 Lilin Huang
Lilin Huang Shumei Peng
Shumei Peng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr. , 21 June 2022
Sec. Pediatric Immunology
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.893568
Kawasaki disease (KD) is a systemic vasculitis that may impact multiple organ systems in children. Myositis is an unusual presentation of KD that presents with muscle weakness. To date, a few pediatric patients with KD and myositis have been reported. Diffuse muscle weakness involving the 4 limbs was the most common presentation in these children. However, isolated lower limb involvement was rarely reported before. Here, we report lower limb muscle weakness in an 18-month-old child with KD. He presented with fever, rash, conjunctival injection, peeling over fingers and toes, and progressive muscle weakness of the lower limbs. Muscle enzymes were normal, but electromyography indicated myositis. The symptom of fever was relieved quickly by intravenous immunoglobulin and aspirin, which were ineffective for myositis. However, lower limb muscle weakness fully recovered 5 days after prednisolone treatment. This rare case might add value to the growing literature exploring the association of KD with myositis.
Kawasaki disease (KD) is a systemic vasculitis with unknown etiology that commonly affects children under 5 years old (1). The principal clinical feature of KD includes polymorphous rash, oral mucosal changes (red and cracking of lips, “strawberry tongue”), bilateral non-purulent conjunctival injection, extremity changes (erythema and edema of the hands and feet in the acute phase, Periungual peeling in the subacute phase), and cervical lymphadenopathy (≥1.5-cm diameter, usually unilateral). Patients with persistent fever (≥5 days) that fulfill ≥ 4 of the five principal clinical features are diagnosed with typical KD (1). Incomplete KD is considered when patients present with less than 4 out of 5 principal clinical features. Patients with atypical KD often involved multiorgan impairment, such as kidney, central nervous system, and muscle (2). The diagnosis of KD is based on the clinical presentation without confirmatory laboratory tests for this disease. KD may impact multiple organ systems due to the systemic inflammatory response. Therefore, KD is an exceptional disease when it presents with unusual presentations (2). Incomplete forms or atypical presentations of KD may create a conundrum of diagnosis and delay therapeutic decision-making for pediatricians (2). To date, a few pediatric patients of KD with myositis have been reported. Myositis is an unusual presentation of KD that presented with muscle weakness, leading to difficulty walking, respiratory failure, eyelid ptosis, dysphagia, and dysphonia in previous studies (3–11). Diffuse muscle weakness involving the 4 limbs was the most common presentation in these children. However, isolated lower limb involvement was rarely reported before. The objective of the study was to report an atypical KD case with lower limb muscle weakness that was resolved by prednisolone within 5 days. Speculation of the potential mechanism of myositis in KD was also discussed.
An 18-month-old boy was admitted to the first hospital with a history of fever for 6 days. On Day 4 of illness, he developed an erythematous rash and muscle weakness of the lower limbs, which presented him with difficulty walking. The muscle strength of the right limb was worse than that of the left limb. On Day 6 of the illness, a non-purulent conjunctival injection appeared. Laboratory investigations showed white blood cell, 20.79 × 109/L; neutrophils, 70.9%; hemoglobin, 95 g/L; lymphocyte, 23%; platelet, 460 × 109/L; procalcitonin, 0.29 ng/ml; and C-reactive protein, 59.94 mg/L. The muscle enzymes were normal. A clinical possibility of KD with neuropathy or arthritis was initially considered. He was treated with intravenous immunoglobulin (IVIG) 2 g/kg, and aspirin, 30 mg/kg/day. The symptoms of fever, rash, and conjunctival injection were relieved. He developed progressive lower limb muscle weakness, leading to difficulty in getting up by Day 10 of the illness. On Day 11 of the illness, the child was brought to us with complaints of persistent muscle weakness without pain. On examination, the muscle strength of the left lower limb was scaled as Grade III, and that of the right lower limb was scaled as Grades II-III. Repeated blood tests showed thrombocytosis (platelet, 698 × 109/L) and an increased erythrocyte sedimentation rate (ESR, 106 mm/h), but creatine kinase (CK), lactate dehydrogenase (LDH), and ferritin were normal by Day 12 of the illness. The child was not exposed to any potential contact with patients affected with COVID-19, and the SARS-CoV-2 reverse transcription-polymerase chain reaction (RT-PCR) test of the nasopharyngeal swab was negative. Serological IgM tests for influenza virus, parainfluenza virus, adenovirus, EB virus, and Mycoplasma pneumoniae were all negative. Echocardiography showed that the coronary artery was normal. Electromyography (EMG) indicated myositis. Lumbar puncture was performed, and cerebrospinal fluid (CSF) analysis was normal. Oligoclonal zone, antibodies of myelin basic protein, aquaporin-4, myelin oligodendrocyte glycoprotein, N-Methyl-d-aspartate receptor, anti-α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid 1/2, contactin-associated protein-like 2, leucine-rich glioma-inactivated 1, gamma-aminobutyric acid receptor in CSF were all negative. The results of cerebral and full-spine MRI were normal. An acetylcholine receptor antibody in serum was negative. On Day 21 of the illness, the child developed pallor and periungual peeling of skin in the fingers and toes (Figure 1). Therefore, atypical KD with myositis was considered. Considering the progressive muscle weakness even though IVIG and aspirin were given, he was treated with oral prednisolone (1 mg/kg/day). He showed rapid improvement in muscle weakness and was willing to walk 3 days after prednisolone treatment. The patient was discharged, and the muscle weakness completely recovered 5 days after prednisolone treatment. A tapering dose of oral prednisolone (0.5 mg/kg/day) was administered for another 7 days. Repeated echocardiography at 6 weeks of follow-up revealed a normal coronary artery. He remained clinically well on follow-up at 6 months (Table 1).

Figure 1. Periungual peeling of skin in both feet.
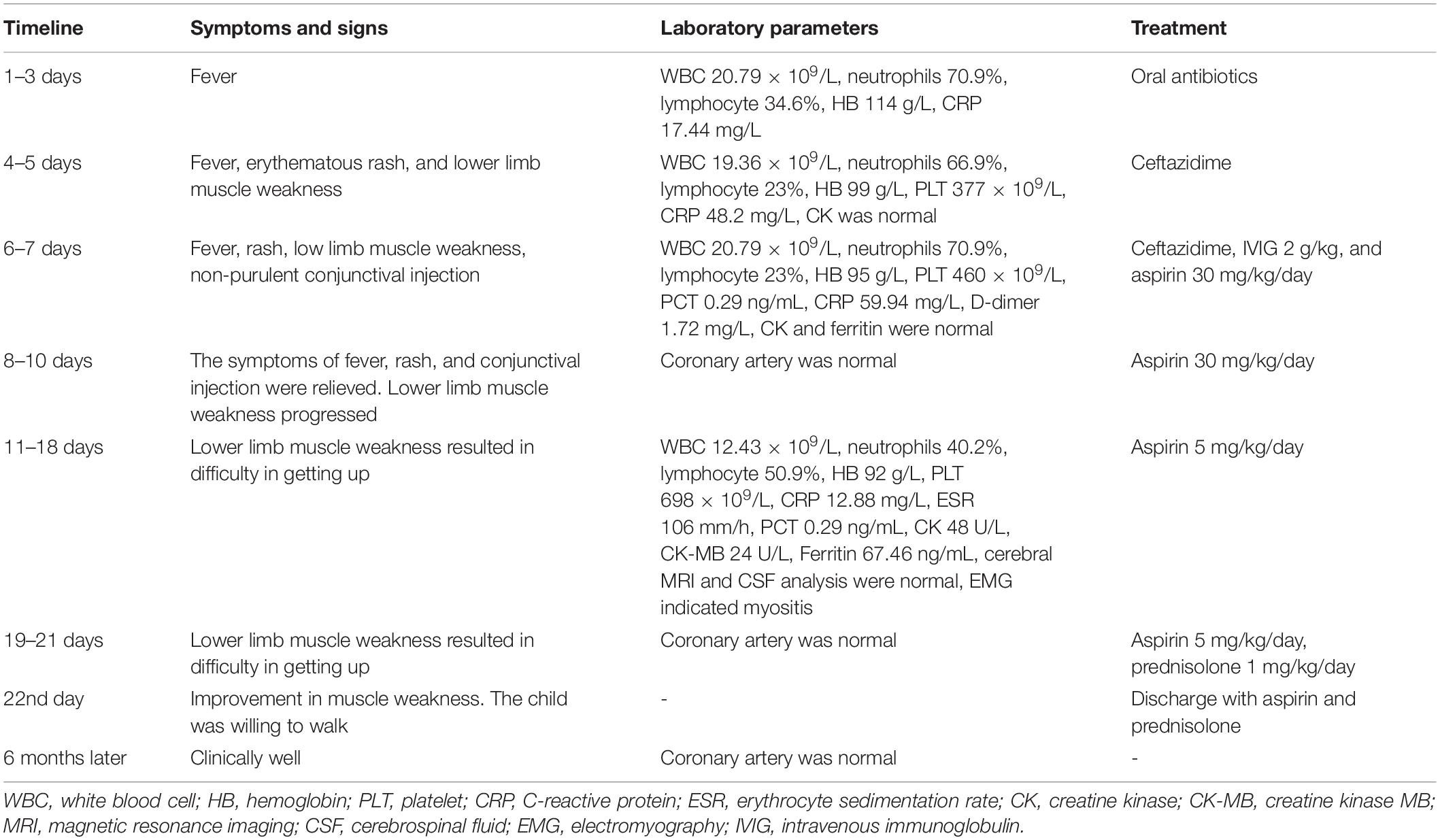
Table 1. The timeline of events.
The KD might involve inflammation in various systems, which requires early diagnosis and prompt treatment to prevent coronary artery injury (12). Myositis is a rare presentation of KD, leading to muscle weakness (2). There have been a few cases with the co-occurrence of KD and myositis. However, isolated lower limb involvement was rarely reported. We reported a child with atypical KD, who showed lower limb muscle weakness. A clinical possibility of juvenile idiopathic arthritis or Guillain–Barre Syndrome was also considered initially since arthritis, arthralgia, myalgia, and neuropathy could also make it difficult for patients to walk. Children under 5 years old might be too young to express the exact symptoms, which could lead to misdiagnosis, especially when muscle enzymes are normal. However, fever was relieved quickly by IVIG, and the sign of peeling over fingers and toes was found on Day 21 of the illness, suggesting the possible diagnosis of atypical KD or multisystem inflammatory syndrome in children (MIS-C) with myositis in our case. MIS-C association with SARS-CoV-2 infection has drawn great attention during the COVID-19 pandemic (13–16). Children with MIS-C might test positive for SARS-CoV-2 by RT-PCR or antibodies in serum since they might be exposed to potential contact with a household member affected with coronavirus disease 2019 (COVID-19) (17, 18). MIS-C might present with KD-like signs and symptoms with more prone to develop toxic shock syndrome (TSS)/macrophage activation syndrome (MAS), resulting in multiorgan failure (19–22). Gastrointestinal and cardiovascular systems are the most affected (14, 17, 23, 24). Children with MIS-C are often older than 5 years of age (18). Laboratory tests might show thrombocytopenia, the elevation of CRP, ferritin, troponin, and D-dimer in patients with MIS-C (25, 26). Our case showed symptoms of fever, skin rash, conjunctival injection, and periungual peeling of skin in the fingers and toes, which could be found in KD and MIS-C. However, the child was 18 months old without the symptoms of abdominal pain, diarrhea, and myocarditis. Laboratory tests showed thrombocytosis with a normal level of total lymphocyte counts, ferritin, CK-MB, and D-dimer. SARS-CoV-2 RT-PCR test of the nasopharyngeal swab was performed three times, which all showed negative results. In addition, the child was not exposed to any potential contact with patients affected with COVID-19. Meanwhile, people were not affected by COVID-19 after contact with this child. Therefore, KD but not MIS-C was diagnosed in our case.
We reviewed previous cases of KD with myositis (Table 2). The age of these cases ranged from 8 months to 10 years, and the timing of muscle weakness that developed in KD ranged from 36 h to 35 days after the onset. Our case was 18 months old, and he developed muscle weakness on Day 4 of the illness, which was consistent with previous reports. Difficulty walking was the most common symptom. Severe myositis could induce respiratory failure, which requires ventilation support. The association of myositis with coronary artery lesions in KD was uncertain since myositis is a rare presentation of KD. To date, coronary artery injury in KD with myositis has been reported in 4 of 10 cases (including our case), which was higher than the 15–25% of untreated patients (2). This might be related to the following reasons: First, patients with myositis might be associated with a latent exaggerated immune response, which results in immune-complex deposits in multiple organs, including the coronary artery. Second, half of the cases with myositis showed atypical presentation or incomplete form, which might induce a delay in the diagnosis and treatment of KD. Finally, the speculation is based on a review of only 10 cases that ask for more data to draw a confirmed conclusion.
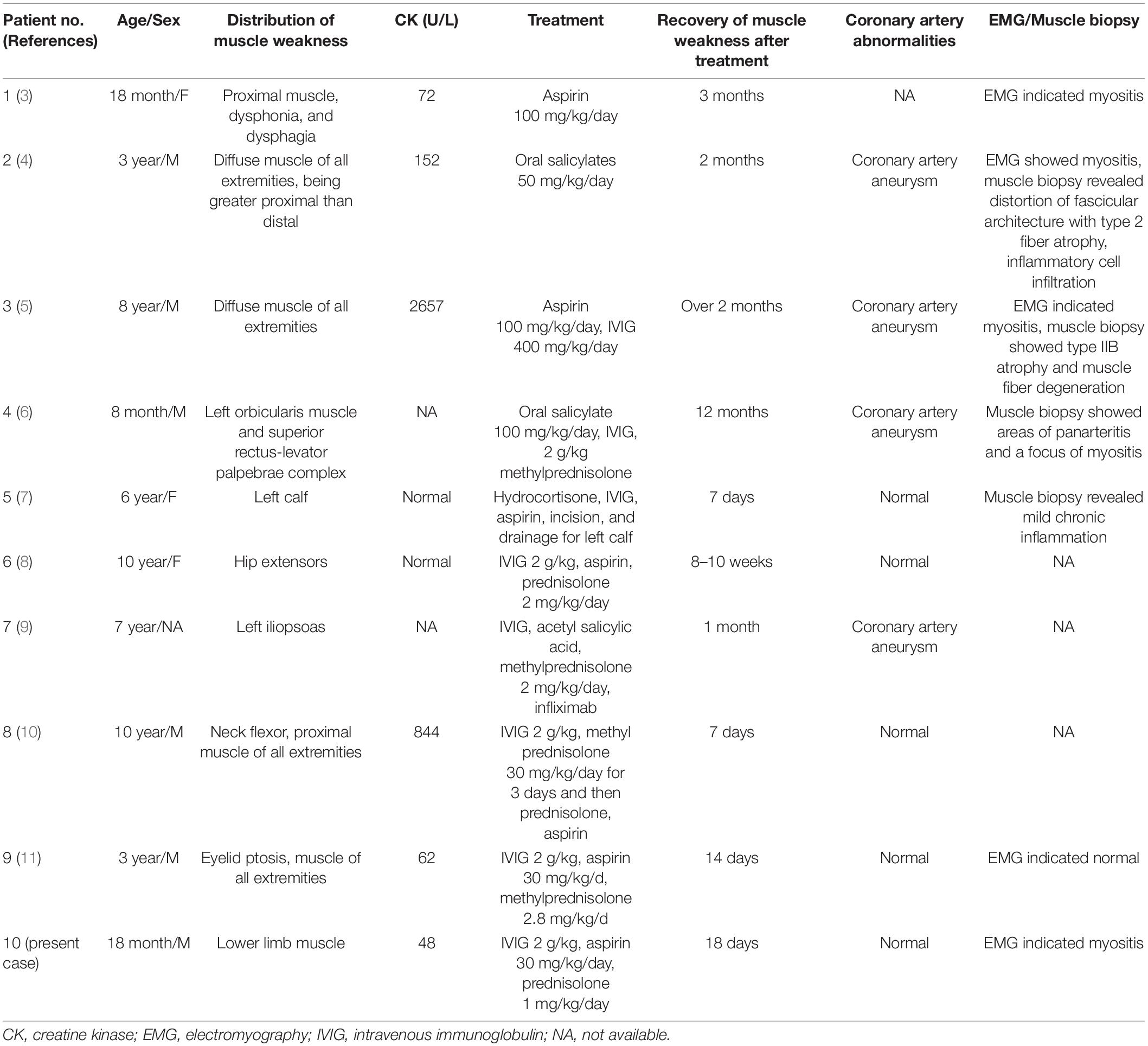
Table 2. Review of previously reported cases with Kawasaki disease and myositis.
The underlying mechanism of KD with myositis has not been elucidated since this complication is rare, and little literature focuses on this subject. KD is a multisystem inflammation that affects multiple organs with elevated inflammatory parameters, including ESR, CRP, and procalcitonin (2, 27). Exaggeration of the immune response plays important role in the pathogenesis of multisystem inflammation. Therefore, KD might develop into life-threatening KD shock syndrome or MAS in some children, which is a characteristic of a hyperinflammatory response (22). MIS-C shares overlapping manifestations with KD, which also induces neurologic manifestations and myositis (28, 29). Therefore, myositis might be one of the presentations of hyperinflammation. It seemed that elevated muscle enzymes were not necessary for myositis in KD. Only 3 of 9 patients in previous studies showed elevated muscle enzymes, while the patient who had the highest CK level showed respiratory failure. Except for muscle enzymes, EMG, muscle biopsy, and imaging of muscles were also performed to diagnose myositis in the previous cases (10). Muscle biopsy is the gold standard for the diagnosis of myositis. However, it is not practical in routine clinical work since it is an invasive test. Muscle biopsies were initially performed on 3 patients and revealed type 2 fiber atrophy with or without vasculitis (4–6). MRI was performed on one patient, which showed hyperintensity on T2-weighted images in the premuscular and intermuscular fascia in the leg (7). EMG was performed on 3 patients with muscle weakness of the extremities, who showed myogenic injury (3–5). The muscle enzymes were normal, but EMG revealed the myogenic injury in our case. However, MRI and muscle biopsy were not performed since he showed prompt clinical recovery with steroid treatment, and his parent did not agree with these investigations at that time. We tried to speculate on the potential mechanism of myositis in KD. Limited studies have postulated that immune-complex deposits in affected muscles result in muscle weakness (10). However, the specific antigen and antibody were not revealed in previous studies. There was only one adult patient with KD and neuromuscular abnormalities, who underwent immunofluorescent staining of related muscle. The result showed linear deposition of IgG along the sarcolemma. Meanwhile, the electron microscopy results showed that the muscle structure was well preserved (30). There was no evidence of nerve impairment in our case and in other children with KD and myositis. Muscle weakness without elevated muscle enzymes might indicate muscle fiber apoptosis but not necrosis; therefore, the cell membrane maintained its integrity, and muscle enzymes were not released into the serum. Therefore, muscle atrophy but well-preserved muscle structure was observed. Conversely, elevated muscle enzymes might indicate severe inflammatory infiltration and necrosis of muscles. This could be proven by the previous case, which had severe muscular weakness, leading to respiratory failure associated with the highest CK (5). Therefore, muscle enzymes need to be monitored closely in patients with KD and myositis.
Early treatment with intravenous immunoglobulin and aspirin for KD is recommended by the American Heart Association (12). Corticosteroids have been recommended for IVIG-resistant cases (10). However, there was no consensus on the treatment of KD with myositis. Corticosteroids were used in 5 patients in previous studies. However, the dose and the period of corticosteroids were inconsistent. All patients with muscle involvement had good prognoses with or without corticosteroid treatment. The duration of myositis ranged from 7 days to 12 months for a full recovery. Our case showed progressive muscle weakness even though IVIG and aspirin were used. It seemed that IVIG and aspirin were invalid or showed delayed effects for myositis. Corticosteroids might quickly reduce inflammation and depress the immune response. The dose of prednisolone in our case was smaller than that in previous studies. However, prednisolone showed good effects for myositis, and the child recovered faster than in previous cases. This might be explained by the following reasons: First, myositis might be self-limited inflammation since three cases were also treated with aspirin and/or IVIG, even though they took more time to recover in these cases. Second, myositis in our case was isolated lower limb involvement, which was less severe than in other children. Muscle weakness without elevated muscle enzymes might indicate limited inflammation in the muscle and a good prognosis of myositis in KD.
In conclusion, we report a case of lower limb muscle weakness with KD. Myositis is a rare presentation of KD that might develop during the course. Pediatricians should be vigilant about this unusual complication for the early diagnosis and treatment of KD. There is no consensus on the treatment of myositis in patients with KD. However, corticosteroids might shorten the course of myositis, which has been reported to be fully recovered in all patients. This rare case might extend the knowledge of isolated lower limb involvement in children with KD. Future studies are needed to further explore the mechanism of myositis in KD.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical approval was obtained from the Ethics Committee of Guangdong Women and Children Hospital for this study. Written informed consent was obtained from the legal guardian, to participate in this study and for the publication of any potentially identifiable images or data included in this article.
LH and SP: study concept and design. JL: acquisition of data. LH and DX: analysis and interpretation of data. LH: drafting of the manuscript. All authors have read and approved the manuscript.
This work was supported by the Youth Program of National Natural Science Foundation of China (Grant No. 81902012 to LH). The funders had no role in the design of the study, collection, analysis, and interpretation of data. They had contributed in supporting the publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rife E, Gedalia A. Kawasaki disease: an update. Curr Rheumatol Rep. (2020) 22:75. doi: 10.1007/s11926-020-00941-4
2. Jindal AK, Pilania RK, Prithvi A, Guleria S, Singh S. Kawasaki disease: characteristics, diagnosis, and unusual presentations. Expert Rev Clin Immunol. (2019) 15:1089–104. doi: 10.1080/1744666X.2019.1659726
3. Koutras A. Myositis with Kawasaki’s disease. Am J Dis Child. (1982) 136:78–9. doi: 10.1001/archpedi.1982.03970370080025
4. Sugie H, Sugie Y, Ichimura M, Mizuno Y, Nishida M, Igarashi Y. A case of polymyositis associated with Kawasaki disease. Brain Dev. (1985) 7:513–5. doi: 10.1016/s0387-7604(85)80120-0
5. Gama C, Breeden K, Miller R. Myositis in Kawasaki disease. Pediatr Neurol. (1990) 6:135–6. doi: 10.1016/0887-8994(90)90048-6
6. Lin H, Burton EM, Felz MW. Orbital myositis due to Kawasaki’s disease. Pediatr Radiol. (1999) 29:634–6. doi: 10.1007/s002470050665
7. Lee EY, Oh JY, Chong CY, Choo JT, Mahadev A, Tan NW. A case of atypical Kawasaki disease with myositis. Glob PediatrHealth. (2015) 2:2333794X15599649. doi: 10.1177/2333794X15599649
8. Agarwal S, Gupta A, Suri D, Rawat A, Singh S. Proximal muscle weakness in a child with Kawasaki disease. Indian J Pediatr. (2015) 82:866. doi: 10.1007/s12098-015-1709-3
9. Vigil-Vazquez S, Butragueno-Laiseca L, Lopez-Gonzalez J, Garcia-San PM, Rincon-Lopez EA. Case of Kawasaki disease presenting as severe myositis. Indian J Pediatr. (2019) 86:1066–7. doi: 10.1007/s12098-019-03009-z
10. Anjani G, Johnson N, Navid A, Saka R, Jindal AK, Singh S. Kawasaki disease malingering as juvenile dermatomyositis: case-based review : myositis in Kawasaki disease. Rheumatol Int. (2021) 42:913–9. doi: 10.1007/s00296-021-04826-2
11. Lin Y, Wang L, Li A, Zhang H, Shi L. Eyelid ptosis and muscle weakness in a child with Kawasaki disease: a case report. BMC Pediatr. (2021) 21:526. doi: 10.1186/s12887-021-02979-4
12. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American heart association. Circulation. (2017) 135:e927–99. doi: 10.1161/CIR.0000000000000484
13. Levin M. Childhood multisystem inflammatory syndrome – a new challenge in the pandemic. N Engl J Med. (2020) 383:393–5. doi: 10.1056/NEJMe2023158
14. Pouletty M, Borocco C, Ouldali N, Caseris M, Basmaci R, Lachaume N, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann Rheum Dis. (2020) 79:999–1006. doi: 10.1136/annrheumdis-2020-217960
15. Viner RM, Whittaker E. Kawasaki-like disease: emerging complication during the COVID-19 pandemic. Lancet. (2020) 395:1741–3. doi: 10.1016/S0140-6736(20)31129-6
16. Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA. (2021) 325:1074–87. doi: 10.1001/jama.2021.2091
17. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. (2020) 324:259–69. doi: 10.1001/jama.2020.10369
18. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with sars-cov-2 and hyperinflammation in pediatric COVID-19: version 3. Arthritis Rheumatol. (2022) 74:e1–20. doi: 10.1002/art.42062
19. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
20. Matucci-Cerinic C, Caorsi R, Consolaro A, Rosina S, Civino A, Ravelli A. Multisystem inflammatory syndrome in children: unique disease or part of the Kawasaki disease spectrum? Front Pediatr. (2021) 9:680813. doi: 10.3389/fped.2021.680813
21. Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC, Herberg J, Bajolle F, Randanne PC, et al. Multisystem inflammatory syndrome in children: an international survey. Pediatrics. (2021) 147:e2020024554. doi: 10.1542/peds.2020-024554
22. Sharma C, Ganigara M, Galeotti C, Burns J, Berganza FM, Hayes DA, et al. Multisystem inflammatory syndrome in children and Kawasaki disease: a critical comparison. Nat Rev Rheumatol. (2021) 17:731–48. doi: 10.1038/s41584-021-00709-9
23. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son M, et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
24. Haslak F, Barut K, Durak C, Aliyeva A, Yildiz M, Guliyeva V, et al. Clinical features and outcomes of 76 patients with COVID-19-related multi-system inflammatory syndrome in children. Clin Rheumatol. (2021) 40:4167–78. doi: 10.1007/s10067-021-05780-x
25. Kostik MM, Bregel LV, Avrusin IS, Dondurei EA, Matyunova AE, Efremova OS, et al. Distinguishing between multisystem inflammatory syndrome, associated with COVID-19 in children and the Kawasaki disease: development of preliminary criteria based on the data of the retrospective multicenter cohort study. Front Pediatr. (2021) 9:787353. doi: 10.3389/fped.2021.787353
26. Giannattasio A, Orlando F, D’Anna C, Muzzica S, Angrisani F, Acierno S, et al. Distinctive phenotype of multisystem inflammatory syndrome in children associated with SARS-CoV-2 according to patients’ age: a monocentric experience. Children (Basel). (2022) 9:468. doi: 10.3390/children9040468
27. Waseem M, Shariff MA, Tay ET, Mortel D, Savadkar S, Lee H, et al. Multisystem inflammatory syndrome in children. J Emerg Med. (2022) 62:28–37. doi: 10.1016/j.jemermed.2021.07.070
28. Gupta L, Lilleker JB, Agarwal V, Chinoy H, Aggarwal R. COVID-19 and myositis – unique challenges for patients. Rheumatology (Oxford). (2021) 60:907–10. doi: 10.1093/rheumatology/keaa610
29. Valderas C, Mendez G, Echeverria A, Suarez N, Julio K, Sandoval F. COVID-19 and neurologic manifestations: a synthesis from the child neurologist’s corner. World J Pediatr. (2022) 18:373–82. doi: 10.1007/s12519-022-00550-4
Keywords: Kawasaki disease, muscle weakness, myositis, systemic vasculitis, child
Citation: Huang L, Peng S, Li J and Xie D (2022) Case Report: Lower Limb Muscle Weakness in a Child With Kawasaki Disease. Front. Pediatr. 10:893568. doi: 10.3389/fped.2022.893568
Received: 10 March 2022; Accepted: 13 May 2022;
Published: 21 June 2022.
Edited by:
Alenka Gagro, Children’s Hospital Zagreb, CroatiaReviewed by:
Amra Adrovic, Koç University Hospital, TurkeyCopyright © 2022 Huang, Peng, Li and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lilin Huang, OTIxMjk1NTk3QHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.