 Simona Nicolì
Simona Nicolì Marcello Benevento
Marcello Benevento Davide Ferorelli
Davide Ferorelli Gabriele Mandarelli
Gabriele Mandarelli Biagio Solarino
Biagio Solarino
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Pediatr., 16 September 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.919710
This article is part of the Research TopicChildren's Health and Safety: What We Learned from the COVID-19 Pandemic and Future Policy's PerspectiveView all 12 articles
Patient safety is an emerging healthcare discipline with the ultimate goal to reduce errors and harm to patients by implementing quality health services. In 1999, the well-known “To Err is Human: Building a safer health system” reported that between 2% and 4% of people die annually in United States hospitals for medical errors (1). Since that publication, the focus on healthcare safety has encouraged efforts by legislators, hospital government, and health professionals to promote policies and behaviors heavily to reduce errors and implement a safe provision of healthcare delivery. In 2019, the World Health Organization (WHO) declared September 17th as Patient Safety Day, confirming that as a global priority (2).
The increasing interest in patient safety has significant repercussions on scientific publications with an ever-increasing production of studies in the growing interdisciplinary field of public health. New concepts and new terms had born, such as “clinical risk,” which refers to the probability that a patient can be the victim of an adverse event due to medical care, although unintentionally.
The WHO proposed to adopt a “universal vocabulary” thus standardizing the terminology and allowing effective scientific research. In clinical risk, the most explored field is adult patient safety, where growing interest is shown primarily to prevent nosocomial infections, falls, and pressure injuries. Instead, a little-explored area concerns the pediatric population (3).
This article aims to overview the spread of pediatric clinical risk management and organizational culture for healthcare quality improvement, looking at what has been done and enhancing healthcare practices to implement inpatient safety. The authors have reviewed the main concerns on pediatric patient safety and issued the main medico-legal aspects. After summarizing the relevant literature, the authors addressed their point of view by writing an opinion article.
Nowadays, we are witnessing a growing interest in errors and harm in the pediatric setting, which differ from adults. Standard textbooks and research literature still give little attention to pediatric inpatient primary care and well-being. The short amount available of scientific works is due to children's particular features, characterizing their health management as different and more complex than adults. A study published in 2005 reported that adverse events occurred in children in 1% of pediatric hospitalizations and that 60% of these events were preventable. Other studies suggest that this rate may be higher (4). Table 1 summarizes the main facets of pediatric patient safety.
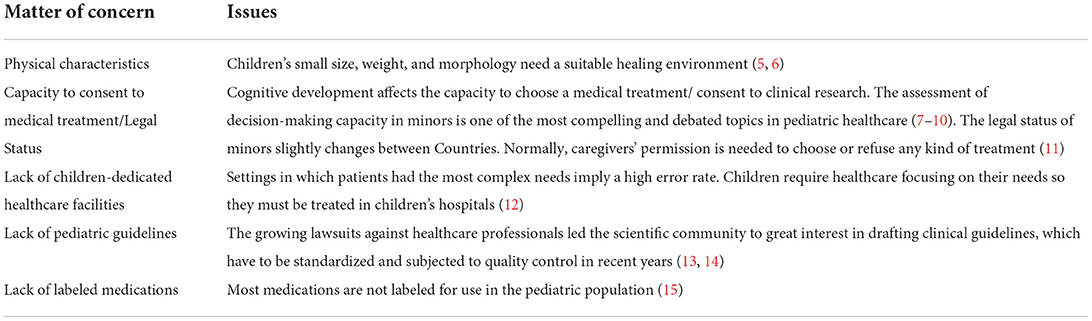
Table 1. Major concerns regarding pediatric patient safety.
Woods highlighted children's physical characteristics can affect the predisposition to errors and harm: weight-based medication dosing, significant variation in size and weight, and predisposition to medical error (5). Moreover, the number of children with chronic diseases and the obesity rate increases, so the physical features of children are sort of changing (16).
It is not unusual for physicians to ask for legal intervention when they believe that a caregiver's refusal of treatment places patients at substantial risk. This phenomenon became most dramatic in pediatric oncology, where the potential need to override caregivers' decision-making when they refuse treatment or replace it with ineffectual alternatives is well-known. Hence the question: are caregivers' rights to make medical decisions on behalf of their children absolute? Decision-making in pediatrics needs a shared approach where children, families, and healthcare multidisciplinary teams cooperate to reach a consensus on decisions in patients' best interests. This “shared” approach is fundamental in pediatric oncology to minimize children's medical and psychosocial impact (17).
The assessment of decision-making capacity for treatment and competence to consent in minors is still far to be validated (18). The acquisition of informed consent is delegated to parents or caregivers, often regardless of their ability to consent to treatment. Since children's capacities develop with growth and experience, their involvement in decisions regarding their health must also increase (19). The involvement of the minor in the diagnostic and therapeutic decision-making process is not solely based on patients' age or ability to read and write and should reduce the stress related to procedures and treatments (20). Some studies have attempted to apply to minors the MacCAT-CR and the MacCAT-T scale in various settings, including the neuropsychiatric one, with surprising results, as adolescents are likely to show the same results as adults (21). Nevertheless, these tools do not have external validation and further research is needed. Finally, all studies regarding this topic emphasize the need to implement communication between minors and parents/caregivers for therapeutic decisions (10, 22).
The outbreak of the COVID-19 pandemic addressed a challenging debate about the administration of new anti-covid vaccines for minors (23). There is a substantial heterogeneity standpoint on this topic in Western Countries. Vaccinating minors to protect them from the COVID-19 virus requires parental permission; the question arises concerning minors' decision-making capacity to consent to such preventive treatment by tracking adults' decisions. In this respect, Morgan et al. suggested a “guide” based on age groups to the consent of minors for the vaccine: is this age-based assessment sufficient? Is it enough to explain to children the benefits and burdens of procedure about a vaccine tested first? One more reason to promote research on assessing children's decision-making capacity for treatment (24).
In addition to these intrinsic factors, the setting of children's care regarding safety is also essential. Currently, the child healthcare system has different intervention levels. Family pediatricians deliver primary care; secondary care is provided in pediatric departments in general hospitals. Children's hospitals were designed to provide optimal care and a multidisciplinary approach to patients and their families (25). Settings in which patients had the most complex needs imply a higher error rate compared with ambulatorial context. The Emergency Department is the place in the pediatric Children's Hospital, where multiple factors related to staff, patients, family members, and pre-hospital communication contribute to various diagnostic and medication mistakes (26).
The healthcare activities carried out in these units often involve multiple urgent interventions for high-risk patients in a complex and stressful environment that exposes children to high frequencies of errors. Applying clinical risk management tools and methodologies changed pediatric intensive care units, reducing medical errors and adverse events and organizational, clinical, and economic impacts, contributing to safety and overall healthcare quality (27). The integrated use of proactive and reactive methods had a growing trend over time, similarly to the increasing use of proactive tools highlighted in two systematic reviews (28, 29).
The pandemic outbreak disclosed the shortages of primary care organizations resulting in inappropriate hospitalizations for non-urgent diseases, thus increasing the risk of errors and unintended harm. Many studies reported a drastic reduction in access to emergency pediatric wards, thus emerging the often inappropriate use of these services (30). The overcrowding of the emergency-urgency department, already characterized by a greater incidence of medical errors, has an even more negative impact on care safety. Therefore, it is evident the need to build a functioning network for the care of the pediatric child, especially concerning primary care (31).
But what about other settings? Although it is evident that some departments are more exposed to risk than others, no hospital ward is risk-free. An interesting article by Lynne Warda reviewed the risks of injury to children in the hospital setting, identifying that those life-threatening hazards mainly concern beds or cribs, concluding that although safety considerations are well entrenched in occupational health and safety, the needs of children are typically not addressed (32). Children require healthcare focusing on their needs. They require more time and specificities for their care; for this reason, these must be treated in children's hospitals where every detail is thought out to optimize patient safety and well-being, from the facilities to the staff specially trained for pediatric care (12).
Another pediatric “silent” crisis, as defined by Corinna Rea, concerns the lack of children's guidelines (13). Some countries favor a more centralized approach to guideline production. Others have a decentralized one, such as the US, where the American Academy of Pediatrics plays the most crucial role in developing guidelines. Decentralization seems to give rise to recommendations' production that may be overlapped, with the consequent detriment of their quality. Moreover, while there is a continuous demand for new guidelines, little importance is given to updating the old ones. Many of these results expired with all their negative consequences: the implementation of obsolete practices that can affect the quality and safety of care and distrust of clinicians and minors' families about the value of outdated guidelines. It is desirable to implement reviewing and validating procedures with greater urgency for the pediatric ones, whose development should be centralized and entrusted to a single organization. Moreover, in a broader perspective, to solve the lack of guidelines and good clinical practices, health practitioners should acquire the so-called “living guidelines” approach for ensuring inpatient high-level quality care: new evidence and recommendations are constantly monitored and possibly updated. A dynamic review approach should ensure the application of the best available practices to the pediatric population, assuring them of high-level quality care to prevent clinical risk (12).
Many barriers exist to conducting pediatric trials, so many therapies used in pediatrics are not evidence-based (15). On the other hand, recent legislation has aimed to stimulate pediatric research and drug labeling (33). In such context, the off-label use of COVID-19 vaccines rises peculiar ethical and legal concerns, as many scientific organizations cautioned against it (34).
In the complex working environment of Children's Hospitals, it is necessary to improve the so-called “safety culture.” It consists, for professionals, in understanding e recognizing problems and risks in safety, understanding that the practice has value both for them and patients. It is also imperative for the hospital to have its safety policies, encouraging tailored and procedures baseline numbers about the safety problems before implementation (35, 36).
In light of these areas of vulnerability, pediatric clinical governance programs deserve specific attention. Several measures and tools could be implemented to reduce errors, promoting the so-called “safety culture”. The efforts to be done can be synthesized in these points:
• Special attention should be paid to training new healthcare professionals and integrating patient safety into ongoing medical education.
• Studies issuing pediatric patient safety should be promoted to improve working knowledge of children's patient safety issues throughout the pediatric community, especially in searching for a validated scale assessing the decision-making capacity of minors.
• Hospitals' safety policies should implement appropriate local procedures and train multidisciplinary teams to seek quality improvement, with a greater focus on the pediatric setting.
• The development process of pediatric guidelines and recommendations should be promoted.
It is our view that one of the best tools for implementing a “safety culture” is the so-called “clinical pathway”, which aims to standardize care processes and improve outcomes without increasing costs or compromising quality. Specifically, clinical pathways aim to integrate evidence into clinical practice and optimize patient outcomes while improving efficiency by translating national guidelines and the latest evidence into the local context. Multidisciplinarity and collaboration between all healthcare professionals are fundamental in the drafting and reviewing process of clinical pathways, also because they measurably improve many aspects of care for pediatric patients. As for guidelines, the spread of clinical pathways should be promoted, and where possible, it would be helpful to create a database to allow their dissemination in as many hospitals as possible and promote collaboration among these.
There is still a long way to go, but multidisciplinarity, the education of young professionals in the culture of safety, and the support of research in less explored fields are the keys to developing a safer healthcare system for pediatric patients.
SN and BS conceived the manuscript. SN, DF, MB, and GM wrote the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Richardson WC, Berwick DM, Bisgard C, Bristow L, Buck CR. To Err is Human: Building a Safer Health System. Washington, D.C.: National Academy Press (2000).
2. World Health Organization. World Patient Safety Day 2019. (2019). Available online at: https://www.who.int/europe/news-room/events/item/2019/09/01/default-calendar/world-patient-safety-day-2019 (accessed February 11, 2022).
3. Group WAFPSD, Sherman H, Castro G, Fletcher M, Hatlie M, Hibbert P, et al. Towards an International Classification for Patient Safety: the conceptual framework. Int J Qual Heal Care. (2009) 21:2–8. doi: 10.1093/intqhc/mzn054
4. Greve P. Pediatrics: A unique and volatile risk. J Healthc Risk Manag. (2011) 31:19–29. doi: 10.1002/jhrm.20084
5. Woods DM, Holl JL, Shonkoff JP, Mehra M, Ogata ES, Weiss KB. Child-specific risk factors and patient safety. J Patient Saf. (2005) 1:17–22. doi: 10.1097/01209203-200503000-00006
6. Ghazali R, Abbas MY. Assessment of healing environment in paediatric wards. Procedia - Soc Behav Sci. (2012) 38:149–59. doi: 10.1016/j.sbspro.2012.03.335
7. van Heerden J, Delport R, Kruger M. Children's ability to consent to medical management in South Africa. SAJCH South African J Child Heal. (2020) 14:25–9. doi: 10.7196/SAJCH.2020.v14.i1.1621
8. Boceta R, Martínez-Casares O, Albert M. The informed consent in the mature minor: Understanding and decision-making capacity. An Pediatr. (2021) 95:413–22. doi: 10.1016/j.anpede.2020.10.011
9. Miano SJ, Douglas SL, Hickman RL, DiMarco M, Piccone C, Daly BJ. Exploration of decisional control preferences in adolescents and young adults with cancer and other complex medical conditions. J Adolesc Young Adult Oncol. (2020) 9:464–71. doi: 10.1089/jayao.2019.0135
10. Mandarelli G, Sabatello U, Lapponi E, Pace G, Ferrara M, Ferracuti S. Treatment decision-making capacity in children and adolescents hospitalized for an acute mental disorder: the role of cognitive functioning and psychiatric symptoms. J Child Adolesc Psychopharmacol. (2017) 27:462–5. doi: 10.1089/cap.2016.0092
11. Vrouenraets LJJJ, de Vries ALC, de Vries MC, van der Miesen AIR, Hein IM. Assessing medical decision-making competence in transgender youth. Pediatrics. (2021) 148:e2020049643. doi: 10.1542/peds.2020-049643
12. Casimir G. Why children's hospitals are unique and so essential. Front Pediatr. (2019) 7:1–5. doi: 10.3389/fped.2019.00305
13. Rea CJ, Alvarez FJ, Tieder JS. The silent crisis of pediatric clinical practice guidelines. JAMA Pediatr. (2021) 175:1201–2. doi: 10.1001/jamapediatrics.2021.2435
14. Cascini F, Contenti M, Scarpetti G, Gelli F, Ricciardi W. Patient safety and medical liability in Italy. Eurohealth (Lond). (2020) 26:34–8.
15. Meliota G, Lombardi M, Benevento M, Console V, Ciccone MM, Solarino B, et al. Off-label use of cardiovascular drugs in the home therapy of children with congenital or acquired heart disease. Am J Cardiol. (2022) 166:131–7. doi: 10.1016/j.amjcard.2021.11.029
16. Nittari G, Scuri S, Petrelli F, Pirillo I, Di Luca NM, Grappasonni I. Fighting obesity in children from European world health organization member states. Epidemiological data, medicalsocial aspects, and prevention programs. Clin Ter. (2019) 170:e223–30. doi: 10.7417/CT.2019.2137
17. Alessandri AJ. Parents know best: Or do they? Treatment refusals in paediatric oncology. J Paediatr Child Health. (2011) 47:628–31. doi: 10.1111/j.1440-1754.2011.02170.x
18. Hein IM, Troost PW, Lindeboom R, Benninga MA, Zwaan C, Michel, Van Goudoever JB, et al. Accuracy of the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR) for measuring children's competence to consent to clinical research. JAMA Pediatr. (2014) 168:1147–53. doi: 10.1001/jamapediatrics.2014.1694
19. Miller VA, Drotar D, Kodish E. Children's competence for assent and consent: A review of empirical findings. Ethics Behav. (2004) 14:255–95. doi: 10.1207/s15327019eb1403_3
20. Coyne I, O'Mathúna DP, Gibson F, Shields L, Leclercq E, Sheaf G. Interventions for promoting participation in shared decision-making for children with cancer. Cochrane Database Syst Rev. (2016) 11:CD008970. doi: 10.1002/14651858.CD008970.pub3
21. Fisher CB, Puri LI, Macapagal K, Feuerstahler L, Ahn JR, Mustanski B. Competence to consent to oral and injectable PrEP trials among adolescent males who have sex with males. AIDS Behav. (2021) 25:1606–18. doi: 10.1007/s10461-020-03077-9
22. Ruhe KM, Wangmo T, Badarau DO, Elger BS, Niggli F. Decision-making capacity of children and adolescents–suggestions for advancing the concept's implementation in pediatric healthcare. Eur J Pediatr. (2015) 174:775–82. doi: 10.1007/s00431-014-2462-8
23. Ferorelli D, Spagnolo L, Marrone M, Corradi S, Silvestre M, Misceo F, et al. Off-label use of COVID-19 vaccines from ethical issues to medico-legal aspects: an italian perspective. Vaccines. (2021) 9:423. doi: 10.3390/vaccines9050423
24. Morgan L, Schwartz JL, Sisti DA. COVID-19 Vaccination of minors without parental consent: respecting emerging autonomy and advancing public health. JAMA Pediatr. (2021) 175:995–6. doi: 10.1001/jamapediatrics.2021.1855
25. Committee on Hospital Care. Family-centered care and the pediatrician's role. Pediatrics. (2003) 112:691–7. doi: 10.1542/peds.112.3.691
26. Kaufmann J, Laschat M, Wappler F. Medikamentenfehler bei Kindernotfällen. Dtsch Arztebl Int. (2012) 109:609–16. doi: 10.3238/arztebl.2012.0609
27. Mueller BU, Neuspiel DR, Stucky Fisher ER, Franklin W, Adirim CT, Bundy DG, et al. Principles of pediatric patient safety: Reducing harm due to medical care. Pediatrics. (2019) 143:e20183649. doi: 10.1542/peds.2018-3649
28. Pilla A Di, Specchia ML, Perilli A, Tofani N, Carini E, Ricciardi W, et al. Impact of clinical risk management in pediatric intensive care units: a systematic review. Eur J Public Health. (2020) 30:ckaa165-603. doi: 10.1093/eurpub/ckaa165.603
29. Specchia ML, Perilli A, Di Pilla A, Carini E, Tofani N, Ricciardi W, et al. The impact of the implementation of clinical risk management tools in pediatric or neonatal intensive care units: a systematic review. Ig Sanita Pubbl. (2020) 76:225–39.
30. Solarino B, Aricò M. Covid-19 pandemic and pediatric healthcare policy in Italy: time for a change. Pediatr Rep. (2020) 12:8823. doi: 10.4081/pr.2020.8823
31. Longhi R, Picchi R, Minasi D, Di Cesare Merlone A. Pediatric emergency room activities in Italy: A national survey. Ital J Pediatr. (2015) 41:1–8. doi: 10.1186/s13052-015-0184-9
32. Warda L. Is your hospital safe for children? Applying home safety principles to the hospital setting. Paediatr Child Health. (2004) 9:331–4.
33. Pasquali SK, Hall M, Slonim AD, Jenkins KJ, Marino BS, Cohen MS, et al. Off-label use of cardiovascular medications in children hospitalized with congenital and acquired heart disease. Circ Cardiovasc Qual Outcomes. (2008) 1:74–83. doi: 10.1161/CIRCOUTCOMES.108.787176
34. Lanphier E, Fyfe S. Pediatric Off-Label Use of Covid-19 Vaccines: Ethical and Legal Considerations. Hastings Cent Rep. (2021) 51:27–32. doi: 10.1002/hast.1296
35. Linden-Lahti C, Holmström A-R, Pennanen P, Airaksinen M. Facilitators and barriers in implementing medication safety practices across hospitals within 11 European Union countries. Pharm Pract (Granada). (2019) 17:1583. doi: 10.18549/PharmPract.2019.4.1583
Keywords: children safety, pediatric clinical pathways, clinical risk management, children's hospital, errors
Citation: Nicolì S, Benevento M, Ferorelli D, Mandarelli G and Solarino B (2022) Little patients, large risks: An overview on patient safety management in pediatrics settings. Front. Pediatr. 10:919710. doi: 10.3389/fped.2022.919710
Received: 13 April 2022; Accepted: 29 August 2022;
Published: 16 September 2022.
Edited by:
Satinder Aneja, Sharda University, IndiaReviewed by:
Maurizio Aricò, Department of Pediatrics, ItalyCopyright © 2022 Nicolì, Benevento, Ferorelli, Mandarelli and Solarino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcello Benevento, bWFyY2VsbG8uYmVuZXZlbnRvQHVuaWJhLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.