 Katharina Meinel1
Katharina Meinel1 Doloresz Szabo2
Doloresz Szabo2 Antal Dezsofi2Sina Pohl1
Antal Dezsofi2Sina Pohl1 Tanja Strini1Theresa Greimel1Victor Aguiriano-Moser1
Tanja Strini1Theresa Greimel1Victor Aguiriano-Moser1 Harald Haidl1
Harald Haidl1 Martin Wagner3
Martin Wagner3 Axel Schlagenhauf1*
Axel Schlagenhauf1* Jörg Jahnel1
Jörg Jahnel1
- 1Division of General Pediatrics, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria
- 2First Department of Pediatrics, Semmelweis University, Budapest, Hungary
- 3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Medical University of Graz, Graz, Austria
Objectives: The exact etiology of pruritus in chronic cholestasis is unknown. Pruritus intensity does not correlate with common biochemical indices and there is a lack of biomarkers guiding diagnosis and treatment. We explored profiles of bile acids (BA) and muricholic acids (MCA) as well as autotaxin (ATX) antigen levels as potential circulating biomarkers of pruritus in pediatric patients.
Methods: In 27 pediatric cholestatic patients [autoimmune sclerosing cholangitis (ASC) n = 20 (with pruritus n = 6, without pruritus n = 14); progressive familial intrahepatic cholestasis (PFIC) n = 7 (with pruritus n = 5, without pruritus n = 2)] and 23 age-matched controls pruritus was assessed by a visual analog scale of pruritus (PVAS). We obtained profiles of serum human BA including MCA using a mass-spectrometry assay and ATX antigen levels with a commercial ELISA.
Results: PFIC and ASC patients exhibited significantly higher BA-, and MCA levels, than healthy controls, but only PFIC patients showed elevated ATX antigen levels higher [median: 1,650 ng/ml, interquartile rang (IQR): 776.9–3,742] compared to controls (median: 315.9 ng/ml, IQR: 251.1–417.2; PFIC p = 0.0003). ASC patients with pruritus showed only a minor increase in total BA (tBA) levels (median: 76.5 μmol/L, IQR: 54.7–205), but strikingly higher T-conjugated BA (median: 16.4 μmol/L, IQR: 8.9–41.4) and total MCA (tMCA) (median: 1.15 μmol/L, IQR: 0.77–2.44) levels compared to ASC patients without pruritus (tBA median: 24.3 μmol/L, IQR: 16.2–80.8; p < 0.0408; T-conjugated BA median: 1.3 μmol/L, IQR: 0.8–4.9; p = 0.0023; tMCA median: 0.30 μmol/L, IQR: 0.13–0.64, p = 0.0033). BA/MCA profiles distinctly differed depending on presence/absence of pruritus. Different from PFIC patients, ATX antigen levels were not significantly elevated in ASC patients with (median: 665.8 ng/ml, IQR: 357.8–1,203) and without pruritus (median: 391.0 ng/ml, IQR: 283.2–485.6). In ASC patients, tBA, tMCA, and ATX antigen levels did not correlate with pruritus severity.
Conclusion: Despite the same underlying disease, pediatric ASC patients with pruritus exhibit significantly altered BA profiles and MCA levels compared to ASC patients without pruritus. ATX antigen levels seem to have little diagnostic or prognostic meaning in ASC patients. An increased ATX activity alone seems not to be causal for pruritus genesis in ASC patients.
Clinical Trial Registration: [www.drks.de], identifier [DRKS00026913].
Introduction
Chronic cholestatic liver diseases (CCLD) are associated with high morbidity and mortality and represent the leading indication for liver transplantation in pediatric patients. Disorders of childhood presenting with chronic cholestasis include autoimmune sclerosing cholangitis (ASC), progressive familial intrahepatic cholestasis (PFIC), and biliary atresia amongst others (1, 2). In children, various CCLD are frequently associated with intractable chronic pruritus. However, pruritus is not imperative in these patients and the exact underlying pathogenesis is unknown (3–5). In the past, enhanced bile acid (BA) levels have been implicated in the etiology of cholestatic pruritus (6, 7). However, no correlation between itch severity and BA levels has ever been established (6, 7) and an occasional reduction of pruritus has been reported in some patients despite progressing cholestatic disorders and persistently increased BA levels (6–8).
Primary BA are synthesized from cholesterol in the liver whereas secondary BA are formed by modification of primary BA in the distal intestine and the colon by bacterial enzymes (9–11). In humans, the primary BA chenodeoxycholic acid (CDCA) and cholic acid (CA) are predominant (9, 12, 13), whereas in mice, tri-hydroxylated, so-called muricholic bile acids (MCA), are prevailing (14). However, MCA were found to be also synthesized in neonates and patients with CCLD (14, 15). Under physiological conditions the major constituent of BA undergoes enterohepatic circulation between liver and small intestine (16, 17), a process which is mainly regulated by BA themselves via the nuclear receptor farnesoid X (FXR) (11, 18, 19). The activation of FXR leads to downregulation of BA uptake systems like ileal BA transporter (IBAT) and increased expression of exporter proteins such as multidrug resistance associated protein 2 and 3 (MRP2/MRP3) amongst others in liver as well as in intestine (11, 16, 20, 21). To increase hydrophilicity most of the BA, but also MCA, are conjugated with either glycine (G) or taurine (T) (10, 22). Two independent enzymatic reactions are particularly involved in the conjugation of BA in the human liver: BA-CoA synthetase (BACS) and BA-CoA amino acid N-acetyltransferase (BAT) (23, 24). The genes encoding for these two key enzymes are direct targets of FXR (24). This may be a hepatoprotective effect as conjugated BA are considered less toxic. Table 1 gives an overview of all BA/MCA investigated in this study.
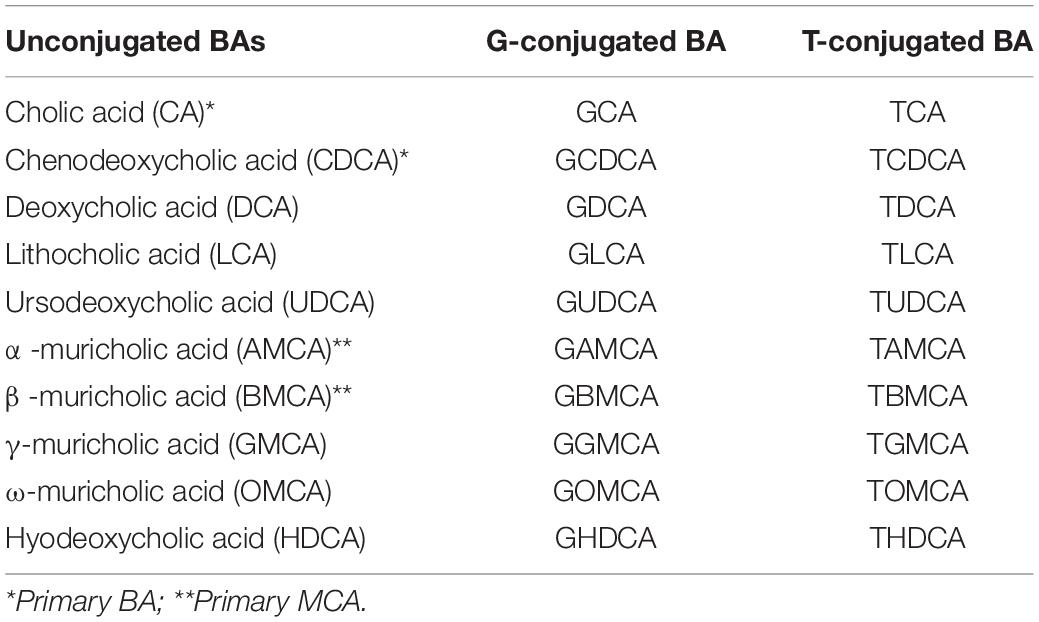
Table 1. Unconjugated bile acids (BA) and C-6 hydroxylated muricholic bile acids (MCA) and their glycine (G) or taurine (T) conjugates analyzed in this study design.
Besides BA, enhanced levels of lysophosphatidic acid (LPA), a potent neuronal activator generated by the enzyme autotaxin (ATX), are assumed to be involved in the pathophysiology of cholestatic pruritus (25, 26). A substantial increase of LPA was found in patients with chronic cholestatic pruritus compared to patients without pruritus (26). Moreover, ATX activity correlated with itch intensity and total BA (tBA) levels in adult and pediatric patients (26, 27), however, the underlying reason for the ATX surge has not been found yet.
We investigated human BA and MCA in pediatric ASC and PFIC patients to test whether specific patterns of human BA including MCA allow discrimination between pediatric ASC/PFIC patients with and without pruritus based solely on laboratory findings that could be used as biomarkers in the future. Furthermore, we wanted to investigate how these alterations correlate with ATX levels and severity of pruritus to gain insight into their specific contribution.
Materials and Methods
Study Design and Patients’ Characteristics
We conducted a prospective study at the First Department of Pediatrics of the Semmelweis University Hungary and the Department of Pediatrics and Adolescents Medicine of the Medical University of Graz, for which we collected serum samples of 50 children aged 1–18 years between August 2018 and March 2020. We included 20 children with ASC (with pruritus n = 6, without pruritus n = 14) and 7 children with PFIC [with pruritus n = 5 (PFIC II n = 5), without pruritus n = 2 (PFIC I n = 1, PFIC II n = 1)], and 23 healthy age-matched controls (Supplementary Figure 1). ASC and PFIC were diagnosed according to the guidelines (28) by liver biopsy and biliary imaging under consideration of laboratory changes of biomarkers indicating hepatobiliary injury. None of our included patients had liver cirrhosis. After an overall comparison of ASC, PFIC patients, and the control group, only ASC patients were stratified according to presence/absence of pruritus. The PFIC cohort had an insufficient number of patients without pruritus.
Visual Analog Scale of Pruritus
The PVAS represents the numbers 0 (“no itch”) to 10 (“worst imaginable itch”). Patients are asked to rate the intensity of their itching using this scale. It features high reliability and concurrent validity and is a popular choice for children 5 years of age, due to its simple format (29). In younger children (<5 years of age), we differentiated only by the existence of pruritus (pruritus: “yes” or “no”). Patients with a PVAS value of 0 were included in the study group of patients without pruritus.
Blood Samples
Non-fasting blood sampling was performed during the routine diagnostic workup. Venous blood samples were collected in serum tubes. Serum of all patients for determination of BA/MCA concentrations and composition of the BA/MCA pool and ATX activity was obtained by centrifugation (2,000 × g, 10 min) before it was frozen at −80°C within 2 h and stored until analysis.
Laboratory Analysis
Concentrations of bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transpeptidase (GGT), alkaline phosphatase (AP) and lactate dehydrogenase (LDH) were measured by standard laboratory methods.
Bile Acid Analysis
BA/MCA levels including unconjugated, T-, and G-conjugated BA/MCA species (Table 1) were measured by high-performance liquid chromatography (HPLC) combined with mass spectrometry (MS) as described previously (30). Briefly, plasma samples were prepared after the protocol of Humbert et al. (31). After addition of internal standards d4-DCA, d4-LCA, d4-GLCA, d4-GCDCA, and d4-TDCA, 0.2 nmol each, plasma samples (10 μl) were vortexed for 1 min. 400 μl of acetonitrile (80% v/v; Sigma Aldrich, Taufkirchen, Germany) were added for deproteination. After vortexing, the precipitate was removed by centrifugation at 3,200 g for 12 min. The supernatant was dried under a stream of nitrogen (40°C). The samples were re-dissolved in 100 μl of mobile phase B (methanol with 1.2% v/v formic acid and 0.38% w/v ammonium acetate) and transferred to an autosampler. Individual BA were separated by HPLC using a reversed-phase C18 column (Macherey-Nagel, Düren, Germany) and a kinetex pentafluorophenyl column (Phenomenex, Aschaffenburg, Germany). Quantification and characterization were achieved using a Q Exactive™ mass spectrometer (Thermo Fisher Scientific, Waltham, MA) and a high-performance quadrupole precursor selection with high-resolution and accurate-mass (HR/AM) Orbitrap™ detection (30).
Human ENPP-2/Autotaxin Immunoassay
The quantitative determination of human ENPP-2/ATX- concentrations in serum samples was performed using the Quantikine® ELISA Human ENPP-2-/ATX Immunoassay (Abcam, Cambridge, MA). Serum samples were diluted 20–50-fold before the assay according to protocol and results were multiplied by the respective dilution factor.
Ethics
This clinical study has been approved by the Hungarian Ethics Committee (43477-/2018/EKU) and the Austrian Ethics Committee (31–337 ex 18/19) and was performed in accordance with the ethics standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Parental consent was obtained for each subject. The trial was registered at the German Clinical Trials Register.1 The trial registration number is DRKS00026913.
Statistical Analysis
The statistical analysis was based on clinical and laboratory findings. A Kruskal-Wallis analysis followed by Dunn’s multiple comparison test was performed to compare data of ASC patients, PFIC patients, and the control group. Comparison of data from ASC patients with/without pruritus was done via Man-Whitney U-test. We calculated BA/MCA profiles for all our ASC patients with and without pruritus and healthy age-matched controls. BA profiling was done through determination of the proportion of every single BA when expressed as a percentage of the tBA level. Spearman’s correlation coefficient and corresponding p-values were used to investigate the relationships between the examined parameters. All statistical analysis was performed in GraphPad Prism software. The changes in the examined parameters (Figures 1–3) were visualized using GraphPad Prism Software.
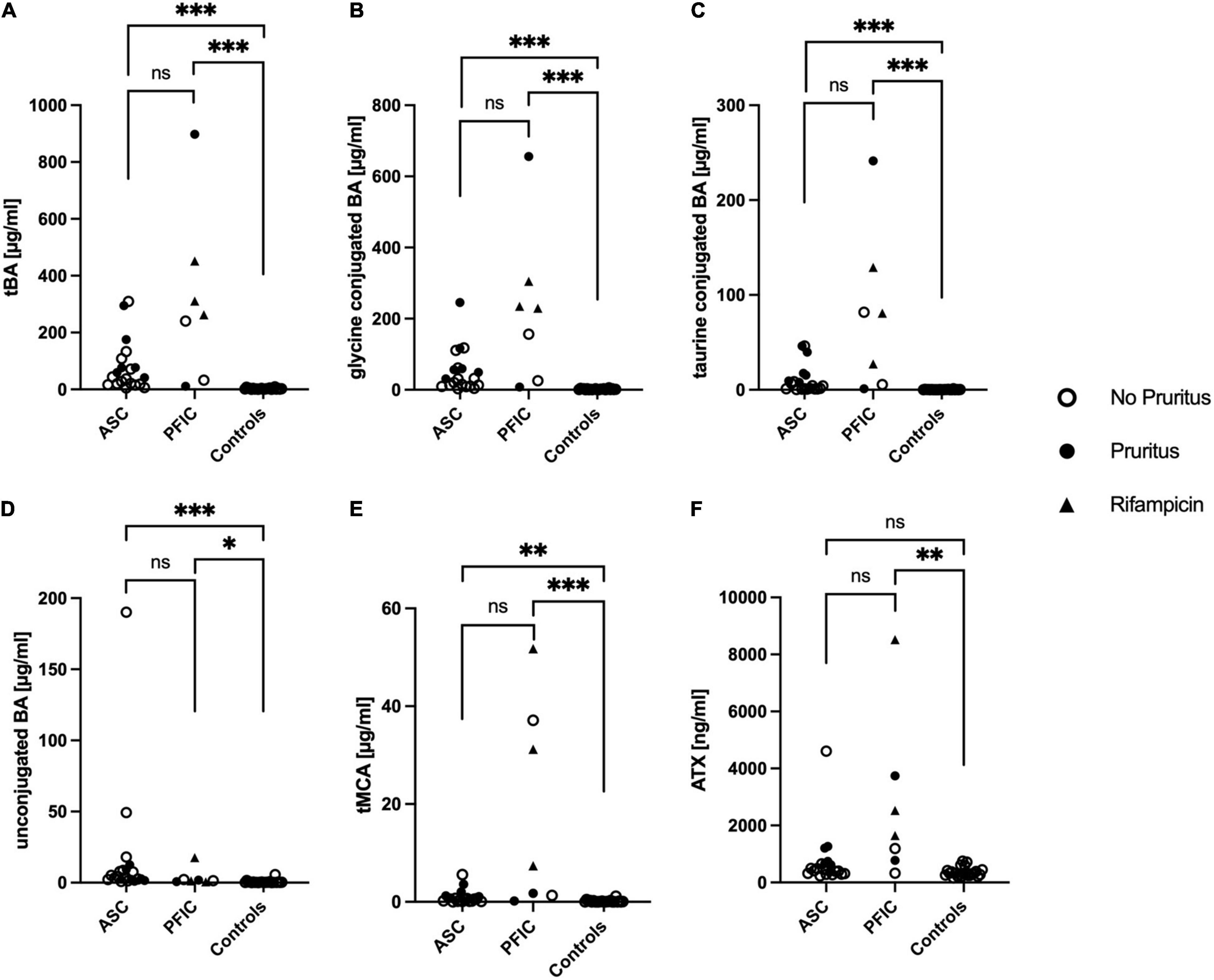
Figure 1. Total bile acids (tBA) (A), taurine conjugated BA (B), glycine conjugated BA (C), unconjugated BA (D), total muricholic bile acids (tMCA) (E), and autotaxin (ATX) antigen levels (F) in pediatric patients with ASC, PFIC and healthy age-matched controls. Significances are indicated with bars and stars within the diagram. *p < 0.05; **p < 0.01; ***p < 0.001.
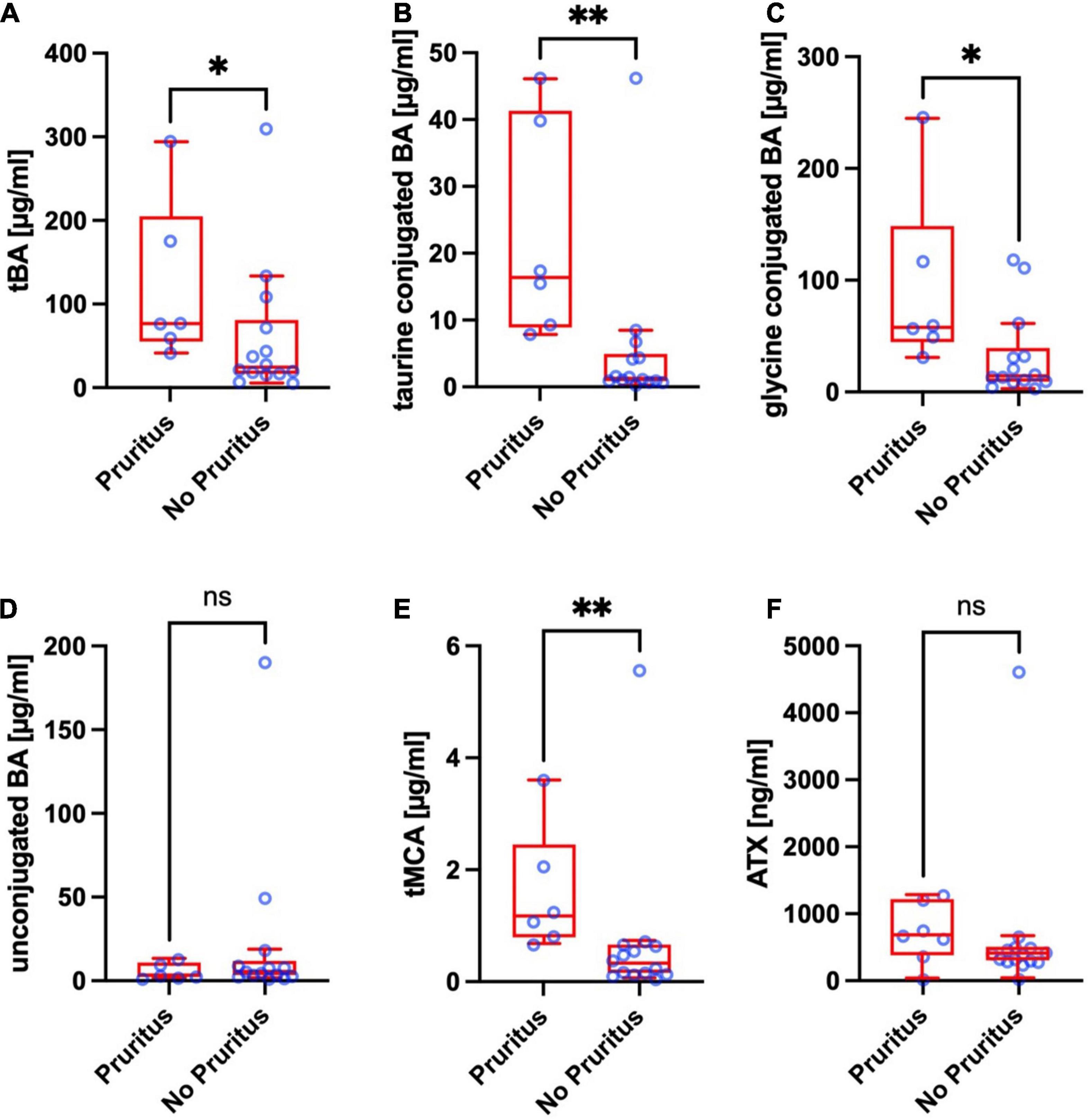
Figure 2. Total bile acids (tBA) (A), taurine conjugated BA (B), glycine conjugated BA (C), unconjugated BA (D), total muricholic bile acids (tMCA) (E), and autotaxin (ATX) antigen levels (F) of pediatric ASC patients with and without pruritus. Significances are indicated with bars and stars within the diagram. *p < 0.05; **p < 0.01.
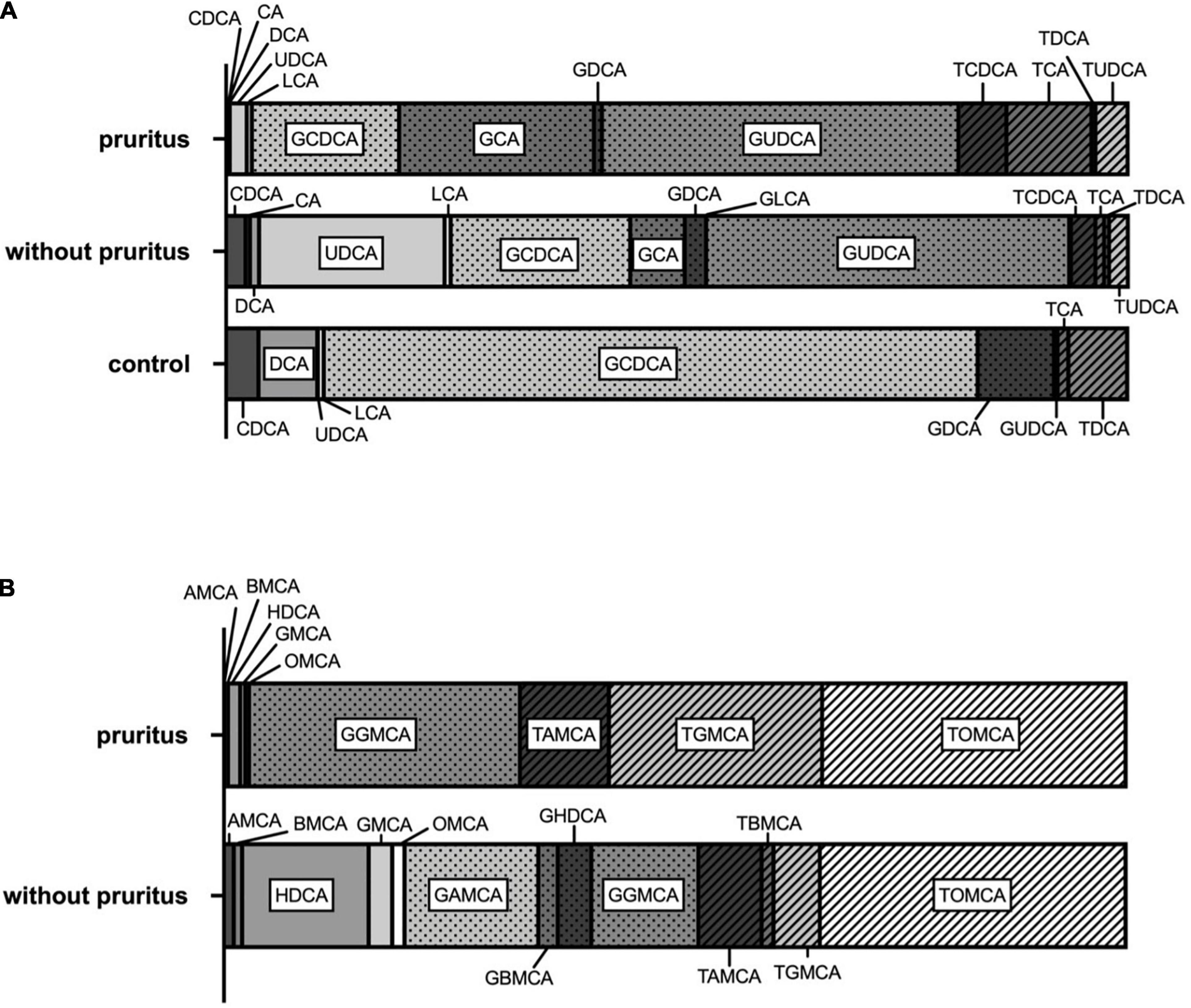
Figure 3. Bile acid profiles (A) and muricholic acid profiles (B) in ASC patients with and without pruritus.
Results
Demographic Data and Clinical Characteristics
The 7 included patients with PFIC were significantly younger [median age 1.5 years, interquartile range (IQR): 1.2–3.0] compared to ASC patients (median age 16 years, IQR: 15–17.8, p < 0.0001) and controls (median age 14 years, IQR: 12.0–16.0, p = 0.0279). This is also reflecting in the smaller height and weight of PFIC patients (median height: 86.0 cm, IQR: 83.0–101.0, median weight: 12.3 kg, IQR: 11.1–16.1) compared to ASC patients (median height 164.0 cm, IQR: 156.3–173.8, p = 0.0004; median weight: 56.1 kg, IQR: 46.9–67.1, p = 0.0001) and controls (median height: 165.0 cm, IQR: 155.0–173.0, p = 0.0010; median weight 57.0 kg, IQR: 42.0–65.0, p 0.0002). All patients with PFIC received oral ursodeoxycholic acid (UDCA). Children with PFIC and intractable pruritus were treated with rifampicin as additional medication (n = 4).
The baseline demographic and clinical characteristics of pediatric ASC patients with and without pruritus and healthy age-matched controls are summarized in Table 2. ASC patients with and without pruritus did not differ significantly concerning age, height, and weight. ASC patients with pruritus showed significantly higher ALT levels (median: 85.5 U/l, IQR: 42.3–135.8) and AST levels (median: 84.5 U/l, IQR: 45.8–84.5) compared to ASC patients without pruritus (ALT: median: 28.5 U/l, IQR: 14.3–59.3, p = 0.0489; AST: median: 32.0 U/l, IQR: 27.3–48.5, p = 0.0322). Furthermore, ASC patients with pruritus had significantly higher serum bilirubin levels (median: 26.0 μmol/l, IQR: 13.5–79.0) than ASC patients without pruritus (median: 10.0 μmol/l, IQR: 6.5–17.9, p = 0.0049). 5 out of 6 patients with ASC with pruritus received oral UDCA. The mean daily dose of UDCA in our ASC patients with and without pruritus is listed in Table 2. In both, pediatric ASC patients with and without pruritus, inflammatory bowel disease (IBD) was the most prevalent comorbidity (IBD in ASC with pruritus n = 3; IBD in ASC without pruritus n = 5). The affected patients received additional medication such as azathioprine, mesalamine, prednisolone, or tacrolimus (Table 2).
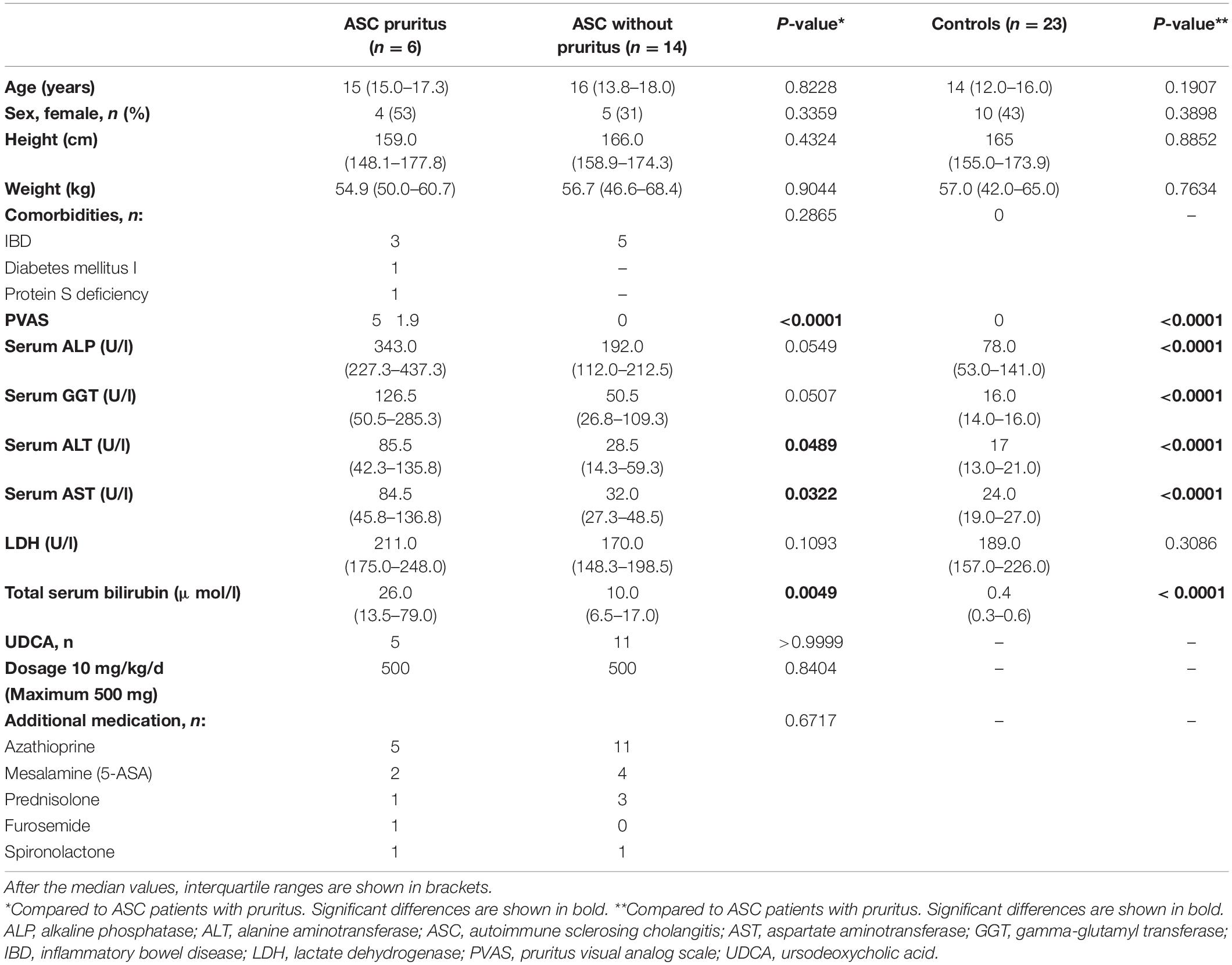
Table 2. Demographic data and biochemical characteristics of ASC patients with and without pruritus and controls.
Comparison of Bile Acid-, Muricholic Acid- and Autotaxin Antigen Levels Between Pediatric Autoimmune Sclerosing Cholangitis Patients, Progressive Familial Intrahepatic Cholestasis Patients, and Healthy Controls
TBA levels were significantly elevated in both, ASC patients (median: 42.4 μmol/L, IQR: 18.5–100.1) and PFIC patients (median: 262.6 μmol/L, IQR: 32.3–451.7) compared to age-matched controls (median: 1.7 μmol/L, IQR: 0.9–3.6; ASC p < 0.0001; PFIC p < 0.0001). There was no statistically significant difference in tBA levels between ASC and PFIC patients (p = 0.7936) (Figure 1A). The G- and T-conjugated BA, as well as the unconjugated BA, were significantly higher in ASC- and PFIC patients compared to age-matched controls (ASC: G-conjugated BA p < 0.0001, T-conjugated BA p < 0.0001, unconjugated BA p < 0.0001; PFIC: G-conjugated BA p < 0.0001, T-conjugated BA p < 0.0001, unconjugated BA p = 0.0262) (Figures 1B–D and Table 3). However, no statistically significant difference between ASC and PFIC patients concerning G-conjugated BA (p = 0.6911), T-conjugated BA (p = 0.4733), or unconjugated BA (p = 0.5628) could have been found (Figures 1B–D and Table 3).
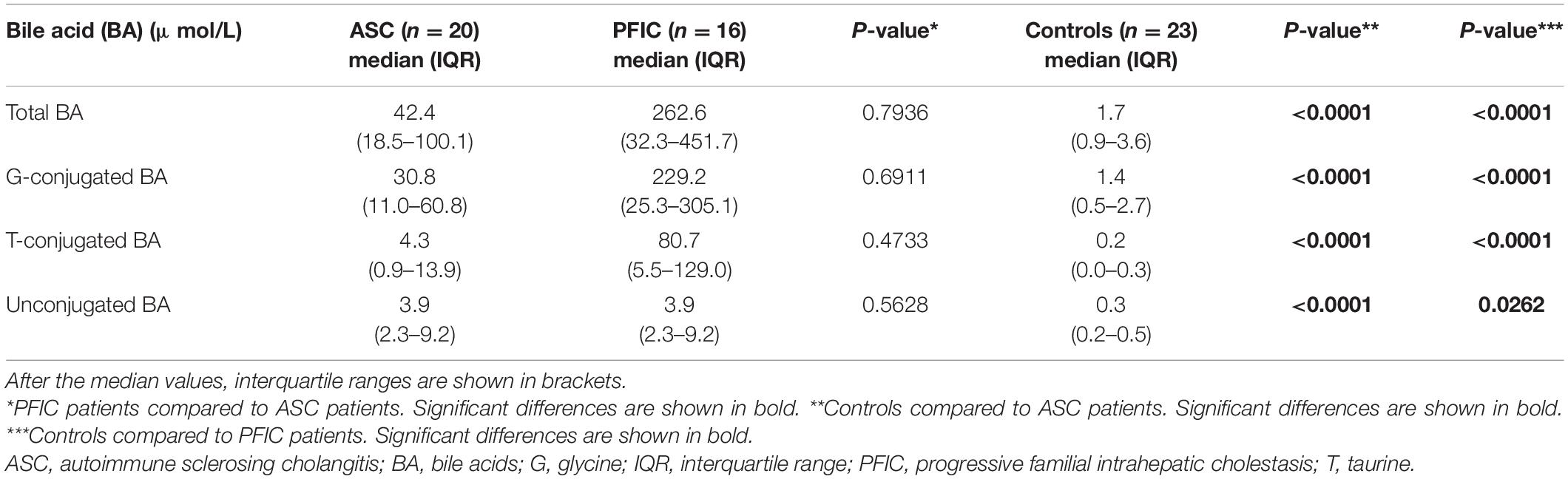
Table 3. Total bile acid levels in pediatric ASC- and PFIC patients with and without pruritus and controls.
Equivalently to tBA, total MCA (tMCA) were significantly higher in ASC patients (median: 0.59 μmol/L, IQR: 0.16–1.00) and in PFIC patients (median: 7.39 μmol/L, IQR: 1.31–37.13) compared to age-matched controls (median: 0.05 μmol/L, IQR: 0.001–0.16, ASC p = 0.0006; PFIC p < 0.0001). TMCA levels in ASC and PFIC patients did not differ significantly (p = 0.1807) (Figure 1E).
Only in PFIC patients, ATX antigen levels were significantly higher (median: 1,650 ng/ml, IQR: 776.9–3,742) than in age-matched controls (median: 315.9 ng/ml, IQR: 251.1–417.2; PFIC p = 0.0003). We could neither find a statistically significant difference of ATX antigen levels between ASC patients (median: 435.9 ng/ml, IQR: 315.8–662.8) and age-matched controls (p = 0.0721) not between ASC- and PFIC patients (p = 0.0713) (Figure 1F).
Due to the small study group of PFIC patients, only ASC patient were stratified according to presence/absence of pruritus in the following.
Total Bile Acid Levels in Pediatric Autoimmune Sclerosing Cholangitis Patients
In ASC patients with pruritus, tBA levels were slightly but significantly higher (median: 76.5 μmol/L, IQR: 54.7–205.1) compared to ASC patients without pruritus (median: 24.3 μmol/L, IQR: 16.2–80.8; p < 0.0408) (Figure 2A). The T-conjugated BA were substantially higher in ASC patients with pruritus (median: 16.4 μmol/L, IQR: 8.9–41.4) than in ASC patients without pruritus (median: 1.3 μmol/L, IQR: 0.8–4.9; p = 0.0023) (Figure 2B). Likewise, G-conjugated BA were significantly increased in ASC patients with pruritus (median: 57.9 μmol/L, IQR: 44.6–148.8) compared to ASC patients without pruritus (median: 14.3 μmol/L, IQR: 9.2–39.3; p = 0.0200) (Figure 2C). There was no statistically significant difference in unconjugated BA between ASC patients with and without pruritus (p = 0.4442) (Figure 2D).
Bile Acid Profiles in Pediatric Autoimmune Sclerosing Cholangitis Patients
The BA profiles of ASC patients with and without pruritus and healthy age-matched controls are shown in Figure 3A. The relative contribution of unconjugated BA levels to the total BA pool was lower in pediatric ASC patients with pruritus compared to ASC patients without pruritus including a substantially smaller fraction of UDCA. In contrast, T-conjugated BA made up a larger proportion in ASC patients with pruritus compared to patients without pruritus. G-conjugated BA predominated in all study groups. The G-conjugated primary BA, CDCA, and CA, and the secondary BA, UDCA, predominated in both, ASC patients with and without pruritus.
Muricholic Bile Acid Levels in Pediatric Autoimmune Sclerosing Cholangitis Patients
TMCA levels in ASC patients with pruritus were substantially higher (median: 1.15 μmol/L, IQR: 0.77–2.44) compared to ASC patients without pruritus (median: 0.30 μmol/L, IQR: 0.13–0.64, p = 0.0033) (Figure 2E).
Muricholic Acid Profiles in Pediatric Autoimmune Sclerosing Cholangitis Patients
The MCA profiles of ASC patients with and without pruritus are shown in Figure 3B. Generally, in ASC patients with pruritus, the MCA pool showed a larger variance. Same as in “typical” BA profiles, unconjugated MCA were lower in ASC patients with pruritus with a predominance of HDCA. In both, ASC patients with and without pruritus, T-conjugated MCA constituted a larger fraction than in “typical” BA profiles. Especially TOMCA was detectable in equal amounts in both groups. In ASC patients with pruritus, TGMCA and TAMCA and GGMCA were the most frequent MCA. In ASC patients without pruritus, the relative contribution of G-conjugated MCA to the total MCA pool was larger than in ASC patients without pruritus with a predominance of GAMCA and GGMCA.
Autotaxin Antigen Levels in Pediatric Autoimmune Sclerosing Cholangitis Patients
ATX antigen levels in ASC patients with pruritus, (median: 665.8 ng/ml, IQR: 357.8–1,203) and in ASC patients without pruritus (median: 391.0 ng/ml, IQR: 283.2–485.6) were not significantly different (p = 0.1061) (Figure 2F).
Correlation of Autotaxin, Visual Analog Scale of Pruritus, Bile Acids and Muricholic Acids in Pediatric Autoimmune Sclerosing Cholangitis Patients
ATX antigen levels correlated significantly with serum tBA levels in pediatric ASC patients with pruritus (Spearman r = 1, p = 0.0028) but not with tBA levels in ASC patients without pruritus (Spearman r = 0.53, p = 0.079). Moreover, ATX antigen levels correlated significantly with T- and G-conjugated BA in ASC patients with pruritus (T: r = 0.8857, p = 0.0333; G: r = 0.9429, p = 0.0167), and without pruritus (T: r = 0.7231, p = 0.0047; G: r = 0.5956, p = 0.0274).
Interestingly, ATX antigen levels did not correlate significantly with tMCA levels in pediatric ASC patients with pruritus (Spearman r = 0.37; p = 0.4972) but with tMCA levels in patients without pruritus (Spearman r = 0.87; p = 0.0001).
PVAS values did not correlate with tBA levels (Spearman r = 0.05, p = 0.9316), tMCA levels (Spearman r = 0.62, p = 0.3787) or ATX values (Spearman r = 0.38, p = 0.4722) in pediatric patients with ASC and pruritus. Moreover, PVAS did not correlate with T-conjugated BA (r = 0.4348, p = 0.3778), G conjugated BA (r = 0.4928, p = 0.3333), or unconjugated BA (r = 0.3189, p = 0.5556) in ASC patients with pruritus.
Discussion
Various CCLD such as PFIC or ASC are frequently associated with chronic pruritus in pediatric but also in adult patients. However, the exact etiology is unknown and itch intensity does not correlate with CCLD severity or common biochemical indices of liver disease (3, 4). Furthermore, the treatment of chronic cholestatic pruritus represents a clinical challenge: Rifampicin is a PXR-agonist, which increases the metabolism and secretion of pruritogenic substances and is often used as first-line therapy in children but not consistently effective (32, 33). Albeit widely prescribed, the use of UDCA in CCLD is highly controversial as it has not been shown to ameliorate pruritus in PBC or PSC (34–36). In cholestatic states in which BA secretion in bile and intestine is low, such as PFIC or biliary atresia, anion exchanger resins as cholestyramine have low efficacy (37, 38). Medications modulating central pruritus-transmission include opioid antagonists, like naltrexone or naloxone, and SSRI. An improvement of pruritus has been suggested in small pediatric series only (39–41). Novel therapeutic options for pruritus in CCLD are ASBT-inhibitors, such as odevixibat, which inhibit ileal BA reabsorption. In children, improvement of pruritus severity was reported with PFIC and various other CCLD (42, 43). Another targeted therapeutic option is the chaperone 4-phenylbutyrate, which has been tested in children with PFIC2. Treatment with 4-phenylbutyrate was associated with re-expression of BSEP and improvement of pruritus (44). As most available therapeutic options are largely empiric new insights into the pathophysiology of chronic pruritus in cholestasis are indispensable in pediatric and adult populations.
In our study, we found significantly higher tBA levels in pediatric PFIC and ASC patients independently of existing pruritus compared to healthy age-matched controls which was expected since it is characteristic for PFIC/ASC pathophysiology. Especially the G- and T-conjugated BA were significantly higher in both, PFIC and ASC patients.
However, in ASC patients with pruritus, we found only slightly higher tBA levels compared to ASC patients without pruritus and no correlation between tBA and PVAS. This is in line with other studies investigating adult and pediatric CCLD patients with pruritus that could not demonstrate a correlation between pruritus severity and tBA levels or single BA levels, respectively (5, 6). Kremer et al. reported a correlation of tBA and PVAS in pediatric CCLD patients with pruritus (26), which we did not observe. However, they included children suffering from Alagille syndrome, extrahepatic biliary atresia, neonatal sclerosing cholangitis, and PFIC but not ASC patients.
On the other hand, we found an altered serum BA profile associated with pruritus. T-conjugated BA were significantly higher and the fraction of unconjugated BA in the total BA pool was lower in ASC patients with pruritus compared to ASC patients without pruritus. A higher degree of conjugation may be caused by upregulation of BACS and BAT secondary to increased FXR stimulation (23, 24). An alternative explanation would be decreased deconjugation by gut microbiomes with reduced bile salt hydroxylase. We could not test this hypothesis, since stool samples were not available for microbiome analysis. Based on our findings, a clinical differentiation of ASC with and without pruritus seems useful in children and adolescents as BA profiles were not comparable despite the same underlying disease. Furthermore, the higher concentration of T-conjugated BA is an interesting finding because differing ratios of G- vs. T-conjugates have been reported in PBC vs. PSC patients (45) and may be associated with a varying autoimmune component. The potential role of T-conjugated BA in the development of pruritus remains to be investigated.
Same as with human tBA, tMCA were significantly increased in PFIC and ASC patients compared to controls. TMCA levels were highest in our PFIC patients with rifampicin-therapy, which is known to induce C6-hydroxylation. Pediatric ASC patients with pruritus had significantly higher tMCA levels compared to ASC patients without pruritus. Furthermore, we found a distinctly different MCA profile in ASC patients with pruritus compared to ASC patients without pruritus featuring less heterogenicity.
Besides usual BA, the existence of MCA, a group of tri-hydroxylated BA mainly found in mice, is reported in umbilical cord blood and amniotic fluid from neonates (14, 15). Interestingly, various MCA have been identified in patients with cholestatic liver diseases (46), which suggests the existence of some altered pathways of BA metabolism in fetal, neonatal, and cholestatic liver. Alternatively, MCA may constitute a minuscule fraction of the normal human BA pool becoming increasingly detectable with accumulation during cholestasis. MCA are also influencing FXR: AMCA is considered to have antagonistic effects (47). Interestingly, T-conjugation (TAMCA) predominated in our ASC patients with pruritus whereas G-conjugation (GAMCA) was prevailing in ASC patients without pruritus. If there is a difference in the antagonistic potential of FXR between TAMCA and GAMCA, however, needs further investigation.
TOMCA was previously found to be significantly increased in preterm neonates with early onset sepsis compared to preterm controls and was therefore considered as potential biomarker in septic neonates (48). However, TOMCA levels were comparable in our study cohort and could therefore not distinguish between ASC patients with or without pruritus. Therefore, the diagnostic potential of TOMCA and MCA in general needs further investigation by ongoing studies in pediatric CCLD patients with pruritus. On the one hand, UDCA and HDCA levels were substantially lower in our patients with ASC patients with pruritus, compared to ASC patients without pruritus. Hence, a potential role of UDCA and HDCA as possible biomarkers for pruritus in pediatric ASC patients are conceivable. On the other hand, reduction of UDCA and HDCA might be a general sign of aggravated cholestasis and upregulation of conjugating enzymes (BAC, BAT) secondary to FXR overstimulation (23, 24).
In our study, ATX antigen levels were significantly elevated in PFIC patients but not in ASC patients compared to control subjects. In ASC patients, ATX antigen levels were neither significantly increased compared to age-matched controls, nor did they significantly differ in dependence of presence/absence of pruritus.
We measured ATX antigen, as it has been shown to play a role in cholestatic pruritus by generating LPA, a potent neuronal activator, which is considered as potential pruritogen (49). Kremer et al. found an increased ATX activity in serum of cholestatic adult patients (intrahepatic cholestasis in pregnancy, primary biliary cirrhosis) with pruritus compared to cholestatic adult patients without pruritus. Furthermore, ATX activity correlated with the intensity of pruritus (27, 50). Besides adult patients, Kremer et al. also described significantly increased ATX levels in pediatric CCLD patients with pruritus (Alagille syndrome, extrahepatic biliary atresia, neonatal sclerosing cholangitis, PFIC) compared to children with BA synthesis defects, in which pruritus is typically not observed and tBA are low (26). Same as in the study of Kremer et al. ATX levels correlated with tBA- but not with tMCA levels in our pediatric ASC patients with and without pruritus (26). Based on our findings, ATX antigen levels seem to have little diagnostic or prognostic meaning in ASC patients different to other CCLD such as Alagille syndrome or PFIC. Furthermore, an increased ATX activity alone seems not to be causal for pruritus genesis in ASC patients.
To the best of our knowledge this is the first study representing a distinct different BA- and MCA profile and enhanced tMCA levels in ASC patients with pruritus compared to ASC patients without pruritus. The novelty of this paper is the investigation of MCA, which, in contrast to “typical” BA show a substantial surge in ASC patients with pruritus and an almost complete differentiation of murine BA levels between the groups. This surge of murine BA is a novel phenotypic observation associated with pruritus that may allow a better classification of ASC patients.
We acknowledge that the representativeness of our result may be limited due to a small number of analyzed patients per study group and need therefore further investigation by ongoing studies. However, we think that our findings have a clinical impact as they give new insights of the pathophysiological course of ASC patients and indicate that the extent of ATX activity alone is not a trigger of pruritus in pediatric ASC patients. Moreover, we acknowledge that the serum samples of our study groups were taken in a non-fasting state which was due to ethical reasons in the pediatric age group. For that reason, alterations compared to fasting states cannot be excluded entirely between our PFIC/ASC patients with and without pruritus. Furthermore, ongoing in-vitro studies investigating the cellular source of ATX and the influence of BA on ATX secretion need to exclude confounding factors.
Conclusion
To date, data in the pediatric population suffering pruritus in cholestasis are sparse. To our knowledge, this is the first study in pediatric patients investigating MCA levels and BA/MCA profiles in children with PFIC and ASC with and without pruritus.
In summary, we observed slightly elevated serum tBA and significantly elevated tMCA levels in pediatric ASC patients with pruritus compared to pediatric ASC patients without pruritus and age-matched controls. Particularly due to increased T conjugated BA/MCA, pediatric ASC patients with pruritus show a distinctly different BA- and MCA profile than ASC patients without pruritus despite the same underlying disease. Different to PFIC patients, ATX antigen levels were not significantly increased in ASC patients compared to controls. Moreover, we could not find significant differences in ATX antigen levels between ASC patients with or without pruritus indicating that ATX is not the sole cause for pruritus genesis in ASC patients contrasting other CCLD such as Alagille syndrome or PFIC. However, our results need further investigation by ongoing in-vitro studies investigating the cellular source of ATX. Even though the exact pathophysiology of pruritus in cholestasis remains unknown, a clinical differentiation of ASC with and without pruritus seems useful in children and adolescents.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Hungarian Ethics Committee (43477-/2018/EKU) Austrian Ethics Committee (31–337 ex 18/19). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
KM and JJ conceived the initial idea and wrote the manuscript with the support of AS. DS and AD provided demographic data and serum samples and our pediatric study group with chronic cholestatic liver diseases. KM, SP, and TS planned and performed the measurements. KM analyzed the data and constructed figures and tables. All authors provided critical feedback and helped shape the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.903360/full#supplementary-material
Supplementary Figure 1 | Overview of groups and number of all pediatric participants. ASC, autoimmune sclerosing cholangitis; PFIC, progressive familial intrahepatic cholestasis.
Footnotes
References
1. Girard M, Franchi-Abella S, Lacaille F, Debray D. Specificities of sclerosing cholangitis in childhood. Clin Res Hepatol Gastroenterol. (2012) 36:530–5. doi: 10.1016/j.clinre.2012.04.003
2. Bull LN, Thompson RJ. Progressive familial intrahepatic cholestasis. Clin Liver Dis. (2018) 22:657–69. doi: 10.1016/j.cld.2018.06.003
3. Bunchorntavakul C, Reddy KR. Pruritus in chronic cholestatic liver disease. Clin Liver Dis. (2012) 16:331–46. doi: 10.1016/j.cld.2012.03.010
4. Mela M, Mancuso A, Burroughs AK. Review article: pruritus in cholestatic and other liver diseases. Aliment Pharmacol Ther. (2003) 17:857–70. doi: 10.1046/j.1365-2036.2003.01458.x
5. Kremer AE, Oude Elferink RPJ, Beuers U. Pathophysiology and current management of pruritus in liver disease. Clin Res Hepatol Gastroenterol. (2011) 35:89–97. doi: 10.1016/j.clinre.2010.10.007
6. Ghent CN, Bloomer JR, Klatskin G. Elevations in skin tissue levels of bile acids in human cholestasis: relation to serum levels and to pruritus. Gastroenterology. (1977) 73:1125–30. doi: 10.1016/s0016-5085(19)31870-0
7. Alemi F, Kwon E, Poole DP, Lieu TM, Lyo V, Cattaruzza F, et al. The TGR5 receptor mediates bile acid-induced itch and analgesia. J Clin Invest. (2013) 123:1513–30. doi: 10.1172/JCI64551
8. Murphy GM, Ross A, Billing BH. Serum bile acids in primary biliary cirrhosis. Gut. (1972) 13:201–6. doi: 10.1136/gut.13.3.201
9. Hofmann AF. The continuing importance of bile acids in liver and intestinal disease. Arch Intern Med. (1999) 159:2647–58. doi: 10.1001/archinte.159.22.2647
11. Perino A, Demagny H, Velazquez-Villegas L, Schoonjans K. Molecular physiology of bile acid signaling in health, disease, and aging. Physiol Rev. (2021) 101:683–731. doi: 10.1152/physrev.00049.2019
12. Theiler-Schwetz V, Zaufel A, Schlager H, Obermayer-Pietsch B, Fickert P, Zollner G. Bile acids and glucocorticoid metabolism in health and disease. Biochim Biophys Acta Mol Basis Dis. (2019) 1865:243–51. doi: 10.1016/j.bbadis.2018.08.001
13. Trauner M, Claudel T, Fickert P, Moustafa T, Wagner M. Bile acids as regulators of hepatic lipid and glucose metabolism. Dig Dis. (2010) 28:220–4. doi: 10.1159/000282091
14. Shoda J, Mahara R, Osuga T, Tohma M, Ohnishi S, Miyazaki H, et al. Similarity of unusual bile acids in human umbilical cord blood and amniotic fluid from newborns and in sera and urine from adult patients with cholestatic liver diseases. J Lipid Res. (1988) 29:847–58. doi: 10.1016/s0022-2275(20)38479-0
15. Nakagawa M, Setchell KDR. Bile acid metabolism in early life: studies of amniotic fluid. J Lipid Res. (1990) 31:1089–98. doi: 10.1016/s0022-2275(20)42749-x
16. Chiang JYL. Bile acids: regulation of synthesis. J Lipid Res. (2009) 50:1955–66. doi: 10.1194/jlr.R900010-JLR200
17. Hofmann AF, Hagey LR. Bile acids: chemistry, pathochemistry, biology, pathobiology, and therapeutics. Cell Mol Life Sci. (2008) 65:2461–83. doi: 10.1007/s00018-008-7568-6
18. Parks DJ, Blanchard SG, Bledsoe RK, Chandra G, Consler TG, Kliewer SA, et al. Bile acids: natural ligands for an orphan nuclear receptor. Science (80). (1999) 284:1365–8. doi: 10.1126/science.284.5418.1365
19. Makishima M, Okamoto AY, Repa JJ, Tu H, Learned RM, Luk A, et al. Identification of a nuclear receptor for bite acids. Science (80). (1999) 284:1362–5. doi: 10.1126/science.284.5418.1362
20. Grobert J, Zaghini I, Fujii H, Jones SA, Kliewer SA, Willson TM, et al. Identification of a bile acid-responsive element in the human ileal bile acid-binding protein gene. Involvement of the farnesoid X receptor/9-cis- retinoic acid receptor heterodimer. J Biol Chem. (1999) 274:29749–54. doi: 10.1074/jbc.274.42.29749
21. Landrier JF, Eloranta JJ, Vavricka SR, Kullak-Ublick GA. The nuclear receptor for bile acids, FXR, transactivates human organic solute transporter-α and -β genes. Am J Physiol Gastrointest Liver Physiol. (2006) 290:G476–85. doi: 10.1152/ajpgi.00430.2005
22. Hofmann AF. Bile acids: the good, the bad, and the ugly. News Physiol Sci. (1999) 14:24–9. doi: 10.1152/physiologyonline.1999.14.1.24
23. Makino I, Nakagawa S, Mashimo K. Conjugated and unconjugated serum bile acid levels in patients with hepatobiliary diseases. Gastroenterology. (1969) 56:1033–103. doi: 10.1016/S0016-5085(69)80004-1
24. Pircher PC, Kitto JL, Petrowski ML, Tangirala RK, Bischoff ED, Schulman IG, et al. Farnesoid X receptor regulates bile acid-amino acid conjugation. J Biol Chem. (2003) 278:27703–11. doi: 10.1074/jbc.M302128200
25. Hausmann J, Perrakis A, Moolenaar WH. Structure-function relationships of autotaxin, a secreted lysophospholipase D. Adv Biol Regul. (2013) 53:112–7. doi: 10.1016/j.jbior.2012.09.010
26. Kremer AE, Gonzales E, Schaap FG, Oude Elferink RPJ, Jacquemin E, Beuers U. Serum autotaxin activity correlates with pruritus in pediatric cholestatic disorders. J Pediatr Gastroenterol Nutr. (2016) 62:530–5. doi: 10.1097/MPG.0000000000001044
27. Kremer AE, Martens JJWW, Kulik W, Rueff F, Kuiper EMM, Van Buuren HR, et al. Lysophosphatidic acid is a potential mediator of cholestatic pruritus. Gastroenterology. (2010) 139:1008–18, 1018.e1. doi: 10.1053/j.gastro.2010.05.009
28. Fawaz R, Baumann U, Ekong U, Fischler B, Hadzic N, Mack CL, et al. Guideline for the evaluation of cholestatic jaundice in infants: joint recommendations of the North American society for pediatric gastroenterology, hepatology, and nutrition and the European society for pediatric gastroenterology, hepatology, and nutriti. J Pediatr Gastroenterol Nutr. (2017) 64:154–68. doi: 10.1097/MPG.0000000000001334
29. Reich A, Riepe C, Anastasiadou Z, Medrek K, Augustin M, Szepietowski JC, et al. Itch assessment with visual analogue scale and numerical rating scale: determination of minimal clinically important difference in chronic itch. Acta Derm Venereol. (2016) 96:978–80. doi: 10.2340/00015555-2433
30. Amplatz B, Zöhrer E, Haas C, Schäffer M, Stojakovic T, Jahnel J, et al. Bile acid preparation and comprehensive analysis by high performance liquid chromatography–high-resolution mass spectrometry. Clin Chim Acta. (2017) 464:85–92. doi: 10.1016/j.cca.2016.11.014
31. Humbert L, Maubert MA, Wolf C, Duboc H, Mahé M, Farabos D, et al. Bile acid profiling in human biological samples: comparison of extraction procedures and application to normal and cholestatic patients. J Chromatogr B Anal Technol Biomed Life Sci. (2012) 899:135–45. doi: 10.1016/j.jchromb.2012.05.015
32. Cynamon HA, Andres JM, Iafrate RP. Rifampin relieves pruritus in children with cholestatic liver disease. Gastroenterology. (1990) 98:1013–6. doi: 10.1016/0016-5085(90)90027-X
33. El-Karaksy H, Mansour S, El-Sayed R, El-Raziky M, El-Koofy N, Taha G. Safety and efficacy of rifampicin in children with cholestatic pruritus. Indian J Pediatr. (2007) 74:279–81. doi: 10.1007/S12098-007-0044-8
34. Lindor KD. Ursodiol for primary sclerosing cholangitis. N Engl J Med. (1997) 336:691–5. doi: 10.1056/NEJM199703063361003
35. Talwalkar JA, Souto E, Jorgensen RA, Lindor KD. Natural history of pruritus in primary biliary cirrhosis. Clin Gastroenterol Hepatol. (2003) 1:297–302. doi: 10.1016/S1542-3565(03)00134-4
36. Beuers U, Spengler U, Kruis W, Aydemir U, Wiebecke B, Heldwein W, et al. Ursodeoxycholic acid for treatment of primary sclerosing cholangitis: a placebo-controlled trial. Hepatology. (1992) 16:707–14. doi: 10.1002/hep.1840160315
37. Kronsten V, Fitzpatrick E, Baker A. Management of cholestatic pruritus in paediatric patients with alagille syndrome: the king’s college hospital experience. J Pediatr Gastroenterol Nutr. (2013) 57:149–54. doi: 10.1097/MPG.0b013e318297e384
38. Kuiper EMM, van Erpecum KJ, Beuers U, Hansen BE, Thio HB, de Man RA, et al. The potent bile acid sequestrant colesevelam is not effective in cholestatic pruritus: results of a double-blind, randomized, placebo-controlled trial. Hepatology. (2010) 52:1334–40. doi: 10.1002/hep.23821
39. Chang Y, Golkar L. The use of naltrexone in the management of severe generalized pruritus in biliary atresia: report of a case. Pediatr Dermatol. (2008) 25:403–4. doi: 10.1111/j.1525-1470.2008.00699.x
40. Zellos A, Roy A, Schwarz KB. Use of oral naltrexone for severe pruritus due to cholestatic liver disease in children. J Pediatr Gastroenterol Nutr. (2010) 51:787–9. doi: 10.1097/MPG.0b013e3181eb5ac0
41. Thébaut A, Habes D, Gottrand F, Rivet C, Cohen J, Debray D, et al. Sertraline as an additional treatment for cholestatic pruritus in children. J Pediatr Gastroenterol Nutr. (2017) 64:431–5. doi: 10.1097/MPG.0000000000001385
42. Baumann U, Sturm E, Lacaille F, Gonzalès E, Arnell H, Fischler B, et al. Effects of odevixibat on pruritus and bile acids in children with cholestatic liver disease: phase 2 study. Clin Res Hepatol Gastroenterol. (2021) 45:101751. doi: 10.1016/j.clinre.2021.101751
43. Thébaut A, Debray D, Gonzales E. An update on the physiopathology and therapeutic management of cholestatic pruritus in children. Clin Res Hepatol Gastroenterol. (2018) 42:103–9. doi: 10.1016/j.clinre.2017.08.007
44. Gonzales E, Grosse B, Cassio D, Davit-Spraul A, Fabre M, Jacquemin E. Successful mutation-specific chaperone therapy with 4-phenylbutyrate in a child with progressive familial intrahepatic cholestasis type 2. J Hepatol. (2012) 57:695–8. doi: 10.1016/j.jhep.2012.04.017
45. Trottier J, Białek A, Caron P, Straka RJ, Heathcote J, Milkiewicz P, et al. Metabolomic profiling of 17 bile acids in serum from patients with primary biliary cirrhosis and primary sclerosing cholangitis: a pilot study. Dig Liver Dis. (2012) 44:303–10. doi: 10.1016/J.DLD.2011.10.025
46. Summerfield JA, Billing BH, Shackleton CH. Identification of bile acids in the serum and urine in cholestasis. Evidence for 6alpha-hydroxylation of bile acids in man. Biochem J. (1976) 154:507–16. doi: 10.1042/bj1540507
47. Sayin SI, Wahlström A, Felin J, Jäntti S, Marschall HU, Bamberg K, et al. Gut microbiota regulates bile acid metabolism by reducing the levels of tauro-beta-muricholic acid, a naturally occurring FXR antagonist. Cell Metab. (2013) 17:225–35. doi: 10.1016/j.cmet.2013.01.003
48. Zöhrer E, Meinel K, Fauler G, Moser VA, Greimel T, Zobl J, et al. Neonatal sepsis leads to early rise of rare serum bile acid tauro-omega-muricholic acid (TOMCA). Pediatr Res. (2018) 84:66–70. doi: 10.1038/s41390-018-0007-y
49. Tokumura A, Majima E, Kariya Y, Tominaga K, Kogure K, Yasuda K, et al. Identification of human plasma lysophospholipase D, a lysophosphatidic acid-producing enzyme, as autotaxin, a multifunctional phosphodiesterase. J Biol Chem. (2002) 277:39436–42. doi: 10.1074/jbc.M205623200
Keywords: muricholic acid, autotaxin (ATX), bile acid (BA), autoimmune sclerosing cholangitis, pediatrics, pruritus, progressive familial intrahepatic cholestasis
Citation: Meinel K, Szabo D, Dezsofi A, Pohl S, Strini T, Greimel T, Aguiriano-Moser V, Haidl H, Wagner M, Schlagenhauf A and Jahnel J (2022) The Covert Surge: Murine Bile Acid Levels Are Associated With Pruritus in Pediatric Autoimmune Sclerosing Cholangitis. Front. Pediatr. 10:903360. doi: 10.3389/fped.2022.903360
Received: 24 March 2022; Accepted: 25 April 2022;
Published: 11 May 2022.
Edited by:
Anshu Srivastava, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaReviewed by:
Patryk Lipiński, Children’s Memorial Health Institute (IPCZD), PolandSayee Anakk, University of Illinois at Urbana-Champaign, United States
Copyright © 2022 Meinel, Szabo, Dezsofi, Pohl, Strini, Greimel, Aguiriano-Moser, Haidl, Wagner, Schlagenhauf and Jahnel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Axel Schlagenhauf, YXhlbC5zY2hsYWdlbmhhdWZAbWVkdW5pZ3Jhei5hdA==