
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr., 07 July 2022
Sec. Pediatric Gastroenterology, Hepatology and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.906924
 Ruth Blanco-Rojo1*
Ruth Blanco-Rojo1* José Maldonado2,3,4Monika Schaubeck5
José Maldonado2,3,4Monika Schaubeck5 Metehan Özen6
Metehan Özen6 Eduardo López-Huertas7
Eduardo López-Huertas7 Mónica Olivares1
Mónica Olivares1Cesarean section (CS) disrupts the natural microbiota colonization process in infants, which might compromise immune system maturation, leading to a higher risk of infections. We evaluated the effect of the probiotic Limosilactobacillus (L.) fermentum CECT 5716 on the incidence of gastrointestinal and respiratory infections in the CS infant subgroups (n = 173) of three randomized clinical trials in which this probiotic strain was demonstrated to be safe and effective for preventing infections. Therefore, the data for the CS infants were extracted to obtain the incidence rate ratio (IRR) and 95% CI for gastrointestinal and respiratory infections for each study and were then combined to obtain a pooled IRR and 95% CI using the generic inverse variance method. There was a significant reduction of 73% in the incidence of gastrointestinal infections in CS infants receiving L. fermentum CECT 5716 compared with those receiving the control formula [n = 173, IRR: 0.27 (0.13, 0.53), p = 0.0002]. Regarding respiratory infections, although pooled results showed a reduction of 14% in the probiotic group, the difference was not statistically significant [n = 173, IRR (95% CI): 0.86 (0.67, 1.11), p = 0.25]. In conclusion, the administration of L. fermentum CECT 5716 to CS-born infants protects them from gastrointestinal infections by reducing the risk by up to 73% in this population.
Vaginal delivery (VD) allows contact of the neonate with the vaginal and enteric microbiota of the mother and therefore influences infants' gut colonization. CS, apart from disrupting this natural colonization process, also imply exposition of the newborn to microbes from the operating theater and perinatal antibiotics, thus promoting a significantly different microbiota compared to that in VD infants (1). Specifically, the microbiota of VD infants is characterized by microbes including Limosilactobacillus, Prevotella, Bacteroides, Escherichia/Shigella, Bifidobacterium spp. and other members of the former genus Lactobacillus (2). In contrast, Staphylococcus, Streptococcus, Corynebacterium, Veillonella and Propionibacterium spp. dominate in the microbiome of CS delivered infants (3, 4) and delay the expected normal intestinal colonization. Moreover, lower amounts of total intestinal bacteria and lower diversity have been observed in CS infants (5–7).
Immune system maturation is dependent on intestinal colonization. The gut-associated lymphoid tissues, such as the Peyer's patches, the mesenteric lymph nodes and the isolated lymphoid follicles require signals from the intestinal microbiota to ensure complete development and maturation. This learning process determines an individual's immune response throughout their life (8–10). The close relationship between the colonization process in infants and the development of the immune system explains, at least in part, the immunological differences in CS children compared to VD children (6, 9). These changes in the immune system due to CS microbiota dysbiosis have been related to a higher risk of infections and an increased frequency of hospital admissions due to any type of infection in CS infants (11–13).
To reduce the potential negative effects of CS delivery on early colonization, strategies to imitate natural microbial colonization by VD have been evaluated, including exposure of infants to the mother's fecal and/or vaginal microbiota (14, 15). Although these strategies may resemble the natural microbiome colonization process during delivery, the physician performed, artificial application is under intense debate due to the high risk of pathogen transmission to infants (16–18). It is important to highlight that breastfeeding seems to help to counteract the deleterious effect of CS on the microbiota without safety concerns related to fecal or vaginal transplant procedures and, therefore, breastfeeding should be encouraged and support should be given by physicians and midwifes (19). However, women who deliver babies by CS are less likely to breastfeed or delay breastfeeding initiation (20). Therefore, if breastfeeding is not possible or insufficient, a feasible strategy would be to introduce bacteria naturally present in human milk into infant formulae.
Limosilactobacillus (L.) fermentum CECT 5716, previously named Lactobacillus fermentum CECT 5716 (2), is a probiotic strain originally isolated from human milk (21). Three randomized clinical trials (RCTs) (22–24) performed in infants demonstrated the safety of the probiotic strain as well as its usefulness for preventing community-acquired infections, such as gastrointestinal and respiratory infections (Table 1).
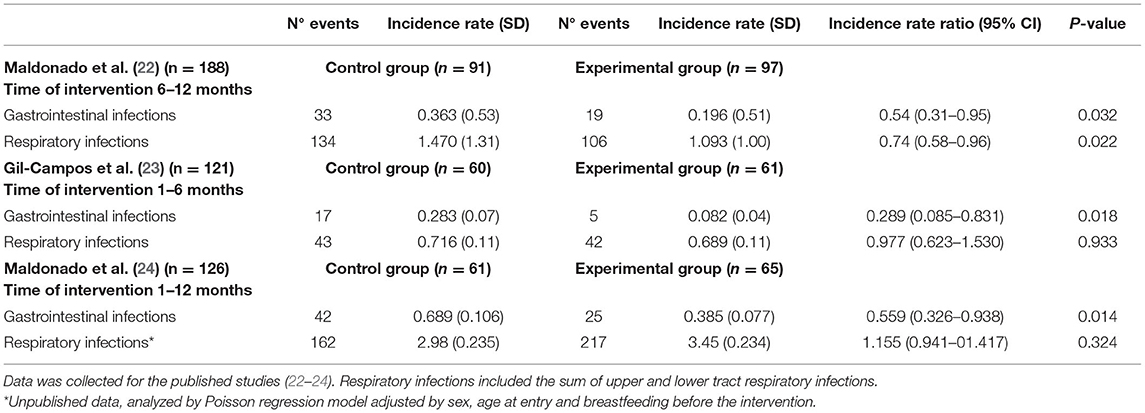
Table 1. Summary of the incidence of gastrointestinal and respiratory infections in infants.
These three studies involved both VD- and CS-born infants. The objective of the present study is to analyze the effect of L. fermentum CECT 5716 consumption on the incidence of gastrointestinal and respiratory infections in the CS subgroup. Therefore, data on CS-born infants in the three aforementioned clinical trials were extracted separately, and the obtained results were pooled in a meta-analysis.
The protocols for the three randomized clinical trials have been previously discussed in detail (22–24). Briefly, all the studies were double-blind, randomized, controlled trials and included healthy infants exclusively fed formula, with an inclusion age ranging from 1 month (23, 24) to 6 months (22) (Table 1). In all the studies, Limosilactobacillus fermentum CECT 5716 (HEREDITUM® LC40) was administered as an ingredient in a powdered infant formula with a nutritional composition in accordance with current EU regulations. All formulae were well tolerated, and compliance was good. Furthermore, no adverse effects related to formula consumption were reported. The CS rates in the studies were 31% in Maldonado et al. (24), 43% in Gil-Campos et al. (23) and 44% in Maldonado et al. (22).
For the purpose of this study, only data for CS-born infants were taken into consideration. The main outcomes of the current study were the incidence of gastrointestinal infections and respiratory infections. In all the studies, the diagnosis of infections was performed by pediatricians based on specific symptoms and standardized definitions, as followed. Gastrointestinal infection was defined as loose or watery stools ≥3 times/day, with or without fever or vomiting in Maldonado et al. (24), and in Gil-Campos et al. (23); whereas in Maldonado et al. (22) was defined as the occurrence of loose or watery stool ≥4 times/day, with or without a fever or vomiting. Respiratory tract infections were defined as the presence of abundant mucosity and/or cough during ≥2 consecutive days with or without fever or the presence of wheezing and/or crepitants with or without fever in all three studies (22–24).
The occurrence of gastrointestinal and respiratory infections was described for each study using the incidence rate (IR) and the incidence rate ratio (IRR) with the 95% CI and p-value for the IRR in each clinical trial. A Poisson regression model was applied to adjust the number of events by sex, age at intervention entry, and whether infants were breastfed before the intervention.
The IRR and 95% CI for gastrointestinal and respiratory infections were extracted from individual studies and combined to obtain a pooled IRR and 95% CI by combining the effect-size estimates (b-coefficients and 95% CIs) from the 3 studies, which were weighted by the inverse of the corresponding standard errors (SEs).
A general alpha level of 0.05 was used as the cutoff point for statistical significance. Statistical analyses were carried out using SPSS software version 27.0 for Windows (SPSS, Chicago, IL, USA) and RevMan 5.4 (25).
Analysis of data from CS infants showed that the incidence of gastrointestinal infections was reduced by the consumption of L. fermentum CECT 5716 (Table 2), reaching significance in two of the three RCTs analyzed separately. Furthermore, pooled results from the 173 CS infants showed a significant reduction of 73% in the incidence of gastrointestinal infections in CS-born children receiving L. fermentum CECT 5716 in comparison to infants receiving the control formula [n = 173, IRR: 0.27 (0.13, 0.53), p = 0.0002] (Figure 1A).

Table 2. Incidence of gastrointestinal and respiratory infections in infant born by CS.
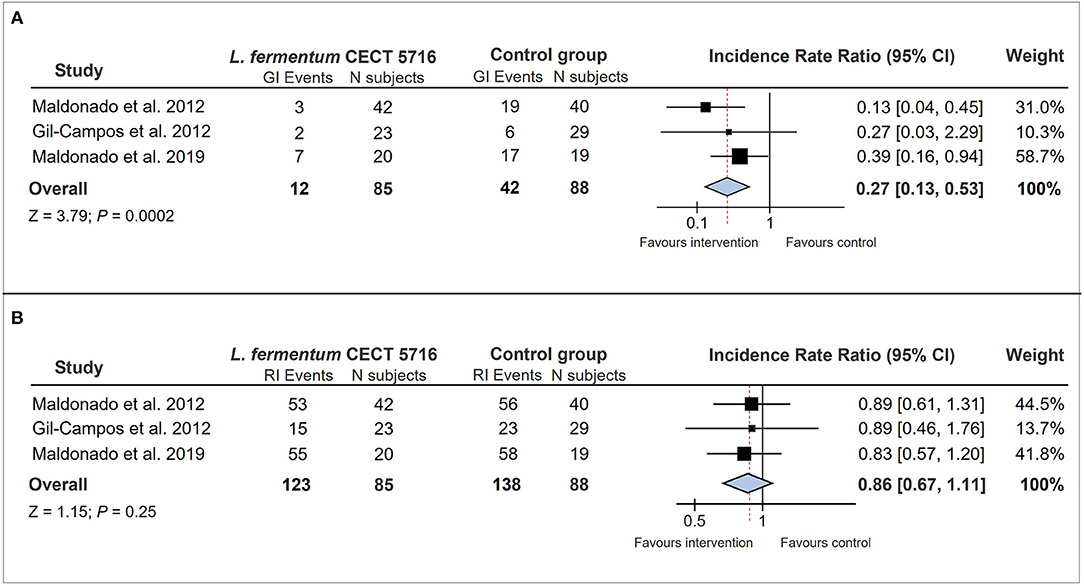
Figure 1. Forest plots illustrating the effect of L. fermentum CECT 5716 interventions on (A) the incidence of gastrointestinal infections and (B) the incidence of respiratory infections in infants born by CS. CI, confidence interval; GI, gastrointestinal infection; RI, respiratory infection; N subjects, number of volunteers participating in each study-intervention group.
Analysis of the incidence of respiratory infections (RI) showed no significant reduction by L. fermentum CECT 5716 in CS-delivered infants (Table 2), although a decreasing trend of these types of infections was observed. The pooled results showed a 14% reduction in the incidence of respiratory infections in CS-born infants receiving the probiotic, although the difference was not statistically significant [n = 173, IRR: 0.86 (0.67, 1.11), p = 0.25] (Figure 1B).
The present study shows that the human milk-isolated probiotic strain L. fermentum CECT 5716 seems to be effective in reducing the incidence of gastrointestinal infections in CS-born and formula fed infants. A recent meta-analysis, which included the total population of the three clinical trials (n = 512), showed a significant overall reduction in the incidence of gastrointestinal infections of 46% (p = 0.0004) (26). However, the effect observed in the specific population born by CS shows an even higher level of reduction (73%), suggesting that the protective effect of this probiotic strain might be even more relevant in the case of CS delivery.
Infectious diseases are the most common type of illness for infants worldwide, resulting in the leading cause of morbidity and mortality during the first year of life (22, 27). Among the risk factors for infections, increasing evidence showed a higher risk for gastrointestinal and respiratory infections, and related hospitalizations in CS infants (12, 28–30). Different studies have been performed to evaluate the effect of probiotic administration to infants born by CS (31–34). However, most of these studies have focused primarily on evaluating the impact on the microbiota. Consequently, there are still few data on whether probiotics may help in the maturation of the immune system and thereby reduce the risk of infections in infants with CS. Therefore, the results of the present study add new evidence regarding the usefulness of administering a probiotic strain in the prevention of community-acquired infections in CS infants, which could be of great interest in this population.
It is interesting to note that the incidence rates of both gastrointestinal and respiratory infections were lower in the study of Gil-Campos et al. (23). Here, infants were followed-up from 1 to 6 months, compared to the other two studies in which the infants were in the study from 6 to 12 months (22) and from 1 to 12 months of age (24). This observation is in agreement with other studies (35), and could be explained by several factors, including the fact that infants that may attend day care centers in Spain—a major risk factor for infection in infants (36–38)—are normally older than 6 months of age (38).
Different mechanisms influenced by gut colonization in early life are involved in protection against gastrointestinal infections, e.g., competition with pathogenic bacteria, production of bacteriocins, strengthening of the epithelial barrier and therefore reduction of intestinal permeability, or modulation of the host's local immune response by inducing the production of antimicrobial proteins (39, 40). Therefore, these mechanisms could be affected in the case of CS-associated dysbiosis. L. fermentum CECT 5716 has been shown to support pathogen defense through all these mechanisms in different in vitro and in vivo models (41). Interestingly, results obtained in newborn rats show a protection in intestinal barrier integrity during stress induced by maternal separation (42). The fact that L. fermentum CECT 5716 can enhance the immune response (43, 44) as it interferes with the mechanisms involved in enteropathogen internalization (45) might be responsible for the improved protective effect observed against gastrointestinal infections. Interestingly, in adults receiving anti influenza vaccination, the consumption of L. fermentum CECT 5716 induced an increase in specific IgA (44). The immunoglobulin A (IgA) is the predominant antibody isotype in the mucosal immune system, which widely exists in the gastrointestinal tract, respiratory tract, vaginal tract, tears, saliva, and colostrum (46). It acts as the first line of defense against pathogens. There is a lack of IgA-secreting B cells in neonates until exposure to bacteria, suggesting that the commensal microorganisms were able to induce sIgA secretion (47). Activation of IgA production might be related to L. fermentum CECT 5716 capability to interact with other immune cells inducing immune response modulating cytokine release (48). Moreover, consumption of L. fermentum CECT 5716 has been shown to increase the load of fecal lactobacilli and bifidobacteria (22, 24). Therefore, the protective effect of this probiotic strain on gastrointestinal infections might also be due to its ability to modulate the microbiota (3, 6, 7). However, as the bacterial quantification methods were different in the three clinical trials included in this analysis, no evaluation of the overall effect of the probiotic strain on the microbiota of the CS-born infants could be made. A more complete analysis of the microbiota in infants and studies focusing on CS-born infants should be performed in the future to elucidate the role of probiotic intervention on the microbiota and its impact on the immune response and susceptibility to infections.
The effect of L. fermentum CECT 5716 on respiratory infections has been attributed to the modulation of the immune response (22, 44). However, the effect in the CS-born population was not as obvious for respiratory infections. In the analysis of the total population in the study reported by Maldonado et al. (22), a reduction in the incidence of respiratory infections in the group consuming the probiotic strain was observed (IRR = 0.74; CI 95% 0.58–0.96; p = 0.022). Separate analyses of upper and lower respiratory infections showed that the difference was due to the effect on upper respiratory infections (19). In the second study of Maldonado et al. (24), a significant reduction in upper respiratory infections in the CS-born subgroup (IRR = 0.492; CI 95% 0.294–0.815; p= 0.006) was observed. In contrast, the analysis of the CS-born subpopulation performed in the present study considering total respiratory infections (upper and lower respiratory infections) did not show a significant effect of the probiotic intervention. As Gil-Campos et al. (23) did not distinguish between upper and lower infections, a global analysis of upper infections could not be performed in the present analysis of the CS-born infant subpopulation. Moreover, no blood samples were collected in any of these studies, so the effect of the probiotic intervention on the immune response in these children could not be analyzed. In addition, the duration and/or severity of the respiratory infections were not recorded. Therefore, further studies to elucidate the effect of L. fermentum CECT 5716 on the prevention and on the severity and duration of respiratory infections in CS infants should be performed.
Some limitations of the study should be noted. First, we included data from three different studies that followed-up the infants in different age ranges, from 1 to 6 months (23), 6 to 12 months (22), and 1 to 12 months old (24). However, we pooled the data by using the most adequate methodology (49). Second limitation is that one of the studies (22) used a different dose of the probiotic. However, results obtained in a previous meta-analysis did not support a dose–response effect for L. fermentum CECT 5716 (26). This observation is also in agreement with the non-dependent dose effect exerted by L. fermentum for other applications (50). Another limitation is that the recorded data did not allow to distinguish between scheduled and emergency CS (51). Finally, although infectious diseases were diagnosed by a pediatrician, definition for gastrointestinal infections were slightly differed in one of the three studies (22).
In conclusion, the administration of L. fermentum CECT 5716 to CS-born infants protects them from gastrointestinal infections by reducing the risk of this type of infection by up to 73% in this population. The protective effect of this probiotic has been extensively demonstrated in several clinical trials, but the results of the present study suggest that it could be even more relevant in the case of CS-born infants, a population at higher risk for infections. The use of probiotics in this specific population should be more deeply studied as a strategy to balance the negative effects of CS on immune system maturation.
The data analyzed in this study is subject to the following licenses/restrictions: Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available. Requests to access these datasets should be directed to cmJsYW5jb0BiaW9zZWFyY2hsaWZlLmNvbQ==.
The studies involving human participants were reviewed and approved by Regional Ethics Committee of the Sistema Andaluz de Salud, Sevilla, Spain. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
RB-R designed the methodology, analyzed the data, and contributed to the manuscript writing. MS and MÖz contributed to the manuscript writing and critically revised the manuscript. JM critically revised the manuscript. EL-H participated in the conception of the study and critically revised the manuscript. MOl designed the study, interpreted the results, and wrote the draft of the manuscript. All authors have read and approved the final manuscript.
RB-R and MOl are employees of Biosearch Life, a Kerry Company. Biosearch Life, a Kerry Company, is the owner of the patent for L. fermentum CECT5716. MS is an employee at HiPP.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hoang DM, Levy EI, Vandenplas Y. The impact of Caesarean section on the infant gut microbiome. Acta Paediatr Oslo Nor. (2021) 110:60–67. doi: 10.1111/apa.15501
2. Zheng J, Wittouck S, Salvetti E, Franz CMAP, Harris HMB, Mattarelli P, et al. A taxonomic note on the genus Lactobacillus: description of 23 novel genera, emended description of the genus Lactobacillus Beijerinck 1901, and union of Lactobacillaceae and Leuconostocaceae. Int J Syst Evol Microbiol. (2020) 70:2782–858. doi: 10.1099/ijsem.0.004107
3. Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci. (2010) 107:11971–5. doi: 10.1073/pnas.1002601107
4. Korpela K. Impact of delivery mode on infant gut microbiota. Ann Nutr Metab. (2021) 77:11–19. doi: 10.1159/000518498
5. Adlerberth I, Lindberg E, Åberg N, Hesselmar B, Saalman R, Strannegård I-L, et al. Reduced enterobacterial and increased staphylococcal colonization of the infantile bowel: an effect of hygienic lifestyle? Pediatr Res. (2006) 59:96–101. doi: 10.1203/01.pdr.0000191137.12774.b2
6. Huurre A, Kalliomäki M, Rautava S, Rinne M, Salminen S, Isolauri E. Mode of delivery – effects on gut microbiota and humoral immunity. Neonatology. (2008) 93:236–40. doi: 10.1159/000111102
7. Jakobsson HE, Abrahamsson TR, Jenmalm MC, Harris K, Quince C, Jernberg C, et al. Decreased gut microbiota diversity, delayed Bacteroidetes colonisation and reduced Th1 responses in infants delivered by caesarean section. Gut. (2014) 63:559–66. doi: 10.1136/gutjnl-2012-303249
8. Maynard CL, Elson CO, Hatton RD, Weaver CT. Reciprocal interactions of the intestinal microbiota and immune system. Nature. (2012) 489:231–41. doi: 10.1038/nature11551
9. Francino MP. Birth mode-related differences in gut microbiota colonization and immune system development. Ann Nutr Metab. (2018) 73 Suppl 3:12–6. doi: 10.1159/000490842
10. Hornef MW, Torow N. “Layered immunity” and the “neonatal window of opportunity” - timed succession of non-redundant phases to establish mucosal host-microbial homeostasis after birth. Immunology. (2020) 159:15–25. doi: 10.1111/imm.13149
11. Laubereau B, Filipiak-Pittroff B, von Berg A, Grübl A, Reinhardt D, Wichmann HE, et al. Caesarean section and gastrointestinal symptoms, atopic dermatitis, and sensitisation during the first year of life. Arch Dis Child. (2004) 89:993–7. doi: 10.1136/adc.2003.043265
12. Christensen N, Søndergaard J, Christesen HT, Fisker N, Husby S. Association between mode of delivery and risk of infection in early childhood: a cohort study. Pediatr Infect Dis J. (2018) 37:316–23. doi: 10.1097/INF.0000000000001778
13. Kristensen K, Henriksen L. Cesarean section and disease associated with immune function. J Allergy Clin Immunol. (2016) 137:587–90. doi: 10.1016/j.jaci.2015.07.040
14. Korpela K, Helve O, Kolho K-L, Saisto T, Skogberg K, Dikareva E, et al. Maternal fecal microbiota transplantation in cesarean-born infants rapidly restores normal gut microbial development: a proof-of-concept study. Cell. (2020) 183:324–34.e5. doi: 10.1016/j.cell.2020.08.047
15. Dominguez-Bello MG, De Jesus-Laboy KM, Shen N, Cox LM, Amir A, Gonzalez A, et al. Partial restoration of the microbiota of cesarean-born infants via vaginal microbial transfer. Nat Med. (2016) 22:250–3. doi: 10.1038/nm.4039
16. Hourigan SK, Dominguez-Bello MG, Mueller NT. Can maternal-child microbial seeding interventions improve the health of infants delivered by Cesarean section? Cell Host Microbe. (2022) 30:607–11. doi: 10.1016/j.chom.2022.02.014
17. van Best N, Dominguez-Bello MG, Hornef MW, Jašarević E, Korpela K, Lawley TD. Should we modulate the neonatal microbiome and what should be the goal? Microbiome. (2022) 10:74. doi: 10.1186/s40168-022-01281-4
18. Mueller NT, Hourigan SK, Hoffmann DE, Levy L, von Rosenvinge EC, Chou B, et al. Bacterial baptism: scientific, medical, and regulatory issues raised by vaginal seeding of C-section-born babies. J Law Med Ethics J Am Soc Law Med Ethics. (2019) 47:568–78. doi: 10.1177/1073110519897732
19. Guo C, Zhou Q, Li M, Letian Z, Xu L, Zhang Y, et al. Breastfeeding restored the gut microbiota in caesarean section infants and lowered the infection risk in early life. BMC Pediatr. (2020) 20:532. doi: 10.1186/s12887-020-02433-x
20. Chimoriya R, Scott JA, John JR, Bhole S, Hayen A, Kolt GS, et al. Determinants of full breastfeeding at 6 months and any breastfeeding at 12 and 24 months among women in Sydney: findings from the HSHK birth cohort study. Int J Environ Res Public Health. (2020) 17:E5384. doi: 10.3390/ijerph17155384
21. Martín R, Olivares M, Marín ML, Fernández L, Xaus J, Rodríguez JM. Probiotic potential of 3 Lactobacilli strains isolated from breast milk. J Hum Lact Off J Int Lact Consult Assoc. (2005) 21:8–17; quiz 18–21, 41. doi: 10.1177/0890334404272393
22. Maldonado J, Cañabate F, Sempere L, Vela F, Sánchez AR, Narbona E, et al. Human Milk Probiotic Lactobacillus fermentum CECT5716 reduces the incidence of gastrointestinal and upper respiratory tract infections in infants. J Pediatr Gastroenterol Nutr. (2012) 54:55–61. doi: 10.1097/MPG.0b013e3182333f18
23. Gil-Campos M, López MÁ, Rodriguez-Benítez MV, Romero J, Roncero I, Linares MD, et al. Lactobacillus fermentum CECT 5716 is safe and well tolerated in infants of 1–6 months of age: a randomized controlled trial. Pharmacol Res. (2012) 65:231–8. doi: 10.1016/j.phrs.2011.11.016
24. Maldonado J, Gil-Campos M, Maldonado-Lobón JA, Benavides MR, Flores-Rojas K, Jaldo R, et al. Evaluation of the safety, tolerance and efficacy of 1-year consumption of infant formula supplemented with Lactobacillus fermentum CECT5716 Lc40 or Bifidobacterium breve CECT7263: a randomized controlled trial. BMC Pediatr. (2019) 19:361. doi: 10.1186/s12887-019-1753-7
26. Pastor-Villaescusa B, Blanco-Rojo R, Olivares M. Evaluation of the Effect of Limosilactobacillus fermentum CECT5716 on gastrointestinal infections in infants: a systematic review and meta-analysis. Microorganisms. (2021) 9:1412. doi: 10.3390/microorganisms9071412
27. Quigley MA, Kelly YJ, Sacker A. Breastfeeding and hospitalization for diarrheal and respiratory infection in the United Kingdom Millennium Cohort Study. Pediatrics. (2007) 119:e837–842. doi: 10.1542/peds.2006-2256
28. Miller JE, Goldacre R, Moore HC, Zeltzer J, Knight M, Morris C, et al. et al. Mode of birth and risk of infection-related hospitalisation in childhood: a population cohort study of 717 million births from 4 high-income countries. PLoS Med. (2020) 17:e1003429. doi: 10.1371/journal.pmed.1003429
29. Bentley JP, Simpson JM, Bowen JR, Morris JM, Roberts CL, Nassar N. Gestational age, mode of birth and breastmilk feeding all influence acute early childhood gastroenteritis: a record-linkage cohort study. BMC Pediatr. (2016) 16:55. doi: 10.1186/s12887-016-0591-0
30. Bentley JP, Burgner DP, Shand AW, Bell JC, Miller JE, Nassar N. Gestation at birth, mode of birth, infant feeding and childhood hospitalization with infection. Acta Obstet Gynecol Scand. (2018) 97:988–97. doi: 10.1111/aogs.13371
31. Yang W, Tian L, Luo J, Yu J. Ongoing supplementation of probiotics to cesarean-born neonates during the first month of life may impact the gut microbial. Am J Perinatol. (2021) 38:1181–91. doi: 10.1055/s-0040-1710559
32. Hurkala J, Lauterbach R, Radziszewska R, Strus M, Heczko P. Effect of a short-time probiotic supplementation on the abundance of the main constituents of the gut microbiota of term newborns delivered by cesarean section—a randomized, prospective, controlled clinical trial. Nutrients. (2020) 12:3128. doi: 10.3390/nu12103128
33. Duar R, Kyle D, Tribe R. Reintroducing Bifidobacterium infantis to the Cesarean-born neonate: an ecologically sound alternative to “vaginal seeding.” FEMS Microbiol Lett. (2020) 367:fnaa032. doi: 10.1093/femsle/fnaa032
34. Martín-Peláez S, Cano-Ibáñez N, Pinto-Gallardo M, Amezcua-Prieto C. The impact of probiotics, prebiotics, and synbiotics during pregnancy or lactation on the intestinal microbiota of children born by cesarean section: a systematic review. Nutrients. (2022) 14:341. doi: 10.3390/nu14020341
35. Van Damme P Giaquinto C Huet F Gothefors L Maxwell M Van der Wielen M on on behalf of the REVEAL Study Group. Multicenter prospective study of the burden of rotavirus acute gastroenteritis in Europe, 2004–2005: the reveal study. J Infect Dis. (2007) 195:S4–16. doi: 10.1086/516714
36. Zutavern A, Rzehak P, Brockow I, Schaaf B, Bollrath C, von Berg A, et al. Day care in relation to respiratory-tract and gastrointestinal infections in a German birth cohort study. Acta Paediatr Oslo Nor. (2007) 96:1494–9. doi: 10.1111/j.1651-2227.2007.00412.x
37. Enserink R, Ypma R, Donker GA, Smit HA, van Pelt W. Infectious disease burden related to child day care in the Netherlands. Pediatr Infect Dis J. (2013) 32:e334–40. doi: 10.1097/INF.0b013e318290601e
38. Del Castillo-Aguas G, Gallego-Iborra A, Gutiérrez-Olid M, Pérez-González O, Moreno-Muñoz G, Ledesma-Albarrán JM. Infectious morbidity and resource use in children under 2 years old at childcare centres. J Paediatr Child Health. (2017) 53:116–22. doi: 10.1111/jpc.13372
39. Li Y, Xia S, Jiang X, Feng C, Gong S, Ma J, et al. Gut microbiota and diarrhea: an updated review. Front Cell Infect Microbiol. (2021) 11:625210. doi: 10.3389/fcimb.2021.625210
40. Iacob S, Iacob D. Infectious threats, the intestinal barrier, and its trojan horse: dysbiosis. Front Microbiol. (2019) 10:1676. doi: 10.3389/fmicb.2019.01676
41. Rodríguez-Sojo MJ, Ruiz-Malagón AJ, Rodríguez-Cabezas ME, Gálvez J, Rodríguez-Nogales A. Limosilactobacillus fermentum CECT5716: Mechanisms and Therapeutic Insights. Nutrients. (2021) 13:1016. doi: 10.3390/nu13031016
42. Vanhaecke T, Aubert P, Grohard P-A, Durand T, Hulin P, Paul-Gilloteaux P, et al. L. fermentum CECT 5716 prevents stress-induced intestinal barrier dysfunction in newborn rats. Neurogastroenterol Motil. (2017) 29:e13069. doi: 10.1111/nmo.13069
43. Díaz-Ropero MP, Martín R, Sierra S, Lara-Villoslada F, Rodríguez JM, Xaus J, et al. Two Lactobacillus strains, isolated from breast milk, differently modulate the immune response. J Appl Microbiol. (2007) 102:337–43. doi: 10.1111/j.1365-2672.2006.03102.x
44. Olivares M, Díaz-Ropero MP, Sierra S, Lara-Villoslada F, Fonollá J, Navas M, et al. Oral intake of Lactobacillus fermentum CECT5716 enhances the effects of influenza vaccination. Nutrition. (2007) 23:254–60. doi: 10.1016/j.nut.2007.01.004
45. Olivares M, Diaz-Ropero MP, Martin R, Rodriguez JM, Xaus J. Antimicrobial potential of four Lactobacillus strains isolated from breast milk. J Appl Microbiol. (2006) 101:72–9. doi: 10.1111/j.1365-2672.2006.02981.x
46. Sutherland DB, Fagarasan S. IgA synthesis: a form of functional immune adaptation extending beyond gut. Curr Opin Immunol. (2012) 24:261–8. doi: 10.1016/j.coi.2012.03.005
47. Pabst O, Cerovic V, Hornef M. Secretory IgA in the coordination of establishment and maintenance of the microbiota. Trends Immunol. (2016) 37:287–96. doi: 10.1016/j.it.2016.03.002
48. Pérez-Cano FJ, Dong H, Yaqoob P. In vitro immunomodulatory activity of Lactobacillus fermentum CECT5716 and Lactobacillus salivarius CECT5713: two probiotic strains isolated from human breast milk. Immunobiology. (2010) 215:996–1004. doi: 10.1016/j.imbio.2010.01.004
49. Bangdiwala SI, Bhargava A, O'Connor DP, Robinson TN, Michie S, Murray DM, et al. Statistical methodologies to pool across multiple intervention studies. Transl Behav Med. (2016) 6:228–35. doi: 10.1007/s13142-016-0386-8
50. Arroyo R, Martín V, Maldonado A, Jiménez E, Fernández L, Rodríguez JM. Treatment of infectious mastitis during lactation: antibiotics versus oral administration of Lactobacilli isolated from breast milk. Clin Infect Dis Off Publ Infect Dis Soc Am. (2010) 50:1551–8. doi: 10.1086/652763
Keywords: cesarean section, probiotics, infant formula, gastrointestinal infections, respiratory infections
Citation: Blanco-Rojo R, Maldonado J, Schaubeck M, Özen M, López-Huertas E and Olivares M (2022) Beneficial Effects of Limosilactobacillus fermentum CECT 5716 Administration to Infants Delivered by Cesarean Section. Front. Pediatr. 10:906924. doi: 10.3389/fped.2022.906924
Received: 29 March 2022; Accepted: 14 June 2022;
Published: 07 July 2022.
Edited by:
Maria Elisabetta Baldassarre, University of Bari Aldo Moro, ItalyReviewed by:
Ruggiero Francavilla, University of Bari Aldo Moro, ItalyCopyright © 2022 Blanco-Rojo, Maldonado, Schaubeck, Özen, López-Huertas and Olivares. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ruth Blanco-Rojo, cmJsYW5jb0BiaW9zZWFyY2hsaWZlLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.