewa Czerwinska4 Kamila Ludwikowska4
Kamila Ludwikowska4 Leszek Szenborn4
Leszek Szenborn4 Ewelina Gowin5
Ewelina Gowin5 Magdalena Okarska-Napierała6
Magdalena Okarska-Napierała6 Ernest Kuchar6
Ernest Kuchar6 Janusz Ksia̧zyk1
Janusz Ksia̧zyk1Background: Macrophage activation syndrome (MAS) is a potentially life-threatening complication of various inflammatory disorders, including multisystem inflammatory syndrome in children (MIS-C). MIS-C refractory to treatment should raise suspicion of MAS, which can be fatal if a definitive diagnosis is delayed. Unfortunately, there is a lack of data on MAS in children with MIS-C.
Objective: Our study aims to analyze the risk factors for the development of MAS in MIS-C, its clinical course and response to treatment, and identify predictive factors for pediatric intensive care.
Material and methods: We analyzed data from the Polish MIS-C registry of the MultiOrgan Inflammatory Syndromes COVID-19 Related Study. Patients were diagnosed according to the WHO MIS-C definition and treated according to national guidelines (Polish Pediatric Society) based on international consensus. MAS definition was based on 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis.
Results: Two-hundred and seventy four children met the study inclusion criteria. Fifty-nine patients fulfilled MAS classification criteria, nine of which required admission to the pediatric intensive care unit (PICU). MIS-C patients with MAS were significantly older than patients without MAS (median 11.2 vs. 8.1 years). Multivariable analysis showed that age, symptoms characteristic of atypical Kawasaki disease, and skin erosions were significant factors associated with MAS in MIS-C patients. Analysis of laboratory parameters showed that on admission, MIS-C patients with MAS had significantly lower median lymphocyte and platelet counts, albumin and sodium levels, and higher median levels of C-reactive protein, procalcitonin, ferritin, D-dimers, triglycerides, serum creatinine, urea, and γ-glutamyl transpeptidase, and neutrophil count. Multivariate analysis showed that higher procalcitonin, ferritin, and fibrinogen levels at admission were predictive of MAS. Only elevated troponin level was a factor indicating a requirement of PICU hospitalization for children with MAS. MIS-C patients fulfilling MAS criteria were treated more often with intravenous immunoglobulins and steroids than children without MAS. Children with MAS more often required mechanical ventilation. None of the patients required biological agents.
Conclusions: The clinical course of MAS in MIS-C seems milder, treatment less aggressive, and the prognosis better than expected based on the current knowledge on MAS complicating other rheumatological diseases.
Multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) is a new condition (reported in April 2020) associated with the ongoing coronavirus disease 2019 (COVID-19) pandemic, (1–5).
MIS-C develops approximately 4 weeks after symptomatic or asymptomatic SARS-CoV-2 infection (6, 7). It involves hyperinflammatory multisystem damage due to immune dysregulation. Although, the exact pathomechanism of this late COVID-19 complication remains unknown. Several hypotheses include: superantigenic stimulation (8, 9); lymphocyte exhaustion due to chronic SARS-CoV-2 exposure (10–12); increased intestine permeability and translocation of the virus particles into the circulation (13); and autoantibodies production (10, 14–17). Genetic susceptibility probably plays a role, too (18, 19). Immune dysregulation of MIS-C involves activation of neutrophils, macrophages, and dendritic cells with robust chemokine and cytokine production (10, 14, 20), profound lymphopenia (10), decreased IFN-α and increased IFN-γ (IFN-γ) responses (9, 10, 20).
MIS-C is characterized by fever, multisystem organ involvement (gastrointestinal, cardiovascular, neurologic, respiratory, mucocutaneous, renal, and hematologic symptoms), and laboratory findings indicating severe inflammation. Precise diagnostic and treatment guidelines were published by different health organizations (21–24). Polish recommendations were proposed based on international publications and adjusted to the local data (25). MIS-C can have various presentations - from mild, self-limiting disease to severe, life-threatening illness requiring pediatric intensive care unit (PICU) hospitalization. The complications usually involve the cardiovascular system (2, 3, 26). The treatment is based on immunomodulating agents – intravenous immunoglobulins (IVIG), steroids or biological therapy, and supportive care (21, 22, 25).
Although MIS-C has specific epidemiological and clinical features, it may resemble other inflammatory disorders like Kawasaki disease (KD), sepsis, and toxic shock syndrome. Since the beginning, the similarity to macrophage activation syndrome (MAS) has also been observed (2, 3, 17).
MAS is a secondary hemophagocytic lymphohistiocytosis (HLH) associated with autoimmune diseases (27). Usually, MAS is described as a severe exacerbation or one of the most serious complications of connective tissue diseases, particularly systemic juvenile idiopathic arthritis (s-JIA). MAS has also been associated with KD, but the exact incidence is unknown (28, 29). There is a lack of data on MAS in children with COVID-19 and MIS-C. In one of the first MIS-C reports, the incidence is as high as 50% of MIS-C children (2).
MAS is a life-threatening systemic extreme-inflammatory syndrome caused by multifactorial immune dysregulation and pathological hyperactivation of the immune system. The main symptoms include fever and hepatosplenomegaly. They can be followed by coagulopathy and circulatory, respiratory, and multiorgan failure, with mortality rates as high as 8–22 % in children with s-JIA (30, 31). It is challenging to distinguish MAS from other complications (such as s-JIA flares, sepsis-like syndromes, and autoinflammatory disorders) because there are no specific clinical or laboratory markers. KD, s-JIA, and MAS share many common clinical and immunologic features (32).
The MAS criteria are validated for s-JIA (2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis) but are commonly used for other systemic autoinflammatory diseases such as KD and other pediatric rheumatic diseases pediatric (33, 34). Some pediatricians use the criteria of a histiocytic society instead (HLH-2004) (35–37). However, according to Davi et al., they are likely not appropriate for identifying MAS in children with s-JIA because they are intended primarily for genetic forms of HLH (38). MAS may frequently be under-recognized in children with KD because there are no distinct criteria for MAS complicating KD (39). Establishing proper criteria for MAS in different entities is crucial, as it is a severe, life-threatening condition requiring prompt and aggressive immunomodulatory treatment (27, 35). The main goal is to implement MAS treatment as soon as possible to stop the “cytokine storm.” The therapy depends on the underlying disease and the experience of clinical centers (35, 37).
Because there are no specific criteria for diagnosis of MAS in MIS-C and given clinical and laboratory features of MIS-C that resemble MAS, 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis were previously applied to MIS-C (2, 40, 41).
Our study aims to (i) identify risk factors for developing MAS (according to 2016 MAS criteria) in the course of MIS-C; (ii) characterize its clinical presentation and response to treatment; and (iii) identify predictive factors for the need for intensive care in this subgroup of patients.
We analyzed the data from the Polish MIS-C registry of the MultiOrgan Inflammatory Syndromes COVID-19 Related (MOIS-CoR) Study, including the period from March 4, 2020 (when the first COVID-19 case in Poland was confirmed) to April 20, 2021 (42). Anonymous patient data from 42 pediatric hospitals across the country were extracted from patient records and collected using a web-based form developed for this purpose. Registry enrolment of patients did not influence decisions for treatment or PICU admission. Ethical approval was obtained from the Bioethics Committee at the Wroclaw Medical University (CWN UMW BW: 313/2020).
The inclusion criteria for the MOIS-CoR registry and patient eligibility have been presented previously (42). We adopted the WHO definition of MIS-C. MAS was diagnosed based on the 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis (33). MIS-C and MAS definitions were established based on the respective peak values of laboratory findings during the hospitalization. We also verified the diagnosis of MAS based on clinical HLH-2004 criteria (except for the concentration of soluble CD25 and natural killer cell activity because these tests were unavailable) (36).
The selected group of 274 patients was divided into two subgroups - one fulfilling the criteria for MAS and the other without MAS. Children with MAS were additionally divided according to the need for PICU hospitalization. Figure 1 shows the patient inclusion process for the study.
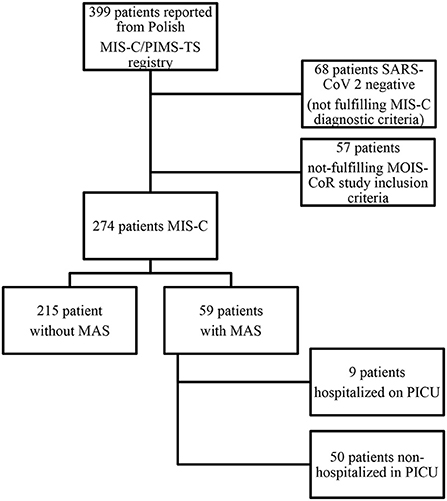
Figure 1. Study flow diagram illustrating the patients' inclusion process for the study.
Demographic characteristics, clinical symptoms, treatment, and outcomes were compared in all subgroups. In addition, laboratory results on admission and at peak (minimum or maximum) were also analyzed. The study's standard definitions and measures, including laboratory and echocardiographic abnormalities, level of consciousness, and nutritional status, have been described in detail in a previous study (42).
Univariate analyses used the t-test or Fisher exact test for quantitative parameters and the χ2 test for qualitative parameters. Continuous parameters with non-normal distribution were analyzed using the Mann-Whitney U test. Normality of distribution was assessed using the Shapiro Wilk test. Logistic regression analysis was used for multivariate analysis, including adjustment for age. Factors deviating from the normal distribution after logarithmic transformation or after conversion to quartiles were examined through these analyses. Analyses were performed using Statistica v10.0 software. Observed differences were considered significant at P < 0.05.
Out of 399 children enrolled in the Polish registry with suspected MIS-C, 274 met the WHO criteria of MIS-C. Fifty-nine patients fulfilled MAS 2016 classification criteria, including nine patients who required admission to PICU (Figure 1). None of the patients with MAS or MIS-C in the whole group met the criteria for hemophagocytic lymphohistiocytosis, according to HLH-2004.
MIS-C patients fulfilling MAS criteria were significantly older than patients without MAS (median 11.2 vs. 8.1 years). For this reason, the age-adjusted analysis was done. MAS was most common in children aged 5–12 years (50.9%) and in MIS-C children with the KD phenotype (57.7%), especially for its atypical form (76.3%). In addition, MIS-C patients with MAS were more likely to have an AVPU score (alert/verbal/pain/unresponsive consciousness assessment scale) below A (12.7 vs. 4.8%), swelling or erythema of the hands and feet (75.5 vs. 49.8%), respiratory distress (41.8 vs. 19.4%), joint pain (32.7 vs. 15.7%), dysuria (27.8 vs. 12.3%), and skin erosions (including chilblains-like phenomenon affecting fingers and toes) (9.6 vs. 1.5%). A small percentage of children had comorbidities, with no significant difference in patients with MAS. Detailed clinical data in the analyzed patient subgroups, including those requiring PICU hospitalization, are presented in Supplementary Table 1. Multivariable analysis showed that greater age, symptoms characteristic of atypical KD, and skin erosion were significantly more common among children with MAS in MIS-C (Table 1).
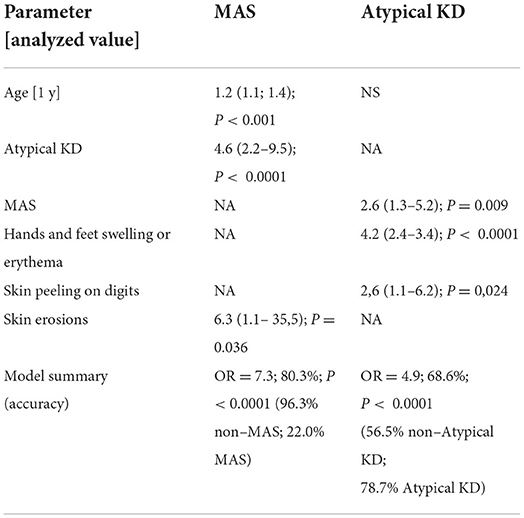
Table 1. Multivariate analysis of the association between symptom occurrence and the presence of macrophage activation syndrome (MAS) or atypical Kawasaki disease (KD) in 274 patients meeting MIS-C criteria.
Analysis of laboratory parameters showed that on admission, MIS-C patients fulfilling MAS criteria had already significantly lower median of lymphocyte (0.74 vs. 1.16 103/μL) and platelet (140 vs. 188 103/μL) counts, albumin (3.1 vs. 3.4 g/dL), and sodium (132 vs. 135 mmol/L) levels compared with patients without MAS. In addition, children with MAS had significantly higher median concentrations of C-reactive protein (CRP) (189.08 vs. 129 mg/L), procalcitonin (8.35 vs. 1.855 ng/mL), ferritin (920.13 vs. 292.3 μg/L), D-dimers (3.78 vs. 2.4 mg/L), triglycerides (210 vs. 140 mg/dL), serum creatinine (0.65 vs. 0.48 mg/dL), urea (27 vs. 22 mg/dL), and activity of γ-glutamyl transpeptidase (40 vs. 20 U/L), and neutrophil count (9.4 vs. 7.04 103/μL). There were also significantly higher median plasma concentrations of bilirubin, B-type natriuretic peptide (BNP) and N-terminal pro-B-type natriuretic peptide (NT-proBNP), troponin, and alanine and aspartate transaminases activities, and estimated glomerular filtration rate (eGFR) in MIS-C patients with MAS. However, the age-adjusted analysis did not confirm any of these differences. Detailed data of laboratory results in MIS-C patients with and without MAS on admission are presented in Supplementary Table 1.
Multivariate analysis of the association between laboratory findings on the admission and MAS criteria fulfillment among 274 children with MIS-C showed that older age, higher procalcitonin, ferritin, and fibrinogen levels were indicative of MAS.
Similar results were obtained by analyzing laboratory parameters at specific peak points in a group of MIS-C children with or without MAS criteria fulfillment. Detailed data are summarized in Supplementary Table 3.
Multivariate analysis showed that elevated leukocyte counts and ferritin plasma concentration were associated with MAS (Table 3).
Among the demographic and clinical characteristics of admission of MIS-C patients with MAS, only hypotension on admission was significantly more common in patients who required treatment in the PICU than other MIS-C children with MAS (62.5 vs. 15.8%) (Supplementary Table 1).
Compared to patients who did not require PICU hospitalization, MIS-C children who finally fulfilled MAS criteria and were treated in the PICU had exceptional laboratory results on admission: significantly higher median leukocyte (13.51 vs. 10.24 103/μL), neutrophil counts (12.4 vs. 8.56 103/μL), and concentrations of procalcitonin (49.87 vs. 6.1 ng/mL), NT-proBNP (32,672 vs. 3,174 pg/mL), serum creatinine (1.4 vs. 0.57 mg/dL), urea (61 vs. 25.5 mg/dL), and fibrinogen (7.14 vs. 5.51 g/L). All children with MAS requiring PICU had elevated serum troponin levels.
Multivariate analysis showed that only elevated troponin level was a predictive factor (Table 2, Figure 2).
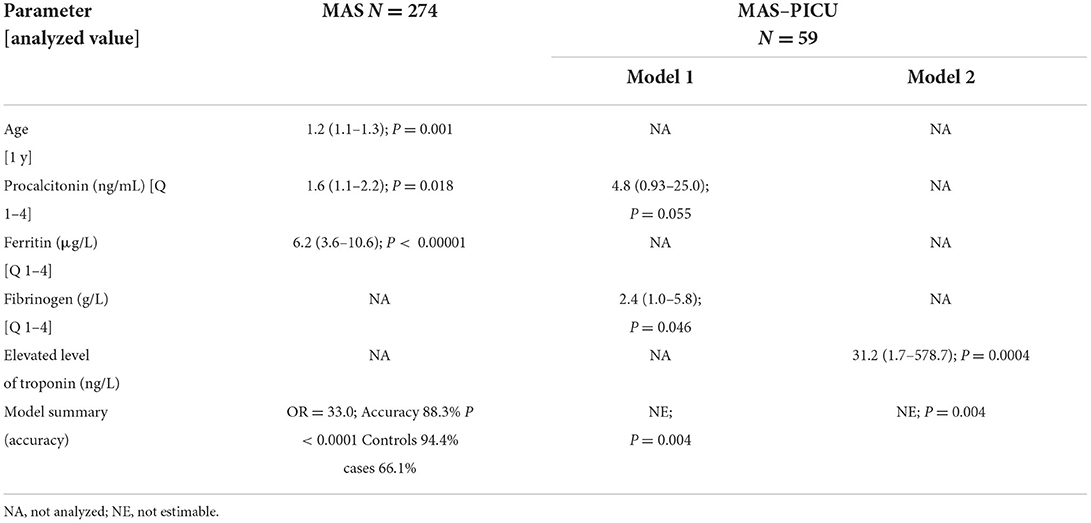
Table 2. Multivariate analysis of the association between laboratory findings on hospital admission and the presence of macrophage activation syndrome (MAS) and MAS requiring pediatric intensive care unit (PICU) hospitalization (MAS–PICU) in 274 patients meeting MIS–C criteria.
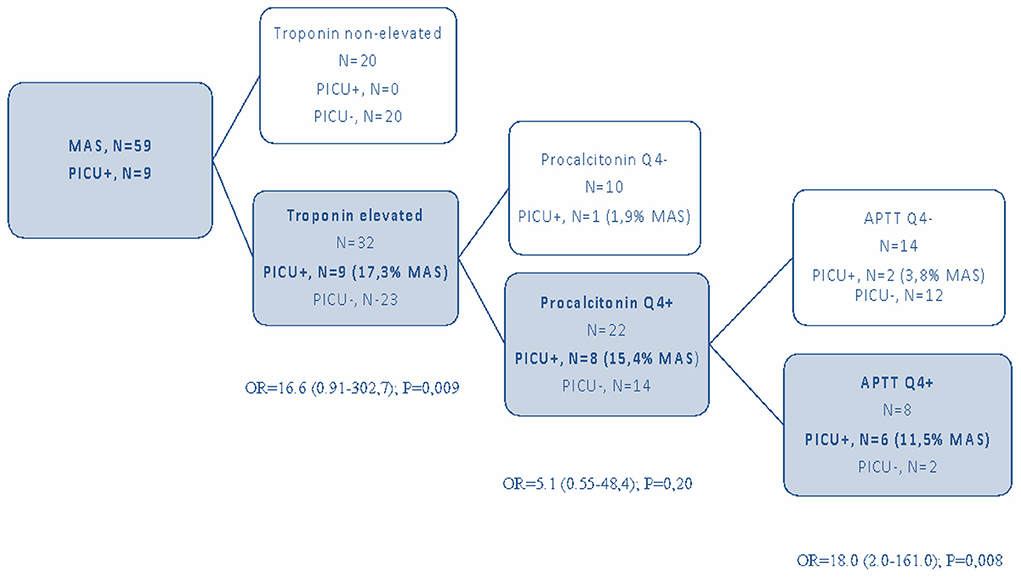
Figure 2. Predictive factors for PICU hospitalization in children with MIS-C and MAS.
Similar results were obtained by analyzing laboratory parameters in the subsequent course of the disease (at its peak). Patients not hospitalized in PICU had a shorter APTT than children admitted to PICU. A detailed analysis of the results is presented in Supplementary Tables 4, 5.
Multivariate analysis showed that high troponin, procalcitonin, and APTT prolongation were significantly more frequently observed in patients with MAS requiring treatment in the PICU (Table 3).
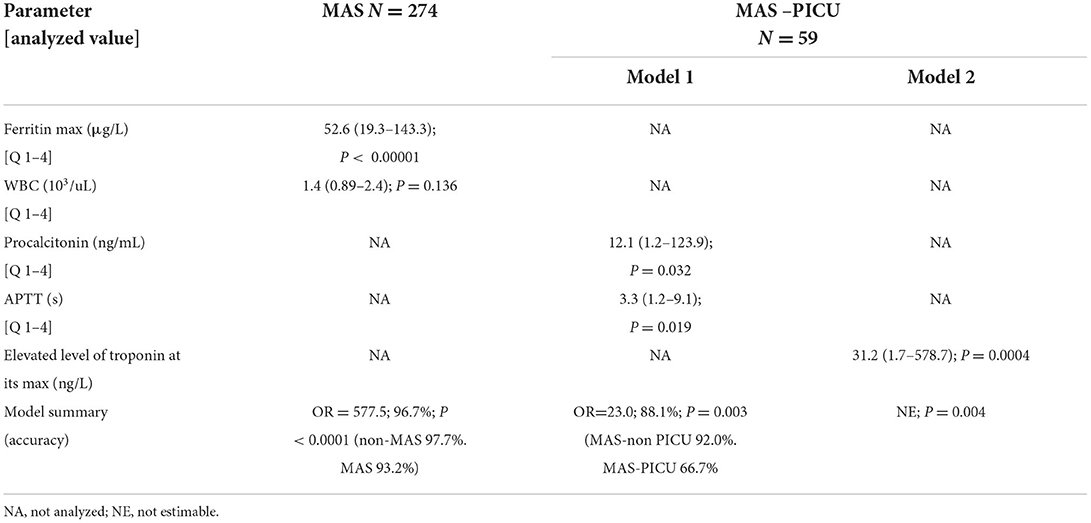
Table 3. Multivariate analysis of the association between laboratory results at respective peaks and the presence of macrophage activation syndrome (MAS) and MAS requiring pediatric intensive care unit (PICU) hospitalization (MAS-PICU) in 274 patients meeting MIS-C criteria.
Various treatment options were used and adjusted to current guidelines (Supplementary Table 6). MIS-C patients fulfilling MAS criteria were treated more often with intravenous immunoglobulins (94.8 vs. 87.6%) and steroids (87.3 vs. 62.7%) than children without MAS. Children with MAS more often required mechanical ventilation (10.9 vs. 1.9%). No significant differences in such treatment when comparing groups of children with MAS only vs. those hospitalized in PICU were found. None of the patients required biologic agents. Therapeutic heparin was used mainly in PICU. The duration of hospitalization was longer in MAS patients, especially those admitted to PICU. No children were treated with extracorporeal membrane oxygenation (ECMO) or renal replacement therapy. Two deaths were reported: one in a severely immunocompromised child and one in a previously healthy teenager with fulminant multiorgan dysfunction, with positive RT-PCR results for SARS-CoV-2. None of these patients fulfilled MAS criteria. Multivariate analysis of the influence of therapy on MAS, MAS-PICU, and the outcome showed that MAS alone is associated with incomplete recovery at discharge (Table 4; Supplementary Table 6).
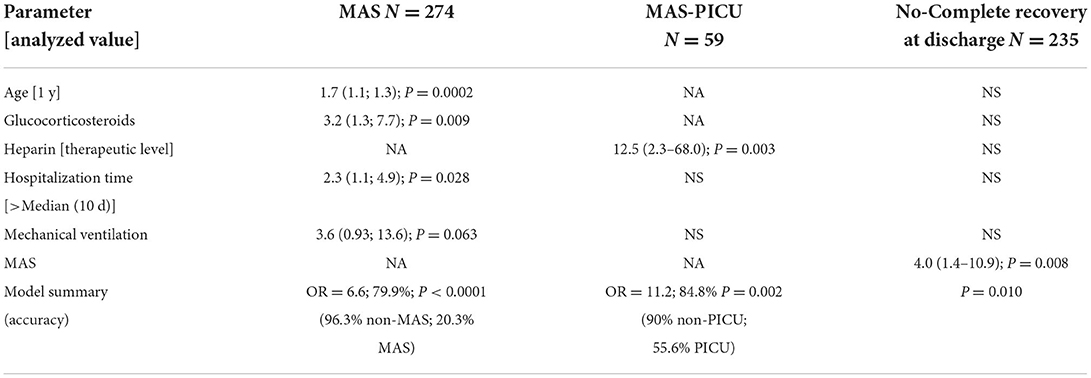
Table 4. Multivariable analysis of the influence of therapy on the presence of macrophage activation syndrome (MAS), MAS requiring pediatric intensive care unit hospitalization (MAS-PICU), and outcome in 274 patients meeting MIS-C criteria.
Our study is one of the few published to date focusing on MAS in MIS-C patients. We found that 21% of MIS-C patients fulfilled 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis. Nevertheless, the outcome of MAS was less severe than we tend to observe in rheumatologic diseases, without requiring more immunomodulating treatment than recommended for MIS-C or PICU management. We have identified some indicators of MAS in MIS-C, such as symptoms characteristic of atypical KD, age within 5–12 years, skin erosion, and highly elevated inflammatory parameters and troponin levels. The overall clinical course and prognosis of MAS in MIS-C were better than expected based on the current knowledge on MAS complicating s-JIA, KD, or other rheumatological disorders. It suggests that these criteria might not apply to MIS-C.
There are several well-described phenotypes of MIS-C. Godfred-Cato et al. distinguished three non-exclusive categories of patients within MIS-C based on latent class analysis: Class 1 (named true” or classic MIS-C) with the highest degree of organ involvement and higher prevalence of shock and lymphopenia, with a little overlap with patients with KD; Class 2 (“acute COVID”) with the predominant respiratory symptoms and more common SARS-CoV-2 positivity by RT-PCR; and Class 3 (“KD-like”), with a phenotype similar to that of pre-pandemic KD (43–45). Rowley et al. confirmed different MIS-C phenotypes and underlined the need for basic science investigations into the host immune response to understand the pathogenesis of these (perhaps different) syndromes (44).
HLH and MAS are not discrete diseases but represent a continuum of hemophagocytic conditions that share a common pathway of impaired cytotoxicity leading to cytokine storm (46). Cytokine excess, particularly IL-18 and IFN-γ, is a common feature of HLH, MAS, and MIS-C. In our study, none of the children met the HLH-2004 criteria. HLH-2004 verification was biased by unavailable results of sCD25 level and NK cell count, which could influence our results. Another explanation of this finding could be immunopathological differences between these entities. A ratio of total IL-18/CXCL9 (C-X-C Motif Chemokine Ligand 9) has been used to differentiate patients with rheumatologic diseases and MAS from patients with HLH (47, 48). The levels of IL-18 reflect inflammasome activation, and CXCL9 indicates interferon-γ pathway activity. There is an impairment of granule-mediated cytotoxicity of natural killer (NK) cells in HLH. In MIS-C, the cytokine storm is linked mostly to INF-γ, which could explain a less severe disease course.
The amplitude of T cell activation and Th1 cytokines is higher in HLH versus MIS-C (48, 49). However, this comparison is of limited value, as it concerned primary HLH or EBV infection-associated HLH that fulfilled HLH-2004 diagnostic criteria, intended primarily for genetically conditioned HLH. MIS-C and HLH also differ in some clinical symptoms, such as cardiac dysfunction and gastrointestinal manifestation, which are typical for MIS-C but usually not in HLH. In addition, although low fibrinogen is a hallmark of HLH and MAS, we found a high level of fibrinogen (together with higher procalcitonin and ferritin) predictive of MAS criteria fulfillment. Considering all the above, we consider HLH-2004 criteria as suboptimal for MAS diagnosis in MIS-C.
Current data suggest distinct clinical features and laboratory differences between MIS-C and MAS (17, 50–54). The studies comparing MIS-C and MAS during s-JIA are restricted by small sample sizes (17, 52, 53). The cardiac, gastrointestinal, and neurological involvements and myalgia were more pronounced in MIS-C. In contrast to the poor prognosis of MAS in s-JIA, in our study, no deaths were reported in patients with MAS-MIS-C. Cytokine-targeting therapy is crucial in controlling hyperinflammation and is used widely in patients with MAS in children with s-JIA. Aggressive treatment is also suggested in patients with MIS-C and MAS, for example, a combination of IVIG plus pulses of methylprednisolone plus anakinra (55). None of the children in our group required such treatment. Children with MIS-C and MAS definitions' fulfillment were treated more often with intravenous immunoglobulins (94.8 vs. 87.6%) and steroids (87.3 vs. 62.7%). This finding is consistent with previous studies. Verdoni et al. diagnosed MAS according to 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis in five (50%) of ten patients with Kawasaki-like disease after the beginning of the SARS-CoV-2 epidemic. All patients were treated with IVIG and methylprednisolone with good clinical response. Two of them required inotropic agents (2). In our group, children diagnosed with MAS more often required mechanical ventilation (10.9 vs. 1.9%). The duration of hospitalization was longer in MIS-C and MAS patients, especially those admitted to PICU; 15% of children with MIS-C and MAS required PICU, while in other secondary hemophagocytic syndromes, the percentage of ICU patients reaches 38% (18, 30). Such difference indicates that MAS in MIS-C has a milder course. It may also be related to the more favorable course of MIS-C in the Polish population - a significantly lower percentage of hospitalizations in PICU was demonstrated (8%) than in reports from Western countries (60–80%), as shown in previous studies (5, 21). In addition, the nationwide MIS-C register and the high awareness of physicians, and thus early treatment, may also contribute to a better prognosis of patients with MAS during MIS-C. However, similar conclusions were reached by Otar et al., who found that patients with MIS-C had shorter hospitalization times than children with s-JIA-MAS. At the same time, they required PICU admission for myocarditis more frequently than children with s-JIA-MAS (53). There are also differences in basic laboratory tests. Patients with MIS-C had significantly lower lymphocyte count, higher CRP, erythrocyte sedimentation rate, and B-type natriuretic peptide levels. Moreover, ferritin concentration is elevated in MIS-C relative to healthy children, higher than in patients with KD but not as high as in patients with MAS complicating other diseases (17, 54).
The cytokine storm reflected in the laboratory findings of patients with MIS-C resembles MAS. However, differences in the degree of elevation of markers such as ferritin, IL-18, and CXCL9 suggest that the pathogenic cytokines in MIS-C differ from those driving MAS (17, 53). It is hypothesized that MIS-C resembles a more likely clinical state named pre-MAS (52). Based on cytokine profiles of children with MIS-C, Esteve-Sole A et al. proposed a more severe form of MIS-C (named MIS-C plus), closer to MAS both clinically and laboratory — related to higher IFN-γ levels (51). Five patients with MIS-C who had multiorgan involvement had higher levels of IFN-γ, IL-18, GM-CSF, RANTES, IP-10/CXCL10, IL-1α, and SDF-1. Authors conclude that such a cytokine profile might be an early sign of MAS.
On the other hand, MAS is not a specific diagnosis but a continuum of severity within MIS-C. Gurlevik et al. assessed the cytokine and chemokine profiles of children with MIS-C. They classified MIS-C patients into those with MAS and without MAS according to laboratory and clinical features of patients. They found that 13 (41.9%) of 31 MIS-C patients fulfilled 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis. Patients with MIS-C that met MAS criteria had higher levels of IL-17A and IFN-γ than those who did not fulfill the criteria; however, it was not statistically significant (40). Rodriguez-Smith et al. reported that eight (42%) of 19 patients with MIS-C who met MAS criteria (also based on 2016 MAS classification) had significantly higher CXCL9 concentration than patients with MIS-C without MAS. They conclude that the stratification of patients with MIS-C by high or low CXCL9 concentration supports MAS-like pathophysiology in patients with severe MIS-C. This finding might lead to a new approach to its diagnosis or management (41).
All these findings suggest that the MAS classification criteria used in MIS-C could correspond to a cytokine storm linked to IFN-γ (as in s-JIA). However, we think that they might still be non-specific. Based on further studies comparing MAS complicating s-JIA vs. MIS-C in the immunological and clinical context, the development and validation of the new definition and clinical criteria for identifying MAS in MIS-C might be required in further studies.
Our study has some limitations. The main one is the small patient population; however, to the best of our knowledge, this is the first study to evaluate and compare the clinical and laboratory characteristics of patients with MIS-C complicated by MAS in a larger cohort based on a multicenter registry. The minimal number of patients admitted to PICU limits the reliability of its risk factors assessment within patients with MAS in MIS-C. Moreover, we did not analyze the subgroup of patients with MIS-C (according to Godfred-Cato S et al. classification) but the whole group with different phenotypes. It would be interesting to classify the patients with MIS-C based on functional studies (INF-γ pathway) and specific cytokine profiles and to analyze these subgroups.
The existing HLH and MAS diagnostic criteria do not address MIS-C. The 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis are easy to apply and help indicate children with a greater risk for more aggressive treatment requirements (including mechanical ventilation). In addition to the well-known signs of MAS (of which laboratory signs are the most prominent), we found that in patients with MIS-C, older age, atypical KD phenotype, and skin erosions are significant factors indicating risk for MAS. Highly elevated inflammatory parameters indicate MAS in children with MIS-C, and elevated troponin levels are predominantly a predictive factor for children with MAS requiring PICU hospitalization. The clinical course of MAS in MIS-C is milder, prognosis better, and treatment less aggressive than in MAS in the course of other diseases, including rheumatologic ones. However, MAS should be regarded not as a specific diagnosis but as a continuum of severity within MIS-C. Further studies are needed to define various aspects of MIS-C better and stratify it according to its severity. Further immunological profiling is required and could serve to choose optimal, individualized treatment.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethical approval was obtained from the Bioethics Committee at the Wrocław Medical University (CWN UMW BW: 313/2020). Komisja Bioetyczna przy Uniwersytecie Medycznym we Wrocławiu 50-367 Wrocław, ul. J.Mikulicza-Radeckiego 4a tel.: 71 784 10 14, 71 784 17 10. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
PB: conceptualization, methodology, validation, formal analysis, writing—original draft preparation, review, editing, visualization, supervision, and project administration. ES and DJ-L: methodology, validation, formal analysis, resources, software, data curation, writing—original draft preparation, review, editing, visualization, and supervision. EC: writing—original draft preparation. EG: methodology, formal analysis, and visualization. KL: methodology, resources, data curation, writing—original draft preparation, review, and editing, LS: resources, data curation, and writing—review and editing. MO-N and EK: resources, data curation, and methodology. JK: methodology, validation, formal analysis, visualization, and supervision. All authors contributed to the article and approved the submitted version.
We would like to thank the MOIS-CoR Study Group and all doctors who provided data for the Polish MIS-C Registry. We would also like to thank Aleksandra Tracewska for proofreading.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.981711/full#supplementary-material
1. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
2. Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the Italian epicenter of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. (2020) 395:1771–8. doi: 10.1016/S0140-6736(20)31103-X
3. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. (2020) 324:259–69. doi: 10.1001/jama.2020.10369
4. Davies P, Evans C, Kanthimathinathan HK, Lillie J, Brierley J, Waters G, et al. Intensive care admissions of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Heal. (2020) 4:669–77. doi: 10.1016/S2352-4642(20)30215-7
5. Okarska-Napierała M, Ludwikowska KM, Szenborn L, Dudek N, Mania A, Buda P, et al. pediatric inflammatory multisystem syndrome (pims) did occur in poland during months with low COVID-19 prevalence, preliminary results of a nationwide register. J Clin Med. (2020) 9:3386. doi: 10.3390/jcm9113386
6. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF. et al. Multisystem inflammatory syndrome in us children and Adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
7. Belay ED, Abrams J, Oster ME, Giovanni J, Pierce T, Meng L, et al. Trends in geographic and temporal distribution of us children with multisystem inflammatory syndrome during the covid-19 pandemic. JAMA Pediatr. (2021) 175:837–45. doi: 10.1001/jamapediatrics.2021.0630
8. Cheng MH, Zhang S, Porritt RA, Noval Rivas M, Paschold L, et al. Superantigenic character of an insert unique to SARS-CoV-2 spike supported by skewed TCR repertoire in patients with hyperinflammation. Proc Natl Acad Sci U S A. (2020) 117:25254–62. doi: 10.1073/pnas.2010722117
9. Sacco K, Castagnoli R, Vakkilainen S, Liu C, Delmonte OM, Oguz C, et al. Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19. Nat Med. (2022) 28:1050–62. doi: 10.1038/s41591-022-01724-3
10. Gruber CN, Patel RS, Trachtman R, Lepow L, Amanat F, Krammer F, et al. Mapping systemic inflammation and antibody responses in multisystem inflammatory syndrome in children (MIS-C). Cell. (2020) 183:982-95.e14. doi: 10.1016/j.cell.2020.09.034
11. Martinez OM, Bridges ND, Goldmuntz E, Pascual V. The immune roadmap for understanding multi-system inflammatory syndrome in children: opportunities and challenges. Nat Med. (2020) 26:1819–24. doi: 10.1038/s41591-020-1140-9
12. Vella LA, Giles JR, Baxter AE, Oldridge DA, Diorio C, Kuri-Cervantes L, et al. Deep immune profiling of MIS-C demonstrates marked but transient immune activation compared to adult and pediatric COVID-19. Sci Immunol. (2021) 6:eabf7570. doi: 10.1126/sciimmunol.abf7570
13. Yonker LM, Gilboa T, Ogata AF, Senussi Y, Lazarovits R, Boribong BP, et al. Multisystem inflammatory syndrome in children is driven by zonulin-dependent loss of gut mucosal barrier. J Clin Invest. (2021) 131:e149633. doi: 10.1172/JCI149633
14. Consiglio CR, Cotugno N, Sardh F, Pou C, Amodio D, Rodriguez L, et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell. (2020) 183:968-81.e7. doi: 10.1016/j.cell.2020.09.016
15. Ramaswamy A, Brodsky NN, Sumida TS, Comi M, Asashima H, Hoehn KB, et al. Immune dysregulation and autoreactivity correlate with disease severity in SARS-CoV-2-associated multisystem inflammatory syndrome in children. Immunity. (2021) 54:1083-95.e7. doi: 10.1016/j.immuni.2021.04.003
16. Carter MJ, Fish M, Jennings A, Doores KJ, Wellman P, Seow J, et al. Peripheral immunophenotypes in children with multisystem inflammatory syndrome associated with SARS-CoV-2 infection. Nat Med. (2020) 26:1701–7. doi: 10.1038/s41591-020-1054-6
17. Lee PY, Day-Lewis M, Henderson LA, Friedman KG, Lo J, Roberts JE, et al. Distinct clinical and immunological features of SARS-CoV-2-induced multisystem inflammatory syndrome in children. J Clin Invest. (2020) 130:5942–50. doi: 10.1172/JCI141113
18. Sancho-Shimizu V, Brodin P, Cobat A, Biggs CM, Toubiana J, Lucas CL, et al. SARS-CoV-2-related MIS-C: a key to the viral and genetic causes of Kawasaki disease? J Exp Med. (2021) 218:e20210446. doi: 10.1084/jem.20210446
19. Brodin P. SARS-CoV-2 infections in children: Understanding diverse outcomes. Immunity. (2022) 55:201–9. doi: 10.1016/j.immuni.2022.01.014
20. Diorio C, Shraim R, Vella LA, Giles JR, Baxter AE, Oldridge DA, et al. Proteomic profiling of MIS-C patients indicates heterogeneity relating to interferon gamma dysregulation and vascular endothelial dysfunction. Nat Commun. (2021) 12:7222. doi: 10.1038/s41467-021-27544-6
21. Harwood R, Allin B, Jones CE, Whittaker E, Ramnarayan P, Ramanan AV, et al. A national consensus management pathway for pediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): results of a national Delphi process. Lancet Child Adolesc Heal. (2021) 5:133–41. doi: 10.1016/S2352-4642(20)30304-7
22. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American College of Rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: Version 1. Arthritis Rheumatol. (2020) 72:1791–805. doi: 10.1002/art.41454
23. Royal college of paediatrics and child health. Royal College of Paediatrics and Child Health. Guidance - Paediatric Multisystem Inflammatory Syndrome Temporally Associated With COVID-19 (PIMS). London: Royal College of Paediatrics and Child Health. (2020).
24. Centers for Disease Control Prevention. Information for Healthcare Providers About Multisystem Inflammatory Syndrome in Children (MIS-C). (2020). Available online at: https://www.cdc.gov/mis-c/hcp/
25. Okarska-Napierała M, Ludwikowska K, Jackowska T, Ksiazyk J, Buda P, Mazur A, et al. Approach to a child with multisystem inflammatory syndrome associated with COVID19. Recommendations by the Polish pediatric society expert group. Update – February 2021. Pediatr Pol. (2021) 96:121-8. doi: 10.5114/polp.2021.107395
26. Belhadjer Z, Méot M, Bajolle F, Khraiche D, Legendre A, Abakka S, et al. Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 PAndemic. circulation. (2020) 142:429–36. doi: 10.1161/CIRCULATIONAHA.120.048360
27. Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. (2002) 14:548–52. doi: 10.1097/00002281-200209000-00012
28. García-Pavón S, Yamazaki-Nakashimada MA, Báez M, Borjas-Aguilar KL, Murata C. Kawasaki disease complicated with macrophage activation syndrome: a systematic review. J Pediatr Hematol Oncol. (2017) 39:445–51. doi: 10.1097/MPH.0000000000000872
29. Agrawal S, Thapa Karki S, Paudel KP, Shrestha AK, Adhikari BN. A case report of macrophage activation syndrome complicating multisystem inflammatory syndrome in children associated with COVID-19: a diagnostic challenge. Clin Pediatr (Phila). (2022) 61:104–6. doi: 10.1177/00099228211040381
30. Avcin T, Tse SM, Schneider R, Ngan B, Silverman ED. Macrophage activation syndrome as the presenting manifestation of rheumatic diseases in childhood. J Pediatr. (2006) 148:683–6. doi: 10.1016/j.jpeds.2005.12.070
31. Ramanan AV, Rosenblum ND, Feldman BM, Laxer RM, Schneider R. Favorable outcome in patients with renal involvement complicating macrophage activation syndrome in systemic onset juvenile rheumatoid arthritis. J Rheumatol. (2004) 31:2068–70. Available online at: https://www.jrheum.org/content/jrheum/31/10/2068.full.pdf
32. Saez-de-Ocariz M, Gámez-González LB, Rivas-Larrauri F, Castaño-Jaramillo LM, Toledo-Salinas C, Garrido-García LM, et al. Kawasaki disease mimickers. Pediatr Int. (2021) 63:880-8. doi: 10.1111/ped.14561
33. Ravelli A, Minoia F, Davì S, Horne A, Bovis F, Pistorio A, et al. 2016 classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Ann Rheum Dis. (2016) 75:481–9. doi: 10.1136/annrheumdis-2015-208982
34. Bennett TD, Fluchel M, Hersh AO, Hayward KN, Hersh AL, Brogan TV, et al. Macrophage activation syndrome in children with systemic lupus erythematosus and children with juvenile idiopathic arthritis. Arthritis Rheum. (2012) 64:4135–42. doi: 10.1002/art.34661
35. Janka GE, Lehmberg K. Hemophagocytic syndromes-an update. Blood Rev. (2014) 28:135–42. doi: 10.1016/j.blre.2014.03.002
36. Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. (2007) 48:124–31. doi: 10.1002/pbc.21039
37. Buda P, Gietka P, Ksiazyk JB, Machaczka M. The influence of various therapeutic regimens on early clinical and laboratory response and outcome of children with secondary hemophagocytic lymphohistiocytosis. Arch Med Sci. (2018) 14:138–50. doi: 10.5114/aoms.2015.56325
38. Davì S, Minoia F, Pistorio A, Horne A, Consolaro A, Rosina S, et al. Performance of current guidelines for diagnosis of macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Arthritis Rheumatol. (2014) 66:2871–80. doi: 10.1002/art.38769
39. Wang W, Gong F, Zhu W, Fu S, Zhang Q. Macrophage activation syndrome in Kawasaki disease: more common than we thought? Semin Arthritis Rheum. (2015) 44:405–10. doi: 10.1016/j.semarthrit.2014.07.007
40. Gurlevik SL, Ozsurekci Y, Sag E, Derin Oygar P, Kesici S, Akca ÜK, et al. The difference of the inflammatory milieu in MIS-C and severe COVID-19. Pediatr Res. (2022) 29:1–10. doi: 10.1038/s41390-022-02029-4
41. Rodriguez-Smith JJ, Verweyen EL, Clay GM, Esteban YM, de Loizaga SR, Baker EJ, et al. Inflammatory biomarkers in COVID-19-associated multisystem inflammatory syndrome in children, Kawasaki disease, and macrophage activation syndrome: a cohort study. Lancet Rheumatol. (2021) 3:e574–84. doi: 10.1016/S2665-9913(21)00139-9
42. Ludwikowska KM, Okarska-Napierała M, Dudek N, Tracewski P, Kusa J, Piwoński KP, et al. Distinct characteristics of multisystem inflammatory syndrome in children in Poland. Sci Rep. (2021) 11:23562. doi: 10.1038/s41598-021-02669-2
43. Godfred-Cato S, Bryant B, Leung J, Oster ME, Conklin L, Abrams J, et al. COVID-19-associated multisystem inflammatory syndrome in children - United States, March-July 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:1074–80. doi: 10.15585/mmwr.mm6932e2
44. Rowley AH, Shulman ST, Arditi M. Immune pathogenesis of COVID-19-related multisystem inflammatory syndrome in children. J Clin Invest. (2020) 130:5619–21. doi: 10.1172/JCI143840
45. Flood J, Shingleton J, Bennett E, Walker B, Amin-Chowdhury Z, Oligbu G, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS): Prospective, national surveillance, United Kingdom and Ireland, 2020. Lancet Reg Health Eur. (2021) 3:100075. doi: 10.1016/j.lanepe.2021.100075
46. Halyabar O, Chang MH, Schoettler ML, Schwartz MA, Baris EH, Benson LA, et al. Calm in the midst of cytokine storm: a collaborative approach to the diagnosis and treatment of hemophagocytic lymphohistiocytosis and macrophage activation syndrome. Pediatr Rheumatol Online J. (2019) 17:7. doi: 10.1186/s12969-019-0309-6
47. Weiss ES, Girard-Guyonvarc'h C, Holzinger D, de Jesus AA, Tariq Z, Picarsic J, et al. Interleukin-18 diagnostically distinguishes and pathogenically promotes human and murine macrophage activation syndrome. Blood. (2018) 131:1442–55. doi: 10.1182/blood-2017-12-820852
48. Canna SW, Marsh RA. Pediatric hemophagocytic lymphohistiocytosis. Blood. (2020) 135:1332–43. doi: 10.1182/blood.2019000936
49. Kumar D, Rostad CA, Jaggi P, Villacis Nunez DS, Chengyu Prince, Lu A, et al. Distinguishing immune activation and inflammatory signatures of multisystem inflammatory syndrome in children (MIS-C) vs. hemophagocytic lymphohistiocytosis. J Allergy Clin Immunol. (2022) 149:1592–606.e16. doi: 10.1016/j.jaci.2022.02.028
50. Poniecka A, Smolewska E. A fine line between macrophage activation syndrome and multisystem inflammatory syndrome in children - literature review based on two case reports. Reumatologia. (2021) 59:47–57. doi: 10.5114/reum.2021.102871
51. Esteve-Sole A, Anton J, Pino-Ramirez RM, Sanchez-Manubens J, Fumadó V, Fortuny C, et al. Similarities and differences between the immunopathogenesis of COVID-19-related pediatric multisystem inflammatory syndrome and Kawasaki disease. J Clin Invest. (2021) 131:e144554. doi: 10.1172/JCI144554
52. Aydin F, Çelikel E, Ekici Tekin Z, Coşkun S, Sezer M, Karagöl C, et al. Comparison of baseline laboratory findings of macrophage activation syndrome complicating systemic juvenile idiopathic arthritis and multisystem inflammatory syndrome in children. Int J Rheum Dis. (2021) 24:542–7. doi: 10.1111/1756-185X.14078
53. Otar Yener G, Paç Kisaarslan A, Ulu K, Atalay E, Haşlak F, Özdel S, et al. Differences and similarities of multisystem inflammatory syndrome in children, Kawasaki disease and macrophage activating syndrome due to systemic juvenile idiopathic arthritis: a comparative study. Rheumatol Int. (2022) 42:879–89. doi: 10.1007/s00296-021-04980-7
54. Bohn MK, Yousef P, Steele S, Sepiashvili L, Adeli K. MultiInflammatory syndrome in children: a view into immune pathogenesis from a laboratory perspective. J Appl Lab Med. (2022) 7:311–21. doi: 10.1093/jalm/jfab114
Keywords: macrophage activation syndrome, MAS, SARS-CoV-2, pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS), PIMS-TS, multisystem inflammatory syndrome in children (MIS-C), MIS-C, Kawasaki disease (KD)
Citation: Buda P, Strauss E, Januszkiewicz-Lewandowska D, Czerwinska E, Ludwikowska K, Szenborn L, Gowin E, Okarska-Napierała M, Kuchar E and Ksia̧zyk J (2022) Clinical characteristics of children with MIS-C fulfilling classification criteria for macrophage activation syndrome. Front. Pediatr. 10:981711. doi: 10.3389/fped.2022.981711
Received: 29 June 2022; Accepted: 17 August 2022;
Published: 15 September 2022.
Edited by:
Alla Volokha, Shupyk National Medical Academy of Postgraduate Education, UkraineReviewed by:
Claudia Bracaglia, IRCCS Ospedale Pediatrico Bambino Gesù, ItalyCopyright © 2022 Buda, Strauss, Januszkiewicz-Lewandowska, Czerwinska, Ludwikowska, Szenborn, Gowin, Okarska-Napierała, Kuchar and Ksia̧zyk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Piotr Buda, cC5idWRhQGlwY3pkLnBs
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.