
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pediatr., 30 August 2022
Sec. Pediatric Critical Care
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.895541
This article is part of the Research TopicWomen in Pediatric Critical Care: 2021View all 19 articles
 Roberta Esteves Vieira de Castro1,2,3*
Roberta Esteves Vieira de Castro1,2,3* Miguel Rodríguez-Rubio4,5
Miguel Rodríguez-Rubio4,5 Maria Clara de Magalhães-Barbosa2
Maria Clara de Magalhães-Barbosa2 Arnaldo Prata-Barbosa2Jaimee Holbrook6
Arnaldo Prata-Barbosa2Jaimee Holbrook6 Pradip Kamat7Anne Stormorken8
Pradip Kamat7Anne Stormorken8Importance: Targeted analgosedation is a challenge in critically ill children, and this challenge becomes even more significant with drug shortages.
Observations: Published guidelines inform the provision of analgosedation in critically ill children. This review provides insights into general approaches using these guidelines during drug shortages in Pediatric Intensive Care Units as well as strategies to optimize both pharmacological and non-pharmacological approaches in these situations.
Conclusions and relevance: Considering that drug shortages are a recurrent worldwide problem, this review may guide managing these drugs in critically ill children in situations of scarcity, such as in pandemics or disasters.
In 1955, the pioneer dedicated Pediatric Intensive Care Unit (PICU) was established in Europe, and pediatric critical care medicine has only been accepted as a distinct specialty since 1981 (1). Many pediatric critically ill patients in these units require life-saving measures, including mechanical ventilation (MV), continuous renal replacement therapy, and extracorporeal membrane oxygenation therapy. These interventions are associated with a protracted PICU stay and the need for analgosedation (2).
Unfortunately, several essential analgesic and sedative agents have been depleted globally primarily due to increased needs and the disruption of manufacturing and supply chains (3). In 2016, the World Health Organization proactively took a stand about the lack of essential medicines, reported in low, middle, and high-income countries. The scarcity of drugs poses risks to the patient's health due to non-treatment, undertreatment, and failure to find suitable alternatives (4).
This review aims to: (1) provide the reader with information regarding drug supply chain issues; (2) highlight the levels of service for dispensing medicines: conventional, contingency and crisis, emphasizing the role of pharmacists in the rationing of them; (3) address the relevance of appropriate management of analgesia and sedation in the PICU; and (4) present dose optimization strategies regarding analgo-sedative choices in addition to considering different approaches to preventing medication overuse.
Numerous definitions for drug shortages have been widely used, as shown in Table 1. Unfortunately, there is a lack of a standardized definition. Moreover, the low and middle-income countries have the absence of an official description (5).
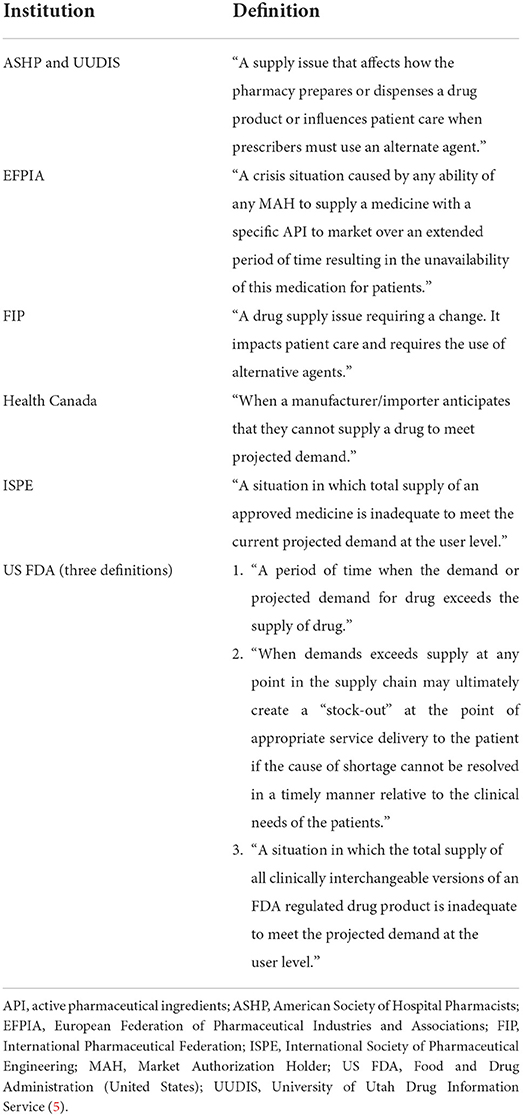
Table 1. Definitions of drug shortages according to different institutions.
Drug shortages are recognized as a global issue (4) and are usually due to several factors. Drug shortage affects high, middle, and low-income countries. In high-income countries, it has more attention when compared to other regions of the globe. The supply chain for delivering raw materials to patient use is complex and involves multiple entities, including manufacturers, group purchasing associations, wholesalers, and healthcare systems. On the manufacturing side, drug shortages occur due to lack of raw materials, regulatory problems, manufacturing interruptions, voluntary and involuntary recalls, promotion reduction (such as patent expiration or generic drug profitability), or manufacturer consolidations. Moreover, drug shortages also occur due to improper stocking practices, changes in clinical practice (resulting in increased demand), and even supply chain disruption due to natural disasters. Otherwise, low-middle income countries have some novel reasons for drug shortage, comprising licensing of manufacturers/products, shortage of raw material for a local producer, drug smuggling, and lodging tax government practices. These countries have insufficient research and lack policies to deal with this problem (5–7).
During a major disaster, such as a pandemic or war, for example, it is necessary to forecast and manage the shortage of drugs essential to critical care from global, national, regional, and institutional perspectives. Drug shortages can be expected to coincide with an interruption of other necessary resources such as personnel, availability of personal protective equipment, and medical devices. Supplies for drug preparation and administration can also be scarce (3).
Burry et al. summarized the main strategies that stakeholders must consider for future steps during a global disaster from the worldwide level to the institutional approach:
• Global: Proactively plan for shortages via substitution and conservation strategies; establish transnational networks with national and regional sharing arrangements; develop recommendations on essential supplies.
• National and Regional Manufacturing: create usage prediction models; couple with inventory management; engage manufacturers; improve pharmaceutical processes; eliminate redundant critical production steps; recommendations on essential supplies; collaborative dashboards; sharing arrangements; decentralize production to multiple sites. Supply disruption is exacerbated if there are limited manufacturing capacity, market concentration, or just-in-time inventory practices that result in minimal product inventory on hand at any given time. However, the Food and Drug Administration (FDA) cannot prevent manufacturing concentration, require redundancy of that capability, require a company to manufacture a drug, maintain a certain level of inventory of the drug, or reverse a business decision to stop manufacturing. Manufacturers may consider opportunities to increase redundant manufacturing capacity, maintain idle capacity, or increase inventory levels to reduce shortage risks, and other stakeholders can explore how to encourage such practices.
• Institutional: Balance drug inventory; identify drugs at risk of shortage; develop drug conservation guidelines; rotate stock; identify therapeutic alternatives (3, 8).
Given this situation, the role of pharmacists in alleviating the current crisis and future challenges is a central one. Notably, among the pharmacist's actions is advocacy for implementing the Interagency Drug Shortage Task Force recommendations by participating in dedicated drug shortage task forces or rationing committees to guide management strategies and keeping informed regarding drug shortages (9).
Finally, Ammar et al. suggest that drug escalation capacity and response be measured based on three levels: conventional care, contingency care, and crisis care. Contingency care comprises all the practices that may be outside usual care notwithstanding they attempt to keep traditional care. On the other hand, crisis care approaches are outside of standard of care, however, provide the best feasible care when resources are severely limited (10).
Children have unique illnesses and are at a singular developmental stage that may need specific medications for which there may not be therapeutic alternatives. Additionally, the evidence supporting the use of substitutes may be limited in pediatric patients and may raise concerns for adverse events. Therefore, a comprehensive and multidisciplinary approach is necessary to ensure that drug shortages do not lead to unfavorable patient outcomes (11).
Alleviating pain and anxiety in critically ill children may be quite challenging. Patient admission and daily care processes within PICUs can be frightening and painful for pediatric patients and their families. Pain can result from the underlying disease or trauma and can be exacerbated by anxiety and emotional stress, two common elements of the PICU stay. The condition in which children find themselves in this environment, surrounded by strange people and machines, separated from their parents, in a hostile, noisy, and bright place most of the time, leading to the interruption of the circadian cycle, causes more anxiety and vulnerability to pain. Pain may also result from diagnostic and therapeutic interventions to which patients are submitted during the hospitalization period. In intensive care, children, and newborns (NB) are often subjected to numerous potentially uncomfortable or painful procedures, such as arterial and venous punctures, thoracic drainage, and endotracheal intubation. These therapeutic interventions place an enormous burden on these patients, affecting the successful performance of these procedures and the patient's recovery (12–16).
An effective analgesia approach facilitates invasive procedures or interaction with invasive equipment such as MV and enhances rehabilitation of the critically ill patient (12). Accurate assessment of pain and comfort using validated scales with targeted, measured goals is central to excellent clinical management (13).
Adequate analgesia and sedation minimize the stress response and improve clinical and psychological outcomes. When inadequate, negative outcomes include undertreated pain or persistent agitation leading to accidental removal of invasive devices. On the other hand, oversedation results in prolonged PICU and hospital stay, prolonged MV, and the development of tolerance, physical dependence, iatrogenic withdrawal syndrome (IWS), and delirium. Accurate assessment of pain, distress, IWS, and delirium in critically ill children can be challenging as these conditions often overlap. The use of validated assessment scales as outlined in the recent PANDEM guidelines facilitates assessment guiding proper care and mitigating their development (12, 17).
The 2018 Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (PADIS Guidelines) have recommended the approach to sedation as “analgesia first” (before sedation) or analgesia-based sedation, which implies that an analgesic (usually an opioid) is used before a sedative to achieve the desired sedative goal. Institutions should have protocols that include periodic evaluations of pain and sedation using validated tools and provide clear guidance on the choice and dose of the drug, ensuring that pain treatment is a priority over the administration of sedatives (18). Recently, Smith et al. developed Society of Critical Care Medicine (SCCM) clinical practice guidelines for critically ill pediatric patients, including pain, sedation/agitation, iatrogenic withdrawal, neuromuscular block, delirium, PICU environment, and early mobility. Key areas included the need for routine monitoring of pain, agitation, withdrawal, and delirium using validated tools in children; improved use of protocol sedation and analgesia, and recognition of the importance of non-pharmacological interventions to improve patient comfort and provision of comprehensive care (17).
The SCCM developed a multicomponent and evidence-based six-step strategy to liberate patients from the ICU. This approach, called “the ABCDEF bundle,” represents A: Assess, prevent, and manage pain; B: Both Spontaneous Awakening Trials (SATs) and Spontaneous Breathing Trials (SBTs); C: Choice of sedation; D: Delirium assessment, prevention, and management; E: Early mobility and exercise; and F: Family engagement and empowerment. The conceptualization of the proposed “ICU Liberation” achieved notable recognition in adult critical care research and has become prominent in PICU. In a recent survey of 161 PICUs in 18 countries, Ista et al. observed that, unfortunately, the A-F bundle items have been adopted with substantial variability internationally (19).
We should emphasize that providing analgosedation is not restricted to the PICU environment. Currently, with the exponential growth in the number of procedures in children and adolescents experience outside the operating room, there has been a greater need for awareness and guidance on procedural sedation by professionals who are not anesthesiologists, including emergency departments, wards, outpatient clinics, imaging centers, and dental offices (20, 21).
Regarding drug shortages, in the specific case of analgosedation, one of the recommended approaches to conserving intravenous analgesic supplies during contingency care is to implement protocols where clinicians would initially use intermittent analgesic boluses before patients transition to continuous infusion. In addition, enteral delivery of opioids and analgesics may help to conserve the supply of intravenous (IV) agents. However, this strategy should be limited to patients with adequate gastrointestinal motility and function. Other situations can also be considered. For example, ketamine has analgesic properties and may spare the use of IV opioids. Furthermore, it is not known to cause significant respiratory depression at moderate doses, and this is advantageous when trying to transition the child off MV (10).
With regard to benzodiazepines, they can also be administered in intermittent doses or as a continuous infusion to obtain mild sedation. However, they should only be considered as first-line sedatives in contingency care settings. When used, IV lorazepam, midazolam, or diazepam in scheduled doses or as needed, can help to conserve drug stocks in the scenario of ongoing shortages. This approach can limit overall sedative exposure while still providing appropriate light sedation, preserving the need for high doses and continuous infusions known to be associated with accumulation. However, if this is not sufficient for adequate sedation, continuous infusion of benzodiazepines can be started. Still intermittent doses may be reconsidered again when continuous infusion is no longer needed and transition from continuous infusion to a less aggressive dose is appropriate (10).
Analgo-sedative regimen selection should take into consideration patient-specific risk factors, targeted level of sedation, anticipated duration, analgesic needs, physician familiarity, and institutional formulary availability. The following strategies that ensure comfort and optimize dosing of analgesics and sedatives. Applying these strategies can be challenging for teams unfamiliar with these measures, particularly when human resources are scarce, and family presence is restricted.
It is highly relevant for the interdisciplinary team to actively participate and discuss the goals of analgesia and sedation when necessary. When determining a sedative and analgesic regimen for a critically ill patient, the first step is to choose the desired degree/depth of sedation.
Moreover, the “Pediatric Brain Roadmap” contributes like a script to disseminate delirium assessment results and crucial information to guide delirium management discussion during interdisciplinary rounds. Its components are pain assessment, target, and actual LOC, delirium assessment, and sedative/analgesic/antipsychotic medications previously received:
• Where is the patient going? → Sedation targets and therapy goals.
• Where is the patient now? → Actual level of consciousness (RASS)/Delirium assessment/Pain assessment.
• How did they get there? → Shock, hypoxia, fever, drug exposure (18, 22).
There are few current indications for continuous deep sedation. These include the treatment of intracranial hypertension, severe respiratory failure, refractory status epilepticus, and prevention of consciousness in patients treated with neuromuscular blocking agents (18, 22).
Non-pharmacological interventions can reduce the total requirement and associated side effects of sedation and analgesia medications and have been recommended by international sedation guidelines. In addition to addressing risk factors, these strategies include daily screening for delirium; environmental orientation; maintaining normal hydration; regulation of bladder and bowel function; early establishment of normal diet; correction of metabolic disorders; cardiorespiratory optimization; early identification of infection; effective treatment of pain; daily mobilization; avoidance of antipsychotic drugs, benzodiazepines, and anticholinergics; sleep promotion; light and noise reduction; early removal of invasive devices; avoidance of physical restraints; attention to the parameters and modes of ventilation; cluster care (18, 22–24).
Consider pain assessment and treatment with opioid-sparing measures using a multimodal analgesia strategy, including non-opioid analgesics such as acetaminophen, dipyrone (metamizole), nefopam, ketamine, lidocaine, neuropathic agents, and NSAIDs (18).
Once the depth of sedation is chosen, it is essential to focus on selecting specific sedatives and pain relievers. In recent years, numerous studies have shown that benzodiazepines are independently associated with the incidence of delirium. Therefore, benzodiazepines should not be used as first-line sedatives in critically ill children. In the last decade, the use of alpha agonists such as dexmedetomidine has increased in PICUs. It may shorten the duration of MV and reduce the need for opioids and the incidence of delirium. In addition, attention should be paid to the individual characteristics of each patient. Care should be taken concerning obese patients and those with organ dysfunction and arrhythmias (18, 24, 25).
Some authors suggest establishing a sedation rotation regime based on the hypothesis that replacing sedative and analgesic drugs targeting different receptors for shorter periods may decrease the incidence of tolerance and IWS (26).
This bundle promotes fast recovery and ICU liberation, with satisfactory evidence in adults and children.
• [A] Assessment and management of pain.
• [B] Both awakening and breathing trials.
• [C] Choosing the optimal sedative (avoiding benzodiazepines when possible) and titrating to the lightest sedation level possible.
• [D] Delirium assessment and management.
• [E] Early mobility and exercise.
• [F] Family engagement and empowerment when possible (27–31).
The inclusion of the letter R (respiratory-drive-control“ “ABCDEF”R”) was suggested by Chanques et al. and should be considered to prioritize the management of factors related to the MV and the respiratory unit, avoiding the unnecessary use of medications that can delay ventilator release and worsen other patient outcomes (32).
In Table 2, we summarize the pharmacological options for providing analgesia and sedation in conditions of scarcity.

Table 2. Alternatives for pediatric analgesics and sedatives according to the desired sedation level.
Care of critically ill children during conditions of scarcity of analgesic and/or sedative drugs has presented numerous challenges globally. Effective approaches to managing drug shortages, implementing evidence-based guidelines for evaluating pain and delirium, and understanding alternative pharmacological and non-pharmacological options for analgesia and sedation will ensure safe and effective management of pain and delirium in the setting of limited resources or future disasters.
RC conceptualized and wrote the first draft of the review. MR-R, MM-B, AP-B, and JH made substantial contributions to the conception, design, literature data, and content of the tables. PK and AS drafted the article and revised it critically for important intellectual content. All authors approved the final version to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Woodruff AG, Choong K. Long-term outcomes and the post-intensive care syndrome in critically ill children: a north American perspective. Children. (2021) 8:254. doi: 10.3390/children8040254
2. Epstein D, Brill JE. A history of pediatric critical care medicine. Pediatr Res. (2005) 58:987–96. doi: 10.1203/01.PDR.0000182822.16263.3D
3. Burry LD, Barletta JF, Williamson D, Kanji S, Maves RC, Dichter J, et al. It takes a village: contending with drug shortages during disasters. Chest. (2020) 158:2414–24. doi: 10.1016/j.chest.2020.08.015
4. World Health Organization. Medicines shortages: global approaches to addressing shortages of essential medicines in health systems. WHO Drug Inform. (2016) 30:180–5.
5. Shukar S, Zahoor F, Hayat K, Saeed A, Gillani AH, Omer S, et al. Drug shortage: causes, impact, and mitigation strategies. Front Pharmacol. (2021) 12:693426. doi: 10.3389/fphar.2021.693426
6. Turbucz B, Major M, Zelko R, Hanko B. Proposal for handling of medicine shortages based on a comparison of retrospective risk analysis. Int J Environ Res Public Health. (2022) 19:4102. doi: 10.3390/ijerph19074102
7. Moffett BS, Mossad EB. Drug shortages: implications on pediatric anesthesia practice and management resources. J Clin Anesth. (2012) 24:677–9. doi: 10.1016/j.jclinane.2012.04.015
8. US Food Drug Administration. Strategic Plan for Preventing and Mitigating Drug Shortages. Available online at: https://psnet.ahrq.gov/issue/strategic-plan-preventing-and-mitigating-drug-shortages (accessed February 10, 2022).
9. Shuman AG, Fox ER, Unguru Y. COVID-19 and drug shortages: a call to action. J Manag Care Spec Pharm. (2020) 26:945–7. doi: 10.18553/jmcp.2020.26.8.945
10. Ammar MA, Sacha GL, Welch SC, Bass SN, Kane-Gill SL, Duggal A, et al. Sedation, analgesia, and paralysis in COVID-19 patients in the setting of drug shortages. J Intensive Care Med. (2021) 36:157–74. doi: 10.1177/0885066620951426
11. Moss JD, Schwenk HT, Chen M, Gaskari S. Drug shortage and critical medication inventory management at a children's hospital during the COVID-19 pandemic. J Pediatr Pharmacol Ther. (2021) 26:21–5. doi: 10.5863/1551-6776-26.1.21
12. Harris J, Ramelet AS, van Dijk M, Pokorna P, Wielenga J, Tume L, et al. Clinical recommendations for pain, sedation, withdrawal and delirium assessment in critically ill infants and children: an ESPNIC position statement for healthcare professionals. Intensive Care Med. (2016) 42:972–86. doi: 10.1007/s00134-016-4344-1
13. Kudchadkar SR, Easley RB, Brady KM, Yaster M. Pain and sedation management. In: Nichols DG, Shaffner DH, editors. Rogers' Textbook of Pediatric Intensive Care. 5. Ed. Philadelphia: Wolters Kluwer Health. (2016). p. 132–64.
14. Lerwick JL. Minimizing pediatric healthcare-induced anxiety and trauma. World J Clin Pediatr. (2016) 5:143–50. doi: 10.5409/wjcp.v5.i2.143
15. Sedrez EDS, Monteiro JK. Pain assessment in pediatrics. Rev Bras Enferm. (2020) 73(Suppl. 4):e20190109. doi: 10.1590/0034-7167-2019-0109
16. Baarslag MA, Jhingoer S, Ista E, Allegaert K, Tibboel D, van Dijk M. How often do we perform painful and stressful procedures in the paediatric intensive care unit? A prospective observational study. Aust Crit Care. (2019) 2:4–10. doi: 10.1016/j.aucc.2018.04.003
17. Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A, et al. 2022 society of critical care medicine clinical practice guidelines on prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the icu environment and early mobility. Pediatr Crit Care Med. (2022) 23:e74–110. doi: 10.1097/PCC.0000000000002873
18. Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. (2018) 46:e825–73. doi: 10.1097/CCM.0000000000003299
19. Ista E, Redivo J, Kananur P, Choong K, Colleti Jr J, Needham DM, et al. ABCDEF bundle practices for critically ill children: an international survey of 161 PICUs in 18 countries. Crit Care Med. (2022) 50:114–25. doi: 10.1097/CCM.0000000000005168
20. Kamat PP, McCracken CE, Simon HK, Stormorken A, Mallory M, Chumpitazi CE, et al. Trends in outpatient procedural sedation: 2007-2018. Pediatrics. (2020) 145:e20193559. doi: 10.1542/peds.2019-3559
21. Tiedt KA, Boriosi JP, Hollman GA. Introduction to procedural sedation within and outside the ICU. In: Kamat PP, Berkenbosch JW, editors. Sedation and Analgesia for the Pediatric Intensivist. Cham: Springer (2021). p. 337–356.
22. Society of Critical Care Medicine. ICU Liberation Bundle (A-F). (2022). Available online at: https://www.sccm.org/Clinical-Resources/ICULiberation-Home/ABCDEF-Bundles (accessed January 28, 2022).
23. Garcia Guerra G, Joffe AR, Sheppard C, Hewson K, Dinu IA, Hajihosseini M, et al. Music use for sedation in critically ill children (MUSiCC trial): a pilot randomized controlled trial. J Intensive Care. (2021) 9:7. doi: 10.1186/s40560-020-00523-7
24. Marra A, Buonanno P, Vargas M, Iacovazzo C, Ely EW, Servillo G. How COVID-19 pandemic changed our communication with families: losing nonverbal cues. Crit Care. (2020) 24:297. doi: 10.1186/s13054-020-03035-w
25. Association des pharmaciens des établissements de santé du Québec,. Foire Aux Questions Pédiatrie. (2020). Available online at: https://www.apesquebec.org/sites/default/files/publications/ouvrages_specialises/SI/20201218_FAQ_PEDIATRIE_VF.pdf (accessed January 28, 2022).
26. Sanavia E, Mencía S, Lafever SN, Solana MJ, Garcia M, López-Herce J. Sedative and analgesic drug rotation protocol in critically ill children with prolonged sedation: evaluation of implementation and efficacy to reduce withdrawal syndrome. Pediatr Crit Care Med. (2019) 20:1111–1117. doi: 10.1097/PCC.0000000000002071
27. Walz A, Canter MO, Betters K. The ICU liberation bundle and strategies for implementation in pediatrics. Curr Pediatr Rep. (2020) 16:1–10. doi: 10.1007/s40124-020-00216-7
28. Society of Critical Care Medicine. ICU Liberation. (2019). Available online at: https://www.sccm.org/iculiberation (accessed January 28, 2022).
29. Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. (2014) 370:444–54. doi: 10.1056/NEJMra1208705
30. Arteaga G, Kawai Y, Rowekamp D, Rohlik G, Matzke N, Fryer K, et al. The pediatric ICU liberation project impact on patient outcomes: the mayo experience. Crit Care Med. (2018) 46:628 doi: 10.1097/01.ccm.0000529292.49511.79
31. Wilson JE, Mart MF, Cunningham C, Shehabi Y, Girard TD, MacLullich AMJ, et al. Delirium. Nat Rev Dis Primers. (2020) 6:90. doi: 10.1038/s41572-020-00223-4
32. Chanques G, Constantin JM, Devlin JW, Ely EW, Fraser GL, Gélinas C, et al. Analgesia and sedation in patients with ARDS. Intensive Care Med. (2020) 46:2342–56. doi: 10.1007/s00134-020-06307-9
33. Yang S, Zhao H, Wang H, Zhang H, An Y. Comparison between remifentanil and other opioids in adult critically ill patients: a systematic review and meta-analysis. Medicine. (2021) 100:e27275. doi: 10.1097/MD.0000000000027275
34. Hall EA, Sauer HE, Davis MS, Anghelescu DL. Lidocaine infusions for pain management in pediatrics. Paediatr Drugs. (2021) 23:349–59. doi: 10.1007/s40272-021-00454-2
35. Lemming K, Fang G, Buck ML. Safety and tolerability of lidocaine infusions as a component of multimodal postoperative analgesia in children. J Pediatr Pharmacol Ther. (2019) 24:34–8. doi: 10.5863/1551-6776-24.1.34
36. Evans MS, Lysakowski C, Tramèr MR. Nefopam for the prevention of postoperative pain: quantitative systematic review. Br J Anaesth. (2008) 101:610–7. doi: 10.1093/bja/aen267
37. Ramirez-Ramon V, Traube C. Delirium. In: Kamat PP, Berkenbosch JW, editors. Sedation and Analgesia for the Pediatric Intensivist. Cham: Springer (2021). p. 275–290.
38. Koriyama H, Duff JP, Guerra GG, Chan AW. Sedation withdrawal and analgesia team. Is propofol a friend or a foe of the pediatric intensivist? Description of propofol use in a PICU*. Pediatr Crit Care Med. (2014) 15:e66–71. doi: 10.1097/PCC.0000000000000021
39. Silver GH, Kearney JA, Kutko MC, Bartell AS. Infant delirium in pediatric critical care settings. Am J Psychiatry. (2010) 167:1172–7. doi: 10.1176/appi.ajp.2010.09111606
40. Smith HA, Brink E, Fuchs DC, Ely EW, Pandharipande PP. Pediatric delirium: monitoring and management in the pediatric intensive care unit. Pediatr Clin North Am. (2013) 60:741–60. doi: 10.1016/j.pcl.2013.02.010
41. Schieveld JNM, Ista E, Knoester H, Molag ML. Pediatric delirium: a practical approach. In Rey JM, editor. IACAPAP e-Textbook of Child and Adolescent Mental Health. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions (2015).
42. Flank J, Sung L, Dvorak CC, Spettigue W, Dupuis LL. The safety of olanzapine in young children: a systematic review and meta-analysis. Drug Saf. (2014) 37:791–804. doi: 10.1007/s40264-014-0219-y
43. Boettger S, Jenewein J, Breitbart W. Delirium and severe illness: etiologies, severity of delirium and phenomenological differences. Palliat Support Care. (2015) 13:1087–92. doi: 10.1017/S1478951514001060
44. Garcia-Amador M, Merchán-Naranjo J, Tapia C, Moreno C, Castro-Fornieles J, Baeza I, et al. Neurological adverse effects of antipsychotics in children and adolescents. J Clin Psychopharmacol. (2015) 35:686–93. doi: 10.1097/JCP.0000000000000419
45. Ruiz Diaz JC, Frenkel D, Aronow WS. The relationship between atypical antipsychotics drugs, QT interval prolongation, and torsades de pointes: implications for clinical use. Expert Opin Drug Saf. (2020) 19:559–64. doi: 10.1080/14740338.2020.1745184
46. Maldonado JR. Acute brain failure: pathophysiology, diagnosis, management, and sequelae of delirium. Crit Care Clin. (2017) 33:461–519. doi: 10.1016/j.ccc.2017.03.013
47. Ahmed R, Maroney M, Fahim G, Ghin HL, Mathis AS. Evaluation of the use of chlorpromazine for agitation in pediatric patients. Ment Health Clin. (2021) 11:40–4. doi: 10.9740/mhc.2021.03.040
48. Tobias JD. Applications of nitrous oxide for procedural sedation in the pediatric population. Pediatr Emerg Care. (2013) 29:245–65. doi: 10.1097/PEC.0b013e318280d824
49. Pettignano R. Nitrous oxide. In: Kamat PP, Berkenbosch JW, editors. Sedation and Analgesia for the Pediatric Intensivist. Cham: Springer (2021). p. 443–450.
50. Society of Critical Care Medicine. Strategies to Approach Drug Shortages of Analgesics and Sedatives During COVID-19 by Joanna Stollings. (2020). Available online at: https://www.sccm.org/COVID19RapidResources/Resources/Strategies-to-Approach-Drug-Shortages-of-Analgesic (accessed January 28, 2022).
51. Jean-Michel V, Caulier T, Delannoy PY, Meybeck A, Georges H. Thiopental as substitute therapy for critically ill patients with COVID-19 requiring mechanical ventilation and prolonged sedation. Med Intensiva. (2022) 46:58–61. doi: 10.1016/j.medin.2020.07.013
52. Stanley TV. Chlormethiazole: an effective oral sedative for cranial CT scans in children. Aust Paediatr J. (1985) 21:191–2. doi: 10.1111/j.1440-1754.1985.tb02132.x
Keywords: pediatrics, COVID-19, sedation, analgesia, delirium
Citation: Castro REVd, Rodríguez-Rubio M, Magalhães-Barbosa MCd, Prata-Barbosa A, Holbrook J, Kamat P and Stormorken A (2022) A review of key strategies to address the shortage of analgesics and sedatives in pediatric intensive care. Front. Pediatr. 10:895541. doi: 10.3389/fped.2022.895541
Received: 14 March 2022; Accepted: 21 July 2022;
Published: 30 August 2022.
Edited by:
Lakshmi Raman, University of Texas Southwestern Medical Center, United StatesReviewed by:
Yves Ouellette, Mayo Clinic, United StatesCopyright © 2022 Castro, Rodríguez-Rubio, Magalhães-Barbosa, Prata-Barbosa, Holbrook, Kamat and Stormorken. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberta Esteves Vieira de Castro, cm9iZXJ0YS5jYXN0cm9AdWVyai5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.