 Rie Wakimizu
Rie Wakimizu Keita Sasaki
Keita Sasaki Mitsuki Yoshimoto
Mitsuki Yoshimoto Akari Miyazaki
Akari Miyazaki Yumiko Saito
Yumiko Saito- 1Department of Child Health Care Nursing, Division of Health Innovation and Nursing, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan
- 2Master Program in Nursing Science, Graduate School of Comprehensive Human Sciences, University of Tsukuba, Tsukuba, Japan
- 3Doctoral Program in Nursing Science, Graduate School of Comprehensive Human Sciences, University of Tsukuba, Tsukuba, Japan
Introduction: Owing to improved prognosis, the number of adult patients with childhood-onset chronic disease (APCCD) has increased. In this systematic review, we evaluated a multidisciplinary approach toward APCCD, focusing on promoting pediatric to adult healthcare transition interventions and their effects.
Methods: We reviewed literature comparing the effects of pediatric to adult healthcare transition interventions in children and adolescents with childhood-onset chronic disease, using PubMed, MEDLINE, and CINAHL, from 2010 to 2021 (keywords: “transition,” “children,” “intervention,” “healthcare,” etc.). The inclusion criteria were as follows: (i) original studies, (ii) studies on pediatric to adult healthcare transition interventions in children with chronic disease, (iii) patients including “adolescents” aged 12 and older receiving intervention, and (iv) studies that included the four elements of the PICO model: Patient/ Problem, Intervention, Comparison and Outcome model.
Results: After evaluating 678 studies, 16 were selected, comprising topics such as “individual education programs” (n = 6), “group meetings” (n = 6), “active learning using information and communications technology” (n = 2), and “transition clinics” (n = 2). The effects obtained varied, depending on the contents and methods of the intervention. Additionally, there was no evidence of adverse outcomes from these interventions.
Conclusions: Pediatric to adult healthcare transition interventions provide systematic support for the transition, patient independence, and social participation; thus, they should be adopted based on their expected effects.
Introduction
Due to the rapid progress in the field of pediatric medicine, including fetal medicine and neonatal care, in recent years, the infant mortality rate per 1,000 births in Japan has decreased from 3.2 (2000) to 1.8 (2020), alongside the neonatal mortality rate reducing from 1.8 (2000) to 0.8 (2020); this trend shows that many lives have been saved during the perinatal period (1). Such advances in medical care have led to a reduction in mortality from childhood-onset diseases (2), and a subsequent increase in the number of adult patients with childhood-onset chronic disease (APCCD). Along with this, support for the transition from pediatric to adult medical care is gaining importance. The transition period to adulthood is one in which physical and psychosocial maturity progresses rapidly even in the developmental stage, alongside new problems due to physical maturity, changes in social roles, maturation of the patient's personality, etc. Therefore, it is necessary to provide seamless medical care in pediatric and adult care.
The transition to adult care is defined as “a purposeful and systematic transition from pediatric to adult care, including the process responsible for managing one's own chronic illness” (3, 4). Self-management for transition includes not only management of illness symptoms but also that of medication and consultation appointment, and communication with healthcare professionals (5). Furthermore, studies investigating the transitional experiences and needs of adolescents with chronic illness have identified a variety of needs. These comprise the importance of peer support; future and occupational issues; pathology and insurance and related information; medication (type, dosage, and side effects); disease knowledge, including understanding of genetic predisposition; difficulty in interacting with the doctor; changes in the doctor-patient relationship due to growth and development; taking responsibility for one's own health; and not relying on parents for disease management (6, 7). Therefore, it is necessary to build comprehensive support for various factors regarding the transition of APCCD to adult medical care.
Even in Japan, interest in adult transitional medical support has been high. In 2015, the Ministry of Health, Labor and Welfare developed tools for transitional support and the “Children with Chronic Specific Diseases Child Transitional Medical Support Model Project” (8), the purpose of which was to improve the transitional medical system by holding training at the pertinent medical institutions. The transitional medical support in this project implied “support for the process of transitioning from pediatrics to adult-centered medical care.” Its goal was to “provide independence support (autonomous support) to encourage patients to acquire self-care skills and actively participate in decision-making, and to lead to appropriate care in adulthood without interrupting necessary care.” Although various adult transition programs aimed at transitional medical support are being developed and evaluated abroad, there are currently no studies that integrate the adult transition programs and their results to evaluate the effectiveness of these interventions.
The PICO (Patient/Problem, Intervention, Comparison, and Outcome) of this study setting was as follows: “Does the adult healthcare transition program for APCCD proceed transition effectively compared with no intervention.” Along with the systematic review, it aimed to integrate the transition support program for the medical support of APCCD and its intervention effect in Japan and overseas, evaluating its effectiveness for adult transition in a multidisciplinary manner.
Methods
Search for Studies
The search date was September 24, 2021, and PubMed, MEDLINE and Cumulated Index to Nursing and Allied Health Literature (CINAHL) were used as the databases. The search target period was set from 2010 to 2021 in each database. Studies were extracted from January 2010 to May 2021 for PubMed, and from January 2011 to December 2020 for both MEDLINE and CINAHL.
Search Keywords for the Papers
The search keywords were a combination of “transition/transfer,” “care/health care/treatment/therapy,” “children/young adult/young people/pediatric,” “intervention,” “chronic disease/chronic illness/APCCD/disease,” and “self-management/selfcare/readiness.”
Inclusion and Exclusion Criteria
Inclusion criteria for this systematic review were as follows: (i) being an original paper; (ii) being a paper on interventions related to adult transition of children with chronic diseases; (iii) including “adolescents,” with the intervention target being individuals aged 12 and older; and (iv) papers with a comparison of the results before and after the intervention being shown. Exclusion criteria for the papers were as follows: (i) the participant had difficulty in self-care due to severely handicapped children, chromosomal abnormalities, intellectual disabilities, etc.; (ii) the paper was intended for palliative care; (iii) the fact-finding survey did not involve intervention; and (iv) the intervention included participants under the target age.
Selection of Target Studies
Excluding duplicate studies from the ones obtained through each database, we perused the titles and abstracts and excluded those that did not fall under P and I of the PICO in this systematic review. We carefully read the entire contents of the papers after the exclusion, eliminated those that lacked pre- and post-comparisons of the intervention, and finally examined the remaining papers. All the authors worked in consultation during each process.
Bias Risk Assessment
The Risk Of Bias In Non-randomized Studies – of Interventions (ROBINS-I) assessment tool (Cochrane | Trusted evidence. Informed decisions. Better health.) was used for the bias risk assessment of the target studies. The tool was capable of measuring confounding, selection, measurement, and missing data, as well as reporting bias, and was ranked low, moderate, serious, no information (NI), and not applicable (NA). The evaluation was conducted independently by the researchers, and the results were shared and discussed among them. Further discussions were held on the suspicions that emerged as a result, and consensus was reached.
Data Extraction Method
From the target papers, “references,” “study design,” “interventions,” “person or group providing interventions,” “participants,” “outcomes,” “main results,” “limits of the study,” and “overall risk of bias” were entered in a table prepared in advance, and made into a list. The data were extracted independently by the researchers, and the results were shared and discussed among them. Based on the opinions obtained through the discussion, the extracted contents were added and revised, and a list was created.
Results
Breakdown of Analysis Target
Of a total of 678 cases obtained from the keywords, the abstract and text were carefully read. And we selected 17 studies, but one of the studies actually did not meet the PICOs. Because of that, we finally analyzed 16 studies. Figure 1 shows the process of selecting the target papers.
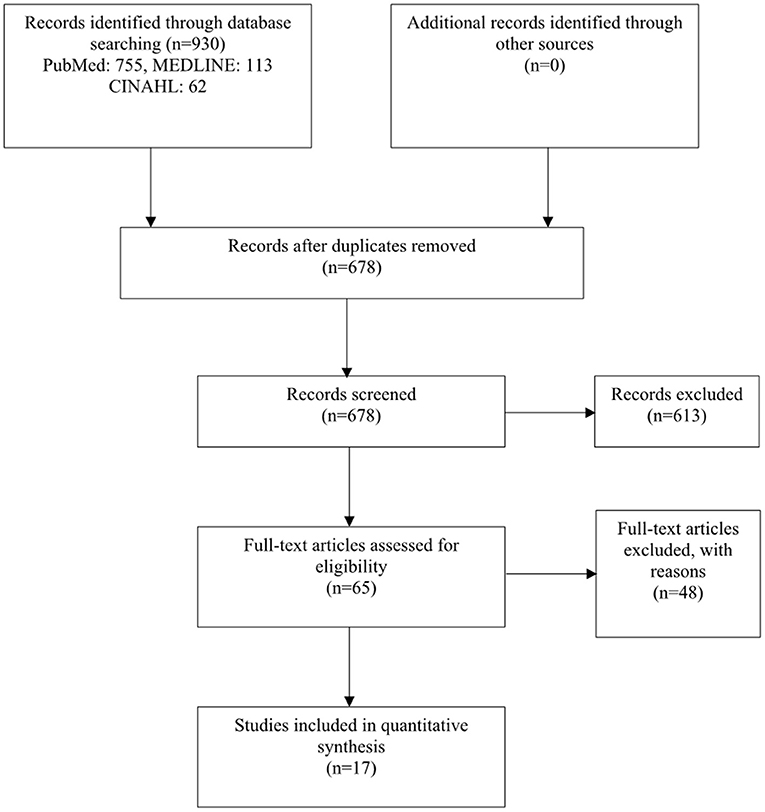
Figure 1. Flowchart of the study selection.
Research Report Year
When the 16 papers considered were classified by their reporting years, one study in 2013 (9), two in 2014 (10, 11), one in 2015 (12), one in 2016 (13), two in 2017 (14, 15), four in 2018 (16–19), two in 2019 (20, 21), and three in 2020 (22–24) were obtained. Of the 16 studies, nine had been reported since 2018, accounting for more than half of the studies considered (Figure 2).
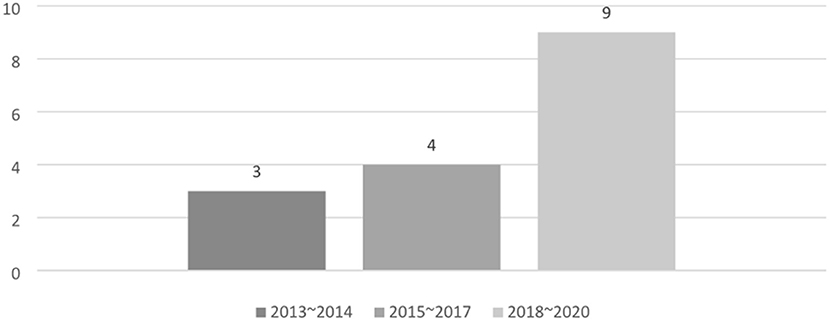
Figure 2. Number of papers by year.
Participants
Most of the studies targeted were regarding the late teens, as they were in the process of transitioning from childhood to adulthood. Of the 16 studies, the minimum age of the target population was 11 years, and the maximum was 25 years.
The breakdown of the diseases examined was shown. Diabetes mellitus (DM) was included in six papers, followed by inflammatory bowel disease (IBD) in five, cystic fibrosis (CF) in four, congenital heart disease (CHD) in four, sickle cell disease (SCD) in two, juvenile idiopathic arthritis (JIA) in one, esophageal atresia (EA) in one, and cardiomyopathy in one. There were six studies involving patients with 2–3 diseases rather than a single disease. Additionally, there was one study on patients with common chronic illnesses, involving 1–6 patients for 15 illnesses (Figure 3).
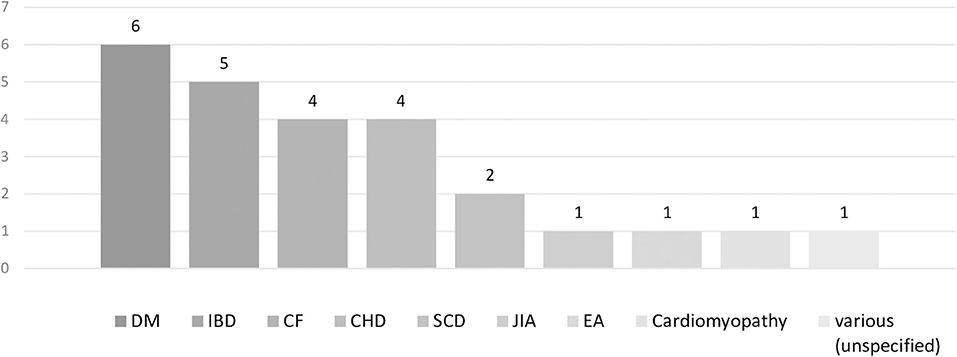
Figure 3. Number of papers by disease of the participant.
Study Design
As a result of classifying the literature by research design, there were six quasi-experimental studies of one-group pre- and post-test design (9, 12, 17, 19–21), seven studies of randomized controlled trial (RCT) research (10, 11, 13, 16, 18, 22, 23), and three non-RCT studies (14, 15, 24). Since the pure experimental study of one-group pre- and post-test design was not a controlled study, it was difficult to determine to what extent interventions and other factors contributed to self-management, transitional readiness, and improved disease activity. In the non-RCT studies, the intervention and control groups were assigned based on the patients' wishes. Therefore, the possibility of selection bias due to the large number of patients or their families who were more interested in the transition from childhood to adulthood could not be ruled out in the intervention group.
Bias Risk Assessment
Bias risk assessment was performed using ROBINS-I for the target studies; one study (11) was assessed to be low, 14 (9, 10, 12–23) were assessed to be moderate, and one (24) was assessed to be serious. The latter was more likely to be biased due to loss of data.
Content of Intervention
The 16 studies analyzed were roughly classified based on the type of intervention. They were classified into four categories: Individual Education Program (IEP) (10, 14–17, 20), Group Meeting (GM) (9, 13, 18, 19, 21, 22), Active Learning using Information and Communications Technology (ALICT) (11, 23), and Transition Clinic (TC) (12, 24) (Figure 4). Educational interventions for coping with the disease and self-management were the actions common to all four groups. From the aspect of patient's age, the characteristics of how the programs were used according to the different ages were not mentioned in any of the studies.
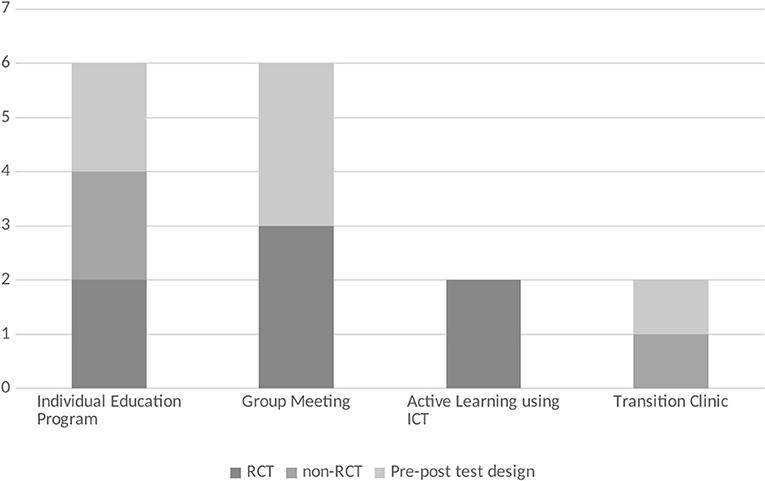
Figure 4. Number of papers by the content of the intervention.
More Specific and Detailed Intervention Content and Its Effects
For each type of intervention, we showed the specific and detailed content of each study and their effects (Table 1).

Table 1. List of study design and intervention contents of review papers.
Individual Education Program
Six studies involved individual programs, in which supporters provided direct face-to-face education, discussions, planning, consultations, follow-ups, etc., according to the requirements of individual patients. The contents of the individual programs were divided into five programs in which supporters provided one-on-one education to patients and their families, and one in which support was mainly provided for planning and implementation. In five education-centered programs, two were conducted as RCT study.
Of the education-centered programs, two RCT (10, 16) and one non-RCT research (14) were programs for CHD patients to gain understanding of diseases, confirmation of the current situation, points to be noted in future daily life, etc., through the creation of a My Health Passport developed in Canada. My Health Passport specifically included CHD anatomy, treatment history, names/amounts/benefits of medications taken, future complications, names and locations of local adult cardiologists, an introduction to a health care website for young people, case study (alcohol, smoking/street drug, sexuality/contraception), introduction to adult CHD clinic consultation, and setting of one education-related goal. The three studies centered on the My Health Passport, including an introduction to adult CHD clinics (16), education on sexually transmitted diseases and substance abuse (10, 14), setting goals for transition, and follow-up (10, 16).
All the three studies found that the intervention group displayed significantly higher knowledge scores for diseases and health than the non-intervention group. In two RCT studies (10, 16) that also included a program with transitional goals and follow-up by healthcare professionals at intervals, self-managed Transition Readiness Assessment Questionnaire (TRAQ) scores were higher than in the non-intervention group in both studies. In addition, compared to the non-intervention group, the transition time from pediatrics to adult specialty was shorter (16), and the self-assertion TRAQ score was higher (10).
A non-RCT study of patients with a history of EA (15) conducted the ModuS-T program developed for patients with type 1 diabetes mellitus (T1DM), IBD, and CF in Germany. Specifically, supporters held discussions with patients and their parents over a 2-day period regarding the changes occurring due to adulthood, examination of changes in the attending physician, health system, stress coping, among others. The study showed improved parental knowledge compared to the non-intervention group, but no significant effect on Health-Related Quality of Life (HRQOL) and self-management ability.
The transition program for patients with CF (17) in Denmark which is conducted as quasi-experimental studies of one-group pre- and post-test design, featured split care for children and parents to create an opportunity for the patient to be seen alone. In addition, two of the 12 consultations a year were held by nurses for 60-min consultations, providing opportunities for consultation on life, self-management, psychosocial risks, and resilience. An annual event for parents was also one characteristic of the program along with individual patient interventions. A mini-lecture on how to deal with chronic diseases and adherence by experts, discussions among parents, and a place to share experiences were provided. The study showed a significant reduction in readiness indicators and respiratory symptoms before and after the intervention.
The study targeting patients with IBD in the United States (20) which is also one-group pretest-posttest design research focused on the formulation and implementation of transition plans. Interviews with patients and their families were conducted by a transition coordinator (social worker) at the time of regular visits. Specifically, during a 15–20-min interview, the IBD Self-Management Handbook was used to explain the concept of transition, provide education on the transition of responsibility from parent to patient, and set migration goals for family and patients. Three months after the interview, a follow-up was conducted on telephone or email regarding the status of the goals set at the time of the interview. The study showed a significant increase in TRAQ transition readiness and self-management ability before and after the intervention.
Group Meeting
The number of studies that involved GMs to promote transition from childhood to adulthood through group education and discussions for patients and parents, was the same as that for IEPs. Among them, by participant, five studies were targeted at children who were patients, and one was targeted at both parents and children.
Of the five studies mainly for children, three RCT (13, 18, 22) were for patients with chronic diseases such as T1DM, CF and IBD in Germany. All programs were offered to four or more patients at a time for two consecutive days, including transition to adult care, health care systems, future plans and professions, illness communication with peers and parents, stress management, etc. The program was primarily conducted by psychologists and pediatricians, and incorporated group-work to facilitate knowledge and information exchange between participants. Of the three studies, in the one on patients with T1DM, CF and IBD (22), and the one on patients with DM and IBD (18), the intervention group had significantly higher empowerment and knowledge scores than the control group. In another study (13) of patients with T1DM, CF and IBD, it was reported that while the transition ability, self-efficacy and satisfaction with school care were significantly higher than in the control group, there was no significant effect on patient activation and quality of life.
Similarly, in a study (9) conducted as one-group pretest-posttest design research in the United States on patients with chronic illness, high school and university students with chronic illness interacted at a dinner party for about 2.5 h every month. After dinner, they were divided into small groups to select and discuss on various topics such as diagnosis, living with illness, and problems that occur at school. Before and after the program centered on the interaction of patients with the same illness, it was reported that the feeling of loneliness decreased and the self-assertion about health care improved.
In a group meeting (21) centered on patients with SCD, a session was held within the group on four questions regarding their own medical condition, self-management of medicines, reservations for medical institutions, etc., after watching a video created for teenage SCD patients transitioning from pediatric to adult care. From this one-group pretest-posttest design research, it was found that drug management, understanding of health problems, communication with medical staff, and improvement of health management in daily life were clarified.
GMs (19) for children with T1DM and their parents in North Africa were held once or twice a year in the pediatrics department of the hospital during school holidays. The group meeting lasted 2–3 h and was attended by 8–12 patients with their families and the hospital's pediatric team (two doctors, one nutritionist, and one nurse), and adult staff including adult endocrine doctors, diabetic nursing educators, nutritionists, and secretaries. Through group meetings, patients and their families had the opportunity to interact with new care providers and raise concerns and questions. Through the one-group pretest-posttest design research, HbA1c levels decreased significantly and more patients achieved HbA1c < 7.5% 1 year after the program intervention.
Active Learning Using ICT
Two programs were identified as ALICT to promote intervention. Both were RCT. There were three specific intervention methods: disease management and learning programs using ICT, and GMs.
Disease management using ICT was conducted in both studies, and it was recommended to provide and use tools for recording symptoms such as the applications “iManage” (23) and “MD2Me” (11). In particular, “iManage,” in addition to self-management such as progress report of self-management goals and input of daily pain and mood discomfort, had provisions for exchanging messages with other participants and sharing of a picture diary of weekly events.
Regarding the learning program (11), information on disease management, communication skills, and lifestyle was provided on the website for 2 months, and self-management in adulthood was learned through case studies by disease. A study (11) that combined ICT disease management and learning programs showed improvements in disease self-management ability, self-efficacy, and patient-led communication.
The ICT GM (23) was used in combination with the in-hospital face-to-face GM to hold a 90-min group session by Zoom. In a study (23) conducted in combination with ICT disease management and GMs, the intervention group had higher self-efficacy and self-management ability than the control group.
Transition Clinic
The TC for the adolescent and young adult (AYA) generation of T1DM or JIA in the Netherlands (12) provided individual intervention conducted with advice from pediatric and adult medical teams for a year, from setting goals to assessing the effectiveness of efforts to improve care. Patients and the medical team discussed with each other about community barriers and shared their experiences in improving adolescent care. In this one-group pretest-posttest design research revealed that the independent behaviors during consultation, general independence, and self-efficacy increased from before the intervention to 1 year after the intervention.
CHD patients in the United States (24) were provided a personalized education program by pediatric cardiologists to assess and promote the preparation and transition of these patients to age-related adult cardiac care. The TC was developed in January 2016 as a monthly subspecialty pediatric heart clinic. Specifically, during the first visit, the method and importance of transition were explained, the degree of understanding of one's own disease was confirmed, an adult cardiovascular clinic was introduced, and goals for self-management were set. During the second and subsequent visits, re-education about heart disease and resetting of self-management goals were conducted. Interviews with adult CHD nurses were also conducted during the intervention. A TC was set up between pediatric and adult care, and the group was recommended for consultation had a higher follow-up rate than the control group. This non-RCT study showed its effectiveness as a program to promote continuous hospital visits and participation in treatment during the transition period.
Discussion
Research Characteristics
The purpose of this systematic review was to provide a multidisciplinary assessment of intervention programs and their effectiveness in supporting the transition of children and adolescents with childhood-onset chronic illness. With the increase in APCCD, support for the transition from pediatric to adult medical care has been emphasized (3), and research reports have been increasing since 2018. DM was the most common disease among the participants of this study, followed by IBD, CF and CHD. In a review of adolescents in transition who require continuous care, the diseases covered were similar to those in this study (26).
Of the 16 research designs, seven were RCTs, six were quasi-experimental studies of one-group pre- and post-test design, and three were non-RCTs, more than half of which were non-RCT research designs. Since the pure experimental study of one-group pre- and post-test design was not a controlled study, it was difficult to determine the extent to which interventions and other factors contributed to self-management, transitional readiness, and improved disease activity. In non-RCT studies, the intervention and control groups were assigned based on the patients' wishes. Therefore, the possibility of selection bias due to the large number of patients or their families who were more interested in the transition from childhood to adulthood, could not be ruled out in the intervention group.
In the bias risk assessment using ROBINS-I, one study had a low overall bias risk, one had serious bias risk, and the rest had moderate bias risk. Bias risks in most studies ranged from moderate to severe, and confounding bias and bias in measuring outcomes were the main factors that underestimated the study quality. The results should, therefore, be interpreted carefully from the study design and bias risk assessment perspective.
The number of RCTs in the four intervention groups was two for IEP, three for GM, two for ALICT, and zero for TC, with no significant differences among the groups other than TC, and the risk of bias in the study design RCTs was Moderate except for one ALICT, which was Low. Based on these results, it was difficult to rigorously estimate which intervention group was more effective.
Intervention Content and Effect
Individual Education Program
The most common transition support intervention program was the IEP. Specifically, the content was to directly provide face-to-face education, discussions, consultations, planning, follow-up, etc. by the supporter, according to the requirements of individual patients. The results of this study and previous studies indicate that there is a wide range of childhood-onset chronic conditions that require transition support (26). In addition, the transition period from childhood to adulthood is a period of rapid physical, psychological, and social maturity. Therefore, it is expected that individual differences will be large in terms of physical and psychological development and changes in social roles. In this way, in order to deal with various diseases and individual situations, it is considered that education and planning are carried out according to individual situations. In many studies, follow-up was conducted not only as a one-time intervention, but also for maintaining the effects.
While many studies included patients and their parents for education, planning and counseling, one study featured interventions regarding the split care of children and parents to facilitate the transition. The purpose of transition support was to support patients' independence and social participation, in addition to a smooth shift from pediatric to adult care (3, 27). Both patients and their parents are the targets of interventions because it is a transitional period from childhood, when parents are responsible for treatment selection and disease management, to adulthood, which aims for patient independence and social participation.
The effects of the IEP included increased knowledge scores regarding illness and health, increased transition preparation scores, increased independence behavior indicators, independence, self-efficacy, improvement of physical symptoms, and shortening the period of consultation from pediatrics to adult specialties. However, one study reported no significant effect on HRQOL and self-management ability. The risk of bias in the study was moderate, and the level of evidence was limited.
Group Meeting
GMs for group education and discussions for patients and parents were the second most common support intervention after IEP. Specifically, discussions were held on disease management, medical care after adult transition, and general life including school life and occupation. While most of the studies were regarding patients only, there was one study which included both parents and children. As an independent support for children with chronic pediatric diseases, it is important to provide a place where patients of the same generation, such as peer groups, can share their worries and exchange information (25, 28). Peers become a primary source of support in mid-adolescence, and peer groups are said to participate in self-selection, self-determination, or social participation through exchanging and sharing experiences, information, and ways of thinking (29, 30). Sharing experiences and information with patients of the same generation having the same disease is considered to be effective for future disease management and life planning.
Similar to the IEP, GMs were attended by pediatric and adult health care providers to interact with new care providers. In addition to doctors and nurses, there were also interventions involving professionals from multiple occupations such as social workers, psychologists, and dietitians. As mentioned above, the objectives of transition support included a smooth shift from pediatric to adult care, and support for patient independence and social participation (3, 27). For a smooth shift from pediatric to adult care, both pediatric and adult health care professionals should participate. In addition, we believe that multidisciplinary interventions are being carried out for a wide range of support, including community life along with disease management.
The effects of GMs have been shown to improve knowledge scores, empowerment scores, self-efficacy, transitional ability, disease management status, and physical status. However, one study reported that there was no significant difference in patient activation and quality of life. The risk of bias in the study was moderate, and the level of evidence was limited.
Active Learning Using ICT
Under ICT interventions, ICT-based disease management and learning programs, as well as, GMs were held. In addition to recommending records related to disease management using applications, providing information on disease management and lifestyle on the website, and content that allows learning of adult self-management through advanced case studies were set. Alongside one-sided transmission of knowledge and information, active learning was devised by exchanging messages with other target people and holding group meetings using Zoom. In recent years, digital therapy using “therapeutic apps” that can change the behavior of patients when they are not visiting the hospital and their way of thinking by acquiring correct knowledge, has attracted attention as a new treatment method in the United States and Europe (31, 32). With the development of ICT, it has spread rapidly, and medical intervention using smartphone applications that are familiar to university students from adolescence, has shown the possibility of smooth symptom and life management (33, 34). We believe that it is also used in intervention programs related to transition support for the same generation.
As an effect of ICT intervention, an increase in disease self-management ability and self-efficacy was observed, and improvement of patient-led communication was shown by devising interactions such as exchanging messages with other participants. All bias risks were moderate, and the level of evidence was limited. However, the use of ICT and the incorporation of further interaction suggested the possibility of a transition-promoting effect.
Transition Clinic
There were two studies in which TCs were set up to assess and promote transition from pediatric to adult care in patients. At the TC, individual education and interviews were conducted by the pediatric and adult health care teams and specialists, such as pediatric cardiologists and adult CHD nurses. Recommendations included assigning doctors with knowledge of transition support to both children and adults, creating teams of specialist nurses, psychological workers, social workers, etc., and establishing organizations for transition outpatients at the American Academy of Pediatrics, the International Society for Pediatric Kidney Disease, etc. (4, 35). Moreover, since many pediatric chronic diseases were highly specific, it was suggested that individual measures should be taken for each disease area, taking into consideration the severity and number of patients (32, 36). Based on these facts, setting up a TC with specialists assigned to each disease area was considered. Although the intervention was shown to be effective in increasing independent behavior, self-efficacy, and continuing hospital visits and promoting participation in treatment during the transition period, the risk of bias was serious and the level of evidence in the study was low.
Limitations
This study had a few limitations. While we clarified the selection criteria and conducted a comprehensive literature search, there is a possibility that the collection of related literature is insufficient, the search being restricted to those available in English only, and also due to the limited availability of databases. Longitudinal studies without a control group did not show a causal relationship. Moderate risk of bias was also reported in studies with control settings and the results should be interpreted with caution. In addition, it was difficult to accumulate research studies based on a clear definition of transition support intervention programs.
Suggestions for Research and Practice
As mentioned above, this systematic review lacked the accumulation of studies based on a clear definition of transition support intervention programs. And it was unclear which actions would have a positive effect on which outcomes. The effectiveness of the intervention may also be influenced by the expertise, skills and attitudes of the intervention program provider. Therefore, future studies will require interventions based on a clear definition of transition support intervention programs, evaluation of which actions are effective for which outcomes, and evaluation of program providers.
In some of the studies considered for this systematic review, both pediatric and adult experts were involved in transition support. Specialists in the pediatric and adult fields are medical providers who can provide specialized medical care through different approaches, and it is expected that these two medical providers will provide seamless care (36, 37). In addition, while the number of patients requiring transition support is increasing, the number of medical staff involved in transition support is currently small, and there is an urgent need to expand the education program for transitional medical care for medical staff (35). It is also important to offer personalized support to young people and their parents when assessing the transition readiness, focusing on self-management skills, illness knowledge, and communication with healthcare professionals (38, 39). For these reasons, the future issues in practice are the cooperation system between the pediatric and adult fields, the construction of a seamless medical care system, and the provision and evaluation of educational programs for transitional medical care for the young people, their parents, and medical professionals.
Conclusion
In this study, we reviewed studies of intervention programs for children and adolescents with childhood onset. The results showed that: (i) DM and IBD were common among the diseases suffered by the study participants, (ii) intervention programs were broadly classified into four categories—IEP, GMs, ALICT and TC, and (iii) education, consultation and planning for disease and disease management through IEPs were common, followed by GMs for group education and discussion. Many studies reported improved knowledge of disease and disease management and improved readiness for transition through the intervention program. Most of the study designs were pre/post comparative studies and RCTs, with the risk of bias being moderate in most of them.
Future challenges include the dissemination of programs with individualized measures for each disease area, as well as the establishment of evaluation and educational methods for program providers.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
RW, KS, MY, and YS: conceived or designed the study. RW, KS, MY, AM, and YS: performed research and wrote the paper. RW, KS, AM, and YS: analyzed data. All authors had full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by Grant-in-Aid for Scientific Research (Grant Number: 22H00490).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the University of Tsukuba URAs for their cooperation, and we would like to thank Editage (www.editage.jp) for English language editing.
Abbreviations
ALICT, Active learning using information and communication technology; APCCD, Adult patients with childhood-onset chronic disease; AYA, Adolescent and young adult; CF, Cystic fibrosis; CFQ-R, Cystic Fibrosis Questionnaire Revised teen/adult version; CHD, Congenital heart disease; CINAHL, Cumulated Index to Nursing and Allied Health Literature; DM, Diabetes mellitus; EA, Esophageal atresia; GM, Group meeting; GSE, General self-efficacy; HRQOL, Health-related quality of life; IBD, Inflammatory bowel disease; IEP, Individual education program; JIA, Juvenile idiopathic arthritis; PAM, Patient activation measure; RCT, Randomized controlled trial; ROBINS-I, Risk of bias in non-randomized studies – of interventions, ; SCD, Sickle cell disease; T1DM, Type 1 diabetes mellitus; TC, Transition clinic; TCS, Transition competence scale; TRAQ, Transition readiness assessment questionnaire.
References
1. Ministry Ministry of Health Labor Welfare. Overview of Vital Statistics (Fixed Number) in 2020. (2021). Available online at: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/kakutei20/index.html (accessed February 27, 2022).
2. Ishizaki Y. Toward the dissemination of transition support programs for adult children with chronic diseases, what has changed with the 2018 revision of medical fees? In: Proceeding of the 121st Annual Meeting of the Japanese Society of Pediatrics; 2018 Apr20-22; Fukuoka. Tokyo (Japan): Journal of the Japan Pediatric Society. (2018). p. 183. Japanese.
3. Blum RW, Garell D, Hodgman CH, Jorissen TW, Okinow NA, Orr DP, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. J Adolesc Health. (1993) 14:570–6. doi: 10.1016/1054-139X(93)90143-D
4. American American Academy of Pediatrics American American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics. (2002) 110:1304–6. doi: 10.1542/peds.110.S3.1304
5. Wood DL, Sawicki GS, Miller MD, Smotherman C, Lukens-Bull K, Livingood WC, et al. The Transition Readiness Assessment Questionnaire (TRAQ): its factor structure, reliability, and validity. Acad Pediatr. (2014) 14:415–22. doi: 10.1016/j.acap.2014.03.008
6. Bomba F, Herrmann-Garitz C, Schmidt J, Schmidt S, Thyen U. An assessment of the experiences and needs of adolescents with chronic conditions in transitional care: a qualitative study to develop a patient education programme. Health Soc Care Community. (2017) 25:652–66. doi: 10.1111/hsc.12356
7. Porter JS, Lopez AD, Wesley KM, Magdovitz-Frankfurt P, Anderson SM, Cole AR, et al. Using qualitative perspectives of adolescents with sickle cell disease and caregivers to develop healthcare transition programming. Clin Pract Pediatr Psychol. (2017) 5:319–29. doi: 10.1037/cpp0000212
8. Ministry Ministry of Health Labor Welfare. Childhood Chronic Specific Illness Child Adult Transitional Medical Support Model Project. (2017). Available online at: https://www.mhlw.go.jp/file/05-Shingikai-10601000-Daijinkanboukouseikagakuka-Kouseikagakuka/0000170347.pdf (accessed February 27, 2022).
9. Maslow G, Adams C, Willis M, Neukirch J, Herts K, Froehlich W, et al. An evaluation of a positive youth development program for adolescents with chronic illness. J Adolesc Health. (2013) 52:179–85. doi: 10.1016/j.jadohealth.2012.06.020
10. Mackie AS, Islam S, Magill-Evans J, Rankin KN, Robert C, Schuh M, et al. Healthcare transition for youth with heart disease: a clinical trial. Heart. (2014) 100:1113–8. doi: 10.1136/heartjnl-2014-305748
11. Huang JS, Terrones L, Tompane T, Dillon L, Pian M, Gottschalk M, et al. Preparing adolescents with chronic disease for transition to adult care: a technology program. Pediatrics. (2014) 133:e1639–46. doi: 10.1542/peds.2013-2830
12. van Staa A, Sattoe JN, Strating MM. Experiences with and outcomes of two interventions to maximize engagement of chronically ill adolescents during hospital consultations: a mixed methods study. J Pediatr Nurs. (2015) 30:757–75. doi: 10.1016/j.pedn.2015.05.028
13. Schmidt S, Herrmann-Garitz C, Bomba F, Thyen U. A multicenter prospective quasi-experimental study on the impact of a transition-oriented generic patient education program on health service participation and quality of life in adolescents and young adults. Patient Educ Couns. (2016) 99:421–8. doi: 10.1016/j.pec.2015.10.024
14. Ladouceur M, Calderon J, Traore M, Cheurfi R, Pagnon C, Khraiche D, et al. Educational needs of adolescents with congenital heart disease: impact of a transition intervention programme. Arch Cardiovasc Dis. (2017) 110:317–24. doi: 10.1016/j.acvd.2017.02.001
15. Dingemann J, Szczepanski R, Ernst G, Thyen U, Ure B, Goll M, et al. Transition of patients with esophageal atresia to adult care: results of a transition-specific education program. Eur J Pediatr Surg. (2017) 27:61–7. doi: 10.1055/s-0036-1592311
16. Mackie AS, Rempel GR, Kovacs AH, Kaufman M, Rankin KN, Jelen A, et al. Transition intervention for adolescents with congenital heart disease. J Am Coll Cardiol. (2018) 71:1768–77. doi: 10.1016/j.jacc.2018.02.043
17. Skov M, Teilmann G, Damgaard IN, Nielsen KG, Hertz PG, Holgersen MG, et al. Initiating transitional care for adolescents with cystic fibrosis at the age of 12 is both feasible and promising. Acta Paediatr. (2018) 107:1977–82. doi: 10.1111/apa.14388
18. Schmidt S, Markwart H, Bomba F, Muehlan H, Findeisen A, Kohl M, et al. Differential effect of a patient-education transition intervention in adolescents with IBD vs. diabetes. Eur J Pediatr. (2018) 177:497–505. doi: 10.1007/s00431-017-3080-z
19. Essaddam L, Kallali W, Jemel M, Kandara H, Kammoun I, Hsairi M, et al. Implementation of effective transition from pediatric to adult diabetes care: epidemiological and clinical characteristics-a pioneering experience in North Africa. Acta Diabetol. (2018) 55:1163–9. doi: 10.1007/s00592-018-1196-x
20. Gray WN, Holbrook E, Dykes D, Morgan PJ, Saeed SA, Denson LA. Improving IBD transition, self-management, and disease outcomes with an in-clinic transition coordinator. J Pediatr Gastroenterol Nutr. (2019) 69:194–9. doi: 10.1097/MPG.0000000000002350
21. Johnson AD, Pines E, Seibenhener S, Wilburn S. Improving transition readiness in young adults with sickle cell disease. J Nurse Pract. (2020) 16:e165–7. doi: 10.1016/j.nurpra.2020.07.026
22. Markwart H, Bomba F, Menrath I, Brenk-Franz K, Ernst G, Thyen U, et al. Assessing empowerment as multidimensional outcome of a patient education program for adolescents with chronic conditions: a latent difference score model. PLoS ONE. (2020) 15:e0230659. doi: 10.1371/journal.pone.0230659
23. Crosby LE, Hood A, Kidwell K, Nwankwo C, Peugh J, Strong H, et al. Improving self-management in adolescents with sickle cell disease. Pediatr Blood Cancer. (2020) 67:e28492. doi: 10.1002/pbc.28492
24. Gaydos SS, Chowdhury SM, Judd RN, McHugh KE. A transition clinic intervention to improve follow-up rates in adolescents and young adults with congenital heart disease. Cardiol Young. (2020) 30:633–40. doi: 10.1017/S1047951120000682
25. Zimmerman C, Garland BH, Enzler CJ, Hergenroeder AC, Wiemann CM. The roles of quality of life and family and peer support in feelings about transition to adult care in adolescents with gastroenterology, renal, and rheumatology diseases. J Pediatr Nurs. (2022) 62:193–9. doi: 10.1016/j.pedn.2021.04.032
26. Campbell F, Biggs K, Aldiss SK, O'Neill PM, Clowes M, McDonagh J, et al. Transition of care for adolescents from pediatric services to adult health services. Cochrane Database Syst Rev. (2016) 4:CD009794. doi: 10.1002/14651858.CD009794.pub2
27. Ishizaki Y. A Guide to Transition Support for Patients With Childhood-Onset Chronic Diseases. Tokyo: Jihou (2018).
28. Tamura A. Development of the structure of chronic illnesses in adolescents for them to obtain information as part of self-care. J Jpn Soc Child Health Nur. (2012) 21:24–31.
29. Nagata M, Miyazato K, Tanaka Y. Recognizing the substantial activities of local citizen's groups for children with chronic diseases. Yokohama J Nur. (2008) 1:26–34.
30. Higginson A, Forgeron P, Harrison D, Finley GA, Dick BD. Moving on: transition experiences of young adults with chronic pain. Can J Pain. (2019) 3:85–97. doi: 10.1080/24740527.2019.1587707
31. Satake K. Changes in medical-related fields in the corona era and the possibility of therapeutic applications using digital therapy. J Health Care Soc. (2021) 31:361–7. doi: 10.4091/iken.31-361
32. Greenwood DA, Gee PM, Fatkin KJ, Peeples M. A systematic review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. (2017) 11:1015–27. doi: 10.1177/1932296817713506
33. Nagamitsu S. Adolescent health promotion through adolescent health screening and CBT application. J Jpn Soc Psychosomatic Pediatr. (2021) 29:359–64.
34. Carey TA, Haviland J, Tai SJ, Vanags T, Mansell W. MindSurf: a pilot study to assess the usability and acceptability of a smartphone app designed to promote contentment, wellbeing, and goal achievement. BMC Psychiatry. (2016) 16:442. doi: 10.1186/s12888-016-1168-z
35. Watson AR, Harden P, Ferris M, Kerr PG, Mahan J, Ramzy MF. Transition from pediatric to adult renal services: a consensus statement by the International Society of Nephrology (ISN) and the International Pediatric Nephrology Association (IPNA). Pediatr Nephrol. (2011) 26:1753–7. doi: 10.1007/s00467-011-1981-z
36. Japan Pediatric Society. Recommendations on Transitional Care for Patients With Childhood-Onset Diseases. (2014). Available online at: http://www.jpeds.or.jp/uploads/files/ikouki2013_12.pdf (accessed March 2, 2022).
37. Rosen DS, Blum RW, Britto M, Sawyer SM, Siegel DM. Society for Adolescent Medicine. Transition to adult health care for adolescents and young adults with chronic conditions: position paper of the Society for Adolescent Medicine. J Adolesc Health. (2003) 33:309–11. doi: 10.1016/S1054-139X(03)00208-8
38. Kuwahara H, Wakimizu R, Kuroki H. Transition readiness assessment tools in patients with chronic conditions: development of Japanese version of the STARx. J Ambulat Gen Pediatr. (2021) 24:2–12.
39. Kuwahara H, Wakimizu R. A transition readiness evaluation tool for the parents of patients with chronic conditions: development of the Japanese version of the STARx (The self-management and transition to adulthood with Rx=Therapeutics) questionnaire parent version. J Child Health. (2021) 80:453–62.
Keywords: childhood-onset chronic disease, systematic review, healthcare transition interventions, multidisciplinary approach, adolescents
Citation: Wakimizu R, Sasaki K, Yoshimoto M, Miyazaki A and Saito Y (2022) Multidisciplinary Approach for Adult Patients With Childhood-Onset Chronic Disease Focusing on Promoting Pediatric to Adult Healthcare Transition Interventions: An Updated Systematic Review. Front. Pediatr. 10:919865. doi: 10.3389/fped.2022.919865
Received: 14 April 2022; Accepted: 25 May 2022;
Published: 14 June 2022.
Edited by:
Yuko Ishizaki, Kansai Medical University, JapanReviewed by:
Dorella Scarponi, Sant'Orsola-Malpighi Polyclinic, ItalyYoshitoki Yanagimoto, Kansai Medical University, Japan
Copyright © 2022 Wakimizu, Sasaki, Yoshimoto, Miyazaki and Saito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rie Wakimizu, cmlld2FraUBtZC50c3VrdWJhLmFjLmpw