 Isabel Tuñón-Domínguez1
Isabel Tuñón-Domínguez1 Alicia Cuesta-Gómez2
Alicia Cuesta-Gómez2 Francisco Molina-Rueda2
Francisco Molina-Rueda2 Raúl Juárez-Vela3Regina Ruiz de Viñaspre-Hernández3*
Raúl Juárez-Vela3Regina Ruiz de Viñaspre-Hernández3* Iván Santolalla-Arnedo3
Iván Santolalla-Arnedo3 Juan Luis Sánchez-González4
Juan Luis Sánchez-González4 María Carratalá-Tejada2
María Carratalá-Tejada2
- 1Hospital Beata María Ana, Madrid, Spain
- 2Motion Analysis, Ergonomics, Biomechanics and Motor Control Laboratory (LAMBECOM), Department of Physical Therapy, Occupational Therapy, Rehabilitation and Physical Medicine, Faculty of Health Sciences, Rey Juan Carlos University, Madrid, Spain
- 3Department of Nursing, University of La Rioja, Research Group GRUPAC, Logroño, La Rioja, Spain
- 4Department of Nursery and Physiotherapy, Faculty of Nursery and Physiotherapy, University of Salamanca, Salamanca, Spain
The central nervous system (CNS) of preterm infants might have some peculiarities which distinguish it from that of full term infants. The difficulties associated with prematurity are the main cause of deaths all over the world during the new-born period after community-acquired pneumonia, and the second cause of deaths worldwide in children under five years old. Early recognition of signs indicating fragile postural control in premature infants can support understanding and help prevent and early intervention on possible future neuromotor dysfunctions in these subjects. The purpose of this paper is to determine if there is a qualitatively different development of postural control in premature infants without neurological involvement and infants born at term. We conducted a systematic review of longitudinal and cross-sectional case-control studies published between 2010 and March 2020 on this topic. The evaluation of parameters related to postural control was also included. The methodological quality of the selected works was evaluated using the CASPe critical reading programme for cases and controls. PRISMA guidelines for systematic reviews were followed for prematurity and postural control. 16 articles were included. The total sample amounted to 3,460 participants, of which 1,860 in the preterm group, and 1,600 in the control group. All the studies found show a poorer postural control by the group of children born preterm compared to the group of children born at term and one study indicating more limited postural control with higher prematurity. Regarding the methodological quality according to CASPe, those studies exceeding half of the total score were considered of adequate quality.
Introduction
The World Health Organization (WHO) defines as children born preterm before 37 weeks of pregnancy are completed (1). The difficulties associated with prematurity are the main cause of deaths all over the world during the new-born period (2). It is estimated that, in 2030, the mortality caused by premature labour difficulties will rise from 15% to 18; however, this will occur especially in low-incomes countries, where half of the children born at 32 weeks die because they do not receive proper care (3). On the other hand, there is a rise of preterm infant survival rate in developed countries, thanks to obstetrics and neonatology advances (4).
Furthermore, prematurity implies an important associated morbidity (5) and an inverse relationship with gestational age (5–8). A study carried out in 2019 concludes that the estimated probability of survival without disabilities up to 25 years old is 4.1% for children born at a gestational age of 22 weeks, 78.3% for those born at 28 weeks, and 97.2% for those born full term (9). It is estimated that approximately 8%–9% of children born between 22 and 32 weeks and 14% of those born between 22 and 25 weeks develop cerebral palsy (CP), this being one of the main associated pathologies (10).
Accordingly, the central nervous system (CNS) of preterm infants might have some peculiarities which distinguish it from that of full term infants. One of these peculiarities could be alterations in postural control.
Having knowledge of postural control in preterm infants can support the understanding of motor competence, thus helping the prevention of and early intervention on future neuromotor dysfunctions. To begin with, it should be understood that postural control has been defined as the act of maintaining, achieving, or restoring a state of balance during any posture or activity. Postural control strategies can be predictive or reactive, and can involve a response of fixed support or change of support (11, 12). Maintaining postural control requires the integration of the information provided by the vestibular, somatosensory, and visual systems (13, 14), in addition to the integrity of the cerebellum as the coordinator of the three systems. However, postural stability does not require only sensory integration, as adequate motor response is also necessary to maintain the effect of the centre of gravity inside the support surface (15). It is important to note that, postural control is primarily prospective (as opposed to reactive) and used to engage with the environment and to support action systems (manipulation, attention, locomotion, orienting); thus, intervention should focus on infant-directed action so that prospective control is inherent in the therapeutic plan. Postural control is the background of all other action systems and thus should be a primary focus as functional skills are changing over time (16).
Considering that a preterm newborn may present higher risk factors, we need to identify how motor development and the trajectory of postural acquisitions differ between preterm and full term infants, in order to provide more specific action protocols and procedure strategies to this vulnerable group. Our aim was to determine the effect of prematurity on the development of postural control during the postnatal/infancy stage in children born before 37 weeks and without disease or neurological sequelae after birth, as compared to healthy children born at term.
Methods
We performed a Systematic Review of longitudinal and cross-sectional case-control studies included in the literature review, published from the year 2010 to March 2020, which confirm a possible relationship between prematurity and postural control. The research question was established according to the “population, intervention, comparison and outcome” model (PICO), where the inclusion criteria are in relation to the selection of studies. Regarding population, the participants of this review were limited to underage patients without diseases and neurological sequelae, divided into two groups according to gestational age; those children born preterm (<37 gestational weeks) made up the preterm group (PG), while those born full term were referred to the control group (CG). The intervention consisted in evaluating specific values of postural control, in order to make a comparison between the results obtained by the preterm group and those obtained by the control group. The measurement of the results included the evaluation of values related with postural control, such as control of the segmental trunk, movement quality in different positions, balance, manual dexterity, etc. Several limits were established concerning the language of the articles; English and Spanish were selected. As for dates of publication, all the articles from January 2010 to March 2020 were included. The following databases were checked: Scopus, Web of Science, CINHAL, Medline Complete, Science Direct, and PubMed. As to the search terms, the ones used, including the Medical Subject Heading (MESH), were: “premature infant”, “premature birth”, “preterm infants”, “full term infants”, “postural balance”, “balance” and “postural control”; all of them combined with the Boolean operators AND and OR. All related articles that used analogous terms that meant prematurity/preterm were considered.
The article selection process included some steps. The first step was to review titles and abstracts and exclude those not relevant to this study; duplicates were excluded next. As for the second step, complete texts were downloaded for review; only those complying with the inclusion criteria and answering the research question were selected. The third step consisted of a manual search to obtain references that might have not appeared during the first step.
All the potentially available articles were examined by two assessors who evaluated the selection independently, by analysing the full texts based on those which kept to the inclusion criteria with the aim of deciding their relevance to the review. The guidelines of the PRISMA statement were followed to improve the quality of this systematic review (17).
The methodological quality of the selected studies was evaluated according to the critical reading programme CASPe for case-control studies, which presents a total of 11 items. The first two are elimination questions, where both answers must be positive to be able to continue. Items 1–5 verify if the results of the study are valid, whereas items 6–9 show which results are obtained, while items 9–11 indicate if the acquired results are applicable. The answers to these items may be “yes”, “I don’t know” or “no”. One point is added for every item answered with a “yes”; “I don’t know” or “no” answers are not scored. Consequently, the highest score for an article cannot be higher than 11 points, and the minimum score may be 0 points. Studies with a higher score are considered to have a higher methodological quality than those with a lower score.
Results
Description of the studies
Searching the different databases yielded 398 studies. After taking out the duplicates, and those which, based on their title or abstract, were not considered adequate to the inclusion criteria, we were left with a total of 57 studies. After an in-depth analysis, we finally included a total of 16 articles (18–33) in the study (Figure 1, Table 1).

Figure 1. Flowchart.
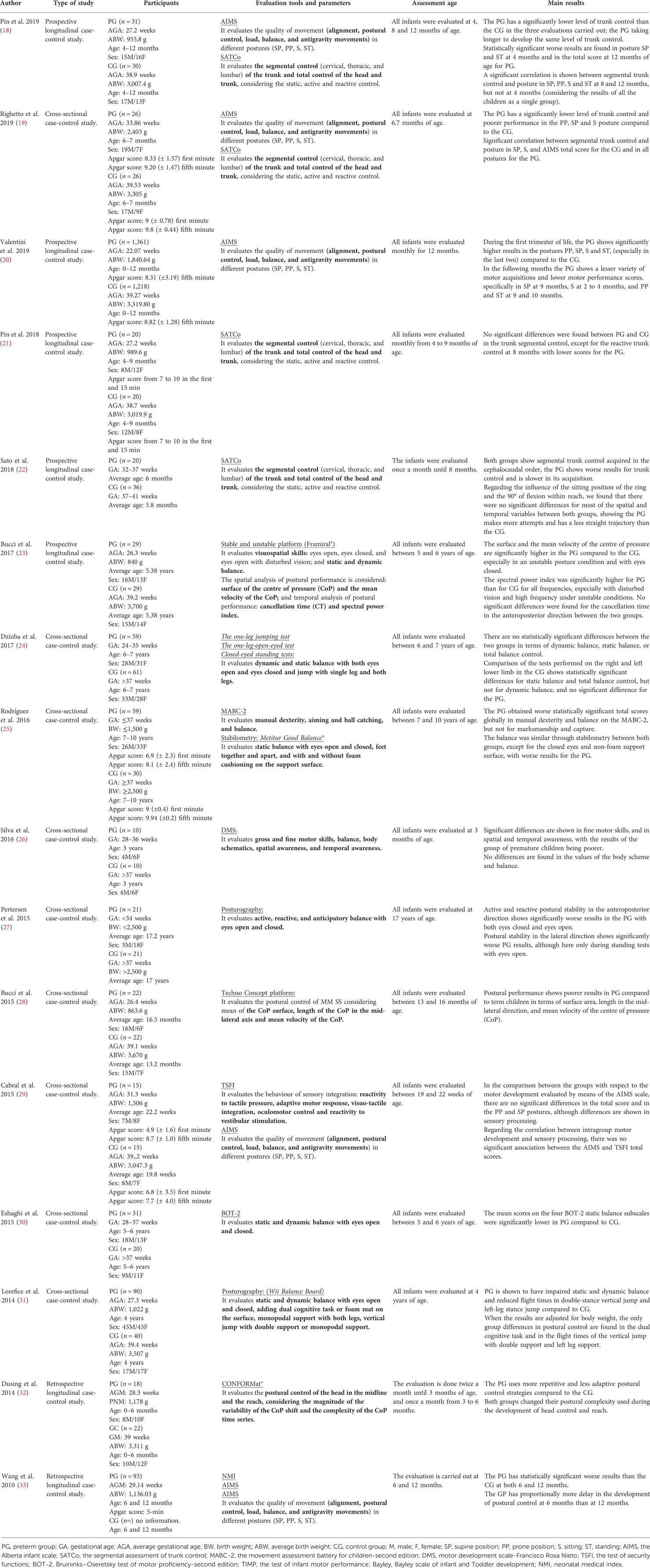
Table 1. Results.
The studies were of an observational nature, case-control, which referred to preterm and full-term infants, respectively.
Altogether, there was a sample of 3,460 participants, 1,860 in the children born preterm group and 1,600 in the control group, referring to those children born at term, although it should be considered that one of the studies did not provide data about the number of participants in the control group (33). All the studies included underage participants, who were classified according to gestational age, regardless of birth weight and sex. Out of the 16 studies, eight provided the average gestational age per group (19–21, 23, 28, 29, 31, 32); seven provided the intervals of gestational age which corresponded to each group (18, 22, 24–27, 30), and one provided the data about the average gestational age of the preterm group, even though it did not provide data referring to the control group (33). The birth weight and sex of both groups was specified in 10 studies. All the studies specified the intervention age, except for one (33), which only made reference to the age of the preterm group. Considering the last condition, it may be observed that seven studies were carried out during the first year of life of the participants (18–22, 29, 32, 33), six were carried out from 3 to 10 years old (23, 24, 26, 30, 31), two were developed at the age of 13–17 years old (25, 27, 28) and one was carried out during the first year of life of the preterm infants group, but here the age of the control group was not specified (33). Out of the 16 studies included, six followed the evolution of the participants during a determined period of time; four were of a prospective nature (18, 20–22), and two of a retrospective nature (32, 33); the rest were cross-sectional studies.
Regarding the evaluation tools, six studies used posturography; four used it exclusively (23, 27, 28, 31); one used it together with the Movement Assessment Battery for Children-second edition (MABC-2) (25); the last one used it together with the Test of Infant Motor Performance (TIMP) and Bayley Scale of Infant and Toddler Development (Bayley) (32). The Alberta Infant Motor Scale (AIMS) was used by five studies; one used it exclusively (20); another used it together with the Test of Security Functions (TSFI) (29); a third study used it together with the Neonatal Medical Index (NMI) (33); and the two remaining studies used it together with the Segmental Assessment of Trunk Control (SATCo) (18, 28). Additionally, two studies carried out the evaluation of SATCo exclusively (21, 22). As for the evaluation tools, the Motor Development Scale-Francisco Rosa Nieto (MDS) (26), Bruininks-Oseretsky Test of Motor Proficiency-second edition (BOT-2) (30), the one-leg jumping test, the one-led-open-eyed test, and the closed-eyed standing test (24) were also used.
Synthesis of the main results
The results obtained from the statistical analysis of all the studies were considered as significant when p < 0.05. Segmental trunk control was evaluated using SATCo, in Pin et al. (18) and Righetto et al. (19), which found worse results during the first year of life for the preterm group than for the full-term group. Pin et al. (21) found worse results for the preterm group only in one item of SATCo (in reactive trunk control), in the articles in which this measure was used, the participants analyzed were in the first year of life. Pin et al. (18) and Sato et al. (22) confirmed that the learning processes in the preterm group were slower. Pin et al. (18) and Righetto et al. (19) checked for correlations between trunk control and gross motor skills during the first year of life. The first study found a significant correlation between trunk control and movement quality in every position at 8 and 12 months old, but not at 4 months old, whereas the second study found a significant correlation between trunk control and the supine and sitting positions, and in the total score of AIMS for the control group, and in every position for the preterm group.
As for movement quality in different positions, which was evaluated by means of AIMS, in the articles in which this measure was used, the participants analyzed were in the first year of life. Pin et al. (18) found lower results for the preterm group in the total score at 12 months old; Wang et al. (33) did as well, at 6 and 12 months old. Significant differences which means worse results for the preterm group were also found: by Pin et al. (18) in sitting and bipedalism at 4 months old; by Righetto et al. (19), in the supine, prone and sitting position at 6–7 months old; by Valentini et al. (20) in the supine position at 9 months old, sitting position at 2 to 4 months old and in bipedalism and the prone position at 9 and 10 months old; and by Cabral et al. (29) in the supine and prone position at 5 months old. However, Valentini et al. (20) found that, during the first term of life, the preterm group obtained higher results in every position, but during the next months the control group showed a wider variety of motor acquisitions and higher scores in motor performance.
On the other hand, balance was evaluated in seven studies (23–28, 30, 31), the children included in these studies had ages from three years. Dziuba et al. (24) and Silva et al. (26) did not find significant differences, and Rodríguez et al. (25) did not find significant results for stabilometry except for the closed-eyes condition and over a viscoelastic foam surface (which were worse for the preterm group), but they did find significant differences for MABC-2. The study by Bucci et al. (23), which considered the surface and the average speed of the centre of pressure (CoP), obtained worse result for the preterm infants group; whereas Petersen et al. (27) showed by means of posturography worse results in the active and reactive postural stability of the preterm group with open and closed eyes in an anteroposterior direction and with open eyes in a lateral direction. Eshagui et al. (30) found that the average scores in the four static balance subscales of BOT-2 were significantly lower in the preterm infants group. Lorefice et al. (31) found that the preterm group had a damaged static and dynamic balance and limited jumping times in vertical double-support jumping and left-leg-support jumping in comparison with the control group.
Lastly, manual dexterity or range were evaluated in four studies (22, 25, 28, 32). Sata et al. (22) and Dursing et al. (32) studied this factor in children in their first year of life, while the children included in the studies by Rodriguez et al. (25) and Bucci et al. (28) comprised ages between 13 and 17 years.
Sata et al. (22) observed more range attempts and a lower straight trajectory to the midfield line for the preterm group than for the control group. Dursing et al. (32) showed that the preterm infants group used more repetitive and less adaptive postural control strategies in comparison with the control group and that both groups changed their postural complexity during the development of the head and range control.
Rodríguez et al. (25) found worse total scores in the preterm infants group in manual dexterity, although not in aiming and ball-catching. Bucci et al. (28), referring to the postural performance of the upper member, showed worse results in the preterm group, regarding the surface area, the medial-lateral direction length, and the average speed of CoP.
Methodological quality
The methodological quality of the studies included in an article was evaluated using the critical reading programme CASPe (Table 2), based on which a maximum score of 9/11 points was obtained in five studies (19, 20, 23, 30, 32), 8/11 points in six studies (18, 22, 25, 27, 28, 31), 7/11 point in four studies (21, 24, 29, 33), and 6/11 point in one study (26). Those with a higher score were considered to have better methodological quality.
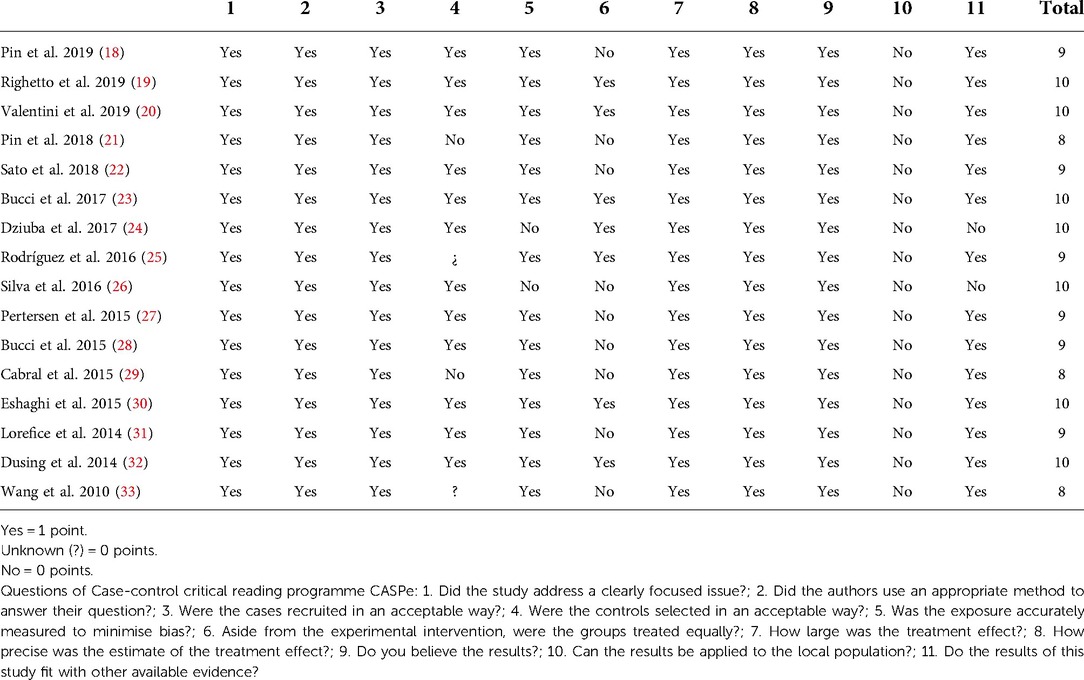
Table 2. Quality assessment: case-control critical Reading programme CASPe.
Discussion
The aim of this study was to carry out a literature review, with the goal of understanding whether the development of postural control of preterm infants without neurological sequelae is different from that of full-term infants, and whether there exists any relationship between prematurity and postural control. All the studies we found compared the postural control of preterm and full-term infants; in addition, one of the studies also checked whether more prematurely born infants have worse postural control than those less prematurely born. The results obtained by the studies showed that the preterm group has worse postural control than the control group.
The findings also showed worse trunk control by the preterm infants group, with slower learning processes. All the studies involving this value considered the improved age, meaning if the baby had been born with 40 weeks of gestation, recommended in order to compensate for biological immaturity until the child is able to walk without help (34), which, added to the equality of the patients' functional status at the beginning of the treatment, confirms the absence of confusion bias. Segmental trunk control was evaluated with SATCo during the first year of life, which is an authentication tool for three different terms in a sitting position: continuity in a neutral vertical position without movement (static control), continuity in a neutral vertical position during voluntary movements of the head or range (active control), and recovery of a neutral position after a balance disturbance due to a push (reactive control). Furthermore, this scale is considered as highly reliable among assessors (ICC ≥ 0.8) (35). The studies carried out by Pin et al. (18) and Righetto et al. (19) showed the same results even though the gestational age in the second study was higher than in the first. However, Pin et al. (18) and Pin et al. (21) had different results in the evaluation of segmental trunk control at 4 and 8 months old. The first study showed worse significant results for the preterm infants group in static, active and reactive control in both evaluations, while the second study only showed worse results in reactive trunk control at 8 months old; although both studies included extremely preterm infants in the preterm group, and used a similar sample size and the same evaluation tool. Pin et al. (18) and Righetto et al. (19) checked for statistically significant correlations between trunk control and gross motor skills during the first year of life, using SATCo and AIMS, and showed coefficients varying between 0.86 and 0.88 (35). However, the first study verified this correlation independently of the gestational age, whereas the second study distinguished the control group from the preterm group, which is the reason why the difference between the findings obtained in both studies can be justified.
As regards movement quality in different positions, worse results were obtained for the preterm infants group. All the evaluations were done using AIMS, a scale authenticated for preterm infants considered to be highly reliable by assessors (ICC ≥ 0.99) (36). Therefore, the implementation of this scale is appropriate, and it should be considered as a positive aspect that every study which evaluated postural control considered the improved age. The evaluations carried out using this scale were in children who were in their first year of life. Valentini et al. (20) found that during the first term of life, the preterm group obtained higher significant results in every position, whereas, during the next months, the preterm group had a smaller variety of motor acquisitions and lower scores in motor performance in comparison with the control group. According to the authors, a possible explanation for the preterm group showing better postural control results during the first term of life may be based on the fact that preterm new-borns, who do have difficulties integrating and modulating stimuli at birth, develop strategies to deal with their organic disadvantages and thus adapt to the environment through behavioural organization and intense motor maturity during the first months. However, this finding did not coincide with the results obtained in any other study, possibly because this study used a far wider sample than all the other studies. Contrary to the above, results revealing worse postural control for the preterm group during the next months of life were found by Wang et al. (33) at 6 and 12 months old, and Pin et al. (18), only at 12 months old, although no significant difference was found at 4 and 8 months old. The rest of the studies did not show significant results for the total score but only for specific positions. Moreover, the study carried out by Wang et al. (33) indicated that the preterm group had proportionally more deficiency in postural control at 6 than at 12 months old, which should be verified by future research.
With regard to balance, the majority of studies obtained unfavourable results for the preterm group. Rodríguez et al. (25), in their patients between 13 and 17 years old, found significant differences for MABC-2 between the two groups but did not find different statistically significant results for stabilometry (except for the closed-eyes condition and the support surface without foam), which is considered as the gold standard for this value in postural control evaluation (37). The disagreement observed between the two balance evaluation tools may be due to the kind of movement analysed, because stabilometry specifically evaluates postural control and adaptive response to various changes controlled in the sensory input, whereas MABC-2 includes exercises which involve not only postural control, but also other variables such as agility. On the other hand, the study carried out by Bucci et al. (23), which also used posturography in children with an average age of 5.38 years, found unfavourable results for the preterm group especially under the closed-eyes condition, although in this case the differences obtained in the unstable condition also stood out, as opposed to the results obtained by the previous study for the support surface without foam condition. These differences might have occurred because the two studies used different samples as far as age and type of platform used. The research carried out by Petersen et al. (27), that included children with an average age of 17.2 years, also used posturography as the evaluation tool; as with the previous studies, unfavourable significant results were obtained for the preterm group in the closed-eyes condition, but also in the open-eyes condition. It should be considered that this study used an older age sample than the previous two as well as a different kind of platform. In the case of the studies carried out by Eshaghi et al. (30) and Lorefice et al. (31), the preterm group, with children from three years, was found to have worse balance than the control group, even though these two studies used different evaluation tools. Lorefice et al. (31) used posturography, whereas Eshaghi et al. (30) used BOT-2, a scale which should be used starting at 4 and a half years and has good reliability (test-retest; ICC = 0.56) and moderate intern consistency (ICC = 0.67). In contrast with these results, the findings obtained by Dziuba et al. (24) and Silva et al. (26), that included children from three year, did not show significant differences between the preterm and full-term groups, although using different sample ages and evaluation tools. Furthermore, it should be considered that the Silva et al. (26) study carried out the evaluation of the preterm group under different conditions than for the control group; the preterm infants were evaluated at home in an environment where the evidence may have been gathered without outside influences, whereas the full-term infants were evaluated at school.
Finally, regarding manual dexterity or range, in total, the preterm group showed worse results than the control group, although with differing samples, average gestation periods, and evaluation tools.
In addition, the degree of prematurity was only considered by Eshaghi et al. (30), who distinguished between extremely preterm infants (average gestational age of 30.60 weeks) and very preterm infants (average gestational age of 34.9 weeks). The age of the sample evaluation comprised 5 and 6 years old, which means the application of BOT-2 as an evaluation tool can be considered adequate although not the gold standard, since this scale should be applied by the age of 4 and a half. However, only 10 extremely preterm infants were evaluated opposite to 21 very preterm infants. Statistically significant results were obtained between both groups with respect to scores for exercises consisting of standing on a straight line with eyes closed for 10 s, and on one leg on a balance beam with eyes closed. This demonstrates that degree of prematurity may be related to postural control. Further studies with a wider sample are needed in this case.
Moreover, it is important to keep in mind that a correct development of postural control depends on a great deal on the vestibulospinal component of vestibular function in early childhood. Vestibulospinal input is important for muscle power regulation, which, in turn, influences postural control. Even though, de Graaf et al. (38), in their study they focused on vestibular function during the first year of life in 67 infants with a very short gestational age (25–27 weeks) At the age of 3 months, 20 infants performed optimally on all items testing vestibular function, increasing to 40 at 6 months and 48 at 12 months. This significant improvement (also seen in muscle power regulation) was primarily caused by better head control (during the traction response and prone position), whereas less shoulder retraction and hyperextension were found in the sitting position. Vestibular function was significantly related to brain ultrasonography classification but not to gestational age, birthweight, the Neonatal Medical Index, or gender. It should be noted that, the developing nervous system has a great potential for plasticity. Functional and anatomic evidence demonstrates that spontaneous plasticity can be potentiated by activity and specific experimental manipulation. Particular attention should be paid to early detection from the clinical continuum of detection, diagnosis, prognosis, and intervention to improve developmental outcome. Therefore, one of the future lines of research that has not been included in this work would be the relationship between the vestibular system, the development of motor control and children born preterm.
One of the limitations of this bibliographic review is that only one of the articles described blinded methodology, as observational type studies do not normally carry out randomization processes and use limited size samples.
Moreover, only one study checked for the correlation between degree of prematurity and postural control, and a few studies measured long-term postural control, which allows to confirm the evolution of postural control differences through the years.
Conclusions
In conclusion, all the studies that we found, demonstrated that the preterm infants group had worse postural control than the full-term infants group, with only one study indicating more limited postural control with higher prematurity. As for the methodological quality, all the studies exceeded a score of 7 according to the critical reading programme CASPe, which considers studies to have adequate methodological quality when they exceed half of the total score.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
IT-D: Designed the study. Participated in the research, and drafted the manuscript. AC-D: Participated in the operation and drafted the manuscript. FM-R: Participated in the operation and drafted the manuscript. RJ-V: Participated in the operation and drafted the manuscript. RRDV-H: Participated in the operation and revised the article. IS-A: Participated in the operation and revised the article. JLS-G: Participated in the operation and drafted the manuscript. MCT: Supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Howson C, Kinney M, McDougall L, Lawn J. Born too soon: preterm birth matters. Reprod Health. (2013) 10(S1). doi: 10.1186/1742-4755-10-S1-S1
2. Blencowe H, Cousens S, Chou D, Oestergaard M, Say L, Moller A. Born too soon: the global epidemiology of 15 million preterm births. Reprod Health. (2013) 10(Suppl 1):S2. doi: 10.1186/1742-4755-10-S1-S2
3. Guilherme R, Gaspardo C, Cordaro G, Martinez F, Martins M. Impact of neonatal risk and temperament on behavioral problems in toddlers born preterm. Early Hum Dev. (2016) 103:175–81. doi: 10.1016/j.earlhumdev.2016.09.015
4. Majewska J, Zajkiewicz K, Wacław-Abdul K, Baran J, Szymczyk D. Neuromotor development of children aged 6 and 7 years born before the 30th week gestation. Biomed Res Int. (2018) 2018:1–12. doi: 10.1155/2018/2820932
5. Synnes A, Anderson P, Grunau R, Dewey D, Moddemann D, Tin W. Predicting severe motor impairment in preterm children at age 5 years. Arch Dis Child. (2015) 100(8):748–53. doi: 10.1136/archdischild-2014-307695
6. Frawley G. Special considerations in the premature and ex-premature infant. Anaesth Intens Care. (2017) 18(2):79–83. doi: 10.1016/j.mpaic.2016.11.001
7. Rebage Moisés V, Ruiz Escusol S, Fernández Vallejo M, Montejo Gañán A, García Íñiguez J, Galve Pradel Z. Neurological newborn in our centre and follow-up. Rev Neurol. (2008) 47(S01):S001. doi: 10.33588/rn.47S01.2008344
8. Crump C, Winkleby M, Sundquist J, Sundquist K. Prevalence of survival without Major comorbidities among adults born prematurely. JAMA. (2019) 322(16):1580. doi: 10.1001/jama.2019.15040
9. Wright C. Predicting survival without disability after preterm birth: some things we know, some things we should know more about. J Pediatr. (2019) 215:1–3. doi: 10.1016/j.jpeds.2019.10.031
10. Patel R. Short- and long-term outcomes for extremely preterm infants. Am J Perinatol. (2016) 33(03):318–28. doi: 10.1055/s-0035-1571202
11. Pollock AS, Durward BR, Rowe PJ, Paul JP. What is balance? Clin Rehabil. (2000) 14(4):402–6. doi: 10.1191/0269215500cr342oa
12. Duclos N, Duclos C, Mesure S. Control postural: fisiología, conceptos principales e implicaciones para la readaptación. EMC Med. (2017) 38(2):1–9. doi: 10.1016/S1293-2965(17)83662-8
13. Hsu Y, Kuan C, Young Y. Assessing the development of balance function in children using stabilometry. Int J Pediatr Otorhinolaryngol. (2009) 73(5):737–40. doi: 10.1016/j.ijporl.2009.01.016
14. Ivanenko Y, Gurfinkel V. Human postural control. Front Neuroscien. (2018) 12:171. doi: 10.3389/fnins.2018.00171
15. Fong S, Tsang W, Ng G. Altered postural control strategies and sensory organization in children with developmental coordination disorder. Hum Mov Sci. (2012) 31(5):1317–27. doi: 10.1016/j.humov.2011.11.003
16. Dusing SC, Harbourne RT. Variability in postural control during infancy: implications for development, assessment, and intervention. Phys Ther. (2010) 90(12):1838–49. doi: 10.2522/ptj.2010033
17. Hutton B, Catala-Lopez F, Moher D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: pRISMA-NMA. Med Clin (Barc). (2016) 147:262–6. doi: 10.1016/j.medcli.2016.02.025
18. Pin T, Butler P, Cheung H, Shum S. Longitudinal development of segmental trunk control in full term and preterm infants- a pilot study: part II. Dev Neurorehabil. (2019) 23(3):193–200. doi: 10.1080/17518423.2019.1629661
19. Righetto Greco A, Sato N, Cazotti A, Tudella E. Is segmental trunk control related to gross motor performance in healthy preterm and full-term infants? J Mot Behav. (2020) 52(6):666–75. doi: 10.1080/00222895.2019.1673694
20. Valentini N, Pereira K, Chiquetti E, Formiga C, Linhares M. Motor trajectories of preterm and full-term infants in the first year of life. Pediatr Int. (2019) 61(10):967–77. doi: 10.1111/ped.13963
21. Pin T, Butler P, Cheung H, Shum S. Segmental assessment of trunk control in infants from 4 to 9 months of age- a psychometric study. BMC Pediatr. (2018) 18(1):182. doi: 10.1186/s12887-018-1153-4
22. Sato N, Tudella E. Influence of sitting positions and level of trunk control during reaching movements in late preterm and full-term infants. Front Pediatr. (2018) 6:185. doi: 10.3389/fped.2018.00185
23. Bucci M, Tringali M, Trousson C, Husson I, Baud O, Biran V. Spatial and temporal postural analysis in children born prematurely. Gait Posture. (2017) 57:230–35. doi: 10.1016/j.gaitpost.2017.06.023
24. Dziuba E, Drzał-Grabiec J, Truszczyńska-Baszak A, Guzek K, Zajkiewicz K. Balance in children born prematurely currently aged 6–7. Biomed Hum Kinetics. (2017) 9(1):181–86. doi: 10.1515/bhk-2017-0025
25. Rodríguez C, Mata D, Rodríguez LM, Regueras L, Reguera MM, de Paz JA. Evaluation of coordination and balance in preterm children. An Pediatr (Barc. (2016) 85(2):86–94. doi: 10.1016/j.anpedi.2015.10.009
26. Silva J, Sargi A, Andrade I, Araújo C, Antonio T. Motor development of preterm and term infants in the fundamental movement phase: a cross-sectional study. Fisioter Mov. (2016) 29(3):581–88. doi: 10.1590/1980-5918.029.003.AO16
27. Petersen H, Tulinius A, Georgsdóttir I, Einarsson E, Patel M, Haraldsson Á. Decreased postural control in adolescents born with extremely low birth weight. Exp Brain Res. (2015) 233(5):1651–62. doi: 10.1007/s00221-015-4239-3
28. Bucci M, Wiener-Vacher S, Trousson C, Baud O, Biran V. Subjective visual vertical and postural capability in children born prematurely. Plos One. (2015) 10(3):e0121616. doi: 10.1371/journal.pone.0121616
29. Cabral T, Pereira da Silva L, Tudella E, Simões Martinez C. Motor development and sensory processing: a comparative study between preterm and term infants. Res Dev Disabil. (2015) 36:102–07. doi: 10.1016/j.ridd.2014.09.018
30. Eshaghi Z, Jafari Z, Jalaie S. Static balance function in children with a history of preterm birth. Med J Islam Republic of Iran. (2015) 29(1):1278–86. PMID: 26913273; PMCID: PMC4764290
31. Lorefice L, Galea M, Clark R, Doyle L, Anderson P, Spittle A. Postural control at 4 years in very preterm children compared with term-born peers. Dev Med Child Neurol. (2014) 57(2):175–80. doi: 10.1111/dmcn.12550
32. Dusing S, Izzo T, Thacker L, Galloway J. Postural complexity differs between infant born full term and preterm during the development of early behaviors. Early Hum Dev. (2014) 90(3):149–56. doi: 10.1016/j.earlhumdev.2014.01.006
33. Wang T, Howe T, Hinojosa J, Hsu Y. Postural control of pre-term infants at 6 and 12months corrected age. Early Hum Dev. (2010) 86(7):433–37. doi: 10.1016/j.earlhumdev.2010.05.022
34. Volpi S, Rugolo L, Pera J, Corrente J. Acquisition of motor abilities up to independent walking in very low birth weight preterm infants. J Pediatr. (2010) 86(2):143–48. doi: 10.2223/JPED.1989
35. Butler P, Saavedra S, Sofranac M, Jarvis S, Woollacott M. Refinement, reliability, and validity of the segmental assessment of trunk control. Paediatric Physical Therapy. (2010) 22(3):246–57. doi: 10.1097/PEP.0b013e3181e69490
36. Pin T, de Valle K, Eldridge B, Galea M. Clinimetric properties of the Alberta infant motor scale in infants born preterm. Paediatric Physical Therapy. (2010) 22(3):278–86. doi: 10.1097/PEP.0b013e3181e94481
37. Visser J, Carpenter M, van der Kooij H, Bloem B. The clinical utility of posturography. Clin Neurophysiol. (2008) 119(11):2424–36. doi: 10.1016/j.clinph.2008.07.220
Keywords: postural control, gestational age, children, gestational age (GA), preterm
Citation: Tuñón-Domínguez I, Cuesta-Gómez A, Molina-Rueda F, Juárez-Vela R, Ruiz de Viñaspre-Hernández R, Santolalla-Arnedo I, Sánchez-González JL and Carratalá-Tejada M (2022) The influence between gestational age and postural control, a systematic review. Front. Pediatr. 10:883218. doi: 10.3389/fped.2022.883218
Received: 24 February 2022; Accepted: 27 October 2022;
Published: 15 November 2022.
Edited by:
Domenico Romeo, Fondazione Policlinico Gemelli, IRCCS, ItalyReviewed by:
Andrzej Myśliwiec, Academy of Physical Education in Katowice, PolandEugen Constant Ionescu, Hospices Civils de Lyon, France
© 2022 Tuñón-Domínguez, Cuesta-Gómez, Molina-Rueda, Juárez-Vela, Ruiz de Viñaspre-Hernández, Santolalla-Arnedo, Sánchez-González and Carratalá-Tejada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Regina Ruiz de Viñaspre-Hernández cmVydWl6ZGVAdW5pcmlvamEuZXM=
Specialty Section: This article was submitted to Children and Health, a section of the journal Frontiers in Pediatrics