 Boris Adasevic
Boris Adasevic Daniel Turudic
Daniel Turudic Danko Milosevic
Danko Milosevic
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
GENERAL COMMENTARY article
Front. Pediatr., 21 June 2022
Sec. Pediatric Nephrology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.921939
by Lamot, M., Miler, M., Nikolac Gabaj, N., Lamot, L., Milošević, M., Harjaček, M., et al. (2022). Front. Pediatr. 10:768260. doi: 10.3389/fped.2022.768260
This article aims to analyze the performance of various biomarkers in distinguishing urinary tract infections (UTI) from viral respiratory illness (RI) using receiver operating characteristic (ROC) and logistic regression (LR) (1). We performed a literature search of three widely available databases (Pubmed, Scopus, Medline), which revealed several similar articles discussing differential diagnoses of UTI from viral RI (2–5).
Suprapubic aspiration or catheterization is the preferred method of obtaining an adequate urine sample and reliable urine culture when there is a concern for UTI in children who are not toilet trained. Since bag urine specimens have a high contamination rate (up to 63%), the American Academy of Pediatrics does not recommend using this method to obtain a urine culture in such children. Urine culture obtained by this method cannot be considered a “gold standard.” Since the diagnosis of bacterial UTI in the published study is likely inaccurate, the statement of the commented article, with sensitivity and specificity of sCal identifying bacterial UTI from RI were 77.6 and 69.0%, respectively, is based on unreliable data (6–11). Since bag urine specimens were used for urine collection, bacterial UTIs were likely overdiagnosed (1).
White blood cell count (WBC) and absolute neutrophil count (ANC) variables analyzed by ROC analysis and univariate binary LR show a higher area under the curve (AUC) and Youden index (YI) values than serum calprotectin (sCal) (Table 4, Table 7). The 95% confidence interval (CI) for AUC in ROC analysis is missing from Table 4, despite being commented on in Results (page 4), and ROC curves for all tested variables have not been illustrated. sCal specificity commented in Results differs between Table 4 and Figure 2 (sCal specificity in Figure 2 and Results—page 4 is 69% vs. 79% in Table 4). Selected results from the predictive model generated by multivariate binary LR were intentionally commented in Results (page 5), but the model itself was not shown. The model should have been presented separately, and variable selection methods (for example forward stepwise, backward stepwise, hierarchical etc.) should have been explained step by step. From the model presented in this manner, it is unclear how the variables were selected and excluded within the model. The prediction values between each and every variable were also not included. Other researchers cannot reproduce the model presented in this manner. This shows a selection bias.
When comparing multiple tests using ROC analysis, it would be necessary to compare multiple ROC curves in a single plot. A pairwise ROC curve analysis can simultaneously compare several diagnostic tests on the same subjects to consider the covariance and significant differences between ROC curves. There is also a significant age difference between UTI cases and viral RI controls (Table 2, UTI age 3.75 (2.0–6.13) vs. 14.0 (5.0–21.25) for viral RI, p < 0.0001). Age is a known confounder that can deviate the ROC curve from its true location in ROC space, thus resulting in over- or under-estimation of its accuracy (12). AUC and Youden index are standard measures of how well a parameter can distinguish between two diseases as they give equal weight to false positive and false negative values. Variables with the same values would have the same proportion of total misclassified patients (13–15). ANC and WBC have more potential for distinguishing between these two diseases above other variables, sCal included.
We found published biomarkers differentiating RI from UTI in children that authors neglected to mention or include in the article. Blood myxovirus resistance protein A has better AUC than sCal (0.96, 95% CI 0.89–1.0) (16).
The authors cite an article analyzing UTIcalc, which uses standard parameters for UTI assessment. UTIcalc was developed to estimate the probability of UTI in children. It reduced testing by 8.1% and decreased the number of missed UTIs and treatment delays, with a faster UTI diagnosis. Why have the authors missed the opportunity to compare UTIcalc with sCal in their work (17)?
The authors also commented an article that describes the superior accuracy of procalcitonin (PCT) for UTI diagnosis (18). The group of children in the cited article without verified renal scarring by DMSA had PCT values (median 0.40; 0.10–8.25) resembling children in the commented article (median 0.31; 0.11–2.05). Children with renal scarring had significantly higher PCT values (9.58, CI 4.0–28.68) (18). As the authors did not perform a DMSA scan, PCT values in commented article correspond with non-complicated UTIs without renal scarring. The high cost of PCT testing was also addressed (1). However, the cost of sCal testing in Croatia is about 30% more than PCT testing 1, (Supplementary data, Table 1).
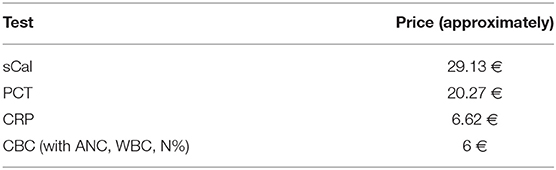
Table 1. Supplementary data—cost of various biomarkers in Croatia.
From the article, it can be deduced that the authors have a dilemma in distinguishing UTIs from viral RI. Recognizing bacterial UTI from viral RI belongs to basic medical skills and can be easily distinguished with clinical examination and common laboratory tests.
From the title itself, and the whole structure of the paper, the article particularly advocates the use of sCal in distinguishing UTIs from viral RI. As sCal is not a new biomarker used to detect bacterial infections, it is unclear why these two diseases were particularly selected for analysis, or what exactly applies to the claim that sCal has “substantial added value in the early management of a child with fever and positive urinalysis?” Are we more and more neglecting basic medical skills at the expense of the ever-increasing and exorbitant price of laboratory testing?
sCal use in routine practice for distinguishing UTIs from viral RI is entirely unacceptable, especially for developing countries and could mislead younger pediatricians about its uncontrolled use.
In most cases, basic medical skills, medical history, clinical examination and follow-up, proper urine sampling and analysis, and simple laboratory tests (WBC, ANC, etc.) are sufficient to distinguish between bacterial UTIs and viral RI. Sophisticated and expensive laboratory tests (sCal included) in no way could supersede the basic medical skills and necessary laboratory tests. This should be the real message of the article.
BA, DT, and DM contributed to conception and design of the study and revised the sections of the manuscript. DT performed the statistical commentary. BA wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lamot M, Miler M, Nikolac Gabaj N, Lamot L, Milošević M, Harjaček M, et al. Serum calprotectin is a valid biomarker in distinction of bacterial urinary tract infection from viral respiratory illness in children under 3 years of age. Front Pediatr. (2022) 10:768260. doi: 10.3389/fped.2022.768260
2. Denis E, Martis N, Guillouet-de Salvador F, Demonchy E, Degand N, Carles K, et al. Bacteraemic urinary tract infections may mimic respiratory infections: a nested case-control study. Eur J Clin Microbiol Infect Dis. (2016) 35:1601–5. doi: 10.1007/s10096-016-2697-6
3. Bouaghroum K, Genillier PL, Neri D, Lameche D, Vassallo M. Prevalence of urinary tract infections mimicking respiratory infections and risk factors associated. Infect Dis. (2018) 50:239–40. doi: 10.1080/23744235.2017.1390249
4. Kim JM, Koo JW, Kim HB. Is it necessary to evaluate urinary tract infection in children with lower respiratory tract infection? J Paediatr Child Health. (2020) 56:1924–8. doi: 10.1111/jpc.15080
5. Bolivar P, de Ponga P, Granda E, Velasco R. Prevalence of urinary tract infection in febrile infants with upper respiratory tract symptomatology. Pediatr Infect Dis J. (2020) 39:e380–2. doi: 10.1097/INF.0000000000002829
6. Tosif S, Baker A, Oakley E, Donath S, Babl FE. Contamination rates of different urine collection methods for the diagnosis of urinary tract infections in young children: an observational cohort study. J Paediatr Child Health. (2012) 48:659–64. doi: 10.1111/j.1440-1754.2012.02449.x
7. Labrosse M, Levy A, Autmizguine J, Gravel J. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. (2016) 138:e20160573. doi: 10.1542/peds.2016-0573
8. Al-Orifi F, McGillivray D, Tange S, Kramer MS. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. (2000) 137:221–6. doi: 10.1067/mpd.2000.107466
9. Bogie AL, Sparkman A, Anderson M, Crittenden-Byers C, Barron M. Is there a difference in the contamination rates of urine samples obtained by bladder catheterization and clean-catch collection in preschool children? Pediatr Emerg Care. (2021) 37:e788–90. doi: 10.1097/PEC.0000000000002578
10. Ballouhey Q, Fourcade L, Couve-Deacon E, Cros J, Lescure V, Bahans C, et al. Urine contamination in nontoilet-trained and uncircumcised boys. Urology. (2016) 95:171–4. doi: 10.1016/j.urology.2016.05.056
11. Subcommittee on Urinary Tract Infection. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. (2016) 138:e20163026. doi: 10.1542/peds.2016-3026
12. Hajian-Tilaki K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Caspian J Intern Med. (2013) 4:627–35.
13. Downing MS. Validity: on the meaningful interpretation of assessment data. Med Educ. (2003) 37:830–7. doi: 10.1046/j.1365-2923.2003.01594.x
14. Feldt LS, Brennan RL. “Reliability”, Educational Measurement. Linn RL, editor. New York, NY: Macmillan Publishing Company (1989).
15. Cook DA, Beckman TJ. Current concepts in validity and reliability for psychometric instruments: theory and application. Am J Med. (2006). 119:166.e7–16. doi: 10.1016/j.amjmed.2005.10.036
16. Piri R, Ivaska L, Yahya M, Toivonen L, Lempainen J, Kataja J, et al. Prevalence of respiratory viruses and antiviral MxA responses in children with febrile urinary tract infection. Eur J Clin Microbiol Infect Dis. (2020) 39:1239–44. doi: 10.1007/s10096-020-03836-5
17. Shaikh N, Hoberman A, Hum SW, Alberty A, Muniz G, Kurs-Lasky M, et al. Development and validation of a calculator for estimating the probability of urinary tract infection in young febrile children. JAMA Pediatr. (2018) 172:550–6. doi: 10.1001/jamapediatrics.2018.0217
Keywords: urinary tract infections, respiratory infections, serum calprotectin, biomarkers, children
Citation: Adasevic B, Turudic D and Milosevic D (2022) Commentary: Serum Calprotectin Is a Valid Biomarker in Distinction of Bacterial Urinary Tract Infection From Viral Respiratory Illness in Children Under 3 Years of Age. Front. Pediatr. 10:921939. doi: 10.3389/fped.2022.921939
Received: 16 April 2022; Accepted: 19 May 2022;
Published: 21 June 2022.
Edited by:
Constantinos J. Stefanidis, “Mitera” Children's Hospital, GreeceReviewed by:
Vaka Kristin Sigurjonsdottir, University of Miami, United StatesCopyright © 2022 Adasevic, Turudic and Milosevic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Turudic, ZGFuaWVsdHVydWRpY0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.