
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 03 May 2022
Sec. Pediatric Infectious Diseases
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.885633
This article is part of the Research TopicStatus of the SARS‑CoV‑2 Pandemic in Pediatric Patients in Latin AmericaView all 9 articles
 Jesus Ángel Dominguez-Rojas1*†
Jesus Ángel Dominguez-Rojas1*† Pablo Vásquez-Hoyos2,3†
Pablo Vásquez-Hoyos2,3† Rodrigo Pérez-Morales4†Ana María Monsalve-Quintero5†Lupe Mora-Robles6†Alejandro Diaz-Diaz7†
Rodrigo Pérez-Morales4†Ana María Monsalve-Quintero5†Lupe Mora-Robles6†Alejandro Diaz-Diaz7† Silvio Fabio Torres8†Ángel Castro-Dajer9†Lizeth Yuliana Cabanillas-Burgos10Vladimir Aguilera-Avendaño11Edwin Mauricio Cantillano-Quintero12
Silvio Fabio Torres8†Ángel Castro-Dajer9†Lizeth Yuliana Cabanillas-Burgos10Vladimir Aguilera-Avendaño11Edwin Mauricio Cantillano-Quintero12 Anna Camporesi13
Anna Camporesi13 Asya Agulnik14
Asya Agulnik14 Sheena Mukkada14
Sheena Mukkada14 Giancarlo Alvarado-Gamarra15,16Ninoska Rojas-Soto17Ana Luisa Mendieta-Zevallos18Mariela Violeta Tello-Pezo19
Giancarlo Alvarado-Gamarra15,16Ninoska Rojas-Soto17Ana Luisa Mendieta-Zevallos18Mariela Violeta Tello-Pezo19 Liliana Vásquez-Ponce20
Liliana Vásquez-Ponce20 Rubén Eduardo Lasso-Palomino5
Rubén Eduardo Lasso-Palomino5 María Camila Pérez-Arroyave5Mónica Trujillo-Honeysberg21Juan Gonzalo Mesa-Monsalve22Carlos Alberto Pardo González23†
María Camila Pérez-Arroyave5Mónica Trujillo-Honeysberg21Juan Gonzalo Mesa-Monsalve22Carlos Alberto Pardo González23† Juan Francisco López Cubillos24†Sebastián Gonzalez-Dambrauskas25,26†
Juan Francisco López Cubillos24†Sebastián Gonzalez-Dambrauskas25,26† Alvaro Coronado-Munoz27†
Alvaro Coronado-Munoz27†Background: Children with cancer are at risk of critical disease and mortality from COVID-19 infection. In this study, we describe the clinical characteristics of pediatric patients with cancer and COVID-19 from multiple Latin American centers and risk factors associated with mortality in this population.
Methods: This study is a multicenter, prospective cohort study conducted at 12 hospitals from 6 Latin American countries (Argentina, Bolivia, Colombia, Ecuador, Honduras and Peru) from April to November 2021. Patients younger than 14 years of age that had an oncological diagnosis and COVID-19 or multisystemic inflammatory syndrome in children (MIS-C) who were treated in the inpatient setting were included. The primary exposure was the diagnosis and treatment status, and the primary outcome was mortality. We defined “new diagnosis” as patients with no previous diagnosis of cancer, “established diagnosis” as patients with cancer and ongoing treatment and “relapse” as patients with cancer and ongoing treatment that had a prior cancer-free period. A frequentist analysis was performed including a multivariate logistic regression for mortality.
Results: Two hundred and ten patients were included in the study; 30 (14%) died during the study period and 67% of patients who died were admitted to critical care. Demographics were similar in survivors and non-survivors. Patients with low weight for age (<-2SD) had higher mortality (28 vs. 3%, p = 0.019). There was statistically significant difference of mortality between patients with new diagnosis (36.7%), established diagnosis (1.4%) and relapse (60%), (p <0.001). Most patients had hematological cancers (69%) and they had higher mortality (18%) compared to solid tumors (6%, p= 0.032). Patients with concomitant bacterial infections had higher mortality (40%, p = 0.001). MIS-C, respiratory distress, cardiovascular symptoms, altered mental status and acute kidney injury on admission were associated with higher mortality. Acidosis, hypoxemia, lymphocytosis, severe neutropenia, anemia and thrombocytopenia on admission were also associated with mortality. A multivariate logistic regression showed risk factors associated with mortality: concomitant bacterial infection OR 3 95%CI (1.1–8.5), respiratory symptoms OR 5.7 95%CI (1.7–19.4), cardiovascular OR 5.2 95%CI (1.2–14.2), new cancer diagnosis OR 12 95%CI (1.3–102) and relapse OR 25 95%CI (2.9–214).
Conclusion: Our study shows that pediatric patients with new onset diagnosis of cancer and patients with relapse have higher odds of all-cause mortality in the setting of COVID-19. This information would help develop an early identification of patients with cancer and COVID-19 with higher risk of mortality.
The mortality associated with COVID-19 in pediatric patients has been lower compared to adults (1–3). However, pediatric patients with comorbidities such as obesity and immunosuppression are at higher risk of morbidity and mortality than healthy patients (4). A population that has been considered at risk are children with cancer.
At the beginning of the pandemic multiple studies from first-line providers and pediatric oncologists from different countries, reported their experience in children with cancer and COVID-19, and shared their concerns regarding possible complications in this population (5–16). Some studies also described the impact of the pandemic on patient care and resulting delays in diagnosis for oncological patients (17–20).
Identification of factors associated with mortality in childhood cancer patients diagnosed with COVID-19 could help providers optimize management of these patients. Factors of interest include the primary oncology diagnosis, the diagnostic stage (new diagnosis vs.stable disease vs. relapse), the stage of treatment (treatment-naïve vs. active treatment), and treatment intensity and their complications. These factors could be associated with higher mortality and critical COVID-19 presentation, leading to prolonged hospitalization, multisystem failure, and prolonged mechanical ventilation. An important study regarding outcomes in this population is the “Global characteristics and outcomes of SARS-CoV-2 infection in children and adolescents with cancer (GRCCC)” study that included 1,520 patients from April 2020 and February 2021 and showed a total mortality of 3.8% and critical illness in 20% of patients (21). The factors associated with critical illness were low-income or lower-middle-income countries, upper-middle-income countries, teenagers (15–18 years of age), lymphopenia (≤300 cells/mm3) and severe neutropenia (≤500 cells/mm3). A study in Peru (2020) reported severe morbidity and mortality in patients with new cancer diagnosed during the COVID-19 admission and without previous cancer therapy (22).
In this study, we sought to analyze the risk factors for mortality in children with cancer from multiple Latin American countries during the second year of the pandemic. We hypothesized that patients with new cancer diagnoses had higher mortality than patients with established diagnoses and ongoing cancer therapy.
We performed a multicenter prospective cohort study including data from 12 hospitals in 6 Latin American countries (Argentina, Bolivia, Colombia, Ecuador, Honduras, and Peru). Centers included are listed in the Supplementary Table 1. Ethical approval was obtained in each participating center. The data collection occurred from April 2021 to November 2021. Patients younger than 14 years of age who had a new or established oncologic diagnosis and a diagnosis of COVID-19 or multisystemic inflammatory syndrome (MIS-C) were included. We included data on patients from inpatient and outpatient settings. A descriptive analysis was done for all the patients included. The cohort analysis included data only from the inpatient setting. Study data were collected and managed using REDCap electronic data capture tools hosted at “Fundación Universitaria de Ciencias de la Salud, Bogota Colombia.” (23, 24). The CRF utilized in Spanish is available in the Supplementary Appendix A.
The primary exposure was diagnosis stage and treatment status. The first group, “new-diagnosis” was defined as patients with no previous diagnosis of cancer, therapy-naïve, and that were diagnosed with cancer during the COVID-19 encounter. The second group, “established diagnosis,” were patients with a known diagnosis of cancer who were on therapy, had not completed initial therapy, and had not achieved remission. A third diagnosis group were patients in “relapse,” defined as patients that had a previous diagnosis of cancer, had a cancer-free period following treatment, and had relapsed active disease on cancer-directed therapy at the time of COVID diagnosis. The diagnosis of relapsed was determined by each treatment group. Another group described in this analysis includes patients in palliative care. This group overlapped with “established diagnosis” and “relapse” groups, and it included patients that were not going to receive further curative cancer treatments.
Clinical data collected for these patients included type of cancer (hematologic vs. solid tumors), the specific cancer diagnosis, and the TNM classification. The data collected about cancer-directed therapy included the dates since last chemotherapy and the diagnosis of COVID-19, if chemotherapy was received within the last 30 days of COVID-19 diagnosis, and if modifications or canceling to chemotherapy were done. Phases of chemotherapy were described as induction, consolidation, and maintenance. Radiotherapy, biologic therapy, and bone marrow transplant data were included. We grouped rituximab, blinatumomab, dasatinib and imatinib as biologic therapies. The primary outcome measured was mortality during the hospital admission. All the data collected is presented in survivors and non-survivors. A descriptive cause of mortality was described for the non-survivors group.
The demographic and epidemiological data included the country of origin. The age of patients was divided into three groups: infant and toddlers, including younger or equal than 5 years of age, school age, including children 6–11 years of age and adolescents aged 12–14 years. Comorbidities were categorized as respiratory, cardiovascular, neurological, genetic, and immunological. Information regarding the COVID-19 diagnosis was also collected, including the type of diagnostic test and symptom duration. The clinical presentation of COVID-19 was included for symptomatic patients. The severity of COVID-19 was classified as defined by the World Health Organization as mild, moderate, severe, and critical (25). We also included the patients who met the criteria for multisystem inflammatory syndrome in children (MIS-C) as defined by the CDC (26). The symptoms at presentation were divided as general symptoms, respiratory, cardiovascular, neurological, gastrointestinal, renal, and dermatological. The occurrence of coinfection was also included, defined as a bacterial or fungal infection with a positive culture, or viral detection with serology, antigen, or PCR (polymerase chain rection). The therapy including respiratory support at admission, the highest respiratory support utilized, steroids, vasoactive medications (measured with vaso-inotropic score), intravenous immunoglobulin, antibiotics, anticoagulation, and surgery were also reported (27). We reported the maximum support required and details about the critical presentation included the presence of shock, hemophagocytic syndrome, and organ failure divided by systems. Laboratory data, radiological tests and echocardiogram information were also included. Findings in chest X-rays and computerized tomographies are reported by delimiting the lungs in 4 areas or quadrants (right upper lobe, right lower and middle lobes, left upper lobe, and left lower lobe).
The data for all the patients is presented as a descriptive analysis for all the variables collected. A frequentist analysis was performed for mortality, including the primary exposure (stage of diagnosis) and all the variables described. The data for inpatient setting is presented as survivors vs. non-survivors. Pearson and Fisher exact test were performed for categorical variables. Wilcoxon rank sum test was performed for all the continuous variables. The data of continuous variables is presented in median and interquartile ranges. A multivariate logistic regression was performed for predictors of mortality. The focus of this analysis was to find variables that could be associated to mortality and that are present on admission. The variables included were stage of diagnosis, type of cancer (hematological vs. solid tumor), co-infection, respiratory, cardiovascular, neurological symptoms, age, time between symptoms and admission, and comorbidities. The results are presented as odds ratio and 95% confidence intervals.
During the study period we included 226 patients with COVID-19 and cancer. Of those, 210 patients were hospitalized and 30 (14%) of those patients died. The enrollment was mainly from Colombia with 95 (41.6%) patients and Peru with 87 (38.5%) patients. The mortality was higher from Peru, with 19 (25%) patients that died vs. 10 (11%) from Colombia, p 0.003. The rest of the countries did not have mortality reported except Honduras that had 1 patient that died. Demographic data and patients baseline characteristics are presented in Table 1. Patients with low weight-for-age (2 standard deviations below in Z score) had higher mortality; other anthropometric measurements were not associated with mortality.
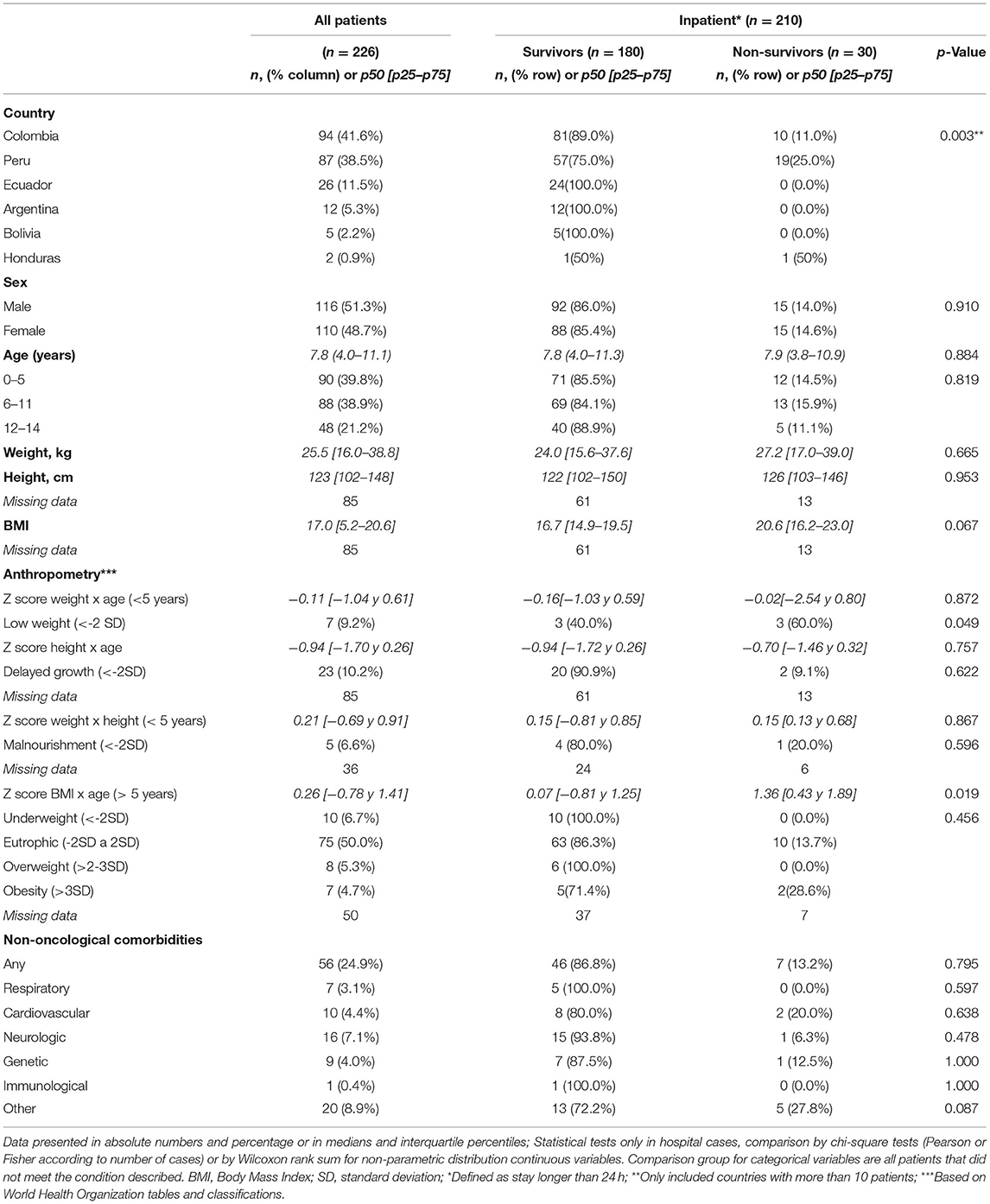
Table 1. Demographic and epidemiological characteristics.
We found a statistically significant difference between the stage of cancer diagnosis and mortality. There was a statistically significant difference in mortality between patients with new diagnosis (n = 11, 36.7%), established diagnosis (n = 1, 3.3%) and relapse (n = 18, 60%, p < 0.001). Four patients who died were on a palliative care. Most patients had hematological cancers (69%) and they had higher mortality (18%) compared to solid tumors (6%, p = 0.032). The list of oncologic diagnoses and analyses regarding oncological characteristics and treatments are presented in Table 2. There were 4 (1.3%) patients from the mortality group vs. 1 (0.6%) of the survivors with biological therapy, p 0.002.
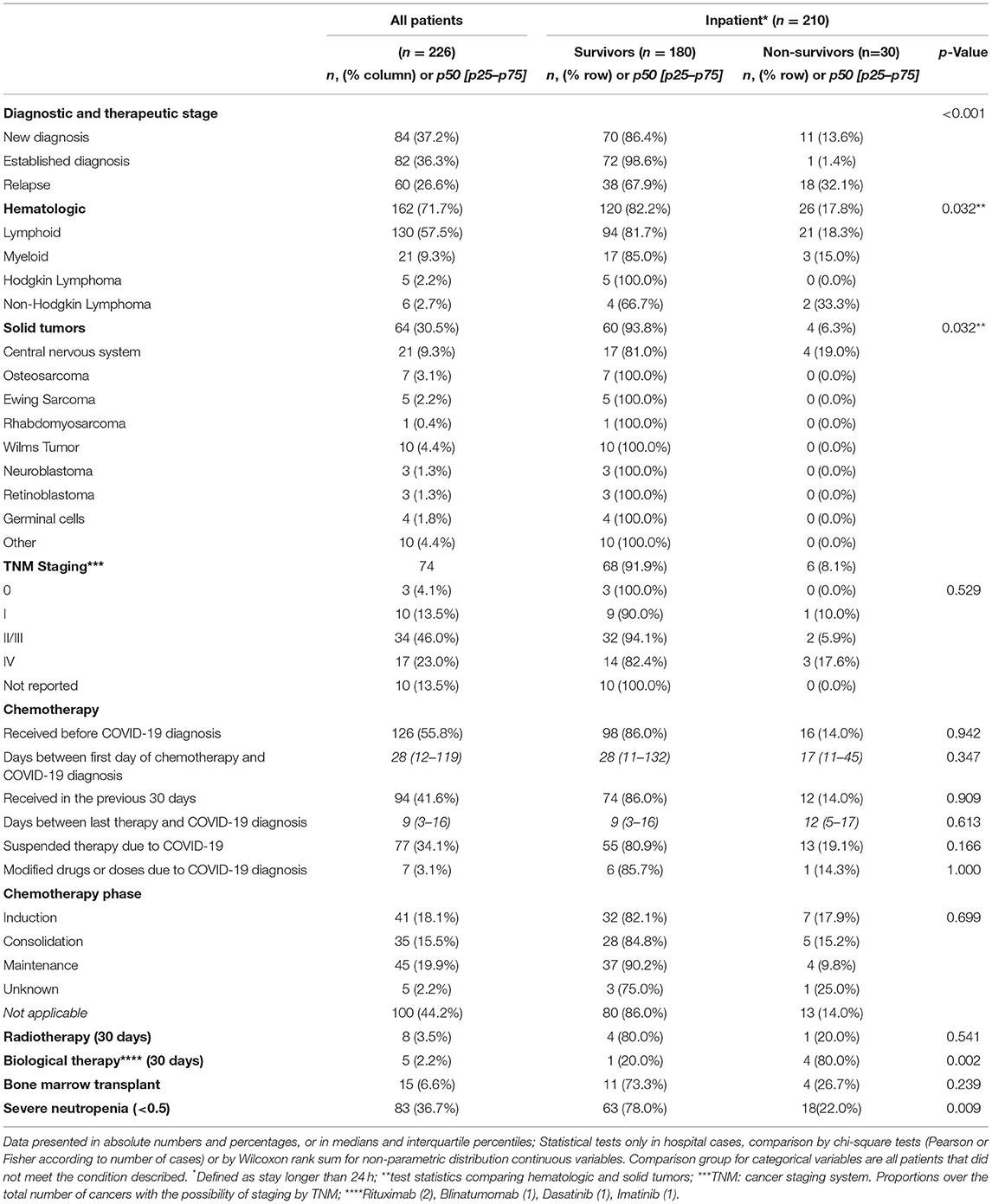
Table 2. Oncological characteristics including diagnosis and oncological therapies.
Table 3 describes details of COVID-19 diagnosis and presentation. Mortality was higher in patients with critical presentation, accounting for 20 (66.7%) of deaths, compared to other COVID-19 severities, p 0.001. Seventeen patients that met MIS-C criteria, which was also associated with mortality, 7 (41%) of them died, p 0.001. Respiratory symptoms were more frequent in the non-survivors, specifically respiratory distress, and hypoxemia. From the cardiovascular system, hypotension and slow capillary refill time were associated with higher mortality. Headaches and altered mental status accounted for neurological symptoms associated with mortality. Renal dysfunction symptoms (decreased urine output and edema) were associated with mortality. Finally, patients with coinfections had higher mortality rates. Half of the patients from the mortality group had a bacterial or viral coinfection, and from the mortality group 12 (40%) had a positive bacterial culture. In the survivors, 36 (20%) of the patients had a coinfection and 26 (14.4%) having a positive bacterial or fungal culture, p 0.001. The details about the infections are described in the Supplementary Table 2.
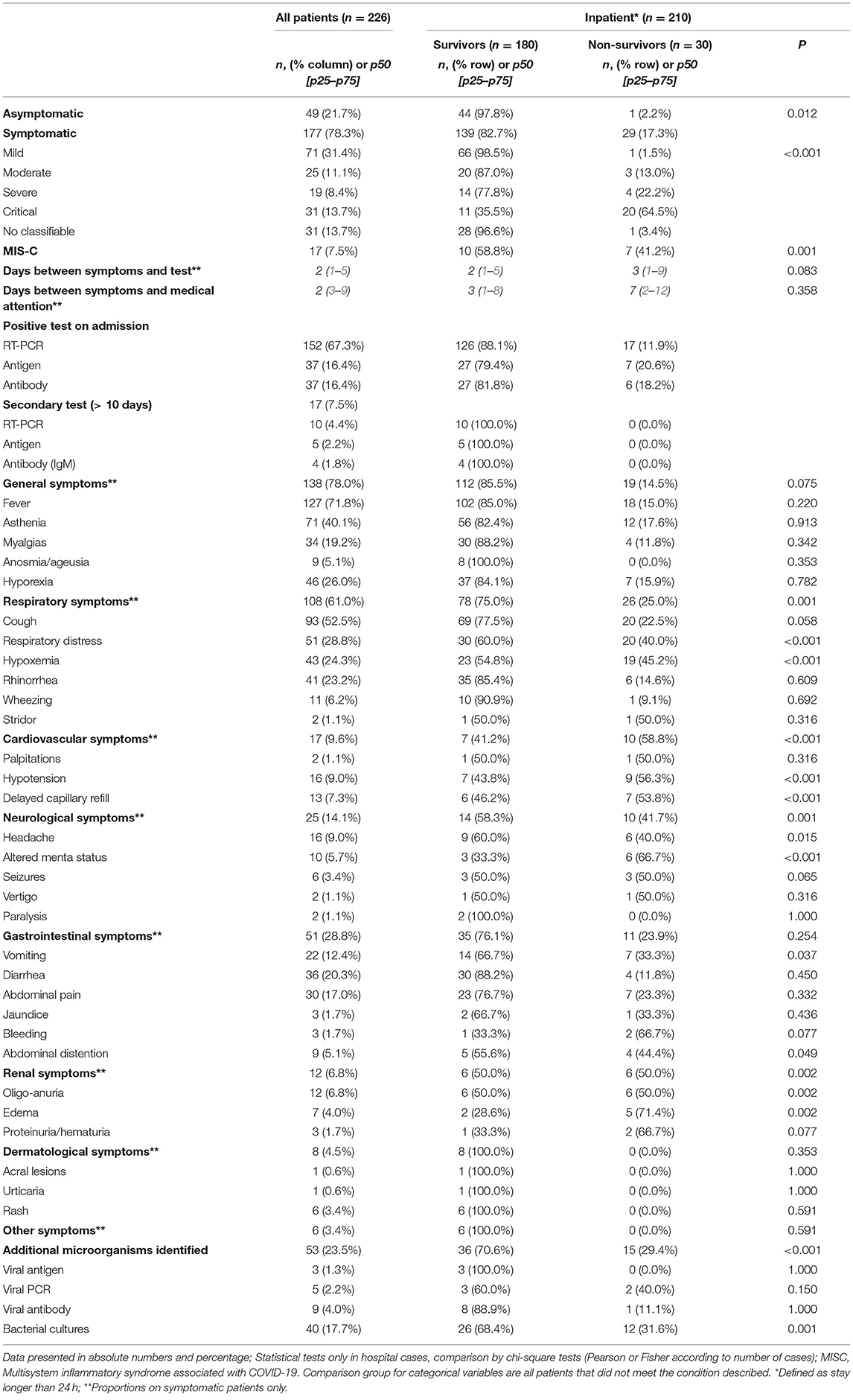
Table 3. COVID-19 characteristics, diagnostic tests, and symptoms presentation.
We also collected laboratory information at admission. Mortality was associated with acidosis, hypercapnia, hypoxemia, PaO2/FiO2 ratio of < 100, lactic acidosis, renal failure, anemia, severe thrombocytopenia, severe neutropenia, severe lymphopenia, liver failure and hyperferritinemia. These results are presented in the Supplementary Table 3. Regarding radiological and imaging studies, 75% of the patients had a chest X-ray and 39% a chest computerized tomography (CT). There was no difference in mortality associated to the number of quadrants with pulmonary infiltrates. However, patients with pleural effusion, 16 (55.3%) of non- survivors vs. 12 (6.7% of survivors, or pneumothorax, 9 (30%) of survivors vs. 7 (3.8%) had higher mortality, p 0.001. The details of this studies are presented in the Supplementary Table 4.
Shock was present more frequently in non-survivors, 25 (83.3%) compared to survivors 26 (14.4%). Multiorgan failure was also more frequent in the mortality group. On admission, most survivors did not require respiratory support, 121 (67.2%) compared to 22 (73.3%) of patients that died. The highest respiratory support during the admission also was different: 20 (66.7%) of the patients that died require invasive mechanical ventilation compared to 107 (59.4%) of the survivors that remained in room air. Vasoactive drugs were used in 23 (76.7%) of the patients that died vs. 23 (12.8%) of the survivors. The details are provided in Table 4.
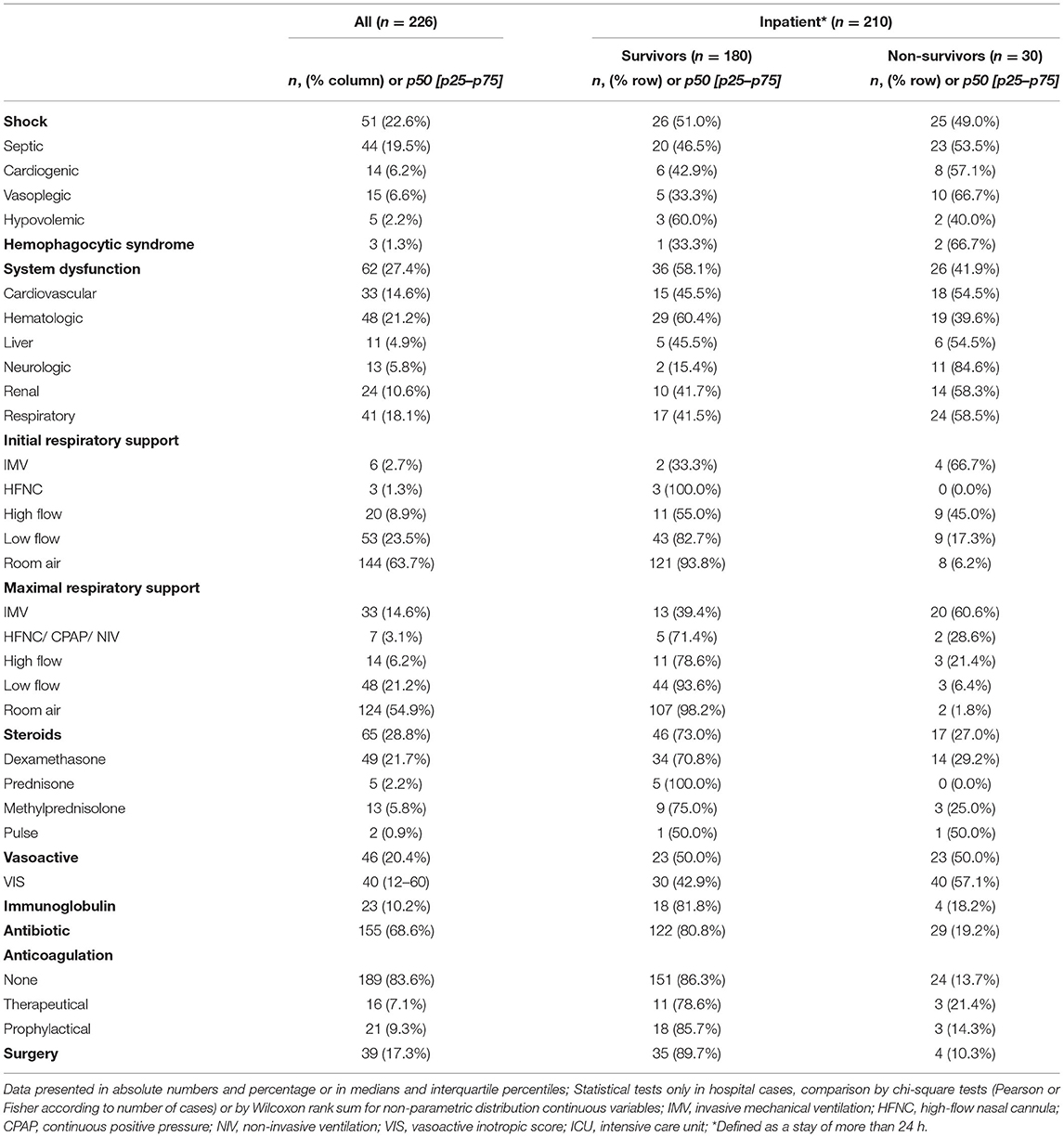
Table 4. Critical presentation, and support therapies.
The causes of death were diverse; 6 (20%) of the patients died from a cancer or cancer treatment-related complications. Two of those had febrile neutropenia, one had complications of tumor lysis syndrome, three had advanced stages of their cancer. One of the patients from this group was in the palliative group. 21 (70%) patients died from septic shock, respiratory failure or multiorgan failure. In all those cases the cause of mortality was attributed to the COVID-19 infection. Three of those patients were in the palliative group. 3 (10%) patients died from hemorrhagic complications, two intracranial bleeds and one pulmonary hemorrhage. These patients represent a combination of complications from COVID-19 infection and high-risk cancer presentations.
A multivariate logistic regression model was performed including variables significant for mortality at presentation from the primary analysis. This model showed factors associated with mortality. Patients with a new cancer diagnosis had an OR 11.5 95%CI (1.31–102) and relapse OR 25 95%CI (2.9–214) (established cancer is the reference). Other factors with higher odds of mortality include concomitant bacterial infection, respiratory symptoms, and cardiovascular symptoms at admission. The details are presented in Figure 1.
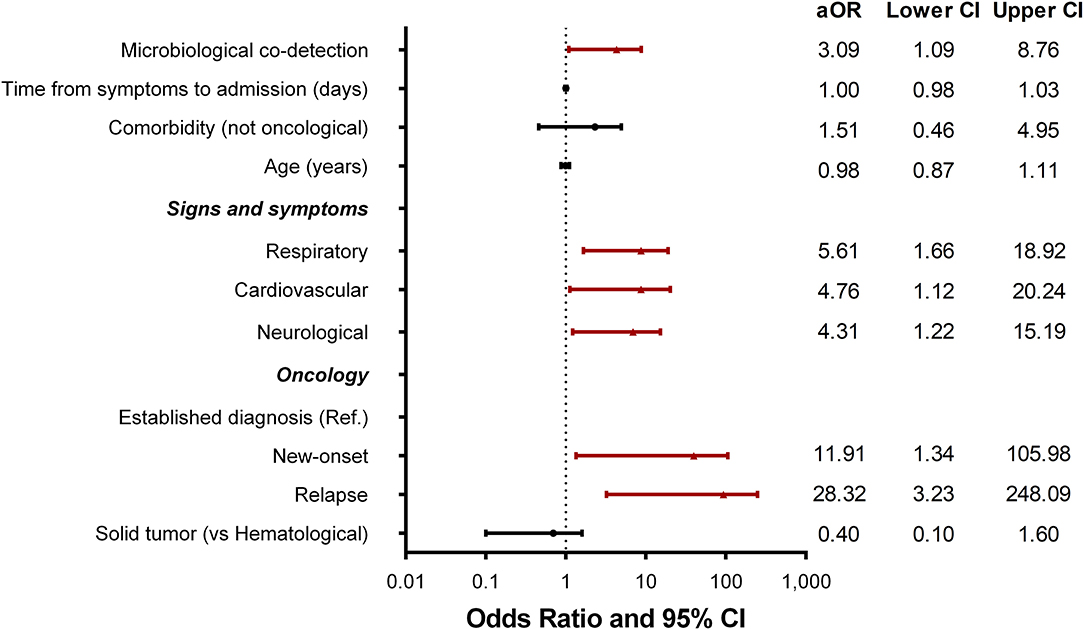
Figure 1. Forest plot for odds–ratio and 95% confidence intervals from multivariate logistic regression model.
The primary objective of our study was to determine if the stage of oncological diagnosis was associated to higher mortality in pediatric patients with COVID-19. Our study found that patients with relapsed oncologic disease and with those newly diagnosed cancer had higher mortality. Upon analyzing the clinical presentation of these patients, we identified that respiratory, cardiovascular, and neurological symptoms were associated with increased mortality.
One of the strengths of our study is to present data for this specific population in Latin American countries and analyze factors of mortality specific for our region during 2021. The global characteristics and outcomes of SARS-CoV-2 infection in children and adolescents with cancer (GRCCC) reported that the all-cause mortality in that study was 6.3%, ranging from 11% in low-middle income countries to 6% in upper-middle income countries (21). The mortality attributed to COVID-19 in this population reported by multiple studies from different countries in Latin America ranged from 6 to 12.3% (28–31). A study by Shahid et al. performed in Pakistan, included 161 cancer patients with and without COVID-19 and compared their outcomes, finding a mortality of 6.8% in COVID-19 patients vs. 2.7% non-COVID-19 patients (32). Meena et al. published a systematic review that included 226 pediatric patients with cancer and COVID-19, showing that 10% of these patients had a critical presentation, requiring critical care admission, and a mortality rate of 4.9% (33). The mortality measured by case fatality rate in pediatric patients with COVID-19 and without cancer reported in different studies from Latin-American varies from 8 to 20% (34–36). However, the mortality and the need for critical care in our study is higher than the findings of other studies looking at patient with cancer and COVID-19. One factor that could explain this difference is that their data is presented for countries from different regions that had different access to medical care during the pandemic. We have a heterogeneous distribution of patients amongst the countries included. However, analyzing mortality factor for each center wouldn't be possible with the number of patients included. Another factor that may explain this difference in mortality is the effect of different variants. Although we did not gather data on variants in our study, our study was conducted during the peak of the Delta variant in our region (37). Our primary objective was to ascertain the mortality associated with different stages of diagnosis including patients that presented with severe forms of COVID-19 at the time of oncological diagnosis. In our study, patients with a new diagnosis of cancer who were therapy naïve also had higher mortality than patients with a prior diagnosis of cancer and ongoing chemotherapy. Further studies would be necessary to determine the immunological impairment of patients with undiagnosed cancer and the possibility of developing a critical form of COVID-19.
In our study, hematological cancer had higher mortality. However, in the regression analysis that was not demonstrated. In the GRCCC study, patients with malignant hematological neoplasms contributed the highest proportion of severe or critical illness (21). In patients with acute lymphoblastic leukemia or acute lymphoblastic lymphoma, severe or critical illness was more common in those who received induction therapy, relapsed or refractory therapy, and the maintenance or continuation phase of therapy. Like GRCCC findings, our study patients with severe neutropenia or severe lymphopenia had higher mortality. We found that concomitant bacterial infection was also associated with mortality. Concomitant bacterial infections in patients with COVID-19 have not been a concern for higher mortality (38). However, bacterial infections in febrile neutropenic patients are a known contributing factor of critical disease and mortality (39, 40). More detailed data regarding the specific chemotherapies utilized for each patient, their microbiological history and timing of the cultures would be necessary to determine if concomitant infections in oncological patients and COVID-19 have a higher risk of mortality than oncological patients without SARS-CoV-2 infection.
The clinical presentation and laboratory profile findings matched the characteristics of patients with severe and critical COVID-19 presentation. There are specific signs and symptoms associated with severe disease described in our study that should trigger the concern for critical disease and mortality. In the regression analysis, the patients that presented with respiratory cardiovascular and neurological symptoms were associated with increased mortality. As described for the general population respiratory symptoms are the most common finding with COVID-19. In our study population respiratory involvement presented as respiratory distress and hypoxemia; cardiovascular involvement with hypotension and prolonged capillary refill and neurological involvement presented with headache and altered mental status and all the above findings were associated with mortality. The symptoms included in the severity criteria for COVID-19 by the World Health Organization include hypoxemia and respiratory distress (25). The frequency of neurological and cardiovascular symptoms in our cohort is low. However, those symptoms found in our study have been associated to severe COVID-19 in other studies (41, 42). More information regarding the etiology of neurological symptoms (COVID-19 vs. oncological disease) is necessary to determine the predictability for severe disease in this population. Cardiovascular symptoms seen in our study are associated to shock which will be a universal severity criterion. Severe neutropenia in our cohort was associated with higher rate of mortality. Studies report mortality for patients with fever and neutropenia as high as 75% (43). Specific comparative studies of patients with and without covid and neutropenia are necessary. The association of bacterial infections and mortality seen in our cohort has been reported in other studies as risk factor for mortality. The patients from our cohort that presented with MIS-C were also associated to higher mortality. Diagnostic criteria of MIS-C can overlap with inflammatory symptoms of cancer and have a strong association with cardiovascular shock (44). Identification of patients at risk for severe disease, critical disease, and mortality in our population is not different than the clinical presentations described by other studies. Early identification of these patients and instructions to the parents with cancer regarding alarm signs can help starting appropriate medical interventions to minimize complications. Further studies specific for MIS-C and COVID-19 are necessary to determine specific and differential symptoms between both with pediatric patients with undiagnosed cancer. A major concern of patients with cancer and COVID-19 are the side effects of therapies and the impact of modification of cancer-directed therapy during the pandemic (17). Authors of a Polish study concluded that the SARS-CoV-2 infection did not increase mortality immediately in patients with cancer, but it was associated to higher chemotherapy rates discontinuation (45). Similar results were obtained by Parambil et al. and the authors concluded that chemotherapy shouldn't be interrupted upon obtaining a positive test identifying SARS-CoV-2 (46). A pending question is if chemotherapy can be continued in patients with severe disease and improve recommendations of treatment for patients with cancer and COVID-19 (47).
Our study has several limitations. We did not have a control group of patients with COVID-19 without cancer during the same period. This limited our ability to analyze if the symptoms, laboratory, and radiographic findings identified in our study are specific to patients with cancer in addition to the variations in each center included. The number of patients included is small and identifying factors associated to mortality in such complex population is difficult. Efforts to minimize selection bias and including all the patients with COVID-19 and cancer in each center were directed by the study investigators in their own centers. The variability observed between countries in enrollment and mortality are probably explained by the capture of all patients with COVID-19 and cancer.
New questions arise from our cohort study. More detailed information regarding the immunogenicity of undiagnosed patients with cancer and the possibility of severe disease with COVID-19 can help multidisciplinary decisions regarding the timing and intensity of treatments. More information regarding patients with relapse therapies and risks for severe disease is needed. Larger studies to analyze differences of chemotherapy drugs and adjusting by characteristics of each center would be helpful. Finally, new studies including the impact of vaccines in this population will be necessary.
Our study shows that pediatric patients with newly diagnosed cancer and patients with relapsed disease have higher odds of mortality in the setting of COVID-19 infection. Pediatric patients with cancer and COVID-19 in Latin America have risk factors associated with mortality, including a clinical presentation with respiratory, neurological, and cardiovascular symptoms. This information would help develop an early identification of patients with cancer and COVID-19 with higher risk of mortality.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Protocolo aprobado IRB Universidad Austral Comité Institucional de Evaluación depende del CEC central Buenos Aires - Argentina P21-035. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
JD-R, PV-H, LV-P, and AC-M had full access to all of the data in the study, takes responsibility for the integrity of the data and the accuracy of the data analysis, and drafting of the manuscript. All the authors contributed equally. JD-R, PV-H, AC-M, LM-R, VA-A, and SG-D: concept and design. JD-R, PV-H, RP-M, AM-Q, LM-R, AD-D, ST, AC-D, LC-B, VA-A, AC, AA, SM, GA-G, NR-S, AM-Z, MT-P, LV-P, RL-P, MP-A, MT-H, JM-M, CP, JL, SG-D, and AC-M: acquisition, analysis, and interpretation of data. JD-R, PV-H, AC-M, LV-P, AC, LM-R, VA-A, SG-D, AA, and SM: critical revision of the manuscript for important intellectual content. PV-H, AC-M, and JD-R: statistical analysis. JD-R: obtained funding. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved, approved the final version for submission, and contributed equally in this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.885633/full#supplementary-material
1. Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, Balough EM, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. (2020) 395:1763–70. doi: 10.1016/S0140-6736(20)31189-2
2. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. (2020) 145:e20200702. doi: 10.1542/peds.2020-0702
3. Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. (2020) 109:1088-95. doi: 10.1111/apa.15270
4. Tsankov BK, Allaire JM, Irvine MA, Lopez AA, Sauve LJ, Vallance BA, et al. Severe COVID-19 infection and pediatric comorbidities: a systematic review and meta-analysis. Int J Infect Dis. (2021) 103:246–56. doi: 10.1016/j.ijid.2020.11.163
5. Andre N, Rouger-Gaudichon J, Brethon B, Phulpin A, Thebault E, Pertuisel S, et al. COVID-19 in pediatric oncology from French pediatric oncology and hematology centers: High risk of severe forms? Pediatr Blood Cancer. (2020) 67:e28392. doi: 10.1002/pbc.28392
6. de Rojas T, Perez-Martinez A, Cela E, Baragano M, Galan V, Mata C, et al. COVID-19 infection in children and adolescents with cancer in Madrid. Pediatr Blood Cancer. (2020) 67:e28397. doi: 10.1002/pbc.28397
7. Ferrari A, Zecca M, Rizzari C, Porta F, Provenzi M, Marinoni M, et al. Children with cancer in the time of COVID-19: an 8-week report from the six pediatric onco-hematology centers in Lombardia, Italy. Pediatr Blood Cancer. (2020) 67:e28410. doi: 10.1002/pbc.28410
8. Gampel B, Troullioud Lucas AG, Broglie L, Gartrell-Corrado RD, Lee MT, Levine J, et al. COVID-19 disease in New York City pediatric hematology and oncology patients. Pediatr Blood Cancer. (2020) 67:e28420. doi: 10.1002/pbc.28420
9. Arous R, Djillali IS, Rouis NO, Boudiaf H, Amhis W, Ziane H, et al. High mortality of COVID-19 in children with cancer in a single center in Algiers, Algeria. Pediatr Blood Cancer. (2021) 68:e28898. doi: 10.1002/pbc.28898
10. Kebudi R, Kurucu N, Tugcu D, Hacisalihoglu S, Fisgin T, Ocak S, et al. COVID-19 infection in children with cancer and stem cell transplant recipients in Turkey: a nationwide study. Pediatr Blood Cancer. (2021) 68:e28915. doi: 10.1200/OP.21.00047
11. Baka M, Michos A, Alexopoulou A, Bouka P, Bouka E, Dana E, et al. COVID-19 among children with cancer in Greece (2020): results from the nationwide registry of childhood hematological malignancies and solid tumors (NARECHEM-ST). Pediatr Blood Cancer. (2021) 68:e29079. doi: 10.1002/pbc.29079
12. Yarali N, Akcabelen YM, Unal Y, Parlakay AN. Hematological parameters and peripheral blood morphologic abnormalities in children with COVID-19. Pediatr Blood Cancer. (2021) 68:e28596. doi: 10.1002/pbc.28596
13. Boulad F, Kamboj M, Bouvier N, Mauguen A, Kung AL. COVID-19 in children with cancer in New York City. JAMA Oncol. (2020) 6:1459–60. doi: 10.1001/jamaoncol.2020.2028
14. Ronsley R, Bouffet E. COVID-19 in pediatric cancer: where are the brain tumors? Neuro Oncol. (2021) 23:1977–9. doi: 10.1093/neuonc/noab189
15. Ruggiero A, Romano A, Attina G. Covid-19 and children with cancer: are they at increased risk of infection? Pediatr Res. (2021) 89:398. doi: 10.1038/s41390-020-0919-1
16. Kotecha RS. Challenges posed by COVID-19 to children with cancer. Lancet Oncol. (2020) 21:e235. doi: 10.1016/S1470-2045(20)30205-9
17. Graetz D, Agulnik A, Ranadive R, Vedaraju Y, Chen Y, Chantada G, et al. Global effect of the COVID-19 pandemic on paediatric cancer care: a cross-sectional study. Lancet Child Adolesc Health. (2021) 5:332–40. doi: 10.1016/S2352-4642(21)00031-6
18. Graetz DE, Sniderman E, Villegas CA, Kaye EC, Ragab I, Laptsevich A, et al. Resilient health care in global pediatric oncology during the COVID-19 pandemic. Cancer. (2022) 128:797–807. doi: 10.1002/cncr.34007
19. Sniderman ER, Graetz DE, Agulnik A, Ranadive R, Vedaraju Y, Chen Y, et al. Impact of the COVID-19 pandemic on pediatric oncology providers globally: a mixed-methods study. Cancer. (2022) 128:1493–502. doi: 10.1002/cncr.34090
20. Vasquez L, Sampor C, Villanueva G, Maradiegue E, Garcia-Lombardi M, Gomez-García W, et al. Early impact of the COVID-19 pandemic on paediatric cancer care in Latin America. Lancet Oncol. (2020) 21:753–5. doi: 10.1016/S1470-2045(20)30280-1
21. Mukkada S, Bhakta N, Chantada GL, Chen Y, Vedaraju Y, Faughnan L, et al. Global characteristics and outcomes of SARS-CoV-2 infection in children and adolescents with cancer (GRCCC): a cohort study. Lancet Oncol. (2021) 22:1416–26. doi: 10.1016/S1470-2045(21)00454-X
22. Coronado Munoz A, Tasayco J, Morales W, Moreno L, Zorrilla D, Stapleton A, et al. High incidence of stroke and mortality in pediatric critical care patients with COVID-19 in Peru. Pediatr Res. (2021) 3:1-5. doi: 10.1038/s41390-021-01547-x
23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
24. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
25. Organization WH. Living Guidance For Clinical Management Of Covid-19. World Health Organization (2021).
26. Godfred-Cato S, Bryant B, Leung J, Oster ME, Conklin L, Abrams J, et al. COVID-19–associated multisystem inflammatory syndrome in children — United States, March–July 2020. MMWR Morb Mrtal Wkly Rep. (2020) 69:1074–80. doi: 10.15585/mmwr.mm6932e2
27. Belletti A, Lerose CC, Zangrillo A, Landoni G. Vasoactive-inotropic score: evolution, clinical utility, and pitfalls. J Cardiothorac Vasc Anesth. (2020) 35:3067-77. doi: 10.1053/j.jvca.2020.09.117
28. Fonseca EV, Pardo CA, Linares A, Lopez JF, Camacho G, Aponte NH, et al. Clinical characteristics and outcomes of a cohort of pediatric oncohematologic patients with COVID-19 infection in the city of Bogota, Colombia. Pediatr Infect Dis J. (2021) 40:499–502. doi: 10.1097/INF.0000000000003135
29. Corso MCM, Soares VJ, Amorim AMP, Cipolotti R, Magalhaes IMQ, Lins MM, et al. SARS-CoV-2 in children with cancer in Brazil: results of a multicenter national registry. Pediatr Blood Cancer. (2021) 68:e29223. doi: 10.1002/pbc.29223
30. Palomo-Colli MA, Fuentes-Lugo AD, Cobo-Ovando SR, Juarez-Villegas L. COVID-19 in children and adolescents with cancer from a single center in Mexico City. J Pediatr Hematol Oncol. (2021) 43:e1047–8. doi: 10.1097/MPH.0000000000002040
31. Montoya J, Ugaz C, Alarcon S, Maradiegue E, Garcia J, Diaz R, et al. COVID-19 in pediatric cancer patients in a resource-limited setting: national data from Peru. Pediatr Blood Cancer. (2021) 68:e28610. doi: 10.1002/pbc.28610
32. Shahid S, Jabbar N, Mansoor N, Rafiq N, Maqsood S. Comparison of clinical and diagnostic features of pediatric oncology patients with or without COVID-19 infection: a retrospective chart review. J Pediatr Hematol Oncol. (2022) 44:e658–64. doi: 10.1097/MPH.0000000000002303
33. Meena JP, Kumar Gupta A, Tanwar P, Ram Jat K, Mohan Pandey R, Seth R. Clinical presentations and outcomes of children with cancer and COVID-19: a systematic review. Pediatr Blood Cancer. (2021) 68:e29005. doi: 10.1002/pbc.29005
34. Undurraga EA, Chowell G, Mizumoto K. COVID-19 case fatality risk by age and gender in a high testing setting in Latin America: Chile, March-August 2020. Infect Dis Poverty. (2021) 10:11. doi: 10.1186/s40249-020-00785-1
35. Schonfeld D, Arias S, Bossio JC, Fernandez H, Gozal D, Perez-Chada D. Clinical presentation and outcomes of the first patients with COVID-19 in Argentina: results of 207079 cases from a national database. PLoS ONE. (2021) 16:e0246793. doi: 10.1371/journal.pone.0246793
36. Domínguez Rojas J, Estupiñan Vigil M, Garcés-Ghilardi R, Alvarado-Gamarra G, Del Águila O, Lope Tenorio AF, et al. [Cross-sectional study of the clinical characteristics and outcomes of children hospitalized with COVID-19 in Lima, Peru]. Medwave. (2021) 21:e8107. doi: 10.5867/medwave.2021.01.8107
37. Twohig KA, Nyberg T, Zaidi A, Thelwall S, Sinnathamby MA, Aliabadi S, et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B. 16172) compared with alpha (B117) variants of concern: a cohort study. Lancet Infect Dis. (2022) 22:35–42. doi: 10.1016/S1473-3099(21)00475-8
38. Langford BJ, So M, Raybardhan S, Leung V, Westwood D, MacFadden DR, et al. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. (2020) 26:1622–9. doi: 10.1016/j.cmi.2020.07.016
39. Lehrnbecher T, Robinson P, Fisher B, Alexander S, Ammann RA, Beauchemin M, et al. Guideline for the management of fever and neutropenia in children with cancer and hematopoietic stem-cell transplantation recipients: 2017 update. J Clin Oncol. (2017) 35:2082–94. doi: 10.1200/JCO.2016.71.7017
40. Al-Mulla NA, Taj-Aldeen SJ, El Shafie S, Janahi M, Al-Nasser AA, Chandra P. Bacterial bloodstream infections and antimicrobial susceptibility pattern in pediatric hematology/oncology patients after anticancer chemotherapy. Infect Drug Resist. (2014) 7:289–99. doi: 10.2147/IDR.S70486
41. LaRovere KL, Riggs BJ, Poussaint TY, Young CC, Newhams MM, Maamari M, et al. Neurologic involvement in children and adolescents hospitalized in the United States for COVID-19 or multisystem inflammatory syndrome. JAMA Neurol. (2021) 78:536–47. doi: 10.1001/jamaneurol.2021.0504
42. Swann OV, Holden KA, Turtle L, Pollock L, Fairfield CJ, Drake TM, et al. Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: prospective multicentre observational cohort study. BMJ. (2020) 370:m3249. doi: 10.1136/bmj.m3249
43. Lekshminarayanan A, Bhatt P, Linga VG, Chaudhari R, Zhu B, Dave M, et al. National trends in hospitalization for fever and neutropenia in children with cancer, 2007-2014. J Pediatr. (2018) 202:231–7.e3. doi: 10.1016/j.jpeds.2018.06.056
44. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in U. S Children and adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
45. Weclawek-Tompol J, Zakrzewska Z, Gryniewicz-Kwiatkowska O, Pierlejewski F, Bien E, Zaucha-Prazmo A, et al. COVID-19 in pediatric cancer patients is associated with treatment interruptions but not with short-term mortality: a polish national study. J Hematol Oncol. (2021) 14:163. doi: 10.1186/s13045-021-01181-4
46. Parambil BC, Moulik NR, Dhamne C, Dhariwal N, Narula G, Vora T, et al. COVID-19 in children with cancer and continuation of cancer-directed therapy during the infection. Indian J Pediatr. (2021) 11:1-7. doi: 10.22541/au.164864286.63566927/v1
Keywords: pediatric cancer, pediatric, COVID-19, child development, PICU (pediatric intensive care unit)
Citation: Dominguez-Rojas JÁ, Vásquez-Hoyos P, Pérez-Morales R, Monsalve-Quintero AM, Mora-Robles L, Diaz-Diaz A, Torres SF, Castro-Dajer Á, Cabanillas-Burgos LY, Aguilera-Avendaño V, Cantillano-Quintero EM, Camporesi A, Agulnik A, Mukkada S, Alvarado-Gamarra G, Rojas-Soto N, Mendieta-Zevallos AL, Tello-Pezo MV, Vásquez-Ponce L, Lasso-Palomino RE, Pérez-Arroyave MC, Trujillo-Honeysberg M, Mesa-Monsalve JG, Pardo González CA, López Cubillos JF, Gonzalez-Dambrauskas S and Coronado-Munoz A (2022) Association of Cancer Diagnosis and Therapeutic Stage With Mortality in Pediatric Patients With COVID-19, Prospective Multicenter Cohort Study From Latin America. Front. Pediatr. 10:885633. doi: 10.3389/fped.2022.885633
Received: 28 February 2022; Accepted: 13 April 2022;
Published: 03 May 2022.
Edited by:
Horacio Márquez-González, Federico Gómez Children's Hospital, MexicoReviewed by:
Alina Gonzalez-Quevedo, Instituto de Neurología y Neurocirugía, CubaCopyright © 2022 Dominguez-Rojas, Vásquez-Hoyos, Pérez-Morales, Monsalve-Quintero, Mora-Robles, Diaz-Diaz, Torres, Castro-Dajer, Cabanillas-Burgos, Aguilera-Avendaño, Cantillano-Quintero, Camporesi, Agulnik, Mukkada, Alvarado-Gamarra, Rojas-Soto, Mendieta-Zevallos, Tello-Pezo, Vásquez-Ponce, Lasso-Palomino, Pérez-Arroyave, Trujillo-Honeysberg, Mesa-Monsalve, Pardo González, López Cubillos, Gonzalez-Dambrauskas and Coronado-Munoz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jesus Ángel Dominguez-Rojas, amVzdXNkb21pbmd1ZXoyNEBnbWFpbC5jb20=
†ORCID: Jesus Ángel Dominguez-Rojas orcid.org/0000-0001-6141-6622
Pablo Vásquez-Hoyos orcid.org/0000-0002-4892-5032
Rodrigo Pérez-Morales orcid.org/0000-0002-7070-7488
Ana María Monsalve-Quintero orcid.org/0000-0002-3891-9368
Lupe Mora-Robles orcid.org/0000-0001-8436-6680
Alejandro Diaz-Diaz orcid.org/0000-0003-0525-9276
Silvio Fabio Torres orcid.org/0000-0001-65228047
Ángel Castro-Dajer orcid.org/0000-0001-7278-4412
Carlos Alberto Pardo González orcid.org/0000-0003-1798-2947
Juan Francisco López Cubillos orcid.org/0000-0003-3175-1651
Sebastián Gonzalez-Dambrauskas orcid.org/0000-0003-4775-227X
Alvaro Coronado-Munoz orcid.org/0000-0001-5349-5260
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.