 Vito Pavone1*
Vito Pavone1* Marco Sapienza1
Marco Sapienza1 Andrea Vescio1
Andrea Vescio1 Alessia Caldaci1
Alessia Caldaci1 Kathryn Louise McCracken2
Kathryn Louise McCracken2 Federico Canavese2
Federico Canavese2 Gianluca Testa1
Gianluca Testa1- 1Department of General Surgery and Medical Surgical Specialties, Section of Orthopaedics and Traumatology, P.O. “Policlinico Gaspare Rodolico”, University of Catania, Catania, Italy
- 2Department of Pediatric Orthopedic Surgery, Jeanne de Flandre Hospital, Lille University Centre, Lille, France
Background: Idiopathic clubfoot, also referred to as congenital talipes equinovarus (CTEV), is one of the most common lower limb deformities observed in newborns, leading to significant functional impairment if untreated. The aims of this study were to (1) assess the developmental milestones in patients with CTEV treated by the Ponseti technique, and to compare them to the unaffected controls; (2) evaluate the possible correlation between developmental milestones, severity of the deformity, and number of casts.
Materials and methods: Seventy-nine subjects were divided into two groups, CTEV group (43 patients; 72 feet) and control group (36 patients). Age, sex, affected side, attainment of babbles (BAL), independent gait (IG), and combined word (CW) were recorded for all patients. In patients with CTEV, Pirani Score (PRS), number of casts (NC), and clinical outcome were collected according to the Clubfoot Assessment Protocol (CAP), The American Orthopedic Foot and Ankle Score (AOFAS), and Foot and Ankle Disability Index (FADI).
Results: IG was achieved later later than the unaffected controls by 12/43 patients (27.9%) with CTEV and 3/36 patients in the control group (8.3%) (p = 0.04) and in a mean time of 16.8 ± 3.5 months and 13.2 ± 2.7 months, respectively (p = 0.001). In the CTEV group the mean value of CAP was 98.6 ± 4.7, of AOFAS of 98.4 ± 4.4 and of FADI equal to 99.9 ± 0.44. There were no statistically significant differences for BAL and CW; and no correlation with PRS, NC, or clinical score were identified.
Conclusion: CTEV patients managed by the Ponseti technique achieve independent gait later than the unaffected controls, although they do so within the age limit of developmental. On the other hand, the Ponseti treatment has no impact on attainment of language development.
Introduction
Idiopathic clubfoot, also referred to as congenital talipes equinovarus (CTEV), is one of the most common lower limb deformities observed in newborns, leading to significant functional impairment if untreated (1, 2). Untreated or neglected CTEV may cause substantial disability due to foot deformity, pain, stiffness, and subsequent gait disturbance (1, 3, 4). Although multiple treatment options are available (5, 6), the Ponseti technique has become the most widely accepted protocol to treat CTEV during infancy. The technique is based on the application of an above-the-knee cast which corrects the foot gently and gradually; the cast is renewed every 5–7 days until the foot reaches between 40° and 50° of abduction in the transverse plane. At the end of cast treatment, up to 95% of patients require a percutaneous Achilles’ tenotomy in order to correct the residual equinus. This can be done either under general or local anesthesia. Following Achille’s tenotomy the foot is casted for an additional 2–3 weeks. Subsequently, the patients wear a foot abduction orthosis (FAO) to hold the foot in external rotation and dorsiflexion for 23 hours/day during the first 3–4 months, and then at night and during nap time until age 5 years (7–10). Several studies have reported patients with CTEV treated by the Ponseti technique with long-term outcomes (7, 10). In addition, more recent research studies have shown that patients treated by the Ponseti technique can achieve superior sports performance compared to patients managed by other techniques (8, 11). Moreover, in the comparison between male and female patients with uni- or bilateral CTEV involvement, functional results and similar sports performance were reported (11).
Overall, the Ponseti technique aims to achieve a pain-free supple and plantigrade foot with minimal surgery. However, there is a paucity of research investigating the gross motor skills (GMS) in children with CTEV managed by Ponseti technique (12, 13).
The aims of this study were to (1) assess the developmental milestones in patients with CTEV treated by the Ponseti technique, and to compare them to unaffected control; (2) evaluate the possible correlation between developmental milestones, severity of the deformity, and number of casts. The study hypotheses were the following: (a) the Ponseti treatment can delay early GMS but not linguistic skills compared to the normal population; (b) severity of the deformity and number of casts are not correlated to developmental milestones.
Materials and methods
Study design
The trial was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies (14). This prospective cross-sectional study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board A.O.U. Policlinico “G. Rodolico-San Marco” of Catania (protocol code 117/2020/PO, October 14, 2020).
Sample eligibility criteria
Between January 2010 and June 2021, 104 patients were managed according to the Ponseti protocol at our institution.
The inclusion criteria were as follows: (1) a diagnosis of idiopathic CTEV at birth managed by Ponseti technique; (2) complete clinical data; (3) follow-up data spanning more than 2 years.
Exclusion criteria were positional clubfoot, non-idiopathic CTEV, prior failed treatment, initial treatment at other Institutions, and clinical follow up of less than 2 years. A total of 43 of 104 patients (41.3%; 77 girls and 100 boys) met the inclusion criteria; the remaining 61 patients (59.7%) were excluded (Figure 1).
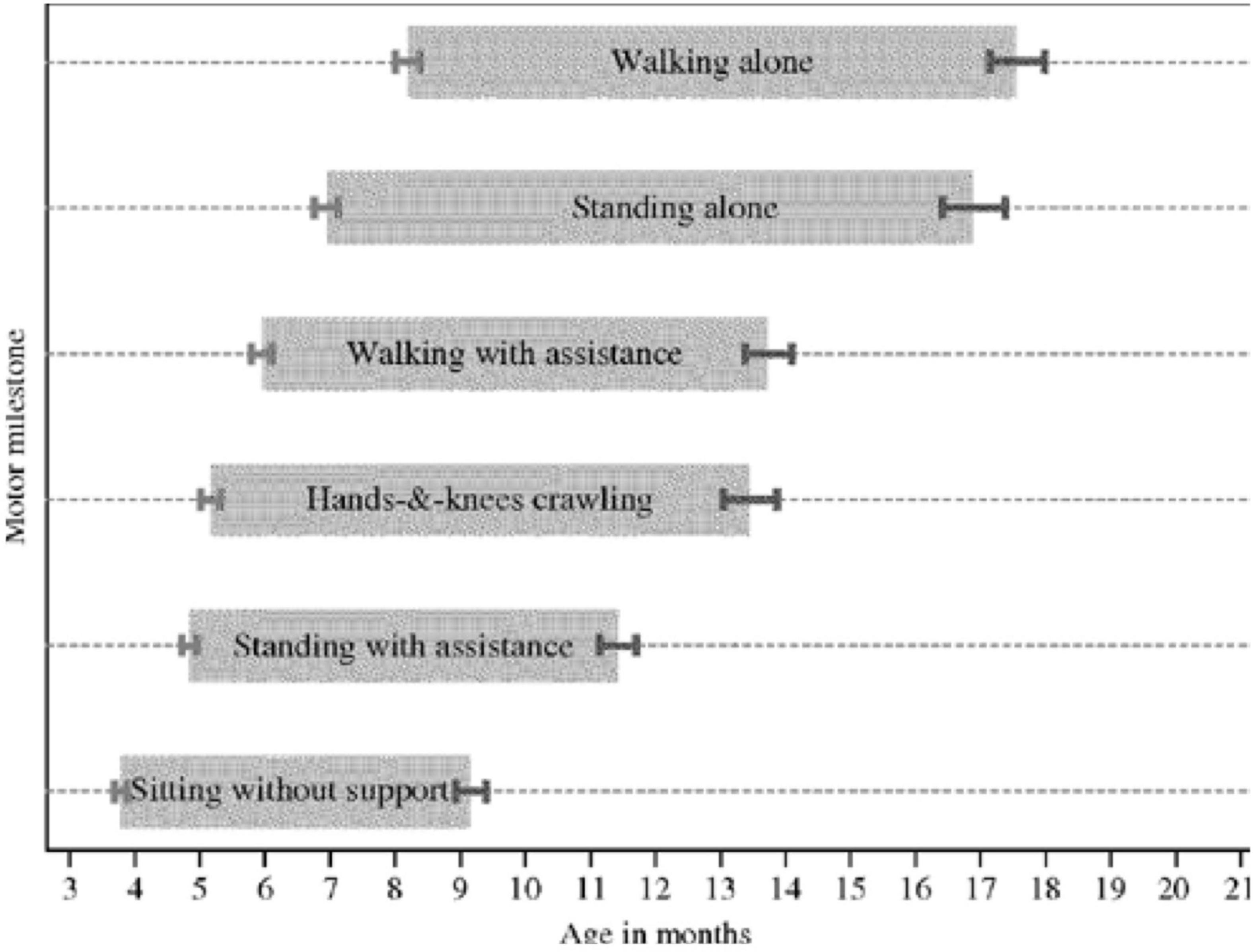
Figure 1. Study flow-chart.
Additional information such as severity of the deformity according to the Pirani classification system (PRS), number of casts (NC), and the need of Achille’s tenotomy were retrieved from the charts (Table 1).
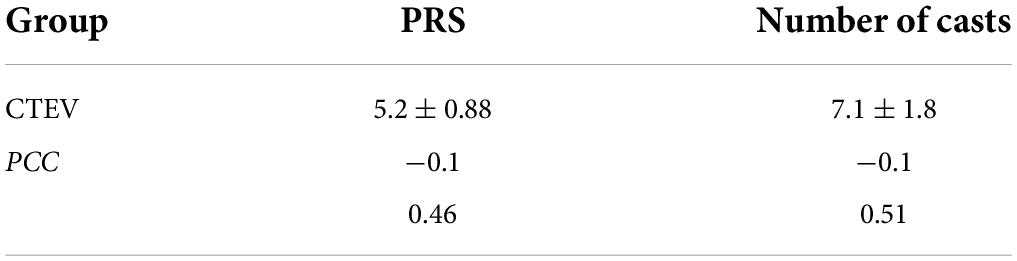
Table 1. Mean PRS and NC.
Thirty-six unaffected children of similar age without CTEV or any other musculoskeletal disorder were included in the study as control group.
All guardians provided an informed consent to have their child participate in the present investigation.
Treatment protocol and follow-up
All patients were treated according to the Ponseti technique and its principles (15). Long-leg cast was changed every 5–7 days, and 7 casts/patient were applied on average (range, 3–11); 43 out of 43 patients (100%) underwent percutaneous Achilles tenotomy under general anesthesia. FAO was prescribed until 5 years of age (15). Clinical follow up was performed every 6 months until 6 years of age and one a year thereafter.
Primary outcome: Developmental milestones
Gross motion milestone assessment
Gross motor skills were investigated at each follow-up, since the patient was 4–5 months of age. Illustrations and demonstrations were provided to clarify the GMS when needed. The age of milestone achievement to the nearest month and the number of interviews per parent were recorded. In particular, as soon as the patient was able to do 10 consecutive steps without support, they were considered to have acquired IG.
The windows of achievement for six gross motor development milestones (Figure 2) described by the World Health Organization (WHO) Multicenter Growth Reference Study Group were chosen to identify the proper cut-off limits (16).

Figure 2. WHO motor development study: windows of achievement for six gross motor development milestones.
Speech milestone assessment
Speech and language developmental milestones are noted in Table 2 and were investigated at each follow-up visit, since the patient was 4–5 months of age (Table 2). In particular, guardians were asked when their child achieved babbles (says “mama” or “papa”) and started to combine words.
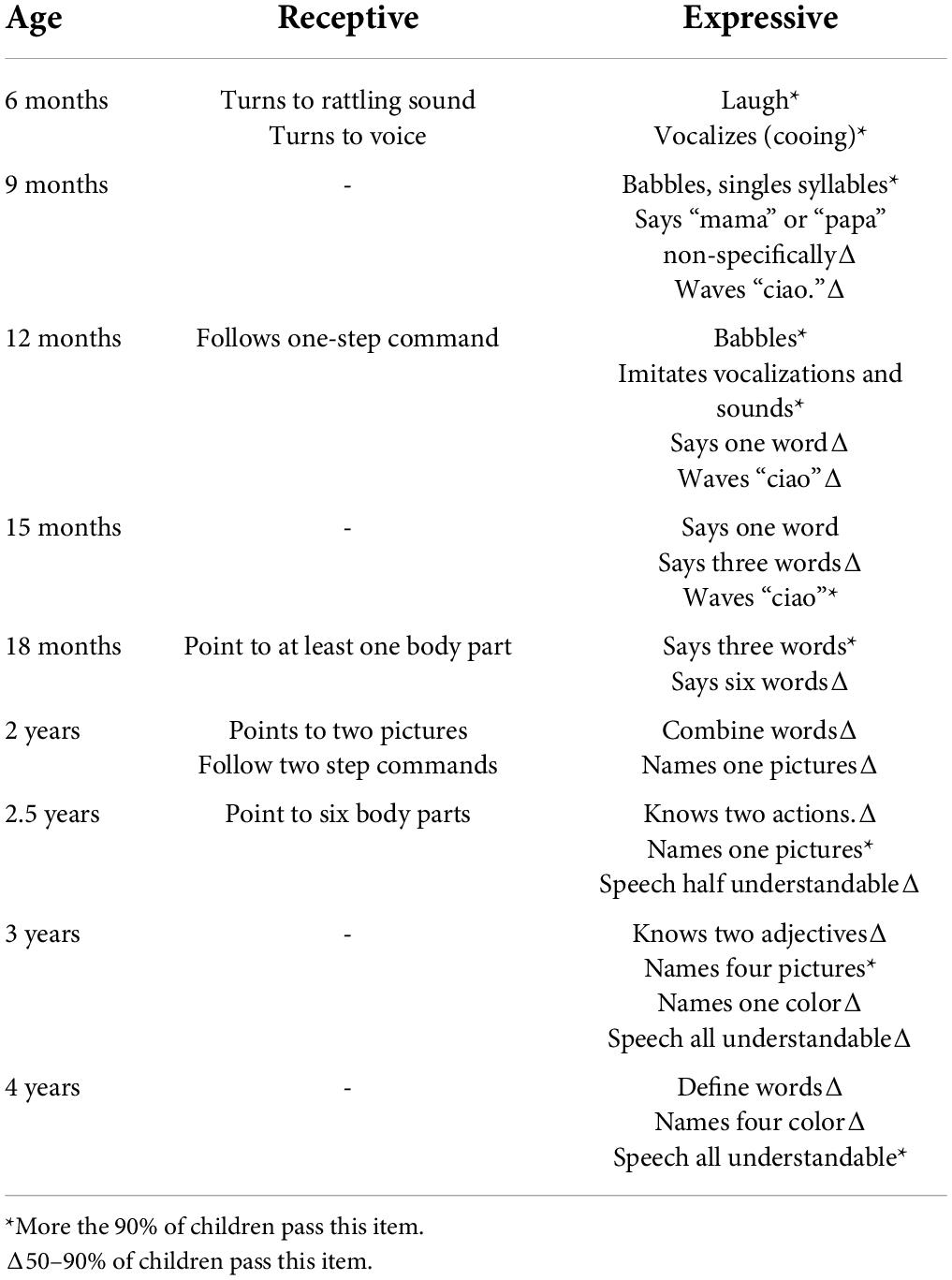
Table 2. Developmental milestones for speech and language in children.
Secondary outcome: Congenital talipes equinovarus severity, number of casts, and clinical assessments
The severity of the clubfoot was assessed according to PRS by a senior pediatric orthopedic surgeon at the first clinical examination. The number of casts was retrieved from medical charts. Clinical and functional outcomes of all patients were evaluated in patients with at least 2 years of follow-up, using the Clubfoot Assessment Protocol (CAP) (17), the American Orthopedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot score (18), the Foot and Ankle Disability Index (FADI) (19). The PRS, CAP, AOFAS, FADI scores in patients with bilateral involvement are the mean between the CTEV.
Pirani score
The PRS includes the presence and the severity of six items: medial crease (MC-PRS), lateral part of the head of talus, curvature of the lateral border, posterior crease, empty heel, and rigid equinus. Each of the six items is scored on a three-point scale (0 = none, 0.5 = moderate, 1 = severe abnormality). The total score ranges from 0 to 6 based on the severity of the deformity (20).
Clubfoot assessment protocol
The CAP contains 22 items in four sub-groups: mobility (8 items), muscle function (3 items), morphology (4 items), and motion quality I and II (7 items). The first three sub-groups relate to body function/structures and the last relates to activity. These groups include standardized questions about pain, stiffness, and daily activity/sport participation. The scoring is divided systematically and proportionally with respect to normal variation and its supposed impact on perceived physical function ranging from 0 (severe reduction/no capacity) to 4 (normal). Score grading varies from 3 to 5 levels. For each subgroup, the sum of the item scores are calculated and visualized as profiles (converted to a 0–100 scale score, with 0 = extremely deviant and 100 within normal variance; sub-group transformation score = actual score/maximal possible score × 100) (17).
American orthopedic foot and ankle society Ankle–Hindfoot
The AOFAS Ankle-Hindfoot score consists of nine items under three different categories, i.e., pain (40 points), functional aspect (50 points), and alignment (10 points), totaling 100 points. Items on pain and functional limitation are answered by the patient, while the alignment items are answered by an examiner (18).
The foot and ankle disability index
Foot and ankle disability index is a region-specific self-reporting scale of function that includes 34 items divided into two subscales, the first (FADI) consisting of 26 items concerning activities of daily living (ADL) and pain, and the second (FADI Sport) consisting of eight items concerning sports activities. Each item is scored on a five-point Likert scale (0–4) and, thereafter, the results are converted into percentages. Higher scores represent higher levels of function for each subscale. The ADL and Sport subscales are scored separately (21).
Statistical analysis
Continuous data are presented as means and standard deviations, as appropriate. The student’s t-test was used to evaluate the mean and standard deviation between groups. The Chi-square test was used to verify the homogeneity of the group and to compare number of patients who achieved the milestone before and after the upper limit milestones. The selected threshold for statistical significance was p < 0.05. The Pearson Correlation Coefficient (PCC) was utilized to assess the correlation between the walking alone milestone and PirS or number of casts. The PCC is a value between −1 and 1, where values close to −1 indicate high negative correlation, values close to 1 indicate high positive correlation, and values close to 0 indicate no or very week correlation. The correlation coefficient is rated according to Colton (22):
• 0 to 0.25 (0 to −0.25) little or no relationship;
• 0.25 to 0.50 (−0.25 to −0.50) fair degree of relationship;
• 0.50 to 0.75 (−0.50 to −0.75) moderate to good relationship;
• 0.75 to 1.00 (−0.75 to −1.00) very good to excellent relationship.
All statistical analyses were performed using IBM SPSS, Version 24.0 (IBM Corp., Armonk, NY, United States).
Results
Sample
The overall cohort of patients consisted of 42 males (53.2%) and 37 females (46.8%) with a mean age of 8.4 ± 3.9 years (range, 2–17).
Forty-three children (74 feet) were treated with the Ponseti technique and composed the CTEV group [27 males and 16 females; mean age 7.8 ± 3.6 years (2–14); mean follow-up 9.3 ± 5.7 years (0–14)], while 36 unaffected children composed the control group [15 males and 21 females; mean age 9.1 ± 4.7 (2–17); mean follow-up 6.8 ± 8.7 (0–16)] (Table 3). The mean age of the two groups were comparable (p > 0.05).

Table 3. Demographics.
Developmental milestones
Statistically significant differences were found regarding the number of patients achieving independent gait after the age of 18 months according to the WHO Multicenter Growth Reference Study Group Cut-off: CTEV Group (12/43 patients; 27.9%) vs. control group (3/36 patients; 8.3%) (p = 0.04) (Figures 3A,B) as well as in the average number of months required to achieve independent gait: CTEV Group: 16.8 ± 3.5 months vs. control Group: 13.2 ± 2.7 months (p = 0.0001) (Table 4 and Figure 4).
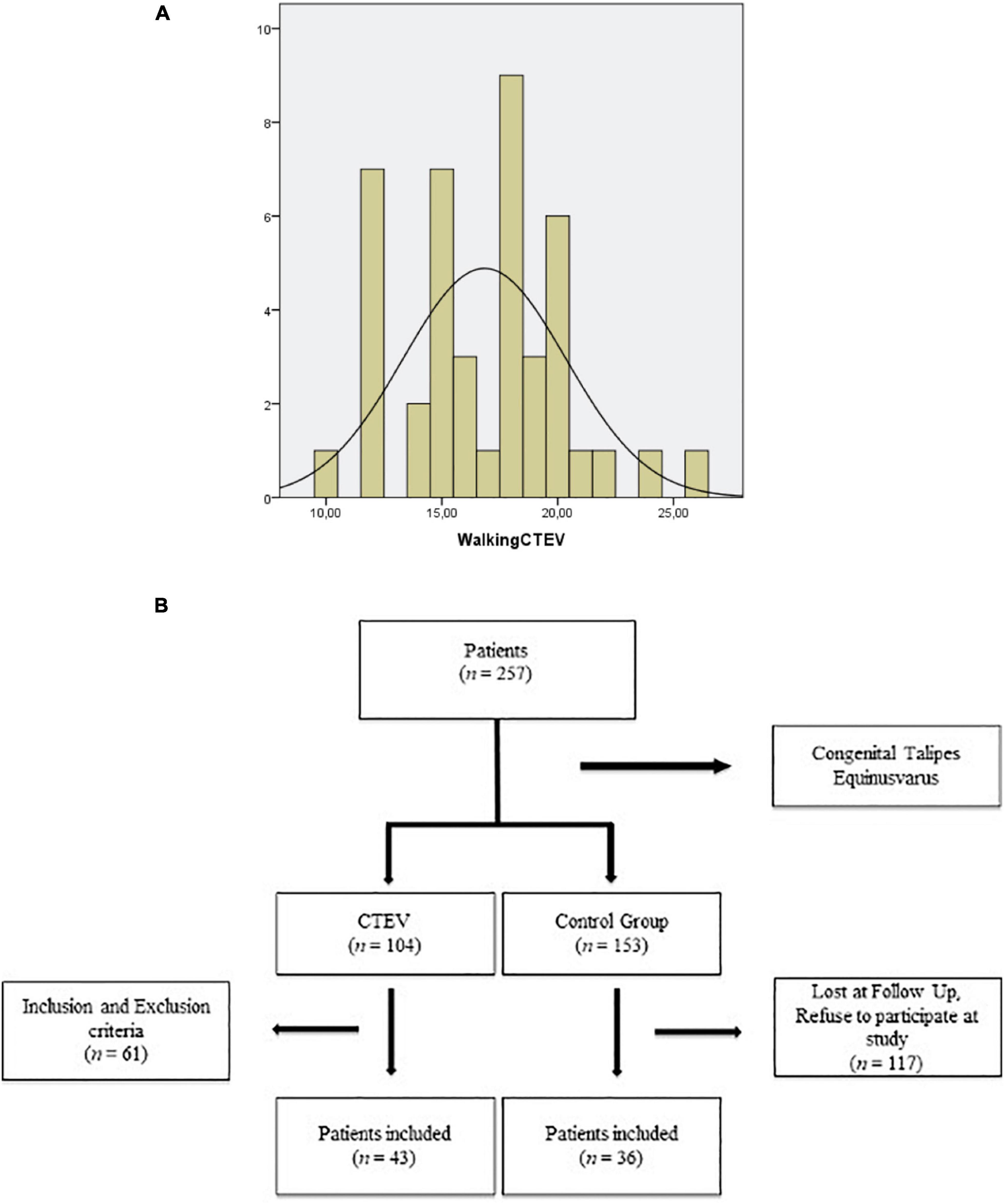
Figure 3. (A) Distribution of patients with CTEV achieving IG. (B) Distribution of unaffected patients achieving IG.

Table 4. Developmental milestones.
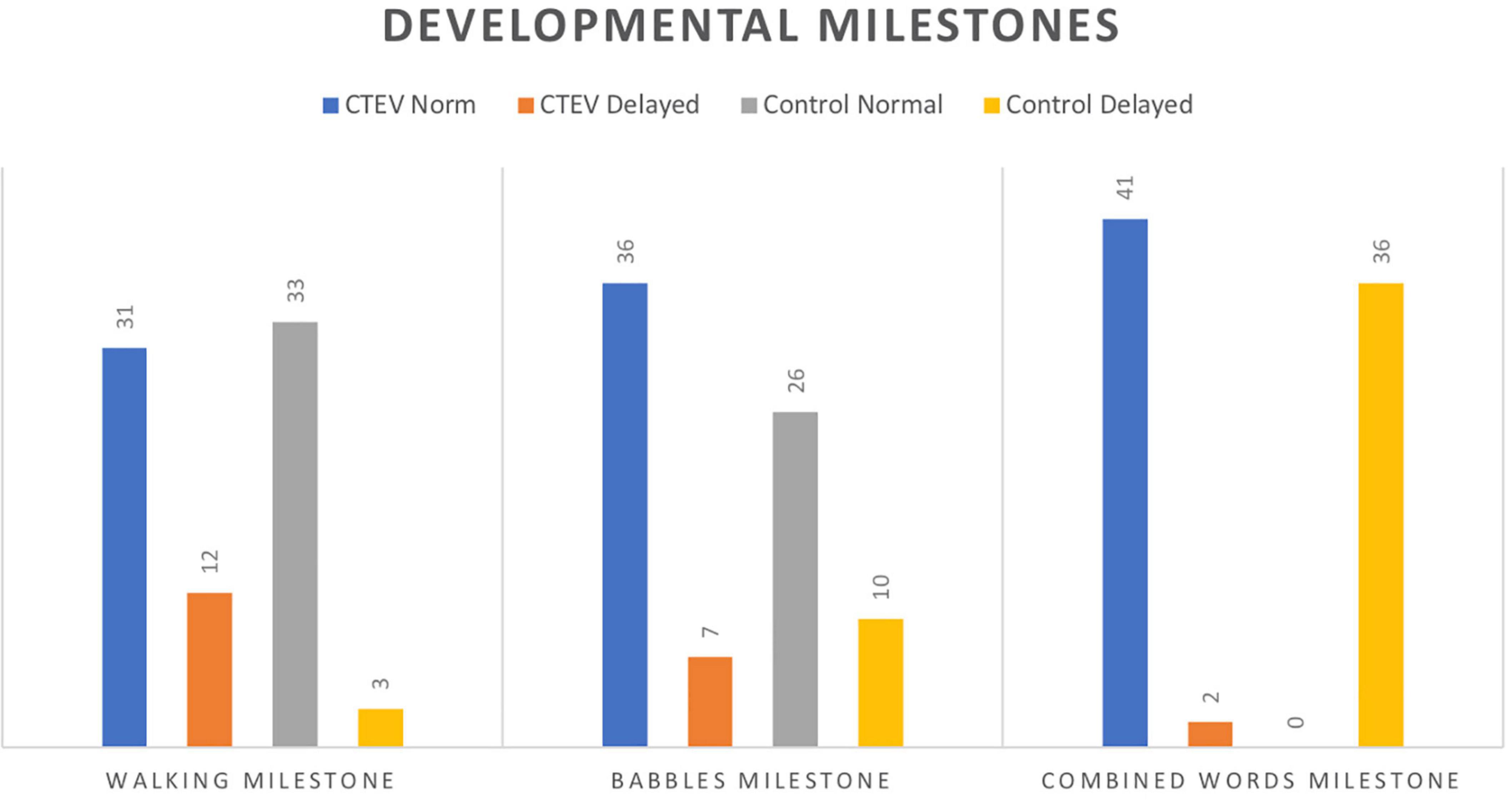
Figure 4. Developmental milestones.
Speech and language developmental milestones (babbles) were achieved by 7/43 patients of CTEV group (16.3%) and by 10/36 patients in control group (27.8%) (p = 0.3), after the age of 10 months, with no statistical differences for the mean time needed to achieve the milestone: CTEV Group: 7.7 ± 2.0 months vs. control Group: 8.3 ± 2.1 months (p = 0.2).
Comparable number of patients did not achieve the “combine words” stage by the age of 24 months. In particular, 2/43 (4.7%) patients in CTEV group vs. 0/36 patients in control group (p = 0.5). Similarly, the average number of months needed to reach the “combined words” stage [CTEV Group (18.9 ± 4.5 months) vs. control group (18.5 ± 5.2 months); p = 0.71] was comparable (Table 4).
Secondary outcome
Clubfoot severity according to Pirani Score
The mean PRS of affected children was 5.2 ± 0.88. The PCC between the two groups for the number of months required to reach independent walking and PRS was not statistically significant (PCC = –0.1; p = 0.46) (Figure 5 and Table 5).
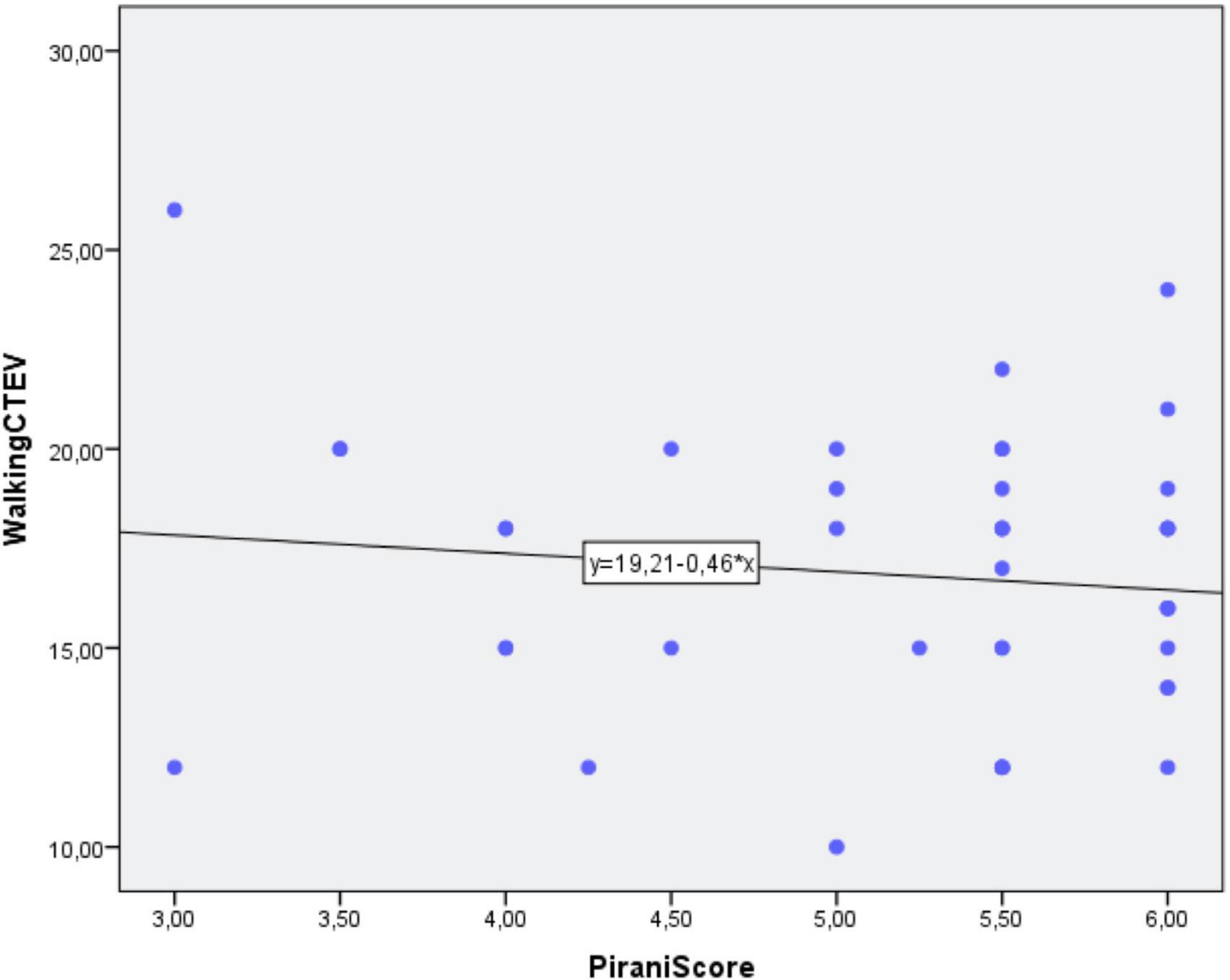
Figure 5. Correlation between independent gait and Pirani score.
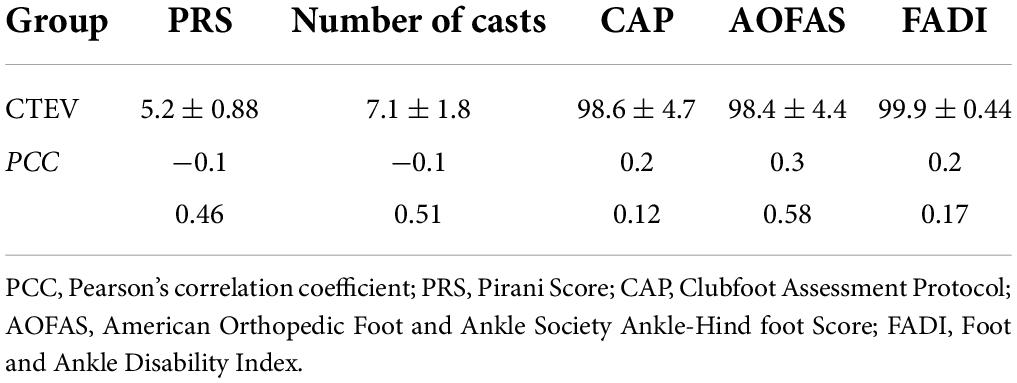
Table 5. Correlation between CTEV severity, number of casts, and outcome.
Number of casts
The mean number of casts was 7.1 ± 1.8 (range, 3–11). The PCC between the two groups for the number of months needed to reach the independent gait stage and number of casts was not statistically significant (PCC = −0.1; p = 0.51) (Figure 6 and Table 5).
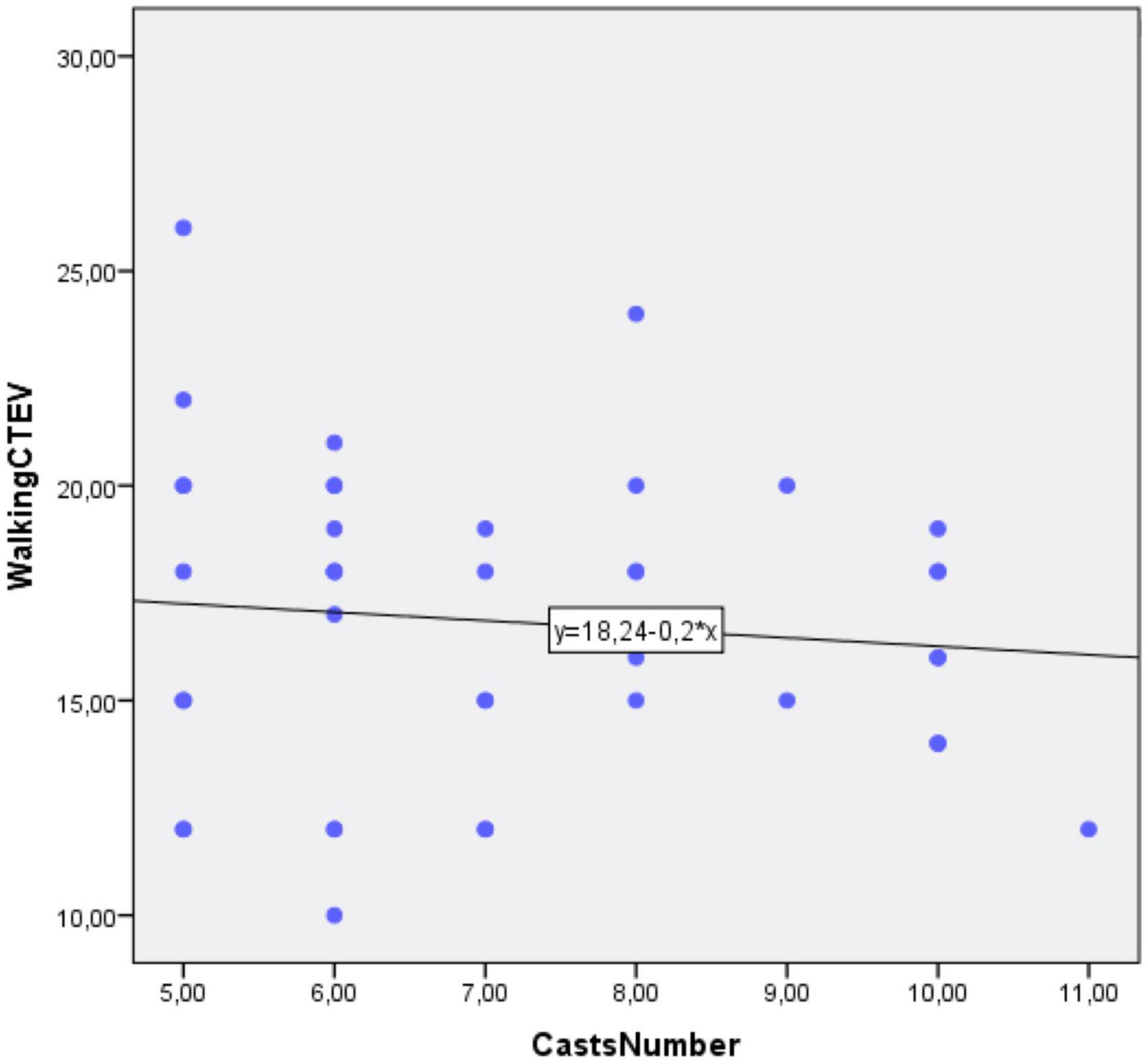
Figure 6. Correlation between independent gait and Number of Casts.
Clinical assessments: Clubfoot assessment protocol, the American orthopedic foot and ankle score, and foot and ankle disability index score
The mean CAP was 98.6 ± 4.7. The PCC between the two groups for the number of months needed to reach independent gait and CAP was not statistically significant (PCC = 0.2; p = 0.12) (Figure 7A).
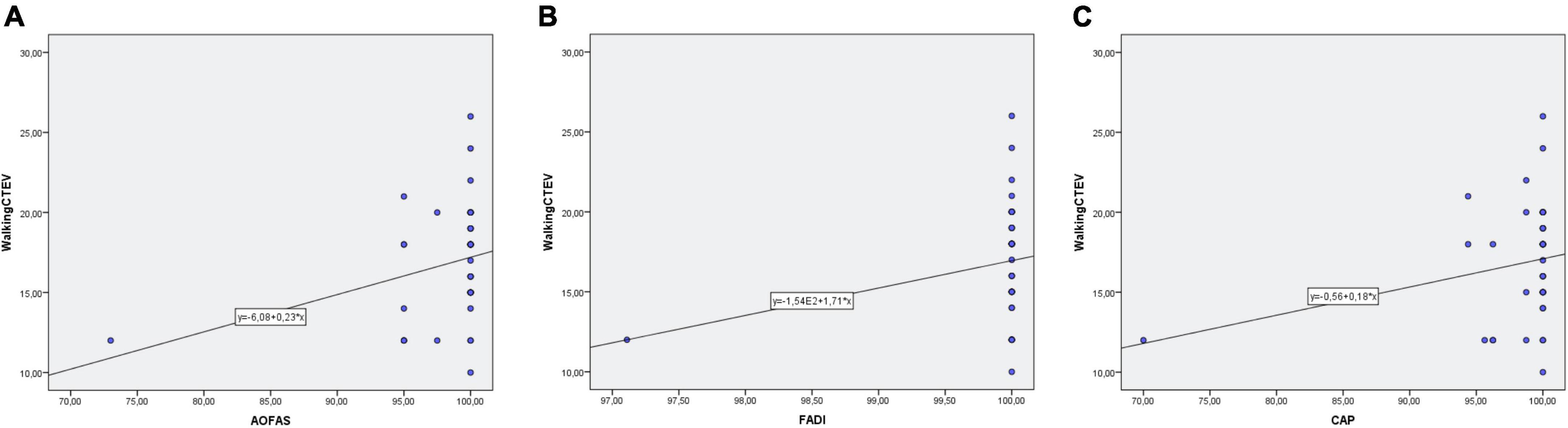
Figure 7. (A) Correlation between independent gait and CAP Score. (B) Correlation between independent gait and AOFAS. (C) Correlation between independent gait and FADI Score.
Mean AOFAS recorded was 98.6 ± 4.7. The PCC between the two groups for the number of months needed to reach independent gait and CAP was not statistically significant (PCC = 0.3; p = 0.58) (Figure 7B).
The mean FADI recorded was 98.6 ± 4.7. The PCC between the two groups for the number of months needed to reach independent gait and CAP was not statistically significant (PCC = 0.2; p = 0.17) (Figure 7C).
Discussion
This study found that patients with CTEV treated according to the Ponseti technique, tend to acquire independent gait later (3 months) than unaffected children (Figures 3A,B and Table 4).
Sala et al. (23) found the delay for independent gait averaged about 2 months with half of the children walking at 13.8 months and nearly all at 17.7 months of age (23).
Karol et al. (12) reported the majority of children with CTEV evaluated with the Peabody Developmental Gross Motor Scale at age 5 years had average gross motor function. The Peabody Developmental Gross Motor Scale assesses whole body development and motor ability, but does not specifically evaluate the quality of lower limb movements. For example, it merges the ability to stand on one foot and to perform sit-ups in the same domain (12).
Andriesse et al. (24) reported a prevalence of 35% of motor impairments in the children aged 7 years with CTEV using the Movement Assessment Battery for Children (24). Alternatively, Lööf al. (13) reported most children with CTEV had difficulties with toe and heel walking and standing and hopping on one foot when patients were evaluated at age 5 years.
However, such delays in developmental milestones are not expected to have a lasting effect on the child’s development. In fact, most children with CTEV have comparable motor skills and can participate in sports without any problems by 9 years of age, as reported by Hughes et al. (25). Therefore, it is more appropriate to look at the age limit of development, which denotes the age by which all children should have achieved a commonly accepted milestone. For walking, the age limit of development is 18 months (26). In the study by Hughes et al., 93% of children with CTEV achieved ambulation by 18 months (25). Therefore, although affected children may be slightly delayed compared to unaffected individuals (17.7 months vs. 13.8 months in our cohort), they will still achieve motor development milestones well within the age limit of the healthy population (18 months).
The Ponseti Technique implies the use of foot and ankle orthosis (FAO) up to the age of 5 years. Therefore, it is possible that the use of FAO may have a clinical impact on the acquisition of independent gait through persistent immobility. The mild delay observed in children with CTEV is likely to be multifactorial, due to a combination of primary pathological factors, secondary treatment factors, and cultural and behavioral factors. FAO compliance was monitored carefully as patients were always assessed by the same surgeon. It is also important to recognize that compliance with FAO is an important predictor of later recurrence (7). Compliance with FAO is unlikely to have had a clinical impact on other developmental milestones (25). According to our results, the two groups of patients had similar speech and language developmental milestones (babbles and “combined words”).
There were some limitations in the analysis of our results. Parental recall of developmental milestones data may be subject to inaccuracy. However, Majnemer et al. found that at age three there was a greater than 70% correlation between parental recall and walking age (27). Secondly, the number of patients enrolled is relatively low. However, all patients were treated and followed up by the same surgeon according to the same protocol. In addition, the demographics of the two groups of patients were comparable, as well as the length of follow-up (Table 3). Lastly, 86.2% of children included in the study had bilateral clubfoot; this should be considered as an additional statistical bias.
Conclusion
Children with CTEV treated by the Ponseti technique show slight developmental delays in reaching independent gait compared to unaffected children. Despite this, they still achieve the milestone within normal time limits and functional outcome is generally good. On the other hand, Ponseti Treatment has no impact on the attainment of language development. Future prospective, randomized trials with a larger sample size of CTEV patients are now needed to confirm the findings of our study.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
VP, GT, AV, and MS treated the orthopedic aspect. MS and KM contributed to early developmental milestones topic. FC revised the manuscript. All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chen C, Kaushal N, Scher DM, Doyle SM, Blanco JS, Dodwell ER. Clubfoot etiology: a meta-analysis and systematic review of observational and randomized trials. J Pediatr Orthop. (2018) 38:e462–9. doi: 10.1097/BPO.0000000000001191
2. Pavone V, Bianca S, Grosso G, Pavone P, Mistretta A, Longo MR, et al. Congenital talipes equinovarus: an epidemiological study in sicily. Acta Orthop. (2012) 83:294–8. doi: 10.3109/17453674.2012.678797
3. Pavone V, Chisari E, Vescio A, Lucenti L, Sessa G, Testa G. The etiology of idiopathic congenital talipes equinovarus: a systematic review. J Orthop Surg Res. (2018) 13:206. doi: 10.1186/s13018-018-0913-z
4. Leo DG, Russell A, Bridgens A, Perry DC, Eastwood DM, Gelfer Y. Development of a core outcome set for idiopathic clubfoot management: a study protocol. Bone Jt Open. (2021) 2:255–60. doi: 10.1302/2633-1462.24.BJO-2020-0202.R1
5. Dimeglio A, Canavese F. The French functional physical therapy method for the treatment of congenital clubfoot. J Pediatr Orthop B. (2012) 21:28–39. doi: 10.1097/BPB.0b013e32834ee5f8
6. Canavese F, Dimeglio A. Idiopathic clubfoot: past, present and future. Ann Transl Med. (2021) 9:1094. doi: 10.21037/atm-21-2392
7. Pavone V, Testa G, Costarella L, Pavone P, Sessa G. congenital idiopathic talipes equinovarus: an evaluation in infants treated by the ponseti method. Eur Rev Med Pharmacol Sci. (2013) 17:2675–9.
8. Švehlík M, Floh U, Steinwender G, Sperl M, Novak M, Kraus T.. Ponseti method is superior to surgical treatment in clubfoot – long-term, randomized, prospective trial. Gait Posture. (2017) 58:346–51. doi: 10.1016/j.gaitpost.2017.08.010
9. Bina S, Pacey V, Barnes EH, Burns J, Gray K. Interventions for congenital talipes equinovarus (Clubfoot). A cura di cochrane neuromuscular group. Cochrane Database Syst Rev. (2020) 5:CD008602. doi: 10.1002/14651858.CD008602.pub4
10. Abdelgawad AA, Lehman WB, van Bosse HJ, Scher DM, Sala DA. Treatment of idiopathic clubfoot using the ponseti method: minimum 2-year follow-up. J Pediatr Orthop B. (2007) 16:98–105. doi: 10.1097/BPB.0b013e32801048bb
11. Pavone V, Vescio A, Caldaci A, Culmone A, Sapienza M, Rabito M, et al. Sport ability during walking age in clubfoot-affected children after ponseti method: a case-series study. Children. (2021) 8:181. doi: 10.3390/children8030181
12. Karol LA, Jeans KA, Kaipus KA. The relationship between gait, gross motor function, and parental perceived outcome in children with clubfeet. J Pediatr Orthop. (2016) 36:145–51. doi: 10.1097/BPO.0000000000000410
13. Lööf E, Andriesse H, André M, Böhm S, Iversen MD, Broström EW. Gross motor skills in children with idiopathic clubfoot and the association between gross motor skills, foot involvement, gait, and foot motion. J Pediatr Orthop. (2019) 39:359–65. doi: 10.1097/BPO.0000000000000964
14. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. (2014) 12:1495–9. doi: 10.1016/j.ijsu.2014.07.013
15. Ignacio PV. The ponseti technique for correction of congenital clubfoot. J Bone Jt Surg Am. (2002) 84:1889–90. doi: 10.2106/00004623-200210000-00026
16. Who Multicentre Growth Reference Study Group Onis. WHO motor development study: windows of achievement for six gross motor development milestones. Acta Paediatr. (2007) 95:86–95. doi: 10.1111/j.1651-2227.2006.tb02379.x
17. Andriesse H, Hägglund G, Jarnlo GB. The clubfoot assessment protocol (CAP); description and reliability of a structured multi-level instrument for follow-up. BMC Musculoskelet Disord. (2005) 6:40. doi: 10.1186/1471-2474-6-40
18. Leigheb M, Janicka P, Andorno S, Marcuzzi A, Magnani C, Grassi F. Italian translation, cultural adaptation and validation of the “American orthopaedic foot and ankle society’s (AOFAS) ankle-hindfoot scale”. Acta Bio Med Atenei Parmensis. (2016) 87:38–45.
19. Martin RL, Burdett RG, Irrgang JJ. Development of the foot and ankle disability index (FADI). J Orthop Sports Phys Ther. (2005) 29:A32–3.
20. Flynn JM, Donohoe M, Mackenzie WG. An independent assessment of two clubfoot-classification systems. J Pediatr Orthop. (1998) 18:323–7.
21. Leigheb M, Rava E, Vaiuso D, Samaila EM, Pogliacomi F, Bosetti M, et al. Translation, cross-cultural adaptation, reliability, and validation of the Italian version of the foot and ankle disability index (FADI). Acta Bio Med Atenei Parmensis. (2020) 91:160–6. doi: 10.23750/abm.v91i4-S.9544
23. Sala DA, Chu A, Lehman WB, van Bosse HJ. Achievement of gross motor milestones in children with idiopathic clubfoot treated with the ponseti method. J Pediatr Orthop. (2013) 33:55–8. doi: 10.1097/BPO.0b013e3182670361
24. Andriesse H, Westbom L, Hägglund G. Motor ability in children treated for idiopathic clubfoot. A controlled pilot study. BMC Pediatr. (2009) 9:78. doi: 10.1186/1471-2431-9-78
25. Hughes K, Gelfer Y, Cokljat M, Wientroub S, Yavor A, Hemo Y, et al. Does idiopathic congenital talipes equinovarus have an impact on attainment of developmental milestones? A multicentre international study. J Childrens Orthop. (2019) 13:353–60. doi: 10.1302/1863-2548.13.190060
26. Lissauer T, Carroll W. Normal child development, hearing and vision. 5th ed. In: T Lissauer, W Carroll editors. Illustrated Textbook of Paediatrics. Amsterdam: Elsevier (2015).
Keywords: developmental milestones, motor milestones, linguistic milestones, idiopathic clubfoot, Ponseti
Citation: Pavone V, Sapienza M, Vescio A, Caldaci A, McCracken KL, Canavese F and Testa G (2022) Early developmental milestones in patients with idiopathic clubfoot treated by Ponseti method. Front. Pediatr. 10:869401. doi: 10.3389/fped.2022.869401
Received: 04 February 2022; Accepted: 02 August 2022;
Published: 24 August 2022.
Edited by:
Luigi Aurelio Nasto, Giannina Gaslini Institute (IRCCS), ItalyReviewed by:
Daniela Dibello, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, ItalyAmeersing Luximon, EMEDS, Hong Kong SAR, China
Copyright © 2022 Pavone, Sapienza, Vescio, Caldaci, McCracken, Canavese and Testa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vito Pavone, dml0b3Bhdm9uZUBob3RtYWlsLmNvbQ==