
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 28 November 2022
Sec. Pediatric Immunology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.916780
This article is part of the Research TopicState of the Art in Immunopathologic Mechanisms Underlying Preterm Birth Pathways and Biomarkers for Prematurity PredictionView all 6 articles
 Jana Matulova1
Jana Matulova1 Marian Kacerovsky2,3*
Marian Kacerovsky2,3* Radka Bolehovska4
Radka Bolehovska4 Rudolf Kukla4
Rudolf Kukla4 Pavel Bostik4
Pavel Bostik4 Klara Kolarova3
Klara Kolarova3 Simona Frydrychová3
Simona Frydrychová3 Bo Jacobsson5,6,7
Bo Jacobsson5,6,7 Ivana Musilova3
Ivana Musilova3
Objective: To assess the association between newborn birth weight and the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation in pregnancies with preterm labor with intact membranes.
Methods: A total of 69 pregnancies with preterm labor with intact membranes between gestational ages 22 + 0 and 34 + 6 weeks who delivered within seven days of admission were included in this retrospective cohort study. Transabdominal amniocentesis to determine the presence of microorganisms and/or their nucleic acids in amniotic fluid (through culturing and molecular biology methods) and intra-amniotic inflammation (according to amniotic fluid interleukin-6 concentrations) were performed as part of standard clinical management. The participants were further divided into three subgroups: intra-amniotic infection (presence of microorganisms and/or nucleic acids along with intra-amniotic inflammation), sterile intra-amniotic inflammation (intra-amniotic inflammation alone), and without intra-amniotic inflammation. Birth weights of newborns were expressed as percentiles derived from the INTERGROWTH-21st standards for (i) estimated fetal weight and (ii) newborn birth weight.
Results: No difference in birth weights, expressed as percentiles derived from the standard for estimated fetal weight, was found among the women with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation (with infection, median 29; with sterile inflammation, median 54; without inflammation, median 53; p = 0.06). Differences among the subgroups were identified in the birth weight rates, expressed as percentiles derived from the standard for estimated fetal weight, which were less than the 10th percentile (with infection: 20%, with inflammation: 13%, without inflammation: 0%; p = 0.04) and 25th percentile (with infection: 47%, with inflammation: 31%, without inflammation: 9%; p = 0.01). No differences among the subgroups were observed when percentiles of birth weight were derived from the birth weight standard.
Conclusions: The presence of intra-amniotic inflammatory complications in pregnancies with preterm labor with intact membranes prior to the gestational age of 35 weeks was associated with a higher rate of newborns with birth weight less than the 10th and 25th percentile, when percentiles of birth weight were derived from the standard for estimated fetal weight.
Preterm labor with intact membranes (PTL), a clinical phenotype of spontaneous preterm delivery, accounts for approximately one-third of all preterm deliveries (1–3). This serious pregnancy complication, considered as one of “the great obstetrical syndromes” (4, 5), still represents an unsolved problem of current perinatology with global medical and socioeconomic impacts (6).
Almost half of PTL cases are complicated by intra-amniotic inflammation (7, 8), a condition characterized by the elevation of a broad spectrum of pro- and anti-inflammatory mediators in the amniotic fluid (9). This pregnancy complication has two phenotypes depending on the presence or absence of microorganisms and/or their nucleic acids in amniotic fluid: intra-amniotic infection and sterile intra-amniotic inflammation (7, 10, 11). Irrespective of its nature, intra-amniotic inflammation in PTL is associated with (i) a lower gestational age at delivery (7, 8, 12); (ii) a higher rate of Apgar score <7 at 5 and 10 min (12); (iii) a higher prevalence of Ureaplasma spp. in the cervix (8), (iv) a higher frequency of acute inflammatory lesions in the placenta (7); and (v) a higher rate of composite neonatal morbidity (7).
Since the presence of intra-amniotic infection and sterile intra-amniotic inflammation in PTL is associated with a lower gestational age at delivery (7, 8, 12), it is evident that the newborn birth weight from these pregnancies is lower than that of those without intra-amniotic inflammation. However, the possible effect intra-amniotic inflammation on the fetal growth cannot be fully excluded owing to the following previously published data: (i) intra-peritoneal administration of lipopolysaccharide in the second half of pregnancy resulted to reduction of birth weight in a rat animal model (13, 14); (ii) intra-amniotic administration of endotoxin (Escherichia coli) decreased birth weight in a rat animal model (15); (iii) a higher expression of the gene for activator protein-1, a transcription factor in the third trimester, predicted a lower birth weight (16); (iv) elevated maternal systemic concentration of interleukin 17A during pregnancy was associated with low birth weight (17); (v) seropositivity for Helicobacter pylori in the third trimester was related to a higher rate of fetal growth restriction (18); and (vi) periodontal disease incidence/progression during pregnancy was associated with higher frequency of newborns with smaller birth weight for gestational age (19).
Our group recently reported that intra-amniotic infection and sterile intra-amniotic inflammation were associated with lower birth/aborted weight of newborns in pregnancies with cervical insufficiency with prolapsed fetal membranes (20) but not in pregnancies complicated by preterm prelabor rupture of membranes (21). However, there is a lack of information on whether intra-amniotic infection and sterile intra-amniotic inflammation affect fetal growth in pregnancies complicated by PTL.
Therefore, a retrospective study on women with singleton pregnancies complicated by PTL, delivering within seven days from admission (to eliminate the possible effects of corticosteroids and other conditions that might affect fetal growth during a long latency between amniocentesis and delivery) was conducted with the following goals: (i) to assess the difference in birth weight, expressed as percentiles derived from standards for estimated fetal weight and newborn birth weight, between the subgroups of those with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation; and (ii) to compare the rates of birth weights that are less than the 1st, 3rd, 10th, and 25th percentiles among the subgroups with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation.
This retrospective study included pregnant women admitted to the Department of Obstetrics and Gynecology of the University Hospital Hradec Kralove, Czech Republic, between March 2017 and November 2021, who met the following criteria: (i) age ≥18 years; (ii) singleton pregnancy; (iii) gestational age between 22 + 0 and 34 + 6 weeks; (iv) PTL with delivery within seven days of admission; and (v) underwent amniocentesis to assess microbial invasion of the amniotic cavity and intra-amniotic inflammation. The exclusion criteria were as follows: (i) pregnancy-related and other medical complications (chronic hypertension, gestational hypertension, preeclampsia, pregestational diabetes mellitus, and gestational diabetes mellitus); (ii) congenital or chromosomal fetal abnormalities; (iii) signs of fetal hypoxia at the time of admission; (iv) significant vaginal bleeding; and (v) preterm prelabor rupture of membranes.
Gestational age was determined based on the first-trimester fetal biometry. PTL was defined as the presence of regular uterine contractions (at least two every 10 min) along with a cervical length <15 mm on transvaginal ultrasound or cervical length of 15–30 mm with a positive PartoSure test (Parsagen Diagnostics Inc., Boston, MA, United States) (22). Transabdominal amniocentesis was performed at the time of admission before administering corticosteroids, tocolytics, or antibiotics.
Women with PTL received an antenatal course of corticosteroids (betamethasone) and tocolytic therapy with either intravenous atosiban (for gestational age ≤28 weeks) or oral administration of nifedipine for 48 h. Women diagnosed with intra-amniotic inflammation received clarithromycin intravenously for seven days, unless delivery occurred earlier. Antibiotic treatment was eventually modified based on the results of microbial assessments of amniotic fluid. Women with PTL who were positive for the vaginal-rectal presence of Streptococcus agalactiae or did not have these results available received intravenous benzylpenicillin (clindamycin, in case of penicillin allergy) during active labor.
The collection of clinical samples and information from women with PTL was approved by the Institutional Review Board Committee (June 2015; No. 201408 I96L). Written informed consent was obtained from all women. All the women in the study were self-reported as Caucasians. Biological samples (amniotic fluid and cervical fluid) from the women included in this study were used in our previous studies (8, 12, 23).
Ultrasonography-guided transabdominal amniocentesis was performed before administration of corticosteroids, antibiotics, or tocolytics. Details of amniotic fluid sampling have been previously described (12, 23).
The concentration of interleukin (IL)-6 in amniotic fluid was assessed using an automated electrochemiluminescence immunoassay method with the immuno-analyzer Cobas e602 (Roche Diagnostics, Basel, Switzerland) (24). The measurable range was 1.5–5,000 pg/ml, which could be extended to 50,000 pg/ml with a 10-fold dilution of the sample. The coefficients of variation for inter- and intra-assay precisions were both <10%.
Commercial AmpliSens@ C. trachomatis/Ureaplasma/M. hominis-FRT kit (Federal State Institution of Science, Central Research Institute of Epidemiology, Moscow, Russia) was used to detect DNA from Ureaplasma species, M. hominis, and C. trachomatis in the amniotic fluid. The details of this specific PCR run in a single PCR tube have been previously described (12, 23).
Details on the detection of microorganisms and/or their nucleic acids besides Ureaplasma spp., Mycoplasma hominis, and Chlamydia trachomatis in the amniotic fluid using non-cultivation methods and aerobic/anaerobic cultivation have been described previously (12, 23).
All newborns were weighed immediately after birth, using a calibrated electronic scale. Birth weights were transformed into percentiles derived from INTERGROWTH-21st standards (25–28) for: i) estimated fetal weight (26, 28) and ii) newborn birth weight (27).
Microbial invasion of the amniotic cavity was determined based on a positive PCR analysis for Ureaplasma spp., M. hominis, or C. trachomatis or a combination of these microorganisms, positive expression of the 16S rRNA gene, positive aerobic/anaerobic cultivation of the amniotic fluid, or a combination of these parameters. Intra-amniotic inflammation was defined as an amniotic fluid IL-6 concentration ≥3,000 pg/ml (29). Intra-amniotic infection was defined as the presence of microbial invasion of the amniotic cavity and intra-amniotic inflammation. Sterile intra-amniotic inflammation was defined as the presence of intra-amniotic inflammation without microbial invasion of the amniotic cavity.
The demographic and clinical characteristics of the patients were compared using the non-parametric Kruskal-Wallis test for continuous variables and the chi-squared test for categorical variables, and the results are presented as median [interquartile range (IQR)] and number (%), respectively. The normality of the data was tested using the Anderson–Darling test. The percentiles of birth weight were not normally distributed; therefore, the non-parametric Jonckheere-Terpstra test was used for the analyses. The Cochran-Armitage test for trends was used to compare birth weight rates among subgroups. Spearman's partial correlation analysis was performed to adjust the results for a potential confounder (antibiotic administration). Differences were considered statistically significant at p < 0.05. All p-values were determined using two-tailed tests, and all statistical analyses were performed using GraphPad Prism v8 for Mac OS X (GraphPad Software, San Diego, CA, United States) and Statistical Package for Social Sciences (SPSS), version 28.0.0.0, for Windows (SPSS Inc., Chicago, IL, United States).
In total, 94 women with singleton pregnancies complicated by PTL who delivered within seven days of admission were eligible for the study. Twenty-five women were excluded for the following reasons: i) gestational diabetes mellitus (n = 17), ii) preeclampsia (n = 4), pregestational diabetes mellitus (n = 2), and gestational hypertension (n = 2). The remaining 69 women were included in the analysis.
Microbial invasion of the amniotic cavity and intra-amniotic inflammation were observed in 15 (22%) and 47 (68%) women, respectively. The microbial findings from the amniotic fluid were as follows: Ureaplasma spp. + Capnocytophaga ochracea + Fusobacterium nucleatum (n = 1), Lactobacillus spp. + Gardnerella vaginalis (n = 1), Ureaplasma spp. (n = 5), Streptococcus spp. (n = 1), Sneathia sanguinegens (n = 1), Lactococcus lactis (n = 1), Haemophilus influenzae (n = 1), Fusobacterium nucleatum (n = 1), Burkholderia cepacia (n = 1), and non-identifiable bacteria by sequencing (n = 2).
Intra-amniotic infection, sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation were found in 15 (22%), 32 (46%), and 22 (32%) women, respectively. None of the women had microbial invasion of the amniotic cavity without intra-amniotic inflammation.
The demographic and clinical characteristics of the study population with respect to the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation are shown in Table 1.
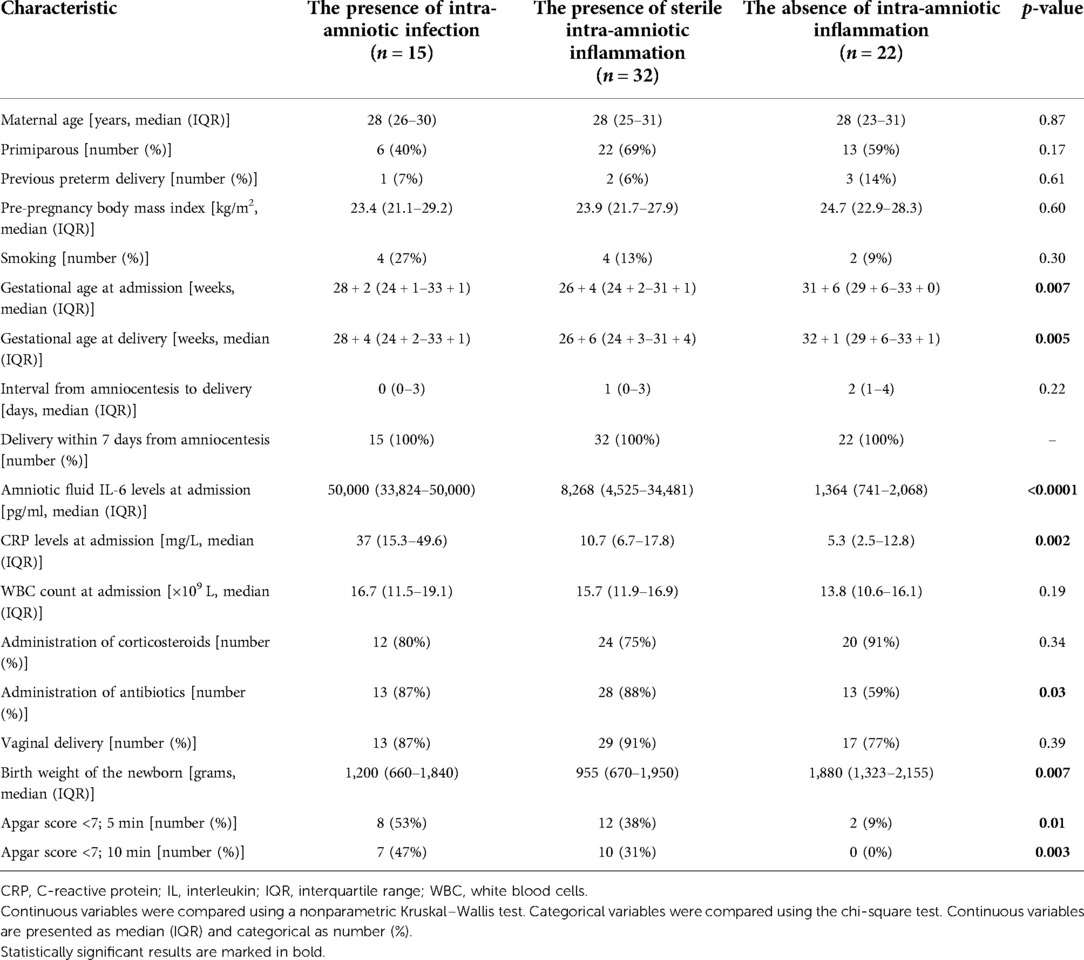
Table 1. Maternal and clinical characteristics of women with preterm labor with intact membranes prior to gestational age 35 weeks with respect to the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation.
No differences were found among the subgroups of women with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation in percentiles of newborn birth weight (the presence of intra-amniotic infection: median 29, IQR 13–62; the presence of sterile intra-amniotic inflammation: median 54, IQR 21–70; the absence of intra-amniotic inflammation 53, IQR 37–78; p = 0.06; Figure 1) and in the rates of the newborn birth weight that were less than the 1st and 3rd percentiles (Table 2). Differences were revealed among the subgroups in the rates of newborn birth weight less than the 10th and 25th percentiles in crude analysis (10th percentile: p = 0.04 and 25th percentile: p = 0.01, Table 2), as well as in the analysis adjusted for administration of antibiotics (10th percentile: p = 0.04; 25th percentile: p = 0.02).
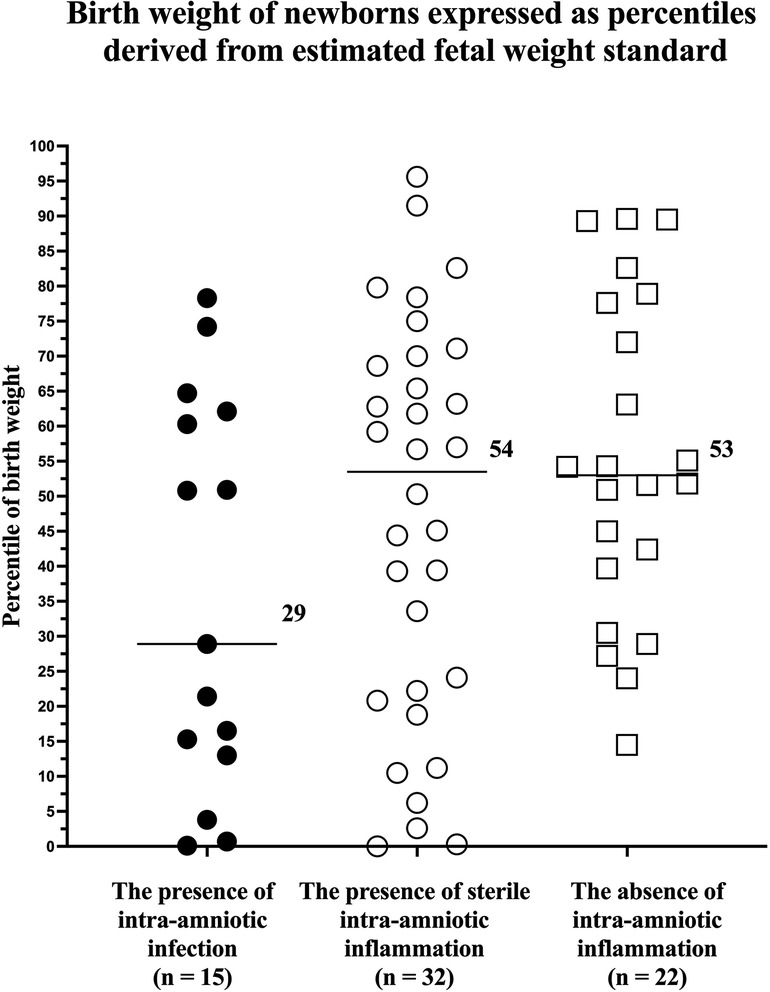
Figure 1. Comparison of newborn birth weight, expressed as percentiles derived from estimated fetal weight standards, from pregnancies with preterm labor with intact membranes prior to a gestational age of 35 weeks with the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation. Medians are marked.

Table 2. The rate of newborns with birth weights, expressed as percentiles derived from estimated fetal weight standards, that were less than or equal to the 1st, 3rd, 10th, and 25th percentiles from pregnancies with preterm labor with intact membranes prior to a gestational age of 35 weeks with the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation.
The INTERGROWTH-21st standards for birth weight are available only for gestational ages ≥24 + 0 weeks. Therefore, it was possible to derive percentiles from these standards only for 80% (12/15), 81% (26/32), and 100% (22/22) of newborns from pregnancies with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation, respectively.
No differences among the subgroup of women with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation were identified in percentiles of newborn birth weight (the presence of intra-amniotic infection: median 54, IQR 35–71; the presence of sterile intra-amniotic inflammation: median 60, IQR 49–71; and the absence of intra-amniotic inflammation: median 52, IQR 44–70; p = 0.98; Figure 2) and in the rates of birth weight that were less than the 1st, 3rd, 10th, and 25th percentiles (Table 3).
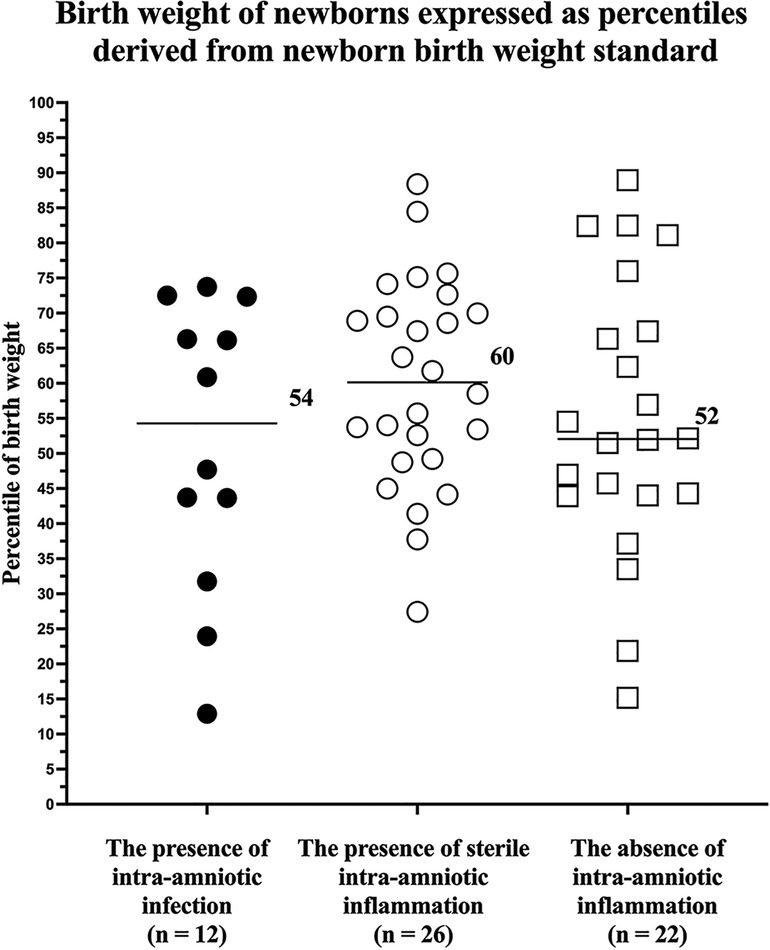
Figure 2. Comparison of newborn birth weight, expressed as percentiles derived from neonatal birth weight standards, from pregnancies with preterm labor with intact membranes prior to a gestational age of 35 weeks with the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation. Medians are marked.

Table 3. The rates of newborns with birth weights, expressed as percentiles derived from birth weight standards, that were less than or equal to the 1st, 3rd, 10th, and 25th percentiles from pregnancies with preterm labor with intact membranes prior to a gestational age of 35 weeks with the presence of intra-amniotic infection, presence of sterile intra-amniotic inflammation, and absence of intra-amniotic inflammation.
The principal findings of the study carried out on women with PTL who delivered within seven days of admission were as follows: (i) no difference in percentiles of birth weight, derived from estimated fetal weight standard, was found among the subgroups of women with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation; (ii) differences in the rates of birth weight that were less than the 10th and 25th percentiles, derived from the standard for estimated fetal weight, were identified among the subgroups of women with intra-amniotic infection, with sterile intra-amniotic inflammation, and without intra-amniotic inflammation; and (iii) no differences among the subgroups were revealed when percentiles were derived from the standard for birth weight.
In this study, no difference in the newborn birth weight, expressed in percentiles derived from the INTERGROWTH-21st standard for estimated fetal weight, was found among the subgroups of PTL pregnancies with intra-amniotic infection, with sterile intra-amniotic inflammation, and without of intra-amniotic inflammation. Nevertheless, the subgroup with intra-amniotic infection had a median percentile of only 29, whereas the medians of the subgroups with sterile intra-amniotic inflammation and without intra-amniotic inflammation reached 54 and 53, respectively. Irrespective of the absence of significant statistical differences among the subgroups, the presence of strong intra-amniotic inflammation (the median IL-6 levels in the amniotic fluid of the subgroup with intra-amniotic infection was 50,000 pg/ml) might have affected fetal growth when compared to the presence of weak intra-amniotic inflammation (the median IL-6 levels in the amniotic fluid of the subgroup with sterile intra-amniotic inflammation was 8,268 pg/ml) or the absence of these conditions. We do not want to overemphasize this observation; however, this hypothesis is further supported by the trend in the rates of newborns with a birth weight less than the 10th and 25th percentiles among the subgroups, with this trend being the highest in those with intra-amniotic infection, lower in those with sterile intra-amniotic inflammation, and the lowest in the absence of inflammation. The difference among the subgroups was revealed only in the cutoff values of the 10th percentile, which is commonly used by clinicians to identify fetuses and newborns with a diagnosis of small for gestational age (30), and the 25th percentile, which represents a cutoff value for the lowest quartile of birth weight that might identify and include a subset of newborns with a mild alteration of fetal growth. However, no association was found between the most severe alteration of fetal growth, represented by the cutoff values of the 1st and 3rd percentiles and both phenotypes of intra-amniotic inflammation. This is in line with observations from a recent animal study, where the intra-amniotic administration of endotoxin (Escherichia coli) at 20 days of gestation (the term is 22 days) led to a 20% and 22% decrease in birth and placental weights, respectively (15). Intra-amniotic administration of endotoxin in the rat model caused not only restriction of fetal and placental growth, but also decreased vascular density of the placenta. This observation is in line with findings from human studies that reported that maternal vascular malperfusion is related to alterations in fetal growth (31–36). In addition, a recent study by Jaiman et al. clearly showed that maternal vascular malperfusion is more frequent in PTL than in uncomplicated pregnancies with delivery at term (37).
Since intra-amniotic infection is considered a cause of cervical insufficiency with prolapsed fetal membranes or PTL rather than a consequence, it is likely that the fetal and placental exposure to this complication might be a long-lasting process compared to preterm prelabor rupture of membranes (PPROM), where this intra-amniotic complication is more likely a consequence. Collectively, the observations from this study are in line with those of our previous studies (20, 21). The results from our studies on the association between intra-amniotic inflammatory complications and cervical insufficiency with prolapsed fetal membranes (20), PPROM (21), and PTL suggest that the possible effect of intra-amniotic inflammation on fetal growth might be dependent on the following: (i) the length of exposure, (ii) the intensity of intra-amniotic inflammation, and iii) several unrecognized underlying endo- and exogenous factors (e.g., impaired placentation).
In this study, aside from the INTERGROWTH-21st standard for estimated fetal weight, the standard for newborn birth weight was also used to derive percentiles for birth weight. When this standard was applied, no differences in percentiles among the subgroups in the rates of birth weight less than the 1st, 3rd, 10th, and 25th percentiles were found. A similar phenomenon was observed in our previous studies (20, 21). We believe that the use of the standard for birth weight in studies such as ours is less appropriate because the standard for birth weight might be affected by the overrepresentation of pathological pregnancies resulting in iatrogenic or spontaneous preterm deliveries where impaired placentation might be expected (38). This limitation of birth weight standard might be seen mainly in the subset of newborns delivered before 33 weeks of gestation (27) and may not identify cases with mildly impaired fetal growth, particularly in newborns delivered very or extremely preterm. Since the subset of newborns delivered before 33 weeks of gestation represented 73% (50/69) of all newborns in this study, it is not surprising that no differences among the subgroups were observed when percentiles derived from the birth weight standard were used.
The main strength of this study was the thorough assessment of microbial invasion of the amniotic cavity based on a combination of three methods to detect microorganisms and/or their nucleic acids in amniotic fluid: (i) aerobic and anaerobic cultivation; (ii) specific PCR for Ureaplasma spp., Mycoplasma hominis, and Chlamydia trachomatis; and (iii) PCR for the 16S rRNA gene followed by sequencing. The employment of such an extensive approach offered us the opportunity to divide the subset of women with intra-amniotic inflammation into those with intra-amniotic infection and those with sterile intra-amniotic inflammation. Second, there is strong evidence that the latency interval between admission and delivery in pregnancy with PTL depends on the presence or absence of intra-amniotic inflammation (7, 8, 12). The latter is associated with a longer latency, which may take weeks instead of days, as is common in those with intra-amniotic inflammation (7, 8, 12). However, a long latency interval might represent a susceptible period for the alteration of fetal growth, independent of the initial intra-amniotic status, due to the possible effect of the antenatal course of corticosteroids (39, 40) or other endo- or exogenous stimuli. To eliminate the effect of a long latency interval, only PTL pregnancies with a meaningful temporal relationship between admission and delivery (≤7 days) were included in this study.
However, this study had some limitations. First, the small cohort of women with PTL used in this study was limited. The monocentric design of the study prevented us from using a larger sample size. Second, the population of women used in this study was homogeneous, involving only Caucasian participants. This potential shortcoming prevents the results of the study from generalizing to populations with broader ethnic and racial disparities. Finally, data regarding ultrasonographically estimated fetal weight obtained at the time of admission were not available. Therefore, we could not compare the percentiles of ultrasonographically estimated fetal weight at the time of admission, derived from the standard for estimated fetal weight, among the subgroups.
In conclusion, in this retrospective cohort study conducted on pregnancies with preterm labor and intact membranes prior to the gestational age of 35 weeks, the presence of intra-amniotic inflammatory complications was associated with a higher rate of newborns with birth weight less than the 10th and 25th percentile, when percentiles of birth weight were derived from the standard for estimated fetal weight.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board Committee University Hospital Hradec Králové. The patients/participants provided their written informed consent to participate in this study.
JM and MK: drafting the paper. JM, MK, RB, RK, PB KK, SF, BJ, and IM: conception and design of the work. JM, MK, KK, SF, and IM: analysis of the data. JM, MK, RB, RK, PB KK, SF, BJ, and IM: revising the draft of the paper critically for important intellectual content. JM, MK, RB, RK, PB KK, SF, BJ, and IM: provided approval for publication. All authors contributed to the article and approved the submitted version.
This work was supported by the Faculty Hospital in Hradec Kralove (a long-term organization development plan).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Romero R, Mazor M, Munoz H, Gomez R, Galasso M, Sherer DM. The preterm labor syndrome. Ann N Y Acad Sci. (1994) 734:414–29. doi: 10.1111/j.1749-6632.1994.tb21771.x
2. Romero R, Dey SK, Fisher SJ. Preterm labor: one syndrome, many causes. Science. (2014) 345(6198):760–5. doi: 10.1126/science.1251816
3. Muglia LJ, Katz M. The enigma of spontaneous preterm birth. N Engl J Med. (2010) 362(6):529–35. doi: 10.1056/NEJMra0904308
4. Di Renzo GC. The great obstetrical syndromes. J Matern Fetal Neonatal Med. (2009) 22(8):633–5. doi: 10.1080/14767050902866804
5. Romero R. Prenatal medicine: the child is the father of the man. 1996. J Matern Fetal Neonatal Med. (2009) 22(8):636–9. doi: 10.1080/14767050902784171
6. Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. (2015) 385(9966):430–40. doi: 10.1016/S0140-6736(14)61698-6
7. Romero R, Miranda J, Chaiworapongsa T, Korzeniewski SJ, Chaemsaithong P, Gotsch F, et al. Prevalence and clinical significance of sterile intra-amniotic inflammation in patients with preterm labor and intact membranes. Am J Reprod Immunol. (2014) 72(5):458–74. doi: 10.1111/aji.12296
8. Kacerovsky M, Stranik J, Kukla R, Bolehovska R, Bostik P, Matulova J, et al. Intra-amniotic infection and sterile intra-amniotic inflammation in women with preterm labor with intact membranes are associated with a higher rate of Ureaplasma species DNA presence in the cervical fluid. J Matern Fetal Neonatal Med. (2021):1–9. doi: 10.1080/14767058.2021.1947231
9. Bhatti G, Romero R, Rice GE, Fitzgerald W, Pacora P, Gomez-Lopez N, et al. Compartmentalized profiling of amniotic fluid cytokines in women with preterm labor. PLoS One. (2020) 15(1):e0227881. doi: 10.1371/journal.pone.0227881
10. Romero R, Miranda J, Chaemsaithong P, Chaiworapongsa T, Kusanovic JP, Dong Z, et al. Sterile and microbial-associated intra-amniotic inflammation in preterm prelabor rupture of membranes. J Matern Fetal Neonatal Med. (2015) 28(12):1394–409. doi: 10.3109/14767058.2014.958463
11. Romero R, Miranda J, Chaiworapongsa T, Chaemsaithong P, Gotsch F, Dong Z, et al. Sterile intra-amniotic inflammation in asymptomatic patients with a sonographic short cervix: prevalence and clinical significance. J Matern Fetal Neonatal Med. (2015) 28(11):1343–59. doi: 10.3109/14767058.2014.954243
12. Stranik J, Kacerovsky M, Andrys C, Soucek O, Bolehovska R, Holeckova M, et al. Intra-amniotic infection and sterile intra-amniotic inflammation are associated with elevated concentrations of cervical fluid interleukin-6 in women with spontaneous preterm labor with intact membranes. J Matern Fetal Neonatal Med. (2021):1–9. doi: 10.1080/14767058.2020.1869932
13. Cotechini T, Hopman WJ, Graham CH. Inflammation-induced fetal growth restriction in rats is associated with altered placental morphometrics. Placenta. (2014) 35(8):575–81. doi: 10.1016/j.placenta.2014.05.002
14. Cotechini T, Komisarenko M, Sperou A, Macdonald-Goodfellow S, Adams MA, Graham CH. Inflammation in rat pregnancy inhibits spiral artery remodeling leading to fetal growth restriction and features of preeclampsia. J Exp Med. (2014) 211(1):165–79. doi: 10.1084/jem.20130295
15. Cookson MW, Ryan SL, Seedorf GJ, Dodson RB, Abman SH, Mandell EW. Antenatal vitamin D preserves placental vascular and fetal growth in experimental chorioamnionitis due to intra-amniotic endotoxin exposure. Am J Perinatol. (2018) 35(13):1260–70. doi: 10.1055/s-0038-1642033
16. Ross KM, Carroll JE, Dunkel Schetter C, Hobel C, Cole SW. Pro-inflammatory immune cell gene expression during the third trimester of pregnancy is associated with shorter gestational length and lower birthweight. Am J Reprod Immunol. (2019) 82(6):e13190. doi: 10.1111/aji.13190
17. Shafiq M, Mathad JS, Naik S, Alexander M, Yadana S, Araujo-Pereira M, et al. Association of maternal inflammation during pregnancy with birth outcomes and infant growth among women with or without HIV in India. JAMA Netw Open. (2021) 4(12):e2140584. doi: 10.1001/jamanetworkopen.2021.40584
18. Eslick GD, Yan P, Xia HH, Murray H, Spurrett B, Talley NJ. Foetal intrauterine growth restrictions with Helicobacter pylori infection. Aliment Pharmacol Ther. (2002) 16(9):1677–82. doi: 10.1046/j.1365-2036.2002.01333.x
19. Offenbacher S, Lieff S, Boggess KA, Murtha AP, Madianos PN, Champagne CM, et al. Maternal periodontitis and prematurity. Part I: obstetric outcome of prematurity and growth restriction. Ann Periodontol. (2001) 6(1):164–74. doi: 10.1902/annals.2001.6.1.164
20. Chalupska M, Kacerovsky M, Stranik J, Gregor M, Maly J, Jacobsson B, et al. Intra-Amniotic infection and Sterile intra-amniotic inflammation in cervical insufficiency with prolapsed fetal membranes: clinical implications. Fetal Diagn Ther. (2021) 48(1):58–69. doi: 10.1159/000512102
21. Matulova J, Kacerovsky M, Bolehovska R, Stranik J, Spacek R, Burckova H, et al. Birth weight and intra-amniotic inflammatory and infection-related complications in pregnancies with preterm prelabor rupture of membranes: a retrospective cohort study. J Matern Fetal Neonatal Med. (2021):1–11. doi: 10.1080/14767058.2021.1956458
22. van Baaren GJ, Vis JY, Wilms FF, Oudijk MA, Kwee A, Porath MM, et al. Predictive value of cervical length measurement and fibronectin testing in threatened preterm labor. Obstet Gynecol. (2014) 123(6):1185–92. doi: 10.1097/AOG.0000000000000229
23. Stranik J, Kacerovsky M, Soucek O, Kolackova M, Musilova I, Pliskova L, et al. IgGFc-binding protein in pregnancies complicated by spontaneous preterm delivery: a retrospective cohort study. Sci Rep. (2021) 11(1):6107. doi: 10.1038/s41598-021-85473-2
24. Fraunberger P, Pfeiffer M, Cremer P, Holler E, Nagel D, Dehart I, et al. Validation of an automated enzyme immunoassay for interleukin-6 for routine clinical use. Clin Chem Lab Med. (1998) 36(10):797–801. doi: 10.1515/CCLM.1998.141
25. Villar J, Papageorghiou AT, Pang R, Ohuma EO, Cheikh Ismail L, Barros FC, et al. The likeness of fetal growth and newborn size across non-isolated populations in the INTERGROWTH-21st project: the fetal growth longitudinal study and newborn cross-sectional study. Lancet Diabetes Endocrinol. (2014) 2(10):781–92. doi: 10.1016/S2213-8587(14)70121-4
26. Stirnemann J, Villar J, Salomon LJ, Ohuma E, Ruyan P, Altman DG, et al. International estimated fetal weight standards of the INTERGROWTH-21(st) project. Ultrasound Obstet Gynecol. (2017) 49(4):478–86. doi: 10.1002/uog.17347
27. Villar J, Cheikh Ismail L, Victora CG, Ohuma EO, Bertino E, Altman DG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project. Lancet. (2014) 384(9946):857–68. doi: 10.1016/S0140-6736(14)60932-6
28. Papageorghiou AT, Ohuma EO, Altman DG, Todros T, Cheikh Ismail L, Lambert A, et al. International standards for fetal growth based on serial ultrasound measurements: the fetal growth longitudinal study of the INTERGROWTH-21st project. Lancet. (2014) 384(9946):869–79. doi: 10.1016/S0140-6736(14)61490-2
29. Musilova I, Andrys C, Holeckova M, Kolarova V, Pliskova L, Drahosova M, et al. Interleukin-6 measured using the automated electrochemiluminescence immunoassay method for the identification of intra-amniotic inflammation in preterm prelabor rupture of membranes. J Matern Fetal Neonatal Med. (2020) 33(11):1919–26. doi: 10.1080/14767058.2018.1533947
30. DiGiulio DB, Gervasi MT, Romero R, Vaisbuch E, Mazaki-Tovi S, Kusanovic JP, et al. Microbial invasion of the amniotic cavity in pregnancies with small-for-gestational-age fetuses. J Perinat Med. (2010) 38(5):495–502. doi: 10.1515/jpm.2010.076
31. Novac MV, Niculescu M, Manolea MM, Dijmarescu AL, Iliescu DG, Novac MB, et al. Placental findings in pregnancies complicated with IUGR - histopathological and immunohistochemical analysis. Rom J Morphol Embryol. (2018) 59(3):715–20.30534809
32. Mifsud W, Sebire NJ. Placental pathology in early-onset and late-onset fetal growth restriction. Fetal Diagn Ther. (2014) 36(2):117–28. doi: 10.1159/000359969
33. Aviram A, Sherman C, Kingdom J, Zaltz A, Barrett J, Melamed N. Defining early vs late fetal growth restriction by placental pathology. Acta Obstet Gynecol Scand. (2019) 98(3):365–73. doi: 10.1111/aogs.13499
34. Salafia CM, Minior VK, Pezzullo JC, Popek EJ, Rosenkrantz TS, Vintzileos AM. Intrauterine growth restriction in infants of less than thirty-two weeks’ gestation: associated placental pathologic features. Am J Obstet Gynecol. (1995) 173(4):1049–57. doi: 10.1016/0002-9378(95)91325-4
35. Salafia CM, Vintzileos AM, Silberman L, Bantham KF, Vogel CA. Placental pathology of idiopathic intrauterine growth retardation at term. Am J Perinatol. (1992) 9(3):179–84. doi: 10.1055/s-2007-999316
36. Tyson RW, Staat BC. The intrauterine growth-restricted fetus and placenta evaluation. Semin Perinatol. (2008) 32(3):166–71. doi: 10.1053/j.semperi.2008.02.005
37. Jaiman S, Romer R, Bhatti G, Jung E, Gotsch F, Suksai M, et al. The role of the placenta in spontaneous preterm labor and delivery with intact membranes. J Perinat Med. (2022) 50(5):553–66. doi: 10.1515/jpm-2021-0681
38. Nicolaides KH, Wright D, Syngelaki A, Wright A, Akolekar R. Fetal medicine foundation fetal and neonatal population weight charts. Ultrasound Obstet Gynecol. (2018) 52(1):44–51. doi: 10.1002/uog.19073
39. Wapner RJ, Sorokin Y, Thom EA, Johnson F, Dudley DJ, Spong CY, et al. Single versus weekly courses of antenatal corticosteroids: evaluation of safety and efficacy. Am J Obstet Gynecol. (2006) 195(3):633–42. doi: 10.1016/j.ajog.2006.03.087
Keywords: amniocentesis, amniotic fluid, estimated fetal weight, fetal growth, intergrowth, intra-amniotic inflammation, microbial invasion of the amniotic cavity, preterm birth
Citation: Matulova J, Kacerovsky M, Bolehovska R, Kukla R, Bostik P, Kolarova K, Frydrychová S, Jacobsson B and Musilova I (2022) Intra-amniotic inflammation and birth weight in pregnancies with preterm labor with intact membranes: A retrospective cohort study. Front. Pediatr. 10:916780. doi: 10.3389/fped.2022.916780
Received: 10 April 2022; Accepted: 7 November 2022;
Published: 28 November 2022.
Edited by:
Offer Erez, Ha'Emek Medical Center, IsraelReviewed by:
Ourlad Alzeus G. Tantengco, University of the Philippines Manila, Philippines© 2022 Matulova, Kacerovsky, Bolehovska, Kukla, Bostik, Kolarova, Frydrychová, Jacobsson and Musilova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marian Kacerovsky a2FjZXJtYXJAZm5oay5jeg==
Specialty Section: This article was submitted to Pediatric Immunology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.