
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 14 April 2022
Sec. Pediatric Infectious Diseases
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.868297
This article is part of the Research Topic Impact of SARS-CoV-2 and COVID-19 Pandemic in Pediatrics View all 25 articles
 Eduardo López-Medina1,2,3*
Eduardo López-Medina1,2,3* German Camacho-Moreno4
German Camacho-Moreno4 Martin E. Brizuela5
Martin E. Brizuela5 Diana M. Dávalos1,6
Diana M. Dávalos1,6 Juan Pablo Torres7
Juan Pablo Torres7 Rolando Ulloa-Gutierrez8Pio López1,2Roberto Debbag9
Rolando Ulloa-Gutierrez8Pio López1,2Roberto Debbag9 Paola Pérez6,10Jaime Patiño6,10
Paola Pérez6,10Jaime Patiño6,10 Ximena Norero11Cristina Mariño12Miguel A. Luengas12Gabriela Ensinck13Carlos Daza14Kathia Luciani15Paola Quintana Kuhner16Mónica Rodriguez16Juan Pablo Rodríguez-Auad17Alejandra Estrada-Villarroel17Mayli Carnevale18Orlando Cesar Mantese19
Ximena Norero11Cristina Mariño12Miguel A. Luengas12Gabriela Ensinck13Carlos Daza14Kathia Luciani15Paola Quintana Kuhner16Mónica Rodriguez16Juan Pablo Rodríguez-Auad17Alejandra Estrada-Villarroel17Mayli Carnevale18Orlando Cesar Mantese19 Eitan N. Berezin20José Iván Castillo21
Eitan N. Berezin20José Iván Castillo21 Abiel Mascareñas22Andrea Jimenez-Zambrano23Lourdes Dueñas24
Abiel Mascareñas22Andrea Jimenez-Zambrano23Lourdes Dueñas24 Mario Melgar25
Mario Melgar25 Nancy Galvez25
Nancy Galvez25 Erika Cantor1,26Edwin J. Asturias23,27
Erika Cantor1,26Edwin J. Asturias23,27Background: Limited data is available from low-middle and upper-middle income countries of the factors associated with hospitalization or admission to pediatric intensive care unit (PICU) for children with COVID-19.
Objective: To describe the factors associated with hospitalization or PICU admission of children with COVID-19 in Latin America.
Method: Multicenter, analytical, retrospective study of children reported from 10 different Latin American countries to the Latin-American Society of Pediatric Infectious Diseases (SLIPE-COVID) research network from June 1, 2020, and February 28, 2021. Outpatient or hospitalized children <18 years of age with COVID-19 confirmed by polymerase chain reaction or antigen detection from the nasopharynx were included. Children with multisystem inflammatory syndrome in children (MIS-C) were excluded. Associations were assessed using univariate and multivariable logistic regression models.
Results: A total of 1063 children with COVID-19 were included; 500 (47%) hospitalized, with 419 (84%) to the pediatric wards and 81 (16%) to the ICU. In multivariable analyses, age <1 year (Odds Ratio [OR] 1.78; 95% CI 1.08–2.94), native race (OR 5.40; 95% CI 2.13–13.69) and having a co-morbid condition (OR 5.3; 95% CI 3.10–9.15), were associated with hospitalization. Children with metabolic or endocrine disorders (OR 4.22; 95% CI 1.76–10.11), immune deficiency (1.91; 95% CI 1.05–3.49), preterm birth (OR 2.52; 95% CI 1.41–4.49), anemia at presentation (OR 2.34; 95% CI 1.28–4.27), radiological peribronchial wall thickening (OR 2.59; 95% CI 1.15–5.84) and hypoxia, altered mental status, seizures, or shock were more likely to require PICU admission. The presence of pharyngitis (OR 0.34; 95% CI 0.25–0.48); myalgia (OR 0.47; 95% CI 0.28–0.79) or diarrhea (OR 0.38; 95% CI 0.21–0.67) were inversely associated with hospital admission.
Conclusions: In this data analysis reported to the SLIPE research network in Latin America, infants, social inequalities, comorbidities, anemia, bronchial wall thickening and specific clinical findings on presentation were associated with higher rates of hospitalization or PICU admission. This evidence provides data for prioritization prevention and treatment strategies for children suffering from COVID-19.
The emergence and rapid global spread of SARS-CoV-2 in early 2020 posed a major threat to populations from low and middle income countries (LMIC), where data on clinical presentations and risk factors for serious COVID-19 infections in children were scarce (1, 2). There are now ~64 million cases of COVID-19 in Latin America (3), with 8–16% of these cases reported among those between 0 and 19 years of age in different countries of the region (4–8). Although COVID-19 presents as mild or asymptomatic in most children, severe disease and hospitalization can occur in ~1% of children and is likely to increase as children represent most of the unvaccinated in these countries (9).
Early identification of factors associated with severe disease in children allows clinicians and public health officials to triage those in need of advanced level of care and is critical as vaccination campaigns are rolled out, allowing the prioritization of those who will benefit the most from early protection. Although several observational studies have provided information on risk factors for hospitalization or critical care admission in children in high-income countries (10–16), detailed demographic, laboratory, radiological and clinical data obtained from a large sample in LMIC countries are scarce.
Pediatric societies around the world have established data registries of pediatric COVID-19 cases to understand the epidemiology, clinical presentation and morbidity and mortality rates in children (9, 17). The Sociedad Latinoamericana de Infectologia Pediatrica (SLIPE) started a multinational collaboration to create a data registry on children being affected with COVID-19 in Latin American countries. The purpose of the present study was to describe the factors associated with hospitalization or pediatric intensive care unit (PICU) admission in children with COVID-19 in Latin America.
Independent pediatricians collected and reported cases of COVID-19 using an online registry created by the SLIPE-COVID network that utilized a standardized data collection form developed in Research Electronic Data Capture (REDCap) hosted by the University of Colorado, Aurora, USA. Investigators from 17 sites in 14 cities from 10 different Latin American countries prospectively identified patients between June 1, 2020, and February 28, 2021 and retrospectively inputted their data. All study sites were level 3 referral hospitals. The registry and study protocol were reviewed and approved by the local institutional review board of each participating center. Since data was collected for routine clinical practice, research was deemed of minimal risk and the requirement for informed consent was waived.
Children <18 years of age who presented to outpatient clinics or hospital emergency departments from participating sites with COVID-19-related symptoms and polymerase chain reaction (PCR) or antigen-confirmed SARS-CoV-2 infection were included. Children with MIS-C were excluded from this analysis.
Case ascertainment varied across sites. Seven cities used an active case surveillance system that allowed to identify children with confirmed COVID-19 from a list of all ambulatory or hospitalized encounters provided by the hospital's epidemiology or microbiology department, while a passive case ascertainment method was used in the remaining seven cities where children were identified after a pediatric infectious disease service consultation was obtained.
Patient characteristics including demographics, clinical, laboratory and radiological data were collected from medical records as documented by the site clinician who evaluated the patient. For children with one or more COVID-19-related consultations during the study period, only data from the first encounter was collected and for children with multiple laboratory reports during their care, only first values were recorded. Nutritional status was classified based on body mass index (BMI) standard deviations (SD) according to the World Health Organization (WHO) into underweight (below −2 SD), normal nutritional status (between −2 and +1 SD), overweight (between +1 and +2 SD) and obesity (above +2 SD) (18). Radiologic findings were categorized according to the density and extent of parenchymal changes. Anemia was defined as hemoglobin below 11 grams/deciliter (19) and thrombocytopenia as platelets < 150,000 × 103 cells/μL (20). C-reactive protein and neutrophil to lymphocyte ratio were dichotomized as previous reports (21–23). For symptoms that were not described in medical records, investigators recorded “non-applicable” when children were too young or too ill to describe their symptoms.
Outcome endpoints for this analysis were divided into (a) outpatient care, (b) hospitalization in a general pediatric ward, or (c) intensive care unit (ICU) admission. Final disposition was at the discretion of primary care team. Data were compared in children requiring admission in the general ward vs. ICU, in those requiring hospitalization (general ward or ICU) vs. outpatient care and in those who did or did not require supplementary oxygen. In the latter two groups laboratory or imaging data were not compared, as children receiving outpatient care seldom had blood drawn or chest X-rays obtained.
Summary statistics were used for description of variables. Medians and interquartile ranges (IQR) were used for continuous variables; categorical variables were reported as absolute numbers and proportions. Chi2 tests and Fisher's exact tests were used for categorical variables as appropriate, and the Mann-Whitney U test was used for comparing median values of non-normally distributed variables. Associations of baseline characteristics and clinical findings with hospitalization, PICU and/or supplementary oxygen requirement were assessed using univariate and multivariable logistic regression models. Covariates that were significant at the 0.20 level in univariate analysis were included in multivariable models. A backward elimination algorithm was performed to select covariates that were independently associated with hospitalization, PICU and/or supplementary oxygen use, setting a p value of <0.05 as significant. Backward variable selection was performed using Rubin's Rules (24). Two multivariate models were created to explore associations with the outcomes of interest. One explored sociodemographic characteristics and comorbidities, and another explored signs/symptoms, laboratory values and radiologic findings. A sensitivity analysis including only children from the seven cities that used an active surveillance system was conducted. In addition, all co-morbidities were integrated in a model that explored the effect of any co-morbidity in the risk of hospital admission or PICU.
For missing data, a multiple imputation chained equation with 90 imputed datasets was used. This value was set using the rule of thumb (25). All variables, including the binary outcomes, were included in the imputation model and further sensitivity analysis was conducted using complete-case data. To control for variability in case ascertainment and non-measured social or cultural confounders, clustered standard errors were estimated to adjust for the correlation between children from the same city in each model. Hospitals from the same city had the same case ascertainment method. Variables that could not be assessed in all children due to age (i.e. anosmia or dysgeusia) were not imputed nor included in multivariable analysis. All statistical analyses were carried out in Stata version 16.0 (StataCorp, College, Station, TX) and p values of <0.05 (two-sided) were considered statistically significant. Imputation was not attempted for variables that had more than 50% of their data missing in the complete dataset except for the C-reactive protein values; this variable was imputed given its relevance in predicting severe outcomes in other studies (23, 26).
A total of 1063 children were included (median age, 3 years [IQR 1–9]; age range 22 days to 17.8 years, 46.4% female, 63% with normal weight and 29% with comorbidity). Of all, 563 (53%) received ambulatory care, while 500 (47%) were hospitalized (419 [84%] in the general ward and 81 [16%] in the ICU) (Table 1). Most children were included from 2 hospitals in Bogotá, Colombia (n = 387); 1 hospital in Quilmes, Argentina (n = 264); 2 hospitals in Cali, Colombia (n = 160) and 2 hospitals in Panamá (n = 109). The remaining cases (n = 143) were included from Asunción, Paraguay; David, Panamá; Guatemala City, Guatemala; La Paz, Bolivia; Lara, Venezuela; Monterrey, México; Rosario, Argentina; San Lorenzo, Paraguay; San Salvador, El Salvador and Uberlandia, Brazil (Figure 1).

Table 1. Demographics and clinical characteristics of pediatric patients with COVID-19.

Figure 1. SLIPE-COVID research network-city locations and sites.
Most children had fever (70%) and cough (55%). Fewer than one third had signs or symptoms of upper respiratory tract infection (Table 1). Ninety-seven children (9%) had diarrhea without respiratory symptoms while 104 children (9.8%) did not have either fever or respiratory symptoms at admission. The frequency of these clinical presentations varied by age groups (Supplementary Table 1). Frequency of missing data is presented in Supplementary Table 2.
Eighteen children died (median age 6.2 years [IQR 1.8–12.2], 11 [61%] males), 11 (61%) had comorbidities (mainly immune deficiency [n = 6, 33%] or neurologic [n = 3, 17%]), and 22% came from a rural area. The majority presented with fever (n = 15, 83%), hypoxia (n = 14, 78%), dyspnea (n = 13, 72%) and cough (n = 11, 61%). Characteristics of hospital admission among 500 hospitalized children are described in Supplementary Table 3.
Five hundred hospitalized children were compared with 563 children who received outpatient care. In the multivariable model using multiple imputation, younger age (<1 year), native race, and the presence of certain underlying medical conditions were associated with an increased risk for hospital admission (Table 2 and Figure 2). In a model that considered all underlying medical conditions together, the odds for hospital admission were 5.3 times higher (95% CI 3.10 to 9.15) in children with any underlying medical conditions. Both sensitivity analysis (using the complete dataset that included missing data and only children who were enrolled from the seven cities that used an active surveillance system) showed similar results (Supplementary Table 4).

Table 2. Demographic and underlying medical conditions associated with hospitalization (general ward and intensive care), among pediatric patients with COVID-19 using multiple imputation chained equations for missing data.
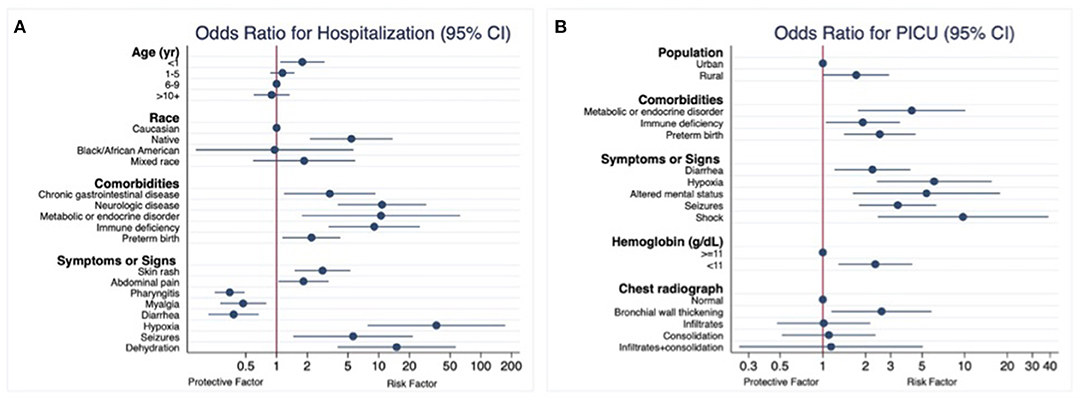
Figure 2. Risk factors among pediatric patients with COVID-19. Multiple imputation chained equations for missing data. (A) Hospital admission (general pediatric ward or pediatric intensive care unit). (B) Pediatric intensive care admission among hospitalized patients.
Children presenting with skin rash, abdominal pain, dehydration, hypoxia, or seizures were at increased risk for hospital admission, while pharyngitis, myalgia and diarrhea reduced the odds of hospital admission (Table 3). Similar results were obtained from both sensitivity analysis (Supplementary Table 5).
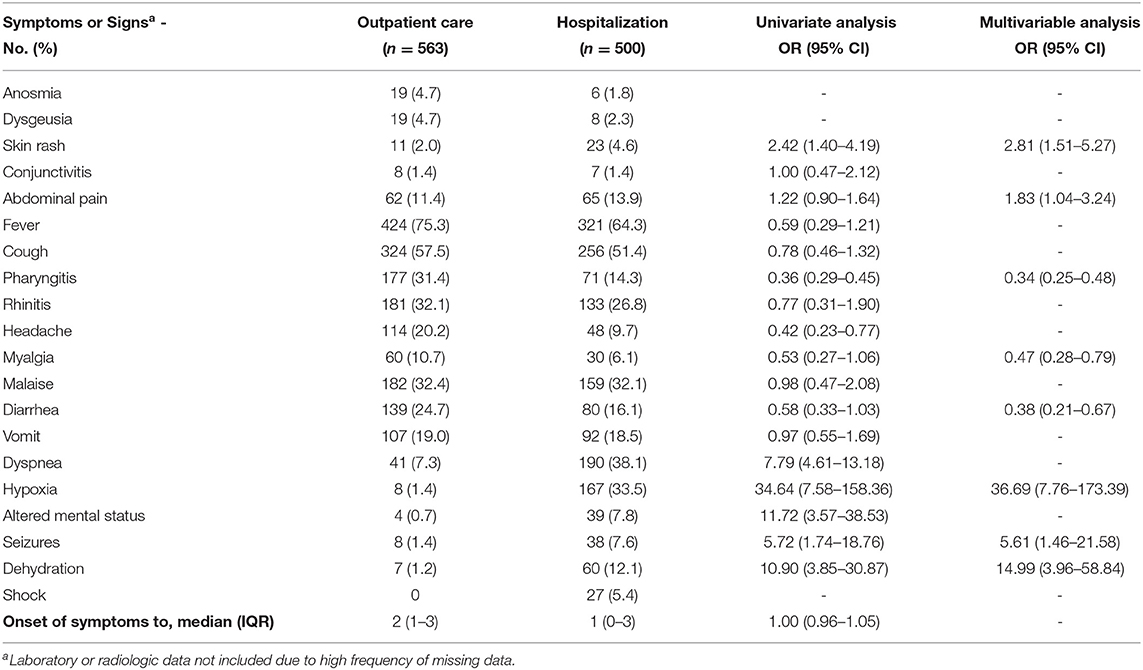
Table 3. Signs or symptoms described or present on initial evaluation associated with hospitalization (general ward and intensive care), among pediatric patients with COVID-19 using multiple imputation chained equations for missing data.
The 81 children who required ICU admission were compared with the remaining 419 children who were hospitalized in the general pediatric ward. In the multiple imputation model, residing in a rural area was the only sociodemographic factor associated with increased odds of ICU care, while metabolic or endocrine disorder, immune deficiency and preterm birth were the underlying medical conditions significantly associated with ICU admission (Table 4). Sensitivity analysis showed similar results (Supplementary Table 6).
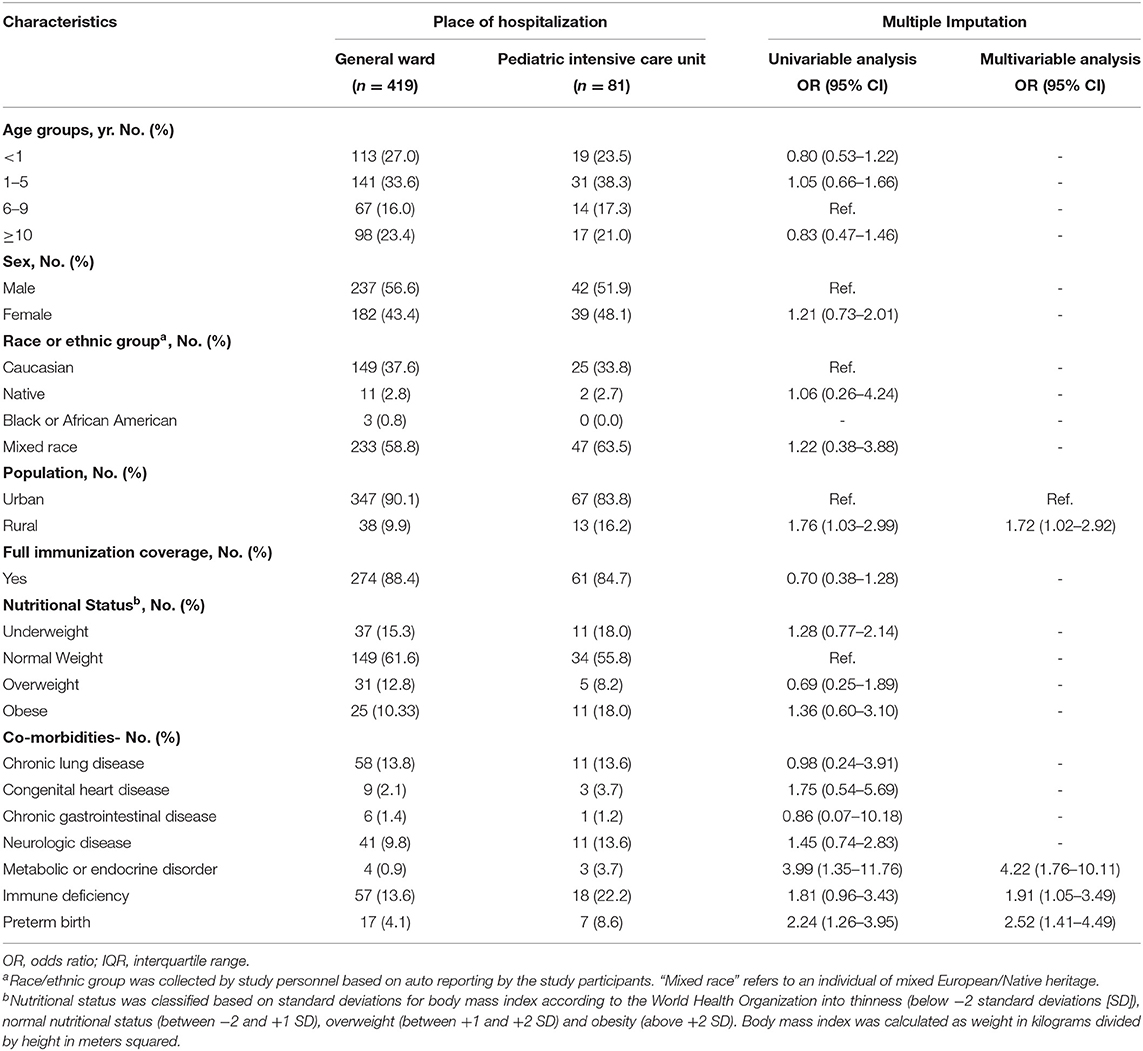
Table 4. Demographic and underlying medical conditions associated with intensive care, among pediatric patients hospitalized due to COVID-19 using multiple imputation chained equations for missing data.
Children presenting with diarrhea, hypoxia, altered mental status, seizures or shock were at higher risk for ICU admission. Anemia and bronchial wall thickening in chest radiograph were also associated with increased risk (Table 5). Sensitivity analysis showed similar results (Supplementary Table 7).
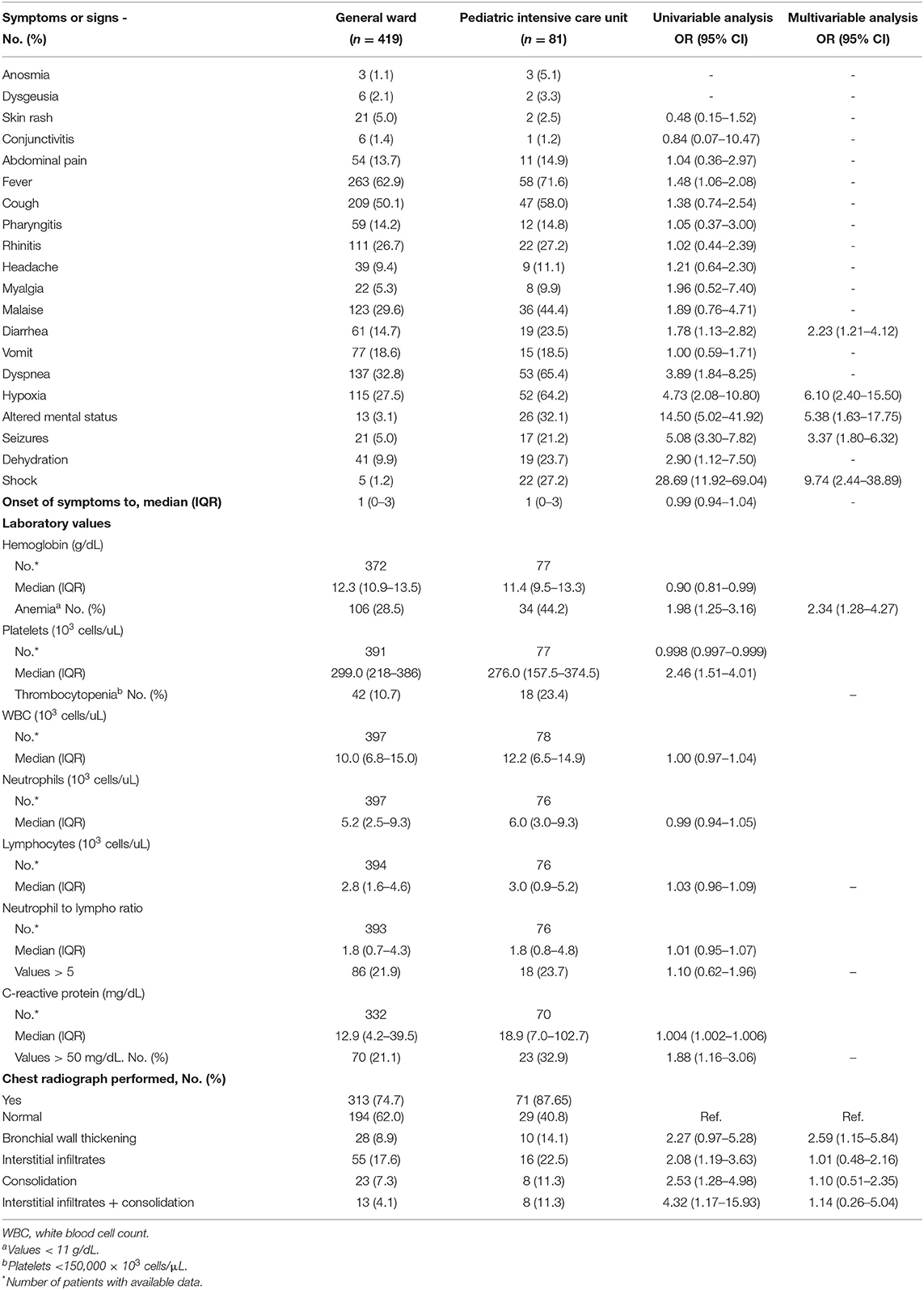
Table 5. Signs or symptoms, laboratory values and chest radiograph findings described or present on initial evaluation associated with intensive care, among pediatric patients hospitalized due to COVID-19 using multiple imputation chained equations for missing data.
Risk factors associated with supplementary oxygen requirement were similar to those associated with hospital admission. In addition, history of chronic lung disease increased the risk for supplementary oxygen requirement (OR 4.45, 95% CI 2.35–8.41) (Supplementary Table 8).
In this multi-country case registry of children with COVID-19 (excluding MIS-C), we identified several factors independently associated with ICU admission, hospitalization and need for supplementary oxygen. Similar to other reports, age under 1-year, comorbidities such as metabolic/endocrine disorders, preterm birth or immune deficiency, certain presenting signs/symptoms and social determinants of health were associated with increased COVID-19-related morbidity (10, 15, 27–30). In addition, low hemoglobin concentrations and bronchial wall thickening on chest radiographs were independently associated with the need for PICU admission.
Social determinants of health have long been recognized to be important predictors as to how epidemics are experienced in terms of infection rates and morbidity (31), particularly in more socially unequal regions, such as Latin America. A multicenter cohort study reported that rates of pediatric PICU admission and deaths due to COVID-19 were higher in Latin American than European children (32). Disparities in health determinants like economic instability, insurance status and housing conditions of patients and their families have consistently placed social, racial, and ethnic minorities at greater risk for severe illness by COVID-19 (31). This is especially true for children and their social determinants influencing life opportunities, disease characteristics and health outcomes. We described greater risks in children with demographic characteristics indicative of lower socio-economic status in Latin America such as native ethnic group or living in rural areas. Social inequalities and low socioeconomic status have also been described as risk factors for death (28), so it is possible that unmeasured socioeconomic or cultural disparities that increase the risk of a more severe or late presentation in children living in rural areas may have been present in this study. For example, although level of education of the caregiver was not imputed or included in multivariable analysis due to the high frequency of missing data, there was a higher proportion of uneducated caregivers among those children who required hospitalization.
Obesity and diabetes mellitus are comorbidities that have been identified as risk factors for disease severity in other studies (12, 15, 33–35). In this study, obesity was not significantly associated with higher risk of hospitalization or ICU admission. However, obesity was more frequent in children requiring ICU admission than in children requiring outpatient care (18 vs. 8.4%, respectively), although no multivariable model comparison was made for these two categories. In addition, obese children were at higher odds of hospitalization (overall and in the ICU), although this was of limited statistical significance. Yet, in studies from high-income countries, obesity has been consistently demonstrated as a risk factor for disease severity in children, especially in adolescents (15, 36). In animal studies, angiotensin-converting enzyme 2 (ACE2) protects against SARS-CoV-2 associated acute respiratory distress syndrome (ARDS) (37). ACE2 expression is decreased in children with diabetes mellitus likely due to glycosylation (38), which may explain their higher risk for hospital or ICU admission in this and other series (33). Although asthma has been suggested as a risk factor for severe illness in children with COVID-19, our study, as well as a registry-based (39) and a cohort study (16) did not confirm this association. Overall, the underlying medical conditions associated with hospital or ICU admission in this Latin American pediatric registry are similar to those described for the same outcomes in US children (39).
As with children with COVID-19 from European and North American countries (11, 40), fever and cough were the predominant clinical features at presentation (70 and 55%, respectively) and approximately a third of children presented with gastrointestinal symptoms. Some clinical manifestations are related to disease progression and complications and are predictive of a higher level of care. As reported in adults (41), children presenting with hypoxia, altered mental status, seizures, shock, dyspnea, or dehydration were more likely to require hospital admission or intensive care. Pharyngitis, myalgia, and diarrhea were identified in this series as inversely associated with hospital admission; and in the complete dataset anosmia and dysgeusia were also found to be protective although of limited statistical significance. A UK study also found that children presenting with upper respiratory signs (rhinorrhea) were less likely to require admission to critical care (35). Preferential distribution of ACE-2 receptors in the upper respiratory or intestinal epithelium (42) may explain the lower frequency of hospitalization in children with these clinical features. Between 9 and 10% of children in this series presented without fever or respiratory symptoms, or only developed diarrhea, findings that need to be considered when developing diagnostic algorithms, especially in settings with actively circulating virus.
Several laboratory findings have been associated with the severity of COVID-19 in adult patients (43). However, data on laboratory values as risk factors for the need for ICU admission in children are scarce. Of routinely collected data in children, only the C-reactive protein has been shown to be a predictor in one study (12), but not in others (44). Similar to our findings, leukocyte indices do not appear to be reliable indicators of disease severity in the pediatric population (45). We found that anemia was the only laboratory predictor for the risk of ICU admission. Whereas this finding has not been described in children, it has been documented as a significant risk factor in adults (46) and should be looked at in detail when assessing children with COVID-19. Like adults (47), bronchial wall thickening was associated with increased risk of ICU admission. Other more severe radiologic abnormalities often described in severe cases (48) were not independently associated with risk of ICU admission in this series, likely due to low number of cases.
Several studies have described risk factors for severe COVID-19 in high-income countries, but data is still scarce from LMIC. Our findings are similar to those from the UK cohort of children for admission to critical care (35). In both studies, children who required PICU were more likely to be of younger age, and had associated comorbidities. Studies from high-income countries have shown that adolescents and patients with elevated C-reactive protein have an increased risk for more severe outcomes (12, 16, 40, 49). These associations were not evident in our data, although different exposure categories and outcome measures may explain these discrepancies.
This study has several limitations. First, seven of the 14 reporting cities used a passive case-ascertainment method which probably introduced a selection bias. Thus, our study population does not represent the full spectrum of COVID-19, but rather children with more severe disease. This is unlikely to impact our results or conclusions given that our goal was to identify factors associated with hospital or ICU admission, and the multilevel regression model clustered by region. To further explore for selection bias, a sensitivity analysis including only children from the seven cities that used an active surveillance system was compared with the analysis that included all children. Factors associated with severity were similar in both analyses suggesting that the effect on our data was minimal.
Second, some relevant variables had missing data, which could reduce the statistical power of the study and produce biased estimates. We tried to overcome this limitation by using multiple imputation, allowing appropriate estimation of the underlying distribution of the data. Results from analyses using the complete dataset (including missing data) and the multiple imputation dataset were similar. Third, we excluded children with MIS-C, who represent one of the most severe clinical forms of pediatric post-infectious COVID-19. A separate full analysis of MIS-C children in Latin American children is ongoing by investigators from the REKAMLATINA network in a cohort of children admitted at several hospitals in the region (50). Finally, due to the multisite nature of the study, full standardization of criteria utilized by all managing clinicians for hospitalization or ICU care was not possible. Therefore, children's outcome disposition may differ by hospitals' capacity and census demands, notwithstanding the severity of the COVID-19 presentation. However, the need for ICU admission or oxygen is an objective measure for a more serious condition.
In conclusion, this evolving collaborative network allowed the collection of detailed data in one of the largest studies from a LMIC region to provide a first description of associated factors for hospital or ICU admission in developing countries. The demographic, clinical and laboratory parameters that were identified could help care providers in different settings (outpatient clinic, emergency room or general pediatric wards) to identify children at higher risk for a complicated disease course, and direct policy makers to prioritize pediatric subgroups for prevention and treatment strategies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and the registry and study protocol were reviewed and approved by the local Institutional Review Board of each participant center. The research was deemed of minimal risk because data was collected for routine clinical practice and the requirement for informed consent was waived. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
EL-M and EA: study conception and design. EL-M, GC-M, MB, DD, JT, RU-G, PL, RD, PP, JP, XN, CM, ML, GE, CD, KL, PQ, MR, JR-A, AE-V, MC, OM, EB, JC, AM, AJ-Z, LD, MM, and NG: data collection. EL-M, EC, and EA: analysis and interpretation of results. E-LM and EA: draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
The Research Electronic Data Capture (REDCap) database used for this study was supported by the Grant Number UL1 TR002535, from NIH/NCATS Colorado CTSA.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the contributions of the physicians, nurses and the administrative team at SLIPE for the work in caring for these patients and to the contributing institutions for participating in the SLIPE-COVID network.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.868297/full#supplementary-material
1. Pathak EB, Salemi JL, Sobers N, Menard J, Hambleton IR. COVID-19 in Children in the United States: Intensive Care Admissions, Estimated Total Infected, and Projected Numbers of Severe Pediatric Cases in 2020. J Public Health Manag Pract. (2020) 26:325–33. doi: 10.1097/PHH.0000000000001190
2. Mehta NS, Mytton OT, Mullins EWS, Fowler TA, Falconer CL, Murphy OB, et al. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clin Infect Dis. (2020) 71:2469–79. doi: 10.1093/cid/ciaa556
3. Panamerican Health Organization. PAHO. Geo-Hub COVID-19 - Information System for the Region of the Americas. (2022). Available online at: https://paho-covid19-response-who.hub.arcgis.com (accessed February 24, 2022).
4. Gobierno de Chile. Plan de Acción Coronavirus (2022). Available online at: https://www.gob.cl/coronavirus/cifrasoficiales/#datos (accessed February 24, 2022).
5. Dirección general de Epidemiología. Gobierno de Mexico. COVID-19 Mexico Tablero general CONACYT. Available online at: https://datos.covid-19.conacyt.mx (accessed February 24, 2022).
6. Ministerio de Salud Argentina. Vigilancia Epidemiologica. Nuevo Coronavirus. Vigilancia, diagnóstico y manejo institucional de casos en pediatría. (2021). Available online at: https://www.argentina.gob.ar/salud/coronavirus/casos-pediatria (accessed February 24, 2022).
7. Instituto Nacional de Salud. Ministerio de Salud y Protección Social Colombia. COVID-19 en Colombia. (2022). Available online at: https://www.ins.gov.co/Noticias/Paginas/coronavirus-casos.aspx (accessed February 24, 2022).
8. Ministerio de Salud Publica y Bienestar Social. Gobierno de Paraguay. Coronavirus/ COVID 19 en Paraguay. (2022). Available online at: https://www.mspbs.gov.py/reporte-covid19.html (accessed February 25, 2022).
9. American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. Available online at: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/ (accessed September 14, 2021).
10. Bellino S, Punzo O, Rota MC, Del Manso M, Urdiales AM, Andrianou X, et al. COVID-19 Disease Severity Risk Factors for Pediatric Patients in Italy. Pediatrics. (2020) 146:e2020009399. doi: 10.1542/peds.2020-009399
11. Gotzinger F, Santiago-Garcia B, Noguera-Julian A, Lanaspa M, Lancella L, Calo Carducci FI, et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health. (2020) 4:653–61. doi: 10.1016/S2352-4642(20)30177-2
12. Graff K, Smith C, Silveira L, Jung S, Curran-Hays S, Jarjour J, et al. Risk Factors for Severe COVID-19 in Children. Pediatr Infect Dis J. (2021) 40:e137–e45. doi: 10.1097/INF.0000000000003043
13. Tsabouri S, Makis A, Kosmeri C, Siomou E. Risk Factors for Severity in Children with Coronavirus Disease 2019: A Comprehensive Literature Review. Pediatr Clin North Am. (2021) 68:321–38. doi: 10.1016/j.pcl.2020.07.014
14. Moreira A, Chorath K, Rajasekaran K, Burmeister F, Ahmed M, Moreira A. Demographic predictors of hospitalization and mortality in US children with COVID-19. Eur J Pediatr. (2021) 180:1659–63. doi: 10.1007/s00431-021-03955-x
15. Woodruff RC, Campbell AP, Taylor CA, Chai SJ, Kawasaki B, Meek J, et al. Risk factors for severe COVID-19 in children. Pediatrics. (2021) e2021053418. doi: 10.1542/peds.2021-053418. [Epub ahead of print].
16. Funk AL, Florin TA, Kuppermann N, Tancredi DJ, Xie J, Kim K, et al. Outcomes of SARS-CoV-2-Positive Youths Tested in Emergency Departments: The Global PERN-COVID-19 Study. JAMA Netw Open. (2022) 5:e2142322. doi: 10.1001/jamanetworkopen.2021.42322
17. Pudjiadi AH, Putri ND, Sjakti HA, Yanuarso PB, Gunardi H, Roeslani RD, et al. Pediatric COVID-19: Report From Indonesian Pediatric Society Data Registry. Front Pediatr. (2021) 9:716898. doi: 10.3389/fped.2021.716898
18. World Health Organization.WHO. Obesity and Overweight. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed September 14, 2021).
19. World Health Organization.WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Available online at: https://apps.who.int/iris/handle/10665/85839 (accessed September 14, 2021).
20. Linkins LA, Dans AL, Moores LK, Bona R, Davidson BL, Schulman S, et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (2012) 141(2 Suppl):e495S–e530S. doi: 10.1378/chest.11-2303
21. Imran MM, Ahmad U, Usman U, Ali M, Shaukat A, Gul N. Neutrophil/lymphocyte ratio-A marker of COVID-19 pneumonia severity. Int J Clin Pract. (2021) 75:e13698. doi: 10.1111/ijcp.13698
22. Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA. (2021) 325:1074–87. doi: 10.1001/jama.2021.2091
23. Sim BLH, Chidambaram SK, Wong XC, Pathmanathan MD, Peariasamy KM, Hor CP, et al. Clinical characteristics and risk factors for severe COVID-19 infections in Malaysia: a nationwide observational study. Lancet Reg Health West Pac. (2020) 4:100055. doi: 10.1016/j.lanwpc.2020.100055
24. Wood AM, White IR, Royston P. How should variable selection be performed with multiply imputed data? Stat Med. (2008) 27:3227–46. doi: 10.1002/sim.3177
25. White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. (2011) 30:377–99. doi: 10.1002/sim.4067
26. Chen X, Yan L, Fei Y, Zhang C. Laboratory abnormalities and risk factors associated with in-hospital death in patients with severe COVID-19. J Clin Lab Anal. (2020) 34:e23467. doi: 10.1002/jcla.23467
27. Team CC-R. Coronavirus Disease 2019 in Children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:422–6. doi: 10.15585/mmwr.mm6914e4
28. Oliveira EA, Colosimo EA, Simoes ESAC, Mak RH, Martelli DB, Silva LR, et al. Clinical characteristics and risk factors for death among hospitalised children and adolescents with COVID-19 in Brazil: an analysis of a nationwide database. Lancet Child Adolesc Health. (2021) 5:559–68. doi: 10.1016/S2352-4642(21)00134-6
29. Gonzalez-Dambrauskas S, Camporesi A, Cantillano EM, Dallefeld S, Dominguez-Rojas J, Gurbanov A, et al. Pediatric critical COVID-19 and mortality in a multinational cohort. Available online at: https://www.medrxiv.org/content/10.1101/2021.08.20.21262122v1.full.pdf (accessed January 15, 2022).
30. Shekerdemian LS, Mahmood NR, Wolfe KK, Riggs BJ, Ross CE, McKiernan CA, et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. (2020) 174:868–73. doi: 10.1001/jamapediatrics.2020.1948
31. Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. (2020) 74:964–8. doi: 10.1136/jech-2020-214401
32. Antúnez-Montes OY, Escamilla MI, Figueroa-Uribe AF, Arteaga-Menchaca E, Lavariega-Saráchaga M, Salcedo-Lozada P, et al. COVID-19 and Multisystem Inflammatory Syndrome in Latin American Children: a multinational study. Pediatr Infect Dis J. (2021) 40:e1–6. doi: 10.1097/INF.0000000000002949
33. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
34. Petrilli CM, Jones SA, Yang J, Rajagopalan H, O'Donnell L, Chernyak Y, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. (2020) 369:m1966. doi: 10.1136/bmj.m1966
35. Swann OV, Holden KA, Turtle L, Pollock L, Fairfield CJ, Drake TM, et al. Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: prospective multicentre observational cohort study. BMJ. (2020) 370:m3249. doi: 10.1136/bmj.m3249
36. Martin B, DeWitt PE, Russell S, Anand A, Bradwell KR, Bremer C, et al. Characteristics, Outcomes, and Severity Risk Factors Associated With SARS-CoV-2 Infection Among Children in the US National COVID Cohort Collaborative. JAMA Netw Open. (2022) 5:e2143151. doi: 10.1001/jamanetworkopen.2021.43151
37. Imai Y, Kuba K, Rao S, Huan Y, Guo F, Guan B, et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature. (2005) 436:112–6. doi: 10.1038/nature03712
38. Pal R, Bhansali A. COVID-19, diabetes mellitus and ACE2: The conundrum. Diabetes Res Clin Pract. (2020) 162:108132. doi: 10.1016/j.diabres.2020.108132
39. Kompaniyets L, Agathis NT, Nelson JM, Preston LE, Ko JY, Belay B, et al. Underlying Medical Conditions Associated With Severe COVID-19 Illness Among Children. JAMA Netw Open. (2021) 4:e2111182. doi: 10.1001/jamanetworkopen.2021.11182
40. Drouin O, Hepburn CM, Farrar DS, Baerg K, Chan K, Cyr C, et al. Characteristics of children admitted to hospital with acute SARS-CoV-2 infection in Canada in 2020. CMAJ. (2021) 193:E1483–E93. doi: 10.1503/cmaj.210053
41. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
42. Zimmermann P, Curtis N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child. (2020) archdischild-2020-320338. doi: 10.1136/archdischild-2020-320338. [Epub ahead of print].
43. Zeng Z, Yu H, Chen H, Qi W, Chen L, Chen G, et al. Longitudinal changes of inflammatory parameters and their correlation with disease severity and outcomes in patients with COVID-19 from Wuhan, China. Crit Care. (2020) 24:525. doi: 10.1186/s13054-020-03255-0
44. Henry BM, Benoit SW, de Oliveira MHS, Hsieh WC, Benoit J, Ballout RA, et al. Laboratory abnormalities in children with mild and severe coronavirus disease 2019 (COVID-19): A pooled analysis and review. Clin Biochem. (2020) 81:1–8. doi: 10.1016/j.clinbiochem.2020.05.012
45. Henry BM, Lippi G, Plebani M. Laboratory abnormalities in children with novel coronavirus disease 2019. Clin Chem Lab Med. (2020) 58:1135–8. doi: 10.1515/cclm-2020-0272
46. Tao Z, Xu J, Chen W, Yang Z, Xu X, Liu L, et al. Anemia is associated with severe illness in COVID-19: A retrospective cohort study. J Med Virol. (2021) 93:1478–88. doi: 10.1002/jmv.26444
47. Li K, Wu J, Wu F, Guo D, Chen L, Fang Z, et al. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Invest Radiol. (2020) 55:327–31. doi: 10.1097/RLI.0000000000000672
48. Ong SWX, Hui TCH, Lee YS, Haja Mohideen SM, Young BE, Tan CH, et al. High-risk chest radiographic features associated with COVID-19 disease severity. PLoS ONE. (2021) 16:e0245518. doi: 10.1371/journal.pone.0245518
49. Fisler G, Izard SM, Shah S, Lewis D, Kainth MK, Hagmann SHF, et al. Characteristics and risk factors associated with critical illness in pediatric COVID-19. Ann Intensive Care. (2020) 10:171. doi: 10.1186/s13613-020-00790-5
Keywords: COVID-19, SARS-CoV-2, children, critical care, hospitalization
Citation: López-Medina E, Camacho-Moreno G, Brizuela ME, Dávalos DM, Torres JP, Ulloa-Gutierrez R, López P, Debbag R, Pérez P, Patiño J, Norero X, Mariño C, Luengas MA, Ensinck G, Daza C, Luciani K, Quintana Kuhner P, Rodriguez M, Rodríguez-Auad JP, Estrada-Villarroel A, Carnevale M, Mantese OC, Berezin EN, Castillo JI, Mascareñas A, Jimenez-Zambrano A, Dueñas L, Melgar M, Galvez N, Cantor E and Asturias EJ (2022) Factors Associated With Hospitalization or Intensive Care Admission in Children With COVID-19 in Latin America. Front. Pediatr. 10:868297. doi: 10.3389/fped.2022.868297
Received: 02 February 2022; Accepted: 14 March 2022;
Published: 14 April 2022.
Edited by:
Hulya Bukulmez, Case Western Reserve University, United StatesReviewed by:
Saul Flores, Texas Children's Hospital, United StatesCopyright © 2022 López-Medina, Camacho-Moreno, Brizuela, Dávalos, Torres, Ulloa-Gutierrez, López, Debbag, Pérez, Patiño, Norero, Mariño, Luengas, Ensinck, Daza, Luciani, Quintana Kuhner, Rodriguez, Rodríguez-Auad, Estrada-Villarroel, Carnevale, Mantese, Berezin, Castillo, Mascareñas, Jimenez-Zambrano, Dueñas, Melgar, Galvez, Cantor and Asturias. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo López-Medina, ZWR1YXJkby5sb3BlekBjZWlwb25saW5lLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.