 Chengcheng Gao
Chengcheng Gao Qi Qian2
Qi Qian2 Zhongxiang Ding
Zhongxiang Ding- 1Department of Radiology, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, Hangzhou, China
- 2Department of Radiology, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
- 3Center for Rehabilitation Medicine, Department of Radiology, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, China
- 4Key Laboratory of Clinical Cancer Pharmacology and Toxicology Research of Zhejiang Province, Hangzhou, China
Background: Bone age assessment (BAA) is an essential tool utilized in outpatient pediatric clinics. Three major BAA methods, Greulich–Pyle (GP), Tanner–Whitehouse 3 (TW3), and China 05 RUS–CHN (RUS–CHN), were applied to comprehensively compare bone age (BA) and chronological age (CA) in a Chinese sample of preschool children. This study was designed to determine the most reliable method.
Methods: The BAA sample consisted of 207 females and 183 males aged 3–6 years from the Zhejiang Province in China. The radiographs were estimated according to the GP, TW3, and RUS–CHN methods by two pediatric radiologists. The data was analyzed statistically using boxplots, the Wilcoxon rank test, and Student’s t-test to explore the difference (D) between BA and CA.
Results: According to the distributions of D, the boxplots showed that the median D of the TW3 method was close to zero for both male and female subjects. The TW3 and RUS–CHN methods overestimated the age of both genders. The TW3 method had the highest correct classification rate for males but a similar rate for females. The GP method did not show any significant difference between the BA and CA when applied to 3-year-old males and 4-year-old females while the TW3 method showed similar results when applied to 6-year-old females. The RUS–CHN method showed the least consistent results among the three methods.
Conclusion: The TW3 method was superior to the GP and RUS–CHN methods but not reliable on its own. It should be noted that a precise age diagnosis for preschool children cannot be easily made if only one of the methods is utilized. Therefore, it is advantageous to combine multiple methods when assessing bone age.
Introduction
The bone age assessment (BAA) is a commonly used procedure in pediatric clinics, including subspecialties such as Endocrinology and Orthopedics (1–3). Bone age (BA) is the primary indicator of maturity status in a child, as various diseases affecting growth can result in a significant discrepancy between bone age and chronological age (CA) (3–6). Therefore, choosing a reliable BAA method for clinic use is essential.
Three major BAA methods are currently applied in Chinese pediatric practices: the Greulich–Pyle (GP) method (7), the Tanner–Whitehouse 3 (TW3) method (8), and the China 05 RUS–CHN (RUS–CHN) method (9). All three methods can be used to assess the development during early and middle childhood, both of which are the stages of rapid growth.
Recently, the performance of a specific BAA method applied in populations from different age groups has been analyzed and reported extensively (2, 10, 11). However, only a few comprehensive studies have used three different BAA methods to correlate results among preschool children. The study aimed to compare the performance of the GP, TW3, and RUS–CHN methods for BAA in a subgroup of Chinese preschool children.
Materials and methods
Data acquisition
We selected 390 left hand-wrist radiographs from the Third Affiliated Hospital of Zhejiang Chinese Medicine University (Hangzhou, China) from January 2019 to August 2021. Radiographs were obtained from the picture archive and communication systems. The subjects resided in the Zhejiang Province and had no remarkable medical history of genetic syndrome or trauma. A total of 390 subjects, consisting of 207 females and 183 males aged 3–6 years, were included in this study (Figure 1).
Figure 1. Flowchart of sample selection process.
Each radiograph for BAA could be evaluated using the following three methods: (i) the GP method comparing a hand-wrist radiograph of a child with the standard films applied in the age-matched atlas, published in 1959 (7); (ii) the TW3 method scoring the skeletal maturity for each hand and wrist bone, published in 2001 (8); (iii) the RUS–CHN method analyzing the skeletal development standards of hand and wrist for children in China, version 05–I, published in 2006 (12).
The skeletal age was analyzed independently for each of the radiographs based on the different assessment methods described above. In order to assess the interobserver error, two pediatric radiologists with extensive training and experience in BAA assessed the radiographs. The differences in the results were not significant, and the average value was considered as the BA.
To compare the difference in performance between the three methods applied in this study, the difference (D) between the CA and BA was calculated (D = CA - BA). Specifically, D represented the underestimation (positive value) or overestimation (negative value).
The Ds of underestimation, overestimation, and correct classifications were determined separately, based on the classification of age measured by CA ± 3 months. Therefore, children whose predicted BA was within CA ± 3 months were considered to be classified appropriately. The two main reasons for assuming this span of age are as follows: (i) the age span predicted using the GP method is in intervals of approximately 6 months (e.g., 3 years, 3 years and 6 months, 4 years and 2 months) (7); (ii) age ± 3 months is regarded as the smallest range for BAA, as assessed by left hand-wrist X-rays (13).
In China, children are enrolled in school at the age of 7 years (14, 15), which is the threshold for BAA. Thus, three different methods have been studied in the sample of children aged 3.01–year–old to 6.99–year–old.
Data analysis
Data was analyzed using the SPSS statistical software (version 25.0, SPSS, Inc., Chicago, IL, United States). Paired Student’s t-test was used to compare CA with BA computed by the GP, TW3, and RUS–CHN methods for the cohort stratified by gender at each age point. Frequency tests were carried out to analyze the correlation between CA and the discrepancy between CA and BA for at least 3 months. Then, two tests of the hypothesis were used to assess the correlation between CA and BA. A p-value < 0.05 was deemed significant in all tests.
Results
Accuracy of the three methods
In the boxplots, the distributions of the D between CA and BA were represented compactly. According to Figure 2, the median D of the TW3 method is close to zero for male (−0.39) and female (−0.40) subjects. In addition, the variability of TW3 in the boxplots was smaller than that of GP and RUS–CHN.
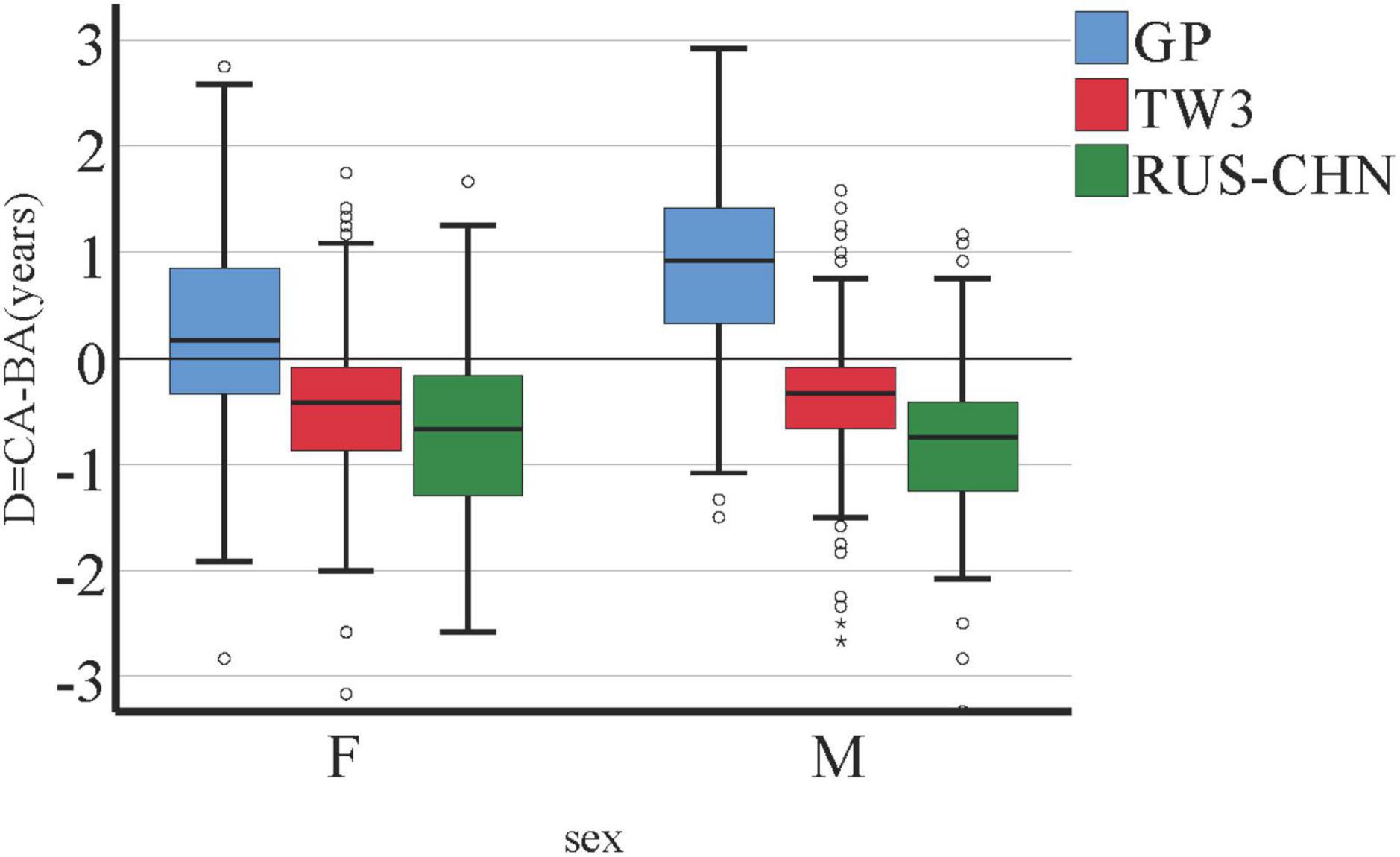
Figure 2. Boxplots of D = CA (chronological age) - BA (bone age), by sex.
In Figure 3, boxplots were separated by age (3–6 years). Evidently, TW3 and RUS–CHN overestimated the age of both male and female subjects, regardless of age. On the other hand, the D in GP might be affected by the age of the individuals (especially in males), with an escalating trend from the age of 3 to 6 years (positive values). In GP method, D was more than zero in 4-, 5-, 6-year-old male group and 5-, 6-year-old female group, which means BA was underestimated. And in 3-year-old male group and 3-, 4-year-old female group, BA was overestimated.
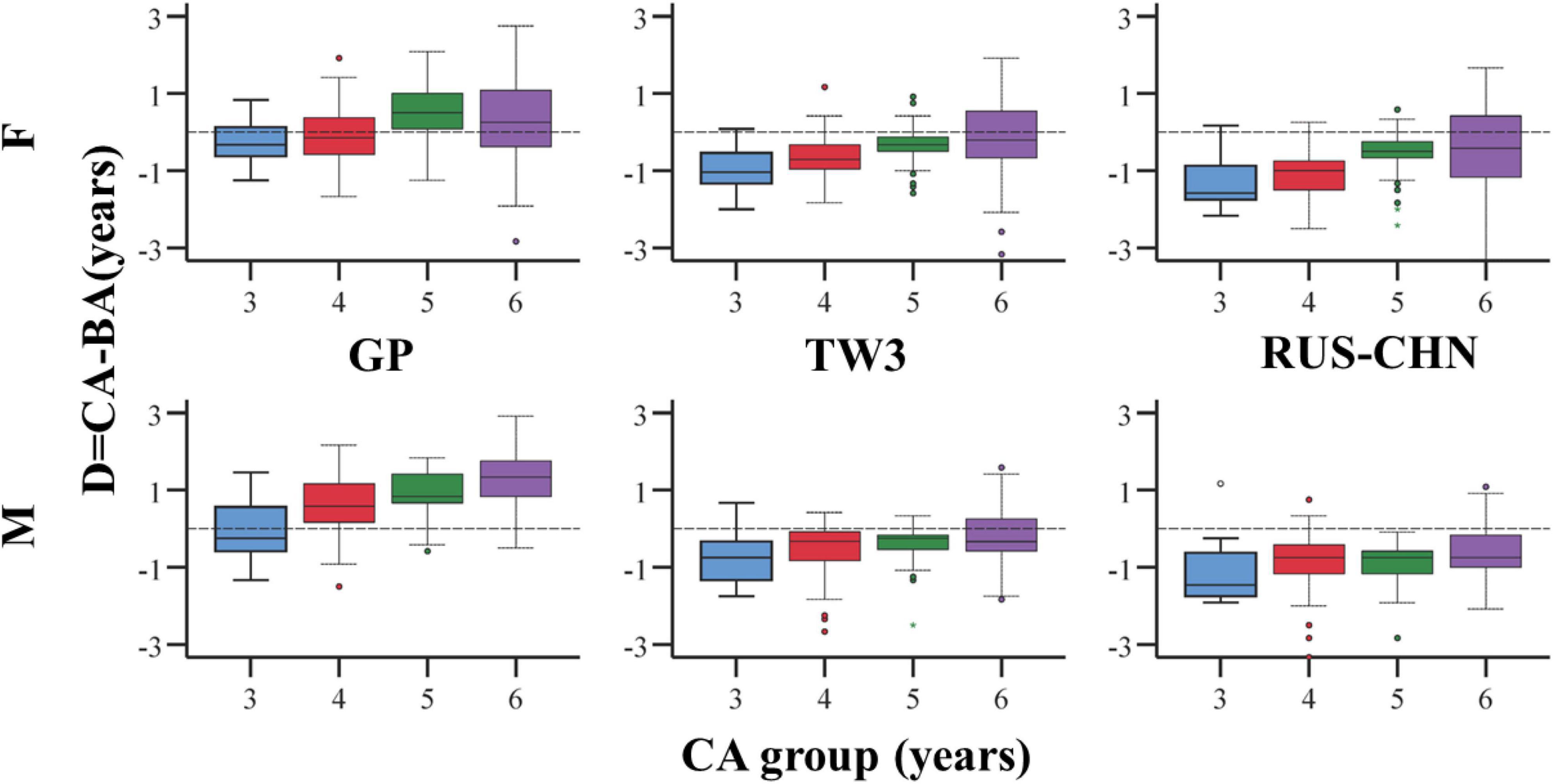
Figure 3. Boxplots of D = CA - BA reported for females (top) and males (bottom) for the three methods and each class of age.
Age prediction
The subsets of subjects with underestimated (under), correctly classified (CC), and overestimated (over) CA regarding CA ± 3 months are summarized in Table 1. Subsequently, the accuracy of these methods in CA prediction was determined.

Table 1. Percentages of subjects with correctly classified (CC), underestimated (under), and overestimated (over) age with respect to the class of CA ± 3 months.
When the D is < 3 months between the CA and BA, indicating that BA is within the range of CA ± 90 days, the correct classification of age was achieved in this study. For males (Table 1), the highest correct classification was achieved using the TW3 method, while for female individuals, the rates of CC in all three methods were similar. Also, it was confirmed that the TW3 and RUS–CHN methods overestimated the age of the subjects (Table 1). Although the percentage of the correct classification in the TW3 method was significantly higher than in the other two methods, it was not a completely reliable result because the accuracy was less than 50%, and that 3-month span was a limited parameter.
Hypothetical test
To further confirm the reliability of the three different BAA methods, we conducted a statistical reasoning process of the mean values of CA and BA. This would determine whether the values varied by the whole sample based on gender (divided by male and female gender) and in an age-dependent manner.
Two types of hypothesis tests were used to compare CA and BA estimated by GP, TW3, and RUS–CHN methods: (i) Wilcoxon signed-rank test was used to evaluate whether the average rank of CA is different from BA. (ii) Student’s t-test was applied to evaluate the significant D in the means of CA and BA.
For both tests, a null hypothesis stated that the two sets (CA and BA) have equal mean ranks. Notably, one difference exists between these two tests: the former is a non-parametric test which does not assume that the population data should be a normal distribution, whereas the latter is a parametric test that assumes the opposite.
In the Q-Q plots for all three BAA methods (Figure 4), the distribution of the difference (D) is close to the normal distribution. This partially proves that the Student’s t-test in this sample is optimal. The Wilcoxon signed-rank test can be adopted.
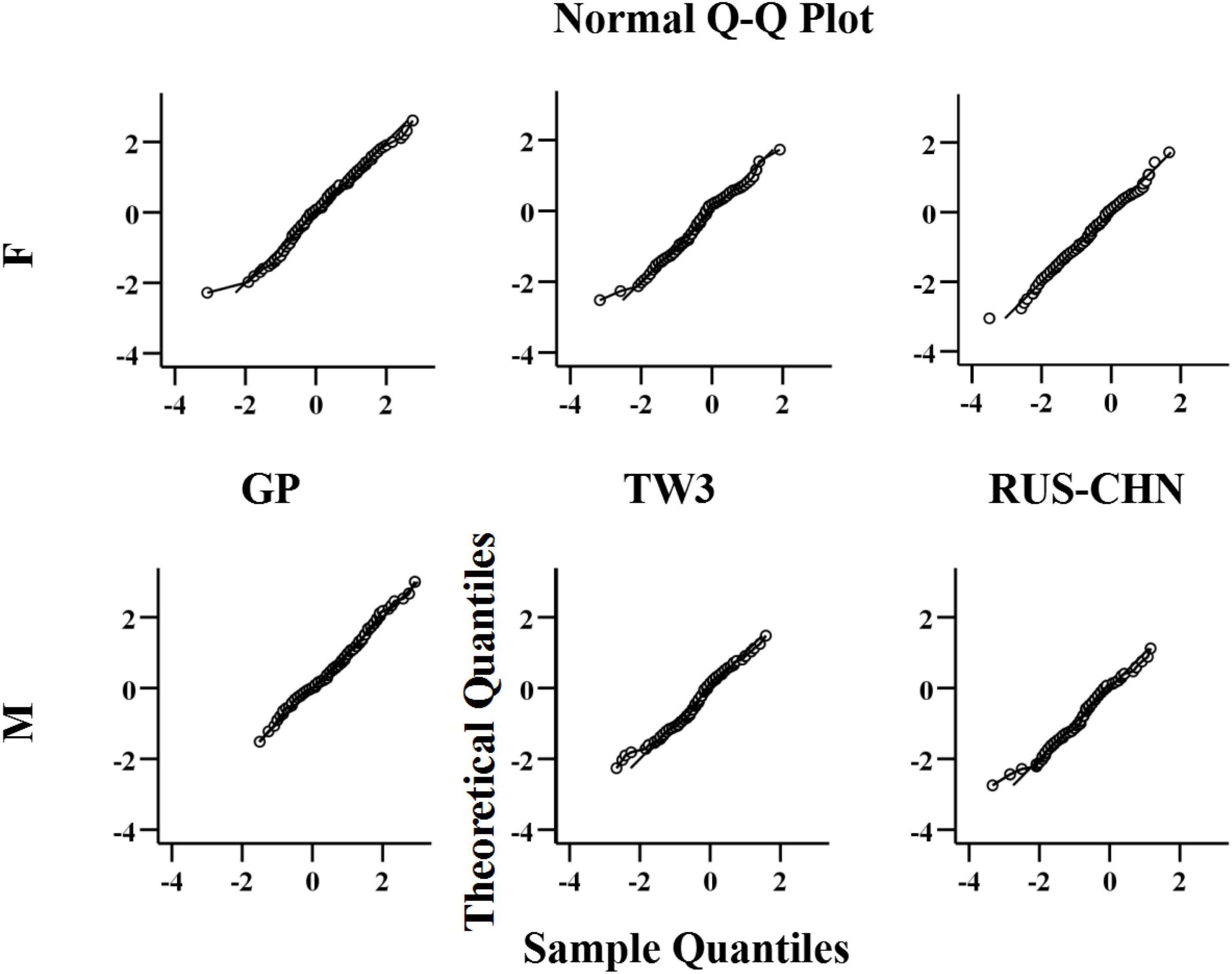
Figure 4. Q-Q plots for D, by sex, for females (top) and males (bottom).
The present study aimed to understand whether any BAA method can evaluate the actual age; it is an optimal indicator when the p-value is > 0.05. The analysis of the age groups revealed similarities between the two test results among the three BAA methods applied to the sample of 183 males and 207 females (p < 0.05). This phenomenon clarified that the Wilcoxon test only accepted the null hypothesis for the 3-year-old male and 4-year-old female groups using the GP method and the 6-year-old female group using the TW3 method. In comparison, the RUS–CHN method was the most unreliable because the tests rejected all the null hypotheses (Table 2).
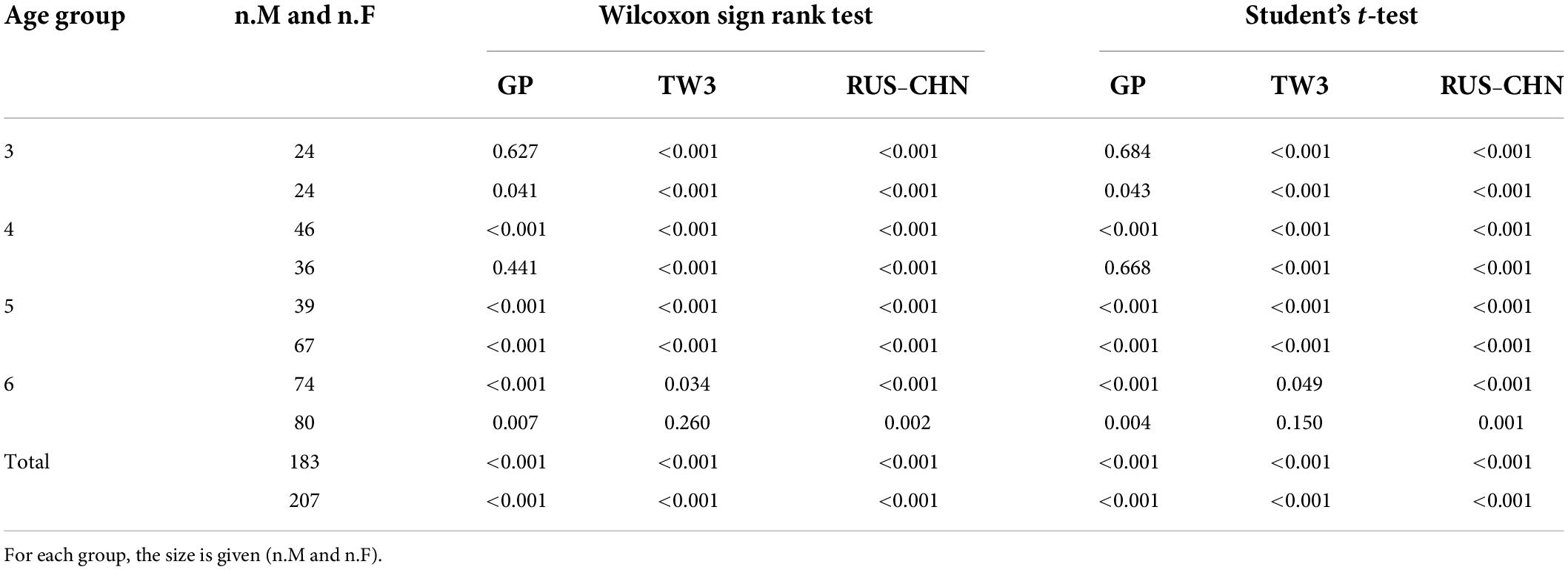
Table 2. P-values for the performed hypothesis tests by sex and age group.
Discussion
Bone age assessment is commonly and widely used in the clinic, reflecting the skeletal maturity, evaluating the growth status, and predicting the future height of children. Although there is an increasing demand for the accurate age estimation of children, studies comparing the reliability of different BAA methods are yet lacking. In China, there are currently a large number of preschool children in the stages of rapid development (ages 3–7). Thus, BAA is of high clinical utility in this population (1, 5, 13, 16–18).
In recent years, studies have reported the inaccuracies of BA predicted by several methods, especially for those under the CA of 7 years (6, 19). The GP method was developed using data from American children in Ohio in the 1950s who belonged to reasonably comfortable families with no medical conditions. This method is simple and easy to implement to determine the BA from 0 to 18 years (7). The original sample for the TW3 method was obtained from a group of healthy British children (8). The TW3 method is time-consuming and complex and thus might require four times longer duration than the GP method. The first sample group consisted of healthy children from upper-middle-class families in the late 1980s (9). The RUS–CHN method was re-assigned for wrist bone morphology according to the classification of the TW series. The different functions and results of the three methods are discussed separately.
Greulich–Pyle method
The GP method is a procedure in which BA can be assessed by evaluating the subject’s X-ray film with the closest reference in the atlas (7). It is a low-cost and widely available method aimed at a specific group of people. The 57 reference images (31 from males and 26 from females) originated from a sample obtained half a century ago. This procedure has a disadvantage that there are huge differences between the reference standards in the series of pictures collected at intervals of 6 months.
Several studies have applied the GP method in clinical and forensic fields to find that the reliability is not consistent. The GP atlas cannot be applied to all populations (20). Age and gender differences were obvious. Suri et al. (10) found the GP method to be reliable in females and accurate in the 4-year-old age group. Other studies (19, 20) demonstrated that the GP method is likely to underestimate the age in males and females, especially in 3-, 4-, and 6-year-old male group. A large error was noted in the BAA procedure using the GP method in a sample from India, and a huge error variability was observed for 5-year-old subjects of both genders. Typically, in the male and female samples between 3- and 6-year-old age groups, the skeletal retardation was in a range of 0.40–1.00 years. However, significant skeletal retardation occurred in the 4-year-old group (0.52 years for male subjects and 0.82 years for female subjects). Mansourvar et al. (21) concluded that the GP method is not reliable for various ethnic groups from all age groups except for Caucasian and Hispanic children. In the sample of Asian children, the skeletal age according to the GP method could be 2 years less than the CA in 4–6-year-old children. According to the present study, the GP method is not applicable in both genders because underestimation was reported in female subjects aged from 5 to 6 and male subjects aged from 4 to 6. In some specific samples, the Ds can be large than 2 years. After collecting 1,390 hand and wrist radiographs obtained in healthy children from Asian, African American, white, and Hispanic children, Zhang et al. (11) concluded that ethnic and racial differences in growth patterns exist at certain ages. When using the GP method to assess BA, it was significantly overestimated in Asian and Hispanic children. This result is the complete opposite. It is not clear whether the GP method can be used in the sample of Chinese during childhood.
Based on the results of the previous and current studies, the GP method should be used with caution in the different populations of preschool children.
TW3 method
The TW3 method can evaluate and score the maturity of each hand and wrist bone (22). The reference children populations were from European and American families with average social economic status during the 1980s and 1990s, and the data were adjusted to the secular trend in 2001.
In recent years, several clinical studies (23–25) have demonstrated that the TW3 method is the most appropriate method showing the highest degree of accuracy in 3–4-year-old males. Despite having a tendency to underestimate the CA in subjects aged 5–6-year-old. The TW3 method was the most accurate among the methods tested.
Various studies have compared TW3 to GP method (24, 26). According to the investigation of the Turkish children, the TW3 method underestimated the age with a mean accuracy of 0.18 and 0.21 years for male and female subjects, respectively (24). Significant differences were detected between CA and BA in both sexes (p < 0.05). For males, the GP method was the most accurate, followed by the TW3 method, while for female individuals, the TW3 method was the most accurate, followed by the GP method. In the sample of normal Korean children, there was a lower absolute error of the TW3 method than that of the GP method for both genders (p < 0.05). The skeletal age using the TW3 and GP methods were overestimated for male individuals (59.6 and 54.6%) and female individuals (72.2 and 74.3%). However, in this study, the TW3 method showed the highest performance for male subjects and similar proficiency for female subjects compared to the GP and RUS–CHN methods.
As demonstrated above, the TW3 method is optimal for subjects between 5- and 6-year-old. TW3 can be regarded as the most reliable BAA method with the highest accuracy compared to the other two methods. However, the numerical accuracy is not remarkable, and our results are not consistent with previous findings (24, 26). When the TW3 method is used clinically, its impact on bone maturation should be considered.
RUS–CHN method
In the past two decades, due to the trend of accelerated growth of Chinese children, Zhang et al. (9) have revised the standards based on the TW3 method and established the RUS–CHN method. The TW3 method is conducted on samples from European and American children, while RUS–CHN is a special BAA method designed for Chinese children. The RUS–CHN method selects new maturity indicators from some of the bone development levels in the TW3 method and divides the original into two levels. In addition, the RUS–CHN method divides the long-term fusion process of the radius and ulna into five grades for improved accuracy (27). Several studies have been carried out on this BAA method (12, 28–30).
According to a study for Chinese children, the RUS–CHN method can be used in all age groups of Han nationality. It showed an accuracy in BAA similar to the TW3 method. After analyzing 2,438 radiographs of 1,137 male and 1,301 female subjects, the differences between the CA and BA of each age group were 0.0–0.3 years in the RUS–CHN and TW3 bone maturity standards.
Recently, Xiong et al. (30) concluded that the RUS–CHN method was reliable for children of Han Nationality and applicable for children of Uygur nationality for various ages, especially in samples of 4.0–9.9-year-old age group. A good consistency was observed between the RUS–CHN and the TW3 methods in 3–6-year-old girls.
In the study by Zhang et al. (31), the radiographs of 45 children were assessed by 13 observers, who demonstrated the advanced reliability of RUS–CHN method in BAA. The study revealed that interobserver percentage agreement of ratings ranged from 70.5 to 92.1% (mean 84.3%) and 69.0–83.3% (mean 78.1%), respectively, and the 95% confidence limits for a single reading were ± 0.26 to ± 0.49 and ± 0.35 to ± 0.56, respectively.
In the present study, the RUS–CHN method shows maximal Ds among the three BAA methods. The prediction of BA is underestimated in each age group of both genders, especially in male individuals. Despite the RUS–CHN method having the advantages of high accuracy and repeatability, it showed an overall overestimation tendency and a false positive rate when applying for BAA in preschool children.
The present study has some limitations. First, this is a cross-sectional study using single-center data, and therefore the sample size was small. Second, it only covered a specific range of the population in the Zhejiang Province without including other areas in China. These results may be applicable only to the urban area of the Zhejiang Province or metropolitan areas with similar development statuses. Third, age groups under 3-year-old were excluded in both sexes. Finally, we could not ascertain full health in children, although no remarkable medical history for any genetic syndrome or trauma was noted in the hospital records. Hence, in-depth multicenter studies are essential to substantiate these findings.
Conclusion
The present study aimed to compare the CA and BA of Chinese preschool-aged children using the GP, TW3, and RUS–CHN methods to determine the reliability. Based on the results, we could draw the following conclusions: (i) the GP, TW3, and RUS–CHN methods are reliable for BAA in clinical practice for selected age classes (e.g., TW3 in 6-year-old); (ii) TW3 is the most suitable method to predict the BA of males, with the highest accuracy among the three methods (TW3: 32.24%, GP: 12.02%, RUS–CHN: 12.02%); (iii) the GP, TW3, and RUS–CHN methods have a low rate of correct classification in females (GP: 25.76%, TW3: 24.15%, and RUS–CHN: 21.26%); (iv) the GP method is not accurate due to its remarkable trend to underestimate the BA, especially in males; (v) the TW3 and RUS–CHN methods are not accurate, given the overestimation of BAA for both genders; and (vi) predictions within 6 months (CA ± 90 days) can rarely provide the correct classification results.
In conclusion, this study demonstrated that the results of BAA using the TW3 method were more reliable than the GP and RUS–CHN methods. Until an effective method is developed, we proposed that TW3 be utilized. However, added diagnostic value is provided by combining multiple methods when assessing BA. Due to the diagnostic value of BAA, improving the accuracy of BA methods is crucial to guide timely pediatric treatments.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
CG, ML, and ZD conceived and designed the study, had full access to the data in the study and took responsibility for the integrity of the data and the accuracy of data analysis. CG, QQ, ML, and ZD drafted the manuscript. CG, QQ, XX, and XH analyzed the data. CG, YL, and XX contributed to data acquisition. All authors critically revised the manuscript for intellectual content and approved the version for publication, agreed to be accountable for all aspects of the work related to the accuracy or integrity for appropriate investigation and resolution of any queries.
Funding
This study was funded by the Medical and Health Science and Technology Fund of Zhejiang Province (No. 2020PY014), Chinese Medicine Science and Technology Plan for the Modernization of Traditional Chinese Medicine Fund of Zhejiang Province (No. 2021ZX011), and Chinese Medicine Science and Technology Fund of Zhejiang Province (No. 2019ZQ031).
Acknowledgments
We thank all the children and their parents or supervisors for their cooperation and willingness to participate in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.976565/full#supplementary-material
References
1. Creo AL, Schwenk WF II. Bone age: a handy tool for pediatric providers. Pediatrics. (2017) 140:1486. doi: 10.1542/peds.2017-1486
2. Duren DL, Nahhas RW, Sherwood RJ. Do secular trends in skeletal maturity occur equally in both sexes? Clin Orthop Relat Res. (2015) 473:2559–67. doi: 10.1007/s11999-015-4213-1
3. Halabi SS, Prevedello LM, Kalpathy-Cramer J, Mamonov AB, Bilbily A, Cicero M, et al. The RSNA pediatric bone age machine learning challenge. Radiology. (2019) 290:498–503. doi: 10.1148/radiol.2018180736
4. Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, et al. Criteria for age estimation in living individuals. Int J Legal Med. (2008) 122:457–60. doi: 10.1007/s00414-008-0254-2
5. Larson DB, Chen MC, Lungren MP, Halabi SS, Stence NV, Langlotz CP. Performance of a deep-learning neural network model in assessing skeletal maturity on pediatric hand radiographs. Radiology. (2018) 287:313–22. doi: 10.1148/radiol.2017170236
6. Alshamrani K, Offiah AC. Applicability of two commonly used bone age assessment methods to twenty-first century UK children. Eur Radiol. (2020) 30:504–13. doi: 10.1007/s00330-019-06300-x
7. Greulich WW. Radiograph Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Redwood City, CA: Stanford University Press (1959).
8. Tanner JM, Healy MJ, Goldstein H, Cameron N. Assessment of Skeletal Maturity and Prediction of Adult Height: TW3 Method. 3rd ed. London: W.B. Saunders (2001).
9. Zhang SY, Liu LJ, Han YS, Liu G, Ma ZG, Shen XZ, et al. [Reference values of differences between TW3-C RUS and TW3-C carpal bone ages of children from five cities of China]. Zhonghua Er Ke Za Zhi. (2008) 46:851–5.
10. Suri S, Prasad C, Tompson B, Lou W. Longitudinal comparison of skeletal age determined by the Greulich and Pyle method and chronologic age in normally growing children, and clinical interpretations for orthodontics. Am J Orthod Dentofacial Orthop. (2013) 143:50–60. doi: 10.1016/j.ajodo.2012.08.027
11. Zhang A, Sayre JW, Vachon L, Liu BJ, Huang HK. Racial differences in growth patterns of children assessed on the basis of bone age. Radiology. (2009) 250:228–35. doi: 10.1148/radiol.2493080468
12. Zhang S, Liu L, Wu Z, Liu G, Ma Z, Shen X. The skeletal development standards of hand and wrist for Chinese children—China 05 I. TW3-C RUS, TW3-C carpal, and RUS-CHN methods. Chin J Sports Med. (2006) 15:509–16.
13. Benjavongkulchai S, Pittayapat P. Age estimation methods using hand and wrist radiographs in a group of contemporary Thais. Forensic Sci Int. (2018) 287:218.e1–218.e8. doi: 10.1016/j.forsciint.2018.03.045
14. Ma CH, Chen LY, Li MF, Wu D, Wang SS, Zhao YJ, et al. Treatment of preschool children with autism spectrum disorder: a trial to evaluate a learning style profile intervention program in China. Front Pediatr. (2022) 10:831621. doi: 10.3389/fped.2022.831621
15. Ke D, Lu D, Cai G, Wang X, Zhang J, Suzuki K. Chronological and skeletal age in relation to physical fitness performance in preschool children. Front Pediatr. (2021) 9:641353. doi: 10.3389/fped.2021.641353
16. Wang F, Gu X, Chen S, Liu Y, Shen Q, Pan H, et al. Artificial intelligence system can achieve comparable results to experts for bone age assessment of Chinese children with abnormal growth and development. PeerJ. (2020) 8:e8854. doi: 10.7717/peerj.8854
17. Lee BD, Lee MS. Automated bone age assessment using artificial intelligence: the future of bone age assessment. Korean J Radiol. (2021) 22:792–800. doi: 10.3348/kjr.2020.0941
18. Ren X, Li T, Yang X, Wang S, Ahmad S, Xiang L, et al. Regression convolutional neural network for automated pediatric bone age assessment from hand radiograph. IEEE J Biomed Health Inform. (2019) 23:2030–8. doi: 10.1109/jbhi.2018.2876916
19. Zhang J, Lin F, Ding X. Maturation disparity between hand-wrist bones in a Chinese sample of normal children: an analysis based on automatic bonexpert and manual Greulich and Pyle atlas assessment. Korean J Radiol. (2016) 17:435–42. doi: 10.3348/kjr.2016.17.3.435
20. Patil ST, Parchand MP, Meshram MM, Kamdi NY. Applicability of Greulich and Pyle skeletal age standards to Indian children. Forensic Sci Int. (2012) 216:200. e1–4. doi: 10.1016/j.forsciint.2011.09.022
21. Mansourvar M, Ismail MA, Raj RG, Kareem SA, Aik S, Gunalan R, et al. The applicability of Greulich and Pyle atlas to assess skeletal age for four ethnic groups. J Forensic Leg Med. (2014) 22:26–9. doi: 10.1016/j.jflm.2013.11.011
22. Wang YM, Tsai TH, Hsu JS, Chao MF, Wang YT, Jaw TS. Automatic assessment of bone age in Taiwanese children: a comparison of the Greulich and Pyle method and the Tanner and Whitehouse 3 method. Kaohsiung J Med Sci. (2020) 36:937–43. doi: 10.1002/kjm2.12268
23. Schmidt S, Nitz I, Ribbecke S, Schulz R, Pfeiffer H, Schmeling A. Skeletal age determination of the hand: a comparison of methods. Int J Legal Med. (2013) 127:691–8. doi: 10.1007/s00414-013-0845-4
24. Büken B, Erzengin OU, Büken E, Safak AA, Yazici B, Erkol Z. Comparison of the three age estimation methods: which is more reliable for Turkish children? Forensic Sci Int. (2009) 183:103.e1–7. doi: 10.1016/j.forsciint.2008.10.012
25. Zhou XL, Wang EG, Lin Q, Dong GP, Wu W, Huang K, et al. Diagnostic performance of convolutional neural network-based tanner-Whitehouse 3 bone age assessment system. Quant Imaging Med Surg. (2020) 10:657–67. doi: 10.21037/qims.2020.02.20
26. Oh Y, Lee R, Kim HS. Evaluation of skeletal maturity score for Korean children and the standard for comparison of bone age and chronological age in normal children. J Pediatr Endocrinol Metab. (2012) 25:279–84. doi: 10.1515/jpem-2012-0028
27. Zhang SY, Liu LJ, Wu ZL, Liu G, Ma ZG, Shen XZ, et al. Standards of TW3 skeletal maturity for Chinese children. Ann Hum Biol. (2008) 35:349–54. doi: 10.1080/03014460801953781
28. Zhao X, Zhang M, Cheng M, Yue X, Li W, Li C. Construction of artificial intelligence system of carpal bone age for Chinese children based on China-05 standard. Med Phys. (2022) 49:3223–32. doi: 10.1002/mp.15554
29. Zhang SY, Wu ZL, Shen XZ, Hua JQ, Chai JZ, Zhang T, et al. The sandards of skeletal maturity of hand and wrist for Chinese-China 05 II. reliability of assessing akeletal Age by RUS-CHN and TW3-C carpal methods. Chin J Sports Med. (2006) 25:641–5.
30. Xiong XX, Li BY, Guo H, Feng ZH. Hand-wrist bone age assessment of Han and Uygur adolescents and children in Urumqi. Chin J Tissue Eng Res. (2015) 19:2341–5.
Keywords: bone age assessment, preschool children, Greulich–Pyle (GP), Tanner–Whitehouse 3 (TW3), China 05 RUS–CHN
Citation: Gao C, Qian Q, Li Y, Xing X, He X, Lin M and Ding Z (2022) A comparative study of three bone age assessment methods on Chinese preschool-aged children. Front. Pediatr. 10:976565. doi: 10.3389/fped.2022.976565
Received: 23 June 2022; Accepted: 29 July 2022;
Published: 16 August 2022.
Edited by:
Jayakumar Jayaraman, Virginia Commonwealth University, United StatesReviewed by:
Samiya Razzaq, Baylor College of Medicine, United StatesPrerna Bansal, Wolfson Children’s Hospital, United States
Copyright © 2022 Gao, Qian, Li, Xing, He, Lin and Ding. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Lin, aGFuZ3pob3VsbTIwMjJAMTYzLmNvbQ==; Zhongxiang Ding, aGFuZ3pob3Vkeng3M0AxMjYuY29t