 Wen-Yuan Jin
Wen-Yuan Jin Ling-Ling Wu
Ling-Ling Wu Li-Fei Hu
Li-Fei Hu Wen-Hao Li
Wen-Hao Li Chao Song
Chao Song Zhi-Wei Zhu
Zhi-Wei Zhu- Department of Developmental Behavioral Pediatrics, Children's Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, China
Objective: The present study was aimed at investigating the intelligence profiles and adaptive behaviors of children with high-functioning autism spectrum disorder (HFASD) and developmental speech and language disorders (DSLDs). We compared the similarities and differences of cognitive capabilities and adaptive functions and explored their correlations in the HFASD and DSLDs groups.
Methods: 128 patients with HFASD, 111 patients with DSLDs and 114 typically developing (TD) children were enrolled into our study. Wechsler Intelligence Scale for Children-IV (WISC-IV) and Adaptive Behavior Assessment System-II (ABAS-II) were respectively applied to evaluate intelligence profiles and adaptive behaviors. Intelligence quotient (IQ) scores and adaptive functioning scores among the HFASD, DSLDs and TD groups were compared through one-way ANOVA. Pearson correlation coefficient was applied to examine the relationships between WISC indices and ABAS domains.
Results: Outcomes showed significantly poorer intelligence profiles and adaptive behaviors in HFASD and DSLDs groups. Both children with HFASD and DSLDs demonstrated impairments in verbal comprehension and executive functions. Processing speed and working memory were the predominant defects of children with HFASD and DSLDs in the field of executive functions, respectively. Whereas perceptual reasoning was a relative strength for them. Children with DSLDs had balanced scores of all the domains in ABAS-II; nevertheless, HFASD individuals demonstrated striking impairments in Social domain. Correlation analysis showed IQs of children with HFASD were positively correlated with all the domains and General Adaptive Composite (GAC) of ABAS-II. Additionally, IQs were positively correlated with Conceptual domain and GAC for children with DSLDs. Compared with DSLDs group, intelligence displayed stronger correlations with adaptive behaviors in HFASD group.
Conclusion: Our study expanded insights regarding intelligence profiles and adaptive behaviors of children with HFASD and DSLDs. Moreover, this study made breakthroughs in discovering positive correlations between IQs and adaptive functions in the two neurodevelopmental disorders.
Introduction
Based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), autism spectrum disorder (ASD) is a kind of neurodevelopmental disorder characterized by impaired social communications, restricted interests and repetitive patterns of behavior (1). According to the Autism and Developmental Disabilities Monitoring (ADDM) Network in United States, the prevalence of ASD is 23.0 per 1,000 (one in 44) children aged 8 years (2). About 31% ASD people are accompanied by intellectual disability (Full-Scale Intelligence Quotient, FSIQ <70) (1). Those ASD individuals without intellectual disability (FSIQ ≥70) are defined as high-functioning ASD (HFASD) (3). Intelligence profiles of HFASD have presented several specific characteristics. Evidence from previous studies suggested that subjects with HFASD showed impairments in Verbal Comprehension Index (VCI), Processing Speed Index (PSI) and FSIQ compared with typically developing (TD) children. PSI (Coding and Symbol Search) was always the lowest index, associated with increased autism communication symptoms (4, 5). In addition, Nader et al. (6) and Mayes et al. (7) discovered that HFASD people had defects in Working Memory Index (WMI), especially in Digit Span and Letter-Number Sequencing. Nevertheless, research findings indicated that HFASD individuals showed a good competence in Matrix Reasoning and Perceptual Reasoning Index (PRI) (4–8).
Developmental speech and language disorders (DSLDs) are defined as communication impairments that interfere the development of speech and language skills in the absence of cognitive disabilities, hearing loss, neurological or psychiatric disorders (9, 10). The prevalence of DSLDs ranges from 2.2% to 15%, covering multiple languages and cultures (11, 12). Subjects with DSLDs may suffer from speech disorders or language disorders, or both of them. DSLDs can affect children's abilities in language comprehension (receptive language) and verbal communication (expressive language). When children with DSLDs grew up, they had elevated risks of learning difficulties and poor performance on school achievements (13). It has been reported that DSLDs subjects had predisposition to dyslexia and problems in executive functions (14, 15). Additionally, increased evidence indicated that children with DSLDs were more prone to having difficulties in motor performance (9, 16). Therefore, DSLDs have distinctive defects in intellectual capabilities as a kind of neurodevelopmental disorder.
Several adaptive behavior measures, including Adaptive Behavior Assessment System (ABAS), Vineland Adaptive Behavior Scales (VABS) and Behavior Assessment System for Children (BASC), have been applied to evaluate the adaptive functions of children and adolescents with HFASD (17–20). All the scales suggested HFASD individuals had significant impairments on adaptive behaviors. Composite scores and all the skill area scores of HFASD group were generally more than one standard deviation (SD) below the population mean (17, 18). Social skill area was the most severe impaired part according to ABAS-Second Edition (ABAS-II). Daily living skill was another significant weakness of HFASD subjects based on VABS (18–20). Functional Academics was a relative strength of HFASD compared with other skill areas. Furthermore, results from previous studies revealed significant discrepancies between HFASD people's IQs and their adaptive functions (17, 18). Kenworthy et al. (20) discovered that communication skills were positively associated with IQs whereas global adaptive functions were negatively associated with autistic symptoms for children with HFASD.
Different from research concerning HFASD, few studies systemically explored the adaptive behaviors of children and adolescents with DSLDs. Self reports from 6-year-old children with DSLDs indicated the most important problem in their daily life was difficulties in academic achievements at school (15). Outcomes of a recent study revealed adolescents with DSLDs showed poorer school adjustment, less adaptive skills and more emotional problems (21). Young adults with DSLDs had lower levels of social self-efficacy and self confidence and higher levels of shyness (22). They were at increased risks of experiencing difficulties in friendships and community integration when they grew up (13). However, their prosocial behaviors, such as being kind, empathetic, sharing and helpful with others, were still within the normal range and stable over time (23).
As described above, previous research has summarized several defects in specific areas of cognitive and adaptive capabilities for children with HFASD and DSLDs. Our study was focused on comparing the similarities and differences of intelligence profiles and adaptive functions among the HFASD, DSLDs and TD groups and exploring the correlations between IQs and adaptive behaviors. Wechsler Intelligence Scale for Children-Fourth Edition (WISC-IV) and ABAS-II have been respectively applied to evaluate the IQ scores and adaptive behavior scores of our participants. The present study was aimed at providing more supports for clinicians to have a comprehensive understanding of intelligence and adaptive behavior characteristics of HFASD and DSLDs.
Materials and methods
Participants
Between January 2019 and January 2022, outpatients aged 6–16 years old visited the Department of Developmental Behavioral Pediatrics, Children's Hospital, Zhejiang University School of Medicine and met the inclusion criteria were enrolled in the present study. Our study was approved by the hospital's Clinical Research Ethics Committee (No. 2022-IRB-099) and the informed consent was obtained from parents or caregivers of every participant. HFASD was diagnosed based on DSM-5 criteria, results of Autism Behavior Checklist (ABC) and determined by two professionally qualified developmental behavioral pediatrics clinicians. Children with HFASD had an FSIQ met or exceeded 70 (according to WISC-IV). DSLDs were characterized by developmental delays in speech and language in the absence of mental or physical retardation, hearing loss, emotional disorder, or environmental deprivation (16). According to ICD-11, DSLDs group included developmental speech sound disorder, developmental speech fluency disorder and developmental language disorder. Children with DSLDs also had an FSIQ score ≥70 (WISC-IV). Participants of TD group were recruited among the outpatients without organic diseases or psychiatric disorders. Exclusion criteria of TD group consisted of ASD, DSLDs, attention deficit hyperactivity disorder, intellectual disorders and other neurodevelopmental diseases; inherited metabolic diseases; serious heart, liver and kidney dysfunctions; traumatic brain injuries and cerebral vascular diseases. A total of 128 patients with HFASD, 111 patients with DSLDs and 114 TD controls participated in our study. All the participants had no psychotropic medication records during the last three months.
Autism behavior checklist
ABC is a widely applied screening tool of ASD introduced into China by Yang in 1993 (24). ABC is consisted of 57 items and five domains (sensory, relating, body concept, language and social self-help domains). It can be used for individuals aged from 18 months to 35 years old. Children and adolescents are highly suspected of ASD if the total scores of ABC meet or exceed 67.
Wechsler intelligence scale for children-fourth edition
WISC-IV is an extensively used measure of intellectual ability, which was introduced into China in 2009 by Zhang (25). WISC-IV is consisted of four index scores: Verbal Comprehension Index (VCI), Perceptual Reasoning Index (PRI), Working Memory Index (WMI) and Processing Speed Index (PSI). It has 10 core subtests and 5 supplemental subtests. The VCI contains Vocabulary, Similarity, Comprehension, Information and Word Reasoning subtests; the PRI contains Block Design, Picture Concept, Matrix Reasoning and Picture Completion subtests; the WMI contains Digit Span, Letter-Number Sequencing and Arithmetic subtests; the PSI contains Coding, Symbol Search and Cancellation subtests. FSIQ is summarized from VCI, PRI, WMI and PSI. In our study, WISC-IV has been conducted for every participant by trained clinicians.
Adaptive behavior assessment system-second edition
ABAS-II is a comprehensive, individualized and psychometrically adaptive behavior scale with good reliability and validity. The scale comprises a General Adaptive Composite (GAC) score, three domain scores (Conceptual, Social and Practical) and 10 skill area scores (Communication, Community Use, Functional Academics, Home Living, Health and Safety, Leisure, Self-Care, Self-Direction, Social, and Work) (26). The Conceptual domain contains Communication, Functional Academics, and Self-Direction; the Social domain contains Social and Leisure; the Practical domain contains Community Use, Home Living, Health and Safety, and Self-Care. Given that the majority of our participants did not have work experience and were under 17 years old, Work skills had not been included into the scale. All the parents or caregivers of participants were required to finish the questionnaire. Finally, 125 copies of ABAS-II in HFASD group, 109 copies in DSLDs group and 108 copies in TD group had been received in the study.
Statistical analysis
Normally and non-normally distributed variables were respectively presented as mean ± SD and median (interquartile range, IQR) in our study. Rates [N (%)] of basic demographic characteristics between HFASD and TD group, between DSLDs and TD group were compared with chi-square test. Existing differences of VCI, PRI, WMI, PSI, FSIQ scores and all the subtests of WISC-IV among the HFASD, DSLDs and TD groups were compared through one-way analysis of variance (ANOVA). Comparisons of GAC scores, Conceptual domain scores, Social domain scores, Practical domain scores and all the skill area scores of ABAS-II among the three groups were conducted through one-way ANOVA. Pearson correlation coefficient was applied to examine the relationships between IQ scores (FSIQ, VCI, PRI, WMI, PSI) and adaptive behavior scores (GAC, Conceptual domain, Social domain and Practical domain). All the analyses were performed with IBM SPSS statistics 25.0 version (SPSS Inc, Chicago, III, USA). P-values <0.05 were defined as statistically significant.
Results
Basic demographic characteristics of subjects
Basic demographic characteristics of subjects were presented in Table 1. Median ages of the HFASD, DSLDs and TD groups were respectively 6.8, 6.9 and 8.2. Male participants in HFASD and DSLDs groups were respectively 88.3% and 87.4%; whereas male participants in TD group was 67.5%. Both HFASD and DSLDs were more likely to occur in boys than in girls (P < 0.01). Children living in town/country were more tended to suffer from DSLDs (P < 0.01). Paternal and maternal education backgrounds of DSLDs group were remarkably poorer than TD group (P < 0.01). Only 30.6% of fathers and 22.5% of mothers in DSLDs group received university or higher education. However, the proportions were approximately 50% in TD group. In DSLDs group, 32.4% of fathers and 26.1% of mothers had an education background of junior school or even lower, which were significantly greater than those in TD group (P < 0.01). However, paternal and maternal education status of HFASD group had no significant differences with TD group. Most of the subjects in all groups had no or only one sibling.
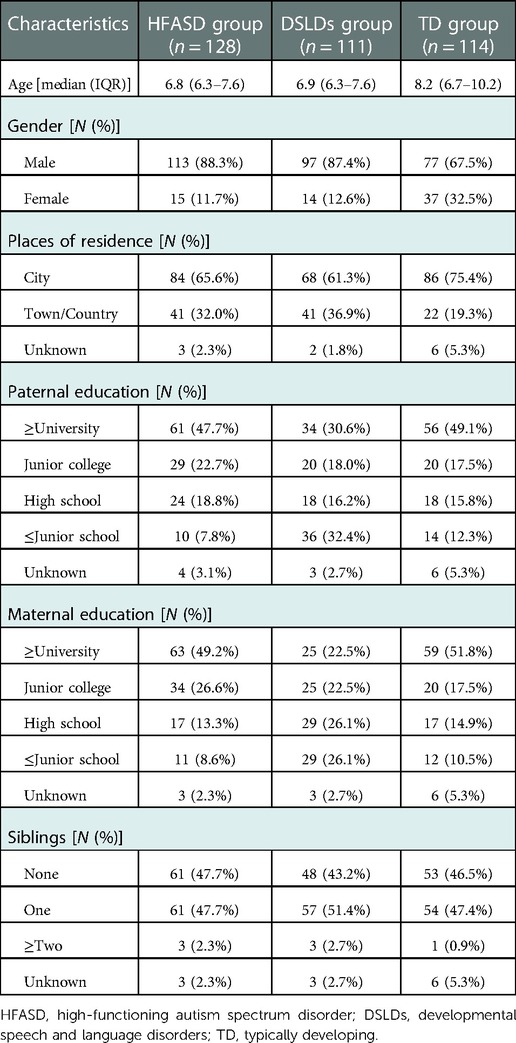
Table 1. Basic demographic characteristics of subjects.
Comparisons of intelligence profiles among the HFASD, DSLDs and TD groups
Intelligence profiles of the HFASD, DSLDs and TD groups were presented and compared in Table 2. Similarity, Vocabulary, Comprehension, Block Design, Picture Concept, Matrix Reasoning, Digit Span, Coding and Symbol Search had been performed for every participant. Given the fact that some participants had never studied English alphabet before, part of the subjects were tested for Letter-Number Sequencing and the others were tested for Arithmetic. Results showed that all the subtests of WISC in HFASD group and DSLDs group were significantly lower than those in TD group (P < 0.05). In addition, all the indices including VCI, PRI, WMI, PSI and FSIQ in HFASD group and DSLDs group were significantly lower than those in TD group (P < 0.01). Participants in HFASD group achieved the highest average score in Block Design and the lowest average score in Comprehension among all the subtests. Children with DSLDs obtained the highest average score in Matrix Reasoning and the lowest average score in Digit Span. Comprehension, Picture Concept, Coding and Symbol Search scores of HFASD group were remarkably lower than DSLDs group, whereas Similarity and Block Design scores of HFASD group were remarkably higher than DSLDs group (P < 0.01). PRI was the highest index score and PSI was the lowest index score for children with HFASD. PRI and PSI were the highest index scores and WMI was the lowest index score for children with DSLDs. Furthermore, PSI scores of HFASD group were significantly lower than those of DSLDs group (P < 0.01).
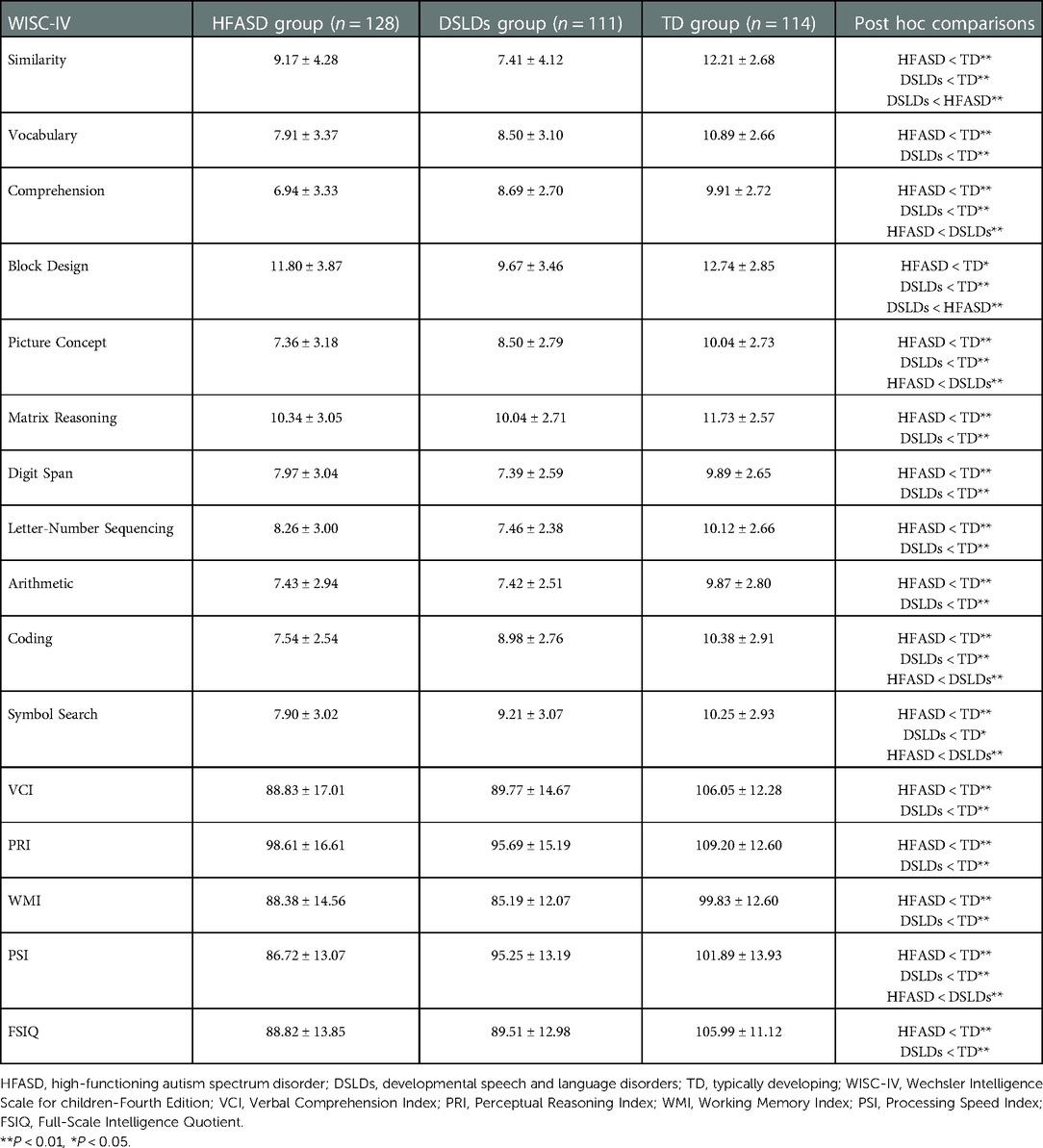
Table 2. Comparisons of intelligence profiles among the HFASD, DSLDs and TD groups.
Comparisons of adaptive behaviors among the HFASD, DSLDs and TD groups
Adaptive behaviors of the HFASD, DSLDs and TD groups were presented and compared in Table 3. All of them were evaluated for Communication, Functional Academics, Self-Direction, Social, Leisure, Community Use, Home Living, Health and Safety, and Self-Care scores. Results indicated that all the skill areas, GAC, Conceptual domain, Social domain and Practical domain in HFASD group were significantly lower than those in TD group (P < 0.01). Except for Self-Care scores, all the skill areas, GAC, Conceptual domain, Social domain and Practical domain in DSLDs group were remarkably lower than those in TD group (P < 0.05). Consistent with previous studies, Social domain was the weakest adaptive functioning area of HFASD people, which was significantly lower than children with DSLDs as well (P < 0.01). Social, Self-Direction, Communication, Leisure and Self-Care scores of HFASD group were remarkably lower than those in DSLDs group (P < 0.05). Additionally, for children with DSLDs, more difficulties had been found in Social and Self-Direction skill areas. Practical domain was a relative strength for individuals with HFASD and DSLDs.
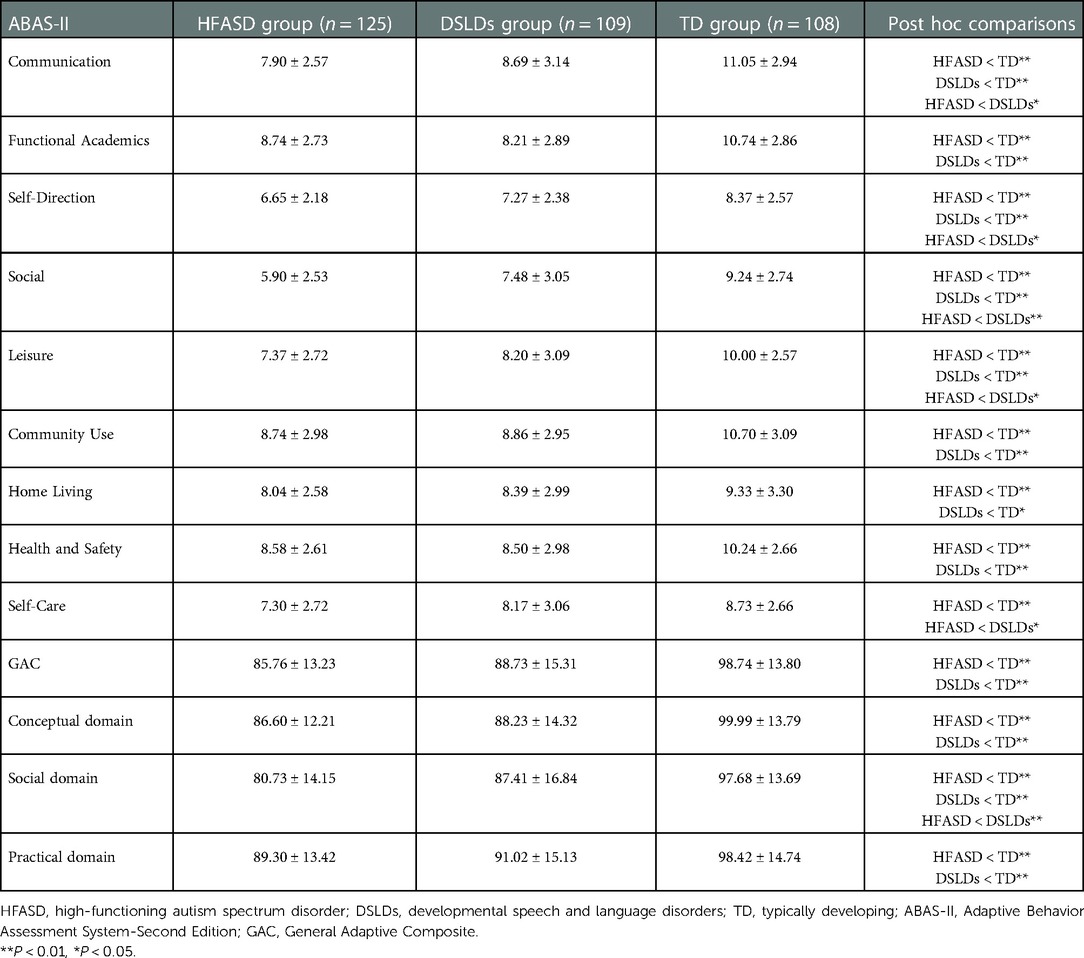
Table 3. Comparisons of adaptive behaviors among the HFASD, DSLDs and TD groups.
Correlations between intelligence profiles and adaptive behaviors in the HFASD group and DSLDs group
Pearson correlations between intelligence profiles and adaptive behaviors in the HFASD group and DSLDs group were respectively presented in Tables 4, 5. Outcomes suggested that VCI, PRI, PSI and FSIQ scores of WISC were positively correlated with all the adaptive behavior domains including Conceptual domain, Social domain, Practical domain and GAC in HFASD group (P < 0.05). Moreover, WMI scores were significantly correlated with Conceptual domain scores for children with HFASD (P < 0.05). Conceptual domain had the strongest positive correlation with FSIQ in HFASD group (r = 0.473, P = 0.000), especially Functional Academics (r = 0.573, P = 0.000). For children with DSLDs, VCI, PRI, WMI and FSIQ scores were positively correlated with Conceptual domain scores (P < 0.05). WMI and FSIQ scores were positively correlated with GAC scores (P < 0.05). However, intelligence had no significant correlations with Social domain or Practical domain in DSLDs group. Compared with DSLDs group, IQs showed stronger relationships with adaptive behaviors in HFASD group.
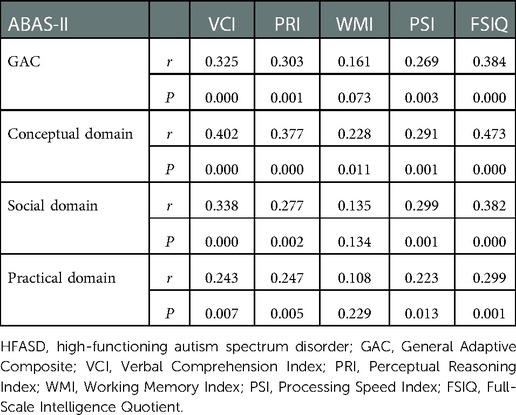
Table 4. Pearson correlations between intelligence profiles and adaptive behaviors in the HFASD group.
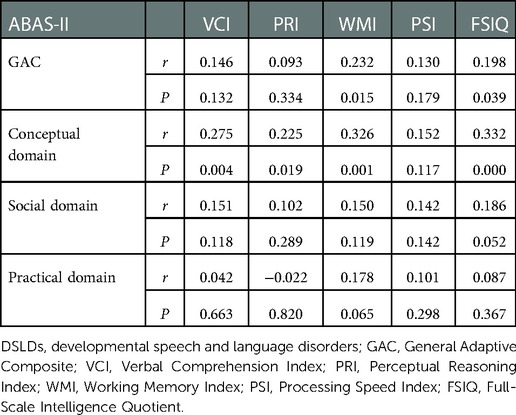
Table 5. Pearson correlations between intelligence profiles and adaptive behaviors in the DSLDs group.
Discussion
HFASD and DSLDs are common neurodevelopmental disorders with molecular biological evidence and imaging basis. Existing research has discovered genetic defects and brain morphological alterations or structural abnormalities in HFASD and DSLDs patients (27–32). The aforementioned pathophysiology mechanisms result in distinctive clinical symptoms, cognitive abilities and adaptive performances of HFASD and DSLDs. Previous studies investigated the intelligence profiles and adaptive functioning characteristics of them, but few studies compared the similarities and differences between them. Our study made comparisons of intelligence levels and adaptive behaviors and explored their interactions in the HFASD and DSLDs groups, which further provided clinical evidence for differential diagnosis and prognosis of HFASD and DSLDs. It was of great importance to expand insights into clinical features of the two neurodevelopmental disorders.
In line with previous research findings (4, 5, 7, 33), the present study convinced PRI was the strongest index and PSI was the weakest index in WISC for children with HFASD. Our results showed participants in HFASD group achieved the highest average score in Block Design and the lowest average score in Comprehension among all the subtests. Coding and Symbol Search in HFASD group were significantly lower than those in DSLDs group and TD group. The largest discrepancies between HFASD and TD group existed in VCI and PSI scores. Above findings reflected difficulties mainly in processing speed and verbal comprehension and advantages in perceptual reasoning for children with HFASD. These phenomenon displayed the impairments of children with HFASD in understanding social rules and sensory processing (5). They also connected phenotypes of HFASD with neuroimaging structures. It had been discovered that increased amygdala size correlated with the severity of social and communication deficits in ASD (29). Thus, our research provided more sufficient evidence supporting the conclusions from previous studies. Consistent with partial previous outcomes (5, 6), the average FSIQ of HFASD group was significantly lower than that of TD group in our study. However, several research held the view that FSIQ of HFASD children had no significant difference with TD children (4, 7). The discrepancy might be caused by limited sample size. Additionally, HFASD children had weaknesses in auditory attention and graphomotor skills. Although WISC-IV captured HFASD children's visual reasoning strength with non-verbal Matrix Reasoning and Picture Concept subtests, it might still underestimate the intelligence of HFASD to some extent as a measurement. Therefore, more large population-based studies with appropriate measurements are required to elucidate this issue in the future.
One noteworthy finding from this study was that IQ scores of all the subtests and indices in WISC of DSLDs children were significantly lower than TD children and WMI was the most severe impaired index for DSLDs individuals. As far as we are concerned, few previous studies systemically explored the intelligence profile of children with DSLDs (34, 35). Our study comprehensively displayed the cognitive characteristics of DSLDs, suggesting DSLDs affect multiple learning abilities at childhood and adolescence. Results demonstrated that children with DSLDs obtained relative lower scores in Similarity, Digit Span, Arithmetic and Letter-Number Sequencing. But they achieved relative higher scores in Matrix Reasoning, Block Design and Symbol Search. Children with DSLDs showed a good competence in perceptual reasoning and processing speed. However, poor performance in VCI and WMI indicated their predominant defects in verbal comprehension and executive functions. Executive attentional control in working memory was implied to be a powerful predictor of language development and a strong determinant of learning capability (regarding both literacy and numeracy) (35–38). Our findings further confirmed children had a history of DSLDs were at increased risks of adverse long-term consequences on academic achievements.
Another interesting finding of our study was that VCI, PRI, PSI and FSIQ scores of WISC were positively correlated with all the adaptive behavior domains including Conceptual domain, Social domain, Practical domain and GAC in HFASD group. Research of Lopata et al. (17) and Tamm et al. (18) reported significant discrepancies between IQ scores and adaptive functioning scores for children with HFASD. Kraper et al. (39) observed a similar phenomenon in young adulthood patients of ASD. Different from previous studies, results of our study displayed smaller gaps between cognitive levels and adaptive behaviors. There existed several factors influencing the outcomes. Unbalanced parental educational backgrounds of participants was speculated to be the reason of lower IQ scores in our HFASD group compared with literature reports. It should also be taken into consideration that overprotection from parents or grandparents and lack of exercise in daily life were important factors interfering progress in adaptive behaviors for Chinese children. Additionally, we found significant positive correlations between IQs and adaptive behavior scores for children with HFASD, which was a novel contribution of our research. Kenworthy et al. (20) and Audras-Torrent et al. (40) once discovered IQ scores were positively associated with adaptive communication skills and Conceptual domain. Rosa et al. (41) reported worse intellectual performance, especially in verbal comprehension and working memory, was significantly correlated with more severe symptoms and poorer adaptive functions. Our results revealed IQ scores (VCI, PRI, PSI and FSIQ) of HFASD were positively correlated with GAC and all the domains (Conceptual domain, Social domain and Practical domain) of ABAS-II. The strong associations suggested intelligence level was a potentially important factor that affected the development of adaptive behaviors for children with HFASD, which was contributed to predicting clinical outcomes (i.e., work performance, self-care, friendship, prosocial behavior and community integration in the adolescence and adulthood) of HFASD patients.
Unlike children with HFASD, cognitive capabilities exerted less impacts on adaptive behaviors in children with DSLDs. Our outcomes convinced significantly poorer adaptive functions of all the domains in children with DSLDs compared with TD children. We also found VCI, PRI, WMI and FSIQ scores of DSLDs group were positively correlated with Conceptual domain. But their associations with Social domain and Practical domain were not statistically significant. WMI and FSIQ scores of DSLDs group were positively related with GAC. The relationships between IQs and adaptive behaviors in DSLDs group were not as strong as counterparts in HFASD group. Moreover, children with DSLDs had balanced scores of all the domains in ABAS-II. Nevertheless, children with HFASD demonstrated striking impairments in Social domain. This discovery proved the underlying biological mechanisms of ASD. It had been reported that functional abnormalities in orbitofrontal-striata-amygdala circuit led to difficulties in social orienting, social seeking and liking, and social maintaining, which resulted in social impairments in ASD children (42). Our findings further disclosed the similarities and differences in cognitive capabilities and adaptive behaviors of the two neurodevelopmental disorders.
There were still some limitations in the present study. First of all, our sample lacked population diversity and the sample size was not big enough. Given that China is a developing country characterized by huge population and imbalanced economic development, a multicenter study with larger sample size and multi-nationalities can be more representative. Secondly, the ages and genders of our participants were not well matched. Median age of TD group was greater than those of HFASD and DSLDs groups. Due to the characteristics of diseases, amounts of female participants in the HFASD and DSLDs groups were limited. Better matched research is required for minimizing the influences by confounders such as age and gender. Thirdly, data of ABAS-II were self-reported and possibly be subject to recall bias. Finally, we cannot rule out the possibility of underestimating intelligence levels for children with HFASD. As we all know, IQ scores of WISC highly depend on the cooperation degree and oral verbal comprehension of subjects. Whether WISC an appropriate measurement evaluating cognition of HFASD is still a controversy and worths further investigation in the future. Therefore, more well-designed prospective studies with innovative methods are needed to clarify this issue.
Conclusion
Our study convinced the consequences of previous studies regarding intelligence profiles and adaptive behaviors in children with HFASD and DSLDs. Both HFASD and DSLDs showed impairments in verbal comprehension and executive functions. Processing speed and working memory were the predominant defects of children with HFASD and DSLDs in the field of executive functions, respectively. Perceptual reasoning was a relative strength for them. Children with DSLDs had balanced scores of all aspects in adaptive behaviors; whereas HFASD individuals demonstrated striking impairments in Social domain. Moreover, this study made breakthroughs in discovering positive correlations between IQs and adaptive functions in children with HFASD and DSLDs. Compared with DSLDs, intelligence displayed stronger relationships with adaptive behaviors in HFASD. Our research findings contributed to more profound insights of the two neurodevelopmental disorders.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Clinical Research Ethics Committee of Children's Hospital, Zhejiang University School of Medicine. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
W-YJ participated in study design, data acquisition, literature review, statistical analysis and drafted the manuscript. L-LW, L-FH, W-HL, CS, Y-YW and X-LL contributed to data acquisition, literature review and performed statistical analysis. Z-WZ conceived the study, participated in its design and was the corresponding author of this manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Natural Science Foundation of Zhejiang Province (LGF20H090015).
Acknowledgments
We are grateful for all of our colleagues from Department of Developmental Behavioral Pediatrics, Children's Hospital, Zhejiang University School of Medicine in data collection and the participation of all the subjects in our study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. (2020) 9:S55–S65. doi: 10.21037/tp.2019.09.09
2. Maenner MJ, Shaw KA, Bakian AV, Bilder DA, Durkin MS, Esler A, et al. Prevalence and characteristics of autism Spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2018. MMWR Surveill Summ. (2021) 70:1–16. doi: 10.15585/mmwr.ss7011a1
3. Ghaziuddin M, Mountain-Kimchi K. Defining the intellectual profile of Asperger Syndrome: comparison with high-functioning autism. J Autism Dev Disord. (2004) 34:279–84. doi: 10.1023/b:jadd.0000029550.19098.77
4. Oliveras-Rentas RE, Kenworthy L, Roberson RB 3rd, Martin A, Wallace GL. WISC-IV profile in high-functioning autism spectrum disorders: impaired processing speed is associated with increased autism communication symptoms and decreased adaptive communication abilities. J Autism Dev Disord. (2012) 42:655–64. doi: 10.1007/s10803-011-1289-7
5. Li G, Jiang W, Du Y, Rossbach K. Intelligence profiles of Chinese school-aged boys with high-functioning ASD and ADHD. Neuropsychiatr Dis Treat. (2017) 13:1541–9. doi: 10.2147/NDT.S136477
6. Nader AM, Courchesne V, Dawson M, Soulières I. Does WISC-IV underestimate the intelligence of autistic children? J Autism Dev Disord. (2016) 46:1582–9. doi: 10.1007/s10803-014-2270-z
7. Mayes SD, Calhoun SL. WISC-IV and WIAT-II profiles in children with high-functioning autism. J Autism Dev Disord. (2008) 38:428–39. doi: 10.1007/s10803-007-0410-4
8. Rabiee A, Samadi SA, Vasaghi-Gharamaleki B, Hosseini S, Seyedin S, Keyhani M, et al. The cognitive profile of people with high-functioning autism spectrum disorders. Behav Sci (Basel). (2019) 9:20. doi: 10.3390/bs9020020
9. Müürsepp I, Ereline J, Gapeyeva H, Pääsuke M. Motor performance in 5-year-old preschool children with developmental speech and language disorders. Acta Paediatr. (2009) 98:1334–8. doi: 10.1111/j.1651-2227.2009.01294.x
10. Fernell E, Norrelgen F, Bozkurt I, Hellberg G, Löwing K. Developmental profiles and auditory perception in 25 children attending special preschools for language-impaired children. Acta Paediatr. (2002) 91:1108–15. doi: 10.1080/080352502760311629
11. O’Hare A, Bremner L. Management of developmental speech and language disorders: part 1. Arch Dis Child. (2016) 101:272–7. doi: 10.1136/archdischild-2014-307394
12. Norbury CF, Gooch D, Wray C, Baird G, Charman T, Simonoff E, et al. The impact of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a population study. J Child Psychol Psychiatry. (2016) 57:1247–57. doi: 10.1111/jcpp.12573
13. Dubois P, St-Pierre MC, Desmarais C, Guay F. Young adults with developmental language disorder: a systematic review of education, employment, and independent living outcomes. J Speech Lang Hear Res. (2020) 63:3786–800. doi: 10.1044/2020_JSLHR-20-00127
14. Doust C, Gordon SD, Garden N, Fisher SE, Martin NG, Bates TC, et al. The association of dyslexia and developmental speech and language disorder candidate genes with Reading and language abilities in adults. Twin Res Hum Genet. (2020) 23:23–32. doi: 10.1017/thg.2020.7
15. Ottosson S, Schachinger Lorentzon U, Kadesjö B, Gillberg C, Miniscalco C. Neurodevelopmental problems and quality of life in 6-year-olds with a history of developmental language disorder. Acta Paediatr. (2022) 111:115–22. doi: 10.1111/apa.16104
16. Visscher C, Houwen S, Scherder EJ, Moolenaar B, Hartman E. Motor profile of children with developmental speech and language disorders. Pediatrics. (2007) 120:e158–63. doi: 10.1542/peds.2006-2462
17. Lopata C, Smith RA, Volker MA, Thomeer ML, Lee GK, McDonald CA. Comparison of adaptive behavior measures for children with HFASDs. Autism Res Treat. (2013) 2013:415989. doi: 10.1155/2013/415989
18. Tamm L, Day HA, Duncan A. Comparison of adaptive functioning measures in adolescents with autism spectrum disorder without intellectual disability. J Autism Dev Disord. (2022) 52:1247–56. doi: 10.1007/s10803-021-05013-9
19. Laghi F, Ferri R, Caramuscio E, Lonigro A, Rea M, Pezzuti L. The floor effect on the ABAS-II in adolescents with autism spectrum disorder. J Autism Dev Disord. (2022) 52:4975–85. doi: 10.1007/s10803-021-05369-y
20. Kenworthy L, Case L, Harms MB, Martin A, Wallace GL. Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. J Autism Dev Disord. (2010) 40:416–23. doi: 10.1007/s10803-009-0911-4
21. Valera-Pozo M, Adrover-Roig D, Pérez-Castelló JA, Sanchez-Azanza VA, Aguilar-Mediavilla E. Behavioral, emotional and school adjustment in adolescents with and without developmental language disorder (DLD) is related to family involvement. Int J Environ Res Public Health. (2020) 17:1949. doi: 10.3390/ijerph17061949
22. Durkin K, Toseeb U, Botting N, Pickles A, Conti-Ramsden G. Social confidence in early adulthood among young people with and without a history of language impairment. J Speech Lang Hear Res. (2017) 60:1635–47. doi: 10.1044/2017_JSLHR-L-16-0256
23. Toseeb U, Pickles A, Durkin K, Botting N, Conti-Ramsden G. Prosociality from early adolescence to young adulthood: a longitudinal study of individuals with a history of language impairment. Res Dev Disabil. (2017) 62:148–59. doi: 10.1016/j.ridd.2017.01.018
24. Yang XL, Huang YQ, Jia MX, Chen SK. Test report of autism behavior checklist. Chin Mental Health J. (1993) 7:275–80.
25. Zhang HC. The revision of WISC-IV Chinese version. Psychol Sci. (2009) 32:1177–9. doi: 10.16719/j.cnki.1671-6981.2009.05.026
26. Harrison PL, Oakland T. Adaptive behavior assessment system, second edition. San Antonio, TX: Harcourt Assessment, Inc (2003).
27. Vorstman JAS, Parr JR, Moreno-De-Luca D, Anney RJL, Nurnberger JI Jr, Hallmayer JF. Autism genetics: opportunities and challenges for clinical translation. Nat Rev Genet. (2017) 18:362–76. doi: 10.1038/nrg.2017.4
28. Thapar A, Rutter M. Genetic advances in autism. J Autism Dev Disord. (2021) 51:4321–32. doi: 10.1007/s10803-020-04685-z
29. Girault JB, Piven J. The neurodevelopment of autism from infancy through toddlerhood. Neuroimaging Clin N Am. (2020) 30:97–114. doi: 10.1016/j.nic.2019.09.009
30. Plug MB, van Wijngaarden V, de Wilde H, van Binsbergen E, Stegeman I, van den Boogaard MH, et al. Clinical characteristics and genetic etiology of children with developmental language disorder. Front Pediatr. (2021) 9:651995. doi: 10.3389/fped.2021.65199
31. Landi N, Perdue M. Neuroimaging genetics studies of specific reading disability and developmental language disorder: a review. Lang Linguist Compass. (2019) 13:e12349. doi: 10.1111/lnc3.12349
32. Lee JC, Dick AS, Tomblin JB. Altered brain structures in the dorsal and ventral language pathways in individuals with and without developmental language disorder (DLD). Brain Imaging Behav. (2020) 14:2569–86. doi: 10.1007/s11682-019-00209-1
33. Nader AM, Jelenic P, Soulières I. Discrepancy between WISC-III and WISC-IV cognitive profile in autism spectrum: what does it reveal about autistic cognition? PLoS One. (2015) 10:e0144645. doi: 10.1371/journal.pone.0144645
34. Acosta-Rodríguez VM, Ramírez-Santana GM, Hernández-Expósito S. Intervention for oral language comprehension skills in preschoolers with developmental language disorder. Int J Lang Commun Disord. (2022) 57:90–102. doi: 10.1111/1460-6984.12676
35. Ralli AM, Chrysochoou E, Roussos P, Diakogiorgi K, Dimitropoulou P, Filippatou D. Executive function, working memory, and verbal fluency in relation to non-verbal intelligence in greek-speaking school-age children with developmental language disorder. Brain Sci. (2021) 11:604. doi: 10.3390/brainsci11050604
36. Vugs B, Knoors H, Cuperus J, Hendriks M, Verhoeven L. Interactions between working memory and language in young children with specific language impairment (SLI). Child Neuropsychol. (2016) 22:955–78. doi: 10.1080/09297049.2015.1058348
37. Chrysochoou E, Bablekou Z, Tsigilis N. Working memory contributions to reading comprehension components in middle childhood children. Am J Psychol. Fall. (2011) 124:275–89. doi: 10.5406/amerjpsyc.124.3.0275
38. Acosta Rodríguez V, Ramírez Santana GM, Hernández Expósito S. Executive functions and language in children with different subtypes of specific language impairment. Neurologia. (2017) 32:355–62. doi: 10.1016/j.nrl.2015.12.018
39. Kraper CK, Kenworthy L, Popal H, Martin A, Wallace GL. The gap between adaptive behavior and intelligence in autism persists into young adulthood and is linked to psychiatric co-morbidities. J Autism Dev Disord. (2017) 47:3007–17. doi: 10.1007/s10803-017-3213-2
40. Audras-Torrent L, Miniarikova E, Couty F, Dellapiazza F, Berard M, Michelon C, et al. WISC-V profiles and their correlates in children with autism spectrum disorder without intellectual developmental disorder: report from the ELENA cohort. Autism Res. (2021) 14:997–1006. doi: 10.1002/aur.2444
41. Rosa M, Puig O, Lázaro L, Vallés V, Lera S, Sánchez-Gistau V, et al. Broad cognitive profile in children and adolescents with HF-ASD and in their siblings: widespread underperformance and its clinical and adaptive correlates. J Autism Dev Disord. (2017) 47:2153–62. doi: 10.1007/s10803-017-3137-x
Keywords: high-functioning autism spectrum disorder, developmental speech and language disorders, intelligence, adaptive behavior, WISC, ABAS
Citation: Jin W, Wu L, Hu L, Li W, Song C, Wang Y, Liu X and Zhu Z (2023) Intelligence profiles and adaptive behaviors of high-functioning autism spectrum disorder and developmental speech and language disorders. Front. Pediatr. 10:972643. doi: 10.3389/fped.2022.972643
Received: 18 June 2022; Accepted: 6 December 2022;
Published: 9 January 2023.
Edited by:
Lori-Ann Rosalind Sacrey, University of Alberta, CanadaReviewed by:
Robert Perna, University of Michigan Medical Center, United StatesSarah Raza, University of Alberta, Canada
© 2023 Jin, Wu, Hu, Li, Song, Wang, Liu and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhiwei Zhu emh1emhpd2VpQHpqdS5lZHUuY24=
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics