 Stephanie Coupal
Stephanie Coupal Kenneth Lukas
Kenneth Lukas Amy Plint2
Amy Plint2 Kevin Smit
Kevin Smit Sasha Carsen
Sasha Carsen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr., 19 May 2022
Sec. Pediatric Orthopedics
Volume 10 - 2022 | https://doi.org/10.3389/fped.2022.863985
This article is part of the Research TopicElbow Injury in Pediatric PatientsView all 14 articles
Purpose: Gartland Type 1 supracondylar humerus fractures are stable, non-displaced injuries treated with non-operative management. This systematic review was performed to gather evidence on the optimal form of immobilization to treat these fractures.
Methods: The review process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. An electronic search was performed in November 2020. Articles were eligible if they included children less than 18 years old, with non-displaced supracondylar fractures, treated non-operatively. Randomized trials, quasi-experimental trials, and prospective cohort studies were included. Outcomes of interest included fracture displacement, pain control, time to return to normal activities, return of range of motion (ROM), child/parent satisfaction, adverse events, and cost. Risk of bias was assessed using the Newcastle-Ottawa scale, Rob-2, and the ROBINS tools.
Results: After duplicate records were removed, 525 records were evaluated with 9 studies meeting the inclusion criteria and 5 reporting clinical outcomes. The studies were heterogenous, in intervention and outcomes, and all at moderate risk of bias. Within the available evidence there were no cases of fracture displacement. Two small studies suggested that cuff and collar treatment provided inadequate pain control and delay in return to normal activities, compared to posterior splints. Two randomized control trials (RCTs) suggested that soft fiberglass casts reduced appointment time and increased parent satisfaction, compared to traditional casts. No studies directly compared posterior splints to circumferential casts.
Conclusion: There is insufficient high-quality evidence to determine the optimal conservative treatment for patients with Gartland type 1 supracondylar fractures. Level of Evidence Level II systematic review of Level II studies.
Systematic Review Registration: [PROSPERO], identifier [CRD42020144616].
Supracondylar humerus fractures are the most common pediatric elbow fracture (1) and account for around 60–70 emergency department visits per 100,000 children annually (2). These fractures are categorized according to the modified Gartland classification system, depending on the degree of displacement, disruption of the posterior cortex, and location of the anterior humeral capitellum line on a lateral radiograph (3). Gartland Type I fractures are non-displaced and are widely accepted as stable fractures that should be treated non-operatively.
The ideal treatment for Type I supracondylar fractures should prevent fracture displacement and result in excellent clinical outcomes while minimizing adverse outcomes, pain, as well as direct and indirect costs to families and healthcare systems. Despite the common nature of these fractures, there remains a lack of consensus regarding which type of immobilization and follow-up care is most appropriate. Emergency department guidelines from Australia and Canada suggest immobilization with an above elbow “backslab” (a posterior splint) and broad arm sling. (4, 5). In comparison, long arm cast immobilization is generally recommended in a number of orthopedic surgery clinical guidelines and textbooks (6).
Given the frequency of the fracture and the existing clinical ambiguity with respect to the type of immobilization, a systematic review was performed to determine the optimal management of Type I supracondylar humerus fractures based on the highest level of evidence available. Our primary objective was to determine which forms of immobilization for Type I supracondylar humerus fractures prevent fracture displacement. Secondary objectives include the determination of relative risks and benefits of different treatment options.
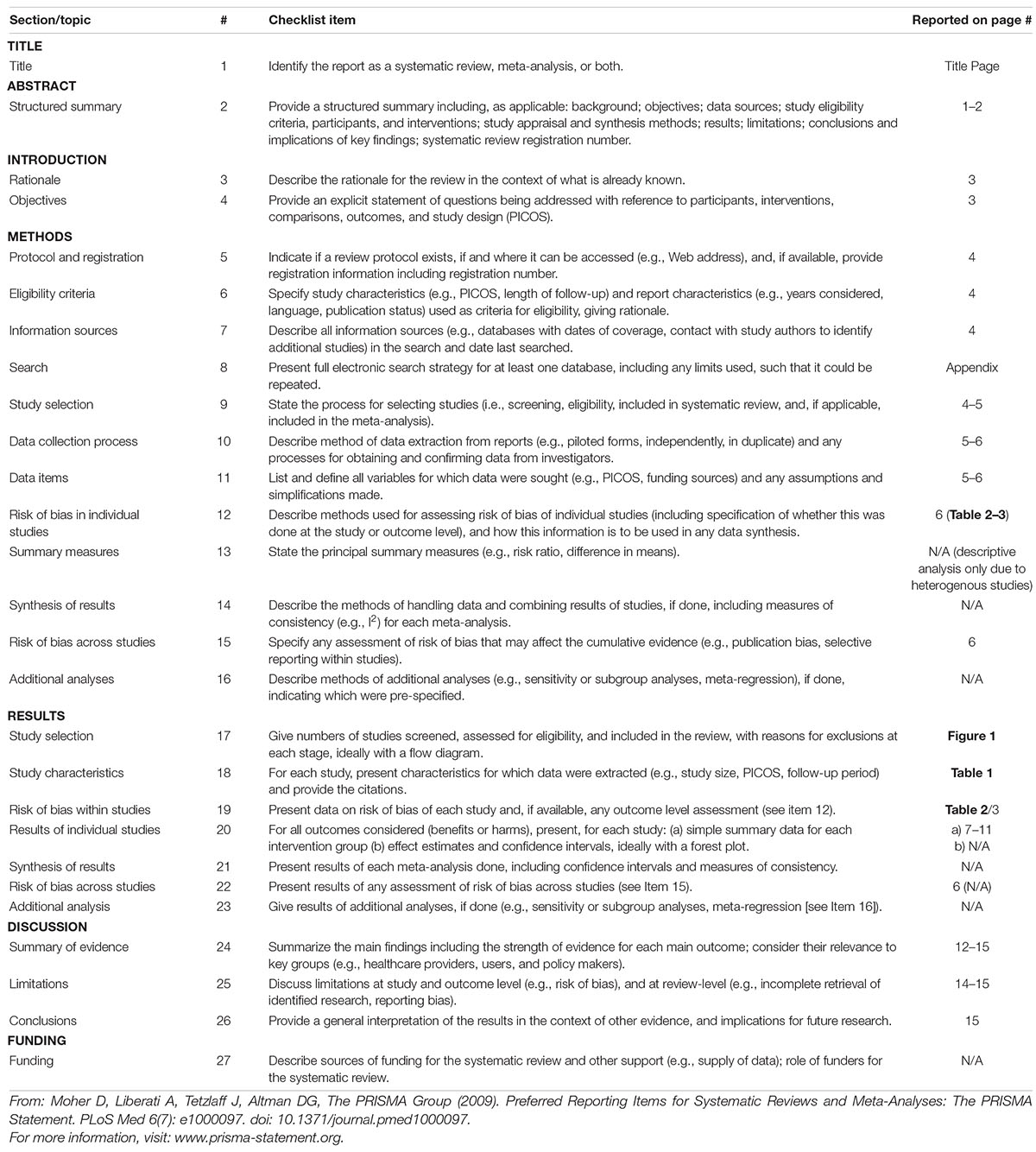
A systematic review was performed to identify publications that reported clinical outcomes and adverse events in pediatric patients with Type I supracondylar humerus fractures treated with immobilization. The review process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, the details of which are available in Appendix A. The review protocol was published on PROSPERO (CRD42020144616).
The following databases were searched on November 13, 2020: MEDLINE, Embase, and CENTRAL Trials Registry of the Cochrane Collaboration, using the Ovid interface. Search terms for intervention included cast, slab, sling, cuff and collar, splint, non-surgical, and immobilization with the appropriate Boolean operators. Population-specific search terms included supracondylar fracture, or distal humerus fracture and babies, neonatal, infant, child, preschool, adolescent, or pediatric using corresponding Boolean operators. The search was not restricted by language or study design. Our search strategy was designed and conducted by a librarian experienced in systematic reviews, using a method designed to optimize term selection (7). A detailed description of the search strategies is presented in Appendix B.
Studies were considered eligible if they met the following criteria: (1) the population included children < 18 years with type 1 (non-displaced) supracondylar fractures; (2) the study type was: randomized trial, quasi-experimental trial (non-randomized interventional study), or prospective cohort; (3) the study involved non-operative fracture management (including: tensor bandage, splint, casting, sling, cuff and collar, no intervention); (4) written in the English language. Fracture displacement was considered the primary outcome, but was not made an explicit inclusion criterion in order to broaden the article pool for reporting on our secondary outcomes. Studies were excluded if they met the following exclusion criteria: (1) narrative and systematic reviews, editorials, letters, surveys, case series and case reports, study protocols, retrospective cohort studies, cross-sectional studies, and studies published only in abstract form; (2) studies that primarily focused on closed reduction, operative management, or traction; (3) studies that primarily focused on adult patients; (3) animal studies; (4) studies that solely focused on patients with displaced (Gartland type II or III) supracondylar fractures, intra-articular distal humerus fractures, or proximal humerus fractures.
Duplicate records were removed, and records retrieved by the electronic search were uploaded to an online systematic review tool (InSight Scope, Ottawa, Canada). Records were appraised against the inclusion and exclusion criteria using a two-step approach. First, two reviewers (KL and SC) independently reviewed the titles and abstracts of the papers for potentially eligible studies. The full-text article of any abstract selected by either reviewer was then reviewed by both reviewers. Conflicts were resolved by the senior author (KL and SC). The reference list from the articles of the included studies was reviewed by KL and SC to identify any further possibly relevant articles. The authors of the included articles were contacted to inquire about additional available data or to clarify results or methodology if unclear.
Data from the included studies were extracted independently by two authors (KL and SC) and compared for consistency before inclusion in the analysis. Full data extraction included study design details, population, and outcomes including fracture displacement, pain control, time to return to normal activities, return of range of motion (ROM), child/parent satisfaction, adverse events, cost (health care, patient/parent, societal), and additional hospital visits. Discrepancies were investigated and rectified by returning to the original paper. In cases where the study population was heterogenous, data was extracted specifically for Type I or non-displaced fractures, where possible. There was no specific data manipulation required to extract this fracture-specific data.
Risk of bias was assessed by two authors (KL and SC) with the Cochrane Rob-2 for randomized control trials (RCTs), Cochrane ROBINS-1 for quasi-experimental studies, and the Newcastle-Ottawa Scale for cohort studies. Discrepancies were resolved with discussion. There is low risk of selection or publication bias across this research topic.
We had originally planned to perform a meta-analysis. However, given the heterogeneity of studies and results a descriptive analysis was instead performed.
The primary database search returned 742 records, and 525 records remained after duplicates were removed. Screening of titles and abstracts further excluded 367 records, leaving 126 for full article review with 9 studies meeting all the inclusion and exclusion criteria (see Figure 1). Four of the studies did not include clinical or adequate radiological outcome data, and therefore could not be used for data extraction. No additional studies were identified through review of the references of included papers.
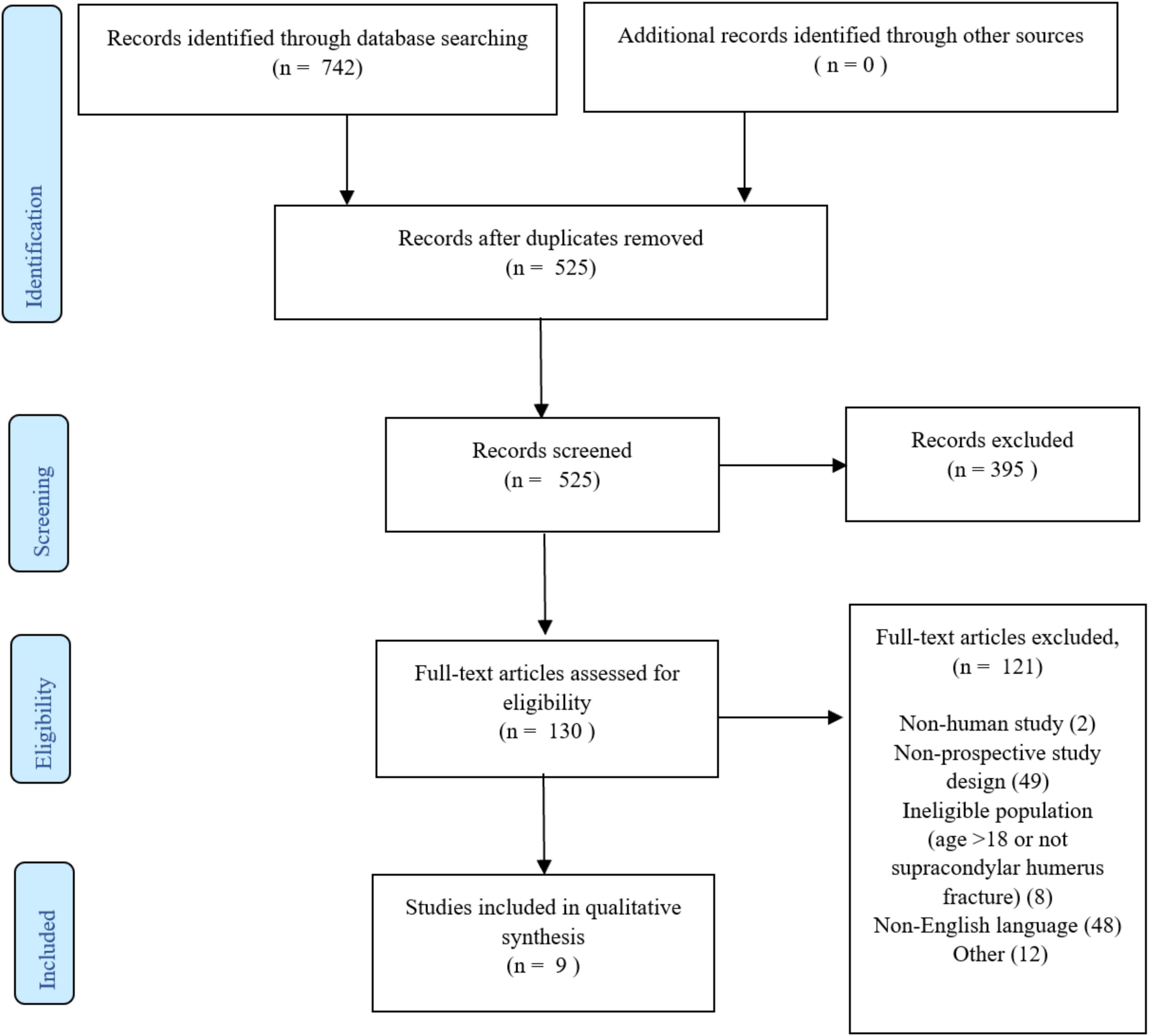
Figure 1. Prisma diagram.
Studies which met the inclusion/exclusion criteria, and contained clinical data, are described in Table 1. There were 3 RCTs, 1 prospective cohort study, and 1 quasi-experimental study. Studies were performed in North America, Europe, and Australia and were all published in the last 20 years. Interventions investigated in the studies were posterior splint, long arm cast, cuff and collar, and “Blount’s immobilization” (cuff and collar with elbow at 100–120 degrees of flexion). Time of immobilization was inconsistently reported but varied from 2 weeks to 4 weeks. Follow-up time ranged from 2 days to 48 weeks. Details of the risk of bias assessment can be found in Tables 2, 3.
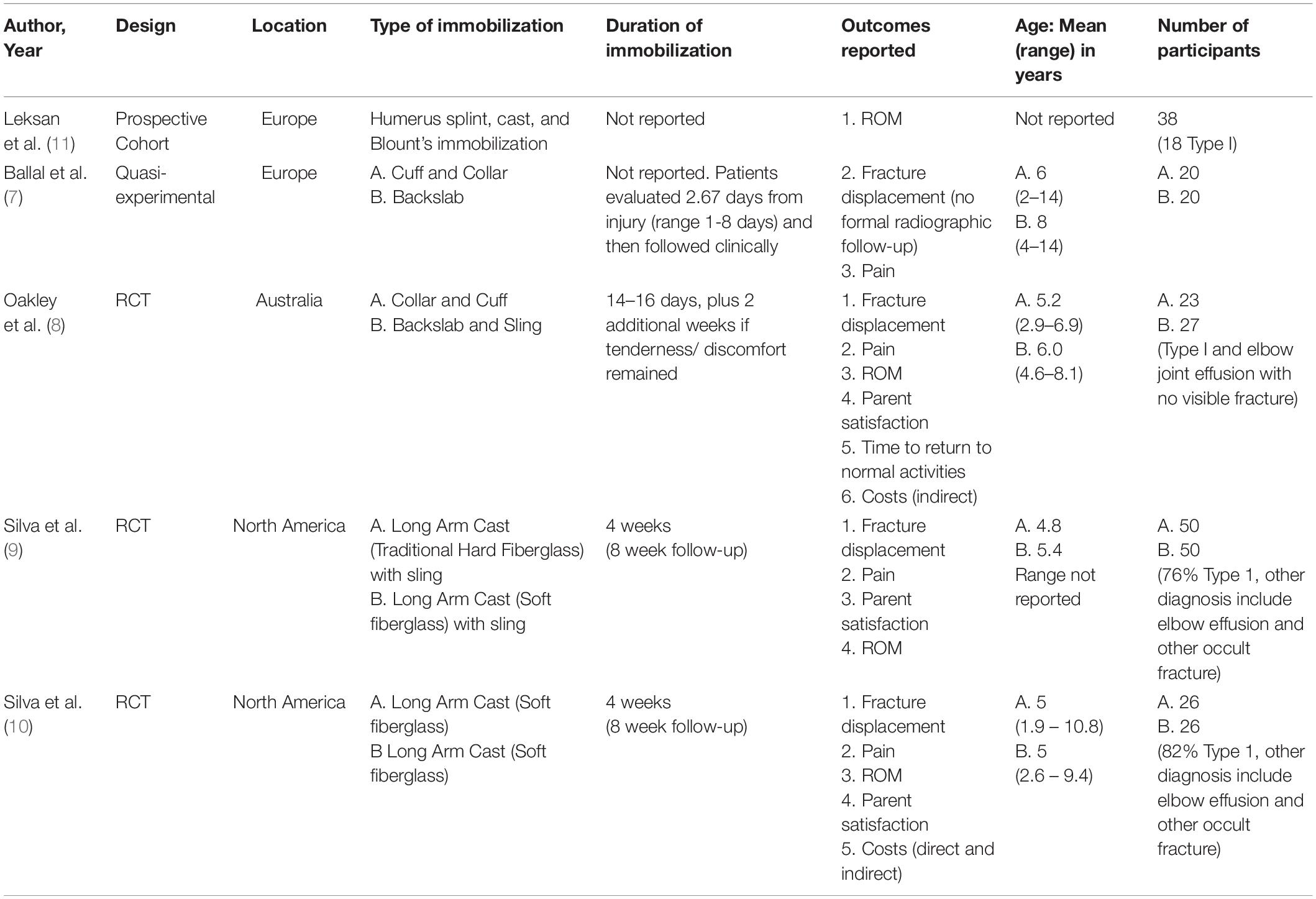
Table 1. Description of studies that met the inclusion criteria and included clinical outcome data.

Table 2. Risk of bias for prospective cohort studies - Newcastle–Ottawa score.
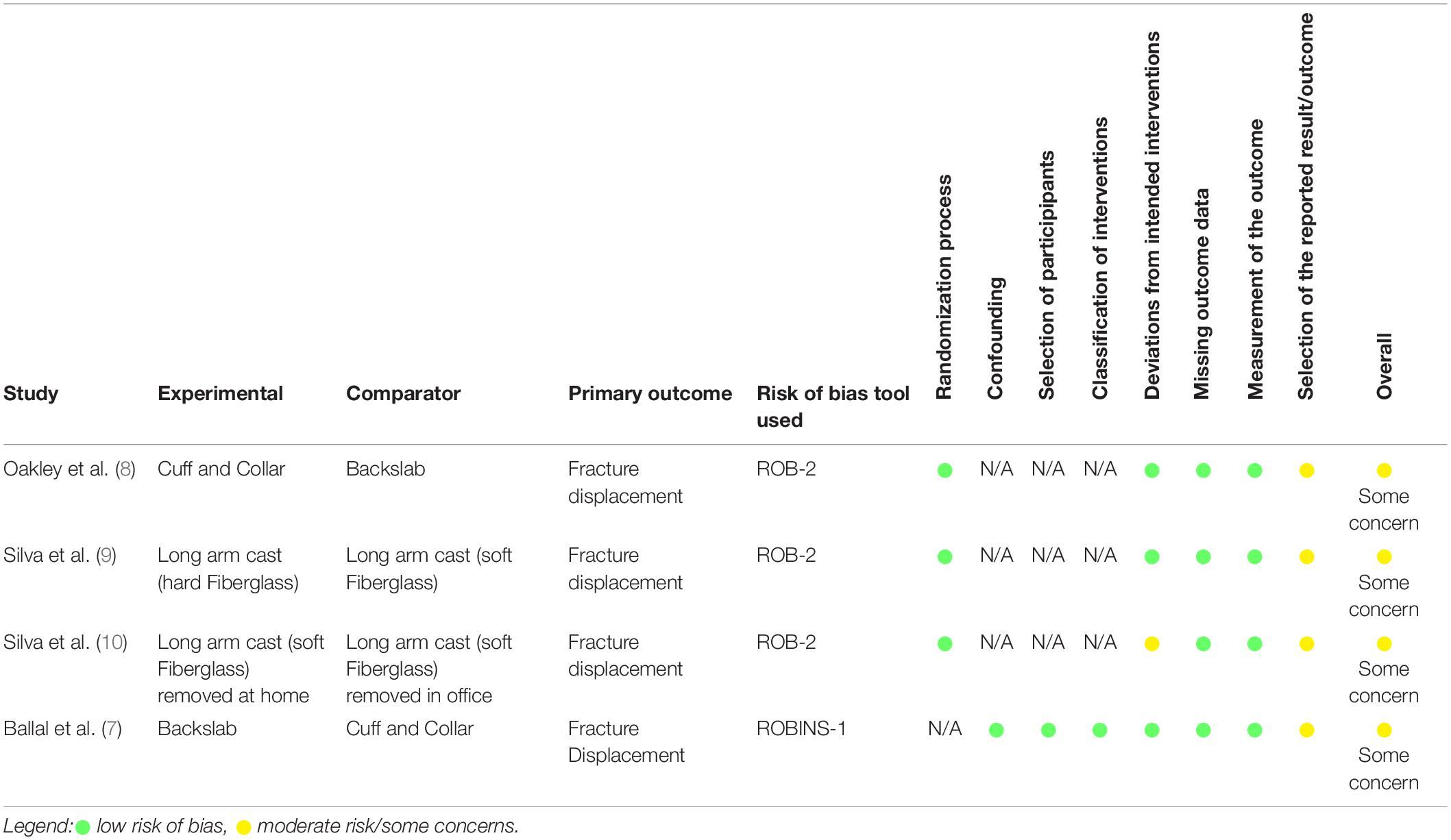
Table 3. Risk of bias for randomized control trials (RCTs) (ROB-2) and non-RCTs (ROBINS-1).
Two studies directly compared cuff and collar management to the use of a posterior splint (7, 8).
A quasi-experimental study by Ballal (7) included children who presented to a fracture clinic on an average of 2.7 days from injury. The patients had been treated with a cuff and collar or posterior splints based on the emergency physician preference. The posterior splints were placed with the elbow in “at least 90 degrees of flexion.” The authors report that “none of the fractures displaced during further management,” although there was no specific protocol for radiographic follow-up. The children treated with posterior splints had significantly less pain (3.4/10 vs. 7.2/10, p < 0.0001) and decreased regular analgesia use (4 times less, p = 0.0002) compared to those treated with cuff and collar. Furthermore, 85% of the patients treated with cuff and collar experienced sleep disturbance, compared to only 45% of the patients in the posterior splint group (7). Range of motion was not compared between the groups. There are moderate concerns with risk of bias since the study protocols were not published a priori (Table 3).
Oakley et al performed an RCT that investigated cuff and collar, compared to posterior splint (with the elbow placed at 90 degrees) (8). There were no cases of fracture displacement with either treatment, as measured on radiographs performed at the follow-up visit 12–16 days after injury. The primary outcome was the difference in pain intensity and duration and the parental or the patient’s willingness to use similar immobilization in the future. There was a trend toward decreased use of analgesia and duration of pain for the posterior splint compared to the cuff and collar (4 vs. 6 days, respectively), but statistical significance was not reported. Time to return to activity was also shorter in the posterior splint group (2 vs. 7 days, respectively). ROM restrictions was 50 degrees in the posterior splint group and 40 degrees in the cuff and collar group (p not reported). Differences in pain, analgesia use, and participation rates in usual activities had resolved by 4 weeks. Parent satisfaction, harms of immobilization, rates of parents who missed work, duration of missed work, and proportion of patients requiring days off from school/daycare demonstrated no differences between the methods of immobilization. Some concerns for risk of bias were identified for the Oakley study, as again there was no pre-specified, published protocol of outcomes prior to the commencement of the study (Table 3).
Long arm casts were investigated in two randomized control studies by Silva et al. (9, 10). In 2018, the authors compared traditional fiberglass to soft fiberglass casts. Both types of casts were placed with the elbow at 90–100 degrees of flexion and the forearm in neutral rotation (9). This study reported no evidence of fracture displacement between the two groups. ROM and parent satisfaction were also found to be equivalent between groups at the 8 week follow-up appointment. Pain scores between the groups showed inconsistent results over time with no difference at 1 week, significant differences at 4 weeks, and no difference at 8 weeks. Overall risk of bias assessment showed some concerns due to measurement of outcome variables, since there was no mention of blinding of the radiographic assessors to intervention (Table 3).
In 2019, Silva et al investigated different methods of cast removal to improve parent satisfaction: clinic removal (Group A) was compared to removal at home by parents via telehealth appointment (Group B) (10). Soft fiberglass casts were used in both the groups studied. There were no cases of fracture displacement in either group. At latest follow-up there was no significant difference in the mean ROM, with Group A: 147 degrees and Group B: 151 degrees (p = 0.5). Significant difference in the length of appointment time was found between the groups, with Group A: 110.7 min and Group B: 17.6 min (p < 0.001). When the parents in the traditional clinic visit learned about the increased appointment time, their satisfaction dropped and was statistically lower than the telehealth group, which was 76.4% for Group A compared to 97.7% for Group B (p = 0.05). Despite this difference in appointment time there was no significant difference in mean professional fee [Group A: $29.22, Group B: $22.51(p = 0.19)]. Quality assessment showed some concern for risk of bias for this study due to deviations from the intended intervention; parents from both groups removed the cast prior to the intended date and the data from these patients was not included in the final analysis (Table 3). In addition, the radiographic assessors measuring the primary outcome were not blinded to intervention.
Leksan et al. performed a prospective cohort study examining the functional status of the patient’s elbow after conservative treatment (11). They included 18 patients with Gartland type 1 fractures treated with a humerus splint, cast, or Blount’s immobilization. Results were not separated by the type of immobilization, but after completion of treatment, patients had an average ROM of 128.83 degrees, ranging from 110 to 140 degrees with a standard deviation of 8.65 degrees. No other clinical measures or outcomes were reported. This study is not of high quality, despite objective outcome measures. The patients selected were involved in traffic accidents (rollerblading or falling from a bicycle), which is a relatively high energy mechanism. In addition, it was unclear how the type of immobilization was ascertained, as there was no direct comparator, the length of follow-up was not described, and neither was loss to follow-up (see Table 2).
Three prospective studies met the inclusion criteria but did not contribute any outcome data to our systematic review, as they did not include radiographic data and the clinical data was not reported specific to Type 1 fractures (i.e., it was grouped with Type 2 and Type 3 fractures treated operatively) (12–14). A small prospective study by Pudas on the utility of MRI in elbow fractures included patients with supracondylar humerus fractures but no clinical or radiographic follow-up data was reported (15).
The quality of evidence in these studies is low, and therefore we cannot make strong conclusions on the effect of each type of immobilization on fracture displacement. However, the results of this systematic review suggest that there is no fracture displacement with the use of cuff and collar, posterior splinting, or long arm casts (7–10). These findings are in alignment with other available literature including a retrospective review of 53 cases, which demonstrated that the use of posterior splint resulted in minimal changes in fracture displacement (16). Specifically, they found only 1 case of change in the anterior humeral line (from posterior 1/3 of the capitellum to middle 1/3) and 1 case of change in the humeral capitellum angle by 7 degrees, which is considered to be within the normal interrater measurement variability.
Cuff and collar immobilization appears to have fewer benefits for patients, compared to posterior splints. The use of cuff and collar resulted in a delayed return to normal activities (8), more interrupted sleep, and increased average pain scores especially early in the injury phase (7). In addition, the cuff and collar did not result in pain scores at levels considered to be the minimum for adequate pain control (<30 mm on a 100 mm visual analog scale), whereas the posterior splint achieved pain levels below this threshold (8). It is therefore reasonable to conclude that the results of this study suggest that immobilization with a splint or cast is significantly better for patients than cuff and collar alone. There were no consistent differences in pain scores between traditional fiberglass and soft cast. When comparing cuff and collar to posterior splints, there was no difference in parent satisfaction. Parent satisfaction for long arm casts was also reported by Silva, with a significant difference in parent satisfaction only when parents were informed of the increased appointment time associated with typical clinic appointments as compared to telehealth visits (9, 14).
Two studies investigated the possible benefits of the use of “soft cast,” otherwise known as “peelable fiberglass” casts, utilizing a form of fiberglass which can be removed at the end of a period of immobilization by a parent at home (9, 10). Such “soft cast” has been investigated for immobilization of pediatric buckle fractures (17), and in small studies appear to result in high patient/parent satisfaction (18). The studies included in this review showed a similar improvement in parental satisfaction. However, these studies contained small patient numbers, and patients who removed their cast prematurely at home were excluded from the final analysis. Therefore, the effect of non-compliance during soft cast treatment of supracondylar humerus fractures is unknown. In addition, it is unclear whether “soft cast” treatment option is widely known, available, or considered reasonable to the pediatric emergency medicine and pediatric orthopedic surgery community. For these reasons, future investigation into this treatment method is warranted.
Orthopedic surgery visits have previously been reported to result in direct costs and societal costs due to loss of productivity for parents (19). Direct healthcare costs were only reported in one study of long arm casts, with no significant difference in cost despite an increased length of appointment in the traditional fiberglass cast (9). The type of immobilization directly impacts the follow-up required, and therefore has downstream societal costs. Rates of missed parental working days, duration of missed work, and proportion of patients requiring days off from school/daycare were only compared between cuff and collar and posterior splint in only one study, but no differences were reported (8).
High rates of improperly placed extremity splints have been reported in other literature, and associated with skin and soft tissue complications (20). However, direct physical harms of immobilization (or lack thereof) were not reported in any of the studies included in this review.
The ideal length of time required to immobilize Type I supracondylar humerus fractures is not clear from the evidence gathered in this review. In addition, an appropriate type of clinical follow-up care is not well defined. Telehealth has been advocated for delivering orthopedic clinical care during the COVID-19 pandemic (21), and is often used in rural/suburban areas, where it can greatly reduce the appointment times in the form of waiting and travel time (22). One small RCT compared telehealth clinical visits to traditional visits, and more research is warranted prior to changing the clinical follow-up methods.
This systematic review is limited in its conclusions by the heterogeneity of the individual studies, which investigated multiple forms of immobilization. There is no study focused on comparing posterior splints and casts, making it impossible to directly compare these two common treatments. The majority of studies also included patients with a variety of elbow injuries (such as occult elbow injuries), which may be more inherently stable than Type I injuries with a visible fracture line. Not all studies included a description of formal radiographic follow-up (8), which restricts the reliability of fracture displacement reporting. In addition, scarce information was presented on adverse events, and therefore it is unclear if these were not present or simply not recorded. A major limitation of the evidence is the short, formal follow-up period (average of 2.7 days to 8 weeks), meaning that long-term ROM and functional data are not available.
Despite the ubiquity of the fracture, there remains very limited high-quality evidence on the treatment of Type 1 supracondylar humerus fractures. In addition, there is significant heterogeneity in the intervention and outcome measures in the current literature. Based on the best available evidence, Type 1 supracondylar fractures are stable fractures with no evidence of displacement reported, regardless of the form of immobilization used. Posterior splint and circumferential long arm casts both provide adequate pain control and early return to activity, whereas cuff and collar alone has been shown to be comparatively less effective or even inadequate for pain control. Therefore, immobilization with a splint or cast is reasonable to recommend. It was not possible to determine the optimal duration and type of immobilization for these fractures. Interestingly, soft fiberglass casts may offer the potential of rigid immobilization with the option of cast removal at home, which, in a small study, resulted in reduced appointment times and increased patient/parent satisfaction while maintaining fracture stability. The results of this systematic review clarify the limitations of the existing evidence, and may help to serve as a guide toward the development of more definitive evidence and guidelines. Further research is needed to better determine the optimal management of Type 1 supracondylar humerus fractures in children.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
SCo: study design, data capture, measurements, analysis, and manuscript preparation and revision. KL: data capture, measurements, and analysis. AP and MB: study design, analysis, and manuscript preparation and revision. KC: analysis and manuscript preparation and revision. KS: study design and manuscript preparation and revision. SCa: study design, measurements, analysis, and manuscript preparation and revision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Katie O’Hearn, Msc (Children’s Hospital of Eastern Ontario Research Institute) for methodological assistance, and Margaret Sampson, MLIS, Ph.D., AHIP (Children’s Hospital of Eastern Ontario) for assisting with the development of electronic search strategies.
1. Landin LA, Danielsson LG. Elbow fractures in children. An epidemiological analysis of 589 cases. Acta Orthop Sand. (1986) 57:309–12. doi: 10.3109/17453678608994398
2. Holt JB, Glass NA, Shah AS. Understanding the epidemiology of pediatric supracondylar humeral fractures in the United States: identifying opportunities for intervention. J Pediatr Orthop. (2018) 38:e245–51. doi: 10.1097/BPO.0000000000001154
3. Wilkins KE. Fractures and dislocations of the elbow region. In: Rockwood CA, Wilkins KE, King R editors. Fractures in Children. Philadelphia, PA: Lippincott (1984). p. 363–575.
4. Victorian Paediatric Orthopaedic Network [VPON]. Supracondylar Fracture of the Humerus. Available online at: https://www.rch.org.au/clinicalguide/guideline_index/fractures/Supracondylar_fracture_of_the_humerus_Emergency_Department/ (accessed June 20, 2021).
5. Ganeshalingam M, Camp R. Supracondylar Fractures: ED Management. (2018). Available online at: http://www.sickkids.ca/POP/TIP/elbow/Supracondylar-fractures/Index.html (accessed January 18, 2020).
6. American Academy of Orthopaedic Surgeons [AAOS]. The Treatment of Pediatric Supracondylar Humerus Fractures Evidence Based Guideline and Evidence Report. (2011). Available online at: https://www.aaos.org/quality/quality-programs/pediatric-supracondylar-humerus-fractures/ (accessed January 17, 2020).
7. Ballal MS, Garg NK, Bass A, Bruce CE. Comparison between collar and cuffs and above elbow back slabs in the initial treatment of Gartland type I supracondylar humerus fractures. J Pediatr Orthop B. (2008) 17:57–60. doi: 10.1097/BPB.0b013e3282f3d162
8. Oakley E, Barnett P, Babl FE. Backslab versus nonbackslab for immobilization of undisplaced supracondylar fractures a randomized trial. Pediatr Emerg Care. (2009) 25:452–6. doi: 10.1097/PEC.0b013e3181ab7898
9. Silva M, Sadlik G, Avoian T, Ebramzadeh E. A removable long-arm soft cast to treat nondisplaced pediatric elbow fractures: a randomized, controlled trial. J Pediatr Orthop. (2018) 38:223–9. doi: 10.1097/BPO.0000000000000802
10. Silva M, Delfosse EM, Aceves-Martin B, Scaduto AA, Ebramzadeh E. Telehealth: a novel approach for the treatment of nondisplaced pediatric elbow fractures. J Pediatr Orthop B. (2019) 28:542–8. doi: 10.1097/BPB.0000000000000576
11. Leksan I, Nikolic V, Mrcela T, Lovirc I, Kristek J, Selthofer R Supracondylar fractures of the humerus in children caused by traffic. Coll Antropol. (2007) 31:1009–2013.
12. Spencer HT, Wong M, Fong YJ, Penman A, Silva M. Prospective longitudinal evaluation of elbow motion following pediatric supracondylar humeral fractures. J Bone Joint Surg Am. (2010) 92:904–10. doi: 10.2106/JBJS.I.00736
13. Schmale GA, Mazor S, Mercer LD, Bompadre V. Lack of benefit of physical therapy on function following supracondylar humeral fracture: a randomized controlled trial. J Bone Joint Surg Am. (2014) 96:944–50.
14. Masumbuko CK, Mutheke EG, Mbindyo B, Hawkes MT. Delayed surgery leads to reduced elbow range of motion in children with supracondylar humeral fractures managed at a referral hospital in Sub-Saharan Africa. Afr Health Sci. (2019) 19:2565–70. doi: 10.4314/ahs.v19i3.32
15. Pudas T, Hurme T, Mattila K, Svedström E. Magnetic resonance imaging in pediatric elbow fractures. Acta Radiol. (2005) 46:636–44. doi: 10.1080/02841850510021643
16. Cuomo V, Howard A, Hsueh S, Boutis K. Gartland type I supracondylar humerus fractures in children: is splint immobilization enough? Pediatr Emerg Care. (2012) 28:1150–3. doi: 10.1097/PEC.0b013e3182716fea
17. Witney-Lagen C, Smith C, Walsh G. Soft cast versus rigid cast for treatment of distal radius buckle fractures in children. Injury. (2013) 44:508–13. doi: 10.1016/j.injury.2012.11.018
18. Kuba MHM, Izuka BH. One brace: one visit: treatment of pediatric distal radius buckle fractures with a removable wrist brace and no follow-up visit. J Pediatr Orthop. (2018) 38:e338–42. doi: 10.1097/BPO.0000000000001169
19. Holm GV, Lurås H, Randsborg PH. The economic burden of outpatient appointments following paediatric fractures. Injury. (2016) 47:1410–3. doi: 10.1016/j.injury.2016.04.007
20. Abzug JM, Schwartz BS, Johnson AJ. Assessment of splints applied for pediatric fractures in an emergency department/urgent care environment. J Pediatr Orthop. (2019) 39:76–84. doi: 10.1097/BPO.0000000000000932
21. Parisien RL, Shin M, Constant M, Saltzman BM, Li X, Levine WN, et al. Telehealth utilization in response to the novel coronavirus (COVID-19) pandemic in orthopaedic surgery. J Am Acad Orthop Surg. (2020) 28:e487–92. doi: 10.5435/jaaos-d-20-00339
22. Sinha N, Cornell M, Wheatley B, Munley N, Seeley M. Looking through a different lens: patient satisfaction with telemedicine in delivering pediatric fracture care. J Am Acad Orthop Surg Glob Res Rev. (2019) 3:e100. doi: 10.5435/jaaosglobal-d-19-00100
Searches were conducted using an Ovid multi-database search, and duplicate records were removed online giving preference to MEDLINE, then Embase, with no field preference. Lines 1–4 are optimized for MEDLINE and the main question constructs are broken out in separate lines for clarity. Lines 5–11 are optimized for Embase and lines 12–15 are optimized for CENTRAL. The next lines associated the records to the database the search was designed for, combine those sets and then remove duplicate records and finally isolate the records from each database again so each can be downloaded and imported into the citation manager using a database-specific import filter.
Database specific: MEDLINE including Epub Ahead of Print, In-Process and Other Non-Indexed Citations (1946- November 13, 2020) and Embase (1947- 2020, November 13) and the CENTRAL Trials Registry of the Cochrane Collaboration (October 20 issue) using the Ovid interface.
1. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kf.
2. Casts, Surgical/or Splits/or [conservative or cast* or immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kf. or “Referral and Consultation”/
3. (child* or adolescent* or infan*).mp.
4. (1 and 2 and 3) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type 3 or type 111 or type iii or type three).ti.
5. gartland type i supracondylar humerus fracture/or humerus supracondylar fracture/or humeral supracondylar fracture/or distal humeral fracture/or (distal humerus/and fracture*.mp.)
6. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kw. not (femur* or femoral or distal radi*).ti.
7. 5 or 6
8. exp “casts and noninvasive traction devices”/or exp splint/or [conservative or cast* or Immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kw. or patient referral/
9. (baby or babies or newborn* or infan* or neonat* or preschool* or pre-school* or child* or pediatr* or paediatr* or teen* or adolescen*).mp.
10. (7 and 8 and 9) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type iii or type 111 or type 3 or type three).ti.
11. limit 10 to embase
12. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kw. not (femur* or femoral or distal radi*).ti.
13. [conservative or cast* or Immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kw.
14. (baby or babies or newborn* or infan* or neonat* or preschool* or pre-school* or child* or pediatr* or paediatr* or teen* or adolescen*).mp.
15. (12 and 13 and 14) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type iii or type 111 or type 3).ti.
16. 4 use medall
17. 11 use emczd
18. 15 use cctr
19. or/16-18
20. 19 use medal
21. 19 use emczd
22 19 use cctr
1. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kf.
2. Casts, Surgical/or Splits/or [conservative or cast* or immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kf. or “Referral and Consultation”/
3. (child* or adolescent* or infan*).mp.
4. (1 and 2 and 3) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type 3 or type 111 or type iii or type three).ti.
5. gartland type i supracondylar humerus fracture/or humerus supracondylar fracture/or humeral supracondylar fracture/or distal humeral fracture/or (distal humerus/and fracture*.mp.)
6. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kw. not (femur* or femoral or distal radi*).ti.
7. 5 or 6
8. exp “casts and noninvasive traction devices”/or exp splint/or [conservative or cast* or Immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kw. or patient referral/
9. (baby or babies or newborn* or infan* or neonat* or preschool* or pre-school* or child* or pediatr* or paediatr* or teen* or adolescen*).mp.
10. (7 and 8 and 9) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type iii or type 111 or type 3 or type three).ti.
11. limit 10 to embase
12. [(Supracondyl* adj2 fracture*) or gartland].ti,ab,kw. not (femur* or femoral or distal radi*).ti.
13. [conservative or cast* or Immobili* or backslab* or slab* or sling* or (cuff* adj2 collar*) or splint* or non-surg*].ti,ab,kw.
14. (baby or babies or newborn* or infan* or neonat* or preschool* or pre-school* or child* or pediatr* or paediatr* or teen* or adolescen*).mp.
15. (12 and 13 and 14) not (femur* or femoral or distal radi* or displaced or type ii or type 11 or type 2 or type two or type iii or type 111 or type 3).ti.
16. 4 use medall
17. 11 use emczd
18. 15 use cctr
19. or/16-18
20. 19 use medal
21. 19 use emczd
22. 19 use cctr
Keywords: pediatrics, systematic review, supracondylar humerus fractures, cast, splint
Citation: Coupal S, Lukas K, Plint A, Bhatt M, Cheung K, Smit K and Carsen S (2022) Management of Gartland Type 1 Supracondylar Fractures: A Systematic Review. Front. Pediatr. 10:863985. doi: 10.3389/fped.2022.863985
Received: 27 January 2022; Accepted: 19 April 2022;
Published: 19 May 2022.
Edited by:
Federico Canavese, Centre Hospitalier Regional et Universitaire de Lille, FranceReviewed by:
Łukasz Matuszewski, Medical University of Lublin, PolandCopyright © 2022 Coupal, Lukas, Plint, Bhatt, Cheung, Smit and Carsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sasha Carsen, c2NhcnNlbkBjaGVvLm9uLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.