 Xueyan Ma1†Xiangzheng Yang2†Hongzhi Yin2Yang Wang3Yuanshuo Tian4
Xueyan Ma1†Xiangzheng Yang2†Hongzhi Yin2Yang Wang3Yuanshuo Tian4 Chaojun Long1
Chaojun Long1 Chen Bai1
Chen Bai1 Fei Dong1
Fei Dong1 Zhendong Wang1Tiegang Liu1*
Zhendong Wang1Tiegang Liu1* Xiaohong Gu1*
Xiaohong Gu1*- 1School of Traditional Chinese Medicine, Beijing University of Chinese Medicine, Beijing, China
- 2Department of Pediatrics, Beijing University of Chinese Medicine Shenzhen Hospital (Longgang), Shenzhen, China
- 3Beijing University of Chinese Medicine Third Affiliated Hospital, Beijing University of Chinese Medicine, Beijing, China
- 4Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China
Background: The impact of COVID-19 has most likely increased the prevalence of stunting. The study aimed to determine the prevalence of stunting among kindergarten children in the context of coronavirus disease 2019 (COVID-19) in Longgang District, Shenzhen, China, and its risk factors.
Methods: A cross-sectional study was conducted to identify children from 11 sub districts of 481 kindergartens in the Longgang District of Shenzhen City from May to July 2021. In the context of COVID-19, an online survey was conducted to gather demographic information, height, birth information, and lifestyle. The prevalence of stunting was calculated, and the risk factors were analyzed using binary logistic regression with three stepwise models.
Results: A total of 118,404 subjects were included from May to July 2021, with a response and questionnaire effective rates of 85.75% and 95.03%, respectively. The prevalence of stunting and severe stunting were 3.3% and 0.8%, respectively. Model 3 showed that risk factors for stunting were male sex [odds ratio (OR) = 1.07], low birth weight (OR = 2.02), insufficient sleep time (OR = 1.08), less food intake than their peers (OR = 1.66), slower eating than their peers (OR = 1.16), accompanied by grandparents alone or non-lineal relatives (reference: parents accompanying) (OR = 1.23, 1.51), and children induced to eat (OR = 1.17). Protective factors included only-child status (OR = 0.66), reported high activity (OR = 0.37, 0.26, 0.23), parents with high education levels (father: OR = 0.87, 0.69; mother: OR = 0.69, 0.58), high monthly income per capita of the family (OR = 0.88, 0.74, 0.68), and allowing children to make food choices (OR = 0.82).
Conclusion: The stunting rate of children in kindergartens in Longgang District is 3.3%, close to the level of developed countries but higher than the average level of developed cities in China. The relatively high stunting rate in children under 3 years old in 2021 may be associated with the influence of COVID-19. Appropriate policies should be formulated for individuals and families with children to help children establish good living habits and reduce stunting.
Introduction
Stunting refers to the height/length-for-age two standard deviations below the median, according to standard growth charts (1). Studies showed that stunting significantly impacts the life and health of children throughout their lives (including adolescence and adulthood) (2–6). Stunting is a major global health priority and was estimated to affect 22.0% or 149.2 million children under 5 years globally in 2020 (7). The World Health Organization (WHO) proposed a 40% reduction in stunted children as the first of six global nutrition targets by 2025 compared with the baseline data in 2010 (8). Although stunting has declined steadily since 2000, there remain challenges to achieving this goal. Coronavirus disease 2019 (COVID-19) increased the difficulty of achieving the goal. The epidemic has impacted social and economic development. Control of public places, the suspension of kindergartens, and the increase of online courses have affected children’s lives and health (9). The WHO reported that the impact of COVID-19 likely increased the prevalence of stunting (7).
Currently, there is a lack of investigations on the stunting rate among preschool children in areas with rapid economic development against the background of the epidemic affecting social and economic operations. Longgang District is in the northeast of Shenzhen. In recent years, its economy has developed rapidly, ranking first among the top 100 industrial regions in China from 2018 to 2021, according to the China Information and Communication Research Institute (10–13). However, due to the impact of COVID-19 and Sino-American trade friction, the gross domestic product in the Longgang District decreased by 7.6% year on year in 2021 (14). In the present study, we aim to perform a cross-sectional study of the prevalence of stunting in the Longgang District in 2021 and identify the risk factors associated with stunting.
Materials and methods
Study design
We conducted a cross-sectional study of enrolled preschoolers from kindergartens of Longgang District, Shenzhen City, Guangdong Province, in 2021. There are 11 sub districts and 481 kindergartens in Longgang District. Sporadic COVID-19 cases were reported in Shenzhen during the survey. The control measures in kindergartens are strict. Because of the epidemic, we conducted an online questionnaire survey in kindergartens. The information included height, demographic data, birth information, and lifestyle. The prevalence of stunting and risk factors among preschoolers in the Longgang District was analyzed.
Based on the previous literature (15), this paper constructed a conceptual framework for analyzing factors associated with stunting (Figure 1). The framework provided a way to understand that different factors affect each other and jointly lead to stunting. Distal factors such as birthplace, ethics, parents’ qualifications, and other socioeconomic factors can affect height/length through intermediate and proximal factors. Family factors such as primary caregiver at home, number of children, and feeding behavior of caregivers belong to intermediate factors, which can affect height/length through proximal factors. Proximal factors include children’s lifestyle and birth factors.
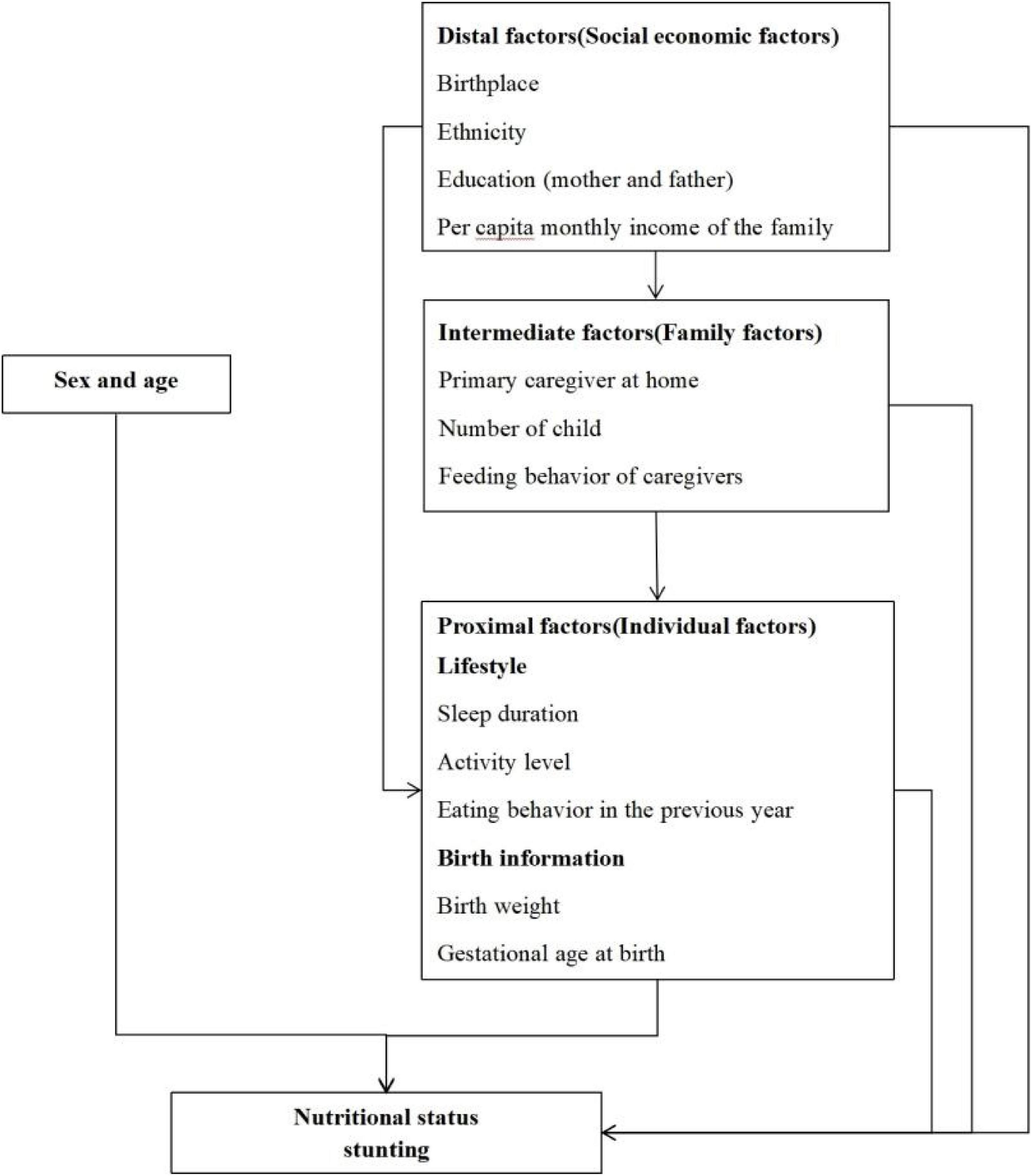
Figure 1. Conceptual framework.
Participants and diagnostic criteria
We investigated children in kindergartens in the Longgang District using a general investigation from May to July 2021. The researcher first contacted the person in charge of all kindergartens in Longgang District, with kindergartens as the unit, and explained the contents and purpose of the survey. If the person in charge of the kindergarten agreed to participate in this survey, all children who met the inclusion and exclusion criteria were included.
The inclusion criteria were as follows: children studying in kindergartens in Longgang District, Shenzhen, in the second semester from 2020 to 2021; guardians possessed reading and writing skills and were willing and able to complete the survey. Exclusion criteria were children who did not complete or submit the questionnaire to the online system.
Criteria for the diagnosis of stunting: children less than 60 months old are judged according to WHO Child Growth Standards (2006 Edition) (16). 5-year-old children (60–71.9 months old) are judged according to WHO Child Growth Standards (2007 Edition). Z-score is the deviation of an individual’s value of the median value of a reference population, divided by the standard deviation of the reference population. If the Z-score of height/length-for-age (HAZ/LAZ) was less than –2, it was considered stunting. If the HAZ was less than –2, it was judged as stunting. For children under 6 years old (less than 72 months old), severe stunting was defined as HAZ less than –3. Children aged 6 and above were judged according to the People’s Republic of China’s “screening for malnutrition in school-age children and adolescents” (WS/T 456-2014). If the child’s height was no more than the cutoff value, the child was judged to be stunted. Stunting was not diagnosed if the child had a clear cause (e.g., genetic metabolic diseases).
Data collection
All investigators were trained uniformly. Unified standard operating procedures were developed for the investigation process to ensure the quality of the investigation. The investigator introduced the survey to the guardians of the subjects, explained in detail the requirements for filling out the questionnaire, and issued a unique identification code for the subject. The guardians of the subjects can enter the online system to participate in the investigation with the unique identification code. The home page of the electronic survey provided the basic introduction and informed consent form. The subjects who chose to agree to participate filled out the questionnaire.
Data included the following: (1) demographic characteristics (gender, date of birth); (2) height/length to one decimal place in centimeters; (3) distal factors (birthplace, nationality, parents’ qualifications, per capita monthly income of the family); (4) intermediate factors (Primary caregiver at home, Number of children, feeding behavior of caregivers). Feeding behavior of caregivers includes forcing or punishing children to coerce them to eat more, inducing them to eat (e.g., using toys or television), and attitudes toward children’s bad eating habits. These behaviors were recorded if the caregiver engages in such behavior more than 3 days per week. (5) Proximal factors (see below).
(i) Sleep duration
Adequate sleep for children under 3 years is at least 11 h daily. For children over 3 years of age, more than 10 h a day is sufficient (17, 18).
(ii) Activity level
There were four activity levels: essential inactivity, less activity, general, and more significant activity.
(iii) Eating behavior in the previous year
This category includes eating less than their peers, eating slowly, not being interested in food, not eating in fixed places, and inattention while eating. Children demonstrating this behavior more than 3 days a week were considered to have this dietary behavior. The caregivers were asked to report whether there was picky eating.
(iv) Birth information
Birth information includes birth weight and gestational age at birth. If the birth weight was less than 2.5 kg, it was considered to be low birth weight. It was considered premature if the gestational age at birth was less than 37 weeks.
Statistical analysis
Categorical data were expressed as percentages and 95% confidence intervals (CI). According to the data type, the chi-square test or Fisher’s exact test was used to compare the differences between groups. Binary logistic regression was used to calculate the correlations between stunting and demographic characteristics, birth status, the lifestyle of children, and the feeding behavior of caregivers in the previous year with three stepwise models based on the conceptual framework. Binary logistic regression was used because the dependent variable, stunting, is dichotomous. Model 1 was constructed with distal factors to estimate their effect on stunting. Model 2 was constructed with distal and intermediate factors. Model 3 was constructed with distal, intermediate, and proximal factors. The statistical analysis was conducted using SPSS 20.0 (IBM, NY, United States). Two-sided p-values less than 0.05 were considered to be statistically significant.
Results
A total of 39 (8.11%) of kindergartens in the Longgang District refused to participate in the survey, and 442 (91.89%) agreed to participate. A total of 145,303 children from 442 kindergartens were investigated. A total of 124,593 children participated in the survey, with a response rate of 85.75%. Of these, 4,211 participants failed to complete the survey, and 1,978 subjects lacked critical information such as birth date or height. Finally, 118,404 subjects were included in the study for an effective rate of 95.03% (Figure 2). We set a test question in the questionnaire to reflect the accuracy of the questionnaire. The subjects were required to choose the kindergartens where the children were. A total of 117,870 subjects answered the test item correctly (99.55%).
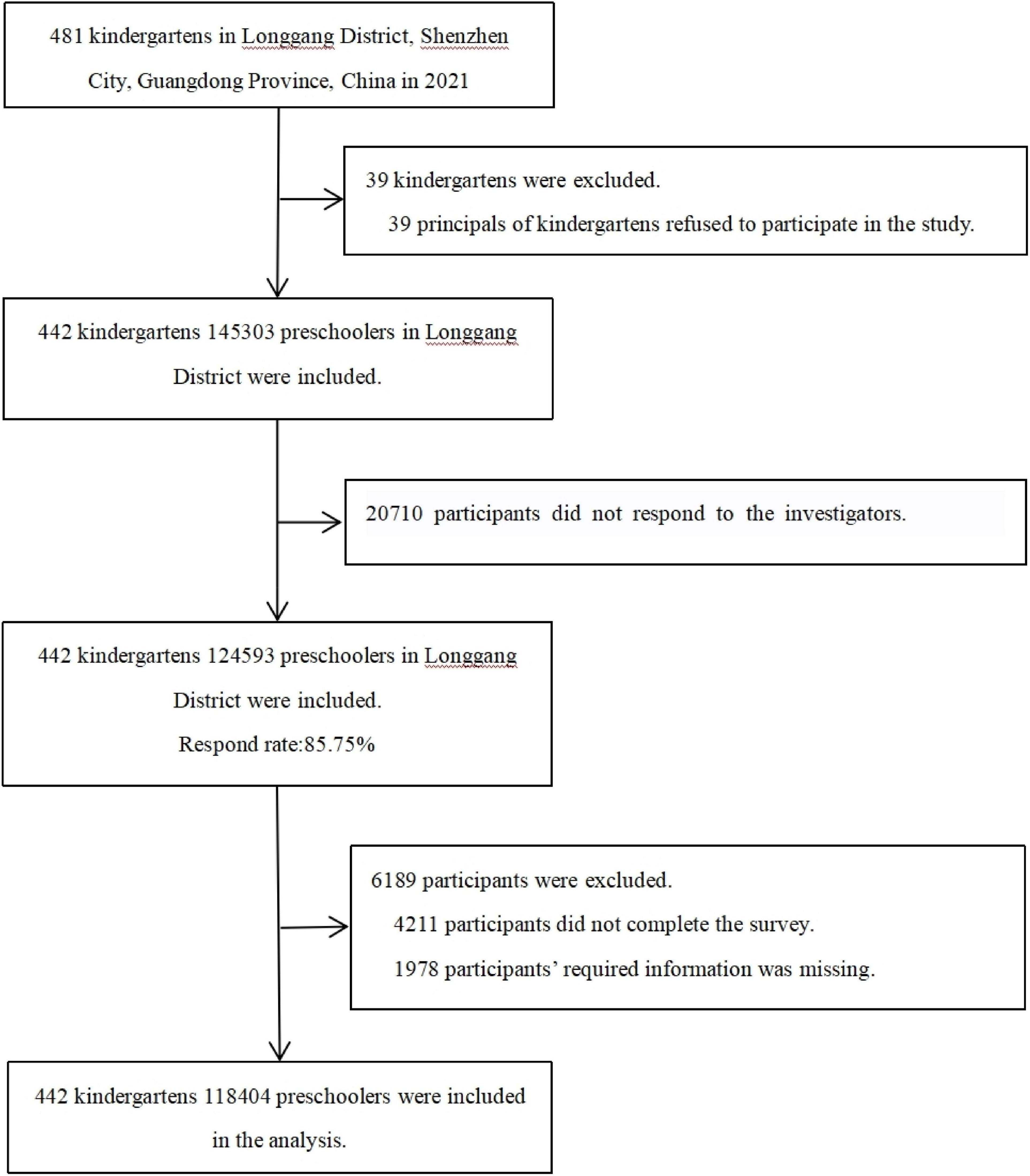
Figure 2. Study population.
The prevalence of stunting was 3.3% (95% confidence interval 3.2–3.4%). The rate of stunting in children under 5 years old was 3.6%, and that of children under 6 years old was 3.6%. There were significant differences in stunting rate among ages, education levels of the father and mother, and per capita monthly income of families and primary caregivers of children. There were no significant differences between genders and nationalities (Table 1).
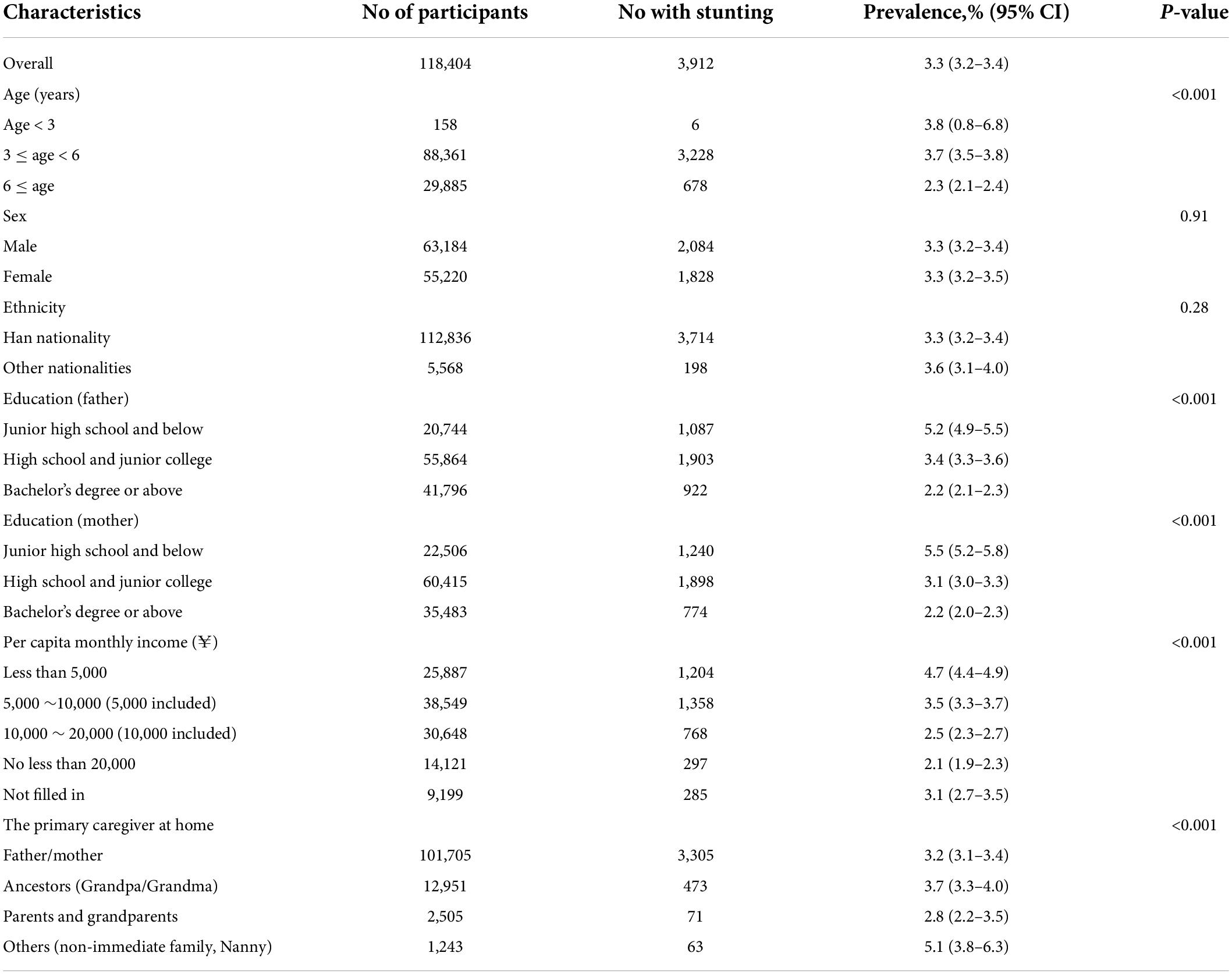
Table 1. Prevalence of stunting among preschoolers in Longgang District, Shenzhen City, China in 2021 (n = 118,404).
Among 88,519 children under 6 years of age, the prevalence of severe stunting was 0.8% (0.7%–0.9%). There were significant differences in the rate of severe stunting among children under 6 years old in gender, education level of the father and mother, and per capita monthly income of family and primary caregivers of children; however, there was no significant difference among nationalities (Table 2).
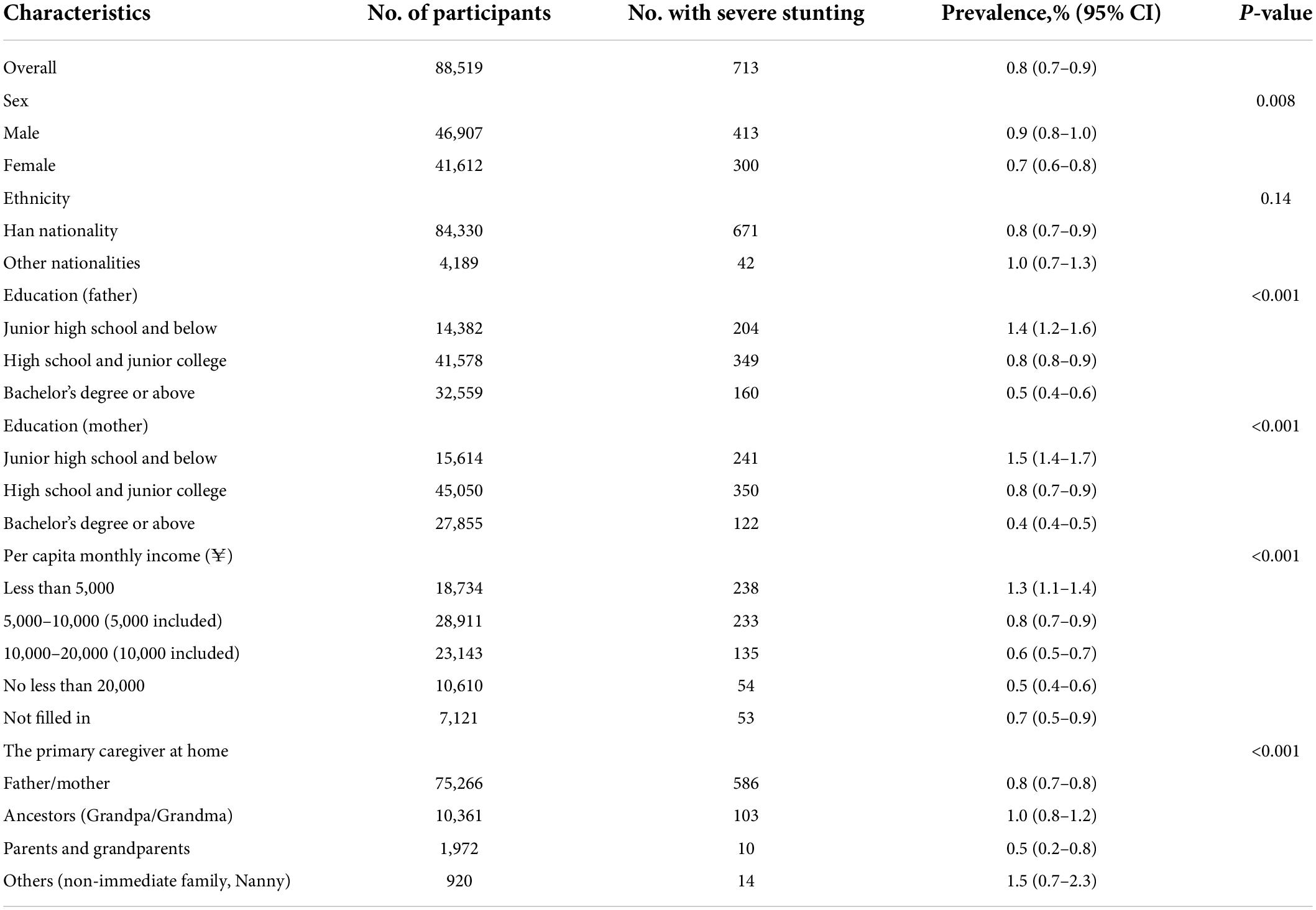
Table 2. Severe stunting rate for children under 6 years of age in Longgang District, Shenzhen City, China in 2021 (n = 118,404).
In model 3, binary multivariate logistic regression showed that showed that risk factors for stunting were male sex [odds ratio (OR) = 1.07], low birth weight (OR = 2.02), insufficient sleep time (OR = 1.08), less food intake than their peers (OR = 1.66), slower eating than their peers (OR = 1.16), accompanied by grandparents alone or non-lineal relatives (reference: parents accompanying) (OR = 1.23, 1.51), and children induced to eat (OR = 1.17). Protective factors included only-child status (OR = 0.66), reported high activity (OR = 0.37, 0.26, 0.23), parents with high education levels (father: OR = 0.87, 0.69; mother: OR = 0.69, 0.58), high monthly income per capita of the family (OR = 0.88, 0.74, 0.68), and allowing children to make food choices (OR = 0.82) (Table 3).
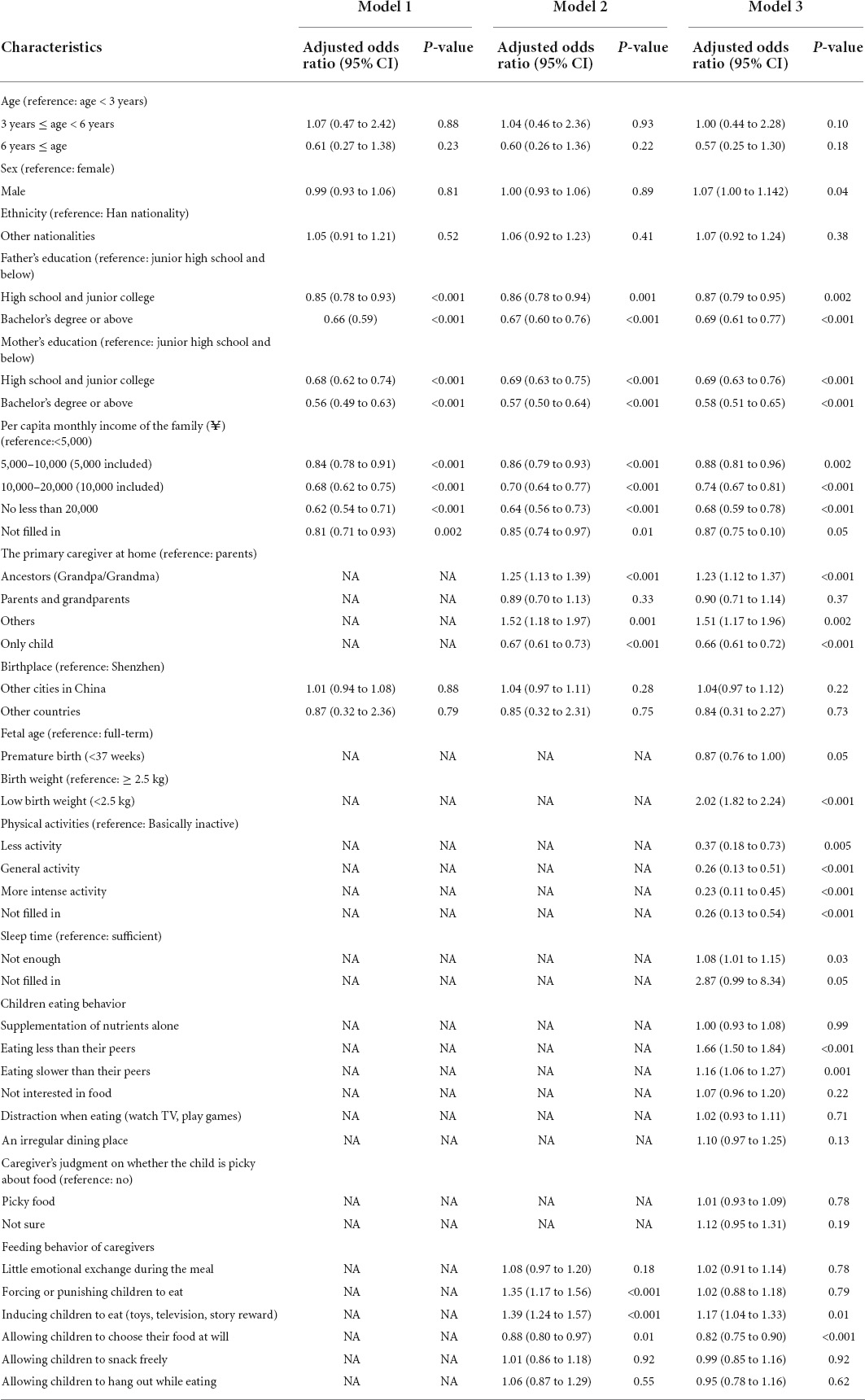
Table 3. Logistic regression models for stunting among preschoolers in Longgang District, Shenzhen City, China, in 2021 (n = 118,404).
Discussion
Prevalence of stunting
Our main finding was that the incidence of stunting among kindergarten children in the Longgang District was 3.3% (3.2–3.4%). The stunting rate of children under 5 years old was 3.6%, significantly lower than that in the world in 2020 (22%) and lower than in East Asia in 2020 (4.9%). The incidence was close to the level of North America (3.2%) and slightly higher than those in northern Europe, Australia, and New Zealand (2.3%–2.9%) (7). Overall, the stunting rate of kindergarten children in Longgang District was significantly lower than that in most developing countries and close to or slightly higher than that in developed countries. The relatively low stunting rate in the Longgang District of China may be associated with improved living standards by improving China’s economic level and children’s health care services. In recent years, China’s economic level has developed rapidly, and Shenzhen is in a golden development period of the superposition of Shenzhen Special Economic Zone and Shenzhen Pioneer Demonstration Zone. Economic development improves living standards, food supply, and quality. The Chinese government launched a series of nutrition improvement projects for Chinese children in several regions, providing good conditions for children’s growth and development.
The stunting rate of children under 6 years old in Longgang District was 3.6%, and that of children over 6 years old was 2.3%. The stunting rate of children under 6 years old was lower than that of children under 6 years old in China reported in 2020 (4.8% Note: The data come from the monitoring of nutrition and health status of Chinese residents from 2015 to 2017), and is comparable to that of urban prevalence (3.5%) (19). The stunting rate of children in Longgang District is higher than that in developed regions of China at 0.4% in 2016 and is comparable to the rate in Hunan Province of China of 3.1% in 2019 (20, 21).
The prevalence of stunting is strongly inversely correlated with the region’s wealth (22). As a region with a developed economy in China, the stunting rate of preschool children in the Longgang District is higher than the average level of developed areas in China, which might be related to the demographic characteristics of the Longgang District. The population mobility of Longgang District is relatively large, and its permanent non-registered population is as high as 2,897,300, accounting for 72.45% of the permanent population, which ranks high nationwide (23). The floating population faces several obstacles to obtaining comprehensive, affordable public health services, and this is one of the weakest links in China’s public health service system (23, 24). Studies showed that immigrant children’s growth and health level might be affected by the relatively unstable living environment and the shortage of medical and health services (25–28).
The COVID-19 epidemic has little effect on the overall stunting rate in Longgang District. A nutritional survey on kindergarten children in Shenzhen was carried out in 2015 (29). A stratified random sampling method was used. The kindergartens were divided into 11 layers according to their affiliated maternal and child health hospital, and 1/4 of kindergartens were randomly assigned in each layer. Kindergartens in the Longgang District were one of the layers. Seventy-nine kindergartens were assigned randomly from 318 kindergartens in the Longgang District in the survey. The height was measured by the maternal and child healthcare system staff, and the measurement method was standardized. Criteria for the diagnosis of stunting were according to the WHO Child Growth Standards. The diagnostic criteria for children under 6 years were the same as in this study; The diagnostic criteria for children aged six and above were similar. So that the data in 2015 and 2021 are comparable. The prevalence of stunting among kindergarten children in the Longgang District of Shenzhen in 2021 was 3.3%, lower than that in 2015 (4.71%) (29). The relatively low stunting rate in 2021 may be associated with improved kindergarten construction in Shenzhen City. In recent years, the Education Bureau of Shenzhen Municipality has printed and distributed documents like The Action Plan for the Development of Preschool Education in Shenzhen (2019–2020) to vigorously develop the kindergartens’ construction. In 2015, private kindergartens accounted for more than 90% in Shenzhen, while this survey shows that public kindergartens have reached nearly 50%. The government has strengthened the health care work and dietary management in kindergartens, providing strong support for improving children’s nutritional status.
Compared with the data of Shenzhen in 2015, the stunting rate of children under 3 years old in Longgang District increased nearly fourfold (3.8% vs. 1.0%). The relatively high stunting rate in 2021 may be associated with the influence of COVID-19. Social quarantine measures during the epidemic have significantly impacted children’s living conditions and lifestyles. Studies showed that during COVID-19, children’s physical activity (PA) decreased significantly, while the time spent watching electronic screens increased and unhealthy diets increased (30). We found that the COVID-19 epidemic significantly impacted the stunting rate of children under 3 years old in kindergartens, which suggests that more attention should be paid to the growth and development of children under 3 years old during the epidemic period.
Distal factors
The high education level of parents and per capita monthly income are related to stunting. The high education level of the father and mother was a protective factor, consistent with the results of observational studies (31, 32). This finding may be due to the higher education level of parents, who may acquire more nutrition knowledge conducive to scientific feeding. Higher per capita monthly income was a protective factor for stunting, similar to previous studies (33, 34). The higher the family’s monthly income, the more parents can spend on nutrition and better feeding environments.
Intermediate factors
Primary caregivers at home and the number of children are associated with stunting. Compared with care by parents alone, care by grandparents alone or non-immediate relatives was a risk factor for stunting. Grandparental care, which has become a worldwide social phenomenon, gives rise to poor dietary behaviors and lower levels of physical activity (35, 36). Only-child status was a protective factor for stunting, similar to previous studies (37).
The feeding behavior of caregivers in the previous year is associated with stunting. Encouraging children to eat using incentives such as toys and television is a risk factor, while allowing children to choose food at will is a protective factor. The feeding pattern of parents’ long-term reward inducing children to eat will reduce children’s enjoyment of food, which is not conducive to establishing long-term good eating behavior. The allowable feeding style provides children with a more relaxed eating environment and improves their food enjoyment (38). However, it may lead to a reduction in the diversity of food intake. More studies are needed to explore the association between stunting and allowable feeding style.
Proximal factors
The present study shows that the risk of boys suffering from childhood stunting is 1.07 times that of girls, the same as many results from China (20, 21, 39, 40) and other regions (41, 42), probably due to the interaction of biological and socio-cultural factors. We also found differences between boys and girls in growth trajectories and immune function beginning prenatally (43, 44). Caregivers treat children of different genders differently (45–47).
Low birth weight is a risk factor for stunting in children, consistent with many other studies (39, 40, 48). Birth weight is an essential indicator of fetal intrauterine nutrition (49). Low birth weight children always have poor digestion ability and low immunity, which may affect their growth and development (50, 51).
We found that lifestyle factors such as insufficient sleep, less PA, less food intake, and slower eating than peers were risk factors for stunting. There are few studies on the correlation between height and sleep deprivation (52). A cohort study of children found no correlation between sleep deprivation and height (53), different from the results of the present study; more studies are needed to explore the relationship between them. PA is associated with children’s growth and development. Studies showed that less active children are shorter, and PA-related epiphyseal loading positively affects the growth of healthy children (54). Poor dietary habits such as eating less and slowly can reduce the diversity of food intake and affect children’s growth and development. Studies showed that measures such as closing kindergartens in the early stage of the epidemic of COVID-19 impacted children’s activities, sleep, and other aspects; short-term changes in PA and sedentary behavior may become permanently involved (55, 56).
This study has some limitations. First, the study was a web-based questionnaire. Compared to the paper version of the questionnaire, this method is more likely to attract responses from younger and more educated people (57, 58); this approach may underestimate the incidence of stunting. Second, a web-based survey cannot rule out the possibility of parents misreporting the children’s heights. However, some major clinical characteristics reported by the participants were in line with the current survey in China. In addition, the correct rate of the questionnaire test was 99.55%, reflecting the accuracy of the survey results. Third, the study focused on the correlation between children’s lifestyle and family environment and stunting; other relevant factors should be included in the future. Finally, although the results gave some insights into the effect of COVID-19 on stunting in kindergarten children, we did not measure the influence of the COVID-19 pandemic in this study.
The stunting rate of children in kindergartens in Longgang in 2021 was low, close to or slightly higher than that of developed countries in the world, but higher than that of other developed cities in China. This finding may be due to the high proportion of the floating population. The stunting rate of children under 3 years old in kindergarten increased significantly, possibly due to the epidemic of COVID-19. Stunting is associated with distal, proximal, and intermediate factors. From a policy perspective, our findings suggest that public health services for migrant children and children under 3 years old should be promoted during the epidemic. Health education for parents with low education levels should be strengthened, and pro-poor policies should be formulated to reduce the effect of distal factors like parents’ education and family income. We should strengthen the guidance of caregivers’ feeding behavior. In addition to parents, grandparents, and other caregivers should be targets of feeding behavior guidance to reduce the effect of intermediate factors. To reduce the effect of proximal factors, we should help children cultivate a healthy lifestyle, including sleep, activity, and eating behavior, through kindergarten and family education. Health management services for boys and maternal health care services should be strengthened to prevent stunting.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The Ethics Review Committee of Shenzhen Hospital of Beijing University of Traditional Chinese Medicine (Longgang) approved the study (SZLDH2021LSYM-030). Written informed consent from the participants or their legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Authors contributions
TL and XG conceptualized and designed the study andreviewed the manuscript. XM and XY drafted the initial manuscript, coordinated and supervised data collection, and analyzed the data. HY, YW, YT, CL, CB, FD, and ZW participated in data collection and analysis. All authors read and approved the final manuscript.
Funding
All phases of this study were supported by the Innovation Team and Talents Cultivation Program of the National Administration of Traditional Chinese Medicine (No: ZYYCXTD-C-202006), Beijing University of Chinese Medicine Scientific Research and Development Fund Project (2021-ZXFZJJ-036), and National Natural Science Foundation of China (Grant no. 81874421).
Acknowledgments
We would like to thank all the subjects and their guardians for providing the information. We would also like to thank Prof. Jianping Liu and Zhaolan Liu for their guidance throughout this study. We would also further like to thank the pediatricians from Shenzhen Hospital—Beijing University of Chinese Medicine for their help recruiting patients for the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID-19, coronavirus disease 2019; WHO, World Health Organization; HAZ, height-for-age; LAZ, length-for-age; CI, confidence intervals; OR, odds ratio; PA, physical activity.
References
1. de Onis M, Branca F. Childhood stunting: a global perspective. Matern Child Nutr. (2016) 12 Suppl 1:12–26. doi: 10.1111/mcn.12231
2. Chidumwa G, Said-Mohamed R, Nyati LH, Mpondo F, Chikowore T, Prioreschi A, et al. Stunting in infancy, pubertal trajectories and adult body composition: the birth to twenty plus cohort, South Africa. Eur J Clin Nutr. (2021) 75:189–97. doi: 10.1038/s41430-020-00716-1
3. Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. (2008) 371:340–57. doi: 10.1016/S0140-6736(07)61692-4
4. Asiki G, Newton R, Marions L, Kamali A, Smedman L. The effect of childhood stunting and wasting on adolescent cardiovascular diseases risk and educational achievement in rural Uganda: a retrospective cohort study. Glob Health Action. (2019) 12:1626184. doi: 10.1080/16549716.2019.1626184
5. De Sanctis V, Soliman A, Alaaraj N, Ahmed S, Alyafei F, Hamed N. Early and long-term consequences of nutritional stunting: from childhood to adulthood. Acta Biomed. (2021) 92:e2021168.
6. Haywood X, Pienaar AE. Long-term influences of stunting, being underweight, and thinness on the academic performance of primary school girls: the NW-CHILD study. Int J Environ Res Public Health. (2021) 18:8973. doi: 10.3390/ijerph18178973
7. UNICEF-WHO-The World Bank. Joint Child Malnutrition Estimates – Levels and Trends 2021 ed. (2021). Available online at: https://data.unicef.org/resources/jme-report-2021/ (accessed January 20, 2022).
8. World Health Organization. Childhood Stunting: Challenges and Opportunities Report of a Promoting Healthy Growth and Preventing Childhood Stunting Colloquium. Geneva: World Health Organization (2013).
9. Araújo LA, Veloso CF, Souza MC, Azevedo JMC, Tarro G. The potential impact of the COVID-19 pandemic on child growth and development: a systematic review. J Pediatr. (2021) 97:369–77. doi: 10.1016/j.jped.2020.08.008
10. China Academy of Information and Communications Technology. 2018 Development Report of China’s top 100 Industrial Counties (cities) and top 100 Districts. (2018). Available online at: http://www.caict.ac.cn/kxyj/qwfb/bps/201811/P020181119514541037558.pdf (accessed January 26, 2022).
11. China Academy of Information and Communications Technology. 2019 Development Report of China’s Top 100 Industrial Counties (cities) and Top 100 Districts. (2019). Available online at: http://www.caict.ac.cn/kxyj/qwfb/bps/201911/P020191115610457502693.pdf (accessed January 26, 2022).
12. China Academy of Information and Communications Technology. 2020 Development Report of China’s Top 100 Industrial Counties (cities) and Top 100 Districts. (2020). Available online at: http://www.caict.ac.cn/kxyj/qwfb/bps/202011/P020201211777084001694.pdf (accessed January 26, 2022).
13. China Academy of Information and Communications Technology. 2021 Development Report of China’s top 100 Industrial Counties (cities) and Top 100 Districts. (2021). Available online at: http://www.caict.ac.cn/kxyj/qwfb/bps/202112/P020211216414627741293.pdf (accessed January 26, 2022).
14. Longgang District Bureau of Statistics. Economic Situation of Longgang District in 2021. (2022). Available online at: http://www.lg.gov.cn/tzcy/tjfx/content/post_9548509.html (accessed February 16, 2022).
15. Darteh EK, Acquah E, Kumi-Kyereme A. Correlates of stunting among children in Ghana. BMC Public Health. (2014) 14:504. doi: 10.1186/1471-2458-14-504
16. Baerug AB, Tufte E, Norum KR, Bjørneboe GE. The WHO child growth standards for children under 5 years. Tidsskr Nor Laegeforen. (2007) 127:2390–4.
17. National Health and Family Planning Commission of the People’s Republic of China. Guideline for Sleep Hygiene Among Children aged 0 5 Years. (2017). Available online at: http://www.nssi.org.cn/nssi/front/107324726.html (accessed February 16, 2022).
18. Ministry of Education of the People’s Republic of China. Management Standards of Compulsory Education Schools. (2017). Available online at: http://www.moe.gov.cn/srcsite/A06/s3321/201712/t20171211_321026.html (accessed February 16, 2022).
19. Bureau of Disease Prevention and Control, National Health Commission. Report on Chinese Residents’ Chronic Diseases and Nutrition 2020. Beijing: People’s Medical Publishing House (2022).
20. Zhang YQ, Li H, Wu HH, Zong XN. Stunting, wasting, overweight and their coexistence among children under 7 years in the context of the social rapidly developing: findings from a population-based survey in nine cities of China in 2016. PLoS One. (2021) 16:e245455. doi: 10.1371/journal.pone.0245455
21. Li HX, Huang GW, Wang H, Liu N, Wu J, Peng ZH, et al. Prevalence and associated factors for malnutrition among children under 6 years of age in hunan province. Chin J Pediatr. (2021) 59:759–66.
22. McGovern ME, Krishna A, Aguayo VM, Subramanian SV. A review of the evidence linking child stunting to economic outcomes. Int J Epidemiol. (2017) 46:1171–91. doi: 10.1093/ije/dyx017
23. Shenzhen Municipality Bureau of Statistics. Survey Office of the National Bureau of Statistics in Shenzhen. Shenzhen Statistical Yearbook. (2021). Available online at: http://www.sz.gov.cn/attachment/0/950/950362/9491392.pdf (accessed February 16, 2022).
24. Guan M. Associations between geodemographic factors and access to public health services among Chinese floating population. Front Public Health. (2020) 8:563180. doi: 10.3389/fpubh.2020.563180
25. Zheng L, Hu R, Dong Z, Hao Y. Comparing the needs and utilization of health services between urban residents and rural-to-urban migrants in China from 2012 to 2016. BMC Health Serv Res. (2018) 18:717. doi: 10.1186/s12913-018-3522-y
26. Xing T, Yin X. A comparative study on the nutritional status of the left behind children, migrant children and Urban children. Sports Sci. (2015) 36:112–20.
27. Liu XF, Sun XM, Sun XW, Yang YQ, Huang CH, Wen H. Epidemiological study on hand, foot and mouth disease in Tongzhou District, Beijing, 2013–2017. J Int Med Res. (2019) 47:2615–25. doi: 10.1177/0300060519841974
28. Kroening A, Dawson-Hahn E. Health considerations for immigrant and refugee Children. Adv Pediatr. (2019) 66:87–110. doi: 10.1016/j.yapd.2019.04.003
29. Shuangyan Qiu. The Investigation on Health Care and Children Nutritional STATUS of Kindergartens in Shenzhen. Guangzhou: Southern Medical University (2015).
30. Zemrani B, Gehri M, Masserey E, Knob C, Pellaton R. A hidden side of the COVID-19 pandemic in children: the double burden of undernutrition and overnutrition. Int J Equity Health. (2021) 20:44. doi: 10.1186/s12939-021-01390-w
31. Ghattas H, Acharya Y, Jamaluddine Z, Assi M, El Asmar K, Jones AD. Child-level double burden of malnutrition in the MENA and LAC regions: prevalence and social determinants. Matern Child Nutr. (2020) 16:e12923. doi: 10.1111/mcn.12923
32. Woodruff BA, Wirth JP, Bailes A, Matji J, Timmer A, Rohner F. Determinants of stunting reduction in Ethiopia 2000 – 2011. Matern Child Nutr. (2017) 13:e12307. doi: 10.1111/mcn.12307
33. Mulyaningsih T, Mohanty I, Widyaningsih V, Gebremedhin TA, Miranti R, Wiyono VH. Beyond personal factors: multilevel determinants of childhood stunting in Indonesia. PLoS One. (2021) 6:e260265. doi: 10.1371/journal.pone.0260265
34. Tekile AK, Woya AA, Basha GW. Prevalence of malnutrition and associated factors among under-five children in Ethiopia: evidence from the 2016 Ethiopia demographic and health survey. BMC Res Notes. (2019) 12:391. doi: 10.1186/s13104-019-4444-4
35. Liu Y, Zhao J, Zhong H. Grandparental care and childhood obesity in China. SSM Popul Health. (2022) 17:101003. doi: 10.1016/j.ssmph.2021.101003
36. Jongenelis MI, Talati Z, Morley B, Pratt IS. The role of grandparents as providers of food to their grandchildren. Appetite. (2019) 134:78–85. doi: 10.1016/j.appet.2018.12.022
37. Global Burden of Disease Child and Adolescent Health Collaboration. Child and adolescent health from 1990 to 2015: findings from the global burden of diseases, injuries, and risk factors 2015 study. JAMA Pediatr. (2017) 171:573–92. doi: 10.1001/jamapediatrics.2017.0250
38. Kutbi HA. The relationships between maternal feeding practices and food neophobia and picky eating. Int J Environ Res Public Health. (2020) 17:3894. doi: 10.3390/ijerph17113894
39. Yu DM, Zhao LY, Yang ZY, Chang SY, Yu WT, Fang HY, et al. Comparison of undernutrition prevalence of children under 5 years in China between 2002 and 2013. Biomed Environ Sci. (2016) 29:165–76. doi: 10.3967/bes2016.021
40. Wang A, Scherpbier RW, Huang X, Guo S, Yang Y, Josephs-Spaulding J. The dietary diversity and stunting prevalence in minority children under 3 years old: a cross-sectional study in forty-two counties of Western China. Br J Nutr. (2017) 118:840–8. doi: 10.1017/S0007114517002720
41. Kismul H, Acharya P, Mapatano MA, Hatløy A. Determinants of childhood stunting in the democratic republic of Congo: further analysis of demographic and health survey 2013-14. BMC Public Health. (2017) 18:74. doi: 10.1186/s12889-017-4621-0
42. Sserwanja Q, Kamara K, Mutisya LM, Musaba MW, Ziaei S. Rural and Urban correlates of stunting among under-five children in Sierra Leone: a 2019 nationwide cross-sectional survey. Nutr Metab Insights. (2021) 14:1518410384. doi: 10.1177/11786388211047056
43. Lipoldova M, Demant P. Gene-specific sex effects on susceptibility to infectious diseases. Front Immunol. (2021) 12:712688. doi: 10.3389/fimmu.2021.712688
44. Fischer J, Jung N, Robinson N, Lehmann C. Sex differences in immune responses to infectious diseases. Infection. (2015) 43:399–403. doi: 10.1007/s15010-015-0791-9
45. Harris H, Mallan KM, Nambiar S, Daniels LA. The relationship between controlling feeding practices and boys’ and girls’ eating in the absence of hunger. Eat Behav. (2014) 15:519–22. doi: 10.1016/j.eatbeh.2014.07.003
46. Bork KA, Diallo A. Boys are more stunted than girls from early infancy to 3 years of age in rural senegal. J Nutr. (2017) 147:940–7. doi: 10.3945/jn.116.243246
47. Thompson AL. Greater male vulnerability to stunting? Evaluating sex differences in growth, pathways and biocultural mechanisms. Ann Hum Biol. (2021) 48:466–73. doi: 10.1080/03014460.2021.1998622
48. Kohlmann K, Sudfeld CR, Garba S, Guindo O, Grais RF, Isanaka S. Exploring the relationships between wasting and stunting among a cohort of children under two years of age in Niger. BMC Public Health. (2021) 21:1713. doi: 10.1186/s12889-021-11689-6
49. Calcaterra V, Cena H, Regalbuto C, Vinci F, Porri D, Verduci E, et al. The role of fetal, infant, and childhood nutrition in the timing of sexual maturation. Nutrients. (2021) 13:419. doi: 10.3390/nu13020419
50. Alderman H, Behrman JR, Glewwe P, Fernald L, Walker S. Evidence of impact of interventions on growth and development during early and middle childhood. 3rd ed. In: Bundy DAP, de SN, Horton S editors. Child and Adolescent Health and Development. Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2017). doi: 10.1596/978-1-4648-0423-6_ch7
51. Unger S, Stintzi A, Shah P, Mack D, O’Connor DL. Gut microbiota of the very-low-birth-weight infant. Pediatr Res. (2015) 77:205–13. doi: 10.1038/pr.2014.162
52. El HC, Nunes ML. Sleep and weight-height development. J Pediatr (Rio J). (2019) 95 Suppl 1:2–9. doi: 10.1016/j.jped.2018.10.009
53. Jenni OG, Molinari L, Caflisch JA, Largo RH. Sleep duration from ages 1 to 10 years: variability and stability in comparison with growth. Pediatrics. (2007) 120:e769–76. doi: 10.1542/peds.2006-3300
54. Meinhardt U, Witassek F, Petrò R, Fritz C, Eiholzer U. Less physically active children are shorter. Minerva Pediatr. (2017) 69:135–40. doi: 10.23736/S0026-4946.16.04287-0
55. Dunton GF, Do B, Wang SD. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health. (2020) 20:1351. doi: 10.1186/s12889-020-09429-3
56. Neshteruk CD, Zizzi A, Suarez L, Erickson E, Kraus WE, Li JS, et al. Weight-Related Behaviors of Children with Obesity during the COVID-19 Pandemic. Child Obes. (2021) 17:371–8. doi: 10.1089/chi.2021.0038
57. Barentsz MW, Wessels H, van Diest PJ, Pijnappel RM, Haaring C, van der Pol CC, et al. Tablet, web-based, or paper questionnaires for measuring anxiety in patients suspected of breast cancer: patients’ preferences and quality of collected data. J Med Internet Res. (2014) 16:e239. doi: 10.2196/jmir.3578
Keywords: stunting, kindergarten children, malnutrition, coronavirus disease 2019, eating behavior, feeding behavior
Citation: Ma X, Yang X, Yin H, Wang Y, Tian Y, Long C, Bai C, Dong F, Wang Z, Liu T and Gu X (2022) Stunting among kindergarten children in China in the context of COVID-19: A cross-sectional study. Front. Pediatr. 10:913722. doi: 10.3389/fped.2022.913722
Received: 06 April 2022; Accepted: 14 July 2022;
Published: 02 August 2022.
Edited by:
Keiko Nanishi, The University of Tokyo, JapanReviewed by:
Asankha Pallegedara, Wayamba University of Sri Lanka, Sri LankaKarim Premji Manji, Muhimbili University of Health and Allied Sciences, Tanzania
Copyright © 2022 Ma, Yang, Yin, Wang, Tian, Long, Bai, Dong, Wang, Liu and Gu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tiegang Liu, bGl1dGllZ2FuZzIwMDlAMTYzLmNvbQ==; Xiaohong Gu, Z3V4aDEwMDNAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship