 Elise Riquin1,2,3*Ramona Sandnes4Fabien Bacro4Aubeline Vinay5Raphaële Miljkovitch6Valérie Rouger7Josué Rakotonjanahary8Géraldine Gascoin7,9Jean-Baptiste Müller7,10,11
Elise Riquin1,2,3*Ramona Sandnes4Fabien Bacro4Aubeline Vinay5Raphaële Miljkovitch6Valérie Rouger7Josué Rakotonjanahary8Géraldine Gascoin7,9Jean-Baptiste Müller7,10,11- 1Department of Child and Adolescent Psychiatry, University Hospital of Angers, Angers, France
- 2CHU Angers, University of Angers, Angers, France
- 3Fondation de Santé des Étudiants de France, Clinique de Sablé sur Sarthe, Sablé sur Sarthe, France
- 4Faculty of Psychology, Centre de Recherche en Education de Nantes (CREN – EA 2661), University of Nantes, Nantes, France
- 5Départements d’Enseignement LLSH - DEP ENS LLSH Psychologie, UFR Lettres Langues et Sciences Humaines – LLSH, Angers, France
- 6Laboratoire Paragraphe, Université Paris 8, Saint Denis, France
- 7Loire Infant Follow-Up Team (LIFT) Network, Pays de Loire, France
- 8Department of Pediatric Oncology, University Hospital, Angers, France
- 9Department of Neonatal Medicine, Toulouse University Hospital, Toulouse, France
- 10Department of Neonatal Medicine, Nantes University Hospital, Nantes, France
- 11National Institute of Health and Medical Research CIC004, Nantes University Hospital, Nantes, France
Context and purpose: Prematurity is a situation that can disrupt parent-child interactions. We hypothesize that establishing relationships with parents in a context of extreme prematurity can alter the development of secure attachment representations in the child. Furthermore, we hypothesize that secure maternal representations and their possible interactions with prematurity factors prevent the development of insecure or disorganized attachment in the child. In addition, maternal representations and their possible interactions with factors related to prematurity may prevent or accentuate the development of an insecure or disorganized attachment in the child.
Methods and analysis: This is a longitudinal, prospective, exploratory, and bi-centric study. Children born in the neonatal intensive care units of Angers or Nantes University Hospitals with a gestational age of up to 28 weeks will be included in the study. The main objective is to describe the attachment representations at 3 and 5 years through the Attachment Story Completion Task scales and to analyze them in regard to the children’s neurocognitive and behavioral outcomes as well as maternal attachment and mental health.
Ethics: The study file received a favorable opinion for the implementation of this research on February 18, 2020 - ID-RCB no. 2019-A03352-55 (File 2-20-007 id6699) 2°HPS. This study has received authorization from the French Data Protection Authority (CNIL) under no. 920229.
Discussion: A better understanding of attachment representations in extreme prematurity and their possible associations with children’s neurocognitive and behavioral outcomes as well as maternal attachment and mental health could pave the way for individualized care at an early stage, or even interventions during the neonatal period to improve the outcome of these vulnerable newborns.
Trial registration: [ClinicalTrials.gov], identifier [NCT04304846].
Introduction
The long-term consequences of prematurity include behavioral and cognitive impairments that may manifest at school age as learning disabilities (1, 2). Indeed, preterm births are also associated with a high risk of neurodevelopmental disabilities (3, 4).
Term or preterm newborns aim to come into contact with those around them and build close relationships with their caregivers (5). These attachment relationships are established gradually and, from the end of the first year, children exhibit individual attachment behavior patterns, depending on the quality of interactions and responses given to them by adults (6).
Prematurity can disrupt parent-child interactions (7, 8). The physiological characteristics of preterm infants attenuate and modify their signals of stress. Visual interactions are shorter, they struggle to stay focused, and their reactions are less visible than those of full-term infants (9). In this stressful and critical period, maternal sensitivity and availability may also be impaired (10). Parental stress, as well as post-traumatic stress disorders, can disrupt the emotional sense of parenthood (11, 12). Thus, in these situations, changes in the quality of mother-child interactions have been reported, with more controlling maternal behavior (13) and the development of behavioral impairments in children (13). It has also been shown that inadequate maternal caregiving is associated with relational withdrawal of the child, especially in the case of prematurity (14).
What is more, maternal attachment representations have been associated not only with children’s developmental outcomes (15–17) but also with children’s brain development (18), and there may be an intergenerational transmission of attachment (19).
In the context of prematurity, literature on the intergenerational transmission of attachment is scarce. To our knowledge, no study has explored this attachment pathway in the context of extreme prematurity with regards to maternal mental health and child neuro-development.
Firstly, we hypothesize that the experience of establishing a relationship with parents in a context of extreme prematurity can alter the development of secure attachment representations in the child. Secondly, we also hypothesize that the potential disorganization of children’s attachment representations is associated with clinical and environmental factors, as well as with maternal attachment representations, the emotional state of parents, and neuro-developmental complications (motor, cognitive, and behavioral) for the child.
Methods and Analysis
Aims:
The primary aim of this study is the description of attachment representations at 3 and 5 years of age, and their links with neurocognitive and behavioral outcomes in children born very prematurely.
The secondary aims are to test:
- The link between attachment representations at 3 and 5 years of age and perinatal and/or prenatal and socio-environmental factors in children born very prematurely.
- The link between maternal attachment representations and:
० children’s attachment representations at 3 and 5 years in children born very prematurely; and
० neurocognitive assessment at 3 and 5 years in children born very prematurely.
Design of the study and characteristics of the participants:
This is a longitudinal, prospective, exploratory, and bi-centric study. The inclusion criteria are: singleton infants born at less than 29 weeks of gestation in the neonatal intensive care unit (NICU) of Angers and Nantes University Hospitals included in the regional monitoring network for vulnerable newborns (Loire Infant Follow-up Team, LIFT Cohort) and with a clinical evaluation planned at 3 years of age in Angers or Nantes Hospital, with an informed consent dated and signed by the parents. The exclusion criteria are: being a child with severe neurocognitive impairment or a severe autism disorder in the 2-year LIFT follow-up evaluation.
Neonatal characteristics of the cohort are presented in Table 1.
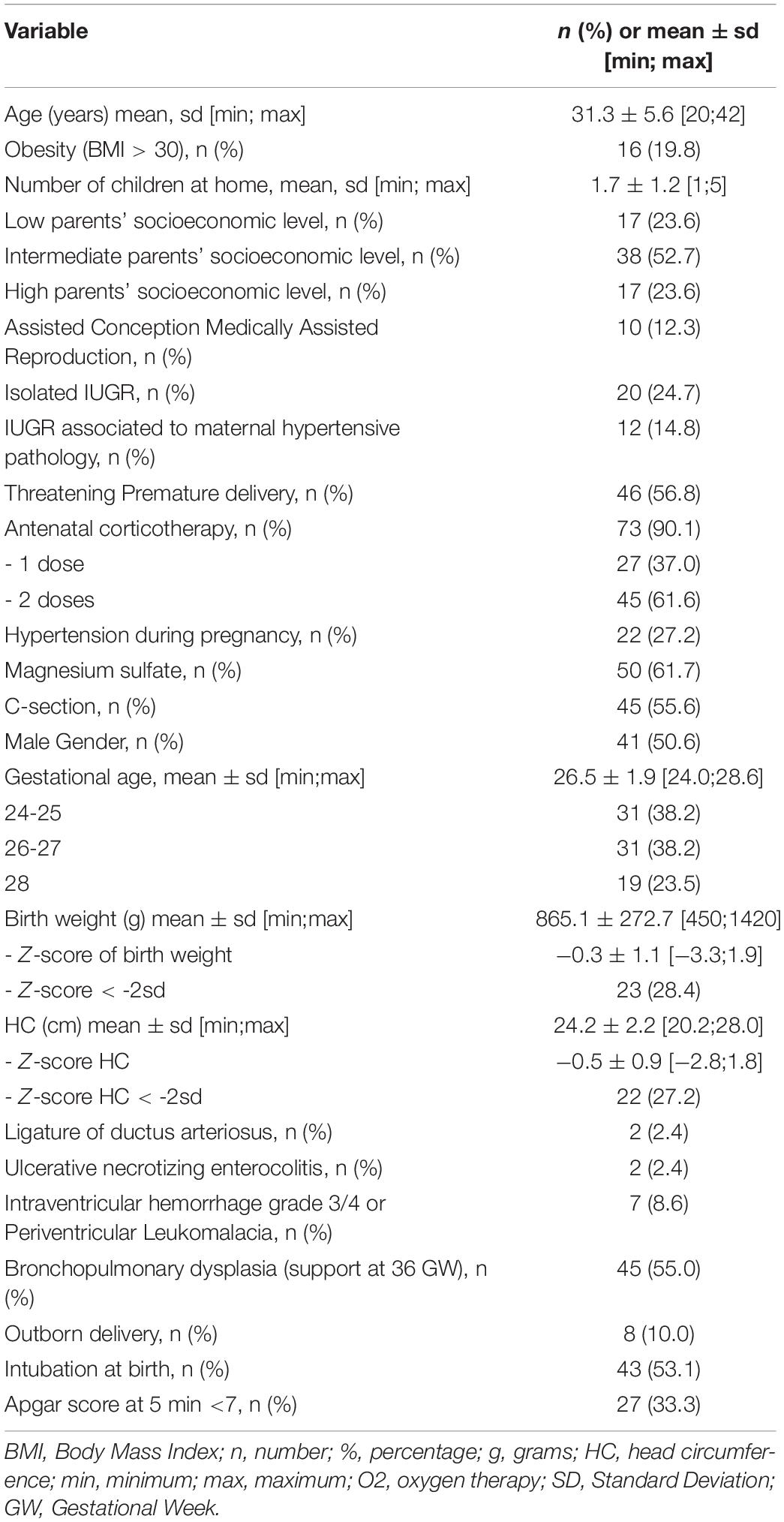
Table 1. Selected baseline characteristics of the preterm children included in the cohort.
Description of materials:
Data collected through the usual LIFT follow-up assessment:
- Parental and socioeconomic data:
Parental data comprised maternal age, number of children at home, parents’ socioeconomic level. The socioeconomic data consisted of the socioeconomic level and eligibility for social security benefits of those with low incomes. The socioeconomic level took into account the parent with the most highly-rated job according to a scale based on the official classification developed by the INSEE institute.
- Obstetrical data:
Obstetrical data comprised the context of Medically Assisted Reproduction, Intra-Uterine Growth Retardation (IUGR), threatening premature delivery, use of assisted conception, antenatal corticotherapy, C-section, the existence of maternal hypertensive disorders during pregnancy, and the use of antenatal corticotherapy or magnesium sulfate.
- Perinatal data:
Perinatal data comprised date of birth, gender, gestational age (GA), birth weight, and head circumference (HC). Birth weight and HC were expressed in Z-scores according to Olsen standards. Data on neonatal morbidity, such as criteria used in the context of the LIFT follow-up, including bronchopulmonary dysplasia at 36 WG, grade 3-4 intraventricular hemorrhage, periventricular leukomalacia, grade 2-3 necrotizing enterocolitis, and persistence of the arterial duct treated, were also collected.
Follow-up data: Questionnaires included in the LIFT cohort follow-up and specific data that will be collected for this study will be analyzed and are described in Table 2. TheAges and Stages Questionnaire (ASQ) (20, 21), the Strengths and Difficulties Questionnaire (SDQ) (22, 23), the Global School Adaptation (GSA) (24, 25), the Attachment Story Completion Task (ASCT) (26, 27), the Attachment Multiple Model Interview (AMMI) (28), the Parenting Stress Index (PSI) (29–31), and the Perinatal Posttraumatic Stress Disorder (PTSD) Questionnaire (PPQ) (29, 32) were used in the study.
The outcome measures are described in Table 3.
Course of the study:
The course of the study is presented in Figure 1.
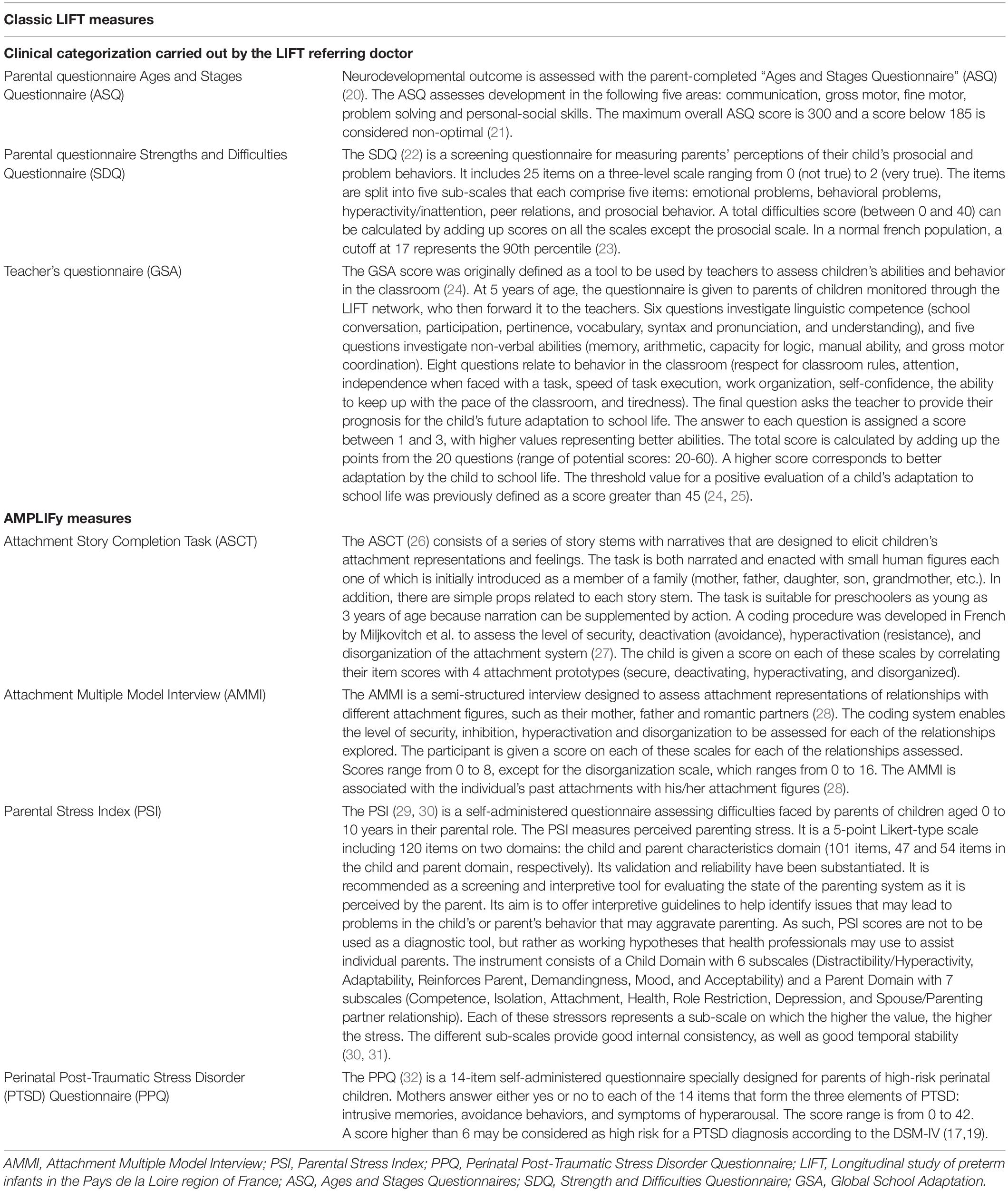
Table 2. Description of assessment tools.
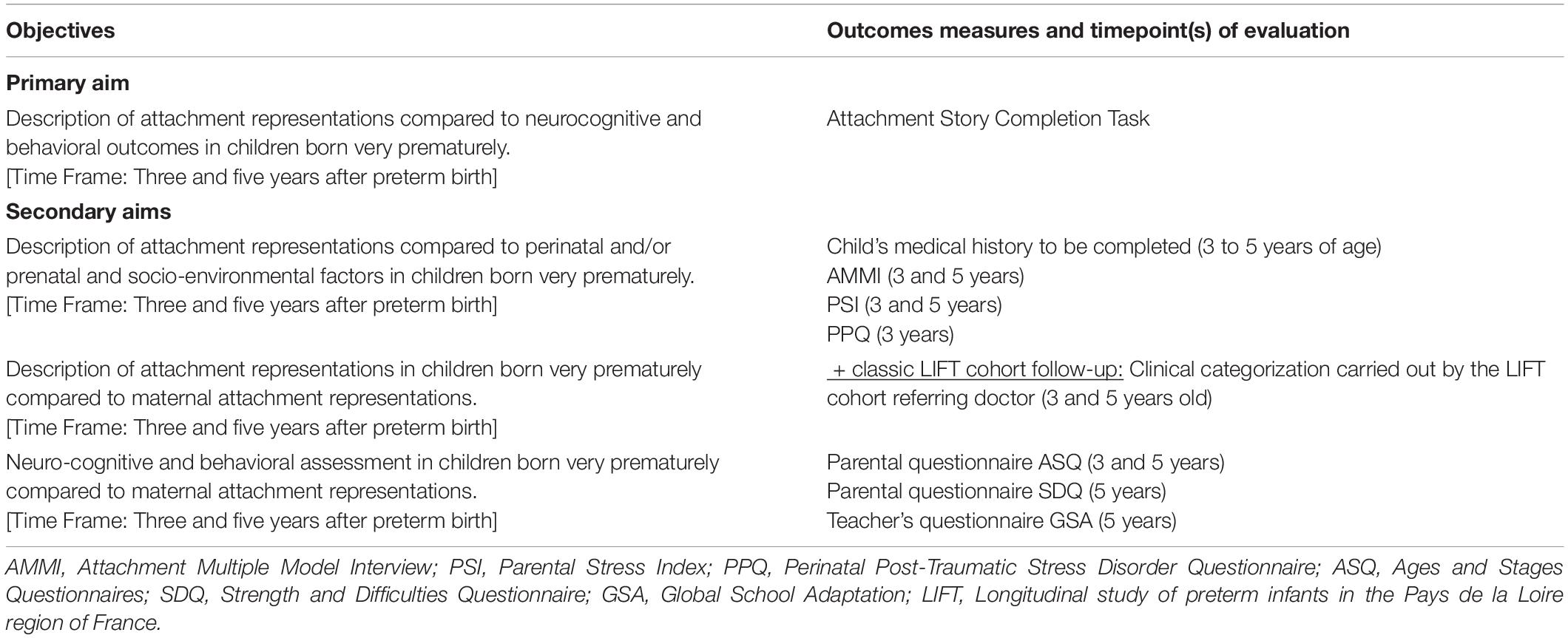
Table 3. Outcome measures.
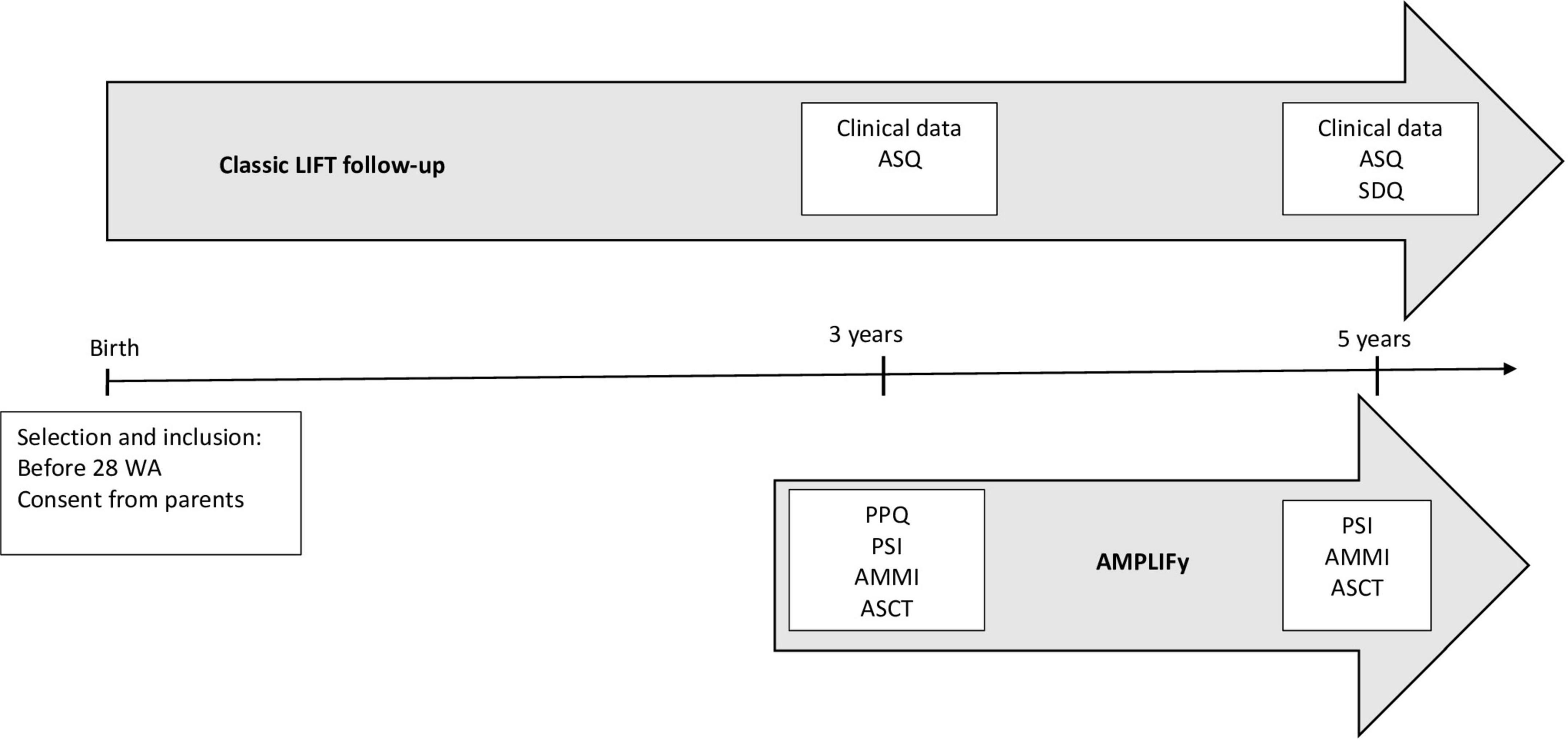
Figure 1. Study time schedule. AMMI: Attachment Multiple Model Interview; PSI: Parental Stress Index; PPQ: Perinatal Post-Traumatic Stress Disorder Questionnaire; LIFT: Longitudinal study of preterm infants in the Pays de la Loire region of France; ASQ: Ages and Stages Questionnaires; SDQ: Strength and Difficulties Questionnaire; GSA: Global School Adaptation; WA: Weeks of Amenorrhea; AMPLIFy: AttachMent Preterm LIFy.
Eligible patients will be identified in the LIFT cohort. The information letter will be sent to parents by post before the follow-up visit at 3 years old. A study investigator then completes the inclusion process by phone (collects additional information, answers questions from the parents, and obtains their express consent). The questionnaires (PSI and PPQ) will be sent by post one month before the appointment scheduled for the visit at 3 years of age.
Visit at 3 years of age:
The standard LIFT cohort follow-up will be performed. As part of the follow-up, prior to the appointment parents will receive the ASQ questionnaire that they will complete before the appointment and return to the LIFT cohort administration department in an enclosed prepaid envelope (one month before), specifying the date on which the questionnaire was completed.
Patients will be asked to provide consent relating to image rights before the interviews are carried out. Data from the follow-up at 3 years, as planned under the LIFT cohort, will be extracted and included in the AMPLIFy study case report forms.
Additional investigations will be carried out as part of this study: collection of the completed PSI and PPQ questionnaires, the AMMI, a 30-min interview (recorded) to assess the mother’s attachment representations to her own mother, father, and spouse and the ASCT, a story-completion task with the child (filmed) in the presence of a second accompanying adult, during which the child is asked to complete five story beginnings.
Visit at 5 years:
The standard LIFT cohort follow-up will be performed. As part of this follow-up, before the parent’s appointment the ASQ, the SDQ, and GSA will be filled out by parents. Questionnaire results will be available for the consultation at 5 years.
Data from the follow-up at 5 years, planned as part of the LIFT cohort, will be extracted and included in the AMPLIFy study case report forms.
Additional investigations will be carried out as part of this study: collection of the PSI and PPQ questionnaires (if not completed during the visit at 3 years), the AMMI, a 30-min interview (recorded) with the child’s mother to assess the mother’s attachment representations to her own mother, father, and spouse and the child’s attachment representations with the ASCT.
The inclusion and participation periods will each last 2 years and the study (inclusion + participation periods) will last 4 years in total.
Sample size calculation:
As this is a pilot study exploring the attachment representations in children born very prematurely, the size of the sample to be analyzed was determined using the data in the LIFT cohort database. Data from centers participating in the study were used to determine the number of participants who were eligible for inclusion at these centers and to estimate the total number of participants eligible for the entire study. Figure 2 shows the details regarding the number of eligible patients.
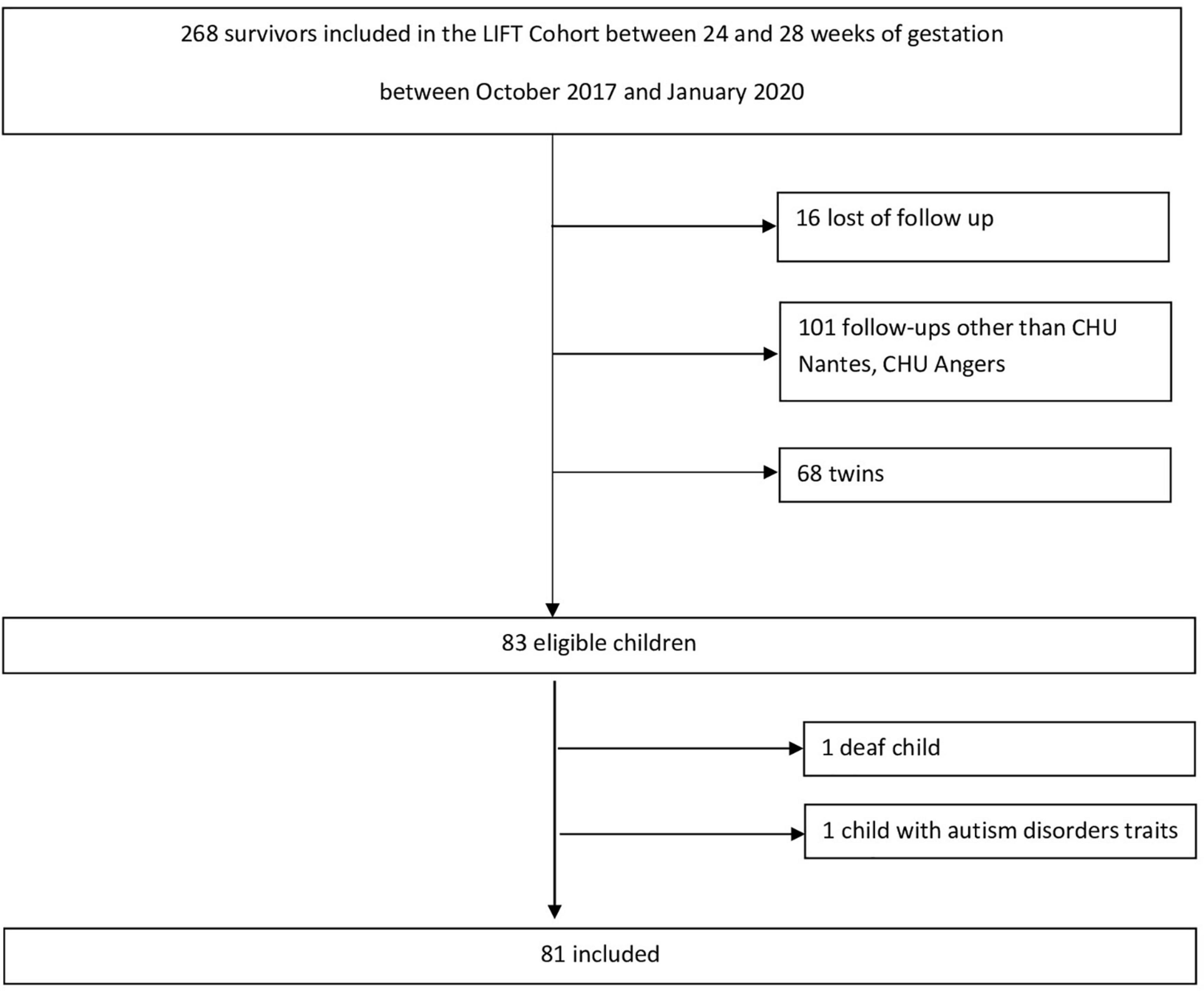
Figure 2. Study flow chart.
A total of 83 children are considered as eligible for inclusion in the two centers and will be screened for study recruitment. Participation will be offered to the parents (or the legal guardians). Assuming the occurrence of a non-participation rate in the study (due to refusal or for another reason) and an incomplete data rate for an estimated total of 25% of the eligible sample, the number of children with complete analyzable data is estimated at 63 in total. This aligns with the desired sample sizes recommended for pilot studies reported in the literature (33, 34). Participation will be offered to the parents (or the legal guardians) of 83 children considered eligible for inclusion. Consistent with the exploratory nature of this pilot study, we did not perform a statistical power analysis. Power calculations are beyond the scope of a pilot study (35). We will use a confidence interval approach to interpret the results (36). After taking into account exclusion criteria, a total number of 81 children will be included in the study.
Statistical analysis design: A flow chart will be used to depict the screening and inclusion of children included in the analysis. A descriptive analysis of the characteristics of the children included in the study will be carried out.
Descriptive analyses will be presented for all of the data collected about the children included in the study, as well as the data relating to the parents. The qualitative variables will be studied in terms of frequency and percentage. Quantitative variables will be analyzed in terms of absolute scores, medians, interquartile ranges (or extreme values), averages, standard deviations, and/or 95% average confidence intervals.
For each Q-sort score derived from the ASCT (secure, deactivating, hyperactivating, and disorganized), the average of each score recorded at 3 years and again at 5 years will be used to describe children’s attachment representations within the population of children born extremely prematurely (27).
The analysis will take place on an exploratory basis by studying the factors associated with the children’s attachment representations at 3 and 5 years old. The factors associated with each Q-score will be studied using a univariate linear regression model. A separate model will be performed for each Q-score. Multivariate analyses will be also carried out on an exploratory basis (one multivariate model for each Q-score). The following different factors will be considered (37), including specifically: neurocognitive development (using the score from the GSA questionnaire as an absolute value and the score from the ASQ questionnaire expressed as a score <285 or not); behavioral development (SDQ score between 17 and 40 or not); perinatal, prenatal, and socioenvironmental factors (term of pregnancy, birth weight and length as a z-score, sex, age of the mother, gravidity, parity); comorbidity at birth (composite criterion used in the context of the LIFT follow-up: bronchopulmonary dysplasia at 36 WG, grade 3-4 intraventricular hemorrhage, periventricular leukomalacia, grade 2-3 necrotizing enterocolitis, ligature of ductus arteriosus); the socioeconomic status and level of education of the parents; the use of medically assisted reproduction; the parents’ marital status (separated or not). The following factors will also be taken into account: parental posttraumatic stress, using the score from the PPQ questionnaire (score greater than or equal to 6), and parental stress using the PSI score as an absolute value, as well as the results of the assessment for maternal attachment representations using the scores from the AMMI dimensions as absolute values. An additional analysis using mixed models will also be performed for exploratory purposes (linear models) to analyze the longitudinal aspects of the follow-up of the children included in the study. As described previously, a separate model will be performed for each Q-score.
All tests will be performed with a two-sided level of significance of 0.05.
Discussion
The study will provide a better understanding of the attachment representations developed by extremely premature infants and the possible association between these attachment representations and maternal mental health, stress, and neurocognitive development. More knowledge and a better understanding could allow for individualized care at an early stage or even interventions from the neonatal period to improve the outcome of these vulnerable newborns.
The study also offers real advantages for the children and families included. An advisory consultation with the LIFT cohort’s usual partners (psychologist, child psychiatrist, etc.) will be offered if mental or interpersonal difficulties come to light during tests performed as part of the study.
The study is registered with ClinicalTrials.gov, identifier: NCT04304846 (retrospectively registered January 11, 2021). URL: https://clinicaltrials.gov/ct2/show/record/NCT04304846.
Ethics and Dissemination
This study involving human participants qualifies as an interventional study with minimal risks and constraints in accordance with the decree of April 12, 2018 establishing the list of types of study mentioned in part 2 of Article L.1121-1 of the French Public Health Code, as an adapted care package may be offered following the results of the investigations carried out as part of the study.
The study file received a favorable opinion for the implementation of this research on February 18, 2020 - ID-RCB n°: 2019-A03352-55 (Dossier 2-20-007 id6699) 2°HPS. This study has received authorization from the French Data Protection Authority (CNIL) as per n° 920229.
The LIFT cohort received ethical approval from the Commission Nationale de l’Information et des Libertés (No. 851117) (37).
Ethics Statement
The studies involving human participants were reviewed and approved by ID-RCB no. 2019-A03352-55 (File 2-20-007 id6699) 2°HPS. This study has received authorization from the French Data Protection Authority (CNIL) under no. 920229. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author Contributions
ER, RS, FB, AV, RM, VR, JR, J-BM, and GG performed the design of the study. ER, VR, JR, J-BM, and GG contributed to the data analysis. All authors have read and approved the article, revised and wrote the manuscript.
Funding
The EnJeu[x] consortium, funded by the region “Pays de la Loire,” contributed to the realization of the Project and the University of Angers, in the name and on behalf of the EnJeu[x] consortium, provided financial support (n°30027892). The study protocol also received financial support from the University Hospital of Angers as part of the 2019 internal call for tenders, following external peer review. These funds permitted the study coordinator to buy the PSI test, four mini-cameras with microSD cards for recording children’s exams (2 cameras in Angers and 2 in Nantes), and toy figurines for exams (family, a bedroom, a dining room, a car, and pets). Time for a clinical research associate for both the inclusion of patients in the study and data collection was also financed by the funds.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank the University of Angers and the EnJeu[x] program for their financial support.
References
1. Delobel-Ayoub M, Arnaud C, White-Koning M, Casper C, Pierrat V, Garel M, et al. Behavioral problems and cognitive performance at 5 years of age after very preterm birth: the EPIPAGE study. Pediatrics. (2009). 123:1485–92. doi: 10.1542/peds.2008-1216
2. Roberts G, Lim J, Doyle LW, Anderson PJ. High rates of school readiness difficulties at 5 years of age in very preterm infants compared with term controls. J Dev Behav Pediatr. (2011) 32:117–24. doi: 10.1097/DBP.0b013e318206d5c9
3. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJS. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA. (2002) 288:728–37. doi: 10.1001/jama.288.6.728
4. Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. (2008) 371:261–69. doi: 10.1016/S0140-6736(08)60136-1
6. Ainsworth MDS, Bell SM, Stayton DJ Individual differences in strange-situation behavior of one-year-olds. In: HR Schaffer editor. The Origins of Human Social Relations. London: Academic Press (1971). p. 17–58.
7. Cambonie G, Muller JB, Ehlinger V, Roy J, Guédeney A, Lebeaux C, et al. Mother-infant interaction assessment at discharge and at 6 months in a French cohort of infants born very preterm: the OLIMPE study. PLoS One. (2017) 12:e0188942. doi: 10.1371/journal.pone.0188942
8. Gatta M, Miscioscia M, Svanellini L, Brianda MH, Guerra G, Battistella PA, et al. Triadic interactions in families with preterm children: a comparative study with children born at term. Neuropsychiatr Dis Treat. (2017) 13:2375–88. doi: 10.2147/NDT.S129225
9. Als H, Butler S, Kosta S, McAnulty G. The assessment of preterm infants’ behavior (APIB): furthering the understanding and measurement of neurodevelopmental competence in preterm and full-term infants. Ment Retard Dev Disabil Res Rev. (2005) 11:94–102. doi: 10.1002/mrdd.20053
10. Muller-Nix C, Forcada-Guex M, Pierrehumbert B, Jaunin L, Borghini A, Ansermet F. Prematurity, maternal stress and mother-child interactions. Early Hum Dev. (2004) 79:145–58. doi: 10.1016/j.earlhumdev.2004.05.002
11. Davis L, Edwards H, Mohay H, Wollin J. The impact of very premature birth on the psychological health of mothers. Early Hum Dev. (2003) 73:61–70. doi: 10.1016/S0378-3782(03)00073-2
12. Muller-Nix C, Forcada-Guex M, Borghini A, Pierrehumbert B, Ansermet F. Prématurité, vécu parental et relations parents/enfant? Psychiatr Enfant. (2009) 52:423–50. doi: 10.3917/psye.522.0423
13. Forcada-Guex M, Borghini A, Pierrehumbert B, Ansermet F, Muller-Nix C. Prematurity, maternal posttraumatic stress and consequences on the mother-infant relationship. Early Hum Dev. (2011) 87:21–6. doi: 10.1016/j.earlhumdev.2010.09.006
14. Guedeney A, Marchand-Martin L, Cote SJ, Larroque B EDEN Mother-Child Cohort Study Group. Perinatal risk factors and social withdrawal behaviour. Eur Child Adolesc Psychiatry. (2012) 21:185–91. doi: 10.1007/s00787-012-0250-4
15. Steele RD, Waters TEA, Bost KK, Vaughn BE, Truitt W, Waters HS, et al. Caregiving antecedents of secure base script knowledge: a comparative analysis of young adult attachment representations. Dev Psychol. (2014) 50:2526–38. doi: 10.1037/a0037992
16. Jones JD, Cassidy J, Shaver PR. Parents’ self-reported attachment styles: a review of links with parenting behaviors, emotions, and cognitions. Pers Soc Psychol Rev. (2015) 19:44–76. doi: 10.1177/1088868314541858
17. Coppola G, Vaughn BE, Cassibba R, Costantini A. The attachment script representation procedure in an italian sample: associations with adult attachment interview scales and with maternal sensitivity. Attach Hum Dev. (2006) 8:209–19. doi: 10.1080/14616730600856065
18. Fitter MH, Stern JA, Straske MD, Allard T, Cassidy J, Riggins T. Mothers’ attachment representations and children’s brain structure. Front Hum Neurosci. (2022) 16:740195. doi: 10.3389/fnhum.2022.740195
19. Verhage ML, Schuengel C, Madigan S, Fearon RMP, Oosterman M, Cassibba R, et al. Narrowing the transmission gap: a synthesis of three decades of research on intergenerational transmission of attachment. Psychol Bull. (2016) 142:337–66. doi: 10.1037/bul0000038
20. Squires J, Bricker D, Potter L. Revision of a parent-completed development screening tool: ages and stages questionnaires. J Pediatr Psychol. (1997) 22:313–28. doi: 10.1093/jpepsy/22.3.313
21. Flamant C, Branger B, Nguyen The Tich S, de la Rochebrochard E, Savagner C, Berlie I, et al. Parent-completed developmental screening in premature children: a valid tool for follow-up programs. PLoS One. (2011) 6:e20004. doi: 10.1371/journal.pone.0020004
22. Goodman R, Ford T, Simmons H, Gatward R, Meltzer H Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. Int Rev Psychiatry. (2003) 15, 166–72. doi: 10.1080/0954026021000046128
23. Shojaei T, Wazana A, Pitrou I, Kovess V. The strengths and difficulties questionnaire: validation study in French school-aged children and cross-cultural comparisons. Soc Psychiatry Psychiatr Epidemiol. (2009) 44:740–7. doi: 10.1007/s00127-008-0489-8
24. Guimard P, Cosnefroy O, Florin A. Évaluation des comportements et des compétences scolaires par les enseignants et prédiction des performances et des parcours à l’école élémentaire et au collège. Lorientat Sc Prof. (2007) 36:179–202. doi: 10.4000/osp.1372
25. Boussicault G, Nguyen The Tich S, Branger B, Guimard P, Florin A, Rozé JC, et al. The Global school adaptation score: a new neurodevelopmental assessment tool for very preterm children at five years of age. J Pediatr. (2013) 163:460–64. doi: 10.1016/j.jpeds.2013.01.052
26. Bretherton I, Ridgeway D, Cassidy J. Assessing internal working models of the attachment relationship: an attachment story completion task for 3-year-olds. In: D John, T Catherine editors. Attachment in the Preschool Years: Theory, Research, and Intervention. Chicago, IL: University of Chicago Press (1990). p. 273–308.
27. Miljkovitch R, Pierrehumbert B, Karmaniola A, Halfon O. Les représentations d’attachement du jeune enfant. Développement d’un système de codage pour les histoires à compléter. Devenir. (2003) 15:143–77.
28. Miljkovitch R, Moss E, Bernier A, Pascuzzo K, Sander E. Refining the assessment of internal working models: the attachment multiple model interview. Attach Hum Dev. (2015) 17:492–521. doi: 10.1080/14616734.2015.1075561
29. Abidin RR. Parenting Stress Index: Manual, Administration Booklet, [and] Research Update. Charlottesville, VA: Pediatric Psychology Press (1983).
30. Bigras M, LaFreniere PJ, Abidin RR. Indice de Stress Parental: Manuel Francophone en Complément à L’édition Américaine. North Tonawanda, NY: Multi-Health systems (1996).
31. Lacharité C, Éthier LS, Couture G. Sensitivity and specificity of the parenting stress index in situations of child maltreatment. Can J Behav Sci. (1999) 31:217–20. doi: 10.1037/h0087090
32. DeMier RL, Hynan MT, Harris HB, Manniello RL. Perinatal stressors as predictors of symptoms of posttraumatic stress in mothers of infants at high risk. J Perinatol. (1996) 16:276–80.
33. Teare MD, Dimairo M, Shephard N, Hayman A, Whitehead A, Walters SJ. Sample size requirements to estimate key design parameters from external pilot randomised controlled trials: a simulation study. Trials. (2014) 15:264. doi: 10.1186/1745-6215-15-264
34. Billingham SAM, Whitehead AL, Julious SA. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom clinical research network database. BMC Med Res Methodol. (2013) 13:104. doi: 10.1186/1471-2288-13-104
35. Kistin C, Silverstein M. Pilot studies: a critical but potentially misused component of interventional research. JAMA. (2015) 314:1561–62. doi: 10.1001/jama.2015.10962
36. Bland JM. The tyranny of power: is there a better way to calculate sample size? BMJ. (2009) 339:b3985. doi: 10.1136/bmj.b3985
Keywords: prematurity, development, attachment, child, infant
Citation: Riquin E, Sandnes R, Bacro F, Vinay A, Miljkovitch R, Rouger V, Rakotonjanahary J, Gascoin G and Müller J-B (2022) A Prospective Observational Study to Assess Attachment Representations With Regard to Neurocognitive and Behavioral Outcomes in Children Born Very Prematurely in the Loire Infant Follow-Up Team (LIFT Cohort). Front. Pediatr. 10:896103. doi: 10.3389/fped.2022.896103
Received: 14 March 2022; Accepted: 16 June 2022;
Published: 13 July 2022.
Edited by:
Andrea Guzzetta, University of Pisa, ItalyReviewed by:
Lynne Murray, University of Reading, United KingdomAnn-Margret Rydell, Uppsala University, Sweden
Copyright © 2022 Riquin, Sandnes, Bacro, Vinay, Miljkovitch, Rouger, Rakotonjanahary, Gascoin and Müller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elise Riquin, Elise.Riquin@chu-angers.fr orcid.org/0000-0002-5956-3014