 Kelly C. Jordan
Kelly C. Jordan Jane L. Di Gennaro1
Jane L. Di Gennaro1 Amélie von Saint André-von Arnim
Amélie von Saint André-von Arnim
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 19 July 2022
Sec. Pediatric Critical Care
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.954995
Background: Burn injuries are a major cause of death and disability globally. The World Health Organization (WHO) launched the Global Burn Registry (GBR) to improve understanding of burn injuries worldwide, identify prevention targets, and benchmark acute care. We aimed to describe the epidemiology, risk factors, and outcomes of children with burns to demonstrate the GBR's utility and inform needs for pediatric burn prevention and treatment.
Methods: We performed descriptive analyses of children age ≤ 18 years in the WHO GBR. We also described facility-level capacity. Data were extracted in September of 2021.
Results: There were 8,640 pediatric and adult entries from 20 countries. Of these, 3,649 (42%) were children (0–18 years old) from predominantly middle-income countries. The mean age was 5.3 years and 60% were boys. Children aged 1–5 years comprised 62% (n = 2,279) of the cohort and mainly presented with scald burns (80%), followed by flame burns (14%). Children >5 years (n = 1,219) more frequently sustained flame burns (52%) followed by scald burns (29%). More than half of pediatric patients (52%) sustained a major burn (≥15% total body surface area) and 48% received surgery for wound closure during the index hospitalization. Older children had more severe injuries and required more surgery. Despite the frequency of severe injuries, critical care capacity was reported as “limited” for 23% of pediatric patients.
Conclusions: Children represent a large proportion of people with burn injuries globally and often sustain major injuries that require critical and surgical intervention. However, critical care capacity is limited at contributing centers and should be a priority for healthcare system development to avert preventable death and disability. This analysis demonstrates that the GBR has the potential to highlight key epidemiological characteristics and hospital capacity for pediatric burn patients. To improve global burn care, addressing barriers to GBR participation in low- and low-middle-income countries would allow for greater representation from a diversity of countries, regions, and burn care facilities.
Burn injuries are a leading cause of death and disability among children globally (1–4). The World Health Organization (WHO) estimates that burn injuries account for ~180,000 deaths annually and are the fifth most common cause of non-fatal childhood injuries (5). The burden of child mortality due to burn injuries reflects the inequity of risk factors and care capacity, as rates of child deaths from burns are over seven times higher in low- and middle-income countries when compared to high-income countries (5). Due to the high risk of mortality for burn-injured patients, the physical and psychosocial impacts on people living with burn injury, and the critical lack of both burn and pediatric care capacity globally, the causes and treatment of pediatric burns deserve special focus (6–8).
Acute pediatric burn management ranges from simple outpatient treatment to complex emergency, critical care, and surgical interventions (9). For children with more severe injuries, critical and surgical care capacity consisting of pediatric airway management, sedation for frequent wound care, surgical debridement and reconstruction, tailored nutritional support, and multidisciplinary rehabilitation services are vital for survival and successful long-term outcomes. However, comprehensive resources for pediatric burn care are not readily available globally (10). A study of Ugandan anesthetists demonstrated that only 13% of those surveyed had the supplies necessary to deliver safe anesthesia to a child (11). Reports from Ghana, Nepal, Mexico, India, and Vietnam suggest that lack of emergency and critical care capabilities, and specialty trained personnel, are common barriers to successful outcomes (6, 12, 13). Outside of high-income countries, availability of burn care resources are variable and often limited (4, 14, 15). Although a significant body of research focuses on burn prevention, there is a dearth of information about the burn care capacity in a diversity of locations, specifically the unique needs of burn-injured children.
Burn injuries can have significant psychological, social, and economic impacts on a child's life and the lives of their caregivers (16). Data regarding pediatric global burn trends is inconsistent and frequently extrapolated from single-center or country-specific studies that fail to provide a clear understanding of the global problem (15, 17). To address gaps in epidemiological understanding of global burn trends and availability of key resources, WHO established the Global Burn Registry (GBR), a central platform for the collection and analysis of burn injuries worldwide. The GBR was designed to define global burn injury epidemiology, support prevention initiatives, and benchmark quality improvement activities (18). Our aim was to describe the epidemiology of and capacity for treating pediatric burn injuries worldwide as represented by the WHO GBR.
The WHO launched the Global Burn Registry in 2017 to improve understanding of burn injuries and care capacity worldwide. The validated data collection form utilized by participating health facilities was developed through the collaboration of experts from the WHO, International Society for Burn Injuries (ISBI), and Global Alliance for Clean Cookstoves. Participating facilities utilize a data collection toolkit, initially recorded on a paper form, and later electronically transcribed and uploaded into the GBR. The finalized version of the data collection form, implementation specifics, and ideal uses was published by the group (18). The GBR is continuously updated and stored on network servers located in Geneva, Switzerland at WHO headquarters. Public and private versions of the registry data are available. Public data are modified to remove potential patient identifiers. For this study the public WHO GBR data were accessed via https://www.who.int/teams/social-determinants-of-health/safety-and-mobility/burns/global-burn-registry on September 17, 2021.
Data were extracted for patients aged ≤ 18 years and were grouped into age categories based on childhood developmental stages: infants (<1 year), toddlers and preschoolers (1–5 years), grade schoolers (6–12 years), and adolescents (13–18 years) (19). Descriptive statistics were used to highlight patient demographics, burn injury risk factors, burn injury characteristics, outcomes (including in-hospital death, discharge with disability), and facility capabilities (access to critical care, an operating theater, nutrition services, physical therapy and rehabilitation services, blood transfusion, and internet connectivity).
The GBR contained data from 8,640 patients with burn injuries from 20 countries: Argentina, Chile, China, Estonia, Ethiopia, India, Iran, Kenya, Laos, Mexico, Nepal, Nigeria, Pakistan, Peru, Philippines, Russian Federation, Saudi Arabia, South Africa, Sri Lanka, and Tanzania. Of entries in the GBR, 3,649 (42%) were children. The mean age of this group was 5.3 years (SD 5.01). Children aged 1–5 years comprised 62% (n = 2,279) of the pediatric cohort and 26% of all burn injuries recorded in the GBR. School aged children (age 6–12 years) were the next most frequently burn-injured group with 20% (n = 732) of pediatric burns recorded by the GBR, followed by adolescents (age 13–18 years) at 13% (n = 487). The overwhelming majority of pediatric patients were from centers in middle-income countries (99%, n = 3,628). More boys (60%) were reported than girls (40%) (Table 1).

Table 1. Pediatric patient demographics.
We defined three burn categories based on data in the GBR which included flame, scald, and other (i.e., burns that were chemical, cooling, electrical, friction, or hot surface related). For all pediatric patients, scald burns were the most common (involving contact with hot liquid, steam, or gas) and accounted for 62% of all pediatric burns reported (n = 2,261) followed by flame burns (27%, n = 997). Children 1-5 years sustained the highest proportion of scald burns (80%, n = 1,826); flame burns only accounted for 14% of burns in this age group (n = 320). Children older than 5 years (grade schoolers and adolescents, n = 1,219) more frequently sustained flame burns (52%, n = 628) followed by scald burns (29%, n = 348). Adolescents (age 13–18 years, n = 487) had the highest frequency of admissions for flame burns at 60% (n = 292) as well as burns of any age group being categorized as “other” (25%, n = 122) (Table 2).
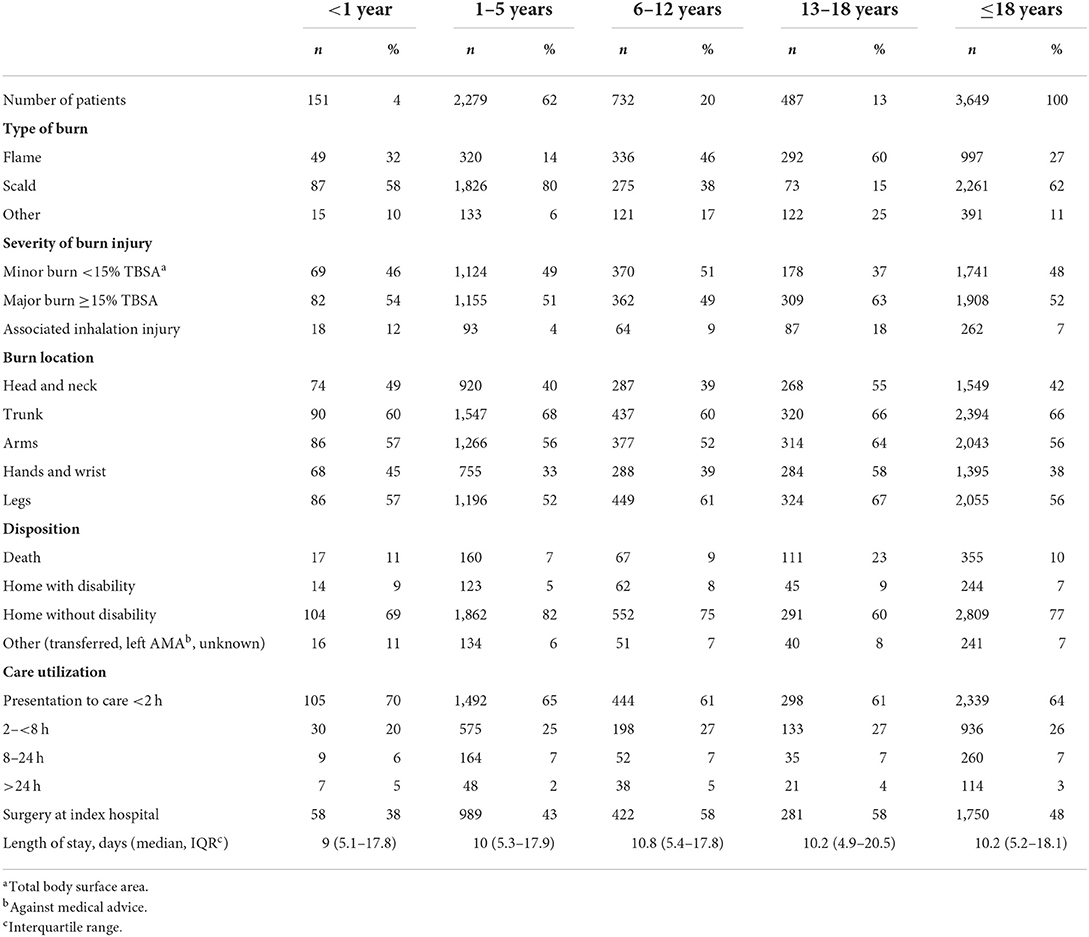
Table 2. Pediatric burn injury etiology, characteristics, and outcomes.
The severity of burns also noticeably varied across age groups. We defined major burns as affecting a total body surface area (TBSA) ≥15% (20). More than half of children (52%, n = 1,908) sustained a major burn. Adolescents (age 13–18 years, n = 487) sustained more severe burns more frequently than other age groups (63% with major burns, n = 309) and commonly had associated inhalation injuries (18%, n = 87) (Table 2).
In terms of burn location, the most frequent area of the body injured was the trunk (66%, n = 2,394); 56% of children sustained burns on their arms or legs (n = 2,043 and n = 2,055). Hand and wrist burns were most frequent amongst adolescents (58%, n = 284) and affected 38% (n = 1,395) of all pediatric patients. Almost half of patients (48%, n = 1,750) received surgery for wound closure while hospitalized. The median length of stay was 10.2 days (IQR 5.2–18.1 days). Adolescents experienced the highest frequency of death (23%, n = 111). For all pediatric patients in the GBR, 10% died during hospitalization (n = 355); 7% of children (n = 244) were discharged home with a disability (as defined by the contributing burn care facility) (Table 2).
The majority of children (64%, n = 2,339) were cared for by the contributing healthcare facility within 2 h of their injury, and 90% (n = 3,275) arrived or were transferred to a contributing hospital within 8 h of injury. Most children were treated in government-operated hospitals (86%, n = 3,143). Participating facilities reported their capacity in terms of critical care (e.g., distinct unit or beds with more care than those on general wards), access to an operating theater, nutrition services, physical therapy and rehabilitation services, blood transfusion capability, and internet connectivity. Of these centers, 23% (n = 832) had limited availability of critical care services. Reliable access to an operating theater was reported by 92% (n = 3,375) of participating facilities. There was limited blood transfusion capability in 19% (n = 703) and physical therapy and rehabilitation services in 14% (n = 502) of facilities. Almost a third of facilities (30%, n = 1,113) reported general nutrition capability with enteral feeds and nasogastric feeds, and 70% (n = 2,536) indicated advanced nutrition capability (e.g., person-centered nutritional support program) (Table 3).
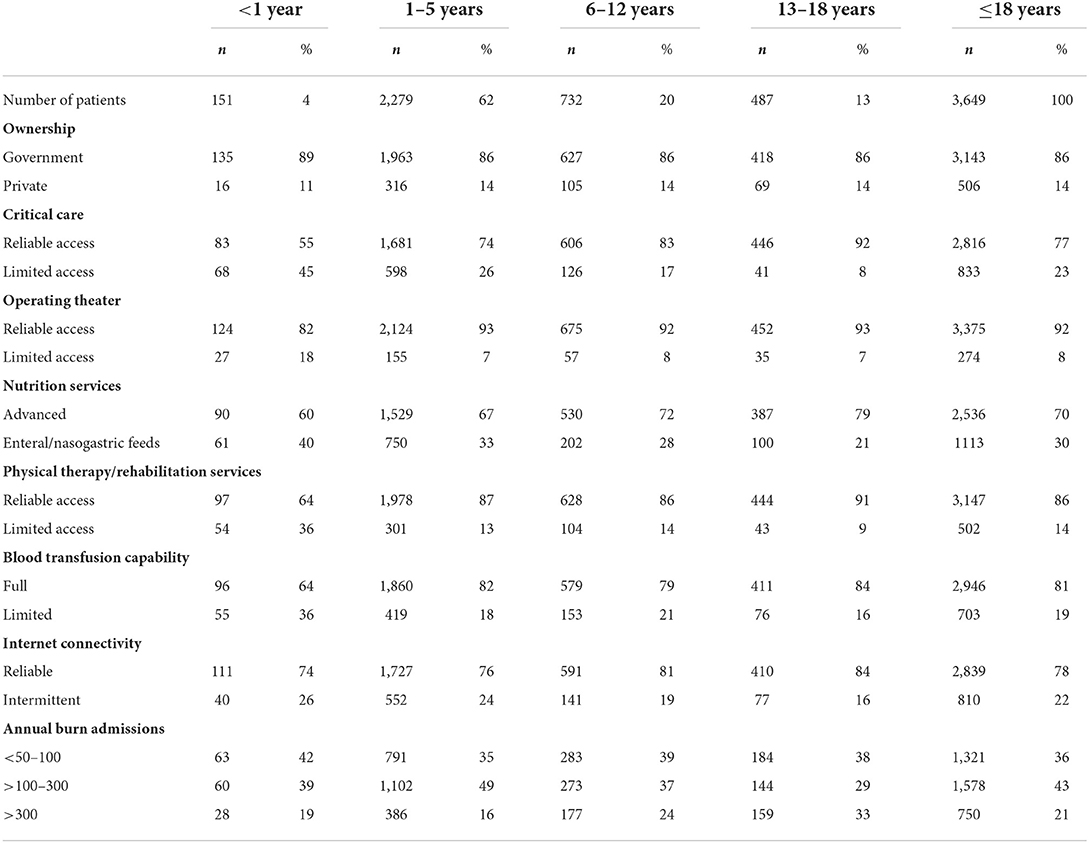
Table 3. Burn facility characteristics.
The WHO GBR is an open-access database that was created to improve understanding of global burn injury epidemiology, identify key prevention targets, and inform quality improvement measures through a standardized and centralized data collection system. This study utilized the WHO GBR to describe the epidemiology of global pediatric burns and evaluate it as a tool for monitoring facility capacity when it comes to the care of burn-injured children. The GBR demonstrates that children (age ≤ 18 years) represent almost half of burn injuries globally (42%) and young children (age 1–5 years) comprise the greatest proportion of pediatric burn injuries (62% of children ≤ 18 years, 26% of all GBR entries). Approximately half of the children in the GBR sustained a major burn (≥15% total body surface area, 52%) and required surgical wound closure (48%). The volume and severity of pediatric burn injuries warrants robust pediatric emergency, critical care, and surgical capacity, however current GBR data demonstrates that critical care capacity is limited in almost a quarter of participating facilities (23%) the majority of which are in middle income countries. Given the prevalence of childhood burn injuries as demonstrated by current GBR data, dedicated efforts to improving participation in the GBR from a diversity of regions and healthcare facilities, as well as evaluating pediatric emergency, critical, and surgical care systems are essential for improving pediatric burn care globally.
The GBR is the first database to allow global monitoring of pediatric burn injury trends, outcomes, and burn care capacity via participating facilities. The GBR demonstrates that the pediatric burn trends observed are consistent with prior smaller, single-center studies that reported young children aged <5 years are the most frequently burned (21), and scald injuries are the most common type of pediatric burn followed by flame burns, particularly in adolescents (1, 22, 23). Current GBR data shows that over half of pediatric patients sustain major burns that would necessitate treatment in a burn center with pediatric emergency and critical care services; however, almost a quarter of pediatric patients were treated in facilities with limited availability of adult critical care, let alone pediatric-specific capabilities. In resource limited settings, access to pediatric critical care providers is limited (10, 24) and the concept of dedicated burn care is often not recognized, with most burn injured patients receiving care from hospital specialists or general surgeons with no specific burn injury training (14). Delays in resuscitation also lead to increased mortality; a study of pediatric burn care in Sub-Saharan Africa found that in Nigeria administration of intravenous saline and dextrose were based on availability and were often not given to children with major burn injuries (25). Pediatric-focused assessments of emergency, surgical, and critical care capacity can be helpful in documenting current equipment and personnel needs at the facility level (6). The availability of personnel trained to employ pediatric emergency care equipment is an important component of effective care and resource utilization (12, 24). Evaluation of pediatric burn care capabilities at the facility level could help improve not only pediatric burn outcomes, but pediatric trauma, respiratory failure, diarrhea, and sepsis outcomes as well; given that shared capabilities are required to manage these emergency conditions. Given the prevalence of child burn injuries globally, and the frequent absence of trained personnel and pediatric specific equipment (10, 24), facility assessment of pediatric capacity is another facet of equitable burn care that the GBR could explore.
Although there is suggestion that burn care and outcomes for children are improving globally (26), the geographic and socioeconomic distribution of high-quality burn care remains inequitable (4, 14, 27, 28). Currently, children under five years of age in sub-Saharan Africa have over twice the incidence of burn deaths compared to children under five worldwide (5). The GBR has the potential to gather and monitor epidemiologic burn data from a diverse range of countries and facilities in response to concerted efforts to improve global trauma care (e.g., dissemination of WHO Emergency Care System products, global promulgation of Advanced Trauma Life Support, uptake of Interburns Quality Improvement Framework at national levels). Currently, the GBR contains data from only 20 countries, with an even smaller number reporting the bulk of current burn data. Additionally, most of the facilities participating in the GBR are in middle-income countries. Thus, facilities in low- and low-middle-income countries, the most likely to contribute to preventable morbidity and mortality, are not being captured by the GBR. It is unclear what the most pressing barriers to participation are currently. There are potential language barriers, as the form is only available in English, French, and Spanish. There are also potential barriers related to human capacity, as healthcare providers in resource limited settings are often stretched into multiple roles in an already overburdened system (25), or due to limited access to reliable internet, as both are necessary to gather and upload data into the GBR. Shifting data entry responsibilities to staff outside of nurses and doctors and improving access to the GBR database via mobile devices might improve participation in certain settings. For facilities with already strained resources, efforts to understand demand-side incentives might also contribute to more rapid and broader uptake of GBR involvement (e.g., including GBR contribution as verification criteria, linking contributions to capacity building initiatives). Assessment of the resources to improve the adoption, penetration, and sustainability of GBR in low- and low-middle-income countries should be pursued.
In addition to the challenges of participating in the GBR, there is also a lack of pediatric-focused assessments that could inform how to improve facility capacity for pediatric burn care. At its inception, the goal of the GBR was to move from a fragmented approach to a standardized, global data collection system to improve public health measures. However, high-quality pediatric burn care requires specialized equipment, monitoring, and personnel that the GBR is not currently capturing (e.g., availability of multiple sizes of supplies, pediatric-specific care knowledge and skills). According to the GBR, over half of the pediatric cohort sustained a burn that would warrant transfer to a burn center with a pediatric intensive care unit, specialized surgical care, and rehabilitation (at a minimum, a volume requirement of >100 children per year) (20, 29). Over a third of facilities in the GBR treating pediatric patients (36%) would not qualify as a burn center according to these criteria. The GBR describes availability of critical care at participating facilities and current data demonstrates insufficient adult critical care capacity. Including availability of pediatric critical care would better inform pediatric burn care capabilities for children with the highest risk of mortality. This would not only establish resuscitation and airway management expertise but would also encompass advanced skill related to pediatric specific post-operative care, procedural sedation and analgesia, nutrition needs in the setting of critical illness, and comfort with patients spanning a broad range of developmental stages.
Part of acute burn care involves surgical debridement and reconstruction (e.g., skin grafting, soft-tissue flap coverage). Children are at increased risk of morbidity due to contractures after a burn as they are smaller and have thinner skin, and a similar injury will cause a deeper burn and more extensive skin loss compared to an adult (22). However, many centers in low-income countries are lacking critical resources including operating time, dedicated burn surgeons, anesthetists, and nurses (14, 25). Currently, GBR participants document access to an operating theater, indicating the potential presence but not the availability of surgeons and anesthetists, and currently there is no way of assessing their capability in terms of pediatric specific care. The capacity for pediatric general anesthesia is often limited in low-resource settings, this is commonly due to the lack of pediatric specific equipment and supplies in addition to human resources (11). A study of pediatric trauma supplies in Ghana showed a consistent scarcity of pediatric-sized items and lack of training when compared to adult-sized items (6). Potential indicators of basic pediatric anesthesia capabilities include an adequate oxygen supply, suction, pulse oximeter, but more specifically a range of pediatric face masks, laryngoscopes, endotracheal tubes, oropharyngeal airways, and breathing circuit (11).
Although equipment and human capacity can have significant impacts on acute burn care, preexisting malnutrition or anemia can also delay the decision to operate as nutritional status is an important consideration for successful burn recovery after surgery (25). Currently the GBR reports whether there are advanced nutritional services vs. general enteral feeding or nasogastric feeding capabilities. However, nutritional needs for children vary by age, with young children being at the highest risk of inadequate nutrition. This coupled with preexisting malnutrition can contribute to increased risk of morbidity and mortality from a burn injury (25). Early feeding in patients with severe burn injuries minimizes the effects of hypermetabolism and catabolism, reduces risk of malnutrition, promotes healing, and decreases length of stay in the ICU (30, 31). However, successful enteral and parenteral feeding is resource intensive, and assessing whether a pediatric patient received supplemental nutrition aids in capturing resource use and can help support burn service planning (32). Assessing a child's nutritional status with a height and weight measurement upon admission and discharge could inform a child's nutritional status at the time of a burn injury, this in addition to documentation of early enteral nutrition could highlight capacity needs for pediatric focused nutrition.
There are multiple limitations to discuss related to this work. First, participation in the GBR is voluntary and therefore not representative of all facilities or communities within a participating country (33). Similarly, a small number of middle-income countries are contributing the largest proportion of data to the GBR, which is currently lacking significant participation from both high-income and low-income countries. This limits the GBR from providing a comprehensive picture of global burn trends to the experience of a much smaller number of centers. Lastly, and most relevant to this study, pediatric specific care capacity information is not currently being collected by the GBR. In settings with limited resources and limited access to providers with specialized skills and equipment, management of pediatric burns constitutes a major challenge that warrants attention from the GBR. Table 4 proposes a pediatric module for assessing the unique capacity needs of burn injured children. Most of these data are already collected currently by the GBR and bolded text are examples of additional information that could inform pediatric burn care capacity in diverse hospital settings. Further exploration of this module would require additional discussion and piloting.
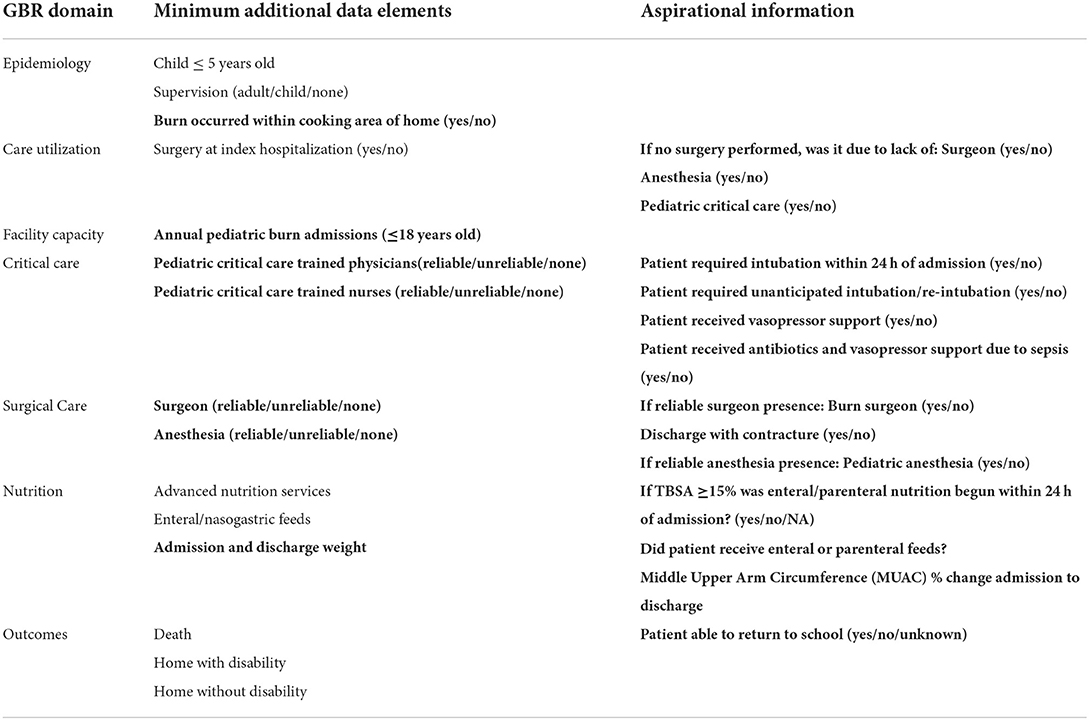
Table 4. Potential global burn registry pediatrics module.
Children experience a large proportion of burn injuries globally and management of pediatric burns is demanding even in the most advanced settings. Current GBR data shows that pediatric patients make up almost half of burn injuries worldwide (42%) and young children (age 1–5 years) comprise the greatest proportion of pediatric burn injuries (62% of children ≤ 18 years, 26% of all GBR entries). Children with burn injuries commonly require unique emergency, surgical, and critical care capabilities, however this study reveals that there is still work to be done to improve capacity for quality comprehensive burn care globally. With greater representation from a diversity of regions and burn care facilities, better understanding of barriers to promulgation and implementation, and addition of modules for key populations for quality improvement initiatives, the GBR will be an excellent resource for monitoring global burn injury trends.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
KJ conceived and designed analysis, performed analysis, and wrote the paper. JD conceived and designed analysis, contributed data and analysis tools, assisted with performing analysis, and assisted with writing the paper. AS assisted with analysis design and writing the paper. BS conceived and designed analysis, contributed data and analysis tools, and assisted with writing the paper. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Atiyeh BS, Costagliola M, Hayek SN. Burn prevention mechanisms and outcomes: Pitfalls, failures and successes. Burns. (2009) 35:181–93. doi: 10.1016/j.burns.2008.06.002
2. Forjuoh SN. Burns in low- and middle-income countries: A review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns. (2006) 32:529–37. doi: 10.1016/j.burns.2006.04.002
3. Grudziak J, Snock C, Zalinga T, Banda W, Gallaher J, Purcell L, et al. Pre-burn malnutrition increases operative mortality in burn patients who undergo early excision and grafting in a sub-Saharan African burn unit. Burns. (2018) 44:692–9. doi: 10.1016/j.burns.2017.10.003
4. Peck MD. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns. (2011) 37:1087–100. doi: 10.1016/j.burns.2011.06.005
5. World Health Organization. Burns. World Health Organization (2018). Available online at: https://www.who.int/news-room/fact-sheets/detail/burns (accessed March 30, 2022).
6. Ankomah J, Stewart BT, Oppong-Nketia V, Koranteng A, Gyedu A, Quansah R, et al. Strategic assessment of the availability of pediatric trauma care equipment, technology and supplies in Ghana. J Pediatr Surg. (2015) 50:1922–7. doi: 10.1016/j.jpedsurg.2015.03.047
7. Butler EK, Tran TM, Nagarajan N, Canner J, Fuller AT, Kushner A, et al. Epidemiology of pediatric surgical needs in low-income countries. Arez AP, editor. PLoS ONE. (2017) 12:e0170968. doi: 10.1371/journal.pone.0170968
8. Kai-Yang L, Zhao-Fan X, Luo-Man Z, Yi-Tao J, Tao T, Wei W, et al. Epidemiology of pediatric burns requiring hospitalization in China: A literature review of retrospective studies. Pediatrics. (2008) 122:132–42. doi: 10.1542/peds.2007-1567
9. Esparaz JR, Anderson SA, Chen MK, Beierle EA. Who manages burn injuries in children? A program director survey evaluating burn training during pediatric surgery fellowship. J Pediatr Surg. (2022) 57:127–9. doi: 10.1016/j.jpedsurg.2021.09.017
10. Tripathi S, Kaur H, Kashyap R, Dong Y, Gajic O, Murthy S. A survey on the resources and practices in pediatric critical care of resource-rich and resource-limited countries. J Intensive Care. (2015) 3:40. doi: 10.1186/s40560-015-0106-3
11. Hodges SC, Mijumbi C, Okello M, McCormick BA, Walker IA, Wilson IH. Anaesthesia services in developing countries: defining the problems. Anaesthesia. (2007) 62:4–11. doi: 10.1111/j.1365-2044.2006.04907.x
12. Mock C, Nguyen S, Quansah R, Arreola-Risa C, Viradia R, Joshipura M. Evaluation of trauma care capabilities in four countries using the WHO-IATSIC guidelines for essential trauma care. World J Surg. (2006) 30:946–56. doi: 10.1007/s00268-005-0768-4
13. Potokar T, Bendell R, Chamania S, Falder S, Nnabuko R, Price PE. A comprehensive, integrated approach to quality improvement and capacity building in burn care and prevention in low and middle-income countries: An overview. Burns J Int Soc Burn Inj. (2020) 46:1756–67. doi: 10.1016/j.burns.2020.05.029
14. Ahuja RB, Bhattacharya S. Burns in the developing world and burn disasters. BMJ. (2004) 329:447–9. doi: 10.1136/bmj.329.7463.447
15. Gupta S, Wong EG, Mahmood U, Charles AG, Nwomeh BC, Kushner AL. Burn management capacity in low and middle-income countries: A systematic review of 458 hospitals across 14 countries. Int J Surg. (2014) 12:1070–3. doi: 10.1016/j.ijsu.2014.08.353
16. Woolard A, Hill NTM, McQueen M, Martin L, Milroy H, Wood FM, et al. The psychological impact of paediatric burn injuries: a systematic review. BMC Public Health. (2021) 21:2281. doi: 10.1186/s12889-021-12296-1
17. Burd A, Yuen C. A global study of hospitalized paediatric burn patients. Burns. (2005) 31:432–8. doi: 10.1016/j.burns.2005.02.016
18. Peck M, Falk H, Meddings D, Sugerman D, Mehta S, Sage M. The design and evaluation of a system for improved surveillance and prevention programmes in resource-limited settings using a hospital-based burn injury questionnaire. Inj Prev. (2016) 22(Suppl 1):i56–62. doi: 10.1136/injuryprev-2015-041815
19. Choi M. Child Development Guide: Ages Stages. CHOC(2021). Available online at: https://www.choc.org/primary-care/ages-stages/ (accessed June 15, 2022).
20. Johnson SA, Shi J, Groner JI, Thakkar RK, Fabia R, Besner GE, et al. Inter-facility transfer of pediatric burn patients from U.S. Emergency Departments. Burns. (2016) 42:1413–22. doi: 10.1016/j.burns.2016.06.024
21. Mashreky SR, Rahman A, Chowdhury SM, Giashuddin S, SvanstrÖm L, Linnan M, et al. Epidemiology of childhood burn: Yield of largest community based injury survey in Bangladesh. Burns. (2008) 34:856–62. doi: 10.1016/j.burns.2007.09.009
22. Meng F, Zuo KJ, Amar-Zifkin A, Baird R, Cugno S, Poenaru D. Pediatric burn contractures in low- and lower middle-income countries: A systematic review of causes and factors affecting outcome. Burns. (2020) 46:993–1004. doi: 10.1016/j.burns.2019.06.001
23. Wesson HKH, Bachani AM, Mtambeka P, Schulman D, Mavengere C, Stevens KA, et al. Pediatric burn injuries in South Africa: A 15-year analysis of hospital data. Injury. (2013) 44:1477–82. doi: 10.1016/j.injury.2012.12.017
24. Muttalib F, González-Dambrauskas S, Lee JH, Steere M, Agulnik A, Murthy S, et al. Pediatric emergency and critical care resources and infrastructure in resource-limited settings: A multicountry survey*. Crit Care Med. (2021) 49:671–81. doi: 10.1097/CCM.0000000000004769
25. Albertyn R, Bickler SW, Rode H. Paediatric burn injuries in Sub Saharan Africa—an overview. Burns. (2006) 32:605–12. doi: 10.1016/j.burns.2005.12.004
26. Haagsma JA, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany EC, et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study (2013). Inj Prev. (2016) 22:3–18. doi: 10.1136/injuryprev-2015-041616
27. Atiyeh B, Masellis A, Conte C. Optimizing burn treatment in developing low- and middle-income countries with limited health care resources (part 1). Ann Burns Fire Disasters. (2009) 22:121–5.
28. Davé DR, Nagarjan N, Canner JK, Kushner AL, Stewart BT. Rethinking burns for low & middle-income countries: Differing patterns of burn epidemiology, care seeking behavior, and outcomes across four countries. Burns. (2018) 44:1228–34. doi: 10.1016/j.burns.2018.01.015
29. Suman A, Owen J. Update on the management of burns in paediatrics. BJA Educ. (2020) 20:103–10. doi: 10.1016/j.bjae.2019.12.002
30. Clark A, Imran J, Madni T, Wolf SE. Nutrition and metabolism in burn patients. Burns Trauma. (2017) 5:11. doi: 10.1186/s41038-017-0076-x
31. Shahi N, Skillman HE, Phillips R, Cooper EH, Shirek GP, Goldsmith A, et al. Why Delay? Early enteral nutrition in pediatric burn patients improves outcomes. J Burn Care Res. (2021) 42:171–6. doi: 10.1093/jbcr/iraa129
32. Gong J, Singer Y, Cleland H, Wood F, Cameron P, Tracy LM, et al. Driving improved burns care and patient outcomes through clinical registry data: A review of quality indicators in the Burns Registry of Australia and New Zealand. Burns. (2021) 47:14–24. doi: 10.1016/j.burns.2020.01.005
Keywords: global health, pediatric burn injuries, pediatric critical care, global burn registry, low-middle income countries (LMIC), low resource settings, burn
Citation: Jordan KC, Di Gennaro JL, von Saint André-von Arnim A and Stewart BT (2022) Global trends in pediatric burn injuries and care capacity from the World Health Organization Global Burn Registry. Front. Pediatr. 10:954995. doi: 10.3389/fped.2022.954995
Received: 27 May 2022; Accepted: 27 June 2022;
Published: 19 July 2022.
Edited by:
Andreas Schwingshackl, University of California, Los Angeles, United StatesReviewed by:
Kayhan Gurbuz, Adana Numune Training and Research Hospital, TurkeyCopyright © 2022 Jordan, Di Gennaro, von Saint André-von Arnim and Stewart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kelly C. Jordan, a2VsbHkuam9yZGFuLm1kQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.